Chronic Suppurative Otitis Media
22
Case Report Chronic Suppurative Otitis Media Presented by: Arjanto Ramadhian Siti Nashria Rusdhy Anindya Khairunnisa Zahra Lee Eng Siang Erlangga Prasamya Malina Raihan Nastiti Hemas Sanger Lintang Unggul Rini Moderator : dr. Ignatius Adhi Akuntanto Otorhinolaryngology and Head Neck Surgery Department Medical Faculty of GadjahMada University / Dr. Sardjito Hospital
-
Upload
andrei-rizqan-akmal -
Category
Documents
-
view
38 -
download
4
description
Chronic Suppurative Otitis Media
Transcript of Chronic Suppurative Otitis Media
Case Report
Chronic Suppurative Otitis Media
Presented by: Arjanto Ramadhian
Siti Nashria Rusdhy
Anindya Khairunnisa Zahra
Lee Eng Siang
Erlangga Prasamya
Malina Raihan
Nastiti Hemas Sanger
Lintang Unggul Rini
Moderator : dr. Ignatius Adhi Akuntanto
Otorhinolaryngology and Head Neck Surgery DepartmentMedical Faculty of GadjahMada University / Dr. Sardjito Hospital
Yogyakarta2011

CHAPTER I
INTRODUCTION
Chronic suppurative otitis media (CSOM) is a major cause of acquired hearing
impairment in children. It is also an important cause of preventable hearing loss, particularly in
developing countries. Chronic suppurative otitis media (CSOM) is the result of an initial episode
of acute otitis media and is characterized by a persistent discharge from the middle ear through a
tympanic perforation. Prevalence surveys, which vary widely in disease definition, sampling
methods, and methodologic quality, show that the global burden of illness from CSOM involves
65–330 million individuals with draining ears, 60% of whom (39–200 million) suffer from
significant hearing impairment. CSOM accounts for 28 000 deaths and a disease burden of over
2 million DALYs.1
Over 90% of the burden is borne by countries in the South-east Asia and Western Pacific
regions, Africa, and several ethnic minorities in the Pacific rim. Incidence of CSOM is higher in
developing countries because of poor socio-economic standards, poor nutrition and lack of health
education. It affects both sexes and all age groups.2 CSOM is uncommon in the Americas,
Europe, the Middle East, and Australia.1
2

CHAPTER II
LITERATURE REVIEW
II.A. ANATOMY OF THE MIDDLE EAR
The middle ear together with the Eustachian tube, aditus, antrum and mastoid air cells is
called the middle earcleft. It is lined by mucous membrane and filled with air. The middle ear
extends much beyond the limits of tympanic membrane which forms its lateral boundary and is
sometimes divided into (i) mesotympanum (lying opposite the pars tensa), (ii) epitympanum or
the attic (lying above the pars tensa but medial to Shrapnell'smembrane and the bony lateral attic
wall), (iii) hypotympanum (lying below the level of pars tensa).The portion of middle ear around
the tympanic orifice of the eustachian tube is sometimes called the protympanum. 2
Middle ear can be likened to a six-sided box with a roof, a floor, medial, lateral, anterior
and posterior walls. The roof is formed by a thin plate of bone called tegmen tympani. It also
extends posteriorly to form the roof of the aditus and antrum. It separates tympanic cavity from
the middle cranial fossa. 2
The floor is also a thin plate of bone which separates tympanic cavity from the jugular
bulb. The anterior wall has a thin plate of bone which separates the cavity from internal carotid
artery. It also has two openings; the lower one for the eustachian tube and the upper one for the
canal of tensor tympani muscle.
The posterior wall lies close to the mastoid air cells. It presents a bony projection called
the pyramid through the summit of which appears the tendon of the stapedius muscle to get
attachment to the neck of stapes. Aditus, an opening through which attic communicates with the
antrum, lies above the pyramid. Facial nerve runs in the posterior wall just behind the pyramid.
Facial recess or the posterior sinus is a depression in the posterior wall lateral to the pyramid. It
is bounded medially by the vertical part of the VIIth cranial nerve, laterally by the chorda tympani
and above, by the fossa incudis. Surgically, facial recess is important, as direct access can be
made through this into the middle ear without disturbing the posterior canal wall. 2
3
The medial wall is formed by the labyrinth. It presents a bulge called promontory which
is due to the basal coil of cochlea; oval window into which is fixed the footplate of stapes; round
window or the fenestra cochleae which is covered by the secondary tympanic membrane. Above
the oval window is the canal for facial nerve. Above the canal for facial nerve is the prominence
of lateral semicircular canal. Just anterior to the oval window, the medial wall presents a hook-
like projection called the processus cochleariformis. The tendon of tensor tympani takes a turn
here to get attachment to the neck of malleus. Medial to the pyramid is a deep recess called sinus
tympani. 2
The lateral wall is formed largely by the tympanic membrane and to a lesser extent by the
bony outer attic wall called the scutum. The tympanic membrane is semi-transparent and forms a
'window' into the middle ear. It is possible to see some structures of the middle ear through the
normal tympanic membrane, e.g. the long process of incus, incudostapedial joint and the round
window. 2
There are three ossicles in the middle ear- the malleus, incus and stapes. The malleus has
head, neck, handle (manubrium), a lateral and an anterior process. Head and neck of malleus lie
in the attic. Manubrium is embedded in the fibrous layer of the tympanic membrane. The lateral
process forms a knob-like projection on the outer surface of the tympanic membrane and gives
attachment to the anterior and posterior malleal (malleolar) folds. The incus has a body and a
short process, both of which lie in the attic, and a long process which hangs vertically and
attaches to the head of stapes. 2 The stapes has a head, neck, anterior and posterior crura and a
footplate. The footplate is held in the oval window by annular ligament. The ossicles conduct
sound energy from the tympanic membrane to the oval window and then to the inner ear fluid.
There are two muscles- tensor tympani and the stapedius; the former attaches to the neck
of malleus and tenses thetympanic membrane while the latter attaches to the neck of stapes and
helps to dampen very loud sounds thus preventing noise trauma to the inner ear. Stapedius is a
2nd arch muscle and is supplied by a branch of CN VII while tensor tympani develops from the 1st
arch and is suppliedby a branch of mandibular nerve (V3).2
Tympanic plexus lies on the promontory and is formed by (i) tympanic branch of
glossopharyngeal and (ii) sympathetic fibres from the plexus round the internal carotid artery.
4

