Market and Network Services Access Line · 2009. 12. 9. · Peptic ulcer complication 1 Total 14...
77
Stay tuned…our webinar will begin shortly! (Please note that your line has been muted.) Market and Network Services Access Line A new, one-stop, easy to use service dedicated for Case Managers, Medical Directors and Corporate Leaders who need assistance in referring patients to Cleveland Clinic, Main Campus. This line is open from 7am – 11pm, seven days a week. 216-738-5439
Transcript of Market and Network Services Access Line · 2009. 12. 9. · Peptic ulcer complication 1 Total 14...

Stay tuned…our webinar will begin shortly! (Please note that your line has been muted.)
Market and Network Services Access Line
A new, one-stop, easy to use service dedicated for Case Managers, Medical Directors and Corporate Leaders who
need assistance in referring patients to Cleveland Clinic, Main Campus. This line is open from 7am – 11pm, seven
days a week.
216-738-5439

The Future of Living Donor Liver The Future of Living Donor Liver
Transplantation:Transplantation:Technological and Ethical Foundations for Technological and Ethical Foundations for
The Way Forward in AThe Way Forward in A--ALDLTALDLT
Charles M. Miller, MDCharles M. Miller, MD
Professor of SurgeryProfessor of Surgery
Director of Liver TransplantationDirector of Liver Transplantation
Cleveland ClinicCleveland Clinic

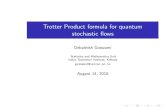
75 98 88133
76
15380
230
95
302
84
423
99
698
122
810
130
880
107
916
133
1202
215
1430
0
200
400
600
800
1000
1200
1400
1600
1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005
Deceased Donor Living Donor
LIVER TRANSPLANTATIONLIVER TRANSPLANTATION IN ASIAIN ASIANumber of OperationsNumber of Operations
* Excluding data from mainland China
Total LDLT = 7573
Lo CM, ILTS Milan 2006
90% of transplants were from living donors

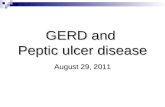
4093
60
4334
54
4461
62
4599
85
4844
92
4947
251
4996
385
5108
505
5298
355
5672
321
5846
323
6444
323
0
1000
2000
3000
4000
5000
6000
7000
1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005
Deceased Donor Living Donor
www.optn.org 2006
LIVER TRANSPLANTATION IN USLIVER TRANSPLANTATION IN USNumber of OperationsNumber of Operations
5% of transplants were from living donors




LDLT: Advantages and LDLT: Advantages and
DisadvantagesDisadvantages
AdvantagesAdvantages
�� Assures a healthy organ Assures a healthy organ with minimal with minimal preservation damagepreservation damage
�� Independence from long Independence from long cadavericcadaveric waiting listwaiting list
�� Optimizes the timing of Optimizes the timing of transplantationtransplantation
�� Helps alleviate the Helps alleviate the severe shortage of severe shortage of cadavericcadaveric livers and livers and death on the waiting listdeath on the waiting list
DisadvantagesDisadvantages
�� Finite risk of donor Finite risk of donor
morbidity and mortalitymorbidity and mortality
�� Both operation are Both operation are
technically complex technically complex
�� The program is The program is
extremely laborextremely labor--
intensiveintensive
�� ReputationalReputational riskrisk

Fundamental Dichotomy:Fundamental Dichotomy:
““PrimunPrimun Non Non NocereNocere”” and LDLTand LDLT
�� Donor safety must have primacy at all Donor safety must have primacy at all
timestimes
However,However,
�� The safest thing for a potential donor is not The safest thing for a potential donor is not
to donate ( The null position)to donate ( The null position)
�� How do we move forward from the null How do we move forward from the null
position?position?

