Management of Biomechanical Complication of Implant-Supported Restoration of a Patient With...
11
J Oral Maxillofac Surg 67:178-188, 2009 Management of Biomechanical Complication of Implant-Supported Restoration of a Patient With Combination Syndrome: A Case Report Len Tolstunov, DDS* Combination syndrome (CS) is a pathologic condition of the stomatognathic system characterized by an edentulous maxilla with an atrophic anterior ridge, maxillary papillary hyperplasia, hypertrophic max- illary tuberosities, super-erupted mandibular anterior teeth, as well as atrophic mandibular posterior ridges. This condition can present a challenging situation to the clinician who needs to assemble evidence from all aspects of dentistry to formulate an appropriate treatment plan. One of the possible treatment choices for the fully edentulous patient with a CS is a full-arch implant-supported reconstruc- tion for both maxilla and mandible. The purpose of this study is to illustrate and discuss a biomechanical complication-fractured maxillary meso bar in a patient with CS, and to present a description of how this complex case was corrected and successfully completed. The analysis of implant-supported and implant- retained full arch restorations in edentulous patients with CS is presented and treatment recommenda- tions are given. A necessity of individualized approach for every implant reconstruction case, especially complicated with a CS, is suggested. © 2009 American Association of Oral and Maxillofacial Surgeons J Oral Maxillofac Surg 67:178-188, 2009 Combination syndrome (CS) is defined in the Journal of Prosthetic Dentistry 1 as: “. . . the characteristic fea- tures that occur when an edentulous maxilla is op- posed by natural mandibular anterior teeth, including loss of bone from the anterior portion of the maxillary ridge, overgrowth of the tuberosities, papillary hyper- plasia of the hard palate mucosa, extrusion of the lower anterior teeth, and loss of alveolar bone and ridge height beneath the posterior mandibular remov- able dental prosthesis bases—also called anterior hy- perfunction syndrome.” It is also defined in the glossary of implant terms in the Journal of Oral Implantology 2 as: “. . . a condi- tion caused by the presence of lower anterior teeth and an absence of the posteriors resulting in signifi- cant maxillary anterior alveolar resorption.” This oral condition is viewed as a rarely occurring syndrome with most signs and symptoms occurring in about 24% of the population wearing a maxillary complete denture opposing a bilateral distal extension partial denture. 3 There are few studies of long-term results or any association between implant outcomes and patient determinants. 4,5 Typically, this condition develops when there is a complete maxillary denture opposing a bilateral distal extension mandibular removable par- tial denture. 6 The anterior maxillary bone atrophies under chronic occlusal pressure from the remaining natural mandibular anterior teeth. Over time, this bone is replaced with fibrous tissue. Concomitantly, super-eruption of the mandibular anterior teeth oc- curs causing instability of the maxillary complete den- ture. An anterior mandibular alveolar bone may ac- company the super-erupted anterior teeth. Severe anterior maxillary resorption is a dominant feature of CS patients. These CS cases, as well as many other clinical cases of extensive 3D maxillary bone loss, have guided oral and maxillofacial surgeons and restorative dental practitioners toward the develop- ment of many innovative surgical and prosthetic tech- niques of correction of maxillary bone atrophy com- *Oral and Maxillofacial Surgery, Private Practice, San Francisco, CA; and Assistant Clinical Professor, Department of Oral and Max- illofacial Surgery, University of the Pacific School of Dentistry, San Francisco, CA. Address correspondence and reprint requests to Dr Tolstunov: One Daniel Burnham Ct, Suite 366C, San Francisco, CA 94109- 5460; e-mail: [email protected] © 2009 American Association of Oral and Maxillofacial Surgeons 0278-2391/09/6701-0027$34.00/0 doi:10.1016/j.joms.2008.09.013 178
-
Upload
marcelo-veliz-garcia -
Category
Documents
-
view
224 -
download
3
description
Sindrome combinacion
Transcript of Management of Biomechanical Complication of Implant-Supported Restoration of a Patient With...
-
J Oral Maxillofac Surg67:178-188, 2009
BmpaS
Renov,
n of, maxior tesituatan apith athis stnt wieted.s witch fo
2009 American Association of Oral and Maxillofacial SurgeonsJ Oral Maxillofac Surg 67:178-188, 2009
Coofturpolosridplalowridabpe
thetioan
*
CA
illo
Fra
On
546
2
027
doimbination syndrome (CS) is defined in the JournalProsthetic Dentistry1 as: . . . the characteristic fea-es that occur when an edentulous maxilla is op-sed by natural mandibular anterior teeth, includings of bone from the anterior portion of the maxillaryge, overgrowth of the tuberosities, papillary hyper-sia of the hard palate mucosa, extrusion of theer anterior teeth, and loss of alveolar bone andge height beneath the posterior mandibular remov-le dental prosthesis basesalso called anterior hy-rfunction syndrome.It is also defined in the glossary of implant terms inJournal of Oral Implantology2 as: . . . a condi-
n caused by the presence of lower anterior teethd an absence of the posteriors resulting in signifi-
cant maxillary anterior alveolar resorption. This oralcondition is viewed as a rarely occurring syndromewith most signs and symptoms occurring in about24% of the population wearing a maxillary completedenture opposing a bilateral distal extension partialdenture.3
There are few studies of long-term results or anyassociation between implant outcomes and patientdeterminants.4,5 Typically, this condition developswhen there is a complete maxillary denture opposinga bilateral distal extension mandibular removable par-tial denture.6 The anterior maxillary bone atrophiesunder chronic occlusal pressure from the remainingnatural mandibular anterior teeth. Over time, thisbone is replaced with fibrous tissue. Concomitantly,super-eruption of the mandibular anterior teeth oc-curs causing instability of the maxillary complete den-ture. An anterior mandibular alveolar bone may ac-company the super-erupted anterior teeth.