Tympanic plexus supplies innervations to the medial surface of the tympanic membrane,
tympanic cavity, mastoid air cells and the bony eustachian tube. It also carries secretomotor
fibres for the parotid gland. Section of tympanicbranch of glossopharyngeal nerve can be carried
out inthe middle ear in cases of Frey's syndrome. 2
Chorda tympani nerve is a branch of the facial nerve which enters the middle ear through
posterior canaliculus, and runs on the medial surface of the tympanic membrane between the
handle of malleus and long process of incus, above the attachment of tendon of tensor tympani. It
carries taste from the anterior two-thirds of the tongue and supplies secretomotor fibres to the
submaxillary and sublingual salivary glands. 2
Mucous membrane of the nasopharynx is continuous with that of the middle ear, aditus,
antrum and the mastoid air cells. It wraps the middle ear structures-the ossicles, muscles,
ligaments, and nerves. Middle ear contains nothing but the air; all the structures lie outside the
mucous membrane. Histologically, the eustachian tube is lined by ciliated epithelium which is
pseudostratified columnar in the cartilaginous part, columnar in the bony part with several
mucous glands in the submucosa. Tympanic cavity is lined by ciliated columnar epithelium in its
anterior and inferior part which changes to cuboidal type in the posterior part. Epitympanum and
mastoid air cells are lined by flat, non-ciliated epithelium. 2
Middle ear is supplied by six arteries, out of which two are the main, i.e.(i) Anterior
tympanic branch of maxillary artery whichsupplies tympanic membrane.(ii) Stylomastoid branch
of posterior auricular artery which supplies middle ear and mastoid air cells. Four minor vessels
are: (i) Petrosal branch of middle meningeal artery (runs along greater petrosal nerve).(ii)
Superior tympanic branch of middle meningeal artery traversing along the canal for tensor
tympanimuscle. (iii) Branch of artery of pterygoid canal (runs along eustachian tube).(iv)
Tympanic branch of internal carotid. Veins drain into pterygoid venous plexus and superior
petrosal sinus.2
Lymphatics from the middle ear drain into retropharyngeal and parotid nodes while those
of the eustachian tube drain into retropharyngeal group.2
5