The Way ForwardThe Way Forward
�� Maximize donor safetyMaximize donor safety
�� Refine and expand candidate selectionRefine and expand candidate selection
�� MELDMELD
�� Special ConsiderationsSpecial Considerations
�� Review new physiologic understandings Review new physiologic understandings
and applied technological innovationsand applied technological innovations
�� Assure Assure Our Way ForwardOur Way Forward is ethically is ethically
soundsound

Living Liver Donors Living Liver Donors
Morbidity and MortalityMorbidity and Mortality
• Mortality
• Death
• Vegetative State
• Remnant loss
• Morbidity
• Surgical Complications
• Quality of life
• Psycho-social and financial hardship

Graft OptionsGraft Options
A) Left lateral section (S2 and 3)A) Left lateral section (S2 and 3)
B) B) Left lobe (S2, 3 and 4) Left lobe (S2, 3 and 4)
With/without MHV With/without MHV
With/without caudate With/without caudate
C) C) Right lobe (S5, 6, 7 and 8)Right lobe (S5, 6, 7 and 8)
With/without MHVWith/without MHV
D) Right posterior (S6 and 7)D) Right posterior (S6 and 7)
7
3
2
4
56
8
MHV
A
B
C
D
Living Liver DonorsLiving Liver Donors
Morbidity and MortalityMorbidity and Mortality

Living Liver Donors Living Liver Donors
Morbidity and MortalityMorbidity and Mortality
• Mortality
• Death
• Vegetative State
• Remnant loss
• Morbidity
• Surgical Complications
• Quality of life
• Psycho-social and financial hardship

Donor DeathsDonor DeathsVancouver Forum: Transplantation 2006Vancouver Forum: Transplantation 2006
3 Left Liver3 Left Liver 11 + 11 + (3)(3) Right LiverRight Liver
US US 11 US US 2 2 Egypt Egypt 1 1
Brazil Brazil 11 BrazilBrazil 2 2 China (HK) China (HK) 1 1
Germany Germany 11 GermanyGermany 2 2 India India 1 1 (1)*(1)*
France France 1 1 (1)(1) S. America S. America 1 1
Japan Japan 11
•• 4 Right lobe Donors4 Right lobe Donors have had remnant loss and liver transplantation have had remnant loss and liver transplantation
•• 1 Right lobe Donor is in a persistent vegetative state 1 Right lobe Donor is in a persistent vegetative state **
Right liver donor:Right liver donor: mortality = 0.5%mortality = 0.5%
Left liver donor:Left liver donor: mortality = 0.1%mortality = 0.1%

Cause of death Number
Sepsis 5
Liver failure 2
Unknown 3
Myocardial infarction 1
Cerebral hemorrhage 1
Pulmonary embolus 1
Peptic ulcer complication 1
Total 14
Trotter et al, Liver Transplantation 2006
Living Liver DonorsLiving Liver Donors
Morbidity and MortalityMorbidity and Mortality

Living Liver Donors Living Liver Donors
Morbidity and MortalityMorbidity and Mortality
• Mortality
• Death
• Vegetative State
• Remnant loss
• Morbidity
• Surgical Complications
• Quality of life
• Psycho-social and financial hardship

Donor ComplicationsBy Graft Type
ELTR 6/2003: Adam et al
No major complication
Complications
Biliary leak
Biliary stenosis
Liver insufficiency
PT<30%
[30%-50%]
PT>=50%
PE
Vascular
Infection
GI
General*
Right liver Left liver
385 (79%)
103 (21%)
28 (6%)
11 (2%)
12 (2.4%)
12 (3%)
181 (48%)
188 (49%)
4 (0.8%)
8 (1.6%)
19 (4%)
3 (0.6%)
18 (3.6%)
88 (92%)
8 (8%)
5 (5%)
0 (0%)
1 (0%)
1 (3%)
6 (20%)
23 (77%)
0 (0%)
0 (0%)
2 (2%)
0 (0%)
0 (0%)
Left lobe
357 (89.5%)
42 (10.5%)
6 (1.5%)
0 (0%)
2 (0.5%)
2 (2%)
8 (9%)
79 (88%)
5 (1%)
6 (1.5%)
16 (4%)
3 (1%)
4 (1%)
P
0.0001
0.005
0.004
ns
0.0001
ns
ns
ns
ns
0.03
Overall complication rate = 15%

