

Maria Grazia Ghi Oncologia Medica 2 - aiom.it Maria Grazia Ghi Oncologia Medica 2 Istituto...
34
Maria Grazia Ghi Oncologia Medica 2 Istituto Oncologico Veneto – IRCCS, Padova Milano, 17 novembre 2017 Tumori testa collo Il ruolo dell’immunoterapia
Transcript of Maria Grazia Ghi Oncologia Medica 2 - aiom.it Maria Grazia Ghi Oncologia Medica 2 Istituto...

Maria Grazia Ghi
Oncologia Medica 2 Istituto Oncologico Veneto – IRCCS, Padova
Milano, 17 novembre 2017
Tumori testa collo
Il ruolo dell’immunoterapia

Rationale for immunotherapy in HNSCC
1. Response to immunotherapy correlates with mutational burden
2. Tumors containing T-cell infiltrates (inflamed phenotype) might
be induced to respond to immunotherapy
3. High mutational burden in H&N cancer (tobacco use and HPV)
1. High expression of PD-L1 (50-78%) 1. Ferris RL, et al. J Clin Oncol. 2015;33:3293-3304 2. Badoual C, et al. Cancer Res. 2013;73:128-138 3. Concha-Benavente F, et al. Cancer Res. 2016;76:1031-1043

Anti PD-1 in HNSCC: finalized studies
- Pembrolizumab, humanized anti PD-1 moAb
- Nivolumab, fully human anti PD-1 moAb

- The majority of pts with R/M are no longer amenable to curative treatment - PF + cetuximab (Extreme regimen) recommended first line for fit patients with R/M disease (median OS 10 mo) - Median OS for pts progressed after platinum-based therapy is 6 months or less - New therapeutic options needed to prolong survival while optmizing QoL
Recurrent/metastatic HNSCC

CheckMate 141 phase III trial
361
54.5% > 2 lines treatment

CheckMate 141 : efficacy
Late separation of the survival curves with a subsequent plateau phase
Overall Survival Progression Free Survival
with ~1-Year Follow-up (ASCO 2017)
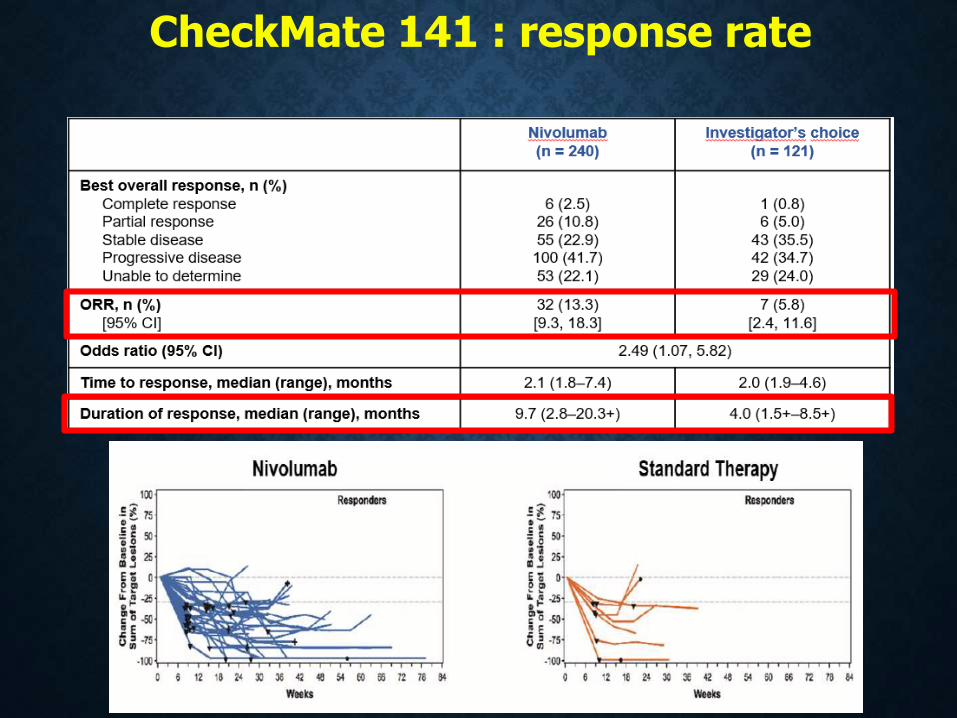
CheckMate 141 : response rate