II.B. Chronic Suppurative Otitis Media
II.B.1. Definition
Chronic suppurative otitis media is defined as a chronic inflammation of the middle ear
and mastoid cavity, which presents with recurrent ear discharges or otorrhoea through a
tympanic perforation.1 Ear discharge may be continuous or intermittent and may be serous,
mucous or purulent.3 The point in time when AOM becomes CSOM is still controversial. The
WHO definition requires only 2 weeks of otorrhoea. Otolaryngologists tend to adopt a longer
duration, e.g. more than 3 months of active disease 1 or more than 2 months.3
II.B.2. Types of CSOM
Clinically, it is divided into two types:
1. Tubotympanic. Also called the safe or benign type; it involves the anteroinferior part of
middle ear cleft and is associated with a central perforation. There is no risk of serious
complications.
2. Atticoantral. Also called unsafe or dangerous type; it involves posterosuperior part of the cleft
(i.e. attic, antrum and mastoid) and is associated with an attic or a marginal perforation. The
disease is often associated with a bone-eroding process such as cholesteatoma, granulations or
osteitis. Risk of complications is high in this variety.2
II.B.3 Etiology
1. It is the sequelae of acute otitis media usually following exanthematous fever and
leaving behind a large central perforation. The perforation becomes permanent and permits
repeated infection from the external ear. Also the middle ear mucosa gets exposed to the
environment and sensitised to dust, pollen and other aeroallergens causing persistent
otorrhoea.
2. Ascending infections via the eustachian tube. Infection from tonsils, adenoids and
infected sinuses may be responsible for persistent or recurring otorrhoea.
3. Persistent mucoid otorrhoea is sometimes the result of allergy to ingestants such as
milk, eggs, fish, etc.
6

Most chronic ear drainage results from mixed infections with both aerobic and anaerobic
pathogens. Aerobic species include the Pseudomonas aeruginosa, Staph. aureus and
epidermidis, Proteus species, Klebsiella, and E. coli are isolated. Anaerobic species include:
Prevotella and Porphyromonas, anaerobic Streptococci, Bacteroides fragilis.
Predisposing factors include:
Acute otitis media Chronic otitis media Traumatic perforation Congenital cholesteatoma
II.B.4. Diagnosis
Diagnosis of CSOM is made based on clinical features and otolaryngologic exam,
especially the otoscopic exam. History-taking should be carried out to elicit the symptoms of
long-standing otorrhea. The ear is usually painless, except when eczematoid otitis interna
intervenes, significant intratemporal or intracranial complications occur, or when malignancy is
present. Vertigo, sensorineural hearing loss, facial paralysis may be present in erosion caused by
long standing cholesteatoma.
A history of previous ear discharge, especially when accompanied by episodes of colds,
sore throat, cough or some other symptoms of upper respiratory infection, should raise the
suspicion of CSOM. Patients usually report hearing loss as well.
Examination frequently reveals a tympanic membrane perforation with moderately
edematous middle ear mucosa and there may be associated granulation tissue in and around the
perforation. Specific attention should be paid to the presence or absence of cholesteatoma.
Cholesteatoma generally requires surgical treatment whereas CSOM without cholesteatoma can
be managed medically, including otomicroscopy and suctioning of secretions. When
cholesteatoma is present, a retraction pocket or squamous debris may present. In these cases,
there may also be evidence of bony external auditory canal erosion. Tuning forks exam will
confirm an associated conductive hearing loss in most cases unless a complication is present. 4
7

