March 2008 NewsLine - National Hospice and Palliative Care ... · PDF fileQuarterly Insights...
56
New CoPs: Planning Tips See Page 55. Access: Beyond Cancer National Hospice and Palliative Care Organization Quarterly Insights Edition March 2008
Transcript of March 2008 NewsLine - National Hospice and Palliative Care ... · PDF fileQuarterly Insights...
New
CoP
s: Plann
ing
Tips
See Pa
ge 55.
Access:Beyond Cancer
National Hospice and Palliative Care
Organization
Quarterly Insights Edition March 2008
The Hospice Pharmacia Difference
Passionate for the Appropriate Use of Medication
Contact Us Today!
877-882-7822 | [email protected]
www.hospicepharmacia.com
HOSPICE PHARMACIA PROVIDES:
• 24/7 access to palliative care-trained PharmDs for clinical consultation
• Medication Use Guidelines (MUGs®) for evidence-based care
• Community pharmacy access plus overnight courier delivery of medications
• Online reporting tools
• Interfaces with hospice software providers
• Per diem pricing providing stable and predictable medication-related costs
• Pharmacy service solutions that are tailored to individual hospices needs
...and more!
COMPREHENSIVE
PHARMACY
SERVICES
FOR HOSPICE
NewsLine 3
Table of ContentsMarch 2008
Insights:
NCHPP 2008 Section Leaders . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
Introduction:
Meeting the Needs of Today’s Patients . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
Section 1 – Obstacles
Using What We’ve Learned to Expand Access . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
Section 2 – Options
The Changing Face of Access . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
ALS Patient Care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14
Spiritual Care for Nonverbal Patients . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18
Understanding the Mindset of Dementia Patients . . . . . . . . . . . . . . . . . . . . . . . . 20
Treating Pain in Nonverbal Patients . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22
Grief and the Older Adult . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26
Section 3 – Opportunities
Not Just for Cancer Anymore: Diversifying Your Patient
Mix Through Proactive Marketing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30
Rehabilitation Tools to Promote Access . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 34
Improving Access to Patients With Pulmonary Fibrosis . . . . . . . . . . . . . . . . . . . . 37
Promoting Responsiveness in End-of-Life Care . . . . . . . . . . . . . . . . . . . . . . . . . 41
NewsLine:
Improving Quality of Life for Patients With Advanced Dementia . . . . . . . . . . . . . .43
People and Places . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 47
A Closer Look at NHPCO’s Inclusion and Access Toolbox . . . . . . . . . . . . . . . . . . . 49
Marketplace Picks . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 50
Dates to Remember . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 50
New CoPs: Planning Tips for Success . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 55
NewsLine is a publication of the National Hospice and Palliative Care Organization • ISSN 1081-5678 • Vol. 19, No. 3
Vice President, Communications: Jon Radulovic Communications Manager: Sue Canuteson Advertising Inquiries: Barry Black, 703/647-1577 Membership Inquiries: 800/646-6460
Copyright © 2008, NHPCO and its licensors. All rights reserved.
NewsLine4
CHAIRShareefah Sabur, MA, MNO, CDPHospice of the Western Reserve, Inc. Cleveland, OHShareefah Sabur has been at Hospice of the Western Reserve since 1993 and serves as director of
planning and evaluation . In addition to her new role as NCHPP chair, she serves on NHPCO’s Standards Committee, the board of Foundation for Hospices in Sub-Saharan Africa, and as faculty for NHPCO’s Manager Development Program . She previously served as the Performance Improvement/Quality Assurance section leader for six years .
VICE CHAIR and VOLUNTEER/VOLUNTEER MANAGEMENTKathy Roble, MSThe Hospice of the Florida SuncoastClearwater, FLKathy Roble has been director of volunteer
services for The Hospice of the Florida Suncoast since 1994 and has been a frequent presenter at local, state and national conferences on topics related to volunteer management . In addition to her service as section leader, she has now been appointed vice chair of NCHPP .
ALLIED THERAPISTValerie Hartman, RN, CHPN, CTRNHoly Redeemer Hospice • Philadelphia, PAValerie Hartman has 21 years of holistic hospice nursing experience and, for the past 10 years, has included the integration of massage and
bodywork therapy into her practice. Since 2002, she has coordinated Holy Redeemer’s complementary therapies program, overseeing and developing an innovative model of professional complementary care . Prior to her appointment as section leader, she served on the section’s steering committee for five years. She also conducts hospice massage workshops around the country .
BEREAVEMENT PROFESSIONALPatti Homan, PhD, LPC, FTHospice of Lancaster County • Lancaster, PAPatti Homan is director for the PATHways Center for Grief & Loss at Hospice of Lancaster County . For more than 20 years, she has focused her clinical
training study and practice in the areas of death and dying, crisis, trauma, and loss. In addition to her role as section leader, Patti is a fellow in thanatology with the Association of Death Education and Counseling where she serves as chair for its Body of Knowledge Committee .
CEO/EXECUTIVE DIRECTOR/PRESIDENTVacant
CNATandra Chandler, CNAII, CHPNAHospice & Palliative CareCenterWinston-Salem, NCTandra Chandler has been a certified nursing assistant for 29 years. For the past 15 years she
has worked for the Hospice and Palliative CareCenter, where she is currently a CNA team leader . In addition to several promotions and continued studies leading to her CNAII designation, Tandra has earned certifications in phlebotomy, EKG, and hospice and palliative care. Prior to accepting her new role as section leader, she served on the section’s steering committee for two years .
CLINICAL AND OPERATIONS MANAGEMENTSharon Stewart-Brown, LMSWHarry Hynes Memorial Hospice • Parsons, KSSharon Stewart-Brown joined Harry Hynes Memorial Hospice in 2004 and has served as its southeast Kansas regional director for the
past two years. Prior to joining the program, Sharon was an adjunct instructor at the University of Kansas where she taught several graduate-level courses in spirituality and cultural diversity . She also served as the director of disability determination services for the state of Kansas for five years, receiving both state and national recognition for her outstanding service and leadership .
DEVELOPMENT/PUBLIC RELATIONS/MARKETINGPam Brown, CFREAlive Hospice, Inc. • Nashville, TNPam Brown is executive vice president of community development at Alive Hospice, where she has worked for 11 years. She earned the Certified Fund
Raising Executive designation in 2002 and has been a frequent presenter at NHPCO conferences. She was selected as the 2007 Fundraising Professional of the Year by the Nashville Chapter of the Association of Fundraising Professionals .
FINANCE/INFORMATION SYSTEMSAnne Hochsprung, CPAThe Hospice of the Florida SuncoastClearwater, FLAnne Hochsprung is vice president of finance for The Hospice of the Florida Suncoast, where she
has worked since 1999. Prior to joining the hospice, she spent 20 years working in the healthcare industry. In addition to her role as section leader, Anne is part of the faculty for NHPCO’s Hospice Manager Development Program and is a member of the NHPCO Audit Committee .
National Council of Hospiceand Palliative Professionals
2008 Section LeadersIn this first quarterly issue of the year, NHPCO extends special thanks to these exemplary
members for service to their disciplines and to the end-of-life care field.

National Council of Hospice and Palliative Professionals
www.nhpco.org/nchpp
NewsLine 5NewsLine 5
NURSEPat Gibbons, BSN, CHPNBeacon Place • Greensboro, NCPat Gibbons is director of Beacon Place, the 14-bed hospice facility operated by Hospice and Palliative Care of Greensboro. Under Pat’s leadership, the facility has been a nursing student placement site for RN to BSN students and
baccalaureate nursing students. In addition to her work as section leader, Pat has served as a faculty coach in NHPCO’s Quality Improvement Collaboratives .
PERFORMANCE IMPROVEMENT/QUALITY ASSURANCESusan Zimmerman, BADelaware Hospice, Inc. • Wilmington, DESusan Zimmerman is the performance improvement coordinator at Delaware Hospice, where she has worked since 2001. She has presented both nationally
and locally on topics related to quality improvement .
PHARMACISTPhyllis Grauer, RPh, PharmDPalliative Care Consulting Group • Dublin, OHPhyllis Grauer has been a palliative care consultant pharmacist for over 20 years and is founder of the Palliative Care Consulting Group . Following PCCG’s merger with Hospiscript Services last year, Phyllis assumed the role of vice
president of clinical development . She is also an assistant clinical professor at the Ohio State University College of Pharmacy .
PHYSICIANJoan K. Harrold, MD, MPH, FAAHPMHospice of Lancaster County • Lancaster, PAJoan Harrold is medical director and vice president of medical services for Hospice of Lancaster County. In addition to serving as section leader, she is president of the Pennsylvania Hospice Network board of directors . She
also serves on the board of directors of the American Academy of Hospice and Palliative Medicine and on the Hospice and Palliative Medicine Examination Committee of the American Board of Internal Medicine .
RESEARCH/ACADEMICS/EDUCATIONJoy Berger, DMA, BCC, MT-BCHosparus • Louisville, KYJoy Berger is director for the Hosparus Education and Volunteer Center as well as an adjunct music therapy faculty member at the University of Louisville . She is board certified as both a music therapist and chaplain, and is author of
“Music of the Soul: Composing Life Out of Loss .”
SOCIAL WORKERSherri Weisenfluh, MSW, LCSWHospice of the Bluegrass • Lexington, KYSherri Weisenfluh has over 25 years of experience as a licensed clinical social worker . She currently serves as associate vice president of counseling for Hospice of the Bluegrass, a position she has held for 16 years. In addition to
her service as section leader, she teaches part-time at the University of Kentucky.
SPIRITUAL CAREGIVERCarlyle Coash, BCCKaiser Permanente • Martinez, CACarlyle Coash has been a hospice chaplain since 2000, in Boulder Colorado and now California. He is board certified with the Association of Professional Chaplains .
IMMEDIATE PAST-CHAIRBob Miller, BA, MDivVITAS Healthcare Corporation® • Miami, FL
NewsLine 6
Meeting the Needs of
Today’sPatients
Introduction:

Expanding access
has become more
than a moral
imperative. It is
a sound business
strategy that can
help ensure your
program’s long-
term viability and
growth.
NewsLine 7
“Expanding access” challenges us to care for all eligible patients—regardless of who they are, where they live, or the disease that is affecting their life . But where does one begin?
While the demographics of each community you serve can influence your access goals and priorities, this issue offers guidance for your work with non-cancer patients and families—a growing segment of our population in need of hospice and palliative care .
According to NHPCO’s most recent research, nearly 56 percent of hospice patients have non-cancer diseases.* In the dozen articles in this issue, your colleagues address some of the special skills and knowledge needed to better serve this population—from clinical guidance for patients with ALS and pulmonary fibrosis to…treating pain in nonverbal patients…educating volunteers on the mindset and needs of dementia patients…and using proactive marketing to promote access in your community .
At times, the very notion of “expanding access” can feel overwhelming because it calls us to re-examine and refine many aspects of our work, but as the authors of this issue’s opening article observe, “in the end, it’s all worth it.” Today, expanding access has become more than a moral imperative . It is a sound business strategy that can help ensure your program’s long-term viability and growth. So, as you read the articles in this issue, consider how the information imparted can help inform your work. As the scientist and inventor, Charles Kettering, once said, “If you’ve always done it that way, it’s probably wrong.”
*NHPCO Facts and Figures: Hospice Care in America, 11/07 edition.
In addition to the insights your colleagues share in this issue, take advantage of the other resources available to you as an NHPCO member. See page 49 for a closer look at NHPCO’s Access and Inclusion Toolbox and visit nhpco.org/access for a wealth of other materials. Finally, consider attending NHPCO’s 2nd National Conference on Access, being held in Minneapolis this coming August (nhpco.org/conferences) .
NewsLine8
Most of us are aware of the history of hospice in the United States . As we know, in the late 1970s, the
industry’s early “pioneers” weren’t satisfied with the way people were being cared for at the end of life and, through their foresight and dedication, challenged the status quo—and largely changed the healthcare system as we knew it .
During the late 1980s and early 90s, hospice leaders also realized that, despite the tremendous number of cancer patients being served, many other people were dying without the benefit of hospice care. Over the years, this too has changed. According to NHPCO, in 2006, people dying from non-cancer diseases comprised more than 55.9 percent1 of hospice patients in this country .
For those newer to hospice this may seem like business as usual, but for those organizations as well as the hospice staff and volunteers who have worked in the field for the past 10 to 15 years, there have been tremendous changes. To name just a few, we have seen changes in clinical care competencies, changes in acuity of patients, changes in psychosocial and spiritual issues affecting patients and families, and changes in documentation related to eligibility . Even though hospice is still a relative newcomer to the healthcare field, we have seen incredible changes over the span of our existence .
As we anticipate the release of the Medicare Conditions of Participation for Hospice Care in May 2008 (“hospice CoPs”)—yet another significant change in our industry—it seems appropriate that we examine what we have already learned from caring for our diverse patient mix and what more we can do to provide better care to more people in need .
Not Everyone Dies on TimeThose of us working in hospice are familiar
with the description of “terminally ill” as defined by the hospice
CoPs—“the individual has a prognosis of six months or less if the disease runs its normal course .”2 The entire structure of the benefit was predicated on people dying in that time frame .
The original regulations allowed for hospice care to be provided for two 90-day periods and one 30-day period, for a total of 210
days of Medicare hospice coverage. As early as 1989,
the government recognized the challenge of relying on
prognostication to determine eligibility which led to the first of
several important changes to the benefit structure. “Because of the scientific difficulty in making a prognosis of six months or less, the 210-day limit was repealed by the Medicare Catastrophic Coverage Repeal Act of 1989.”3 As a result, the benefit periods were restructured into two 90-day periods, one 30-day period, and a fourth unlimited period .
While this was a monumental change, it did not address all the issues related to the challenge of prognostication. For example, if a patient either decided to leave hospice by revoking his/her benefit or was discharged during the fourth benefit period, that patient could never again be admitted to hospice under Medicare. Fortunately, the Balanced Budget Act of 1997 changed this; it provided two 90-day periods, followed by an unlimited number of 60-day periods, and allowed people to be discharged from or revoke their hospice benefit and still be re-admitted.
These simple changes to what now seems like an illogical provision of the original Medicare Hospice Benefit (MHB) was a tremendous relief to hospice providers .
Using What We’ve Learned to Expand Access
By Kathy Brandt, MS, and John Mastrojohn III, MSN, MBA