Severe anterior maxillary resorption is a dominantfeature of CS patients. These CS cases, as well as manyother clinical cases of extensive 3D maxillary boneloss, have guided oral and maxillofacial surgeons andrestorative dental practitioners toward the develop-ment of many innovative surgical and prosthetic tech-niques of correction of maxillary bone atrophy com-
Oral and Maxillofacial Surgery, Private Practice, San Francisco,
; and Assistant Clinical Professor, Department of Oral and Max-
facial Surgery, University of the Pacific School of Dentistry, San
ncisco, CA.
Address correspondence and reprint requests to Dr Tolstunov:
e Daniel Burnham Ct, Suite 366C, San Francisco, CA 94109-
0; e-mail: [email protected]
009 American Association of Oral and Maxillofacial Surgeons
8-2391/09/6701-0027$34.00/0
:10.1016/j.joms.2008.09.013
178Management ofComplication of I
Restoration ofCombination
A CaseLen Tolstu
Combination syndrome (CS) is a pathologic conditioedentulous maxilla with an atrophic anterior ridgeillary tuberosities, super-erupted mandibular anterridges. This condition can present a challengingevidence from all aspects of dentistry to formulatetreatment choices for the fully edentulous patient wtion for both maxilla and mandible. The purpose ofcomplication-fractured maxillary meso bar in a patiecomplex case was corrected and successfully complretained full arch restorations in edentulous patienttions are given. A necessity of individualized approacomplicated with a CS, is suggested.iomechanicallant-SupportedPatient Withyndrome:portDDS*
the stomatognathic system characterized by anillary papillary hyperplasia, hypertrophic max-eth, as well as atrophic mandibular posteriorion to the clinician who needs to assemblepropriate treatment plan. One of the possibleCS is a full-arch implant-supported reconstruc-udy is to illustrate and discuss a biomechanicalth CS, and to present a description of how thisThe analysis of implant-supported and implant-h CS is presented and treatment recommenda-r every implant reconstruction case, especially
-
binimrecillagebillardeialedgramacobonaingphplawiplaimpredillaplatiotheanplamadibin
beedcoplabetheveofprdisCSthebo
anmabaimtoimcaedbio
metrebioch
Ca
surplalarch(exyeyemahewitieanShhetheoradeetaovplehygromathebebareqpo
FIGtati
Len
LEN TOLSTUNOV 179ed with immediate or delayed placement of dentalplants. Based on literature review, some of theseonstructive approaches for the compromised max-ry bone include: vertical alveolar distraction osteo-nesis,7,8 horizontal distraction in combination withateral sinus lift/bone grafting procedure,9,10 maxil-y ridge-splitting techniques followed by immediatental implants,11 autogenous iliac crest12 and calvar-bone grafting,13 reconstruction of the resorbedentulous maxilla with autogenous rib grafts,14 tibialfting for maxillary bone loss,15 treatment of severexillary atrophy with vascularized free fibula flap inmbination with dental implants,16 interpositionalne grafting with Le Fort I osteotomy,17 orthog-thic surgery with or without onlay bone graft-,18,19 use of the osseoinductive effect of bone mor-ogenic protein within endosseous dental implantsced in the maxilla,20 zygomatic implants with orthout sinus lift/bone graft,21,22 pterygomaxillary im-nts combined with zygomatic and conventionalplants,23 the Marius implant bridge for the surgical-osthetic rehabilitation of the resorbed completelyentulous maxilla with 6 implants,24 All-on-4 max-ry edentulous rehabilitation with 4 strategicallyced and immediately-loaded implants,25 combina-n of short implants and osteotome technique forposterior maxilla,26 use of transitional implants
d bone grafting before placement of definitive im-nts,27 optimal use of the anatomic features of thexillary arch with tilted implants,28 use of transman-ular implant,29 Tatum custom ramus frame implantCS patients,30 and many others.Osseointegrated implant-supported prostheses haveen advocated as an excellent treatment option forentulous jaws.31 In clinical cases of CS with ampromised atrophic maxillary bone, dental im-nt-retained and supported prostheses have alsocome a highly successful and predictable pros-tic treatment option.32,33 However, residual al-olar ridge width may decrease in time regardlessthe type of prosthesis.34-37 An implant-supportedosthetic treatment can change the occlusal forcetribution that induced an osseous pattern of the. This decrease of traumatic overload or stress tounderlying bone may attenuate any further
ne resorption.Prevention of loss of posterior occlusion and avoid-ce of anterior hyperfunction are considered thein treatment approaches of the CS. An implant-sed reconstruction of the mandibular arch withplant stabilization of the maxillary arch consideredbe a modern maxillomandibular surgical-prostheticplant therapy for many CS cases.38 The followingse report shows an implant-supported treatment ofentulous CS patient. It describes the encounteredmechanical complication (fracture of maxillaryso bar), the modification and correction of theatment, the discussion on the management of thismechanical complication, and optimal treatmentoices for this complex case.
se Report
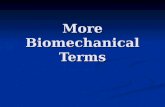
A 65-year-old healthy female presented to our oralgery practice for implant treatment. Her chief com-ints were inadequate function of her existing maxil-y and mandibular complete dentures, and inability toew comfortably and smile. She became edentulouscept for the mandibular anterior teeth) about 20ars prior. The lower front teeth remained for 10 morears and were eventually extracted (except for thendibular right canine). The patient mentioned thatr facial features have changed over the last 20 yearsth her lower jaw becoming more pronounced. Pa-nt has had 2 sets of unsuccessful complete maxillaryd mandibular dentures made over the last 10 years.e was somewhat informed about implant dentistry byr general dentist and desired implant-supported pros-ses. Her medical history was unremarkable. A clinicall examination of the patient with both completentures showed the patient with pseudo Class III skel-l maxillomandibular relationship (Fig 1) that wasercorrected by Class I occlusal pattern of her com-te dentures, an edentulous maxilla with papillaryperplasia of the anterior hard palate mucosa, over-wth of maxillary tuberosities, hypertrophy of thendibular alveolar ridge with single remaining root ofmandibular right canine, and loss of the ridge height
neath the posterior mandibular removable dentureses. Complete dentures were severely unstable anduired significant soft tissue (cheeks and tongue) sup-rt to stay in place.
