
Massive Thrombotic Occlusion the Large Arteries -...
19
Massive Thrombotic Occlusion of the Large Pulmonary Arteries By K. P. BALL, M.D., M.R.C.P., J. F. GOODWIN, M.D., M.R.C.P., AND C. V. HARRISON, M.D., B.Sc. In 23 cases of massive thrombotic occlusion of the large pulmonary arteries thrombosis secondary to pulmonary embolism was the major cause, but a proportion (30 per cent) was considered to have primary thrombosis in situ. The pathologic criteria, symptoms, signs, and results of special investigations are given in detail, and the diagnosis, etiology, and precipitating factors are discussed. P ULMONARY heart disease resulting from thrombotic occlusion of the small pulmonary arteries due to re- peated emboli has been recognized for some years," 2 and the occurrence of repeated "silent" emboli to the lungs has been reported by Owen and associates.3 Massive thrombosis of the large pulmonary arteries is infrequently considered in the differential diagnosis of obscure cases of right-sided heart failure, although over 200 cases have been described in the literature. The first report apparently was that of H6lie in 1837,4 while Savacool and Charr5 collected 88 cases from the literature and added 12 of their own. Brenner6 found 4 cases in 100 unselected autopsies, and Middleton7 found 53 cases in autopsies over a period of 16 years at the Wisconsin General Hospital. In 5 of the 12 cases of widespread repeated pulmonary emboli reported by Owen and associates,3 the occlusion involved the large branches of the pulmonary artery. The condition has recently been reviewed by Magidson and Jacobson8 who have added 7 more cases. Massive thrombotic occlusion of the main pulmonary arteries has usually been described in association with other diseases, notably pulmonary tuberculosis, carcinoma of the lung, congenital heart disease, and various forms of acquired heart disease. It may, however, occur in the absence of any other disorder, but few cases have been diagnosed in life. The object of this paper is to present a total From the Central Middlesex Hospital, London, and the Departments of Medicine and Morbid Anat- omy, Postgraduate Medical School of London and Hammersmith Hospital, London, England. of 23 cases, 9 of whom were seen in life, while the remaining 14 were obtained from an examination of 7,000 autopsy records in the the Department of Pathology, Postgraduate Medical School. The diagnosis was made before death in 3 of the 9 patients seen in life, and autopsy confirmation was obtained in all cases. The diseases associated with thrombosis of the main pulmonary arteries included pulmo- nary disease (carcinoma of the lung, chronic bronchitis), cardiovascular disease (valvular disease, coronary artery disease, and congenital heart disease), and gastrointestinal disorders. In 4 cases no associated disease was present, although in 3 of these a generalized thrombo- embolic tendency of unknown etiology was manifested by repeated episodes of venous thrombosis at various sites. The cases without associated disease will be considered first. CASE MATERIAL Thrombosis of the Main Pulmonary Arteries without Associated Disease Case 1. A 48-year-old woman developed progres- sive dyspnea on exertion, followed by syncopal at- tacks in 1951. In 1952, she was found to have an iron-deficiency anemia and was treated with intra- venous iron. During treatment she developed signs of congestive cardiac failure, with peripheral edema, ascites, hepatic pulsation, and an elevated jugular venous pressure. There was a blowing systolic mur- mur over the pulmonary artery and down the left sternal border, and right ventricular enlargement. Fluoroscopy revealed large pulsating pulmonary arteries. She subsequently developed thrombosis of the left iliofemoral vein, for which she was treated with dicumarol. Congestive cardiac failure increased and Circulation, Volume XI V, November 1956 766 by guest on July 12, 2018 http://circ.ahajournals.org/ Downloaded from
-
Upload
dinhkhuong -
Category
Documents
-
view
222 -
download
0
Transcript of Massive Thrombotic Occlusion the Large Arteries -...

Massive Thrombotic Occlusion of the Large
Pulmonary ArteriesBy K. P. BALL, M.D., M.R.C.P., J. F. GOODWIN, M.D., M.R.C.P., AND C. V. HARRISON, M.D., B.Sc.
In 23 cases of massive thrombotic occlusion of the large pulmonary arteries thrombosis secondaryto pulmonary embolism was the major cause, but a proportion (30 per cent) was considered tohave primary thrombosis in situ. The pathologic criteria, symptoms, signs, and results of specialinvestigations are given in detail, and the diagnosis, etiology, and precipitating factors are discussed.
P ULMONARY heart disease resultingfrom thrombotic occlusion of thesmall pulmonary arteries due to re-
peated emboli has been recognized for someyears," 2 and the occurrence of repeated"silent" emboli to the lungs has been reportedby Owen and associates.3Massive thrombosis of the large pulmonary
arteries is infrequently considered in thedifferential diagnosis of obscure cases ofright-sided heart failure, although over 200cases have been described in the literature.The first report apparently was that of H6lie in1837,4 while Savacool and Charr5 collected 88cases from the literature and added 12 of theirown. Brenner6 found 4 cases in 100 unselectedautopsies, and Middleton7 found 53 cases inautopsies over a period of 16 years at theWisconsin General Hospital. In 5 of the 12cases of widespread repeated pulmonaryemboli reported by Owen and associates,3 theocclusion involved the large branches of thepulmonary artery. The condition has recentlybeen reviewed by Magidson and Jacobson8 whohave added 7 more cases.
Massive thrombotic occlusion of the mainpulmonary arteries has usually been describedin association with other diseases, notablypulmonary tuberculosis, carcinoma of the lung,congenital heart disease, and various forms ofacquired heart disease. It may, however,occur in the absence of any other disorder, butfew cases have been diagnosed in life.The object of this paper is to present a total
From the Central Middlesex Hospital, London,and the Departments of Medicine and Morbid Anat-omy, Postgraduate Medical School of London andHammersmith Hospital, London, England.
of 23 cases, 9 of whom were seen in life, whilethe remaining 14 were obtained from anexamination of 7,000 autopsy records in thethe Department of Pathology, PostgraduateMedical School. The diagnosis was madebefore death in 3 of the 9 patients seen in life,and autopsy confirmation was obtained in allcases.The diseases associated with thrombosis of
the main pulmonary arteries included pulmo-nary disease (carcinoma of the lung, chronicbronchitis), cardiovascular disease (valvulardisease, coronary artery disease, and congenitalheart disease), and gastrointestinal disorders.In 4 cases no associated disease was present,although in 3 of these a generalized thrombo-embolic tendency of unknown etiology wasmanifested by repeated episodes of venousthrombosis at various sites.The cases without associated disease will be
considered first.
CASE MATERIAL
Thrombosis of the Main Pulmonary Arterieswithout Associated DiseaseCase 1. A 48-year-old woman developed progres-
sive dyspnea on exertion, followed by syncopal at-tacks in 1951. In 1952, she was found to have aniron-deficiency anemia and was treated with intra-venous iron. During treatment she developed signsof congestive cardiac failure, with peripheral edema,ascites, hepatic pulsation, and an elevated jugularvenous pressure. There was a blowing systolic mur-mur over the pulmonary artery and down the leftsternal border, and right ventricular enlargement.Fluoroscopy revealed large pulsating pulmonaryarteries.
She subsequently developed thrombosis of theleft iliofemoral vein, for which she was treated withdicumarol. Congestive cardiac failure increased and
Circulation, Volume XI V, November 1956766
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from