CheckMate 141 : Adverse Events

CheckMate 141 trial OS according to PD-L1 expression (tumor cells)
The magnitude of OS benefit of nivo greater in PD-L1 positive
Increasing PD-L1 expression did not result in further OS benefit
Nivolumab effective regardless of PD-L1 expression
Dako, IHC 28-8

CheckMate 141 trial OS according to HPV status (25% HPV +)
Nivolumab effective regardless of HPV status
The magnitude of OS benefit of nivo greater in HPV positive

Harrington KJ et al, Lancet Oncol 2017
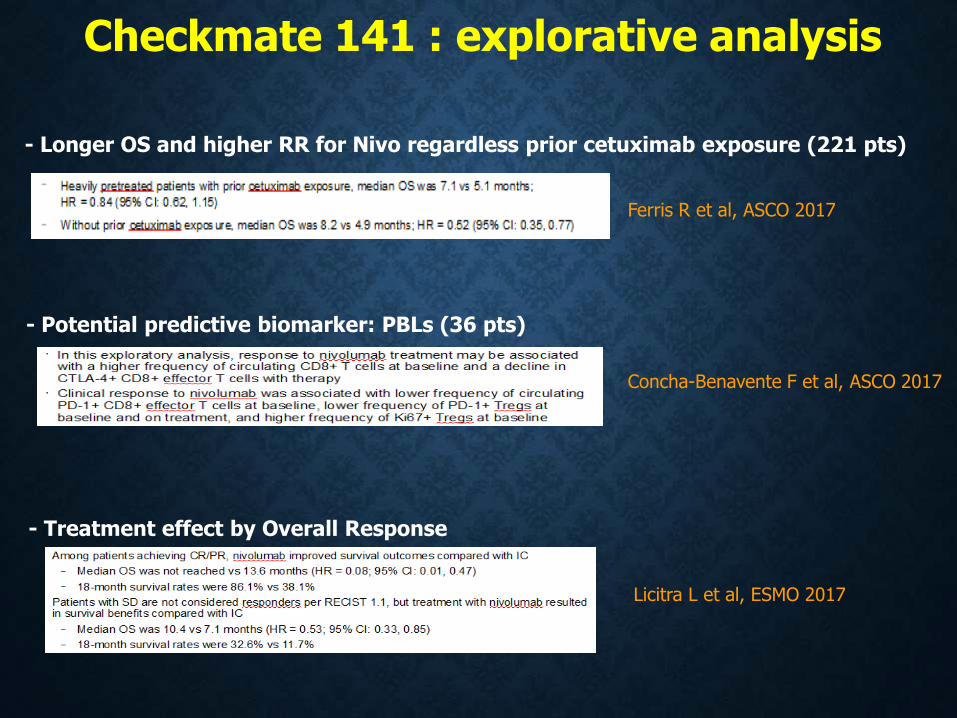
Checkmate 141 : explorative analysis
- Longer OS and higher RR for Nivo regardless prior cetuximab exposure (221 pts)
Ferris R et al, ASCO 2017
- Potential predictive biomarker: PBLs (36 pts)
Concha-Benavente F et al, ASCO 2017
- Treatment effect by Overall Response
Licitra L et al, ESMO 2017
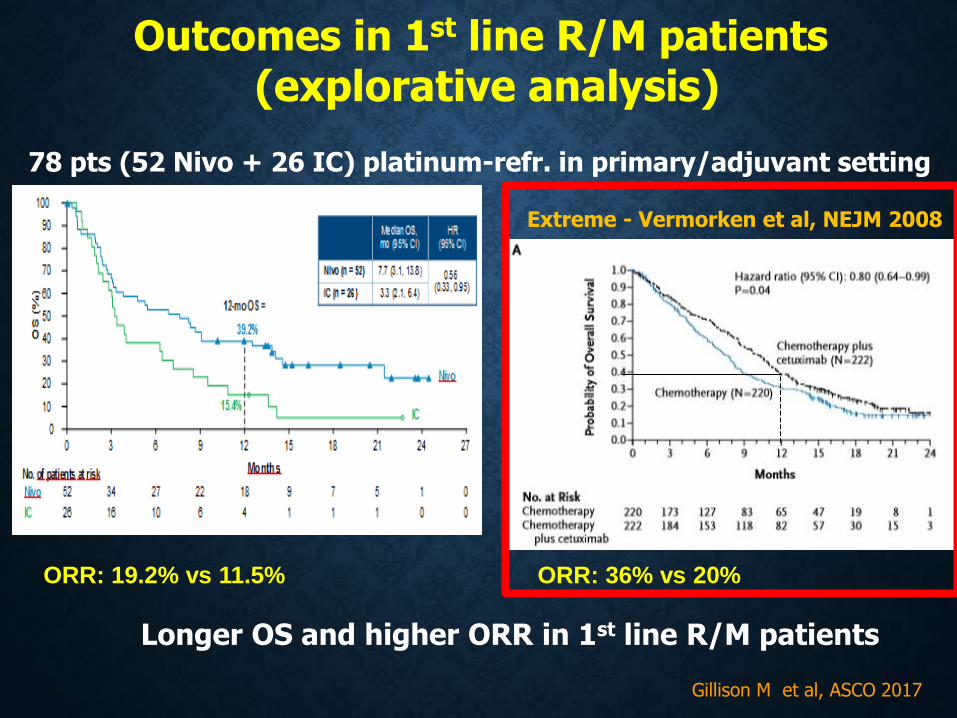
Outcomes in 1st line R/M patients
(explorative analysis)
78 pts (52 Nivo + 26 IC) platinum-refr. in primary/adjuvant setting
Gillison M et al, ASCO 2017
Longer OS and higher ORR in 1st line R/M patients
Extreme - Vermorken et al, NEJM 2008
ORR: 19.2% vs 11.5% ORR: 36% vs 20%