Umeshita et al, Lancet 2003
Living Liver DonorsLiving Liver Donors
Morbidity and MortalityMorbidity and MortalityJapanese Liver Transplantation SocietyJapanese Liver Transplantation Society

LL (n=598) L (n=327) R (n=554)
Bile leakage 33 8 34
Biliary stricture 1 0 6
Hyperbilirubinaemia 2 0 41
PV thrombosis 0 0 3
Small bowel obstruction 5 1 4
Pulmonary embolism 0 1 3
Intraabdominal bleeding 0 0 3
Intraabdominal collection 0 0 20
Pancreatitis 1 0 2
Bleeding duodenal ulcer 1 0 2
Wound infection 9 10 26
Gastric outlet obstruction 4 3 1
Pneumonia 0 1 2
Pleural effusion 0 0 6
Pressure sore 0 0 1
Peroneal nerve palsy 0 0 1
Total 56 (9.4%) 24 (7.3%) 155(28%)
CM Lo et al, Transplantation 2003
Living Liver DonorsLiving Liver DonorsSurgical Complications: Asian Collective Surgical Complications: Asian Collective

Adult Patient / Graft SurvivalAdult Patient / Graft Survival
Left LobeLeft Lobe
0
20
40
60
80
100
3 6 12 18 24 36 48
MonthsMonths
% S
urv
ival
% S
urv
ival
78%
57%
45%
34%
Patient -----
Graft Graft ----------

Adult LD Patient / Graft SurvivalAdult LD Patient / Graft Survival
Right LobeRight Lobe
0
20
40
60
80
100
3 6 12 18 24
MonthsMonths
% S
urv
ival
% S
urv
ival
87%
84%
81%
76%
Patient -----
Graft Graft ----------

The Way ForwardThe Way Forward
�� Maximize donor safetyMaximize donor safety
�� Refine and expand candidate selectionRefine and expand candidate selection
�� MELDMELD
�� Special ConsiderationsSpecial Considerations
�� Review new physiologic understandings Review new physiologic understandings
and applied technological innovationsand applied technological innovations
�� Assure Assure Our Way ForwardOur Way Forward is ethically is ethically
soundsound

Functional Graft SizeFunctional Graft Size
•• ChildChild’’s classification s classification
(MELD)(MELD)
•• Actual graft sizeActual graft size
•• RecipientRecipient’’s portal flow s portal flow
dynamics & HABRdynamics & HABR
•• Restricted venous outflow Restricted venous outflow
(global or segmental)(global or segmental)

Adult to Adult LDLT: US ExperienceAdult to Adult LDLT: US ExperienceRecipient CharacteristicsRecipient Characteristics
MELD Status at TransplantMELD Status at Transplant
(%) (%) Meld 6Meld 6--1010 Meld 11Meld 11--2020 Meld 21Meld 21--3030 Meld 31 Meld 31
++
live live
donorsdonors19.8 %19.8 % 49.2 %49.2 % 6.6 %6.6 % 1.0 %1.0 %
cad cad
donorsdonors13.4 %13.4 % 39.9 %39.9 % 19.9 %19.9 % 11.7 %11.7 %
2003 UNOS / 2003 UNOS / UStransplant.orgUStransplant.org / SRTR/ SRTR

Improvement in Survival Associated With Adult-to-Adult Living Donor Liver TransplantationCARL L. BERG,* and the A2ALL Study Group
GASTROENTEROLOGY 2007;133:1806–1813
Conclusions:
Adult LDLT was associated with lower mortality than the alternative of waiting for DDLT. This reduction in mortality wasmagnified as centers gained experience with LDLT.
Results:
Overall (n = 807) a LDLT (n= 389) Non-LDLT (n = 418)
MELD 15.6 +/-6.8 14.8+/- 6.4 16.4+/- 7.2 ( p=.002)

Berg for the A2ALLBerg for the A2ALL
�� ““Thus, in plainer language, once centers in Thus, in plainer language, once centers in A2ALL had done 20 A2ALL had done 20 LDLTsLDLTs, there was marked , there was marked survival benefit (reduction in mortality hazard survival benefit (reduction in mortality hazard ratio) to proceeding to LDLT even if the ratio) to proceeding to LDLT even if the candidate's MELD was under 15 at time of their candidate's MELD was under 15 at time of their donor's evaluation.donor's evaluation.””