BALL, GOODWIN, AND HARRISON
tr'icuspid incompetence developed. Thrombosis ofthe inferior vena cava was suspected. Treatmentwith digitalis, mercurial diuretics, and ion-exchangeresins was without effect during any of her repeatedadmissions to the Central MXiddlesex Hospital, andon August 30, 1953, she was transferred to Hammer-smith Hospital.On examination she was an anxious, slightly cya-
nosed woman with orthopnea and cold extremities.The pulse was of small volume and regular. The
FIG. 1. Case 1. lPosteroanterior roentgenogram ofthe chest showing enlargement of the right ventricle,main pulmonary trunk, and right main branch. Thelung fields are underfilled.
jugular venous pressure was raised to 8 cm. abovethe sternal angle with a large systolic wave, indi-cating tricuspid incompetence. There was extensiveedema. The cardiac impulse was diffuse, tapping,and with sternal pulsation, indicating right ven-tricular hypertrophy. The second heart sound wasnormally duplicated and not accentuated. A grade4 systolic murmur was maximal in the third andfourth left intercostal spaces. The blood pressurewas 90/60 mm. Hg. The lungs were clear, and therewas aseites. The liver was enlarged and pulsated insystole. The spleen was not enlarged.
Chest x-ray and fluoroscopy (fig. 1) showed alarge right ventricle, considerable enlargement ofboth pulmonary arteries, which did not pulsate, andoligemic lung fields. An electrocardiogram showedsinus rhythm, right ventricular, and right atrial hy-pertrophy (fig. 2). The phonocardiogram showed asystolic murmur maximal in midsystole in the pul-monary area. Liver function tests were normal, ex-cept for albumin of 2.6 and globulin of 3.5 Gm. percent. The blood count was normal, with a hemo-globin of 90 per cent.On cardiac catheterization the right atrial pres-
sure was 11/6 mm. Hg. The tracing was typical oftricuspid incompetence. The right ventricular pres-sure was 90/18, with a mean of 35 mm. Hg. Thepulmonary artery was not entered. There was noevidence of a septal defect with left-to-right shunt.The arterial oxygen capacity was 94 per cent satu-rated. The cardiac output by the Fick method was1.6 L./min. It was concluded that there were rightventricular hypertension, tricuspid incompetence,low cardiac output, and no cardiac shunt.
,V49
Deso_itb . IP_;.,
FIG. 2. Case 1. Electrocardiogram, showing augmented P waves indicating right atrial enlarge-ment, and qR patterns in leads V4R and V, indicating right ventricular hypertrophy.
767
va1,
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from
MASSIVE THROMBOTIC OCCLUSION OF LARGE PULMONARY ARTERIES
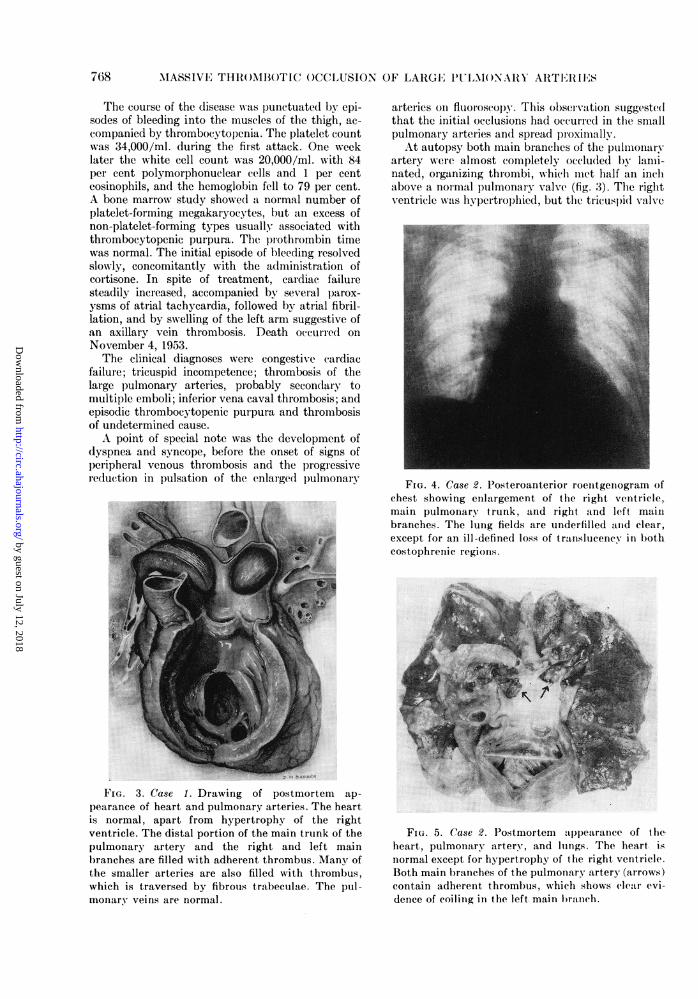
The course of the disease was punctuated by epi-sodes of bleeding into the muscles of the thigh, ac-companied by thrombocytopenia. The platelet countwas 34,000/ml. during the first attack. One weeklater the white cell count was 20,000/ml. with 84per cent polymorphonuclear cells and 1 per centeosinophils, and the hemoglobin fell to 79 per cent.A bone marrow study showed a normal number ofplatelet-forming megakaryocytes, but an excess ofnon-platelet-forming types usually associated withthrombocytopenic purpura. The prothrombin timewas normal. The initial episode of bleeding resolvedslowly, concomitantly with the administration ofcortisone. In spite of treatment, cardiac failuresteadily increased, accompanied by several parox-ysms of atrial tachycardia, followed by atrial fibril-lation, and by swelling of the left arm suggestive ofan axillary vein thrombosis. Death occurred onNovember 4, 1953.The clinical diagnoses were congestive cardiac
failure; tricuspid incompetence; thrombosis of thelarge pulmonary arteries, probably secondary tomultiple emboli; inferior vena caval thrombosis; andepisodic thrombocytopenic purpura and thrombosisof undetermined cause.A point of special note was the development of
dyspnea and syncope, before the onset of signs ofperipheral venous thrombosis and the progressivereduction in pulsation of the enlarged pulmonary
FIG. 3. Case 1. Drawing of postmortem ap-pearance of heart and pulmonary arteries. The heartis normal, apart from hypertrophy of the rightventricle. The distal portion of the main trunk of thepulmonary artery and the right and left mainbranches are filled with adherent thrombus. Many ofthe smaller arteries are also filled with thrombus,which is traversed by fibrous trabeculae. The pul-monary veins are normal.
arteries on fluoroscopy. This observation suggestedthat the initial occlusions had occurred in the smallpulmonary arteries and spread proximally.At autopsy both main branches of the pulmonary
artery were almost completely occluded by lami-nated, organizing thrombi, which met half an inchabove a normal pulmonary valve (fig. 3). The rightventricle was hypertrophied, but the tricuspid valve
FIG. 4. Case 2. Posteroanterior roentgenogram ofchest showing enlargement of the right ventricle,main pulmonary trunk, and right and left mainbranches. The lung fields are underfilled and clear,except for an ill-defined loss of translucency in bothcostophrenic regions.
FIG. 5. Case 2. Postmortem appearance of theheart, pulmonary artery, and lungs. The heart isnormal except for hypertrophy of the right ventricle.Both main branches of the pulmonary artery (arrows)contain adherent thrombus, which shows clear evi-dence of coiling in the left main branch.
768
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from

