Marginal Zone Lymphoma: Pathobiology and treatment · Antigen influx occurs in the marginal zone of...
49
Marginal Zone Lymphoma: Pathobiology and treatment Date October 27,2017 Ariela Noy, MD Attending Physician MSKCC Professor of Medicine Weill Cornell Medical College www. MSKCC.org
Transcript of Marginal Zone Lymphoma: Pathobiology and treatment · Antigen influx occurs in the marginal zone of...

Marginal Zone Lymphoma:
Pathobiology and treatment
Date October 27,2017
Ariela Noy, MD
Attending Physician MSKCC
Professor of Medicine Weill Cornell Medical College
www. MSKCC.org

Speaker Disclosure
• Research funding from Pharmacyclics LLC, an AbbVie Company
• Travel, accommodation, or expenses from Pharmacyclics LLC, an
AbbVie Company; Janssen Global

Lymphomas reflect the biology of the cell at which maturation occurs.

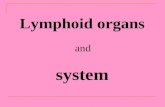
Antigen influx occurs in the marginal zone of the lymphoid follicle, the splenic white pulp or the mucosa associated lymphoid area.
Phenotype: medium sized cells with irregular nuclei and abundant pale cytoplasm, and typically express IgM and CD25 but not CD5, CD10, CD23, and usually not IgD
Anne Tierens et al. Blood 1999;93:226-234
©1999 by American Society of Hematology

• An indolent B cell lymphoma with similarities to follicular lymphoma.
• About 5-15% of all non-Hodgkin lymphoma.
• Stage I disease is more common in MZL than follicular lymphoma due to marginal zone biology.
• Stage I disease is curable by surgery or radiation.
• Indolent lymphomas are generally incurable when they present with disseminated disease, but patients can live for years or even decades.
• Judicious use of therapy is warranted to preserve QOL.
5
Marginal Zone Lymphoma: Basics

6
Three major categories of marginal zone lymphoma have a unique biology
% of MZL % of NHL
Mucosa associatedlymphoma of lymphoid tissue (MALT)
50-70% 7-8%
Splenic MZL 10-30% <1%
Nodal MZL 10-30% <1%

• 50% of MALT has an t(11;18)(q21;q21) fusion gene link the N-terminal portion of API2 linked to the C-terminus of a novel protein, MLT (MALT1).
• API2 fusion likely leads to increased anti-apoptotic activity
• API2-MLT may lead to activation of NF-κB
• The less common t(1;14)(p22;q32) activates Bcl-10, an anti-apoptosis gene.
7
Translocations sometimes play a role in the pathogenesis of distinct.

• Hashimoto thyroiditis
• Myoepithelial sialoadenitis (MESA) with or without associated Sjögren syndrome
• Lymphoid interstitial pneumopathy.
8
MZL may be associated with autoimmunity.

• Helicobacter pylori in gastric MALT.• Triple antiobiotic therapy is 80% effective.
• Relapses can occur
• Hepatitis C virus (HCV with MALT, splenic and nodal)• Virtually 100% effective in splenic MZL
• Borrelia burgdorferi (Lyme disease) possible role in cutaneousMALT.
• Campylobacter jejuni in small intestine has been associated with immunoproliferative small intestinal disease (IPSID)
• Chlamydia psittaci infection with ocular adnexal MALT lymphoma
9
5 microbial antigens are known to be related to MZL and have therapeutic implications.

10
MALT: Example of lymphoepithelial lesion in the parotid gland
A. Heavy infiltrationFew residual folliclesCystic dilation
B. “monocytoid” cells form a haloaround the ducts and infiltrate
into the duct epitheliumC. CD20 D. interstitial infiltrate of CD3+T cellsE. CD21 stains follicular dendritic cell
meshworkF. IgD stains non tumor cells compared with the CD20 stain in slide C.
MALT is typically IgM +, IgD neg.

Standard first-line treatment approaches in adult NMZL not associated with HCV or H. Pylori. Treatment follows the approach used with
follicular lymphoma.
Catherine Thieblemont et al. Blood 2016;127:2064-2071
©2016 by American Society of Hematology
Rituximab monotherapy-moderate tumor burden.

Approach to splenic MZL includes splenectomy which used to be first line.