Nivo beyond progression subgroups
(explorative analysis)
146 pts progressed -> 62 (42%) treated beyond progression 25.8% of the pts in tne Nivo arm
Haddad R et al, ESMO 2017
Tumor reduction in 24% of pts (15/62) median OS of 12.7 months

1. Seiwert T et al, Lancet Oncol 2016 2. Chow L et al, J Clin Oncol 2016
Pembrolizumab in R/M HNSCC
Bauml J et al, JCO 2017
PD-L1 expression: Dako, IHC 22C3

Keynote-012 and Keynote 055 trials
1. Seiwert T et al, Lancet Oncol 2016 2. Chow L et al, J Clin Oncol 2016 3. Bauml et al, J Clin Oncol 2017
Cohen E et al, ESMO 2017
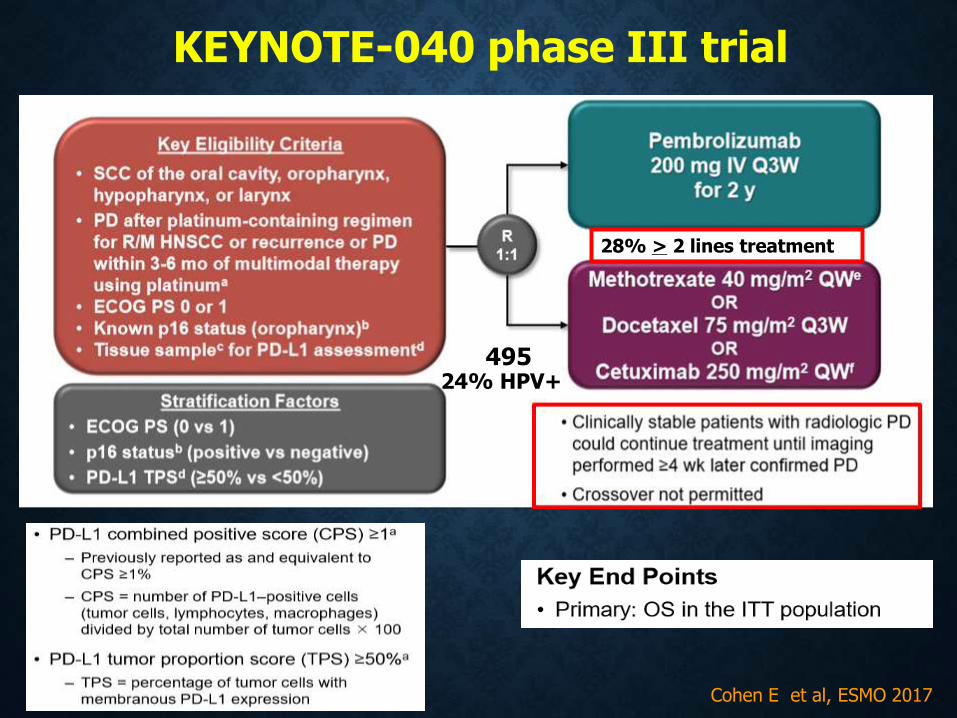
KEYNOTE-040 phase III trial
495
28% > 2 lines treatment
24% HPV+