IBALL, GOODWIN, AND HARRISON
was not dilated. The mitral and aortic valves werenormal, as were the septa. There was no evidenceof thrombosis of the caval, iliac, or femoral veins.
Antemortem thrombus extended into the periph-eral branches of the pulmonary artery on both sides,being more recent on the left. No pulmonary infarctswere present. The thrombus in the main pulmonaryarteries and their immediate branches was pale andhad clearly been deposited in layers. In the smallerarteries the lumina were frequently broken up byfibrous strands into a number of channels, and thesein their turn were occluded by recent red thrombi.Histologic examination confirmed that the thrombusin the main arteries had been deposited in layers, ofquite different ages, the deeper being well organizedand the superficial being relatively recent. There wasno evidence of atheroma of any significance and noneof arteritis.The bronchial arteries were more prominent and
dilated than normal. The lung parenchyma andbronchi were normal.The liver was markedly congested and showed
changes of early cirrhosis. The bone marrow wasnormal; the spleen was very congested.
Case 2. A 56-year-old woman began her illnesswith swelling and tenderness of the calf, followed 1month later by dyspnea on exertion and orthopnea.Two weeks later she developed pleuritic pain on theright side, and suffered 2 hemoptyses. Death oc-curred suddenly, despite anticoagulant therapy.
On examination she was a dyspneic, cyanosedwoman, with a small regular pulse, elevated jugularvenous pressure, and edema of the legs. There wasdoubtful enlargement of the light ventricle, thesecond heart sound was normal, and there was aloud systolic murmur over the pulmonary artery.The blood pressure was 140/80 mm. Hg. There wasdullness at the base of the right lung, but no club-bing of the fingers.
X-ray film of the chest showed large main pul-monary arteries and right ventricle. The lungs wereclear except for an opacity at the right costophrenicangle (fig. 4). (The patient was too ill for fluoros-copy.) Electrocardiogram showed low voltage withfirst degree atrioventricular block, and doubtfulright ventricular hypertrophy.The clinical diagnosis was thrombosis of main pul-
monary arteries, probably secondary to repeatedpulmonary emboli.At autopsy the main pulmonary artery was oc-
cluded by an adherent laminated thrombus thatshowed coiling (fig. 5). No underlying disease of thepulmonary artery was present. The appearanceswere those of embolism with secondary thrombosis,the age of the thrombus being consistent with theduration of the symptoms. The heart was normal,apart from hypertrophy of the right ventricle. Bothfemoral veins were thrombosed. No other diseasewas present.The diagnosis was suspected in these patients be-
TABLE 1.-Cases* of Thrombosis of the Large Pulmonary Arteries without Associated Disease
SexAge
3 FMF 46
4HB
F79
History
Attacks offever, sub-sternalpain, he-moptysis,and dysp-nea; diedsuddenly
Admitted be-cause ofsevere
epistaxis;vomitedtwice; diedsuddenly 9days afteradmission
Clinical findingsand progress
Signs of ve-nous throm-bosis inlegs;fluid inright chest;apical sys-tolic mur-mur; triplerhythm;falling B.P.
No abnormalsigns; B.P.130/80;slight albu-minuria
X -ray
Heart en-
larged
* Cases 1 and 2 discussed in detail in text.
Electro-cardiogram
Left bundle-branchblock;largerightatrium, ?largerightventricle
Autopsy findings
Description
Thrombosis of mainpulmonary arteries toright lower and upper
lobes; dissectionshows emboli em-
bedded in localthrombus; histologyshows organizing
clots; multiplethromboses in legand arm veins
Thrombosis of rightand left main pulmo-nary arteries; recog-
nizable embolus liesin mass of secondarythrombus; histologyshows severe pulmo-nary atheroma; clotlies over atheromatousplaques; no source forembolus
Infarctsin lungs
4+
Comments
Thrombosissecondary toembolism;generalizedthrombo-embolicdisease; ?cause
Thrombosissecondary toembolism;generalizedthrombo-embolic dis-ease; ? cause
No.
769
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from

m~~~~_
ba
e P4
a 0 D=4.> r . ~
.. m ce ¢ te
770 MASSIVE THROMBOTIC OCCLUSION OF LARGE PULMONARY ARTERIES
,
Cdo.¢
X) ° , C)
O ;- c UQ~ a) :
Q-0 ¢ + .= .=~~~~~~c-4,
c0
E Cd
,= O1
4)
Ern
-0
0
rn~
ce * £
f.
c3
rn+0
cs* tvi,
o
_>
3
t!;
.S3
3* v^;
ocscs,cs
.;
,
oI3
CD*<tCDoo
o
*
q)rt
,;
¢
4_ O
P,
c 0
W; O
*-Csi
gC4._
m3 ~
rnlc) rnM -z
c)t .)
to._
;gr.kr
._l
cn
-
cz._
D._
* $*o . __s K
._ ;_ e
*e z
od
*_ b_
.rnrnc; ¢._;r .cs EC:5 *_
:3u:
rt:
V ¢*;
rrnce ce rm i 02 C) rnCe
LO-4 O cece °4- C>
ccCd
om., o rn
~ C ~ -
bemm ;.~~~~~~~~~~~~~~~~~~~ -0~~~~~~~y 1
F) t_g Vv to
6 t, P.z p
cc Pc
S.. c;l Q _cE cEs ,E¢;4
, e ~ _ r
ce *B Q d e
~ a)$:. cd9) 0.> - - - 'n--- cd r. En ce .~M W 0 :., W M
.~ M $:: P-.a) 1$-. $:L, -4- -4..AM o P4 m..biG m 5.1 m
o P. 'M cd >, 0L.. o a) 0. -o
P..
b.0
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from

BALL, GOODWIN, AND HARRISON
cause of progressive right ventricular failure asso-ciated with signs of peripheral venous thrombosis.The pulmonary systolic murmur and normal pul-monary component of the second heart sound sug-gested obstruction to the pulmonary arteries nearthe pulmonary valve, rather than in the smallbranches, when signs of pulmonary hypertensionmight have been expected. Virtual disappearance ofpulmonary artery pulsation in case 1, strongly fa-vored the main branches as the site of obstruction.Progressive diminution in pulsation has been notedin cases of atrial septal defect with thrombosis of themain pulmonary arteries by Canada and co-workers.9In case 1, the original finding of marked pulsationof the main pulmonary arteries, after signs of cardiacfailure had appeared, suggests that retrogradethrombosis may have followed multiple emboli inthe small branches.
The remaining 2 cases without associated diseases(case 3 and case 4) were not seen in life by the au-thors, and their clinical findings are therefore verybriefly summarized in table 1.
Thrombosis of the Main Pulmonary ArteriesAssociated with Mitral StenosisMitral stenosis was the most frequent single dis-
ease associated with pulmonary artery thrombosisin the series, and was present in 6 of the total of 23patients. Five of these 6 patients were seen duringlife, but the diagnosis of thrombosis of the pulmonaryarteries was not made. The symptoms and signs at-tributable to mitral valve disease overshadowed anyreferable to pulmonary artery thrombosis in all ex-cept 3 patients, who, in retrospect, might have beencorrectly diagnosed in life. Two of these 3 patientsare described in detail.
Case 5. A woman, aged 55, complained of pro-gressive dyspnea on exertion for 11 years. More re-cently substernal pain on exertion, relieved by rest,was noticed, and repeated hemoptyses occurred for4 weeks. She also had a cough with sputum. Onexamination she was an orthopneic woman with amalar flush. The arterial pulse was of small volume,and there was an augmented 'a' wave in the jugularvenous pulse. The diffuse tapping cardiac impulsesuggested right ventricular hypertrophy. The secondheart sound was split with marked accentuation ofthe pulmonary element, and there was a very faintpulmonary diastolic murmur. Triple rhythm and asoft middiastolic murmur were heard at the apex.The blood pressure was 110/60 mm. Hg. There wasan effusion at the base of the right lung and slightclubbing of the fingers. The abdomen was normaland there was no peripheral edema.
The hemoglobin was 99 per cent, the white cellcount was 18,000, and the platelet count was350,000/ml.
Fluoroscopy and roentgenogram of the chest(fig. 6) showed enlargement of the right ventricle.
The main pulmonary arteries were grossly enlargedand pulsating slightly. The right main branch wasirregular in contour. The left atrium was enlarged,and there was a right pleural effusion. There was arounded shadow in the right lower midzone. An elec-trocardiogram showed right ventricular hyper-trophy.On cardiac catheterization, the right ventricular
pressure was 70/10 mm. Hg and the pulmonaryartery pressure was 74/52 mm. Hg. The cardiac out-put was 2 L./min. An angiocardiogram showed alarge right ventricle and very large pulmonary ar-teries. No shunt was visualized. The shadow in theright midzone appeared to become denser, suggestingpulmonary artery origin. There was poor contrastand poor filling of the distal pulmonary arteries.The clinical course was marked by repeated pul-
monary infarcts and increasing cardiac failure. Thepatient improved sufficiently to be discharged fromhospital, but was readmitted in acute circulatoryfailure, with an impalpable pulse, high venous pres-sure, and rapid atrial fibrillation; death occurredwithin 24 hours.The clinical diagnosis was pulmonary hyperten-
sion, probably due to mitral stenosis.At autopsy there was tight mitral stenosis. The
distal half of the main pulmonary artery containedlaminated antemortem thrombus extending downthe right and left main branches. No thrombosis wasfound in the femoral or abdominal veins. There weremultiple pulmonary infarcts.On histologic examination, in both main pulmo-
nary arteries, the thrombus lay over severe athero-mas and was deposited in successive layers, the deep-est being well organized. It was thought to be athrombus in situ.
In this patient the flow through the mitral valvemust have been so reduced as to prevent almost com-pletely the production of the typical murmurs. Thelow cardiac output would favor stasis and thrombosisin the pulmonary arteries, especially in the presenceof local disease and severe pulmonary hypertension.Poor pulsation of the main pulmonary arteries isunusual with severe pulmonary hypertension; if thishad been associated with the abnormal contour ofthe right main pulmonary artery and signs of re-peated pulmonary infarcts, the correct diagnosismight have been made.
Case 6. A woman, aged 27 years, complained ofdyspnea on exertion for 7 years; 3 weeks before ad-mission the dyspnea increased and was accompaniedby peripheral edema and cough with purulent spu-tum. There were several attacks of acute dyspneaand syncope. On examination there were signs ofmitral stenosis, with right ventricular hypertrophy.The pulmonary component of the second heart soundwas accentuated. The jugular venous pressure was4 to 5 cm. above the sternal angle. An early diastolicmurmur of either pulmonary or aortic incompetence
771
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from