URE 1. Three-quarter lower facial view of the patient at presen-on. Skeletal pseudo Class III maxillomandibular relationship.
Tolstunov. CS and Implants. J Oral Maxillofac Surg 2009.
-
osetatio2).waaptom
PrRa
tip(Fi3Dthaboatradplasevtrofordibalv
osprthisuplario
Di
no
FIGviethe
Len
FIGpos
Len
FIGshopre
Len
FIGviebas
Len
180 CS AND IMPLANTSA screening panoramic radiograph showed anseous pattern suggestive of pseudo Class III skel-l maxillomandibular relationship and CS condi-n with severe atrophy of anterior premaxilla (FigMounted study casts were made. A diagnosticx-up of proposed dentures was made to show anpropriate tooth position. A definitive computedography (CT) radiographic survey was ordered.
eoperative Computerizeddiographic Scan Analysis
The computerized tomographic scan showed mul-le anatomic features important for considerationgs 3-6). The anterior maxilla was severely atrophic, especially in the buccal-palatal dimension (width)t precluded an implant insertion without majorne grafting. The posterior maxilla had moderateophy in the buccal-palatal dimension and had anequate height and overall bone volume for an im-nt placement. The mandible was moderately toerely atrophic in the posterior and slightly hyper-phic in the anterior regions. Bilaterally, the mentalamina opened on the alveolar crest and the man-ular canal was proximate to the surface of theeolar crest. These features presented a challenging
URE 3. Computerized tomographic NewTom scan (panoramicw) shows atrophy of the anterior maxillary ridge extending tofirst premolar area bilaterally.
Tolstunov. CS and Implants. J Oral Maxillofac Surg 2009.
URE 2. Panoramic radiograph shows mandibular atrophicterior edentulous ridges and moderate anterior hypertrophy.
Tolstunov. CS and Implants. J Oral Maxillofac Surg 2009.seous terrain and required advanced surgical andosthetic skills for an adequate implant treatment ofs patient. A careful 3D analysis of CT sectionsggested that bone volume was satisfactory for im-nt placement in the anterior mandible and poste-r maxilla with large bone grafting.
agnosis
Based on clinical and radiographic findings a diag-sis was made. It included pseudo Class III skeletal
URE 4. Computerized tomographic NewTom scan (axial view)ws atrophy of the anterior maxillary ridge extending to the firstmolar area bilaterally.
Tolstunov. CS and Implants. J Oral Maxillofac Surg 2009.
URE 5. Computerized tomographic NewTom scan (sagittalw) shows severe atrophy of the anterior maxillary ridge to theel bone.
Tolstunov. CS and Implants. J Oral Maxillofac Surg 2009.
-
ma1-6matrocietur
Tr
Shedaskpr
theplaabpapoincarcforvaimwiofpareaplaretea
chhismipapr
plamadibwifix
scaanmiatinmmthepommAmanlatrigosThen
O
paprthewicothecis17(Ome(sisevaretiocu
(Bsitmmlinaumaboba
FIGphi
Len
LEN TOLSTUNOV 181xillomandibular relationship in the CS patient (Figs), severe 3D anterior maxillary atrophy, relativendibular prognathism with anterior alveolar hyper-phy, complete edentualism with functionally defi-nt and unstable full maxillary and mandibular den-es, and a Class I denture relationship.
eatment Plan
Treatment options were discussed with the patient.e declined proposed iliac crest bone grafting forentulous premaxilla requiring hospitalization buted for upper and lower jaw implant-supportedostheses.A discussion with the patient focused on 2 issues:
differences between implant-retained and im-nt-supported restorations, and benefits of remov-le versus fixed prostheses. During the discussiontient understood the advantages of implant-sup-rted full-arch restoration (removable or fixed) thatluded proper bone loading throughout the dentalh and adequate bone maintenance with less needfuture adjustments and relines. The bone preser-
tion principle of implant-supported prosthesis wasportant for the patient because she was concernedth already existing severe bone loss in certain areasher jaws. The patient also wished to have herlate finally exposed (freed) for comfort and tastesons. Thus, the patient selected a removable im-nt-supported maxillary prosthesis with clip-barention that would give her hygienic access forse of cleaning and desired comfort, and for psy-
URE 6. Computerized tomographic scan slice showing atro-c posterior mandible.
Tolstunov. CS and Implants. J Oral Maxillofac Surg 2009.ological reasons (eg, the patient with a previoustory of maxillary removable denture did notnd a removable prosthesis). In the lower jaw, thetient chose to have a fixed implant-supportedosthesis.The patients treatment plan included a surgicalcement of 6 endosseous implants into posteriorxilla and 5 endosseous implants into anterior man-le followed by a restorative prosthetic treatmentth an implant-supported removable maxillary and aed mandibular prostheses.Detailed measurements of available bone on CTn guided an implant insertion. In the maxilla, anterior maxillary atrophy extended 17 mm from thedline bilaterally. An implant position was planned20 mm, 27 mm, and 45 mm mark on each side andproximity to maxillary sinuses. In the mandible, 20of alveolar length was measured on CT scan frommidline to mental foramina bilaterally. An implant
sition was considered at the midline (0 mm), 10, and 17 mm mark from the midline on each side.axillary implant placement was deemed to requireincrease of the alveolar bone volume by a direct oreral approach for the sinus lift procedure on theht side and an indirect or crestal approach for theteotome subantral augmentation on the left side.e different approaches were based on the differ-ces in radiographic bone volume at each side.