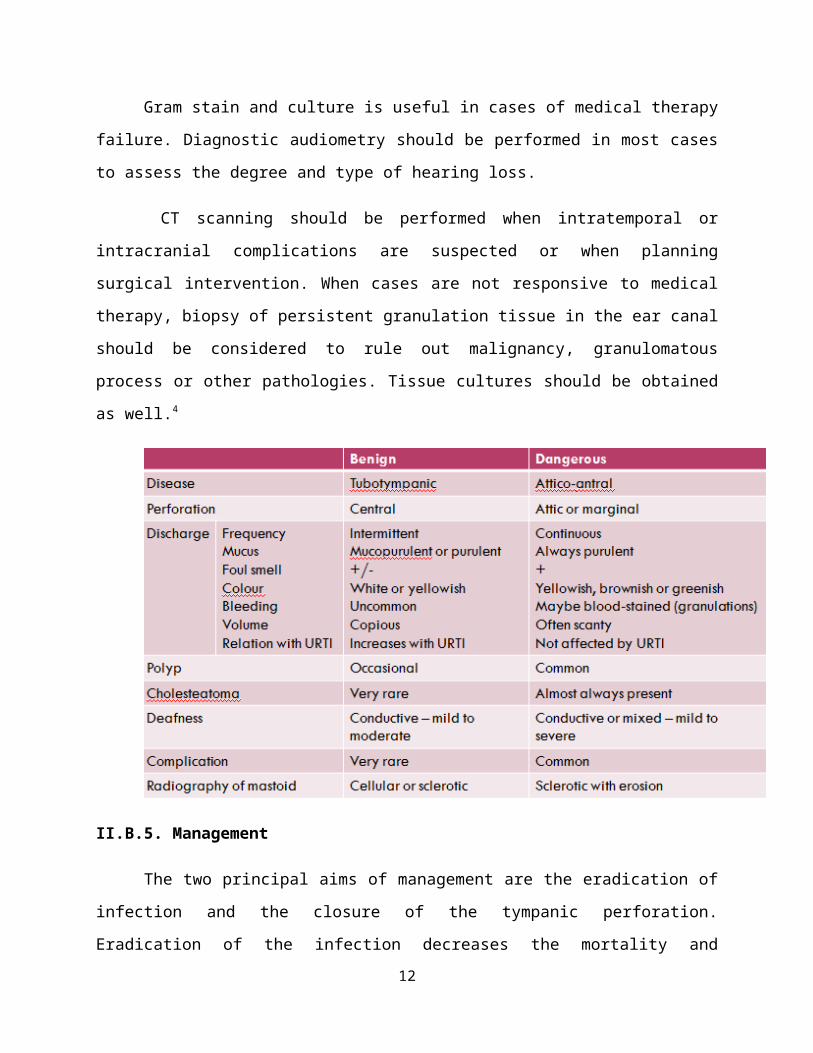
Gram stain and culture is useful in cases of medical therapy failure. Diagnostic
audiometry should be performed in most cases to assess the degree and type of hearing loss.
CT scanning should be performed when intratemporal or intracranial complications are
suspected or when planning surgical intervention. When cases are not responsive to medical
therapy, biopsy of persistent granulation tissue in the ear canal should be considered to rule out
malignancy, granulomatous process or other pathologies. Tissue cultures should be obtained as
well.4
II.B.5. Management
The two principal aims of management are the eradication of infection and the closure of
the tympanic perforation. Eradication of the infection decreases the mortality and morbidity
associated with severe CSOM and the closure of the tympanic perforation aims to relieve hearing
loss and to prevent microbial infection.
Patients with safe type CSOM can be managed by conservative medical treatment.
Among such patients, medical treatment can be aimed at control of infection and elimination of
ear discharge as short-term goals and eventual healing of the tympanic perforation and
improvement of hearing as ultimate goals.
8
Aural toilet
Aural toilet must be part of the standard medical treatment for CSOM. Cleaning the ear
of mucoid discharge could reduce, even if temporarily, the quantity of infected material from the
middle ear and could facilitate middle ear penetration of topical antimicrobials.1 Aural toilet is
best performed in the clinics by means of small suction tips, forceps and curettes to remove small
mucosal granulations from the middle ear.
Topical antiseptics
Topical antiseptics tended to be more effective than aural toilet alone in resolving
otorrhoea. 1 Topical antiseptics, include Zinc peroxide powder, Dilute acetic acid drops.
Antibiotics
Aural toilet combined with antimicrobial treatment is more effective than aural toilet alone.
The Cochrane review found that topical antibiotics were more effective than systemic antibiotics
in resolving otorrhoea and eradicating middle ear bacteria.
Topical quinolones were found to be better than topical non-quinolones.1 They represent the
first line drugs in treatment of CSOM.6 Ciprofloxacin otic drops and ophthalmic drops and
ofloxacin (Floxin) otic drops carry no risk of ototoxicity when they pass through a tympanic
perforation into the middle ear and are foudn to be safe and effective in children.
According to the WHO publication on CSOM1 combined oral-topical antibiotics were no
more effective than topical antibiotics alone.
Surgery
Polypectomy and granulomectomy may be performed to remove polyps and granuloma.
Tympanic perforations may be closed by placement of a graft on the inner surface of the ear
drum. Unsafe ears should undergo mastoidectomy which involves removing the mastoid air
cells, granulations and debris using bone drills and microsurgical instruments. Tympanoplasty
involves closure of the tympanic perforation by a soft tissue graft with or without reconstruction
of the ossicular chain.
9

Patient Education
Patients must be educated to prevent the entry of water or soap into the ear, particularly
during bathing. This can be done by plugging the ear with rubber or cotton wool covered with
vaseline.1 This also prevents soiling and irritating the skin surrounding the ear canal with
infected discharge.
10