7MASSIVE1 THR(O)MBO()TIC OCCLUSION OF LARGE 'PULMONARY ARTERIES
FIG. 6. Case 5. llosteroanterior roentgenogram ofthe chest showing enlargement of the right ventri-cle and enormous distention of the main and leftmain pulmonary arteries. The right main pulmonaryartery is also greatly enlarged, and its contour isirregular. There is a large effusion in the right cos-tophrenic angle, overlying a pulmonary infarct.
and a fourth heart sound were heard. The pulse wasregular and of normal volume, and the blood pres-sure was 120/65 mm. Hg. There were peripheraledema and hepatomegaly. Bronchial breathing wasaudible at the base of the iight lung, and scatteredrales were heard throughout Loth lungs. Roentgeno-gram of the chest and fluoroscopy showed a lack ofmarked pulsation of the main pulmonary arteries.There was enlargement of the right atrium and ven-tricle, pulmonary artery, and left atrium. An elec-trocardiogrami showed right ventricular and atrialhypertrophy, with first dlegrec atrioventricular block.
There was steadc- deterioration and (leath in con-gestive heart failure.
At autopsy there was mitral stenosis and aorticincompetence, with a thromibus in the right atrium.The iight ventricle was hvpcrtrophied. The lungsshowed edema, bronchitis, and pulmonary infarets.There was adherent thrombus in the right main pul-monar.v artery. The smaller arteries showed hyper-plasia of the internal elastic lamina, fibrinoid necro-sis, a(utC arteritis, and local thrombosis (fig. 7).There was no source for emboli other than possiblythe right atrium and the lesion was considered to bea thronmbus in situ in the pulmonary artery, over-
lying severe vascular disease.
FIG. 7. Case 6. Oblique section of a small pulmonary artery. On one side is a pla(lue of atheroma(arrow), and over this, filling the lumen, is antemortem thrombus, apparently formed in situ. (X 90.Weigert's elastic stain and van Giesen's stain.)
772
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from

BALL, GOODWIN, AND HARRISON
The rapidly progressive deterioration and conges-tive heart failure, coupled with the episodes of acutedyspnea and fainting, in this case might have sug-gested the diagnosis.
The details of the other cases of mitral stenosis areoutlined in table 2 (cases 7-10). The signs of throm-bosis of the pulmonary arteries were obscured incases 7, 9, and 10, by other complications of themitral valve disease, but might have been suspectedin case 8, since there were episodes suggestive ofrepeated pulmonary infarction.
Four of the 6 patients with mitral stenosis hadapparently developed a primary thrombosis in situ,and this aspect of pulmonary artery thrombosis isconsidered later.
OVER-ALL FINDINGS
Thrombosis of the Main Pulmonary Arteries inAssociation with Other DiseasesThese cases are outlined in table 3. With the
exception of patients no. 20 and 22, who wereseen in life, the remainder were studied onlyretrospectively from case notes and autopsyreports. In many patients any signs or symp-toms attributable to pulmonary arterythrombosis were completely overshadowed bysome other clinical catastrophe, such as acerebral vascular accident.
Clinical PictureSymptoms. The commonest was dyspnea;
symptoms compatible with pulmonary infarc-tion (pleural pain or hemoptysis) were presentin 11 of the 23 patients. Fainting was a strikingsymptom in 3 cases. In most cases, however,the symptoms of the associated or underlyingdisease overshadowed any due to the pulmo-nary lesion itself. Several patients died incoma; while in the group with mitral disease,many of the symptoms could be accounted forby the valvular lesion.
Physical Signs. The commonest sign washypertrophy of the right ventricle, but in anumber of these patients it was due to mitralstenosis. The same was true of accentuation ofthe pulmonary element of the second heartsound and of abnormalities in the centralvenous pulse. Two patients had a systolicmurmur in the pulmonary area, and neitherhad any cardiac lesion other than right ven-tricular hypertrophy. The diagnostic value ofthe pulmonary systolic murmur and normal
second heart sound in these patients is discussedlater. The arterial pulse was small in volume in5 patients, 1 of whom had mitral disease.Congestive cardiac failure was noted in 10patients, but there were signs suggestingperipheral venous thrombosis in only 3, while4 patients had no signs referable to disease ofthe heart or lungs.Mode of Death. This was gradual in 18 and
sudden in 5.Radiology. Adequate chest films were avail-
able in 14 patients. Right ventricular and pul-monary artery enlargement was a constantfeature and the lung fields appeared under-filled in 3 patients, (1 of whom, however, hadpulmonary atresia). Restricted pulsation of themain arteries was striking in 2 patients, but inmany cases fluoroscopy was not possible. In 1patient with mitral stenosis (case 5), anirregular enlargement of the right pulmonaryartery due to the thrombus partly obscured bya large pleural effusion was seen (fig. 6).The important radiologic signs were under-
filled lung fields and enlarged, poorly pulsatingmain pulmonary arteries.
Electrocardiography. Recent, adequate elec-trocardiograms were available in 12 patients:8 showed right ventricular hypertrophy (4gross and 4 moderate), and 4 showed rightatrial hypertrophy. There was no evidence ofenlargement of the right heart in 4 patients.
Pathologic Findings in Twenty-three Cases ofMassive Thrombosis of the Large PulmonaryArteriesThrombosis was considered to be secondary
to embolism in the majority of the cases, butappeared to have arisen in situ in a minority.
In making this differentiation we haverelied mainly on the naked-eye appearances ofthe dissected specimen, supplemented by thehistologic appearances. One source of error thatwe cannot exclude is the initiation of throm-bosis by a small, undetected embolus. Sincewe are concerned here with thrombosis in thelarge pulmonary arteries where only massiveemboli are likely to lodge, we believe that thissource of error is not great.Table 4 sets out the criteria we have used
in the differentiation of primary from secondary
773
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from