NewsLine 9
Yet even with these important changes, the MHB six-month prognosis requirement—which works quite well for most people with cancer—puts a tremendous burden on hospices when serving non-cancer patients . Dr Joanne Lynn’s research regarding the trajectory of patients living with end-stage disease shined light on the need for even more flexibility in the MHB when meeting the needs of people with non-cancer diagnoses . The graphs at right clearly illustrate what hospice providers have always known— not all patients die in a predictable manner or “on time .”
In 1995, NHPCO (then the National Hospice Organization) published the first edition of the Medical Guidelines for Determining Prognosis in Selected Non-Cancer Diseases . These guidelines offered hospice providers a resource to help determine and document eligibility for the MHB for those with non-cancer diagnoses . While these criteria are far from perfect, they still serve as a model for most of the hospice Local Coverage Determinations (LCDs), developed by the RHHI fiscal intermediaries. Readers should be cautioned however, that the Centers for Medicare & Medicaid Services (CMS) clearly describe the limitation of the LCDs in establishing prognosis:
“These criteria form a reasonable approach to the determination of life expectancy based on available research….Coverage of hospice care for patients not meeting the criteria in this policy may be denied. However, some patients may not meet the criteria, yet still be appropriate for hospice care, because of other comorbidities or rapid decline . Coverage for these patients may be approved on an individual consideration basis .” 4
With more than 50 percent of all hospice patients dying from non-cancer diseases and no reliable way to predict prognosis, hospices are performing a delicate balancing act . The most recent data reveals the median length of stay in hospice declined in 2006 to 20.6 days—or less than three weeks of hospice care .1 In light of Operation Restore Trust, focused medical review, probe edits, targeted medical review and recent comments from government officials that long lengths of stay in hospice are troubling, many hospices may be reluctant to admit people with non-cancer diagnoses until they are able to indisputably document terminality .
continued on next page
Short period of evident decline
Prolonged dwindling
Long term limitations with intermittent serious episodes
Fun
ctio
nFu
nct
ion
Fun
ctio
n
High
Low
High
Low
High
Low
Death
Specialist palliativecare input available
Time
Time
Time
Death
Death
Onset of incurable cancer
Mostly cancer
Mostly heart and lung failure
Mostly frailty and dementia
Often a few years, but declineusually over a few months
Sometimes emergencyhospital admissions
Onset could be deficits in functionalcapacity, speech, cognition
Quite variable –up to 6-8 years
2-5 years, but deathusually seems “sudden”
The Typical Illness Trajectories for People With Progressive Chronic Illness*

Not All Patients and Families “Look the Same”What we have learned from all those we’ve cared for is that each patient and family is very different . These differences can be related to diagnoses, physical symptoms, emotional needs, spiritual preferences, and cultural beliefs and practices, along with many other factors.
Over the past 25 years of the MHB, we have cared for increasing numbers of patients with ALS, end-stage Alzheimer’s and dementia, and end-stage cardiac, pulmonary, and renal diseases . Moreover, we have seen the ravages of the AIDS epidemic when we cared for patients who were diagnosed only a short time before their death, and conversely, we experienced the joy of discharging AIDS patients due to their positive response to the then-newly released protease inhibitors .
Caring for this diverse patient mix has challenged us to expand our clinical expertise to learn about new and different medicines, treatments, and therapies. Patients come to us receiving treatments that were formerly considered solely curative in nature, but are now considered proper and acceptable to palliate symptoms . Many hospice patients require more complex care management and many have lived with chronic illness for years, sometimes even decades . All of these patients have taught us new ways to manage symptoms and alleviate suffering .
As we have already mentioned, certifying patients for the MHB has become more challenging, yet never has it been more important. Increasingly, hospices are relying on pulmonologists, immunologists, cardiologists, geriatricians and neurologists in addition to the oncologists and primary care physicians previously found on staff to ensure they have the expertise needed to document eligibility and meet the complex care needs of patients . Some programs are forming innovative partnerships with local specialists to serve as advisors and teach clinical staff the complexities of caring for non-cancer patients .
Yesterday’s Hospice Isn’t Meeting the Needs of Today’s PatientsHealthcare is rapidly evolving to try and meet the complex care needs of patients living with chronic conditions, yet the basic model of hospice has not changed much over the past 25 years. Some hospices are still reluctant to remove artificial barriers to admission—barriers that make some patients and their healthcare
providers feel like they have to “jump through hoops” to gain admission .
On the upside, however, are the hospice innovators who
began providing access for all eligible patients in the past several years. But, how does that work?
Eligibility is based on the existing regulations under the MHB . It should be an organizational philosophy that can help a program enhance access for all eligible patients—that
is, those who meet the regulatory requirements—by
removing self-imposed barriers to admission .
For example, programs committed to providing access for all eligible patients
would only admit patients who meet the MHB definition of “terminally ill” (i.e., those with a six-month or less prognosis). However, they would also admit people who:
do not have a primary caregiver living in their • home;
are not ready or willing to sign an advance • directive;
may be receiving palliative radiation or • chemotherapy; and/or
are receiving treatments to aggressively treat • symptoms that, 10 years ago, would not have been defined as palliative but are considered palliative today .
Providing access to all eligible patients also means being staffed to perform after-hours and weekend admissions and extended office hours to meet the needs of referral sources, patients and family caregivers .
It is also important to note, however, that there is increased scrutiny of any programs with lengths
NewsLine 10
continued from previous page

Some hospices are
still reluctant to
remove artificial
barriers to
admission—barriers
that make some
patients and
their healthcare
providers feel like
they have to “jump
through hoops” to
gain admission.
NewsLine 11
of stay that exceed the national average. Thus, hospices which embrace the concept of access for all eligible patients must vigorously ensure that patient documentation includes sound, consistent, clinically-based evidence of continuing eligibility .
In the End, All the Work is Worth ItHospice team members can provide countless examples of times when patients and families struggled through the challenging work needed to repair relationships with friends, family, God, or themselves as a means to find peace. The same holds true for hospice programs. While it is clearly a challenge to do the work that is necessary—to increase clinical competency, to revise admission criteria, to serve patients with complex care needs, and to continue to re-certify patients who meet the clinical criteria for admission—in the end, all the hard work is worth it. It is worth it because we know that hospice is the best model of care for people living with a life-limiting illness .
So, while we have experienced great change and many challenges since the inception of hospice in America, we can be proud as we reflect on the care and comfort we have provided to patients and families. And, as we forge ahead, we should anticipate the many changes to come with enthusiasm—knowing that as we improve the care of those we serve, we will one day look back on our work and conclude that, yes, it’s all been worth it .
Kathy Brandt is NHPCO’s vice president of professional leadership, consumer and caregiver services. She has more than 18 years of experience in the hospice field, including seven years at The Hospice of the Florida Suncoast in Clearwater, Florida where she focused on community engagement and education.
John Mastrojohn is NHPCO’s vice president of quality and palliative care. John has worked in various leadership roles within the healthcare field for 26 years, most recently as founding director of the Department of Palliative Care and Hospice Service, a hospital-based program at Summa Health System in Akron. Ohio.
References:1 NHPCO Facts and Figures: Hospice Care in America, November 2007
Edition. Retrieved January 26, 2008 from www.nhpco.org/research.2 [48 FR 56026, Dec. 16, 1983, as amended at 52 FR 4499, Feb. 12,
1987; 50 FR 50834, Dec. 11, 1990]. Retrieved January 26, 2008 from http://a257.g.akamaitech.net/7/257/2422/12feb20041500/edocket.access.gpo.gov/cfr_2004/octqtr/pdf/42cfr418.3.pdf .
3 Federal Register/Vol. 70, No. 224/Tuesday, November 22, 2005 / Rules and Regulations. Retrieved January 28, 2008 from www.cms.hhs.gov/quarterlyproviderupdates/downloads/CMS1022F.PDF .
4 LCD for Hospice - Pulmonary Disease (L314). Retrieved January 26, 2008 from www.cms.hhs.gov/mcd/viewlcd.asp?lcd_id=314&lcd_version=19&show=all .
5 Retrieved January 27, 2008 from http://www.hospicenyc.org/access.html .
NewsLine 12
In 1998, I wrote an article for NHPCO’s membership magazine on “Caring for Non-Cancer Patients.” Now, 10 years later, it
is both interesting and rewarding to revisit this topic—and think about what has been accomplished over this past decade .
Certainly we have a new vocabulary within hospice. The word “palliative,” for example, is more frequently used when referring to hospice . Many organizations, including NHPCO, have included palliative in their name . Many hospice providers are developing palliative care programs and many hospital systems are partnering with hospices to offer such services . End-of-life care is now viewed as part of the continuum of care . Those of us who are hospice professionals have also added the word “palliative” to our name and credentials. Our publications, as well, reflect this new vocabulary .
When I wrote that article in 1998, NHPCO had recently published its Medical Guidelines for Determining Prognosis in Selected Non-Cancer Diseases . Those guidelines presented programs with an opportunity to expand access to more people with a range of life-limiting illnesses . At that time, over 60 percent of all hospice care was provided to patients with a cancer diagnosis (NHO, 1996). According to NHPCO’s figures for 2006, non-cancer diagnoses now represent just 44.1 percent of the patients we serve, with 55.9 percent representing non-cancer diseases (NHPCO’s Facts and Figures, 2007). Overall, access to hospice care has increased .
Phrases such as “open access” and “just say yes” have challenged us to think outside the box . Programs are developing ways to provide quality end-of-life care to more eligible patients with life-limiting illnesses—regardless of their specific disease . Newer treatments and technologies have also pushed us to think critically and integrate palliative care into hospice care and hospice care into palliative care . Collaboration is now the norm in most areas. However, it’s important to remember that palliative care and hospice care are not synonymous, but are both part of a continuum of care—with palliative care oftentimes leading to hospice care .
We have seen many times when palliative interventions have been used in hospice and, conversely, we have seen many hospice concepts used in palliative care . A prime example of this is in our work with HIV patients. Today, many people with HIV are living much longer with new targeted therapies, but at the same time, they are living long enough to develop some of the more chronic conditions like COPD, cardiac and renal diseases, and even cancers. Establishment of goals of care in such situations can only be accomplished through conversations with skilled clinicians who understand the concepts of both hospice and palliative care . Because hospice has been helping to ensure access since the early days of the HIV epidemic, we are a respected resource to help now . Hospice programs are establishing relationships with cardiology, renal, and pulmonary specialists to enhance access for the many eligible patients who can benefit from it.
Now, more than ever, access is not just about diseases. We, in hospice, are serving those at end of life in whatever location they may be . We have worked very diligently to be a presence in long-term care environments, in assisted living facilities, in hospitals, in homeless shelters—and even under a bridge if need be . Programs have continued to be creative in programming in order to reach some of our most vulnerable populations . Many prison programs are being recognized as models for both volunteerism and care . The Partnership Initiative of the Foundation for Hospices in Sub-Saharan Africa continues to grow in ways that enrich programs in Africa, but also those here in the states which participate (fhssa .org > Programs) . There are other models similar in Eastern Europe. Partnering for Children, a collaborative effort between NHPCO, the Children’s Hospice and Palliative Care Coalition, and the National Hospice Foundation, is yet another example of how we are increasing awareness among underserved populations—in this case, children with life-threatening conditions.
In the past, such documents as the AIDS Resource Manual and Access to Hospice Care, and Expanding Boundaries, Overcoming Barriers were very helpful . Newer publications such as the Inclusion and Access Toolbox (see page 49)
The Changing Face of AccessBy Pat Gibbons, BSN, CHPN
NewsLine 13
give programs the tools and resources necessary to create an inclusive organization capable of meeting the needs of their own communities.
Today, we are clearly—and fortunately—expanding to embrace a concept of care that meets diverse end-of-life care needs . The language may have changed, the resources may be greater, the populations may be more diverse, but our vision is still the same: “A world where individuals and families facing serious illness and grief will experience the best that humankind can offer .”
It is unclear what the next 10 years will bring. There may be changes in reimbursement, changes in the Medicare Hospice Benefit, and, possibly, decreasing lengths of stay in hospice and increased access to palliative care. Whatever may happen, hospice and palliative care is here to stay as a recognized—and critical—component of the healthcare continuum. We can be very proud of how far we have come and we can look forward to continued service to those in need whomever they are and wherever they call ‘home’ .
Pat Gibbons is director of Beacon Place, the 14-bed hospice facility operated by Hospice and Palliative Care of Greensboro in North Carolina. She currently serves as NCHPP’s Nurse Section Leader.
Because hospices
have been helping
to ensure access
since the early
days of the HIV
epidemic, we are a
respected resource
to help now.
NewsLine 14
Amyotrophic Lateral Sclerosis is a progressive, incurable neurological disease that affects the nerve cells responsible for
controlling voluntary muscles . The nerve cells that become affected take away the muscles’ ability to function and, as a result, the muscles gradually weaken, waste away, and twitch (i.e., “fasciculate”) .
Although people diagnosed with ALS will eventually not be able to move without assistance, they will still be able to control their eye muscles and rectal/urinary sphincters. An article in March 2006 also showed evidence that almost a third of the people diagnosed with ALS may demonstrate some cognitive impairment or dementia, even though the disease does not usually affect a person’s thinking or cognitive abilities .6
The Prognosis for ALS PatientsIndividuals with ALS will experience progressive weakness with moving, swallowing, speaking and breathing . They will also experience the eventual wasting away and paralysis of the muscles of the limbs and trunk, and those that control speech, swallowing and breathing .
As the disease advances, choking spells become common when the
person attempts to eat or drink, due to jaw weakness and fatigue . These episodes can be very frightening for the patient and caregivers . Nutritional support can be
provided via a feeding tube and this can provide another route for medication administration . Recommendations for placement of a feeding tube are made soon after the onset of dysphagia (i.e., difficulty swallowing) and the decision about whether or not to insert the feeding tube is based on prolongation and quality of life .7
When muscles in the diaphragm and chest wall fail, individuals lose the ability to breathe without the support of mechanical ventilation . Even though a respirator can ease problems with breathing and prolong survival, it does not affect the progression of the disease . Most people with ALS die of respiratory failure or pneumonia, not the disease itself.8
Palliative Care RecommendationsPharmacological and non-pharmacological interventions should focus on symptomatic relief, prevention of complications, maintenance of maximum function and optimal quality of life .
Pharmacological treatment includes Riluzole (Rilutek©), which is the only FDA-approved medication for the treatment of ALS. Riluzole may prolong the patient’s life by a few months by slowing down the disease’s progression .8
Sialorrhea, an excessive secretion of saliva, is a prominent symptom in people with ALS . Pharmacological interventions include Robinul (Glycopyrrolate), Cogentin, Scopolamine patch, Atropine or Elavil (Amitriptyline) .4
Pseudobulbular effect or “pathological laughing or crying” may also be seen in up to 50 percent of ALS patients . Pharmacological treatment for this symptom includes Elavil (amitriptyline) or Fluvoxamine (Luvox) .4
Pain may be present from stiff joints, muscle cramps, or a preexisting
condition . I recommend that you refer to your pain
assessment, and guidelines for pain management and bowel regimen to determine the appropriate
treatments .
ALS Patient CareBy Beth Whidden, ARNP, BSN, MS