Treatment naïve group: (n=23)
• ORR 87% with 48% CR
• Median DOR of 22 months;
Beyond first line therapy group: (n=11)
• ORR of 45% with 36%CR in 36%
• Median time to treatment failure of 12 months.
13
Rituximab monotherapy: (n=34) extranodal MZL:
Conconi, Blood, 2003

• Rituximab in combination with chemotherapy (alkylating agents or purine analogs) has shown ORRs of 71%-94% (CR in 20%-78%) in predominantly chemotherapy-naïve or treatment-naïve patients.
• Treatment is associated with 30% grade 3/4 cytopenias.
14
Immunochemotherapy for treatment naiive pt with MZL
Total n %OR/CR
DOR Grade 3/4
Becker2015
R-Benda 37 85/46 Unknown 17% heme
Finn 2014 RCHOP 18 71/24 Unknown 90%
Finn 2014 R-Benda 28 92/20 Not reached >40%
Zucca 2014 chlorambuci 44 87/65 Not reached (mdn f/u 62 mo)
>10%
Zucca 2014 R-chorambucil
52 94/78 Not reached mdn f/u 62 mo
>10%

Transformation to diffuse large B cell lymphoma (DLBCL) requires a different approach
• Occurs in about 15% of patients
• At a median of 4.5 years after diagnosis (range, 1-22)
• Poorly studied
• Maybe associated with p53 mutation or mycactivation
• Approaches generally follow that of DLBCL
• Prior therapies likely portends a worse prognosis

• B-cell receptor signaling
• JAK/STAT
• NF-κB
• NOTCH
• Toll-like receptor signaling pathways
• Intracellular processes such as the cell cycle, chromatin remodeling, and transcriptional regulation in terms of epigenetic modifiers, histones, or transcriptional co-repressors
• Immune escape via T-cell–mediated tumor surveillance.
Deregulated pathways in MZL amenable to therapeutic intervention.

NMZL: 41 genes in 35 patients showed recurrent mutations in >9% of cases including 4 commonly mutated genes in NHL
Spina Blood 2016

Total n/ Rel-Refr
%OR/CR DOR Grade 3/4
Raderer2006
RCHOP/CNOP
26/10 77/23 85% at 19 mo 31%
Kisewetter2014
R-Benda 14/8 93/71 86% at 23 mo 29%
Rummel2016
R-Benda 10/10 82/51 No subtype data
20%
R-fludara 8/8 40/17 No subtype data
20%
Total 58/38
Second line chemoimmunotherapy in MZL

BCR-Signaling Pathway & Inhibition of BTK With Ibrutinib
• MZL is often linked to chronic antigen stimulation by microbial and viral pathogens (infections),1,2 which may induce aberrant BCR signaling.2
• BTK is a critical component of the BCR signaling pathway.
• Ibrutinib is a first-in-class, once-daily, oral inhibitor of BTK.
1. Suarez et al. Blood 2006;107:3034-44; 2. Niemann et al. Semin Cancer Biol 2013;23:410-21.Figure adapted from Buggy and Elias. Int Rev Immunol. 2012;31:119:32; de Rooij et al. Blood 2012;119:2590-94
DAG InsP3
BCR
Nucleus
SYK
CXCR4/5C
D7
9A
CD
79
B
• Cell Viability
• Cell Adhesion• Cell Migration
and Homing
Lyn/Fyn
BTKP
PLCgP
P
PKCb
IKK
PI3K
ibrutinib
CXCL12/13
Simplified signaling pathway adapted from Buggy and Elias. Int Rev Immunol. 2012;31:119-13 andde Rooij et al. Blood. 2012;119:2590-2594.

Ibrutinib was previously US FDA approved for other B cell malignancies
• Chronic lymphocytic leukemia including del17p (p53) (now also upfront for all CLL)
• Mantle cell lymphoma (MCL) with at least 1 prior therapy
• Waldenström macroglobulinemia
• All with high levels of activity and a better safety profile compared with cytotoxic chemotherapy
20

• Due to paucity of randomized trials, no standard of care was established in patients with disseminated disease who require systemic therapy (either frontline or at relapse).
• Patients were treated along follicular lymphoma paradigms, but did not have access to non-chemotherapy approaches.
• Targeted therapies are• Based on pathogenesis
• Non-cytotoxic
• Expected to be better tolerated .
• We evaluated the efficacy and safety of single-agent ibrutinib in patients with relapsed/refractory MZL.
Background for PCYC 1121 study

PCYC-1121 Study Design
1. Cheson et al. J Clin Oncol 2007;25:579-86.
This Phase 2 study is the largest prospective trial to date conducted in patients with relapsed/refractory MZL including all subtypes (splenic, nodal, extranodal).
R/R MZL
N = 63
ibrutinib 560 mg PO once daily until disease progression or
unacceptable toxicity
Key eligibility criteria
Histologically confirmed MZL of all subtypes
Refractory or progressive MZL
At least 1 measurable lesion (>1.5 cm in longest dimension) outside of the spleen
ECOG PS ≤2
≥1 prior therapy including at least 1 anti-CD20-directed regimen (CIT or rituximab monotherapy)
Primary endpoint ORR by
independent review committee (IRC) by 2007 IWG criteria1
Secondary endpoint DOR
PFS OS Safety*
*Adverse events (AEs) were assessed according to CTCAE v4.03. Collection period for AEs: from screening to 30 days after last ibrutinib dose.