l~~~~~~~~~~~~h toGt~~~~~~~~~~~~~~~~~~0c
2~~~~~~~~~~~~~U cc:
m m
oe 02 7 i.., ....... c) uUi
V)~~~~~~~~~~~~~~s c> [- 5 c at atNe W
774 MASSIVE THROMBOTIC OCCLUSION OF LARGE PULMONARY ARTERIES
0¢~
To -4->.-
~ c
4ic,vE9U
e A.,.. Cd + To 0o
her.
a
A:
mQ m
-0
; _c
.0
aC) ro =-4-' .o O
J20me2
0n+ET
:302 o
P. U2Q0
~r.S.
. -
¢.S_ - v.
~ C
' wo.C: s.
biDu0C.~ C~ TCt 'V
Mq Q
E mcS0 Q;.=.CX;
._i OcMr3t-.VtP.4
C.
1.U)
en
Is
Is* and
To-
s
s
ToIsAt
DO
;qua
To
's
At<sAtToo
To
1.ce
¢
6 ~ .zz 1-4 .t
0
02 M m
ce biD - U2 W:j 0
k--4
To
O +
0 c
* S-
-W
muoEEl-- z
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from
7-, 0 ;-.4 (40
m 0 0 0:2 -0 C .c00 0 .: .~ g E. >, .0 C) C) o
ct 421 Cd 0Go 0 .4 0 a) Cd0 4.5 m 4a) -4_;0 .4J0
P.. W
+ + 0
bl) 0 0 cc ct ccc) F-4 ~ 0 9) 00 0 0 :2 ce cd P.1 0
0 0 Cd F.0 W r-4 L#-,02 Cd
Z: be cj c)CdCd ce c) J20 a) bl) 76. m
CD .> m +.;, W 0 0;-4 4- 0 C ;m -4- Or, cd5-5 cd 0 -0 0
.~ 00
UD big ce Cd7..4 94-4 M 0 0 C) 0-C 4d(1) 0 $:: .C cj
0 ,~ P, ~ .4 0ce C) cc 5:: P.4 g.
ce cj4. P4 W0 b£ r. c! ce ce j2 ce cc;. r4 0 4J c.. bo .-P -4-J cc0 ce
'd be.~ cd-m L4ce 0 ce cjc) o ce ce
C.) c) m cd :S g:$.., 4 0 L#-4 be cd -4 cd m 4.;lce C) 0 o ES ho o ZPL.4 o c0 m be ce E "F4 CJ bib m
4->ce
0 ce cl
cd ce
cc c) ce r,ctce
ce ;. $., ccjP.4 z be o m cc ce
cj 0 F..,CP:
b£ cj M CJbe -C +
0 cj 0 10 0 0cc r. ccC) C, 07-4 m m m M ce11:5 .i >.. $:. 4 0 0 b£
W cc $:: .O 0 U2 0 0 he cd4.cj c) . - -4-. cd4-4 :2 Q) d C.? -0 m ce
c) Q " C -4.>9: M C) ce cd o.2 (L) Z
4JJ W4
cj C) "cj 0 r.
bi) 0cc0 CS gi :2 c) 0
ct 9: cj cc ce c;. 14 C. c) ce 4-4 9 Cd M cj -00
Cd b£ c) .4j C...,bl) r. W
0 4_) ce -4-.ce cd9 c)
W04. cj g m c ccC4-4 C4-4 ;-4 ce c ;., Q) "
U2 CJcc C4. ce m P. Wm m bi) 0 0
0 0 cebc cjc: ce W0 cd -4-
0c) P.4
0 > -4-5
A4ce ce 0
o r4C)
ce 4.?2 4.50 0C4-4
0 ce 0 0ce :2
oo c
r_ cc
775BALL, GOODWIN, AND HARRISON
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from

MASSIVE THROMBOTIC OCCLUSION OF LARGE PULMONARY ARTERIES
C
4C
C
E
E0
U
z0
cn
c)
63.ce EU ce0 'A....I hoU.2W
rn .~
0 -0H~ r 4>
+,...4 ce ~ ~ Ci
¢
p~ _
Em 0
E -)Lzm
t. m
C) Ci)"o~~~~~~C
.~~~~~~~
++
>4 4-~~~ J-0
C4)
4) C)~~~~~~~~4
c)4 :3'>Qt > =~~~~~~~~~~~~~c
*) Cc
J2 ~~~~~~~~~~~C)
m V0C) bl
C) 0
A~~- *c),;
Z ~c)C
o~~~~~~~~~~~~~r
xnf
6 cq h.1z cm S
776
Q1)
Im
.
C)
C)
b5
C_
-z
b1t._
b5
.
-z
*-C
-AC
I-C
C.-
zci
C=C0SC)4
4-C
CI00r
mQ
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from

BALL, GOODWIN, AND HARRISON
thrombosis. A source for an embolism inperipheral veins is of only limited value in thedifferential diagnosis, since it may sometimesbe difficult or impossible to find in manifestcases of embolism.6Using these criteria, we consider that 7 of
the 23 cases had an initial pulmonary throm-
TABLE 4.-Criteria for the Differentiation of Primaryand Se(co(nla.ii 7'htothrbosis
Primary Thrombosis
Local disease of pulmon1aryNIartery.
Thrombus is a Cast of thevessel.
There is often deposition inepisodes produicinig lami-nation of the clot inl layersroughly parallel to the ar-terial wall. (No source forthe embolus ceai be fouind(l).
Secondary Thrombosis
No local disease pres-ent.
The embolus is usti-ally coiled.
The source of the em-bolus is often foundand corresponds tothe shape of the clotin the pulmonaryartery.
bosis in situ, 6 had definite initial pulmonaryemboli, and in 10 the nature of the initialincident was uncertain. It seems highlyprobable that these last were in reality due toemboli. Five of the 7 cases with primarythrombosis had pulmonary arterial disease orother local pathology. The histologic differencesbetween primary embolism and thrombosisare shown in figures 8 and 9. No single 1 of theabove criteria, however, is alone decisive indifferential diagnosis, and figure 10 illustratesthis point. In this case the lamination of thethrombus implies that the upper layers havebeen deposited locally, but the lack of localarterial disease and the presence of a sourcefor emboli in the femoral veins suggest thatthe thrombus probably originated from anembolus.Pulnonary Infarction. This was frequent,
but not invariable, and occurred in 4 of the
FIG. 8. Case 7. Section at bifurcation of lower lobe pulmonary artery. There is a plaque of ath-eroma on the lower side of the artery, 1, covered by a layer of partly organized thrombus, 2. Thisin turn is covered by a layer of more recent thrombus, 3. (X 9. Hematoxylin and eosin staini.)
777
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from

MASSIVE THRO.MBOTIC OCCLUSION OF LARGE lPULMO()NAIRY ARTERIES
7 cases with primary thrombosis and in 10 ofthe 16 remaining cases, in which the thrombuswas certainly or probably secondary to embo-lism.
FIG. 9. Section of a pulmonary artery branchcontaining an embolus that appears as 2 separatepieces. Note the absence of arterial disease. (X 9.Hematoxylin and eosin stain.)
DiS(Cu.SSION-
Our cases confirm the reports in the literaturethat thrombotic occlusion of the main pulmo-nary arteries may occur as a complication ofa number of diseases, especially of the heartand lungs, and to a lesser extent, of the gastro-intestinal tract, but may occasionally beunassociated with any other disease. It isclear that the occlusion may develop gradually,although it may be very difficult to determinethe exact age of the thrombus.Symptoms. The symptoms of thrombotic
occlusion are insidious, and in general arethose of right heart failure aiid low cardiacoutput. In AMiddleton's7 33 cases, dyspnea Naspresent in 90 per cent, hemoptysis in 62 percent, apprehension in 30 per cent, cough in 24per cent, and substernal pain in 24 per centt.Savacool and Charrs listed the principalsymptoms in their own 12 cases as dyspnea,pain in the chest or epigastriuim, and mentalconfusion. The last symptom was striking, andpresumably due to cerebral ischemia. Brenner6stressed dyspnea as a constant feature in hiscases of thrombosis of the main pulmonary
a& _ ^'-I_s_>.=.7,,h.s M.. ..S~ ~~---,,J
FIG. 10. Case 10. Section of a large pulmonary artery showing local thrombosis occurring in epi-sodes. The first 3 layers of thrombus (1, 2, and 3) have undergone partial organization from theiredges, as can be seen by the dark lines of fibrous tissue growing in toward the middle. The topmostlayer of recent thrombosis shows Zahn's lines. Note the absence of disease of the underlying ar-terial wall. (X 5.5. Weigert's elastic and Van Giesen's stains.)
778
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from