NewsLine 15
Substantial physical caregiving is also required for the person diagnosed with ALS . Common equipment needs may include an electronic wheelchair, letter and picture board for communication, BiPap machine, and feeding tube equipment .
The options for respiratory support should be discussed before the development of respiratory muscle weakness . Involvement of respiratory muscles and the risk of an upper respiratory infection can lead to sudden decline and death . Signs and symptoms of respiratory muscle weakness include shortness of breath (SOB) with exertion, dizziness, inability to lie flat without SOB, anxiety, morning headaches, weight loss (which may be due to decreased intake) and extreme fatigue .1
Discussions concerning the choice of mechanical ventilation should take place between the patient, caregivers and healthcare professionals before a crisis situation occurs .4 If the patient has completed an advance directive, such information can also help guide healthcare providers and caregivers regarding the patient’s wishes .
Aggressive psychological and spiritual support for patients and families is also critical, especially since these patients often experience fear, anxiety and depression . Support groups—including online chat groups—are an excellent resource in particular . To assist patients and caregivers in finding a support group, visit the Web sites of the Muscular Dystrophy Association (als-mda .org) and the ALS Association (alsa .org) . NHPCO’s consumer engagement initiative, Caring Connections, also provides general resources that may be helpful (caringinfo .org) .
Hospice and the ALS PatientALS patients, like so many other patients at the end of life, can benefit from the holistic care that hospice provides. For example, one study reviewed the medical records of ALS patients and found that 94 percent were “peaceful and settled” at the time of their death while in the care of hospice .5
According to the ALS Association, the majority of people diagnosed with the disease die from respiratory failure, usually within three to five years from the onset of symptoms. Approximately 20 percent will live five years or more, up to 10 percent will survive more than 10 years, and five percent will live 20 years from the time of diagnosis.8 Hospice care is an important part of the care a person with ALS receives—but when is the right time for hospice?
NHPCO collaborated with researchers at the University of Pennsylvania to determine what clinical findings could serve as indicators as to when ALS patients have six months or less to live and, therefore, could be referred to hospice .3 The proposed eligibility criteria were released in 2006 in the NHPCO disease-specific report, Expanding Access to Hospice Care for People with ALS (see page 17). These criteria, along with documented clinical judgment, can guide the hospice team to earlier and appropriate hospice admissions of ALS patients .
One study
reviewed the charts
of ALS patients
and found that
94 percent were
“peaceful and
settled” at the
time of death
while in the care
of hospice.5
continued on next page
NewsLine 16
The criteria review nutritional status and respiratory function for a prognosis of limited life expectancy. Nutritional status is defined if dysphagia is present with a weight loss of five percent of body weight with or without a feeding in place .2
Critical impaired respiratory status can be measured with a Forced Vital Capacity of less than 40 percent, and two of the following signs and symptoms: Dyspnea at rest; orthopnea; the use of accessory muscles to breath; paradoxical abdominal motion; respirations greater than 20; reduced speech/volume; weak cough; symptoms of sleep disorder breathing; and/or unexplained headaches, confusion, anxiety or nausea. If the patient cannot perform the Forced Vital Capacity test, documentation should reflect that at least three of the above-mentioned signs and symptoms are present .2
Through the use of NHPCO’s proposed eligibility requirements, clinicians can better determine the right time for hospice . By choosing the proper time to involve hospice, facilities and providers alike will be better able to serve the needs of both early and late stage ALS patients .
continued from previous page
Beth Whidden has been in the nursing profession for 17 years, and has practiced in the fields of oncology, and hospice and palliative care. Since 1996, she has focused her work on education and training and is currently a professional development coordinator for the Advancement of Nursing at The Hospice of the Florida Suncoast in Clearwater, FL.
Since ALS is a progressive and fatal disease, hospice is uniquely qualified to handle the increasingly intensive care the ALS patient requires . As hospice treats the increased physical needs, it is also well-versed in managing the patient’s suffering as well as lending care and support to caregivers and families . With a compassionate partnership between the patient, caregivers and clinicians, hospice can ensure the most positive experience possible for ALS patients at the end of life .
References:1 Gilani A, Hinn A & Jacobson PL. Management of
respiratory failure in ALS . EPERC, 2004.2 Expanding access to Hospice Care for People
with ALS . National Hospice and Palliative Care Organization. 2006.
3 McClusky L, Houseman G, Medicare hospice referral criteria for patients with Amyotrophic Lateral Sclerosis: A need for improvement . Journal of Palliative Medicine. 7(1):47-54, 2004.
4 Miller RG et al . Practice Parameter: The care of the patient with ALS (an evidence-based review) . American Academy of Neurology . 52:1311-1323, 1999.
5 O’Brien T, Kelly M, Sunders C. Motor neuron disease: a hospice perspective . BMJ; 304:471–473,1992.
6 Rippon G et al . An observational study of cognitive impairment in ALS . Archives of Neurology; 63:345-352, 2006.
7 Slowie LA, Paige MS, Antel JP. Nutritional considerations in the management of patients with amyotrophic lateral sclerosis . J Am Diet Assoc. Jul; 83(1):44-7, 1983.
8 What is ALS: The ALS Association (www .alsa .org) .
9 Muscular Dystrophy Association’s ALS Dvision (www .als-mda .org) .

NewsLine 17
A Guide to ALS Prognostication and Clinical Management
The NHPCO monograph, Expanding Access to Hospice Care for People With ALS, was produced in 2006 to help inform hospices and other health professionals about advances in prognostication and clinical management of the disease .
The report provides prognostic criteria for ALS eligibility, along with stories of hospices that have successfully met the challenges of providing care to these patients through collaborations with ALS groups and professionals in their communities .
To order your copy, visit nhpco.org/marketplace (Item 821011; Member: $14.99). For more resources and helpful links, visit nhpco.org/access > ALS .
Through the
use of NHPCO’s
proposed eligibility
requirements,
clinicians can better
determine the right
time for hospice.
NewsLine 18
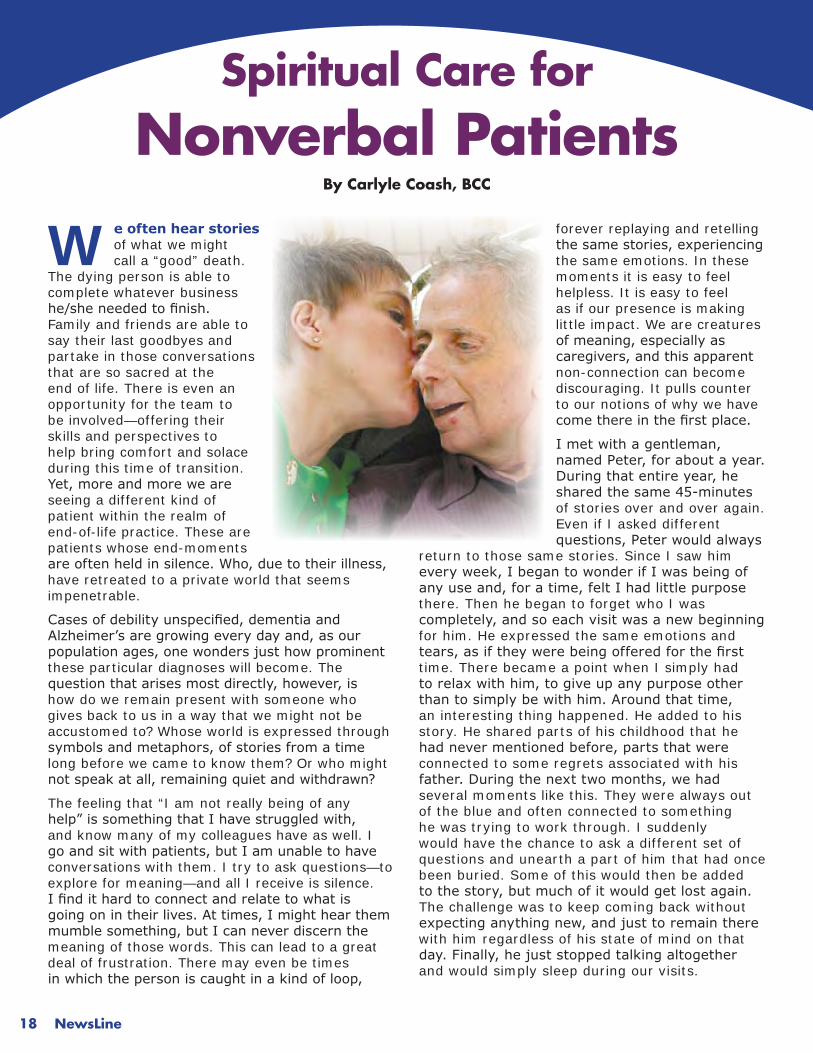
We often hear stories of what we might call a “good” death .
The dying person is able to complete whatever business he/she needed to finish. Family and friends are able to say their last goodbyes and partake in those conversations that are so sacred at the end of life . There is even an opportunity for the team to be involved—offering their skills and perspectives to help bring comfort and solace during this time of transition . Yet, more and more we are seeing a different kind of patient within the realm of end-of-life practice . These are patients whose end-moments are often held in silence. Who, due to their illness, have retreated to a private world that seems impenetrable .
Cases of debility unspecified, dementia and Alzheimer’s are growing every day and, as our population ages, one wonders just how prominent these particular diagnoses will become . The question that arises most directly, however, is how do we remain present with someone who gives back to us in a way that we might not be accustomed to? Whose world is expressed through symbols and metaphors, of stories from a time long before we came to know them? Or who might not speak at all, remaining quiet and withdrawn?
The feeling that “I am not really being of any help” is something that I have struggled with, and know many of my colleagues have as well . I go and sit with patients, but I am unable to have conversations with them . I try to ask questions—to explore for meaning—and all I receive is silence . I find it hard to connect and relate to what is going on in their lives. At times, I might hear them mumble something, but I can never discern the meaning of those words . This can lead to a great deal of frustration . There may even be times in which the person is caught in a kind of loop,
forever replaying and retelling the same stories, experiencing the same emotions . In these moments it is easy to feel helpless . It is easy to feel as if our presence is making little impact . We are creatures of meaning, especially as caregivers, and this apparent non-connection can become discouraging . It pulls counter to our notions of why we have come there in the first place.
I met with a gentleman, named Peter, for about a year. During that entire year, he shared the same 45-minutes of stories over and over again . Even if I asked different questions, Peter would always
return to those same stories . Since I saw him every week, I began to wonder if I was being of any use and, for a time, felt I had little purpose there . Then he began to forget who I was completely, and so each visit was a new beginning for him . He expressed the same emotions and tears, as if they were being offered for the first time . There became a point when I simply had to relax with him, to give up any purpose other than to simply be with him. Around that time, an interesting thing happened . He added to his story . He shared parts of his childhood that he had never mentioned before, parts that were connected to some regrets associated with his father. During the next two months, we had several moments like this . They were always out of the blue and often connected to something he was trying to work through . I suddenly would have the chance to ask a different set of questions and unearth a part of him that had once been buried . Some of this would then be added to the story, but much of it would get lost again. The challenge was to keep coming back without expecting anything new, and just to remain there with him regardless of his state of mind on that day. Finally, he just stopped talking altogether and would simply sleep during our visits .
Spiritual Care for Nonverbal Patients
By Carlyle Coash, BCC

NewsLine 19
Islands of ClarityIn 1990, the noted doctor and teacher, Edward Podvoll, proposed a unique approach to supporting illness in his book Recovering Sanity . The basic notion was to connect to the sanity of a patient, rather than the illness. In this case, it meant creating an environment in which the patient would be cared for by a team of people who would focus on supporting the wholeness of the patient. In addition, the team would support each other, so that the entire community was involved. By doing this, it was not uncommon for there to be moments in which the people, despite their cognitive issues, were able to experience what Podvoll termed “islands of clarity” or a “coming to the senses” in which there manifests a balance between mind and body . This occurred because the patients were surrounded by people who were bearing witness to their wholeness, not their limitations . They were able to discover healing and would often be able to shift out of their states of confusion .
This notion of “islands of clarity” has always struck me as being an essential element to what we do as caregivers . By being deeply grounded and present with those we support, we allow them the chance to settle. If our only outcome is to see the whole person, then we allow that person the chance to shine through . Meaning-making takes on a whole new purpose as well. It becomes a purpose based in stillness, without agenda or disappointment that a meaningful connection has not been made . For what is a meaningful connection? What do we need from our work as caregivers to make it meaningful? Is a patient any less a person because he/she cannot express or otherwise share with us some “meaningful” experiences? Or is his/her confusion unsettling to us? Does it reflect our own fears about facing such an illness—and state of mind?
The hardest part of my time with Peter was the realization that I could be in the very same situation as he was at some point in my life . I not only felt powerless in my conversations with him, but also felt that powerlessness was a constant reminder of the fear I had for myself . I feel that for us to be of service in a deeper way, it is important for us to reflect on these kinds of situations and how they affect us. It is important to be curious about why a certain patient or family member activates an emotion within us, especially if it is a feeling of helplessness or unease.
We should also remember that our mere arrival at a patient’s door is an important act in and of itself . An immediate and inherent connection is made though our willingness to “be there .” This alone can help appease our “need for more” and, at the same time, relieves the patient of a tremendous burden. From there, anything is truly possible.
Carlyle Coash has been a hospice chaplain since 2000, in Boulder Colorado and now California. He is board certified with the Association of Professional Chaplains and currently serves as NCHPP’s Spiritual Caregiving Section Leader.
What do we need
from our work as
caregivers to make
it meaningful?
Is a patient any
less a person
because he/she
cannot express or
otherwise share
with us some
“meaningful”
experiences?
NewsLine 20
For many volunteers, the opportunity to visit with patients and families is the main motivation behind their desire to give of their
time . We read frequently on their applications that they want to “help people on their journey” or “bring a little joy to someone” or “give the family support .” But what happens when the patient doesn’t respond to the visit and, most likely, never will? Or the person is pleasant enough, but may never remember the volunteer was there?
About two years ago, we realized that there was an unusual turnover of volunteers in one particular Extended Care Facility (ECF) . We certainly allow our volunteers to change roles as they feel the need, but the burn-out rate had gone from years to six months or less . After meeting with all the ECF volunteers, we realized that the patients in this particular location had an additional diagnosis of dementia and that the volunteers felt their visits were frustrating and meaningless . Even though we were instructing them in the basics of visiting with dementia and Alzheimer’s patients, they felt they were sometimes making the patients feel unsettled by their presence .
Lessons from Aunt LynnWe recognized an excellent educational opportunity in this situation—and called in an expert to assist us. Over the course of five months, we offered eight in-service sessions with Lynn Ritter, PhD., the education coordinator for the Northwest Ohio Chapter of the Alzheimer’s Association .
Dr. Ritter, who is a dynamo of a presenter, explained all of the medical aspects of the disease—but then assumed the persona of “Aunt Lynn,” an 86-year-old with dementia, to help us understand what it’s truly like to have the disease and how we could make a difference . Here are some of the things “Aunt Lynn” shared with us:
In the early stages of the illness, I know there • is something wrong, but I am unable to identify the cause and feel helpless to fix it. As a result, I can become frustrated, angry and confused.
Please don’t bring your purse, coat or anything • else that you are not willing to leave with me . My reasoning and judgment are changing and I think those items may be mine . I may also think that when you prepare to leave that I should be going with you and will become upset and confused when you won’t take me with you .
During the visit, try not to ask me too many • questions . I may not be able to accurately remember the answer and may become frustrated at realizing I should know the
answer, but I don’t. It also may be that I know the answer, but you can’t understand the words I’m using and they confuse you—not me .
Always treat me as the adult that I • am when choosing your words and tone of voice . Please never argue with me if I think you are someone you are not . Correcting me is rude and it makes me think that you don’t know who you are . It’s okay to be my sister or brother, or other familiar person on any given day .
Do have conversations with me, • even if I don’t talk, because I may recognize your voice from previous visits. Tell me your name again, tell me you are glad to be with me, tell me the weather, and tell me about the seasons
as they change. Talk to me about my family, bring me examples of my hobbies, show me the photo album again, and play my favorite music for me . You may have done these things dozens of times before, but to me it’s familiar and comforting, whether I can express that to you or not .
If I become unsettled while you are with me, it • may be that I need to use the rest room, may be having pain, may be hungry, may be feeling too hot or too cold, or experiencing something only known to me . There is usually a reason for my expression of emotion .
If I should fall asleep, sit quietly and do not be • offended; the gift of sleep is a sign that I am relaxed in your company .
Understanding the Mindset of
Dementia PatientsBy Deborah A. Braun, CVA
Visit the Web site of the
Alzheimer’s Association,
to learn about programs
and services available in your area, including
educational workshops:
alz.org > In Your
Community.

