MANAGEMENT OF THE PATIENT WITH A LARYNGECTOMY€¦ · Web viewKnowledge and skills relating to...
17
MANAGEMENT OF THE PATIENT WITH A LARYNGECTOMY Learning objectives : Raise awareness of the specific needs of laryngectomy patients. Recognise the anatomical/airway differences in laryngectomy patients. Understand the basic methods for administration of oxygen therapy. Understand the appropriate methods for artificial ventilation in an emergency. Appreciate the need to adhere to the recommended safety measures. Introduction : A person with a laryngectomy has had the larynx (voice box) removed. This may be part of the treatment of cancer, burns, injury or infection. The nature of surgery means that there is no longer any connection between the oral/nasal passages and the trachea following the procedure. An artificial opening (stoma) is made. The upper portion of the trachea is brought to the stoma and secured, making a permanent pathway for air to get to the lungs. The patient will then breathe through this stoma for the rest of their lives. It is important to recognise that patients with a laryngectomy can only breathe through this stoma and CANNOT breathe through the mouth. Some patients admitted to ICU or ENT may have a tracheostomy tube in situ. Most patients admitted elsewhere are unlikely to have a 1
Transcript of MANAGEMENT OF THE PATIENT WITH A LARYNGECTOMY€¦ · Web viewKnowledge and skills relating to...

MANAGEMENT OF THE PATIENT WITH A LARYNGECTOMY
Learning objectives:
Raise awareness of the specific needs of laryngectomy patients.
Recognise the anatomical/airway differences in laryngectomy patients.
Understand the basic methods for administration of oxygen therapy.
Understand the appropriate methods for artificial ventilation in an emergency.
Appreciate the need to adhere to the recommended safety measures.
Introduction:
A person with a laryngectomy has had the larynx (voice box) removed. This may be part of the treatment of cancer, burns, injury or infection.
The nature of surgery means that there is no longer any connection between the oral/nasal passages and the trachea following the procedure.
An artificial opening (stoma) is made. The upper portion of the trachea is brought to the stoma and secured, making a permanent pathway for air to get to the lungs.
The patient will then breathe through this stoma for the rest of their lives. It is important to recognise that patients with a laryngectomy can only breathe through this stoma and CANNOT breathe through the mouth.
Some patients admitted to ICU or ENT may have a tracheostomy tube in situ. Most patients admitted elsewhere are unlikely to have a tracheostomy tube in situ but will always have a tracheostomy stoma or put simply a ‘hole in the neck’.
These individuals are known as neck breathers and require special care in an emergency.
These patients may be at risk when receiving emergency care if Staff are not aware of how to manage their respiratory needs.
The only way these patients can breathe or receive oxygen is through their stoma.
1

As a result of their altered anatomy and physiology, laryngectomees have particular needs in the event of requiring oxygen therapy, respiratory support or emergency care.
All staff involved in the patient’s care need to be aware of the differences in managing the patient’s airway.
Not only is this necessary during an emergency situation but it is equally important during what may be regarded as routine procedures, for example: oxygen administration or nebuliser therapy.
.
2
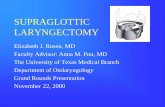
The picture opposite shows airflow after surgery:
The upper portion of the trachea is brought to the stoma and secured, making a permanent airway for air to get to the lungs.
The nature of the surgery means that there is no longer a direct connection between the oral/nasal passages and the trachea.
Post surgery, the patient can no longer breathe via the nose or the mouth.
The only way that the patient can now breathe is via the stoma that is formed in their neck.
The picture opposite shows airflow prior to surgery:
Air flows between the nose and the mouth and there is a direct passage towards the lungs.
Surgery involves removing the larynx and forming a stoma in the patient’s neck.