perative Phase
The surgical procedure was carried out in an out-tient surgical suite with intravenous sedation. Theocedure started from the right maxilla, followed byleft maxilla. After administering a local anesthesia
th lidocaine with epinephrine, a full thickness mu-periosteal flap was raised from the canine area tomaxillary tuberosity with vestibular releasing in-
ions. A lateral osseous window was created with a03 burr (SS White) and #6 round diamond bursteoMed, Addison, TX) exposing the Schneiderianmbrane of the antrum to visualize the superiornus) surface of the atrophic alveolar ridge. Theerely atrophic ridge mesial to the first premolara was directly observed. The separation and eleva-n of the membrane was accomplished with Tatumrettes (Tatum Dental, St Petersburg, FL).3i Osseotite Certain internal connection implantsiomet 3i, Palm Beach Gardens, FL) were placed ates 2, 4, and 5 using a surgical guide at positions 45, 27 mm, and 20 mm, respectively, from the mid-
e of the maxilla (Table 1). Approximately 3 cc oftogenous bone was then harvested from the rightxillary tuberosity and mixed with a particulatene allograft material (Puros, Zimmer Dental, Carls-d, CA) to make about 6 cc. The right sinus was then
-
auTasintheturScthethemaouancregracetatsuteoplathe27respliwaradprpaallthe
ulamithewasuacosusmiCtheatgu
of(0Hetimthe
3-micaDemamesiapeapthe
atefixthetheimrecabtritra
allo
T TECHN
LoM
autogeautogeautoge
Len
182 CS AND IMPLANTSgmented with this mixture. A collagen tape (Colla-pe, Zimmer Dental) material was placed over theus window and a water tight primary closure offlap was achieved with a horizontal mattress su-
ing technique with 4-0 chromic gut sutures (Henryhein, Melville, NY). Attention was then turned toleft side. A full-thickness flap was raised to identifyosseous anatomy. Proposed implant sites were
rked with a round burr and an osteotomy carriedt with an initial 2-mm twist drill. The left maxillad sinus was surgically treated from an alveolar ridgestal approach (osteotome technique) and a xeno-ft material (Bio-Oss, Osteohealth, Luitpold Pharma-uticals, Shirley, NY) was used for subantral augmen-ion. Each osteotomy site was expanded withccessive Summers type round end-cupped os-tomes. 3i Osseotite Certain implants wereced at sites 12, 13, and 15 using a surgical guide atsame (similar to the right side) positions 45 mm,mm, and 20 mm from the midline of the maxilla,pectively (Table 1). A primary closure was accom-shed with 4-0 chromic gut sutures. The left sides treated with a crestal approach because of aiographically greater available bone volumeesent for initial implant stability. A postoperativenoramic radiograph confirmed good placement of6 implants. The patient tolerated the sedation andprocedure well.
Three weeks later the patient underwent mandib-r implant surgery under intravenous sedation. Adcrestal full thickness arch length flap was raised inanterior mandible. The mandibular right canine
s extracted. The exposed hypertrophic ridge wasrgically reduced by about 5 mm with a large roundrylic/bone bur (OsteoMed) until a 6-mm wide, flatseous surface was obtained. A surgical guide wased to locate the 5 proposed implant sites. Osteoto-es were carried out for each site. All of the 3iertain internal connection implants were placed inusual manner recommended by the manufacturersites 21, 22, midline, 27, and 28 using a surgicalide at positions 17 mm and 10 mm from the midline
able 1. MAXILLA: IMPLANT POSITION, SIZE, SURGICAL
cationaxilla
Distance FromMidline (mm)
Implant(Biomet 3i)
Right side2 45 4 13 Puros 4 27 4 10 Puros 5 20 4 13 Puros
Left side12 20 4 11.5 Bio-Oss13 27 4 8.5 Bio-Oss15 45 5 11.5 Bio-Oss
Tolstunov. CS and Implants. J Oral Maxillofac Surg 2009.the mandibular ridge bilaterally and at the midlinemm) (Table 2). No bone graft material was placed.aling abutments (stage 2) were placed at the samee and the flaps were mobilized and sutured aroundabutments with 4-0 chromic gut sutures.
The patient wore existing complete dentures foronth healing phase. These dentures were period-lly adjusted and relined with a soft liner (CoeSoft,ntsply, Philadelphia, PA) during this phase. Thexillary stage 2 with placement of healing abut-nts was done 6 months later under local anesthe-. All 6 maxillary and 5 mandibular implants ap-ared to be successfully osseointegrated. Afterpropriate healing, the patient was dismissed intocare of the restorative dentist.
RESTORATIVE PHASE
Following the stage 2 surgery, the clinician evalu-s whether to construct implant prosthesis on thetures directly or connect multiunit abutments tofixtures and construct the prosthesis on them. Incase presented, both mandibular and maxillary
plant-supported prostheses were constructed di-tly on implant fixtures using UCLA permanentutments. Study casts, an acrylic base to record cen-c relation, and custom impression trays for an openy technique were used.In the maxilla, a platinum-palladium-gold (type IV)y single meso bar was cast to the abutments (Fig 7).