NewsLine 21
When it’s time to leave me, please go quickly and without much ado. • Say ‘please excuse me’ or ‘I’ve enjoyed our time today’ and then make your way to the door quietly . Trying to explain to me that you will be back again in two days or next Thursday only makes me anxious about when that is and what will happen to me in the meantime . If you put on your coat, go for the keys, and say a hearty “goodbye,” I will definitely and naturally want to go with you! Then, your departure will cause me much unhappiness, confusion and distress.
Aunt Lynn also reassured volunteers that they do make a positive difference with each visit by simply offering acceptance to patients, just as they are. She says what they are thinking, but perhaps not communicating, is “Thank you for coming, thank you for caring, and please come back .”
Stimulating Positive Responses in PatientsFinding out as much as you can about the life story of the patient from the staff and family will help you direct topics of interest and familiarity . Likes and dislikes, hobbies, work experiences, music preferences, and family history are very important to “framing” a quality visit. Likewise, creating a “goodie bag” with inexpensive items to help stimulate memories, feelings and comfort can help you connect with patients.
For example, volunteer Tim Galvin was assigned to a gentleman in an inner city ECF who was uncommunicative and angry . Tim did his homework and found out that at one time, years before, the patient liked to play cards. Tim had a deck of cards in his goodie bag, but the patient did not seem interested. On his next visit, Tim brought an UNO deck which sparked the patient’s interest . They ended up playing cards for hours. Afterwards, the ECF staff remarked on how the patient’s anger seemed to diminish, he cooperated more easily, and his appetite improved .
As another example, volunteer Fred Dannhauser and his therapy dog, Tango, were visiting with a hospice patient at a local ECF. While Tango was, of course, the center of attention during the visits, Fred played a big part in involving the other seven patients in on the fun . After the hospice patient died, the ECF staff asked Fred and Tango to continue their visits because the residents were always more calm afterwards and slept much better .
Positive Effects on Volunteer TurnoverOur volunteer turnover in ECFs has improved since we conducted the training with Dr . Ritter . The ECF staffs welcome the volunteer visits and team leader, Cathy Richards, RN, CHPCN, tells us that patients’ families are comforted in knowing that, with additional visits from volunteers, their loved ones not only benefit from companionship, but also in having another advocate for excellent care .
Deborah Braun has 15 years of volunteer administration experience and is certified with the Council for Certification in Volunteer Administration. She has served as director of volunteer services for Hospice of Northwest Ohio (Perrysburg, Ohio) since 2001, where she oversees the work of 425 volunteers.
Dr. Ritter…
assumed
the persona of
“Aunt Lynn,” an
86-year-old with
dementia, to help
us understand
what it’s truly
like to have the
disease.
NewsLine22
Our journey toward improving the management of pain in nonverbal patients started with the uncomfortable realization
that we were not always performing at the level we wanted to as a quality hospice organization. Overall, we felt like our patients were well-managed and cared for. But, like so many other organizations getting ready for the new Conditions of Participation—particularly the QAPI (Quality Assessment Performance Improvement) CoP— we needed to take a hard look at “how we were planning to measure and demonstrate successful pain management in nonverbal patients .”
Discovering even an occasional clinical record without a measurement of pain severity upon initial assessment or subsequent reassessments was unacceptable to us . When several chart audits revealed “no complaints of pain” documented in patients who were non verbal, we identified a very real opportunity for improvement .
We felt our clinicians understood the nonverbal behaviors indicative of pain in older persons (American Geriatrics Society, 2002), but how could we be certain? Also, dismissing pain behaviors as “just part of dementia” is an ever-present risk, especially among nurses new to hospice care . So, our goal was to ensure that we were indeed addressing the pain levels of those patients most
vulnerable to unrecognized pain: Those who were cognitively impaired or otherwise unable to reliably respond to questions about their pain .
As part of a renewed organizational emphasis on improved performance and clinical documentation, we joined “Wave 3” of NHPCO’s Quality Improvement Collaboratives .
These collaboratives use the “Model for Improvement” developed by the Institute for Health Care Improvement (aka “IHI Model”) to help teams accomplish their goals . Following a process of “plan, do, study, act,” the model lets you plan small changes, test the changes, evaluate the effects, and then act on the results. This approach is effective because it does not overwhelm an organization, and can result in achievable goals within a short time that can then be expanded within the organization in a planned and organized fashion .
We specifically set out to involve staff members from all parts of our organization in this project—not just clinicians—because we wanted all staff to learn the IHI model. Through direct involvement, they would be better able to integrate it into our new QAPI program description . Here is a step-by-step description of the process we followed during the nine-month collaborative .
Treating Pain inNonverbal Patients
By Ronalda Dick, RN, MSN
NHPCO’s Quality Improvement Collaboratives were launched in September 2006 as part of the Quality Partners program . They are a series of six-to-nine month programs (or “waves”) which offer participating hospice teams the training, resources, and support to make improvements within their organizations.
Each team identifies: (1) precisely what they want to improve, (2) by how much, (3) the changes they will make to realize their goal, and (4) how they plan to measure and/or determine if the change resulted in an improvement. Then, over the course of nine months, they work together to make measurable improvements toward their goal—with guidance from interdisciplinary team members who serve as coaches .
In this article, Ronalda Dick, director of quality and clinical information at Hospice of Central Iowa, shares with us her team’s work on one of NHPCO’s collaboratives.
NewsLine 23
Step 1:Our first step was to identify what changes we should make that would likely result in improvement .
In researching the literature on pain assessment, it became clear that few tools have been thoroughly evaluated with respect to validity, reliability or usefulness . Much study is still needed to determine which pain assessment tools work best for different hospice patient populations .
We found that other hospice agencies and some of our long-term care facility partners had begun using the Pain Assessment in Advanced Dementia (PAINAD) scale (Warden, Hurley & Volicer, 2003). Their use of the scale and its endorsement by the American Medical Directors Association led us to consider it for our project .
We soon realized that compared to other available tools, the brevity of the PAINAD scale and our clinicians’ familiarity with its concepts (i.e., watching for the five components of facial expression, body language, breathing, negative vocalization and consolability) made it particularly feasible for our project. Each item is scored on a three-point scale (0-2) for severity. The total score can range from 0-10, mirroring the commonly used numerical rating scale familiar to clinicians, with higher scores indicating more severe pain .
During our first learning session in the collaborative, held in April 2007, we completed our Aim Statement: “By November 2007, 90 percent of nonverbal cognitively impaired patients assessed as having moderate to severe pain upon admission will demonstrate an improvement (a decrease) of at least one level in pain severity within 48 hours.”
The beauty of the IHI model is that we were quickly able to make changes as needed based on our observations. For example, by the beginning of our second learning session, we realized that our sample population, as noted in our Aim Statement, should be more broadly defined as “older nonverbal adults .” Ultimately, we determined that “older patients unable to reliably self-report pain” more accurately defined our target population .
continued on next page
Hospice of Central Iowa Collaborative
Team Members:
Linda Clauson
Ronalda Dick
Christine Doubleday
Cindy Fenoglio
Mary Hall
Rosy Harrington
Liz Mayer
Amy Mobley
Kelly Stackhouse
Step 2:Our next step was to carry out our plan—on a small scale first to make sure it worked .
For this initial cycle of change, we selected one of our 10 home-based teams . As the IHI model suggests, we purposefully selected a small sample size and a team that we felt could embrace the change project. However, we also reviewed the records of all admissions for that team to ensure that the patients we targeted for our project (i.e., those who were cognitively impaired or otherwise unable to reliably respond to questions about their pain) were represented . This proved to be the tipping point which truly focused our clinicians’ attention on those patients for whom the planned change was intended .
Step 3:In this step, we summarized what we learned over the course of this nine-month project through collection and analysis of the data . In essence, we asked ourselves “What obstacles and successes did we encounter?”
First, adding “another piece of paper” to the chart was simply not going to work. Initially, we had provided the PAINAD scale within a new form that required staff to document their visits, interventions, etc. But staff saw this new form as burdensome, and we quickly realized we needed to integrate the PAINAD scale into our existing documentation .
Thus, we provided clinicians with a hole-punched, laminated 4x6 card with the PAINAD tool and scoring guide which they could attach to other quick reference cards, making the tool and scoring guide portable and easily accessible . Staff then started documenting the PAINAD scores in the locations typically reserved for the verbal Numerical Rating Scale (NRS) scores .
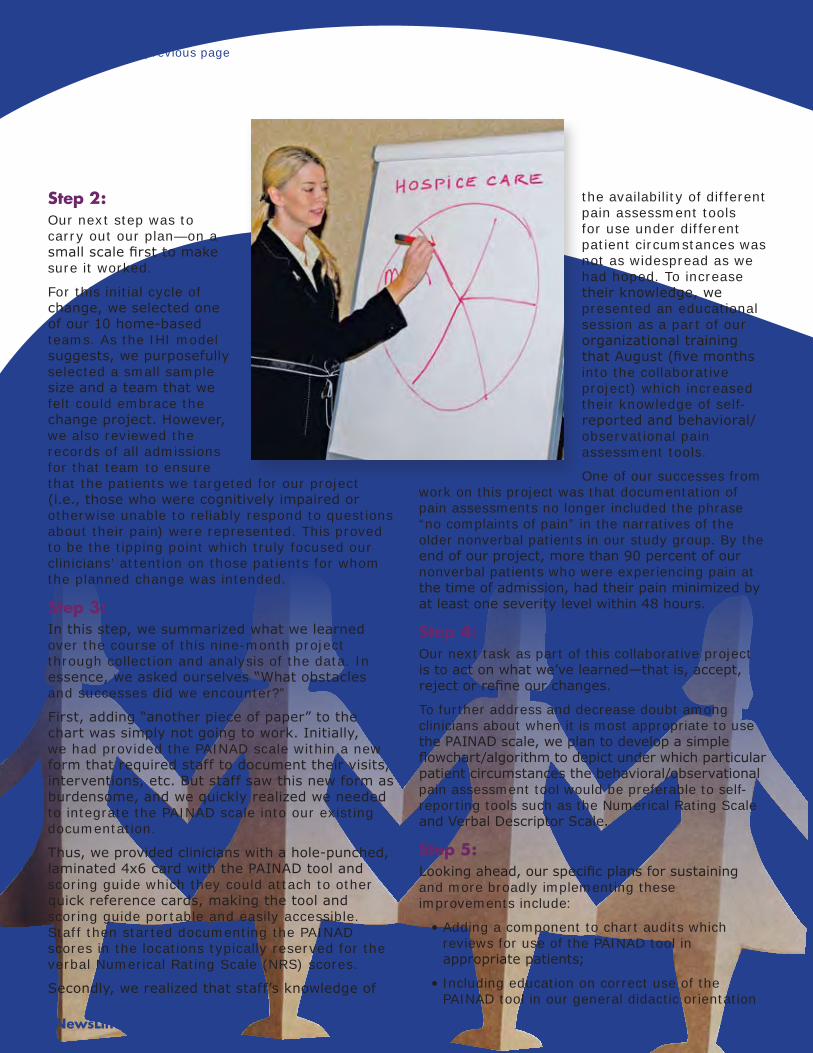
Secondly, we realized that staff’s knowledge of
the availability of different pain assessment tools for use under different patient circumstances was not as widespread as we had hoped . To increase their knowledge, we presented an educational session as a part of our organizational training that August (five months into the collaborative project) which increased their knowledge of self-reported and behavioral/observational pain assessment tools .
One of our successes from work on this project was that documentation of pain assessments no longer included the phrase “no complaints of pain” in the narratives of the older nonverbal patients in our study group . By the end of our project, more than 90 percent of our nonverbal patients who were experiencing pain at the time of admission, had their pain minimized by at least one severity level within 48 hours.
Step 4:Our next task as part of this collaborative project is to act on what we’ve learned—that is, accept, reject or refine our changes.
To further address and decrease doubt among clinicians about when it is most appropriate to use the PAINAD scale, we plan to develop a simple flowchart/algorithm to depict under which particular patient circumstances the behavioral/observational pain assessment tool would be preferable to self-reporting tools such as the Numerical Rating Scale and Verbal Descriptor Scale.
Step 5:Looking ahead, our specific plans for sustaining and more broadly implementing these improvements include:
Adding a component to chart audits which • reviews for use of the PAINAD tool in appropriate patients;
Including education on correct use of the • PAINAD tool in our general didactic orientation
NewsLine24
continued from previous page

NewsLine 25
for new clinicians and in our skills labs for new and existing nursing staff; and
Conducting the project in the remainder of our home-based and • inpatient facility teams .
In Summary:Overall, our team concurred that our work in this Quality Partners Improvement Collaborative definitely moved us toward our project goal and has stimulated an organization-wide re-evaluation of how we will approach all of our future quality initiatives . We believe the project has improved—and will continue to improve—the way clinicians think about pain assessment and management in one of our most vulnerable populations: those who cannot speak for themselves .
Ronalda Dick is director of quality and clinical information at Hospice of Central Iowa, based in West Des Moines. She has 30 years of experience as a registered nurse, including 10 years in hospice care at both free-standing and hospital-based systems.
References:
American Geriatrics Society Panel on Persistent Pain in Older Persons . (2002) Clinical Practice Guideline: The management of persistent pain in older persons; retrieved 12/12/07; www.americangeriatrics.org/products/positionpapers/JGS5071.pdf .
Feldt K. (2007) Pain measurement: Present concerns and future directions . Pain Medicine, 8(7), 541-543.
Herr K, Bjoro K, & Decker S. (2006) Tools for the assessment of pain in non verbal older adults with dementia: A state of the science review . Journal of Pain and Symptom Management, 31(2), 170-192.
Langley GL, Nolan K, Nolan TW, Norman C, Provost LP. (1996) The Improvement Guide: A Practical Approach to Enhancing Organizational Performance . San Francisco: Jossey-Bass Publishing .
Warden V, Hurley A, & Volicer L. (2003) Development and psychometric evaluation of the pain assessment in advanced dementia (PAINAD) scale . Journal of the American Medical Directors Association, 4(1), 9-15.
To learn more
about NHPCO’s
collaboratives and
how your
program can
participate, visit
nhpco.org/quality
> Discover the
Collaboratives.
NewsLine 26
Grief and the
Older AdultBy Diane Snyder Cowan, MA, MT-BC