Knowledge and skills relating to airway management:
As a result of their altered anatomy and physiology, laryngectomees have particular needs in the event of requiring oxygen therapy, respiratory support or emergency care.
All staff involved in the patient’s care need to be aware of the differences in managing the patient’s airway.
Not only is this necessary during an emergency situation but it is equally important during what may be regarded as routine procedures, for example: oxygen administration or nebuliser therapy.
Laryngectomy patients have particular needs in the event of requiring emergency care as a result of their altered anatomy and physiology.
There are a few potential risks:
Inappropriate nose and mouth ventilation.
Tube difficulties
Problems with neck seals.
Failure to appreciate risks of crusting and mucous plugging of the stoma.
Possibility of speaking valve inhalation.
3

Trachoeostomy masks:
In the event that oxygen therapy is required, this must be humidified using a ‘tracheostomy’ mask that is applied directly over the stoma.
These masks are available from Ward 11 or Ward 3B.
ICU do not stock tracheostomy masks.
In the event that nebuliser therapy is required, the nebuliser chamber is attached to the tracheostomy mask using a t-piece connector.
The mask must not be used in patients with a cuffed tracheostomy tube.
Safety action notice 1998:
Relates to the use of tracheostomy masks and tracheostomy tubes.
Never use a tracheostomy mask on patients with a cuffed tracheostomy tube.
Rationale from adverse event:“ A tracheostomy mask was used to supply humidified oxygen to a spontaneously breathing patient with a cuffed tracheostomy tube. As water from the humidifier condensed in the loop of the corrugated tubing, its weight increased and the tracheostomy mask was pulled to one side. The soft moulding of the mask covered and occluded the tracheostomy tube, obstructing the patient’s airway”.
Ensure that the correct humidifier temperature is selected:
Press the button next to the tube and mask icons.
Confirm that the mask setting has been selected.
After sufficient warm-up time, the temperature that appears on the display should approximate 31°C.
Oxygen administration:
4
Never use face masks, nasal catheter or nasal prongs.
Never administer nebulisers via face-mask or mouthpiece.
Use a tracheostomy mask and apply directly over the stoma.
YES!

Reducing the risks of crusting and mucous plugging of the stoma:
Use humidified oxygen or air. Good positioning: sitting upright > 45° Encourage deep breathing and coughing exercises. Chest physiotherapy as appropriate. Suction of secretions may be required.
Patients with speaking valves:
If suctioning is required care should be taken when passing the suction catheter as the speaking valve may become dislodged.
Not all patients will present with speaking valves.
Some patients may regularly use the trachi-naze device:
The trachi-naze helps maintain airway heat, moisture and filtration. It is an HME (heat moisture exchanger) and offers similar principles to the ‘swedish nose’ device. It is designed to help reduce mucous production, coughing, tracheal irritation and crusting around
the stoma. The device must be removed if the patient requires humidified oxygen as excessive saturation
may increase the risk of airway occlusion.
Other protective devices:
Some patients may wear a ‘Buchanan protector’. This is an airway device designed to provide filtration and deliver efficient heat and moisture
exchange to the patient. This helps to maintain a healthy respiratory function in order to
avoid discomfort caused by coughing and chest infections.
The Buchanan protector needs to be removed:
When humidified oxygen is required. For access during emergency resuscitation.
5

Stoma-gastric tube:
A stoma-gastric tube is a term used to describe the insertion of a feeding tube through a laryngectomy stoma into the oesophagus, then fed down into the stomach.
A puncture is made (usually at the time of surgery) through the back wall of the trachea into the oesophagus. This is done in preparation for the fitting of a voice prosthesis. A patient would be discharged into the community with a stomagastric tube for 2 reasons:
1. The patient has developed a fistula post-op requiring a lengthened period of nil by mouth and needs to continue with enteral feeds.
2. The patient is eating and drinking orally but the stomagastric tube is maturing for fitting of their speaking valve.
Communication:6
Accidental dislodgement:
In the event that the stoma-gastric tube is accidentally dislodged contact the ENT team at the earliest opportunity. It is important that the stoma-gastric tube is reinserted as soon as possible as the fistula can close very quickly.