BALL, GOODWIN, AND HARRISON
artery. Carroll'0 mentioned dyspnea in all his5 cases and syncope on exertion in 1. Pleuriticpain and hemoptysis are likely to occur withinfarction, but are often absent. Brysonl"considered that half the cases had an acuteonset of symptoms and thought that hemop-tysis might arise from bronchopulmonaryanastomoses. Substernal pain and syncope arepresumably due to diminished coronary andcerebral blood flow, respectively. Abdominalpain may be caused by hepatic engorgementdue to tricuspid incompetence. Sudden deathhas often been reported.
Our own cases showed a similar symp-tomatology, especially sudden dyspnea, faint-ing, and pulmonary infarction, althoughmental confusion was not a striking feature,and in several cases there were no symptomsattributable to the thrombosis. Sudden onsetand sudden death were not common.
Physical Signs. Cyanosis was present in 68per cent of Middleton's 53 cases. It is pre-sumably peripheral in nature and is due to alow cardiac output, except when there is aright-to-left shunt, which would be intensifiedby the occlusion of the pulmonary arteries.9Signs of tricuspid incompetence, peripheraledema, hepatic engorgement, and increasedjugular venous pressure, together indicatingcongestive failure of the right ventricle, werereported by Carroll'0 and by Hanelin andEyler.J' Signs of pulmonary hypertension(enlarged right ventricle and accentuatedpulmonary element of the second heart sound)have also been frequently mentioned. Two ofthe 7 cases described by Keating and co-workers'3 had a lone apical systolic murmur,2 had diastolic murmurs over the pulmonaryartery, which in 1 was associated with anapical systolic murmur; but 3 had no murmursat all. Carroll's10 5 cases all had systolicmurmurs in the region of the pulmonaryartery, as had Middleton's7 case. Savacool andCharr' stress the small pulse, low bloodpressure, and restlessness as signs of lowcardiac output, but these probably do notoccur until the main pulmonary arteries aresubstantially occluded. Gibbon and asso-ciates'4 in experimental studies on dogs, foundthat the systemic blood pressure did not
fall until 60 per cent occlusion of more than75 per cent of the pulmonary arteries causeddeath.The physical signs in our own cases were
often difficult to evaluate, since the asso-ciated or underlying disease tended to maskthem. However, the 3 cases with repeatedthromboembolic episodes of unknown causepresented the features of right-sided heartfailure with low output, a systolic murmurover the pulmonary artery or at the apex, anormal or soft pulmonary component of thesecond heart sound, and enlargement of theright ventricle. Accentuation of the pulmonarycomponent of the second heart sound suggest-ing pulmonary hypertension was found onlyin patients in whom pulmonary hypertensionwas present before the occurrence of thethrombosis. It is probable that a thrombusin the main pulmonary arteries extendingdown close to the valve could be associatedwith a low pressure in the pulmonary arteryand, hence, a normal or soft pulmonarycomponent of the second heart sound, whichwas in fact present in 2 of our patients.
Radiologic Signs. The radiologic signs havebeen reviewed by Hanelin and Eyler.'2 Themain pulmonary arteries were enlarged, whilethe peripheral branches were small; the lungfields appeared clear, with the exception ofshadows cast by pulmonary infarcts. Keatingand associates" found right ventricular andpulmonary arterial enlargement and clearlung fields in all their 7 cases. Absence ofpulsation of the main pulmonary arteries(which had previously pulsated strongly) wasnoted by Canada and co-workers9 in 1 of their3 cases with thrombosed pulmonary arteries,but comment has not been previously madeon this point. Absence of pulsation in anenlarged right main branch is unusual, and washelpful in diagnosis in 1 of our cases. But itshould be remembered that enlargement ofthe main pulmonary artery and left mainbranch may be associated with poor pulsationin cases of pulmonary stenosis.Adequate radiology in many of our cases
was not possible, but in 2 patients (cases 1 and2) a combination of clear lung fields andenlarged pulmonary arteries was seen. In a
779
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from

MASSIVE THROMBOTIC OCCLUSION OF LARGE PULMONARY ARTERIES
third case (case 5) the contour of the enlargedright pulmonary artery was irregular, beingquite unlike the smooth convex margin usuallyseen when this vessel is enlarged.
The Electrocardiogram. As might be expected,the electrocardiogram has been reported toshow hypertrophy of the right ventricle, anddid so in many of our patients.
Diagnosis. The diagnosis of pulmonaryartery thrombosis should be considered when-ever a patient presents unexplained congestivecardiac failure, dyspnea, fainting, repeatedepisodes of pulmonary infarction, or pain inthe chest. If the clinical picture includesevidence of peripheral venous thrombosis, asystolic murmur over the pulmonary artery,and a normal or soft component of the secondheart sound the diagnosis becomes moreprobable. If, in addition, x-ray films of thechest show enlargement of the right ventricleand pulmonary arteries (without significantpulsation of the latter) and clear lung fields orshadows suggesting infarction, together withelectrocardiographic evidence of right ven-tricular hypertrophy, the diagnosis becomesalmost certain.
Cardiac catheterization is of value in exclud-ing other lesions, such as septal defects andpulmonary stenosis, but contributes littlepositive information other than confirmingright ventricular hypertension. Exclusion ofpulmonary stenosis may be difficult owing tothe difficulty of passing the catheter into athrombosed main pulmonary artery.
Differentiation from mitral stenosis mayalso be difficult, especially as pulmonaryartery thrombosis may complicate this condi-tion, and the typical murmurs may be difficultto hear in patients with severe pulmonaryhypertension. The characteristic radiologicvascular changes seen in mitral disease,', 16and enlargement of the left atrium, shouldassist in making the differential diagnosis.Absence of a history or clinical evidence of lungdisease should exclude a diagnosis of chronicanoxic cor pulmonale. Differentiation fromidiopathic pulmonary hypertension may bedifficult, and it is possible that pulmonaryartery thrombosis might complicate this condi-tion.3 Obscure forms of chronic pulmonary
fibrosis would be likely to show characteristicradiologic changes in the lungs, which areabsent in pulmonary artery thrombosis.
Angiocardiography should be the mostsatisfactory diagnostic method, but was notfound to be of real value in case 5, while theother cases in which the condition was sus-pected were too ill for the investigation to becarried out. With improved and safer technicsof angiography, it might be performed if thediagnosis is suspected.
Treatment. Lack of success has probablybeen due to failure of early diagnosis. Prolongedanticoagulant therapy offers the only hope ofpreventing extension of the thrombus. If thethrombosis is secondary to repeated pulmonaryemboli from thrombosis of the leg veins thatcannot be controlled by anticoagulants, liga-tion of the inferior vena cava might have to beconsidered.
Genesis of the Thrombosis and Associated DiseaseIt is often considered that thrombosis in the
pulmonary arterial tree is always secondary toembolism. Brenner6 considered that primarythrombosis did sometimes occur, especially inassociation with disease of the pulmonaryarteries, and our own findings of local pulmo-nary artery disease in 5 of 7 cases with primarythrombosis support this view. Differentiationbetween primary thrombosis and that second-ary to embolism may be impossible, however.While a recent embolus is easy to recognizebecause the clot is not a cast of the artery andis usually coiled, after a few days furtherthrombus is deposited around it, tending toobscure the original outline. Where a clot doesnot fully obstruct an artery, endotheliumrapidly grows over it, while organization fromthe arterial wall fixes it in position.'7 Bycontrast, a local thrombus fits the vessel and isoften laid down in layers at different times.Glynn and Knowles'8 considered this lamina-tion to be good evidence of primary thrombosis,although Brenner6 maintained that laminatedthrombi from peripheral veins may be dislodgedand carried to the pulmonary artery, so thatthe phenomenon might be found in thrombisecondary to embolism. In our view, however,the presence of a clot laminated in planes
780
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from