NewsLine 27
A study in the journal, Brain, Behavior and Immunity (2006), shows that stress caused by the death of a spouse or close friend can have a negative effect on the immune system of older adults .
In fact, researchers found that flu shots were not as effective in building immunity against influenza in older adults who recently experienced the death of a loved one .
Older adults experience grief in much the same way as younger and middle-aged adults; however, their age, life experiences, and oftentimes physical and mental illnesses, can impact their grief reaction. In addition, many older adult patients in hospice care have non-cancer diagnoses such as heart failure, dementia, ALS or renal disease, and the losses that accompany these diseases can affect their hospice stay as well as their loved ones’ bereavement period .
Older adults often experience several losses within a short period of time . They may have a dwindling roster of family and friends and they may be grieving any number of losses simultaneously . These multiple losses can result in feeling overwhelmed or numb. In addition, older adults who lose their spouses may also feel they’ve lost their financial security, their best friend, and other social contacts and supports.
The natural process of aging involves many losses. These include, but are not limited to, loss of physical strength and endurance, independence, mobility, youth and beauty, the home, and purpose. If the older adult has a debilitating disease, there are also losses associated with the disease progression . Older adults may have to give up their role in the family which can cause a change in the family dynamics . Older adults may feel sad, but not identify this feeling as grief. Often, they are reluctant to share these feelings with others . Many do not want to be a burden to their family. Some fear if they share their sadness and grief, they may be perceived as unable to take care of themselves and will need to be “put somewhere .”
Older adults are more likely to become physically ill after a loved one dies. If they already have a chronic illness, it may progress more quickly while they are grieving . The practical issues surrounding one’s own health can also interfere with a person’s ability to grieve or complicate their grief reactions . Some older adults actually develop symptoms experienced by the deceased, such as cardiovascular or gastrointestinal problems . It is important that bereaved older adults maintain contact with their healthcare providers .
Older adults often lack the support systems they had in their younger years. After the funeral, family members return to their own lives, leaving the bereaved older adult feeling very alone . If the person had depended on his/her spouse to create social contacts, the person may, literally, have no one to talk to.
Some fear if they
share their sadness
and grief, they
may be perceived
as unable to take
care of themselves
and will need to be
“put somewhere.”
continued on next page
NewsLine 28
continued from previous page
The elderly may also find themselves struggling with their own mortality . Many older adults begin their day by reading the obituaries . They may experience more anticipatory grief than younger adults—anticipating another loved one’s death or thinking about how they will cope if they lose something special to them such as their family home . Some people think older adults overreact to losses when, in reality, any loss—big or small—may trigger a grief reaction . It is common to hear older people say, “all my friends have died” or “I’ve been to 12 funerals in the past year.” Each of these deaths has a different level of significance to the person experiencing the loss .
Complicated GriefSome older adults develop complicated grief . The experience of multiple death losses, combined with the losses that occur naturally as part of aging and the anticipation of more death, can become overpowering . Some older adults need more time than others to adjust to change—and too much change can be overwhelming .
Many older adults suffer from untreated depression . While depression can occur with other medical illnesses such as cardiovascular disease, stroke, diabetes or cancer, healthcare professionals often mistakenly conclude that depression is a normal result of these illnesses; the elderly often assume this as well . What’s more, some people believe that depression is a normal part of growing older and, as a result, depression is often underdiagnosed and undertreated. In fact, there exists a marked increase in depression and suicide in the elderly. According to Caruso (2006), older adults comprise only 13 percent of the population, yet individuals ages 65 and older account for 18 percent of all suicides .
Recognizing the Difference Between Grief and DepressionIt is important to note that while depression can include grief, grief can also mimic depression. Recognizing differences and similarities between the two is critical .
Grief encompasses a broad spectrum of behaviors and feelings that are common after loss . Many normal grief reactions may seem like characteristics of depression, but in reality, grief and depression are very different . Clinical depression can include suicidal ideation, plans, or attempts . It is important to be aware of these differences and to acknowledge that complicated
grief can progress to clinical depression if not addressed . A comprehensive clinical assessment can aid in determining if the older adult is becoming depressed and can guide the clinician in recommending additional treatment as necessary .
How can you support an older adult who is grieving?
Older adults may need more time to become • aware of and express their feelings . Giving them extra time shows empathy, compassion and respect .
You may need to point out signs of changes • in behavior and sadness . This will help older adults become more aware of their feelings and help them more readily talk about them .
Older adults who are isolated can benefit • from the company of others . Spend time with them . Give them the gift of presence .
Talk about the deceased . Encourage the older • adult to share memories . Recalling memories and telling stories are part of the healing process .
Since many older adults have experienced • multiple losses, encourage them to talk about each loss separately . This will help them feel less overwhelmed and better able to cope with their grief .
Be aware of the signs of complicated grief and • depression. If you have concerns, encourage the older adult to consult a healthcare provider .
References:
Bereavement and marriage are associated with antibody response to influenza vaccination in the elderly . Brain, Behavior and Immunity, 20 (3): 279-289, 2006.
Caruso, K. Elderly Suicide, 2006. Retrieved November 15, 2006 from www .suicide .org .
Diane Snyder Cowan is the director of The Elisabeth Severance Prentiss Bereavement Center, a program of Hospice of the Western Reserve in Cleveland, Ohio. This is her first term as an NCHPP Bereavement Professional steering committee member.
NewsLine 29
Some people
believe that
depression is a
normal part of
growing older
and, as a result,
depression is often
underdiagnosed
and undertreated.
NewsLine 30
Hospice continues to be plagued by many myths and misperceptions—perhaps none more detrimental than the idea that hospice
is a benefit exclusively for cancer patients.
We all recognize that, in most of our communities, today’s hospice population does not accurately represent the ways in which people die . It’s important that we all recognize the opportunity and mission-driven obligation we have to find new ways of connecting to all terminally ill patients and their families .
Rather than seeing diversification as an insurmountable obstacle to growth, some hospices are successfully turning it into an opportunity to engage in meaningful dialogue . It’s a chance to shift to a more inclusive discussion of the hospice benefit, and it can help you balance your length-of-stay, the acuity of your patient mix, and the locations in which you’re providing care .
The key to success comes in both the planning and the execution, and it requires a hard, honest look at your organization’s needs, your referral community’s capacity for change, and your willingness to invest the time in building and executing a proactive marketing strategy .
Step 1: Assess Your SituationThis requires a willingness to look honestly and objectively at your current business and at trends that may have emerged over the past 12 to 18 months .
How’s your length-of-stay? Is your average • length of stay being bolstered by a few extremely long-term patients while your median length of stay hovers well below the national average?
Are you facing any Medicare Cap issues? As • you explore ways to diversify your patients, you’ll want to stay mindful of any potential for Cap deficits.
How penetrated is your market? If 90 percent • of eligible patients are already under the care of hospice, your plan will look very different than if your community’s utilization of hospice is very low .
How do your numbers stack up against the • national averages? Recognize that there can be significant differences based on geography and demographics (e .g . a rural community with fewer oncologists and hospitals might expect to have a lower percentage of cancer patients than a major metropolitan area) . You also will want to look at the overall causes of death (available at cdc .gov) and see how close your patient mix matches these numbers (removing such non-eligible categories as homicide) .
Your goal in this process is to make sure you know where you stand today—and to identify your most significant areas of opportunity. This will also help you identify your core objectives and how you’ll measure the success of your efforts . Make sure your leadership team is in agreement on these objectives, and gain consensus. A successful strategy will require across-the-board support .
Not Just for Cancer AnymoreDiversifying Your Patient Mix Through Proactive MarketingBy Mike Fleming
NewsLine 31
Rather than seeing
diversification as
an insurmountable
obstacle to growth,
some hospices
are…turning it into
an opportunity
for meaningful
dialogue.
Step 2: Analyze Your BusinessNow that you have a sense for some key metrics and have identified your objectives, take a step back and ask yourself these questions:
Where are your referrals coming • from (i.e., what are your key accounts)? Are you extremely dependent on a certain cancer center, nursing home, or hospital? Look for diversification and depth.
Do these areas of referral emphasis • (e.g. physicians, hospitals, nursing homes) match your objectives in terms of a referral mix?
Who are your prospects (i.e., referral • sources you are approaching, but ones which have not yet begun sending referrals)? Are these prospects likely to help you diversify your mix?
Consider your competition and where their business comes from . • Are they doing a better job of balancing their patient mix or are they competing with you for the very same accounts?
If you haven’t yet developed a database of your current referral sources and prospects, use this as an opportunity to do so. And whether it’s a giant Excel spreadsheet or a more robust CRM system, be sure to keep track of both the number of referrals and patient mix (by diagnosis) you expect from each referral source .
Step 3: Research Your Heart OutNow that you know your situation, your objectives, and your target audiences, you need to assess your effectiveness in reaching these folks with a message that will move them to action. In other words, what can you say that will lead them to add to your mix of non-cancer patients?
Assess the knowledge gaps within your targets . Are they not aware • that hospice is available to non-cancer patients? Or is it that they don’t believe hospice is helpful to the non-cancer population? Or maybe it’s that they tend to make all hospice referrals in the last week or two? This assessment will tell you a lot about what it will take to spark action .
Look at results of your family satisfaction surveys—especially • questions that prompt comments about the timeliness of hospice referrals . Search for gems that might open doors to future conversations with your referral sources .
continued on next page
NewsLine 32
continued from previous page
Consider holding focus groups with referral • sources, bereaved families, and/or community leaders . Use this as an opportunity to assess knowledge gaps and key issues . You can also use this time to begin the education process . By taking the time to tell them that their opinions matter, you’ll be taking a huge step toward building life-long ambassadors and advocates for hospice care .
Use this research to identify your core • messages, and align these messages with your key audiences . This will give you the ability to target your audiences with the most impactful (and motivating) stories possible .
Step 4: Tell Your StoryConsider all the creative ways to reach your identified target audiences with the right messages . Here are some ideas:
Educate referral sources on individual hospice • diagnoses that might be prevalent among their patient population . Use case studies (preferably of actual patients you have cared for) to make it real for them, and connect these studies to eligibility criteria to illustrate how to identify when a patient should be referred .
Take the time to educate on the leading causes •
of death from the research you’ve already done. For example, imagine the power of telling a cardiologist what a small fraction of heart disease-related deaths are under the care of hospice? This can be a real conversation starter because it makes the discussion bigger than just your hospice or any one individual physician or patient .
Debunk myths by providing targeted • education—and use evidence-based research whenever you can . Consider the use of talking points from research articles like the one in the Journal of Pain & Symptom Management (March 2007) that proved how some hospice patients actually live longer than their non-hospice cohorts (on average, 29 days longer). For any referral source hesitant to refer because of the fear that hospice equates to “a death sentence” or “giving up hope,” this research can be a real eye-opener .
Develop a few specific, targeted sales calls • that you can make with your key audiences . Maybe you have decided that cardiologists and pulmonologists are your primary targets . Think about how to get time with them (maybe an introduction through direct mail followed by a phone call or personal visit) and what you’ll say when you get the chance to speak with them . (Again, case studies and statistics can be huge credibility builders!)
Consider how your medical director can help . • Sure, CMEs are great and valuable—but think about the little things, too. Does your medical director do physician-to-physician consults? How connected is she within the healthcare community? Does she attend meetings at the local hospital? Maybe he’s a member of the state medical society? These are built-in opportunities for someone with great clinical credibility to communicate your key messages . You just need to help them feel comfortable telling the story .
Think about how you use your Web site—and if you don’t yet have a web presence, now’s the time to get started . Use your web presence to educate and inform, and make sure that your print collateral, advertisements, and other materials tell the same story . By showcasing all the many types of patients (and their diagnoses) that you serve, you begin broadening the minds of all who come to you for information and education .

Diversifying
your patient mix
is really very
much like any
other marketing
initiatives. Good
upfront planning
and research will
go a long way.
NewsLine 33
Step 5: Measure Your SuccessYou’ll want to keep track of your progress since you will be learning so much along the way. Pull out your original objectives, and keep a progress report to see how you’re doing . Some possible measures could be:
Overall diagnosis mix (maybe comparing your mix to leading causes of • death and/or to national hospice averages);
Average and/or median length of stay;•
Number of new non-cancer referral sources developed and the volume • of referrals/admissions.
How often should you track your progress? The ideal answer is daily—because you should be able to keep your finger on the pulse of whether your efforts are moving the needle. However, a more realistic goal is to formally track these metrics at least quarterly, if not monthly. After all, if the outcomes aren’t following your investments, then it’s time to reset your goals .
Final ThoughtsDiversifying your patient mix is really very much like any other marketing initiative. Good upfront planning and research will go a long way, and you always need to keep track of your progress. However, if you find yourself getting overwhelmed as you work through this process, return to these four questions to get back on track:
1. What do you want to accomplish (measurable objectives)?
2 . Who can help you accomplish these objectives (target audiences)?
3. What do they need to hear in order to be moved to action (key messages)?
4. How will you reach them with these messages (marketing tools and tactics)?
Also, make sure that you don’t lose sight of your cancer referral sources. The goal is a diversified and balanced mix—and that mix needs to include cancer patients too .
Finally, always take time to celebrate your successes along the way and to celebrate the work that you and your colleagues do each day . Hospice is indeed special work, and our overarching goal should always be to bring this amazing benefit to as many eligible patients as possible—regardless of their diagnoses .
Mike Fleming is vice president of marketing and communications for VistaCare, a national hospice provider headquartered in Scottsdale, Arziona. Prior to joining VistaCare in 2003, Mike spent more than 10 years in hospital marketing and public relations with health systems in California and Kentucky. He has been a member of NCHPP’s Development/Marketing/PR Steering Committee since 2006.
NewsLine 34
Recently, I had a conversation with a hospice medical director about changes in her practice . She mentioned that in the last
week, six patients had asked her about having physical therapy during their hospice care . “How can we meet their needs and desires, and still do hospice care?” she had asked .
Better informed and more vocal consumers are now expecting a broader range of care than hospices have traditionally offered . At the same time, access to hospice care continues to improve, as evidenced by today’s average lengths of stay (59 days, per NHPCO’s 2006 findings), and the growing number of patients now living with non-cancer diagnoses (55.9 percent, per NHPCO’s 2006 findings). While these are both positive indications of our professional success, these changes also require that we become more flexible in changing the mix of care we provide—through foresight and planning .
Care Needs of the Non-Cancer PatientNeurological conditions such as ALS, Parkinson’s Disease, and recurrent cerebrovascular accidents (i.e., strokes) bring with them often complex arrays of muscular strength/weakness, muscle tone abnormalities (spasticity, flaccidity, rigidity), and sensory changes. These physical manifestations may be present in lower or upper extremities, or the oral and bulbar structures, and can best be evaluated by the team’s physical, occupational, or speech therapists, who routinely address such conditions and the functional impairments that result. Being limited in mobility,
self-care, and/or communication and eating dramatically affects quality of life. Specialized equipment, adaptive devices, and communication aids may be needed or already in place . Different techniques can be used to facilitate movement, normalize muscle tone, and educate the family caregivers about the evolution of the disease process and ways to effectively provide care . The care plan and interventions that result will assure that optimal mobility, comfort, and safety will be achieved .
Similarly, end-stage cardiac and pulmonary conditions bring their own sets of physical limitations . Due to often extreme limitations of cardiac output, with ejection fractions of less than 20 percent and diminished oxygen saturation, energy conservation measures are extremely important to allow functional mobility without causing undue cardio-pulmonary stress and the resultant symptoms of anxiety . The physical therapist can adjust walking devices to lower heights, allowing for improved efficiency and decreased exertion . A gentle exercise program can improve peripheral muscular performance . And, monitored ambulation with breathing control exercises can educate patients about their limits and ways to work within a relative comfort zone to decrease anxiety and the need for medications with activity. Using occupational therapy, patients and families can learn the easiest way to successfully accomplish activities of daily living which, in turn, can promote improved dignity and quality of life .
These cases also bring a much more complex
Rehabilitation Tools
to Promote AccessBy Richard Briggs MA, PT