• Suspicion of large cell transformation required a pre-treatment biopsy. • High LDH
• Rapidly growing masses
• High SUVs on FDG PET
• Concurrent use of warfarin or other vitamin K antagonists
• Use of a strong CYP3A inhibitor
Ineligible patients

Patient Demographics & Baseline Characteristics
Characteristic Total (N = 63)
Median age (range), yearAge ≥65 years, n (%)
66 (30-92)36 (57)
MZL subtype, n (%)SplenicNodalExtranodal
14 (22)17 (27)32 (51)
Bulky disease 6 cm, n (%) 14 (22)Bone marrow involvement, n (%) 21 (33)Baseline cytopenias, n (%)
Any cytopeniaHemoglobin ≤11 g/dlPlatelet count ≤100,000 per mm3
Absolute neutrophil count ≤1500 per mm3
27 (43)27 (43)6 (10)1 (2)
Lactate dehydrogenase (LDH), ≥350 unit/liter, n (%) 12 (19)
Creatinine clearance <60 ml/min, n (%) 9 (14)

Prior Therapies and Indications for Treatment
Characteristic Total (N = 63)
Median no. of prior therapies (range)No. of prior systemic therapies, n (%)
12≥3
2 (1-9)
23 (37)18 (29)22 (35)
Types of prior therapies, n (%)Rituximab monotherapy onlyRituximab-based chemoimmunotherapyRadiationSplenectomyAutologous hematopoietic stem cell transplantation
17 (27)40 (63)9 (14)4 (6)2 (3)
Refractory to most recent therapy, n (%) 14 (22)
15 (24%) patients had B symptoms at baseline.
Indications for treatment (investigator-reported) included symptoms (52%), bulky disease (24%), threatened end-organ function (16%), and need for transfusions (10%).

26
Patient Disposition
Median duration of ibrutinib exposure was 11.6 months (range, 0.2-30.4), with exposure ≥12 months in 48%.
At a median follow-up of 19.4 months for the all-treated population (N=63), 38% of patients continue study treatment.
Primary reasons for discontinuing ibrutinib at any time during study were— Disease progression (n=20, 32%)— Adverse event (n=11, 17.5%)— Withdrawal of consent (n=4, 6%)— Investigator decision (n=4, 6%)

Majority of Patients With R/R MZL Had Tumor Reduction With Ibrutinib
*Data based on investigator assessment for 60 patients; 3 patients who discontinued treatment prior to first response assessment were not evaluable. Investigator-assessed data were used given that IRC assessment included 2 separate sets of SPD data due to readings by 2 radiologists
Tumor shrinkage was seen in 79% (50/63) patients, implying BTK signaling as an important growth and survival factor in MZL.

Best Response Results in Clinical Benefit in the Majority of Patients With R/R MZL
Clinical efficacy (IRC assessment) as judged by ORR was 48%, and clinical benefit rate (CBR = PR+CR+SD) was 83%.
Concordance rate for ORR between IRC and investigator assessment was 85%.
Median time to initial response: 4.5 months and to best response: 5.2 months.
0
10
20
30
40
50
60
70
80
90
100
SD PD SD PD
Be
st R
esp
on
se (
%)
4/195 2/195 1/196
CRPR
7%ORR 48%
35% 35%
5%
47%
12%
3%
45%
CRPR
ORR 53%
IRC Assessment (N=60) Investigator Assessment (N=60)
CBR= 83% CBR= 88%

Ibrutinib Was Effective Across All MZL Subgroups
ORR by IRC assessment

Ibrutinib Was Effective Across All MZL Subgroups
*Results of bone marrow assessment were considered indeterminate in 4 patients.
Patients who received prior rituximab only (n=16) and who received CIT (n=39) showed good outcomes with ibrutinib (ORR of 69% and 46%, respectively)
ORR by IRC assessment