Special ConsiderationsSpecial Considerations
�� Blood Type O or BBlood Type O or B
�� Large shunts with severe encephalopathyLarge shunts with severe encephalopathy
�� Tumors outside Milan criteria (UnTumors outside Milan criteria (Un--MELDableMELDable))
�� Severe itching in PBCSevere itching in PBC
�� Multiple episodes of Multiple episodes of cholangitischolangitis in PSCin PSC
�� NeuroendocrineNeuroendocrine tumorstumors
�� All small childrenAll small children

The Way ForwardThe Way Forward
�� Maximize donor safetyMaximize donor safety
�� Refine and expand candidate selectionRefine and expand candidate selection
�� MELDMELD
�� Special Special ConsidertionsConsidertions
�� Review new physiologic understandings Review new physiologic understandings
and applied technological innovationsand applied technological innovations
�� Assure Assure Our Way ForwardOur Way Forward is ethically is ethically
soundsound

Functional Graft SizeFunctional Graft Size
•• ChildChild’’s classifications classification
•• Actual graft sizeActual graft size
•• RecipientRecipient’’s portal flow s portal flow
dynamics & HABRdynamics & HABR
•• Restricted venous outflow Restricted venous outflow
(global or segmental)(global or segmental)

GRBWR
outflow capacity portal hypertension
(+)
(-) (+)(+) (-)
(-)
Balance of Critical Factors for Success in LDLT
1)The larger the size of the triangle, the greater the functional graft size
Adopted from A. Marcos



GRBWR
outflow capacity portal hypertension
(+)
(-) (+)(+) (-)(-)
Balance of Critical Factors for Success in LDLT
This is the balance that is necessary for success when using left lobes










Yamada, T et al, American
Journal of Transplantation 2008;
8: 847–853
This is the Fuel Injector

What about What about ““Fuel Additives?Fuel Additives?””
�� Pharmacologic manipulationsPharmacologic manipulations
�� OctreotideOctreotide
�� AdenosineAdenosine
�� ProstaglandinsProstaglandins
�� Can these help tip the balance from Can these help tip the balance from
cholestatic hypertrophy to normal cholestatic hypertrophy to normal
regeneration?regeneration?

Recent Strategy in 3 Transplant CentersRecent Strategy in 3 Transplant Centers
UCSFUCSF
Since inception,15 left lobe LDLTs out of 117. However, 10 of Since inception,15 left lobe LDLTs out of 117. However, 10 of
the 20 LDLTs in the past 2 years were left lobes. the 20 LDLTs in the past 2 years were left lobes.
U of NebraskaU of Nebraska
6 left lobes in the past 2 years. Now with a 6 left lobes in the past 2 years. Now with a ““philosophical philosophical
commitment to move exclusively to the left lobe in all but commitment to move exclusively to the left lobe in all but
exceptional casesexceptional cases””
Cleveland ClinicCleveland Clinic
In 15 adultIn 15 adult--toto--adult LDLTs since 2004, 50% was left lobe LDLT. adult LDLTs since 2004, 50% was left lobe LDLT.
Our philosophy is to prefer left lobes if at all possible.Our philosophy is to prefer left lobes if at all possible.