NewsLine 35
psychosocial dynamic, as these diseases are not so easily recognized by those living with them as “terminal conditions .” It is likely that such patients have received the benefits of intermittent rehabilitation therapy in their struggle to continue living at the highest functional level . A hospice-appropriate therapy program, on the other hand, would also include instruction and caregiver support which would help promote a sense of wellness and easier acceptance of the transition to end-of-life care .
Hospice Models for Rehabilitation TherapiesThe models for rehabilitation therapies in hospice differ significantly from those in traditional rehabilitation programs. Acute care, outpatient, and rehabilitation settings—with a high intensity of therapy services—all demand that significant and timely progress be documented to assure reimbursement from the payment source . People receiving therapy under a hospice benefit, however, are likely to make gains in a much more gradual way, if able, and over time transition to a state of declining function. This trajectory of activity, along with a different reimbursement system, necessitates a much lower visit frequency (i.e. weekly or biweekly), with the emphasis on family instruction and home programs, and ongoing re-assessment and intervention by the therapist when needed. Palliative care models of “light rehabilitation,” “rehabilitation in reverse,” and “case management” work well in the hospice spectrum of end-of-life care .
Earlier referrals will bring us patients who are not as far along in their end-of-life care journey . What would hospice care look like if the average length of stay was 90, or even 120 days? We do the ‘dying’ part well, but sometimes struggle with the ‘living’ if it takes us from an accustomed pattern or practice . As the frequency of longer stays becomes more common, our familiarity and comfort with a different and evolving focus will become more the norm .
The utilization of therapies for our changing patient demographic necessitates close interaction and communication among members of the interdisciplinary team. For example, social work and nursing must recognize the short-term therapeutic goals of the patient who desires to continue his/her struggle to live, and may not yet even partially accept the hospice goal of acknowledging death. At the same time, the different perspective of therapy early on in care can create confusion between the patient, family, and the hospice team, if members of the interdisciplinary team are not aligned and in concurrence. As we know, this is work in progress, and part of our eventual objective over the course of care. It is also an exceptional challenge for the team to accept and to execute together, requiring much self-knowledge, sensitivity to the patient and family, and communication amongst themselves.
The therapist, who is well-integrated into the hospice team and adept at negotiating the transitions of a patient’s functional decline and changing status, can be an extremely valuable team member in facilitating the
What would
hospice care look
like if the average
length of stay
was 90 days?
We do the ‘dying’
part well, but
sometimes struggle
with the ‘living’ if
it takes us from an
accustomed pattern
or practice.
continued on next page

NewsLine 36
focus of care toward understanding the inevitable outcome by patient and family . Support is provided in recognition of the patient’s significant efforts, the lack of control over improvement, stabilization, or decline of the body, and the ultimate wholeness of a person despite these changes . Initially seen as a beacon of hope, the therapist becomes a catalyst for change . If an activity is not possible with therapy intervention and support, it is recognized as unrealistic, and more easily accepted by all.
Challenges abound in the ever-changing environment of end-of-life care . We must continue to recognize the opportunities we have to expand our outreach in support of those living in the final phases of their lives. Using appropriate rehabilitation therapy services can be of great benefit to hospice care for the earlier admissions and non-cancer patients we serve .
Richard Briggs has 20 years of experience as a physical therapist with Enloe Homecare and Hospice in Chico, California. He is the immediate past-chair of NCHPP’s Allied Therapist Section and continues to serve as a member of the section’s steering committee. In addition to his work with NCHPP, Rich writes, lectures, and consults with agencies to integrate physical therapy into hospice care through his practice, Hospice Physical Therapy Associates.
References:
Complementary Therapies in End-of-Life Care . National Hospice and Palliative Care Association, 2001, Chapter 6, 7, 8, for Occupational, Physical, and Speech Therapy .
Pizzi MA, Briggs R., Occupational and Physical Therapy in Hospice: The Facilitation of Meaning, Quality of Life, and Well-being. Topics in Geriatric Rehabilitation. 2004; 20 (2): 120-130.
Briggs R . Models For Physical Therapy Practice in Palliative Medicine . American Physical Therapy Association, Home Health Section Quarterly 1999; 34(4): 6-7.
Resources:
Hospice and Palliative Care Special Interest Group for Physical Therapists (oncologypt.org/sigs/hospice .cfm) .
American Occupational Therapy Association (aota .org) .
American Speech Language and Hearing Association (asha .org) .
continued from previous page
NewsLine 37
Seven years ago, my dad died of pulmonary fibrosis. His name was Jim, and he and my mom were married for 53 years. He had been a conductor on the railroad for 36 years, riding at the tail
end of freight trains as the conductor in the caboose, inhaling brake dust laced with asbestos . He also spent time as a tire-shop worker and a fuel truck driver . We lived in a steel town and he spent his working life around polluted air. For many of those years, the aroma of Borkam Riff pipe tobacco also meandered through our house .
Any, all, or none of these noxious factors may have contributed to his disease. By the time he was diagnosed, it didn’t really matter . He’d been a robust man before the disease . When he died, Dad was stick-thin, his only bulk contributed by years of steroids . He required six liters of oxygen on a continual basis and suffered severe dyspnea (difficulty breathing) with just a few steps . But always, he managed a positive spirit . Even when he struggled for the next breath, lips slack and purple, chest heaving in rapid little gasps, he would simply mutter, “I’m outta puff .” It’s no wonder that over my years as a hospice nurse, patients with pulmonary fibrosis have been some of my favorites . I believe that we can serve more of them than we do .
According to the Pulmonary Fibrosis Foundation, there are over five million people affected by the disease throughout the world14—and over 200,000 in the United States alone. Due to the difficulty in establishing an accurate diagnosis, this may actually be a low figure.10 In our country, more than 40,000 patients die each year of this disease, a number which matches the rate of death from breast cancer .3 The most frequent cause of death is respiratory failure, leading to 80 percent of the deaths.10 Heart
Improving Access for Patients With Pulmonary FibrosisBy Sue Montgomery, RN, BSN, CHPN
In our country,
more than 40,000
patients die
each year of this
disease, a number
which matches the
rate of death from
breast cancer.3
continued on next page
failure, bronchogenic carcinoma, ischemic heart disease, infection, and pulmonary embolism are also common causes .10
There is no cure for pulmonary fibrosis. Yet, according to data compiled by the Centers for Medicare and Medicaid Services, this appears to be a population underserved by hospice providers . In the CMS data for the year 2006, breast cancer falls within the top 10 diseases served by hospice while pulmonary fibrosis, as a lung disease distinct from Chronic Obstructive Airway (COA) disease, is not even mentioned— despite the fact that breast cancer and pulmonary fibrosis have the same mortality rate .7,8 While it may be possible that data for pulmonary fibrosis is included within the COA group, this would be a major error in nomenclature and reflective of the difficulty in gathering accurate statistics for the disease . If we know that the rates of mortality for pulmonary fibrosis match those of breast cancer, yet we are unable to measure our frequency of services to this population, we certainly have opportunities to improve access for these patients .
What is Pulmonary Fibrosis?To define pulmonary fibrosis, let’s start first with what it is not. Pulmonary fibrosis is not COPD. COPD (Chronic Obstructive Pulmonary Disease) is characterized by a chronic, progressive, obstructive pulmonary process. Conversely, pulmonary fibrosis, which is often called Idiopathic Pulmonary Fibrosis (IPF), is a chronic, progressive, restrictive pulmonary disease .11 [The word “idiopathic” in the name simply means the cause is not known.] It is characterized by chronic inflammation of the lungs which leads to tissue injury. Irreversible scarring occurs, leading to restriction of the lungs and chronic impairment of gas exchange . Breathlessness upon exertion and a dry, irritating cough are classic symptoms of the disease .6
The disease’s progression can be variable, but most patients experience progressive decline toward respiratory failure and death within three to five years from the time they are diagnosed.11 Although such patients are often treated with steroids, immunosuppressives and antifibrotics, research has yet to provide evidence that the use of such regimens improves a patient’s outcome .5,1
What’s more, side effects from these therapies are numerous . Still and all, physicians and patients try what they can in an attempt to slow disease progression .4
Differences in Symptom ManagementPatients with pulmonary fibrosis—or IPF—benefit from traditional approaches to dyspnea management .1,6 There are, however, two significant differences between the treatment of dyspnea in patients with IPF and those with COPD . These differences are related to oxygen dosage and the use of diuretics .
Donald Simmler, MD, is an associate medical director at The Hospice of the Florida Suncoast and is board certified in internal medicine with a subspecialty in pulmonary medicine . Dr . Simmler notes that, “unlike patients with COPD, who may be harmed by high levels of oxygen, patients with IPF benefit from higher oxygen flow. Also, clinicians may attempt to treat the dry rales of pulmonary fibrosis as fluid overload. Inappropriate use of diuretics with these patients can lead to dehydration and discomfort.” These dry, “Velcro-like” rales are due to the formation of scar tissue and cannot be treated away .6 An additional difference for these patients involves the severe and rapid onset of dyspnea . Depending on the level of disease progression, patients with IPF may actually appear fairly comfortable at rest with good saturation rates. However, with the slightest amount of exertion, rapid and severe oxygen desaturation occurs . This is an important distinction for clinicians to note, since these patients are often evaluated at rest .
Challenges and OpportunitiesDifficult to Diagnose
IPF is very difficult to diagnose and patients sometimes spend years being treated for other pulmonary conditions with similar characteristics before obtaining a diagnosis .6,10 Although use of pulmonary function tests, chest x-rays and high-resolution CT scans are common, surgical lung biopsy is recommended as the gold standard to confirm diagnosis.2 Continued improvements in methods for efficient, accurate diagnosis are sorely needed .
NewsLine 38
continued from previous page

Pulmonary
fibrosis is not
COPD…. Often
called Idiopathic
Pulmonary Fibrosis,
it is a chronic,
progressive
restrictive
disease.
NewsLine 39
Difficult to Prognose
Although median survival time has been established,11 difficulty still exists in the timing of hospice referral . The objective measurement of impact on quality of life through traditional health-related quality of life tools is a challenge since none exists specific to IPF.11 However, the use of current tools reflect some correlation between traditional measures of lung disease severity and scores which reflect a negative impact on quality of life .11,13 If community physicians use such tools to link disease severity with quality of life measurements, they may refer to hospice earlier .
Difficult to Discuss
Many physicians continue to struggle with the difficult discussions surrounding a terminal diagnosis. Often, physicians fear that the patient will feel that they have given up .9 However, research shows that patients are usually waiting for their physicians to initiate such discussions .9 Additionally, the interpretations of the Hospice Medicare Benefit regulations by physicians may hinder such discussions .9 Our physician partners in the community need help to be better equipped to carry out these crucial conversations .
Difficult to Let Go
Physicians may view a referral to hospice as a loss of control over the care of someone they’ve grown very fond of,9 and patients and their families may feel that they are losing a close friend . Both need to be educated and reassured that hospice is a partner, not a replacement.
In his study of patients’ perceptions regarding the impact of IPF on quality of life, Jeffrey James Swigris, DO, MS, notes the following:
“Participants yearned for more attention to end-of-life issues from the medical community. In general, they felt insecure about the dying process, afraid their symptoms would not be controlled toward the end of their lives and that the experience of death would be that of conscious suffocation. However, more than the dying process itself, many patients feared that they would be living a ‘worthless existence’ toward the end of their lives . Many voiced concerns that they had several things that they wanted to do before dying .”12
Patients with IPF, their families, and their physicians, need to be educated about hospice—and what it can offer to them . They need the message that we’re not about letting go…we’re about quality of life in every manner possible .
continued on next page
NewsLine 40
continued from previous page
In SummaryPatients with IPF and their families are in great need of the unique care that only hospice and palliative care can provide . Through increased education and support, we must strive to meet the needs that are before us every day . My dad didn’t have hospice before he died . Maybe the fact that his daughter was a hospice nurse gave him some sense of comfort, thinking that I’d be able to control things that I really didn’t have any control over . Or maybe he was afraid of all that the “H” word conjured up in the small town where his physician wouldn’t even entertain thoughts of low-dose morphine, let alone hospice care. Despite this, we were blessed with Dad’s peaceful death—with our family at his side . As hospice and palliative care providers, we know that such comfort and peacefulness can be a challenge for these patients. However, if we improve access to our services, we improve the odds that hospice will be there to help make that happen .
Sue Montgomery has been a nurse for 23 years. She is currently the director of interdisciplinary practice at The Hospice of the Florida Suncoast in Clearwater, Florida, where she has worked in various staff and leadership positions for more than 12 years.
References:1 Allen, S., Raut, S., Woollard, J., & Vassallo,
M. (2005). Low Dose Diamorphin Reduces Breathlessness Without Causing A Fall in Oxygen Saturation in Elderly Patients With End-Stage Idiopathic Pulmonary Fibrosis . Palliative Medicine, 19(2), 128-130.
2 American Thoracic Society, Idiopathic Pulmonary Fibrosis: Diagnosis and Treatment . International Consensus Statement . American Thoracic Society (ATS), and the European Respiratory Society (ERS), American Journal of Respiratory and Critical Care Medicine, 161 (2000), pp. 646–664.
3 Breast Cancer: Statistics on Incidence, Survival and Screening . (n .d .) Retrieved November 28, 2007 from http://www.imaginis.com/breasthealth/statistics.asp#1 .
4 Collard, H. R., Loyd, J. E., King Jr., T. E., & Lancaster, L. H. (2007). Current Diagnosis and
Management of Idiopathic Pulmonary Fibrosis: A Survey of Academic Physicians . Respiratory Medicine, 101(9), 2011-2016.
5 Davies HR, Richeldi L.(2002). Idiopathic Pulmonary Fibrosis: Current and Future Treatment Options . American Journal of Respiratory Medicine. 1(3), 211-224.
6 Lindell, K. O., & Jacobs, S. S. (2003). Idiopathic Pulmonary Fibrosis: New Guidelines for Diagnosing and Managing the Disease Demand—A Fresh Approach to Nursing Care . American Journal of Nursing, 103(4), 32-43.
7 Medicare Hospice Data-1998-2005. (n.d.) Retrieved November 28, 2007 from http://www.cms.hhs.gov/ProspMedicareFeeSvcPmtGen/downloads/HospiceData1 998-2005.pdf .
8 NHPCO Facts and Figures: Hospice Care in America. November 2007 Edition. Retrieved November 30, 2007, from http://www.nhpco.org/research .
9 Quill, T. E. (2000). Perspectives On Care at the Close of Life . Initiating End-of-Life Discussions With Seriously Ill Patients: Addressing the “Elephant in the Room .” JAMA, 284(19), 2502-2507.
10 Raghu, G., Weycker, D., Edelsberg, J., Bradford, W., & Oster, G. (2006). Incidence and Prevalence of Idiopathic Pulmonary Fibrosis . American Journal of Critical Care Medicine, 174(7). 810–816.
11 Swigris, J.J., Gould, M.K. & Wilson, S.R. (2005). Health-Related Quality of Life Among Patients with Idiopathic Pulmonary Fibrosis . Chest, 127(1), 284-94.
12 Swigris, J.J., Gould, M.K. & Wilson, S.R. (2005). Patients’ Perspectives on How Idiopathic Pulmonary Fibrosis Affects the Quality of Their Lives . Health and Quality of Life Outcomes. Retrieved November 28, 2007 from pubmedcentral .nih .gov .
13 Tzanakis, N., Samious, M., Lambiri, I., Antoniou, K., Siafakas, N. & Bouros, D. (2005). Evaluation of Health-Related Quality-of-Life and Dyspnea Scales in Patients With Idiopathic Pulmonary Fibrosis: Correlation With Pulmonary Function Tests . European Journal of Internal Medicine, 16(2), 105-112.
14 What is Pulmonary Fibrosis? (n .d .) Retrieved November 28, 2007 from http://www.pulmonaryfibrosis.org/ipf.htm .