Ibrutinib Was Effective Across All Relapsed Patients Regardless of Duration of Response to Prior Therapy
55%
45% 44%
54%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Time to Relapse From Start of Last Prior Therapy
OR
R, %
≤6 months 6 months 12 months≤12 months

Ibrutinib Demonstrated Durable Responses
Median follow-up: 19.4 mo(95% CI: 17.6, 22.3)
IRC Investigator
Median DOR (95% CI) NR (16.7, NR) 19.4 mo (7.3, NR)
18-mo DOR rate 62% 54%
NR, not reached
DOR

• Median PFS by MZL subtype was 19.4 months (95% CI, 8.2-NR) for splenic, 13.8 months (95% CI, 8.3-NR) for extranodal, and 8.3 months (95% CI, 2.8-NR) for nodal MZL.
Progression-Free Survival and Overall Survival
Median follow-up: 19.4 mo(95% CI: 17.6, 22.3)
PFS OS
IRC Investigator
Median PFS (95% CI)
14.2 (8.3, NR)15.7 (12.0, NR)
18-mo PFS rate 45% 49%
Investigator
Median OS (95% CI)
NR (NR, NR)
18-mo OS rate 81%
Median follow-up: 19.4 mo(95% CI: 17.6, 22.3)
NR, not reached

Summary of Efficacy Outcomes by IRC
At a median follow-up of 19.4 months, clinical efficacy as judged by ORR was 48%, and clinical benefit rate was 83%.
Durable responses were observed in this population in which all patients had prior rituximab exposure (DOR at 18 months=62%).
Median PFS was 14.2 months, and median OS was not reached.

Common Any-Grade Adverse Events
AEs were largely grade 1-2 events, and the discontinuation rate due to AEs was low.
Most common serious AEs occurring in ≥2 patients included
— Pneumonia (8%)
— Cellulitis, autoimmune hemolytic anemia, pneumothorax, and sepsis (3% each).
Adverse Event (≥20%), n (%) N = 63
Fatigue 28 (44)Diarrhea 27 (43)Anemia 21 (33)Nausea 16 (25)Arthralgia 15 (24)Peripheral edema 15 (24)Thrombocytopenia 15 (24)Cough 14 (22)Dyspnea 13 (21)Upper respiratory tract infection 13 (21)

Grade ≥3 Adverse Events
Grade ≥3 AE Occurring in ≥2 Patients (3%) , n(%) N = 63
Anemia 9 (14)Pneumonia 5 (8)Fatigue 4 (6)Cellulitis 3 (5)Diarrhea 3 (5)Hypertension 3 (5)Lymphocyte count decreased 3 (5)Neutropenia 3 (5)Asthenia 2 (3)Autoimmune hemolytic anemia 2 (3)Blood bilirubin increased 2 (3)Muscle spasms 2 (3)Neutrophil count decreased 2 (3)Pneumothorax 2 (3)Sepsis 2 (3)

• AEs leading to dose reductions occurred in 6 patients (10%):
– Fatigue and stomatitis (3%) were the most common.
– 4 patients had 1 dose reduction, and 2 patients had 2 dose reductions.
• Of the 11 (17.5%) AEs leading to treatment discontinuation, diarrhea was the most common AE (3%).
• Three treatment-emergent AEs resulted in death:
– Progressive disease (after 30 days of treatment)
– Cerebral hemorrhage (19 days after discontinuing ibrutinib; reported as unlikely related to study treatment)
– Multiple system organ failure (in a patient with extensive pulmonary involvement by lymphoma who contracted parainfluenza pneumonia)
Dose Reductions, Discontinuations, and Deaths Due to Adverse Events

• Bleeding events– Occurred in 37 patients (59%), primarily grade 1-2 events.
– Any-grade bleeding events occurring in ≥2 (3%) patients included:
• Increased tendency to bruise (19%)
• Epistaxis (13%)
• Contusion (10%)
• Ecchymosis (10%)
• Hematuria (8%)
• Petechiae (5%)
• Hematoma and purpura (3% each)
– AE of major bleeding reported in 1 patient (grade 5 cerebral hemorrhage 19 days after ibrutinib discontinuation).
Bleeding

• Atrial fibrillation – Occurred in 4 patients (6%), which was grade 1-2 in all cases
– Did not lead to dose reductions or treatment discontinuation
• Other malignancies– Reported in 2 (3%) during the treatment-emergent period
– Included basal cell carcinoma [n=1 (2%)] and plasma cell myeloma [n=1 (2%)]
Atrial Fibrillation and Other Malignancies