IQUE, AND BONE GRAFT USED
Graft-Mix Material Sinus Lift
nous (maxillary tuberosity) bone Direct (lateral)nous bone Directnous bone Direct
Indirect (crestal)IndirectIndirect
able 2. MANDIBLE: IMPLANT POSITION, SIZE, ANDISTANCE FROM THE MIDLINE
cationndible
Distance FromMidline (mm)
Implant(Biomet 3i)
21 17 4 1322 10 4 13idline 0 4 1527 10 4 1528 17 4 13
Tolstunov. CS and Implants. J Oral Maxillofac Surg 2009.TD
LoMa
M
Len
-
BethetheDuinsmaadattasde
meanthebil
thelatintsuan
Atanremwaad
Ca
antiethesenframieryare(dumi
ca
FIGwit
Len
FIGme
Len
Len
FIG
Len
LEN TOLSTUNOV 183cause of the length of the bar, it was separated inmid arch and cast as 2 pieces. The 2 segments ofbar were then tried against the implants and set inralay for soldering. Another try-in was done toure a passive fit. For an additional retention of thexillary overdenture, a milling machine was used tod a 4 taper to the meso bar. Four Hader-type clipachment retainers (CM Gold Riders Co) were usedmain retentive components. The denture was thenlivered to the patient.In the mandible, the passive fit of 5 UCLA abut-nts was confirmed radiographically. The acrylicd teeth of the prosthesis were fully supported byframework and extended to the first molar area
aterally.The mandibular prosthesis was delivered first andmaxillary overdenture prosthesis was delivered
er (Figs 8-11). All implant abutments were torquedo position at 20 Ncm. A vertical dimension, lippport, and speech function with regard to fricativesd sibilants were observed and deemed acceptable.
URE 7. Maxillary anteriorly cantilevered, cross-arched singleso bar based on 3 posterior implants on each side.
Tolstunov. CS and Implants. J Oral Maxillofac Surg 2009.
FIGURE 8. Intaglio of the maxillary clip-bar overdenture.
Tolstunov. CS and Implants. J Oral Maxillofac Surg 2009.delivery, the patient was instructed for functiond care (Fig 12). Initially, she was not able to easilyove the maxillary overdenture, so 1 clip assemblys removed (3 clips were remaining) to provideequate retention (Fig 8).
se Completion
About 9 months after the delivery of both maxillaryd mandibular implant-supported prostheses, the pa-nt noticed discomfort in the anterior maxilla underbar that slowly progressed. When patient pre-ted to the office of the general practitioner thecture of the single maxillary meso bar left off thedline was evident. An examination also showed anthema of the premaxillary gingiva underneath thea of the fracture. A bar fractured at the solder jointe to the length of the bar, it was separated in thed arch, cast as 2 pieces, and then soldered).A traumatic overload and fracture of the anteriorlyntilevered maxillary single meso bar underneath
URE 10. Panoramic radiograph of the restorative treatmenth the single meso bar.
Tolstunov. CS and Implants. J Oral Maxillofac Surg 2009.
URE 9. Intaglio of the screw-retained mandibular prosthesis.
Tolstunov. CS and Implants. J Oral Maxillofac Surg 2009.
-
thecotoentersalancomofunfin
Di
jawmashofpode
Heteepegioocuasitpleexmoim
FIGsup
Len
FIGI oc
Len
FIGis b
Len
F
Len
184 CS AND IMPLANTSimplant-supported prosthesis, the biomechanicalmplication, was diagnosed. The decision was madehave 2 separate posterior maxillary bars instead tocourage posterior functional load and free the an-ior resorbed maxilla from the heavy anterior occlu-stress. After this approach, the condition of the
terior maxilla normalized, and function and patientmfort improved (Figs 13-17). Over the following 24nths, the patient has been very comfortable withction, esthetics, phonetics, and comfort of theal upper and lower implant prostheses.
scussion
An atrophy and hypertrophy of different regions ofs in many CS cases derive from abnormal trau-tic occlusal forces that over time unfavorablyape the alveolar bone.39 The progressive resorptionthe posterior mandibular bone causes a loss ofsterior occlusion with opposing maxillary posteriornture teeth, a key initiating feature of CS.35,40
URE 12. Pleasing lower facial proportions and satisfactory lipport and esthetics on delivery of the prostheses.
Tolstunov. CS and Implants. J Oral Maxillofac Surg 2009.
URE 11. Both prostheses in centric relation at delivery. Classclusal relationship.
Tolstunov. CS and Implants. J Oral Maxillofac Surg 2009.avy masticatory load from remaining lower anteriorth transferred to the anterior region (anterior hy-rfunction) leads to CS changes. The resultant re-ns of bone deficiency and overgrowth, as well asclusal plane discrepancy present a challenging sit-tion to the clinician.41 The most common clinicaluation of CS is encountered when there is a com-te maxillary denture opposing a bilateral distaltension mandibular removable partial denture. Thest common prosthetic treatment with endosseousplants for these patients is to construct a mandib-
URE 13. Maxillary 2 posterior meso bars (split-bar), each barased on 3 implants on each side.
Tolstunov. CS and Implants. J Oral Maxillofac Surg 2009.
IGURE 14. Left maxillary meso bar connecting 3 implants.
Tolstunov. CS and Implants. J Oral Maxillofac Surg 2009.
-
ulalinforstathestaof
casigthe
ninlommawabodupatioClatotionatieocmaturabpatio
beprmequrioevgra(Averemtyptiooracepranca
F
Len
FIGwit
Len
FIGthesatma
Len
LEN TOLSTUNOV 185r implant-supported prosthesis and to redo or re-e a maxillary conventional complete denture. Un-tunately, in many cases, if some form of implantbilization of the maxillary arch is not considered,maxillary bone resorption continues.42 An ideal
bilization of the same caliber requires placementdental implants in both maxilla and mandible.The 2-jaw implant rehabilitation in advanced CSses is one of the most difficult to treat and requiresnificant expertise of the entire dental team. One ofimportant factors in prosthetic treatment plan-
IGURE 15. Right maxillary meso bar connecting 3 implants.
Tolstunov. CS and Implants. J Oral Maxillofac Surg 2009.
URE 16. Panoramic radiograph of the completed treatmenth 2 maxillary posterior meso bars.