NewsLine 41
Recently I attended a workshop where the question was asked: Are we advocates for patients
and families prior to admission?
Social workers should have no trouble answering this question with a yes . The profession’s core value of social justice calls on social workers to “strive to ensure access to needed information, services and resources, equality of opportunity, and meaningful participation in decision making for all people.” Additionally, the preamble to the National Association of Social Work Code of Ethics states that “social workers should seek to promote the responsiveness of organizations, communities and other social institutions to individual’s needs and social problems .”
Social workers clearly have an opportunity to play an important role in hospice and palliative care organizations by advocating for improved access for underserved populations . A number of examples help to illustrate how social workers might proactively advocate for access prior to admission:
Partner with existing organizations to conduct a community-wide • needs assessment. One social worker worked with a local United Way organization to better determine unmet healthcare needs. Another program utilized social work students to conduct a needs assessment.
Conduct a series of focus groups with underserved populations to • determine how best to meet their needs. One hospice program conducted focus groups with parents of children with life-limiting illness to determine how best to serve pediatric patients .
Partner with minority groups to share information about hospice • services and to uncover disparities. Social workers are aware that programs need to be sensitive to cultural barriers that might prevent individuals from accessing needed services .
Routinely review admissions/referral policies to look for barriers to • being served. Some hospice programs have policies that keep them from admitting patients without a caregiver .
Promoting Responsiveness in End-of-Life CareBy Sherri Weisenfluh, MSW, LCSW
continued on next page

NewsLine 42
Once a patient is admitted to a hospice program, a social worker might also:
Advocate for clients who might be viewed as • difficult. Patients who are homeless, have long histories of mental illness, or refuse to comply with treatment plans challenge and frustrate staff. Despite the challenges, such patients need and qualify for services .
Review complaints to determine any pattern • relating to access .
Make sure patients have equal access to • continuous care and respite services .
Review the entire range of services under • the Medicare Hospice Benefit to determine if patients have access to inpatient services when appropriate .
By being an advocate for patients and families—prior to admission as well as after— social workers have an opportunity to daily live up to the core value of social justice and ensure that hospice and palliative care programs are responsive to those we serve .
continued from previous page
Sherri Weisenfluh is the associate vice president of counseling for Hospice of the Bluegrass in Lexington, Kentucky, a position she has held for 15 years. In addition to her service as NCHPP’s Social Work Section Leader, she teaches part-time at the University of Kentucky.
Are you sure?
Are you protected if something goes wrong here?It can easily happen. The patient’s condition changes. The orders arenot quite clear, or a subtle observation is not made. Maybe the patient’sfamily is just unhappy. In any event, the result can be a serious lawsuitagainst your organization and your employee or volunteer.
Lawsuits are expensive to defend, and some result in very high-dollarlosses. That’s why liability insurance coverage is so important.Hospice and Community Care Insurance Services is administered byGlatfelter Insurance Group, a national agency. We work closely withyour insurance agent to provide competitive proposals and friendly service for special businesses like yours.
Remember, before you can take care of others, you have to
take care of yourself.
Insurance for Hospices and Home Health Care Agencies� Professional Liability� General Liability
For more information, call 800-233-1957 • www.hccis.com
� Property Insurance� Non-owned Auto Liability
� Directors & OfficersLiability
Administered by Glatfelter Underwriting Services, Inc.a/k/a Glatfelter Insurance Services in CA, MN, NV, TX, and UT and Glatfelter Brokerage Services in NY
4ads_HalfPg cmyk 12/4/07 11:16 AM Page 1
AD
VER
TIS
EMEN
T
March 2008NewsLine 43
An estimated five million Americans have dementing diseases, one million of them in advanced stages . Dementia refers to the progressive loss of memory and other cognitive
functions, often but not always resulting from illnesses such as Alzheimer’s disease.
NHPCO estimates that 10.3 percent of patients who died in 2006 while under hospice care had dementia as their primary diagnosis . This estimate is based on data submitted by 603 hospices in response to NHPCO’s annual National Data Set survey .1 An unknown number admitted with other diagnoses such as cancer, organ failure or general debility may have had dementia as a comorbidity or secondary diagnosis. What’s more, the Centers for Medicare and Medicaid Services reports that 77,577 Medicare hospice patients were diagnosed with either Alzheimer’s disease or Senile Dementia in 2005 (up from 31,797 in 2000). This growth in the number of Medicare hospice patients with the disease, in addition to the number of non-Medicare hospice patients, suggests a total annual hospice dementia caseload of 100,000.
Estimating life expectancy, recognizing when people with dementia have an appropriate prognosis for hospice care, and successfully obtaining coverage for their care from Medicare can pose significant challenges . NHPCO’s Dementia Work Group is exploring these challenges, promoting additional prognostic research, and engaging in dialogue on coverage issues with Medicare fiscal intermediaries.
A new report from NHPCO suggests, however, that hospices can work within the current system to open doors for eligible patients and provide them with the palliative care services they need and deserve. The 27-page report, Caring for Persons with Alzheimer’s and Other Dementias, is filled with concrete information on providing high-quality, evidence-based care and helping to maximize the quality of life of these patients and their families . It also features examples of hospices that are working effectively within existing eligibility guidelines . (Members can download a copy of the report, free of charge. See page 46.)
Improving theQuality of Lifefor Patients with Advanced DementiaBy Larry Beresford
continued on next page
NewsLine 44
Hospice Care Can Make a DifferencePatients with dementia who qualify for and are enrolled in hospice care are typically no longer able to express their end-of-life care preferences verbally . For such patients, it is important to look for guidance from advance directives or from their family’s surrogate representations of their values, especially when it comes to clarifying important treatment decisions related to feeding tubes, antibiotics, rehospitalizations and the like.
But patients with advanced dementia may still express themselves through facial expressions, body language and how they react at meals or bathing times—challenging their caregivers to work with these demonstrated preferences rather than trying to force a meal or a bath on them using traditional language and interventions . Even if it takes a little longer, there are techniques that can be used to recognize, interpret and accommodate those behaviors in order to enhance, rather than detract from, the person’s quality of life .
Most of all, the NHPCO report argues that hospices need to recognize that their skills—in symptom management, psychosocial and spiritual support, and bereavement counseling—can be extremely valuable to these patients and families . These individuals are in our communities today, eligible for hospice care and, in some cases, already on our caseloads .
Hospices are encouraged to seek out more information about the specific needs of these patients and provide targeted education to the staff members who care for them . In some cases, it may also be appropriate to consider the development of specialized services, teams, or programs for patients with advanced dementia .
For hospices, advanced dementia is the ultimate challenge, but also the ultimate opportunity to share the very best that is in our hearts and minds as caregivers . Strategies to promote and enhance quality of life—even when the patient is close to
death—are the essential work of hospice teams . But we need to recognize that the life of a person with dementia has value and the treatment he/she receives can have significant impact on his/her life, for better or for worse.
Developing Specialized Dementia ServicesSome leading hospices have developed specialized programs for dementia patients, using a variety of individualized responses appropriate to their particular settings, often in partnership with local chapters of the Alzheimer’s Association . They have found tremendous responses to their specialized dementia programs in the elevated confidence and job satisfaction of their staff
and volunteers, in the reactions of long-term care facilities, community physicians and other partners, from the public and, most importantly, from patients with advanced dementia and their families .
One of the more impressive examples comes from Beacon Hospice, headquartered in Boston, Massachusetts, with 20 offices across New England. In 2005, the organization began to assess what its teams were doing to enhance quality of life and preserve dignity and personhood for end-stage dementia patients . It made a major commitment to identifying and sharing best practices with its staff . A one-year exploration of these issues by a work group of about 20 members—representing different office locations and disciplines—led to the development of a menu of optimal, evidence-based interventions.
The program is called Deep Harbors, inspired by Beacon Hospice’s lighthouse logo and the nautical theme in its publicity materials, reports CEO Betty Brennan, “We had the objective of developing a program that would create value for these patients, but also bring value to our own staff to feel more rewarded in providing the care . We recognized that it was difficult to measure the value of our services for these patients, but we went into this process saying there has to be something better .”
continued from previous page

NewsLine 45
Hospices need
to recognize that
their skills…can be
extremely valuable
to these patients
and families.
Certain topics came up again and again in explorations of the medical literature and interviews with local experts in dementia and geriatrics . Eventually it was necessary to distill this broad dialogue down to a manageable menu of interventions, chosen based on their validation in the literature, feasibility of implementation by the hospice, and opportunities to involve all members of the hospice team . The work group’s initial menu included four broad intervention areas aimed at enhancing quality of life for end-stage dementia patients and their families:
Music therapy•
Therapeutic touch•
Advanced feeding techniques•
Pre-death bereavement support•
A full-day training curriculum was developed to introduce the four intervention areas, along with a four-hour competency certification process. The hospice’s expert consultants helped teach the curriculum, which was offered at multiple locations and times for the convenience of staff. Required certification for all agency staff (450 at the time of roll-out in January 2006), including office staff, has been monitored for compliance . New hires are oriented to the same content .
Hospice of the Western Reserve (HWR) in Cleveland, Ohio, offers another example of an agency-wide response to advanced dementia . “In the Cleveland area, with its aging community, we were seeing our dementia numbers increase, particularly in our nursing home program,” reports Bridget Montana, HWR’s chief operating officer. “At the same time, our counselors were asking us how to make their visits with dementia patients richer and more engaging. They wanted our help, feeling that they weren’t contributing much of value .”
The agency convened a multi-disciplinary committee to study the issues of dementia care, and its members spent nine months attending professional conferences and reviewing hundreds of journal articles and other sources of expertise . As with Beacon Hospice, a few key themes emerged. These included:
Understanding and assessing pain in people • who can’t communicate verbally;
Distinguishing dementia from similar • symptoms of delirium, which may be reversible;
Finding ways to manage difficult • behaviors by non-pharmacological means; and
continued on next page
NewsLine 46
Placing a greater emphasis on making every • interaction with dementia patients deliberate and purposeful .
The planning group agreed that the human connection between hospice caregivers and patients with dementia is one of the most important aspects of the care provided . HWR’s philosophy of person-centered care affirms and honors the value of the person, regardless of severity of cognitive impairment . It also recognizes the need for creativity, flexibility, and attention to the emotional needs of patients .
“Based on what we learned from the literature, we developed a teaching curriculum for person-centered hospice care, regardless of whether the patient can communicate verbally,” Montana says . A basic four-hour course was offered to all clinical staff, with additional content for nurses. Patient care volunteers were trained in the basics of dementia and were given activity bags with
continued from previous page
Larry Beresford is a freelance writer who has authored numerous articles on end-of-life care. He can be reached at [email protected].
AD
VER
TIS
EMEN
T
sensory stimulation tools to help them in their work with patients . Expressive arts therapists offered in-services to hospice teams and shared a screening tool they developed to assist in determining when patients could benefit from art or music therapy .
These are just two of the programs highlighted in the 27-page NHPCO report—Caring for Persons with Alzheimer’s and Other Dementias . Members can download a copy of the report—free of charge . Visit nhpco.org/access and scroll to “Dementia .”
Hiring Coaches�e Studer Covenant Alliance is hiring coaches. Coaches bring a strong knowledge base of end-of-life care operations coupled with the ability to articulate the passion partners expect from the Studer Covenant Alliance. Our coaches function directly with our partner organizations. �ey work at the partner facility and assist in implementing our framework in order to achieve results. Travel is required. Management/leadership experience in hospice or palliative care is required. Excellent personal and public communication/grammar/speaking skills, the ability to relate well to people, strong organizational development, and training skills are a must. Strong computer skills with an emphasis on Microso� business applications is required. If you are interested in positively a�ecting end of life care organizations throughout the country, give us a call or send your resume to:
HR - Studer Covenant Alliance913 Gulf Breeze Parkway
Gulf Breeze, FL 32561Or preferably email to [email protected]