Nebraska/UCSF Left Lobe LDLT With PCSNebraska/UCSF Left Lobe LDLT With PCS
PCSPCS1.001.00 GoodGood22M22MAHNAHN --2020
PCSPCS0.930.93 Poor, SFSSPoor, SFSS24M24MHCVHCV --2323
PCSPCS0.960.96 GoodGood33M33MPBCPBC --1818
PCSPCS0.640.64 GoodGood37M37MCryptogenicCryptogenic ----
PCSPCS0.510.51 GoodGood26M26MHCVHCV 4254251212
PCSPCS0.620.62 GoodGood42F42FNASH/HCCNASH/HCC ----
PCSPCS0.530.53 GoodGood42M42MHCVHCV --2020
Inflow Inflow
modulationmodulationGBWRGBWR
Graft Graft
functionfunctionDemoDemoDiagnosisDiagnosis PVFPVF
PV pressure PV pressure
gradientgradient
PCSPCS0.370.37 GoodGood25F25FPBCPBC --1717
PCSPCS0.880.88 GoodGood40F40FPBCPBC --1414
PCSPCS0.740.74 GoodGood46F46FPBCPBC 100010001010

LDLT at Cleveland ClinicLDLT at Cleveland Clinic
�� June 2005 June 2005 –– May 2009May 2009
�� 20 LDLTs (5 pediatrics and 15 Adults)20 LDLTs (5 pediatrics and 15 Adults)
�� Graft type Graft type
�� Left lateral segment (n = 5)Left lateral segment (n = 5)
�� Left lobe (n = 8)Left lobe (n = 8)
�� Right lobe (n = 7)Right lobe (n = 7)

CCF Left Lobe LDLTCCF Left Lobe LDLT
PCS, SAL, OctPCS, SAL, Oct
Shunt stentShunt stent21.921.90.590.59
GoodGood51M51MHCVHCV52/M52/M
PCS, SALPCS, SAL22.122.10.460.46PoorPoor
SFSSSFSS55M55MPSCPSC38/M38/M
SALSAL4.74.70.730.73 GoodGood37M37MPSCPSC71/F71/F
NoneNone3.53.50.650.65 GoodGood42F42FNASHNASH62/F62/F
OctOct3.23.20.910.91 GoodGood56M56MPSCPSC60/F60/F
OctOct1.81.81.001.00 GoodGood53F53FNETNET50/F50/F
NoneNone1.11.11.541.54 GoodGood26F26FCaroliCaroli’’s s
diseasedisease10/M10/M
Inflow Inflow
modulationmodulationPostPost--opeope
Peak BiliPeak BiliGBWRGBWR
Graft Graft
functionfunctionDemoDemoDiagnosisDiagnosisAge/SexAge/Sex
SAL, OctSAL, Oct7.17.10.650.65 GoodGood30F30FPSCPSC28/F28/F
14261426
896896
350350
15401540
536536
480480
930930
PVFPVF
833833
2424
2020
1010
1111
1111
22
--
PV pressure PV pressure
gradientgradient
44

Case # 8 Spontaneous Spleno-renal shunt

Pre and IntraPre and Intra--op Hemodynamic Studiesop Hemodynamic Studies
Case #8Case #8
�� PressuresPressures� Free hepatic pressure = 6 mm Hg
� Hepatic wedge pressure = 11 mm Hg
�� Cardiac Output Cardiac Output 7.57 L/min
�� Cardiac IndexCardiac Index 3.88 L/min/m(2)
�� Estimated L lobe graft volume/wt: Estimated L lobe graft volume/wt:
610cc/ 555g 610cc/ 555g
�� GRBWR = 0.84 / 0.76GRBWR = 0.84 / 0.76

Pre and IntraPre and Intra--op Hemodynamic Studiesop Hemodynamic Studies
Case #5Case #5
�� PressuresPressures�� Right atrium Right atrium 12 mmHg12 mmHg
�� Portal vein Portal vein 40 mmHg40 mmHg
�� Cardiac Output Cardiac Output 7.78 L/min7.78 L/min
�� Cardiac IndexCardiac Index 3.5 3.5 L/min/m2L/min/m2
�� Actual graft volume: 620g Actual graft volume: 620g (GRWR 0.57)(GRWR 0.57)


Shunt Flow Shunt Flow --AnhepaticAnhepatic
CO =10 L/min
CI = 4.4 CO/M2


Final Pressures and FlowsFinal Pressures and Flows
Hepatic Artery Augumentation Post Hepatic Artery augumentation
CO = 9.2 L/min
Portal Pressure = 19