Patients have had their voice box removed so communication methods may vary with each patient.
Methods of communication:
All patients must have access to a call bell.
It may be necessary to communicate using pen and paper.
Some patients may have ‘voice’ valves (requires surgery) but this is not suitable for everyone.
Other patients may use an electronic device that is held against the neck and transmit sound through the tissues.
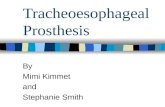
Medical alerts:
Laryngectomees may not be able to communicate even during a minor emergency.
Some patients may wear medical identification bracelets similar to those shown above.
Specially designed necklaces, medallions (or an alert card in the patient’s wallet) may also contain important information on medical conditions, allergies, medication and emergency contacts.
Laryngectomy alert information:
Every member of staff needs to be aware that the patient has had a laryngectomy and that the only way that the patient can breathe is via the stoma.
It should be clear from the bedside, handover, ward safety brief and the patient notes that the patient has had a laryngectomy.
Immediate bedside information includes the use of the bedside alert sign and alert sticker for observation chart.
Providing artificial ventilation in an emergency event:
7

ESSENTIAL BEDSIDE EQUIPMENT
8
Never apply the mask to the patient’s face.
In the event of a respiratory or cardiac arrest, artificial respiration can only be carried out via the stoma.
A small round mask (infant mask size 1) is preferable to an adult ambu mask as it provides a better seal around the stoma.
Intubation may be required and an endotracheal tube may need to be inserted directly via the stoma.
The patient must NOT be intubated via the mouth or the nose.
YES!

Patients that do NOT have a tracheostomy tube require access to the following equipment :
Oxygen supply. Wall suction. Suction apparatus. Resuscitator bag. Facemask: ambu-infant size 1. Yankaeur suction catheter. Single-use suction catheters: size 14FG. Protective wear: apron, gloves, full-face visor. Heated humidification may be required.
Remember to use:
Bedside alert sign. Alert sticker for observation chart.
Patients that have a tracheostomy tube in situ require access to the following equipment:
Oxygen supply. Wall suction. Suction apparatus. Resuscitator bag. Facemask: ambu-infant size 1. Tracheostomy tube: same size & one smaller size. Tracheostomy tube holder/velcro tapes. Yankaeur suction catheter. Closed suction system. Cuff pressure gauge Single-use suction catheters: size 14FG. Protective wear: apron, gloves, full-face visor. Heated humidification will be required.
PRACTICAL ASPECTS OF MAINTAINING AIRWAY SUPPORT IN AN EMERGENCY IN THE PATIENT WITH A LARYNGECTOMY
9
Recognise problems and seek immediate help
If any of the following occur seek urgent medical assistance and follow emergency guidelines as appropriate:
Patient expresses sudden difficulty in breathing. Patient suddenly becomes agitated or distressed. Cyanosis. Reduced oxygen saturations <90%. Reduced air entry or breath sounds. Tachypnoea/increased work of breathing with use of accessory muscles. Stridor or any abnormal breathing sounds. Inability to pass suction catheter in a patient that has a tracheostomy tube in situ.
Remember to use:
Bedside alert sign. Alert sticker for observation chart.

DIAL 2222 AND USE THE ABOVE EQUIPMENT.
Hand-ventilate the patient: at least 2 persons are required for the procedure:
MANAGEMENT OF SUSPECTED TUBE BLOCKAGE IN THE LARYNGECTOMY PATIENT WITH A TRACHEOSTOMY TUBE
10
Seek urgent assistance from a member of staff and dial 2222
Laryngectomy patients CANNOT be intubated via the mouth.
They must be ventilated via the laryngectomy stoma using bag-valve-mask.
The mask must be small: ambu-infant mask size 1 is used.
The attending Anaesthetist may attempt intubation via the stoma using an endotracheal tube.
Apply ambu mask over the stoma
Use ambu-infant mask size 1(available from Theatre)
Connect to resuscitator bag. Apply suction to the stoma if needed and apply ambu mask over the stoma.
Extend the patient’s neck and attempt to maintain a good seal
directly over the stoma.
Use both hands to hold the mask in place.
The 2nd person connects the resuscitator bag to the ambu mask and proceeds to hand-ventilate.
Check pulse and maintain BLS/ALS until medical help arrives