Tolstunov. CS and Implants. J Oral Maxillofac Surg 2009.g of edentulous implant patients is skeletal maxil-andibular relationship. In this case, generalizedxillary atrophy caused by complete edentulisms exacerbated by an advanced 3D premaxillaryne loss caused by the CS. Both factors (resorptione to edentulism and resorption due to CS) led to thetients pronounced loss of maxillary bone in rela-n to the mandible. Initially (naturally) skeletalss I patients jaw relationship has changed slowlyskeletal Class III pseudo maxillomandibular rela-nships with severely resorbed maxilla and prog-thic-appearing mandible. Over the years, the pa-nts traditional denture treatment with Class Iclusal overcorrection of her skeletal pseudo Class IIIxillomandibular relationship has been done but den-es were functionally poor, unstable, and uncomfort-le. The described implant treatment corrected thetients skeletal relationship with implant reconstruc-n in a stable, functional, and controlled way.Many other surgical and prosthetic factors have toconsidered in these cases. These factors include:oper evaluation of causes of bone loss and assess-nt of the existing bone condition (quality andantity), position of the maxillary sinuses and infe-r alveolar canals, alveolar arch and palatal vaultaluation, necessity to reinforce bone with bonefting, quantity, distribution and spread of implants-P spread), prosthetic design (implant-supportedrsus joint implant mucosal-supported prosthesis,ovable implant overdenture versus fixed hybrid-e prosthesis), and many others. Clinical examina-n, photographic extra- and intraoral records, pan-mic and 3D CT scans, study casts, full wax-up, andntric relations records are among the importanteoperative work-up that is necessary to determineoptimal surgical-prosthetic treatment plan in eachse.
URE 17. Three-quarter lower facial view at the completion ofcase showing improved and pleasing lower facial proportions,isfactory lip support, and esthetics. Class III skeletal maxillo-ndibular relationship with Class I occlusal relationship.
Tolstunov. CS and Implants. J Oral Maxillofac Surg 2009.
-
ofsyntothe
mateaimillama
ononcoditprbyprsitcroreastrre-pa
thesentwpamamo(masanonanaft
chyeantel
mareccaofsigthemaimitivthean
comiterinco
bebatilecoprofarcpoprlowaftdewiextiebeerameontiotoma
hamachillavesidposualvanantaitiosevridalrcluthepefulpafactioreswo
186 CS AND IMPLANTSIn this severe CS case, the surgical-prosthetic goalimplant treatment was not set to eliminate thedrome (it was deemed impossible). The goal wascontrol CS and provide stability and longevity forpatients stomatognathic system.
A variety of prosthetic designs were discussedny times by all members of the surgical-restorativem and concluded with splinting of all upper 6plants with a single meso bar, constructing a max-ry implant-supported removable overdenture, andndibular fixed implant-supported hybrid prosthesis.The rationale for the proposed treatment was based4 factors: 1) necessity to treat both arches (notly mandibular) with dental implants to preventntinuation of maxillary bone loss (underneath tra-ional complete upper denture); 2) necessity foroper bone loading throughout the alveolar archesimplant reconstruction with an implant-supportedosthesis (avoid future bone resorption); 3) neces-y to splint implants in the arch together following ass-arch stabilization principle to reinforce the al-dy weakened and resorbed maxillary bone with aong meso structure (meso bar); and 4) necessity toestablish lost posterior occlusion (correct developedthologic anterior hyperfunction) in this CS case.A severe premaxillary bone loss that extended tofirst premolar region bilaterally (Figs 3-5) pre-ted an extreme challenge due to discrepancy be-een available bone in maxilla and mandible in thisrticular case. Placement of implants in the posteriorxilla (first premolar, second premolar, and secondlar position bilaterally) and anterior mandibleidline, lateral incisor, and first premolar position),well as splinting maxillary implants with a longteriorly cantilevered bar caused an overload (stress)the anterior portion of the unsupported meso bard eventually led to its dynamic fracture 9 monthser the delivery of both prostheses.Could we foresee and prevent the occurred biome-anical complication that developed within the firstar after delivery of the prosthesis? A retrospectived careful analysis of the presented complex casels us, yes, we probably could.A cross-arch stabilization principle of splinting of allxillary implants with a single meso bar (usuallyommended in most full arch maxillary implantses) was not a good choice in this case. The lengththe unsupported anteriorly cantilevered bar wasnificant (approximately 50 mm and about 50% ofwhole length of the bar) (Fig 9). Interforaminal
ndibular fixed hybrid prosthesis, reinforced by 5plants, created an inappropriately heavy and repet-e force (traumatic occlusion) directed upward tounsupported maxillary meso bar at the midline
d eventually caused its fracture.Retrospectively, other implant prosthetic optionsuld have been selected in this case. Keeping innd that implants could be placed only in the pos-ior maxilla (the only regions of the preserved bonethis CS case), these alternative prosthetic optionsuld have included the following.The first alternative treatment option would haveen an implant-only supported design with a doubler (split-bar) and without or with small anterior can-vers. Management of developed biomechanicalmplication of a bar fracture eventually led us to thisosthetic design (Fig 15). The perceived advantagethis choice is a proper bone loading through theh with establishment of posterior occlusion (im-rtant in CS cases). According to the restorativeactitioner (patient moved and was not able to fol--up in our surgical practice), a 2-year follow-up
er fracture of the bar with new 2-bar prostheticsign showed a very comfortable and happy patientth no clinical sign of traumatic occlusion aroundisting 6 maxillary implants. According to the pa-nt, her masticatory function for the last 2 years hasen adequate without any chewing deficiency bilat-lly. A choice of Hader type clips, locator attach-nts, or other retentive components often dependsthe overall restorative plan. In this case, construc-n of a meso bar guided the restorative practitionerthe choice of Hader clip-bar retentive design of thexillary prosthesis.The second alternative treatment option wouldve been a joint implant- and mucosal-supportedxillary restoration. If this treatment option wasosen, the bar would connect 2 to 3 posterior max-ry implants on each side without anterior cantile-rs and with Hader type clip(s) retention on eache. The maxillary prosthesis would be implant-sup-rted posteriorly (both sides) and have a mucosalpport anteriorly (anterior palate with or withouteolus). The disadvantage of this option is a slowd progressive bone resorption underneath palated alveolar mucosa that is known for implant re-ned or mixed implant mucosa-supported restora-ns. It is especially complicated in cases of CS whereere anterior resorption of the premaxillary alveolarge, and often anterior portion of the palate, iseady present. The advantages of this treatment in-de a more even distribution of anterior load frommandible over a large surface of the implant su-
rstructure and anterior palate. Retrospective care-analysis of the biomechanical complication in thistient with a high-arched palatal vault points to thet that this alternative (not selected) treatment op-n with a joint implant mucosal-supported maxillarytoration with a partial anterior palatal coverageuld have been a more secure, stable, and lasting
-
resfra
be(Tnegothothereja rdebilovthesithefrres
thebesioitscroprthopopoowtio
cluimsensisso
solowsumaprmaplawaRetiogujoiinwistametio
ticforlatThtheandearcing
Ac
AQuproNoass
Re1.