0
5
10
15
20
25
5 10 15 20
Bil INR Cr
Post-operative Course
5
4
3
2
1
Bili
INR, Cr
Shuntgram,Ex lapa
Shunt stenting
LRLTDC
MRI
POD



0
5
10
15
20
25
5 10 15 20
Bil INR Cr
Post-operative Course
5
4
3
2
1
BiliINR, Cr
Shuntgram,
Ex lapa
Shunt stenting
LRLTDC
MRI
POD


Ethical PrinciplesEthical Principles
�� Respect for AutonomyRespect for Autonomy
�� Full, voluntary Informed ConsentFull, voluntary Informed Consent
�� BeneficenceBeneficence
�� Psychological or spiritualPsychological or spiritual
�� No physical benefitNo physical benefit
�� NonNon--maleficencemaleficence
�� Justice Justice

Transplantation • Volume 81,
Number 10, May 27, 2006

Vancouver Ethics StatementVancouver Ethics Statement
�� Donor SelectionDonor Selection�� Legal Competency and NonLegal Competency and Non--Traditional SituationsTraditional Situations
�� Informed Consent and AutonomyInformed Consent and Autonomy�� VoluntaryVoluntary
�� Autonomy and consent is necessary but not sufficient Autonomy and consent is necessary but not sufficient (Paternalism vs. autonomy)(Paternalism vs. autonomy)
�� Provide full R/B/A/P information and a comprehensive processProvide full R/B/A/P information and a comprehensive process
�� Responsibility of the Transplant CenterResponsibility of the Transplant Center�� Donor Advocacy Team Donor Advocacy Team
�� Establish Establish medical, psychological and social suitability
�� Provides freedom to withdraw with supportive environmentProvides freedom to withdraw with supportive environment
�� Provide a period of reflectionProvide a period of reflection
�� Assure full retention of informationAssure full retention of information

Who Should Do Living Donor Liver Who Should Do Living Donor Liver TransplantsTransplants??
�� Centers where the need is greatCenters where the need is great�� Significant waiting list and relative donor scarcitySignificant waiting list and relative donor scarcity
�� A well resourced program in a financially secure A well resourced program in a financially secure institutioninstitution
�� Centers with excellent surgical/transplant/ancillary Centers with excellent surgical/transplant/ancillary experience, commitment and planningexperience, commitment and planning
�� An experienced surgeon who really believes in it. An experienced surgeon who really believes in it. �� Living donor surgery should be an academic focus, not a hobby. Living donor surgery should be an academic focus, not a hobby.
�� Participating team members should be committed to the Participating team members should be committed to the growth and development of the field.growth and development of the field.

Fundamental Ethical DimensionsFundamental Ethical Dimensions
�� Need (chance to timely DD?) Need (chance to timely DD?) �� Individual Individual notnot globalglobal
�� Not too much, not too littleNot too much, not too little
�� Donor SafetyDonor Safety
�� MorbidityMorbidity
�� MortalityMortality
�� Probability of a good recipient outcomeProbability of a good recipient outcome�� ShortShort--termterm
�� LongLong--termterm

Ethical Dimensions of Equipoise inLiving Donor Liver Transplantation
The larger the size of triangle, the greater the ethical good.This is the average situation for a right lobe aLDLT
Expected Recipient Outcome
Donor safety Need

Ethical Dimensions of Equipoise inLiving Donor Liver Transplantation
The fundamental tension between autonomy and nonon--
maleficencemaleficence is best equated with the length of the blue line. In
fact, ERO and DS may be the most important two factors
influencing public opinion and in promulgating public policy.
Expected Recipient Outcome
Donor safety Need