Suspicion that the tube is blocked?
Call for help
Apply suction via the tracheostomy tube.Remove inner liner and replace with the spare inner liner.
Attempt to hand ventilate via the tracheostomy tube.
IF THERE IS NO CHEST WALL MOVEMENT: DIAL 2222
Check pulse and follow BLS/ALS guidelines as appropriate
Remove velcro tapes, deflate the cuff and remove the tracheostomy tube.
DO NOT VENTILATE VIA MOUTH/NOSE
Anaesthetist may insert endotracheal tube via the stoma.
Laryngectomy patients CANNOT be intubated via the mouth.
NURSING STAFF CHECKLIST FOR MANAGING PATIENTS WITH A LARYNGECTOMY
REQUIRING HUMIDIFIED OXYGEN OR REQUIRING A TRACHEOSTOMY TUBE
11
LARYNGECTOMY PATIENTS CAN ONLY BREATHE THROUGH THE STOMA AND NOT VIA THE MOUTH
Extend the neck and check the stoma site for obvious blockages and remove.
Do NOT cover the stoma: the stoma must remain exposed.
Apply ambu-infant face mask size 1 over the stoma and hand-ventilate using bag-valve-mask.
Observe for bilateral chest wall movement.

• Highlight in the Safety Brief.
• Use the bedside alert sign and attach the laryngectomy alert sticker to the patient’s main observation chart.
• Refer to the laryngectomy guidelines in the Tracheostomy Care Manual.
• If the patient requires oxygen this must be humidified and delivered via a tracheostomy mask applied over the patient’s stoma. Never administer oxygen via nasal prongs or facemask. The patient can only receive oxygen via the stoma as they are ‘neck breathers’. Complete the section below at least every 4 hours. However, if the patient is sleeping or if conscious level is reduced the section below should be completed each hour.
Safety aspects of the patient receiving humidified oxygen Date Time Signature
Ensure that the humidifier hose tubing is emptied regularly so that heavy condensate does not drain in to the patient’s stoma.
Check that the weight of heavy condensate in the tubing does not pull on the tracheostomy mask.
Potentially, the weight of heavy condensate may pull the tracheostomy mask in such a way that it occludes the patient’s stoma.
0800120016002000
Midnight
Increased observation is required whilst the patient receives humidified oxygen. Hourly observation is required whilst the patient is sleeping or where the conscious level is reduced.
If the patient has an airway device similar to an HME e.g. trachi-naze: this should be removed whilst humidified oxygen is being administered. Such devices can be reinstated when humidified oxygen is no longer required.
0800120016002000
Midnight
When a tracheostomy mask is used (and provided that the patient does not have a tracheostomy tube in situ) ensure that the humidifier is programmed to mask mode.
The humidifier temperature should approximate 31°C when a tracheostomy mask is used.
Ensure the humidifier is kept away from the direction of direct draughts e.g. open window or cooling fans.
0800120016002000
Midnight
When a tracheostomy tube is in situ, ensure that the humidifier is programmed to tube mode.
Date Time Signature
080012001600
12
Affix patient identification label

The humidifier temperature should approximate 37°C when a tracheostomy tube is in situ.
2000Midnight
Ensure that the humidifier is safely mounted on a drip stand and do not allow the water chamber to run dry.
Check the remaining volume in the water bag at least every 4 hours. Change the bag if it appears to be near empty.
0800120016002000
Midnight
A tracheostomy tube may need to be inserted if the patient develops excessive secretions. If this is required an ICU Consultant will undertake the procedure. Any patient requiring a tracheostomy tube must be nursed in a designated area. These patients will also require a fully assembled trachi-case and this will be provided by the Outreach Team.
Patients with speaking valves : if suctioning is required care should be taken when passing the suction catheter as the speaking valve may become dislodged.
Patients requiring advanced respiratory support : e.g. non-invasive ventilation will require this management in ICU.
The Outreach Team will assess and review the patient once daily. Outreach will discontinue when the patient no longer requires oxygen therapy.
Any concerns must be communicated to the Outreach Team.
Devised by: Mairi MascarenhasApproved by: Dr J Whiteside
Reviewed: October 2013
13
LARYNGECTOMY: not for oral intubation
Follow the laryngectomy guidelines if breathing difficulties develop.
Bag-valve-mask to stoma/tracheostomy