BALL, GOODWIN, AND HARRISON
roughly parallel to the wall of the artery,fitting the vessel, and overlying local arterialdisease is virtually diagnostic of primarythrombosis in situ.A number of different forms of intrathoracic
disease have been described in associationwith thrombosis of the large pulmonaryarteries, particularly congenital heart diseaseand pulmonary tuberculosis. Mitral stenosishas not featured prominently.
Savacool and Charr' reported 12 casesassociated with pulmonary tuberculosis. Theywere convinced that the thrombi arose in situin view of their size and shape, their firmadherence to the intima, invasion by strands ofconnective tissue from the intima, and thedeposition of fibrin platelets and other bloodconstituents. The primary site of thrombosisappeared to be the termination of the smallbranches of the main pulmonary artery, whichwere often embedded in fibrous tissue ortuberculous consolidation. Furthermore, theynoted that the right pulmonary artery wasinvolved more frequently than the left, whichthey attributed to the fact that the rightpulmonary artery is compressed between thevein and bronchus and is crossed by the aorticarch, while the left pulmonary artery isrelatively free. Gordon and Perlal9 describedpulmonary arterial thrombosis in a child withpatent ductus arteriosus, pulmonary stenosis,and subacute bacterial endocarditis, andWhipham20 described an infant of 7 months,with patent ductus arteriosus and a thrombusin the pulmonary artery that projected throughthe valve into the right ventricle. Dickinson2ldescribed occlusion of the main trunk and bothmain branches of the pulmonary artery in a boyaged 412 years who had pulmonary stenosisand a ventricular septal defect. Canada9reported 3 cases of atrioseptal defect withpulmonary artery thrombosis. Widespreadfocal thrombosis in the small pulmonaryvessels has been described by Rich22 in cases ofthe tetralogy of Fallot, while in 1 of our 23cases widespread thrombosis, including themain pulmonary arteries, occurred in associa-tion with partial pulmonary atresia and a
large ventricular septal defect.Thrombosis of the large pulmonary arteries
has been reported in children in the absence ofcongenital heart disease. Gehrt23 found 7cases in 600 autopsies, 5 of which followedmeasles. Gunter24 described thrombosis in apair of identical twins, one of whom died ofgastroenteritis and the other after mastoid-ectomy. Since children rarely develop pulmo-nary embolism, these cases provide evidencein favor of primary thrombosis, and there was 1such in our series.Primary thrombosis might be expected to
occur in association with disease of the pul-monary arteries, such as atherosclerosis, whichmay be found in chronic lung disease and incongenital and acquired heart disease. Wheredisease of the arterial wall is combined with alow cardiac output, a sluggish pulmonaryblood flow, and enlargement of the mainpulmonary arteries, thrombosis in situ isparticularly favored (fig. 8).
Disease of the pulmonary arteries is animportant complication of mitral valve diseasewhere atherosclerosis may involve the largebranches, as in our cases 5 and 7. Furthermore,pulmonary hypertension is common, and thecardiac output is often reduced in severecases. The summation of these 3 factors wouldbe conducive to primary thrombosis.
It is not surprising, therefore, that 19 of 88cases of pulmonary artery thrombosis collectedby Savacool and Charr' occurred in associationwith mitral disease, and the incidence in ourseries is of the same order (6 out of 23 cases).An additional case of thrombosis of the rightpulmonary artery in a patient with mitralstenosis, thought to have occurred followingcardiac catheterization, has recently beenreported by Nightingale and Williams.21 Afurther factor favoring thrombosis is thetendency to peripheral venous thrombosis andpulmonary embolism from peripheral throm-bosis in mitral disease. This has recently beenstressed by Wood26 in cases with a low cardiacoutput and very high pulmonary vascularresistance. It is possible, however, that someof the organic occlusive lesions in the smallerarteries, which are not infrequently found inmitral stenosis, might be originally thromboticor embolic in nature. Thrombosis of the small
781
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from

7MASSIVE THROMBOTIC OCCLUSION OF LARGE PULMONARY ARTERIEXS
pulmonary arteries, together with arteritis,was a feature in our case 6 (fig. 7).
Pulmonary Infarction in Association withThrombosis of the Pulmonary Arteries
Pulmonary infarction is not an invariablefeature in cases of thrombus of the largepulmonary arteries. Of 7 cases reported byKeating and co-workers,'3 infarcts were presentin only 2, in both of which previous pulmonaryemboli had occurred. Infarcts were absent inPou and Charr's27 6 cases, and in 4 ofBrenner's28 cases. Fowler19 found no infarctionin a single case of thrombosis of the right andleft main pulmonary arteries and explained itsabsence by the presence of anastomosesbetween the bronchial and pulmonary arteries.In this connection, the observation of Carroll10is of interest. At thoracotomy in 1 of his cases,the left pulmonary artery was found to beoccluded, but aspiration distal to the blockyielded oxygenated blood, which must havebeen due to retrograde bronchial flow. Gradualocclusion of the main arteries would allowtime for these anastomoses to enlarge. Theabsence of infarction does not, however, permitdistinction between primary and secondarythrombosis, since progressive thrombosis on thesite of an embolus would create the samecondition. A survey of the literature suggeststhat infarcts were more common in cases inwhich there was a definite source for, or historyof, pulmonary embolism, than in those thoughtto have primary thrombosis of the pulmonaryarteries.
In our own series, 14 of 23 cases had pulmo-nary infarcts that occurred with equal fre-quency in association with primary andsecondary thrombosis. In 1 patient (case 5)the bronchial arteries were enlarged.
SUMMARY
A series of 23 cases of thrombotic occlusionof the large pulmonary arteries, not due toacute massive embolism, has been presented.The clinical, radiologic, electrocardiographic,and pathologic features have been described,together with the results of special investiga-tions in certain cases. It is concluded thatthrombotic occlusion of the large pulmonary
arteries can occur insidiously and present acharacteristic picture of progressive rightventricular failure, the special features ofwhich are outlined in detail. In most cases thethrombosis was secondary to embolism, but in7 it was considered to have arisen primarily inthe pulmonary artery. Six of the 23 cases hadmitral stenosis, which appeared to favorprimary thrombosis of the large pulmonaryarteries. The etiology, diagnosis, differentialdiagnosis, and possible treatment have beendiscussed, and it is suggested that the diagnosisshould be considered in any, patient withobscure right ventricular failure, attacks ofsyncope, acute dyspnea, or chest pain; andespecially if there have been episodes suggestiveof pulmonary infarction. Patients with mitralstenosis who deteriorate for no apparentreason and shots alteration in the second heartsound and decrease in the pulsation of thepulmonary arteries, should also be suspected ofhaving developed a massive pulmonary arterythrombosis.
ACKNOWLEDGMENTWe are grateful to Dr. J. Edmunds for permission
to use his notes on case 1 and to Dr. C. S. Treip forhis postmortem findings. We wish to thank ProfessorJ. \Iclichael for permission to publish cases 5 and 7and Dr. J. Shillingford for his help and advice. AMissR. Klein, _Mr. Knowlden, and \Mr. Booker providedthe photographs. The draw-ing was executed by -MissD. M. Baker.
SUMMARIO IN INTERLINGUA
Es presentate un serie de 23 casos de occlu-sion thrombotic del grande arterias pulmonar,non causate per acute embolismos massive. Esdescribite le aspectos clinic, radiologic, electro-cardiographic, e pathologic, insimul con leresultatos de investigationes special interpren-dite in certe casos. Le autores conclude queocclusion thrombotic del grande arterias pul-monar pote occurrer insidiosemente e que illopresenta alora un tableau characteristic deprogressive disfallimento dextero-ventricular.Le aspectos special de illo es delineate in de-talio. In le majoritate del casos le thromboseesseva secundari a embolismo. In 7 casos, delaltere latere, illo pareva haber occurrite pri-marimente in le arteria pulmonar. Sex de 23
782
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from