Pediatric LRD as a ModelPediatric LRD as a Model
Why is it less conflictedWhy is it less conflicted??
�� Donor usually a parent with clear cut motivationDonor usually a parent with clear cut motivation
�� Donor morbidity and mortality very lowDonor morbidity and mortality very low
�� Minimal concerns regarding graft size or Minimal concerns regarding graft size or recipient statusrecipient status
�� Major indication is Biliary Atresia; a disease that Major indication is Biliary Atresia; a disease that does not recurdoes not recur
�� Recipient outcomes with LRD are better than DDRecipient outcomes with LRD are better than DD
�� Waiting list now dramatically reducedWaiting list now dramatically reduced

Ethical Dimensions of Equipoise in LDLT
This is the equipoise that exists for pediatric living donor transplantation.
Expected Recipient Outcome
Donor safety Need

Ethical Dimensions of Equipoise in LDLT
Expected Recipient Outcome
Donor safety NeedThis is the equipoise that exists in Asia
where deceased donor options are small

Ethical Dimensions of Equipoise in LDLT
This is the equipoise represents the use of standard right lobe LDLT for “Beyond Milan” HCC’s. The blue line is
shorter and the perceived ethical tension is higher, despite great need.
Expected Recipient Outcome
Donor safety Need

Ethical Dimensions of Equipoise in LDLT
Expected Recipient Outcome
Donor safety NeedThis is the equipoise that would exist where excessive recipient need influenced the decision to use a high risk
donor for high risk recipient: Not a good situation

Ethical Dimensions of Equipoise in LDLT
This is the equipoise that might support the use of low risk left lobes for “ Beyond Milan” HCC’s,
Expected Recipient Outcome
Donor safety Need

Ethical Dimensions of Equipoise in LDLT
This is the equipoise that exists for left Lobe transplantation for patients with MELD 10-15.
Expected Recipient Outcome
Donor safety Need

Summary: TechnologicalSummary: Technological
•• It is not all about size!It is not all about size!
•• PrePre--operative measurements of CI and hepatic operative measurements of CI and hepatic wedge pressure, along with GRWR, should wedge pressure, along with GRWR, should guide the choice of left lobe or right lobe guide the choice of left lobe or right lobe
•• The extent of inflow modification should be The extent of inflow modification should be determined by intradetermined by intra--operative hemodynamic operative hemodynamic measurements (flow and pressure).measurements (flow and pressure).
•• Normalization of hepatic Normalization of hepatic -- portal pressure portal pressure gradient (<10 mmHg) with parenchymal flow gradient (<10 mmHg) with parenchymal flow between 1between 1--2 ml/g/min should be achieved2 ml/g/min should be achieved

Summary: EthicalSummary: Ethical
�� Ethical equipoise in LDLT demands the careful Ethical equipoise in LDLT demands the careful balance of need, donor safety and chance for a balance of need, donor safety and chance for a good outcomegood outcome
�� The proper balance is effected by societal The proper balance is effected by societal beliefs that effect deceased donor organ beliefs that effect deceased donor organ donation and availability, and specific recipient donation and availability, and specific recipient and donor characteristicsand donor characteristics
�� There is continuous tension between personal There is continuous tension between personal autonomy and physician/center/society desire autonomy and physician/center/society desire for nonfor non--maleficencemaleficence

ConclusionsConclusions
�� Use of left lobes improves donor safety, satisfies our Use of left lobes improves donor safety, satisfies our ethical principles and is expanding.ethical principles and is expanding.
�� There is a continuing shortage of livers that can be There is a continuing shortage of livers that can be relieved by expanded utilization of living donorsrelieved by expanded utilization of living donors
�� The clear indications (ex. HCC) that existed prior to The clear indications (ex. HCC) that existed prior to MELD are now more vague and candidate selection is MELD are now more vague and candidate selection is more complexmore complex
�� Carefully selected patients with even with MELDCarefully selected patients with even with MELD’’s < 15 s < 15 show survival benefit with Ashow survival benefit with A--toto--A LDLTA LDLT
�� Left lobe grafts should be used preferentially if graft size Left lobe grafts should be used preferentially if graft size and recipient parameters are favorableand recipient parameters are favorable
�� ““Primum Non NocerePrimum Non Nocere”” is The Way Forward is The Way Forward