KEYNOTE-040: efficacy
Median FU 7.3 mo (range 0.03-28.4)
Cohen E et al, ESMO 2017

OS by PD-L1
expression
PFS by PD-L1
expression
Cohen E et al, ESMO 2017

KEYNOTE-040: ORR and AEs
Cohen E et al, ESMO 2017

Cohen E et al, ESMO 2017
KEYNOTE-040
cross over from SOC to Pembro= 12.5%

CheckMate 141 vs KEYNOTE 040
. Different drug effect?
* TPS vs CPS; different assays
ChecMate 141 Nivo n=240
ChecMate 141 IC n=121
Keynote-040 Pembro n=247
Keynote-040 IC n=248
ECOG PS > 1
79.2%
80.2% 71.3% 72.6%
> 2 previous treatment line
55.8% 52.1% 29.1% 27%
P 16 +ve 26.2% 24% 24.7% 23.4%
PDL-1* >1 36.7% 50.4% 79% 77%
Cross over - nr - 12.5%
Immune checkpoint inhibitor beyond PD
25.8% - 4.5% -

Anti PD-L1 in HNSCC
- Durvalumab, humanized anti PD-L1 moAb
- Atezolizumab, fully human anti PD-L1 moAb

Zandberg ZP et al, ESMO 2017
112 pts :TC > 25%, Ventana IHC SP263

Bahleda R et al, ESMO 2017
32 pts ; 53% > 2 lines treatment
PD-L1 expression of ≥ 5% on IC =78% (IC2/3)
ORR median duration: 7.4 mo (26.2 mo in IC2/3) PFS: median 2.6 mo; 31% at 6 mo OS: median 6 mo; 36% at 1 y

Future directions
Integration of immunotherapy
in earlier lines of treatment
- Combination with concomitant CRT
- Combination with surgery
- Combination with targeted therapy
- Combination with other immunotherapies