CHAPTER III
CHAPTER III
CASE REPORT
Patient Identity
Name : Mrs. W. L.
Age : 32 years old
Address : Delanggu Klaten
Occupation : Housewife
Medical record number : 654763
A. Anamnesis
Chief complaint : Discharge from both ears.
History of present illness : Patient complains that there is a yellowish, thick, odorless
discharge issuing from both ears intermittently accompanied by a decrease in hearing in
both ears since around three months ago. The patient also complains of tinnitus and
occasional pain in the left ear. The patient denies suffering from any cold before the ear
discharge. The patient frequently cleans her ears using cotton buds.
History of previous illness : Previous history of ear ache and discharge. History of
hypertension, diabetes mellitus, heart disease, asthma and allergies were denied.
Family history of illness : A family history of hypertension, diabetes mellitus, heart
disease, asthma and allergies were denied.
Resume anamnesis : mucopurulent discharge (+), >3 months duration,
hearing loss (+), tinnitus (+)
B. Physical Examination
General status : compos mentis, good nutritional status
11
Vital sign:Blood pressure : 110/80 mmHgPulse : 84 x/minRespiratory Rate : 20 x/minTemp : 37 C
ENT Examination:Ear : mucopurulent discharge from AD/AS (+), AD/AS tympanic
membranes hyperemic (+), AD/AS cone of light (–), AD/AS central perforations (+)
Nose : within normal limits
Throat : within normal limits
Tuning fork exam:
AD AS
Rinne BC>AC BC>AC
Weber Lateralisation to the left ear
Schwabach Increased Increased
Result: suspected conductive hearing loss of both ears.
C. DiagnosisThe diagnosis of this patient is chronic suppurative otitis media AD/AS
D. ManagementBaquinor 2 x 4 drops both ears
Efedrin 2 x 1 tab
Ambroxol 3 x 1
E. ProblemRecurrency.
F. PlanningPatient education.
Follow up visit at the clinic in 5 days.
12

Culture sensitivity test.
13

CHAPTER IV
DISCUSSION
Based on the findings of the anamnesis and the physical examination the diagnosis of this
case is correct. The findings of mucopurulent, viscid otorrhea signify a discharge originating
from the middle ear. The duration of ear discharge of around 3 months with previous history of
ear infection signify the chronicity of the disease. On physical examination, central perforations
were found in both discharging ears. Thus the diagnosis of chronic suppurative otitis media can
be made.
The treatment, aural toilet followed by antibiotic ciprofloxacin is ideal for this patient.
Topical ciprofloxacin treatment was given which is ideal. As mentioned previously, studies have
found that topical application of antibiotics are more effective than systemic antibiotics.
Fluoroquinolones are effective against Pseudomonas and S. Aureus species which are commonly
found in CSOM. The use of decongestants is to help the function of the Eustachian tube in
clearing secretions from and aeration of the middle ear.
Patient education was adequate in that patient were educated to means must be taken to
prevent water from entering the ear during bathing. The patient was asked to follow up at the
hospital clinic in 5 days, when repeat aural toilet can be performed. The patient was also
educated to check up at the hospital whenever she suffers from an upper respiratory infection.
14

CHAPTER V
CONCLUSION
It has been reported, that a patient, female, 32 years old, based on history taking and
physical examination was diagnosed with chronic suppurative otitis media, benign type of both
ears. The patient was treated with ciprofloxacin ear drops, ephedrine, ambroxol and given
appropriate patient education.
15

CHAPTER VI
REFERENCES
1. World Health Organization. Chronic suppurative otitis media: Burden of Illness and Management Options. Geneva, Switzerland, 2004.
2. Dhingra PL. Diseases of Ear, Nose and Throat. 4th edition, Elsevier 2005: p 66-69.3. Soepardi E.A, Iskandar N, Bashiruddin J, Restuti R, Buku Ajar Ilmu Kesehatan Telinga
hidung tenggorok Kepala & Leher. Edisi Keenam. Balai Penerbit FK UI, 2007.4. Lee K.J. Essential otolaryngology Head and Neck Surgery. 9th edition, McGraw-Hill
2008: p 322-324.5. Baley BJ and Johnson JT, Head and Neck Surgery-Otolaryngology, 4th edition,
Lippincott Williams & Wilkins 2006.6. Fairbanks D. Pocket guide to Antimicrobial Therapy in Otolaryngology – Head and
Neck Surgery. 13th edition. American Academy of Otolaryngology—Head and Neck Surgery Foundation, Inc 2007: p 33.
16