BALL, GOODWIN, AND HARRISON
casos habeva stenosis mitral, lo que parevasupportar le interpretation de thrombosisprimari in le grande arterias pulmonar. Esdiscutite le etiologia, le diagnose, le diagnosedifferential, e le formas possibile de tracta-mento. Es suggerite que le diagnose de occlu-sion thrombotic del grande arterias pulmonardebe esser prendite in consideration in omne
patients con obscur disfallimento dextero-ventricular, attaccos de syncope, dyspneaacute, o dolores thoracic, specialmente in lepresentia de un historia de episodios que sug-gere infarcimento pulmonar. Le suspicion deun disveloppamento de massive thrombosis delgrande arterias pulmonar es etiam justificate inpatientes con stenosis mitral qui se deteriora sincausa apparente e qui monstra alteration in lesecunde sono cardiac insimul con reduction delpulsation in le arterias pulmonar.
REFERENCES1 LJUNGDAHL: Gibt es eine chronische Emboli-
sierung der Lungenarterie? Deutsche Arch.klin. MXed. 160: 1,1928.
2 MC1\IICHAEL, J.: Heart failure of pulmonary ori-gin. Edinburgh Ml. J. 55: 65, 1948.
OWEN, W. R., THOMAS, W. A.. CASTLEMAN, B.,AND BLAND, E. F.: Unrecognized emboli to thelungs with subsequent cor pulmonale. NewEngland J. _Med. 249: 919, 1953.
4 HELIE, M.: Inflammation de I'artere pulmonaire.Mort subite. Bull. Soc. Anat., Paris 12: 254,1837. Quoted by Bryson, W. J.11
5 SAVACOOL, J. XV., AND CHARR, R.: Thrombosis ofthe pulmonary artery. Am. Rev. Tuberc. 44:42, 1941.
6 BRENNER, 0.: Pathology of the vessels of the pul-monary circulation. V. Tuberculosis of the pul-monary vessels. Arch. Int. 'Med. 56: 1189, 1935.
7 MIDDLETON, W. S.: Abdominal pain in pulmonarythrombosis. Ann. Int. Med. 18: 345, 1943.
8 MAGIDSON, 0., AND JACOBSON, G.: Thrombosis ofthe main pulmonary arteries. Brit. Heart J.17: 207, 1955.
'CANADA,)W. J., GOODALE, F., AND CURRENS, J.H.: Defect of the interatrial septum with throm-bosis of the pulmonary artery. New England J.Med. 248: 309, 1953.
10 CARROLL, D.: Chronic obstruction of major pul-monary arteries. Am. J. Med. 9: 175, 1950.
BRYSON, XV. J.: Propagating pulmonary arterythrombosis (a specific syndrome). Dis. Chest15: 366, 1949.
12 HANELIN, J., AND EYLER, WV. R.: Pulmonary ar-
tery thrombosis; roentgen manifestations. Ra-diology 56: 689, 1951.
13 KEATING, D. R., BURKEY, J. N., HELLERSTEIN,H. K., AND FEIL, H.: Chronic massive throm-bosis of pulmonary arteries. A report of sevencases with clinical and necropsy studies. Am. J.Roentgenol. 69: 208, 1953.
14 GIBBON, J. H., JR., HOPKINSON, M., AND CHURCH-ILL, E. D.: Changes in circulation produced bygradual occlusion of the pulmonary artery. J.Clin. Invest. 11: 543, 1932.
15 GOODWIN, J. F., STEINER, R. E., AND LOWE, K. G.:The pulmonary arteries in mitral stenosis dem-onstrated by angiocardiographv. J. Fac. Radiol.4: 21, 1952.
16 DAVIES, L. G., GOODWIN, J. F., STEINER, R. E..,AND VAN LEUVEN, B. D.: The clinical and ra-diological assessment of the pulmonary arterialpressure in mitral stenosis. Brit. Heart J. 15:393, 1953.
17 DUGUID, J. B.: Thrombosis as a factor in the path-ogenesis of aortic atherosclerosis. J. Path. &Bact. 60: 57, 1948.
18 GLYNN, E., AND KNOWLES, R. E.: Some observa-tions on fatal cases of pulmonary thrombosis.Brit. WM. J. 2: 1412, 1910.
19 GORDON, H., AND PERLA, D.: Subacute bacterialendarteritis of pulmonary artery associated withpatent ductus arteriosus and pulmonic stenosis.Am. J. Dis. Child. 41: 98, 1931.
20 WHIPHAM, T. R.: A heart showing an infectivepolypoid thrombus in the pulmonary artery andextending into the right ventricle, mistaken forpatent ductus arteriosus. Proc. Roy. Soc. _Med.4: 199, 1911.
21 DICKINSON, L.: Thrombosis of the pulmonary ar-tery in a case of congenital stenosis of the orifice.Tr. Path. Soc. London 48: 57, 1897.
22 RICH, A. R.: A hitherto unrecognized tendency todevelopment of widespread pulmonary vascularobstruction in patients with congenital pulmo-nary stenosis (tetralogy of Fallot). Bull. JohnsHopkins Hosp. 82: 389, 1948.
23 GEHRT: Thrombose der Arteria pulmonalis imKindesalter. Ztschr. Kinderh. 36: 221, 1923.
24 GUNTER, J. U.: Thrombosis of pulmonary arteryin identical twins; report of cases with autopsy.Arch. path. Anat. 31: 211, 1941.
25 NIGHTINGALE, J. A., AND ILLIAMS, B. L.: Pul-monary artery thrombosis following cardiaccatheterisation. Brit. Heart J. 17: 113, 1955.
26 'WOOD, P.: An appreciation of mitral stenosis. Brit.'M. J. 1: 1050, 1113, 1954.
27 PoU, J. F., AND CHARR, R.: Thrombosis of pul-monary artery; a clinico-pathological study ofsix cases. Am. Rev. Tuberc. 37: 394, 1938.
28 BRENNER, 0.: Sclerosis of pulmonary artery) withthrombosis. Lancet 1: 911, 1931.
29 FOWLER, W. M.: Obliterating thrombosis of thepulmonary arteries. Ann. Int. _Ied. 7: 1101,1934.
-78:S3
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from
K. P. BALL, J. F. GOODWIN and C. V. HARRISONMassive Thrombotic Occlusion of the Large Pulmonary Arteries
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1956 American Heart Association, Inc. All rights reserved.
75231is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TXCirculation
doi: 10.1161/01.CIR.14.5.7661956;14:766-783Circulation.
http://circ.ahajournals.org/content/14/5/766located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer
of the Web page under Services. Further information about this process is available in thewhich permission is being requested is located, click Request Permissions in the middle columnClearance Center, not the Editorial Office. Once the online version of the published article for
can be obtained via RightsLink, a service of the CopyrightCirculationoriginally published in Requests for permissions to reproduce figures, tables, or portions of articlesPermissions:
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from


