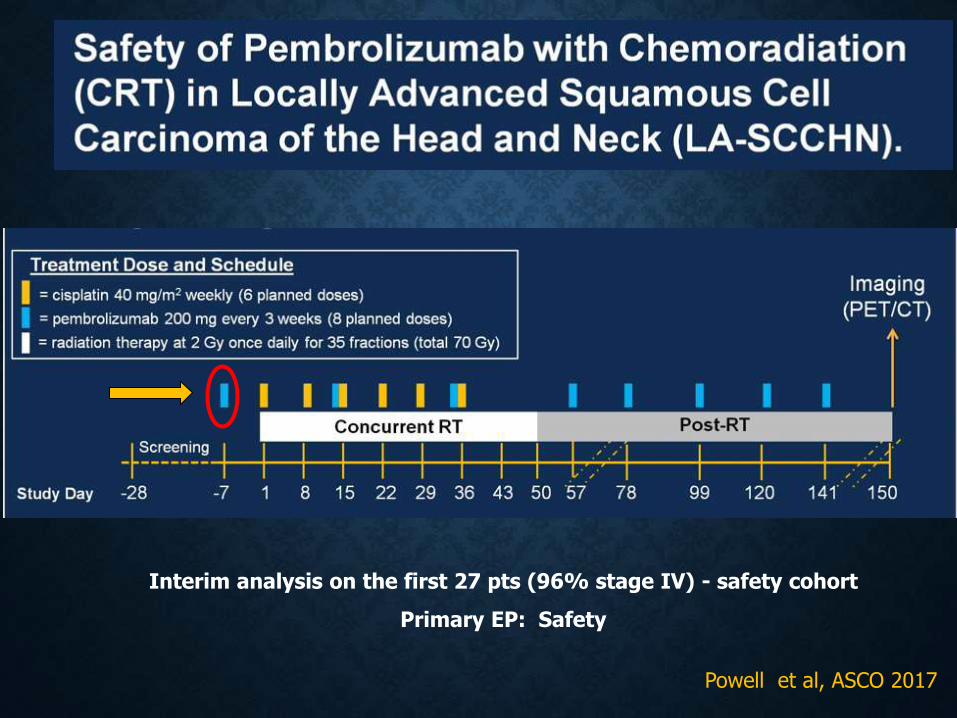
Powell et al, ASCO 2017
Interim analysis on the first 27 pts (96% stage IV) - safety cohort
Primary EP: Safety
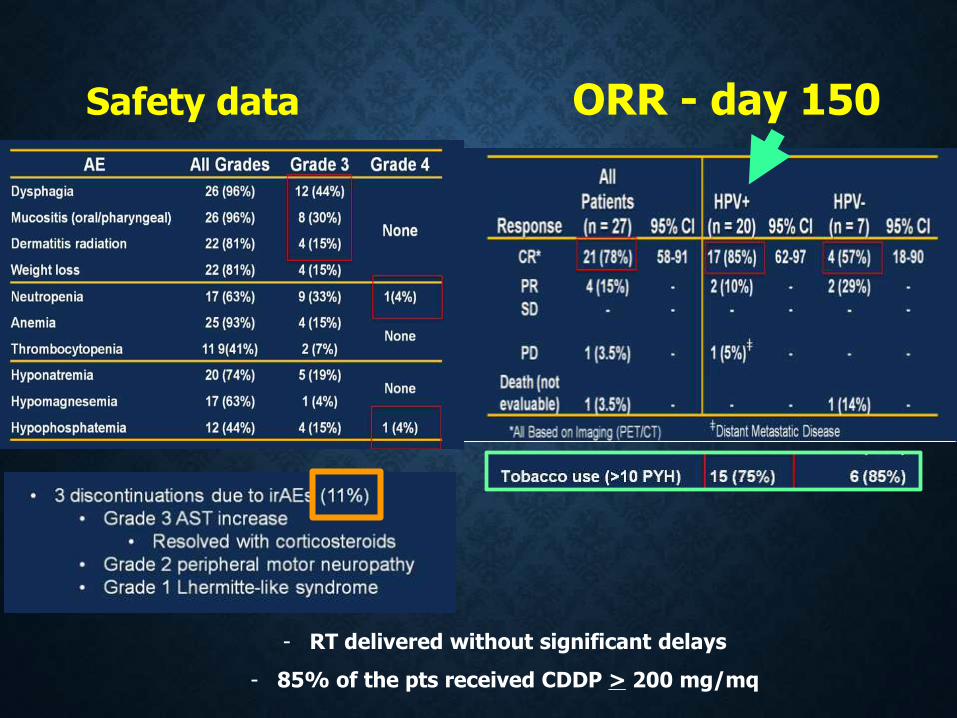
Safety data ORR - day 150
- RT delivered without significant delays
- 85% of the pts received CDDP > 200 mg/mq

Primary EP: LRR and DM rate reduce from 35% to 15% in high risk pts
High risk
Low risk
Preliminary data on the first 25 patients (monocenter)
96% stage IV; 58% PD-L1 >1%
Planned sample size: 46 pts, HPV - ve
Uppaluri et al, ASCO 2017
Pathologic treatment effect : tumor necrosis and/or giant cell/histiocytic reaction to keratinous debris in > 10% of tumor area

Preliminary data on 29 patients evaluable for safety (PD-L1 > 1% =65%)
Primary EP: safety and tolerability
Ferris R et al, ESMO 2017

Immunotherapy in HNSCC
- Similar activity/efficacy data for Pembro and Nivo
- Well tolerated, with manageable toxicity profile
- RR and median PFS are not good surrogates for clinical benefit
- Evidence of benefit regardless of PD-L1 expression and HPV
status but benefit of different size
- Preliminary data for combination treatment strategies in earlier
line of treatment
Unanswered questions
- Criteria for response evaluation: Recist vs Immunological
- Optimal timing of immunoth and treatment duration
-PD-L1 expression as a predictive marker is still controversial
standardized definition of PD-L1 positivity
ICH cut off
tumor cells vs tumor infiltrating inflammatory cells
-Timing biopsy (archival or fresh), primary vs metastatic
-A single biomarker may not be enough
Patient selection and biomarker crucial for further development
Cost : 120-150,000 $/year/patient


