2.3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
LEN TOLSTUNOV 187torative solution that would not have caused thecture of the meso bar.The third alternative treatment option would haveen a fixed implant-supported hybrid prosthesisoronto bridge) based on 6 implants rigidly con-cted by the metal-supported superstructure (analo-us to the mandibular treatment in this case). Al-ugh this option was possible and discussed withpatient at the beginning of the treatment, it was
ected for 2 reasons: 1) the patients desire to haveemovable upper implant prosthesis with an ease ofntal hygiene; and 2) clinical judgment of the possi-ity of maxillary bone and prosthetic frameworkerload. It was a joint feeling of the whole team thatremovable prosthesis is more forgiving in this
uation. Clip-bar removable overdenture with its in-rent micro movement offers some benefit, eg,eedom over the rigidity of the fixed bridge-typetoration in full-arch maxillary-bone-deficient cases.All 3 alternative maxillary prosthetic options haveir advantages and disadvantages and could haveen selected for this case initially. Anterior exten-n of the occlusion, the length of the cantilever andbiomechanical effect, A-P spread/ratio, necessity ofss-arch stabilization, superstructure design of theosthesis, and other factors have to be evaluatedroughly by the whole team to select the bestssible restorative option that has a considerablessibility to last. Each case has to be evaluated on itsn merits to decrease the likelihood of complica-ns.Mandibular treatment choices could have also in-ded different 2 to 4 implant-retained or 4 to 6plant-supported restorations. It seems that the cho-5-implant-supported mandibular hybrid prosthe-
with small posterior cantilevers is the best possiblelution in these cases.The case of CS with severe anterior maxillary re-rption was treated initially with 6 upper and 5er endosseous dental implants, maxillary implant-
pported clip-single bar removable overdenture, andndibular implant-supported fixed acrylic-basedosthesis. The biomechanical complication of thexillary meso bar fracture changed the prostheticn and the split-bar (double bar) restorative designs chosen and proved to be a successful choice.trospective analysis of biomechanical complica-n-fracture of a cross-arched single meso bar willide our team in the future toward considering ant implant mucosal-supported maxillary restorationsimilar cases. Careful follow-up of these patientsth periodic x-ray evaluation of implant fixtures andbility of adjacent crestal bone levels is recom-nded as one of the important on-going confirma-ns of a successful implant treatment.It seems that an ideal treatment option in this par-ular case could have been an iliac crest bone graftthe anterior maxilla and inferior alveolar nerve
eralization procedures for the posterior mandible.at would create a favorable bone situation alongentire alveolar ridge of both maxilla and mandible
d would allow placement of an adequate amount ofntal implants into solid bone throughout bothhes with proper implant distribution, bone load-, and functional occlusion.
knowledgments
ll surgeries were carried out by Len Tolstunov, DDS. Noreenimson, DDS, provided the restorative treatment, and laboratorysthetic construction was done by Curtis Names, CDT, andrman Cho, CDT. The author thanks Edward Shaw, DDS, for hisistance with this manuscript.
ferencesThe glossary of prosthodontic terms. J Prosthet Dent 94:10,2005Glossary of implant terms. J Oral Implantol 28:3, 2003Shen K, Gongloff RK: Prevalence of the combination syndromeamong denture patients. J Prosthet Dent 62:642, 1989Palmqvist S, Carlsson GE, Owall B: The combination syndrome:A literature review. J Prosthet Dent 90:270, 2003Attard NJ, Zarb GA: Implant prosthodontic management ofpartially edentulous patients missing posterior teeth: The To-ronto experience. J Prosthet Dent 89:352, 2003Jameson WS: The use of linear occlusion to treat a patient withcombination syndrome: A clinical report. J Prosthet Dent 85:15, 2001Rachmiel A, Gutmacher Z, Blumenfeld I, et al: Vertical alveolarridge augmentation using distraction osteogenesis. RefuatHapeh Vehashinayim 18:64, 2001Yalcin S, Ordulu M, Emes Y, et al: Alveolar distraction osteo-genesis before placement of dental implants. Implant Dent15:48, 2006Gaggl A, Rainer H, Chiari FM: Horizontal distraction of theanterior maxilla in combination with bilateral sinus lift opera-tionPreliminary report. Int J Oral Maxillofac Surg 34:37, 2005Jensen OT, Leopardi A, Gallegos L: The case for bone graftreconstruction including sinus grafting and distraction osteo-genesis for the atrophic edentulous maxilla. J Oral MaxillofacSurg 62:1423, 2004Guirado JL, Yuguero MR, Carrion del Valle MJ, et al: A maxillaryridge-splitting technique followed by immediate placement ofimplants: A case report. Implant Dent 14:14, 2005Maiorana C, Santoro F, Rabagliati M, et al: Evaluation of the useof iliac cancellous bone and anorganic bovine bone in thereconstruction of the atrophic maxilla with titanium mesh: Aclinical and histologic investigation. Int J Oral Maxillofac Im-plants 16:427, 2001Iizuka T, Smolka W, Hallermann W, et al: Extensive augmenta-tion of the alveolar ridge using autogenous calvarial split bonegrafts for dental rehabilitation. Clin Oral Implants Res 15:607,2004Kondell PA, Nordenram A, Moberg LE, et al: Reconstruction ofthe resorbed edentulous maxilla using autogenous rib graftsand osseointegrated implants. Clin Oral Implants Res 7:286,1996Aboul-Hosn S, Monner A, Juarez I, et al: Tibial bone harvestingtechnique for filling maxillary bone gaps in implantology. RevStomatol Chir Maxillofac 107:93, 2006Rohner D, Bucher P, Kunz C, et al: Treatment of severe atrophyof the maxilla with the prefabricated free vascularized fibulaflap. Clin Oral Implants Res 13:44, 2002Nystrom E, Lundgren S, Gunne J, et al: Interpositional bonegrafting and Le Fort I osteotomy for reconstruction of the
-
atrophic edentulous maxilla. A two-stage technique. Int J OralMaxillofac Surg 26:423, 1997
18. McFadden DD: Pre-prosthetic surgery options for fixed dentalimplant reconstruction of the atrophic maxilla. Ann R AustralasColl Dent Surg 15:61, 2000
19. Schoeman R, Subramanian L: The use of orthognathic surgeryto facilitate implant placement: A case report. Int J Oral Max-illofac Implants 11:682, 1996
20. Boyne P, Jones SD: Demonstration of the osseoinductive effectof bone morphogenic protein within endosseous dental im-plants. Implant Dent 13:180, 2004
21. Branmark PI, Grondahl K, Ohrnell LO, et al: Zygoma fixture inthe management of advanced atrophy of the maxilla: Tech-nique and long-term results. Scand J Plast Reconstr Surg HandSurg 38:70, 2004
22. Ferrara ED, Stella JP: Restoration of the edentulous maxilla: Thecase for the zygomatic implants. J OralMaxillofac Surg 62:1418, 2004
23. Penarrocha-Diago M, Uribe-Origone R, Guarinos-Carbo J: Im-plant-supported rehabilitation of the severely atrophic maxilla:A clinical report. J Prosthodont 13:187, 2004
24. Fortin Y, Sullivan RM, Rangert BR: The Marius implant bridge: Surgi-cal and prosthetic rehabilitation for the completely edentulous upperjaw with moderate to severe resorption: A 5-year retrospectiveclinical study. Clin Implant Dent Relat Res 4:69, 2002
25. Malo P, de Araujo Nobre M, Petersson U, et al. A pilot study ofcomplete edentulous rehabilitation with immediate functionusing a new implant design: Case series. Clin Implant DentRelat Res 8:223, 2006
26. Toffler M: Treating the atrophic maxilla by combining shortimplant with minimally invasive osteotome procedure. PractProced Aesthet Dent 18:301, 2006
27. Petrungaro PS: Reconstruction of severely resorbed atrophicmaxillae and management with transitional implants. ImplantDent 9:271, 2000
28. Krekmanov L: Placement of posterior mandibular and maxillaryimplants in patients with severe bone deficiency: A clinical reportof procedure. Int J Oral Maxillofac Implants 15:722, 2000
29. Barber HD, Scott RF, Maxson BB, et al: Evaluation of anteriormaxillary alveolar ridge resorption when opposed by transman-dibular implant. J Oral Maxillofac Surg 48:1283, 1990
30. Beals R, Lefkove MD: Tatum custom frame implant: Multipleoptions including treatment for combination syndrome. J OralImplantol 18:257, 1992
31. Henry PJ: A review of guidelines for implant rehabilitation ofthe edentulous maxilla. J Prosthet Dent 87:281, 2002
32. Sadowsky SJ: Mandibular implant-retained overdentures: A lit-erature review. J Prosthet Dent 86:468, 2001
33. Langer Y, Laufer BZ, Cardash HS: Modalities of treatment forthe combination syndrome. J Prosthodont 4:76, 1995
34. Narhi TO, Geertman ME, Hevinga M, et al: Changes in theedentulous maxilla in persons wearing implant-retained man-dibular overdentures. J Prosthet Dent 84:43, 2000
35. Kelly E: Changes caused by a mandibular removable partialdenture opposing a maxillary complete denture. J ProsthetDent 27:140, 1972
36. Thiel CP, Evans DB, Burnett RR: Combination syndrome asso-ciated with a mandibular implant-supported overdenture: Aclinical report. J Prosthet Dent 75:107, 1996
37. Carlsson GE: Clinical morbidity and sequelae of treatment withcomplete dentures. J Prosthet Dent 79:17, 1998
38. Tolstunov L: Combination syndrome: Classification and casereport. J Oral Implantol 33:139, 2007
39. Carlsson GE: Responses of jawbone to pressure. Gerodontol-ogy 21:65, 2004
40. Gupta S, Lechner SK, Duckmanton NA: Maxillary changes un-der complete dentures opposing mandibular implant-sup-ported fixed prostheses. Int J Prosthodont 12:492, 1999
41. Cabianca M: Combination syndrome: Treatment with dentalimplants. Implant Dent 12:300, 2003
42. Lechner SK, Mammen A: Combination syndrome in relation toosseointegrated implant-supported overdentures: A survey. IntJ Prosthodont 9:58, 1996
188 CS AND IMPLANTS
Management of Biomechanical Complication of Implant-Supported Restoration of a Patient With Combination Syndrome: A Case ReportCase ReportPreoperative Computerized Radiographic Scan AnalysisDiagnosisTreatment PlanOperative PhaseRESTORATIVE PHASE
Case CompletionDiscussionAcknowledgmentsReferences