• 66 yo man at study entry. BMI 45.• 2009 dx with lymphocytosis on routine office visit and cell markers
c/w MZL.• 2012 progressive nodal disease, massive splenomegaly to the pelvic
brim. ALC 44/ANC 4.4 HB 9 platelets 140• Feb 2013 rituximab refractory• July 2013 splenectomy with improvement in Hb • October 2014 progressive diffuse adenopathy• Started ibrutinib on protocol 14-058 on 10/2014 ALC 6/Hb 12• CT 2/2017: 3.7 cm largest node; ALC 10/ANC 2 Hb 14 platelets 140• AE: atrial fibrillation treated with ablation.• 10/2017 remains on therapy with near CR now on long term f/u
study.
Patient Vignette #1: splenic MZL with nodal disease and marrow compromise

Pre-treatment 10/2014 On treatment 2/2017

• 59 yo man at study entry• 2011 with massive splenic marginal zone lymphoma, • Rituximab without response.• Splenectomy 2/7/2012.• After splenectomy pt developed progressive lymphocytosis and
anemia.• Started ibrutinib on protocol 14-058 on 8/27/14, for progressive
lymphadenopathy throughout up to 4 cm and ALC 60 ANC 3.4; Hb 9, platelets 184
• 03/2017 No lymphadenopathy and ALC 4.3 ANC 5.2; HGB 14, Platelets 328.
• AE: symptomatic bigeminy and grade 2 HTN: 560420 mg ; 30 days off drug bigeminy persisted. Pt elected 280 mg ongoing dosing and is now on long term follow up study.
Patient vignette #2: splenic MZL with nodal disease and marrow compromise

Pre-treatment 8/2014 On treatment 3/2017

• An ORR of 48% (with CR in 2 patients)
• Responses occurred across all the subtypes
• Duration of response 62% at 18 months despite prior chemoimmunohtherpay in most patients.
• Clinically meaningful tumor shrinkage (79%), high clinical benefit rate (83%).
• Well tolerated; AE profile consistent with previously published studies of ibrutinib.
• These results support BTK signaling blockade via single-agent ibrutinib as an effective, well tolerated, chemotherapy-free treatment option for patients with relapsed/refractory MZL.
Conclusions

3rd Annual MSK Symposium on
LYMPHOMA State-of-the-Art in Biology, Therapy and Pat ient Care
MAY 11-12, 20 18 Zuckerman Research Center
New York City
# MSKLYMPHOMACME
For more informat ion or t o register, visit :
www.mskcc.org/ lymphomacourse

• The baseline PET/CT scan (1/6/2015) showing no evidence of supraclavicular lymphadenopathy(Panel A).
• At study week 13 of treatment (4/22/2015), the PET/CT scan demonstrated multiple hypermetabolic bilateral supraclavicular lymph nodes, which increased in number, size, and metabolism (Panel B). Biopsy did not show lymphoma.
• Ibrutinib was continued, and at study week 25 of treatment (7/15/2015), PET/CT demonstrated multiple hypermetabolic bilateral supraclavicular nodes with either resolution of a few, appearance of new foci, and either increased, decreased, or no significant change in size and metabolism of previous foci indicating a “mixed response” (Panel C).
Tumor Flare: Patient 1
PET/CT Baseline Week 13 Week 25A B C

Tumor Flare: Patient 1
Fig 2.) Core biopsy of a new right supraclavicular node (Week 13) showed small to intermediate lymphocytes in a fibrous background (Panels A-D). Overall immunostains showed mixed small B and T lymphocytes. Black arrows indicate fibrosis, and red arrows indicate lymphocytes.

Ibrutinib was continued, and at study week 73 (D) CT/PET scan showed 2 new metabolically active right lower cervical lymph nodes compared to a prior study. Treatment was discontinued to assess for disease progression (repeat biopsy was not performed.)
Four weeks later (week 77), the CT/PET scan showed interval resolution of the hypermetabolic right cervical lymph nodes, and development of a hypermetabolic confluent R perihilar lymphadenopathy which measures 6.1 x 5.6 cm with an SUV 22.0. VATS directed biopsy did not show lymphoma.
Tumor Flare: Patient 1Week 73 Week 77

• Ibrutinib was continued, and at week 85 (9/7/16) the PET CT demonstrated a significant decrease in the perihilar lymphadenopathy that now measures 4.8 x 4x4 cm with an SUV of 19.5.
Tumor Flare: Patient 1 Week 85