NewsLine 47
People and Places
continued on next page
VITAS Recognized for DiversityThe Greater Miami Society of Human Resource Management has awarded VITAS Innovative Hospice Care® (Miami, FL) its prestigious Diversity Award. The program was recognized for
the diversity of its workforce (57 percent of its workplace is comprised of minorities) as well as its longstanding commitment to serving patients of every age, race, gender, religion, sexual orientation and income level .
Cooney Named President-Elect of AAHPMGail Austin Cooney, MD, FAAHPM, has been named president-elect of the American Academy of Hospice and Palliative Medicine . The Academy is the professional organization for physicians committed to improving the quality of life for patients and families facing serious illness .
Cooney, who is the medical director at Hospice of Palm Beach County (West Palm Beach, FL), officially assumed the role during AAHPM’s Annual Assembly this past February . She will become the Academy’s president in February 2009 .
HospiceCare of Boulder and Broomfield Counties Awarded $50,000HospiceCare of Boulder and Broomfield Counties (Lafayette, CO) has received a $50,000 grant from the Amgen Foundation in support of its Bridge Palliative Home Health Program . The Bridge program was launched in 2006 to improve quality of life for people with end-stage disease .
Among its goals, the Amgen Foundation seeks to improve patient access to quality care and strengthen the communities where Amgen staff members live and work . Since 1991, the Foundation has made more than $85 million in grants to nonprofit organizations. Shown here: Amgen’s executive director of quality and its vice president of site operations with Kathy Coyne, director of fund development for HospiceCare, and Darla Schueth (far right), executive director of HospiceCare .
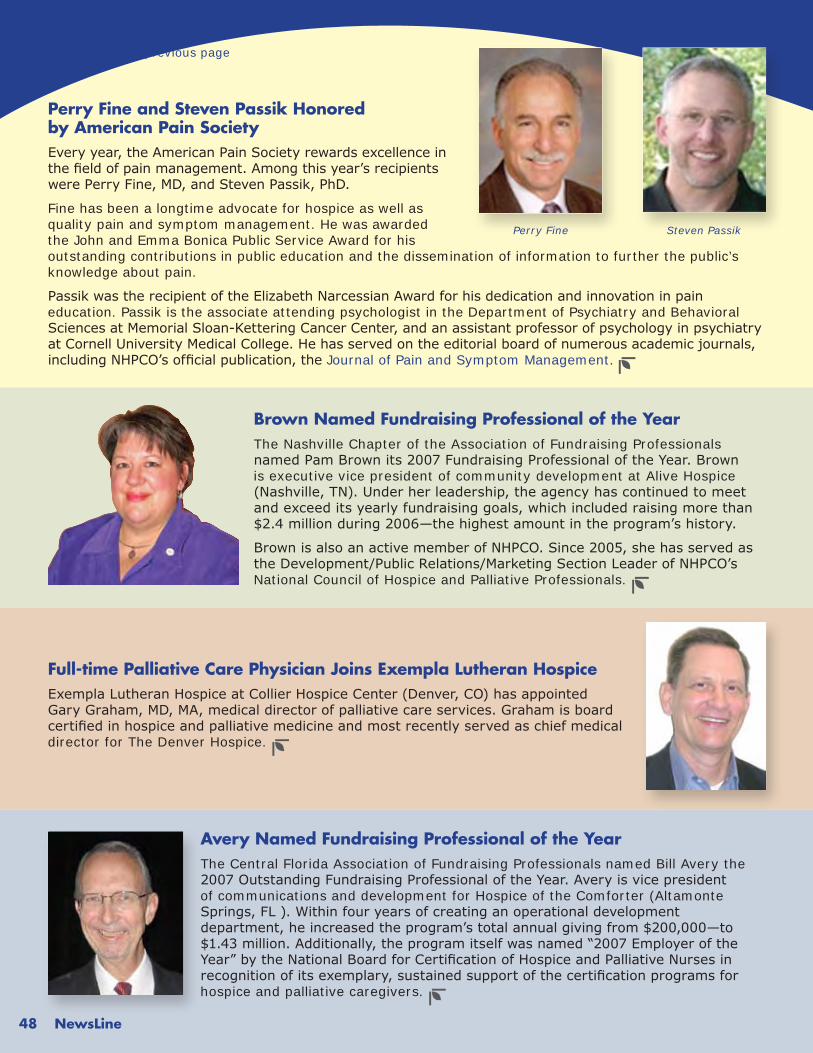
NewsLine 48
continued from previous page
Avery Named Fundraising Professional of the YearThe Central Florida Association of Fundraising Professionals named Bill Avery the 2007 Outstanding Fundraising Professional of the Year. Avery is vice president of communications and development for Hospice of the Comforter (Altamonte Springs, FL ). Within four years of creating an operational development department, he increased the program’s total annual giving from $200,000—to $1.43 million. Additionally, the program itself was named “2007 Employer of the Year” by the National Board for Certification of Hospice and Palliative Nurses in recognition of its exemplary, sustained support of the certification programs for hospice and palliative caregivers .
Full-time Palliative Care Physician Joins Exempla Lutheran HospiceExempla Lutheran Hospice at Collier Hospice Center (Denver, CO) has appointed Gary Graham, MD, MA, medical director of palliative care services. Graham is board certified in hospice and palliative medicine and most recently served as chief medical director for The Denver Hospice .
Perry Fine and Steven Passik Honored by American Pain SocietyEvery year, the American Pain Society rewards excellence in the field of pain management. Among this year’s recipients were Perry Fine, MD, and Steven Passik, PhD.
Fine has been a longtime advocate for hospice as well as quality pain and symptom management . He was awarded the John and Emma Bonica Public Service Award for his outstanding contributions in public education and the dissemination of information to further the public’s knowledge about pain .
Passik was the recipient of the Elizabeth Narcessian Award for his dedication and innovation in pain education . Passik is the associate attending psychologist in the Department of Psychiatry and Behavioral Sciences at Memorial Sloan-Kettering Cancer Center, and an assistant professor of psychology in psychiatry at Cornell University Medical College. He has served on the editorial board of numerous academic journals, including NHPCO’s official publication, the Journal of Pain and Symptom Management .
Brown Named Fundraising Professional of the YearThe Nashville Chapter of the Association of Fundraising Professionals named Pam Brown its 2007 Fundraising Professional of the Year. Brown is executive vice president of community development at Alive Hospice (Nashville, TN). Under her leadership, the agency has continued to meet and exceed its yearly fundraising goals, which included raising more than $2.4 million during 2006—the highest amount in the program’s history.
Brown is also an active member of NHPCO. Since 2005, she has served as the Development/Public Relations/Marketing Section Leader of NHPCO’s National Council of Hospice and Palliative Professionals .
Perry Fine Steven Passik
NewsLine 49
NHPCO’s Inclusion and Access Toolbox offers guidance—and resources—to help you meet the diverse cultural needs of your own community . The 116-page manual includes chapters on the:
Business Case for Inclusion• Community Presence• Marketing and Public Relations• Board Development• Administration• Quality Assessment and Performance Improvement• Workforce Development• Patient and Family Care Services• Plus—Appendices on Engagement Strategies, • Individual and Organization Self Assessments, and more.
Practical Guidance From Your ColleaguesYou will also find practical advice from hospice practitioners throughout the country on such issues as recruiting and retaining a diverse workforce, promoting your services to diverse communities, and providing culturally relevant care to patients and families .
The Toolbox is available as both a manual and CD through NHPCO’s Marketplace. Visit nhpco.org/marketplace (Item 821026; Member: $24.99). More details about this resource can also be found at nhpco .org/access .
A Closer Look at NHPCO’s
Inclusion and Access Toolbox
NHPCO is grateful
to the Aetna
Foundation, HCR
Manor Care
Foundation and
Heartland Hospice
for their generous
financial support of
the Inclusion and
Access Toolbox.

Dates to Remember
MarketplacePicks
NewsLine 50
This month we spotlight special items to help you serve patients with a range of non-cancer diagnoses .
A Caregiver’s Manual: Caring for a Loved One With Advanced Dementia By Family Centered Care Item: 821013, Member: $8.50
Expanding Access to Hospice Care for People With ALS
Item: 821011, Member: $14.99
Medical Guidelines for Determining Prognosis in Selected Non-Cancer Diseases Item: 713008, Member: $9.99
Palliative Care for Non-Cancer Patients
By Julia M . Addington-Hall and Irene J . Higginson
Item: 820431, Member: $63.60
The Family Guide to Alzheimer’s Disease: Five Volume DVD Set Item: 820866, Member: $108.80
Hospice Care for Patients with Advanced Progressive Dementia
Edited by Ladislav Volicer and Ann Hurley
Item: 820727, Member: $41.65
To order, visit Marketplace (nhpco.org/marketplace) or call 800/646-6460. Source Code: NL01.
NHPCO’s Audio Web Seminars
Interdisciplinary Topics: Second Thursday of the Month, 2:00 – 3:30 p.m. (EDT)
03/13/08—Supporting Patients and Families Toward Peaceful Life Closure
04/03/08—Just a Heartbeat Away: Caring for People with Defibrillators
Leadership Topics:
Fourth Tuesday of the Month, 2:00 – 3:30 p.m. (EDT)
03/25/08—Hot Regulatory Topics
04/22/08—Nurse Practitioners in Palliative Care and Hospice: The Business Case for Hiring a NP
NHPCO Conferences04/10 - 04/12/08—23rd Management and Leadership Conference, Advocacy in Action: Mobilizing People and Organizations to Lead Change Washington, DC
08/18 – 08/20/08—2nd National Conference on Access to Hospice and Palliative Care, Obstacles, Options and Opportunities Minneapolis, MN
Hospice MDP Two-Day Foundational Course04/08 - 04/09/08—Washington, DC*
05/13 – 05/14/08—Providence, RI Hosted by Home and Hospice Care of Rhode Island
*Additional MDP Modules will be available as MLC preconference seminars on April 9. For details, visit nhpco.org/mdp.

NewsLine 51
AD
VER
TIS
EMEN
T
Hospice Medical Director
Hospital employed Medical Director position with brand new 30-bed inpatient Hospice House in desirable 400,000 multi university South Carolina metro area associated with growing 319-bed health system.Palliative care experience.
$180K salary, bonus and benefits.
P: 800-831-5475F: 314-984-8246Email: [email protected]
Being Held in Conjunction with NHPCO’s 23rd Management and Leadership Conference
Save the Date...2008 National Hospice Foundation Gala
A Red Carpet AffairFriday, April 11, 2008 – Omni Shoreham Hotel, Washington, DC
Cocktails & Silent Auction - 6:30 PMDinner & Awards - 7:30 PM
Post Party Immediately FollowingMaster of Ceremonies - Bob Schieffer
CBS News Chief Washington Correspondent and Moderator, Face the Nation
HonoringMelissa Gilbert
Actor, Advocate, and President, Board of Directors, Children’s Hospiceand Palliative Care Coalition
Recipient of the Humanitarian Leadership Award and
Mary FisherArtist, Author and Speaker
Recipient of the Global Vision Award
Gala sponsorships are now available. For information contact NHF at 877/470-6472,or visit: www.nationalhospicefoundation.org.
Let Optimum Hospice Solutions help you achieve measurable outcomes and become the number one choice for end-of-life-care. OHS provides comprehensive solutions exclusively for hospice because we know the “business.”
Inpatient/Residential Feasibility StudiesCertificate of Need ApplicationsFull Range of Capital Campaign Services from Feasibility Studies to CompletionStrategic AuditsThe Watchman™ Program — The First Hospice Specific Faith-Based Marketing Strategy.
•••
••
(828) 247-0979(828) 429 - 4847
Do You Want to Be theNumber One Provider in
Your Service Area?
AD
VER
TIS
EMEN
T
AD
VER
TIS
EMEN
T

NewsLine 52 NewsLine52
AD
VER
TIS
EMEN
T
AD
VER
TIS
EMEN
T
866-263-3795 | www.corridorgroup.com
TCG can help you stay close to the issues most important
while achieving results that drive your success. Contact us at
866-263-3795 or visit www.corridorgroup.com.
Professional. Responsive. Expert.
RESULTS YOU CAN SEESince 1989, The Corridor Group, Inc. (TCG) has provided
the knowledge, resources and expertise to help clients be
resilient through times of change and growth.
Whether implementing quality initiatives, identifying an
executive candidate or fortifying education resources,
TCG is focused on helping you achieve your goals.
R your single source of contactTHE CORRIDOR GROUP, INC.

Choices®
A pioneer and leader in the American hospicemovement, and an advocate for the rights of theterminally ill, VITAS works to expand hospice access to population groups historically underserved by healthcare providers.
When life is limited, aging in place is what peoplewant. Our professional team of hospice expertshelps patients remain at home.
At VITAS, patients and families come first.
Wouldn't you choose America's hospice leader? Please call 305.350.6957 www.VITAS.com
NewsLine 5353NewsLine
AD
VER
TIS
EMEN
TAD
VER
TIS
EMEN
T
Specializes in the recruitment of hospice/homecareprofessionals.
Has filled hundreds of openings throughout theUnited States for both large and small
hospice/homecare organizations.
Works on a contingency basis, which means a feeis only payable if a candidate is hiredis only payable if a candidate is hired
as a direct result of our efforts.
HMR conducts searchesfor the following types of candidates:
Senior Level Managers
Administrator/General Manager
Director of Patient Care Services
Clinical Directors/Patient Care Managers
Hospice/Homecare Sales RepresentativesHospice/Homecare Sales Representatives
FOR MORE INFORMATIONPLEASE CONTACT:
Brian JohnsonDirector of Recruitment
[email protected], FloridaHollywood, Florida
(888) 818-6887
RECRUITING PROBLEMS?
NewsLine 54
Eternal Reefs creates permanent living cremation memorials that preserve, protect and enhance the
marine environment.
These living legacies benefit future generations.
www.eternalreefs.com 1-888-423-7333
Learn how you can help families create a memorial that will contribute to the environment and become a permanent home for life beneath the sea
- Contact us now for a free information kit -
AD
VER
TIS
EMEN
TAD
VER
TIS
EMEN
T
As NHPCO has previously reported, the final rule of the new hospice Conditions of Participation is expected to be published in
the Federal Register in May 2008. Will your hospice be ready?
As we begin the countdown to the new CoPs, you can begin preparing and planning for implementation success . It is expected that hospices will have 60 days from the date the final rule is published to become compliant with the
new regulations. There will be changes in the final hospice CoPs, but reviewing the proposed language now, and beginning the process of updating your organizational materials, will save you time and effort once the CoPs are final.
Follow the easy steps below to begin your plan for CoP success! And, be sure to use NHPCO’s “Checklist for Success” that is posted at the Regulatory & Compliance Center of our Web site (nhpco.org/regulatory) .
Look for more planning tips in next month’s NewsLine.
DON’T DELAY!CoPs on the Way!★ ★ ★ ★ ★ ★ ★ ★ ★ ★ ★ ★ ★ ★
★★★★★★★★★★★
★★★★★★★★★★
★★
★★★★★★★★★★
★★★★★★★★★★★★★★★★★★★
★★★
★★★★★★★★★★
★★
★★★★★★★★★★
★★★★★★★★★★★
Review your patient handout materials and update them with new information from the Patient Rights section of the proposed hospice CoPs (418.52).
Review your policies and procedures—incorporating language from these proposed hospice CoPs:
• Comprehensive assessment of the patient,
• IDG care planning & coordination of services, and
• Quality assessment and performance improvement.
Form a CoP implementation workgroup within your hospice organization—and involve field and office staff. You will have more success if staff members have a stake in the process.
Planning Tips for Success
NewsLine 55
Na
tiona
l Hosp
ice a
nd
Pa
lliativ
e C
are
Org
aniza
tion
1700 Diagonal R
oad • Suite 625
Alexandria, VA
22314
Non-Profit O
rg.U .S
. Postage PAID
PERM
ITN
O. 6
418M
errifield, VA
Please visit o
ur Web
site at n
hpco.o
rg.
This year’s National H
ospice Gala is set for Friday,
April 11—
in conjunction with N
HPC
O’s 23rd M
LC
in Washington, D
C. A
s part of the festivities, M
elissa Gilbert, board president of the C
hildren’s H
ospice and Palliative Care C
oalition, will be
honored with the 2008 H
umanitarian Leadership
Aw
ard for her advocacy efforts on behalf of pediatric palliative care . Join us for this special event. For details, see the display ad on page 51 or visit w
ww
.nationalhospicefoundation .org .
![Rasinski, Homan Biggs.515.106[1]](https://static.fdocuments.in/doc/165x107/55cf9ceb550346d033ab87b5/rasinski-homan-biggs5151061.jpg)