Management & Leadership role of Pharmacists in HIV & MCH care – towards achieving Millenium...
92
Management & Leadership role of Pharmacists in HIV & MCH care – towards achieving Millenium Development Goals 4, 5 & 6. Dr. Jaydeep Tank MD, DNB, DGO, FCPS, MICOG. FOGSI representative to the Consortium for Safe Abortion, FIGO Project on Unsafe Abortion, PMNCH – WHO (Geneva). Co Chair Reproductive Endocrinology Committee – Asia Oceania Federation of Obstetrics and Gynecology (AOFOG) Convener- Sub Committee on Unsafe Abortions – (AOFOG). Ex Chairman MTP committee (FOGSI) 2004 - 09. Member Advisory Committee for Operational Research on Safe abortion of the Ministry of Health and Family Welfare - Government of India
-
Upload
mervin-thomas -
Category
Documents
-
view
215 -
download
0
Transcript of Management & Leadership role of Pharmacists in HIV & MCH care – towards achieving Millenium...

Management & Leadership role of Pharmacists in HIV & MCH care – towards achieving Millenium Development Goals 4, 5 & 6.
Dr. Jaydeep TankMD, DNB, DGO, FCPS, MICOG.
FOGSI representative to the Consortium for Safe Abortion, FIGO Project on Unsafe Abortion, PMNCH – WHO (Geneva).
Co Chair Reproductive Endocrinology Committee – Asia Oceania Federation of Obstetrics and Gynecology (AOFOG)
Convener- Sub Committee on Unsafe Abortions – (AOFOG).Ex Chairman MTP committee (FOGSI) 2004 - 09.
Member Advisory Committee for Operational Research on Safe abortion of the Ministry of Health and Family Welfare - Government of India
Ashwini Maternity and Surgical Hospital, Center for Endoscopy and IVF
Visiting Consultant for IVF- Akola, Jabalpur and Jalandar

A classic—something that
everybody wants to have read
and nobody wants to read.
~ Mark Twain ~

• The problem of HIV and MTCT
• The problem of resources.
• The treatment of HIV
• The role of pharmacists
• Role of partnerships

• The problem of HIV and MTCT
• The problem of resources.
• The treatment of HIV
• The role of pharmacists
• Role of partnerships

“Dr. Robert Gallo of the National Cancer Institute had isolated the virus
which caused AIDS,
It was named HTLV-III,
There would soon be a
commercially available test
for the virus”.
Margaret Heckler
Human Services Secretary
23rd April 1984
Margaret Heckler
Dr. Robert Gallo
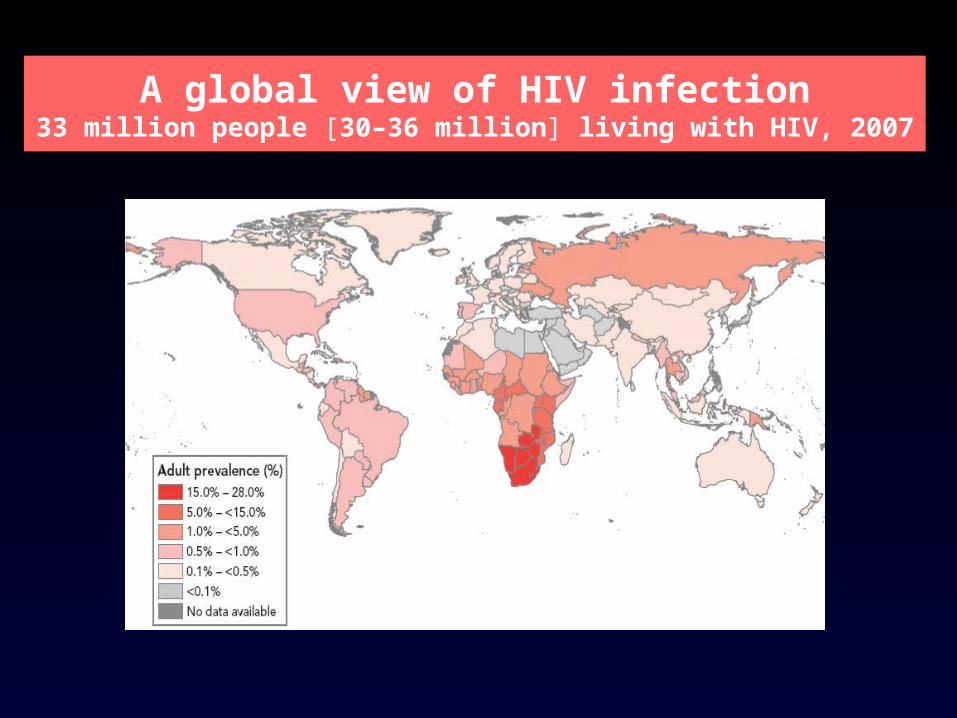
A global view of HIV infection33 million people [30–36 million] living with HIV, 2007

In India…• The first AIDS case in India was detected in 1986; since then HIV
infection has been reported in all states and union territories. • The highest HIV prevalence rates are found in Maharashtra, Andhra
Pradesh and Karnataka in the south; and Manipur, Mizoram and Nagaland in the north-east.1
• Four southern states (Andhra Pradesh, Maharashtra, Tamil Nadu and Karnataka) account for around 63% of all people living with HIV in India.
HIV Sentinel Surveillance and HIV Estimation, 2006", NACO, 2007
• It is now thought that around 2.5 million people in India are living with HIV.
UNAIDS/NACO/WHO, 6 July 2007

Children and HIV/AIDS
• Everyday about 1200 children under 15 years of age become infected with the virus
• The majority acquire the virus before birth, during pregnancy, delivery or when breastfed.
• Over 90% of new infections in infants occur through MTCT.
• HIV/AIDS is particularly aggressive in children:– ±50% of those infected and without treatment, die
before their second birthday.
Prophylaxis – current status
• Only 9% of HIV+ pregnant women in low/ middle income countries received ARV prophylaxis in 2005.
• Only 7 countries provided ARV prophylaxis to more than 40% of pregnant women in 2005 (Brazil, Argentina, Jamaica)

PMTCT – Possibilities
• High income countries have reduced infection rates at birth to less than 2%.
• Cost for pediatric ARVs has been reduced to less than US$0.16 or US$ 60.00 per year.
• Annual mortality rates due to AIDS among children began to fall since 2003 due to scale up treatment and PMTCT.

PMTCT and MDG’s
PMTCT directly affects the achievement of three MDGs (to be met by 2015):
• 4th MDG: Reduce by two thirds the mortality rate among children under five
• 5th MDG: Reduce by three quarters the maternal mortality ratio
• 6th MDG: Halt and begin to reverse the spread of HIV/AIDS
Policy – ahead of its time
• United Nations Comprehensive Approach - 2003
• Universal Access of Prevention, Treatment and Care – G 8 at Gleneagles July 2005
• Abuja Call to Action 2005
• The Declaration of Commitment - UNGASS June 2001-

• The problem of HIV and MTCT
• The problem of resources.
• The treatment of HIV
• The role of pharmacists
• Role of partnerships

Overall Strategic Approach
• Decentralized approaches:– Sub national teams are responsible for the planning,
implementation and monitoring of PMTCT services, including the training of service providers
• Continuous political commitment• Incorporating whole family care with models such as
MTCT Plus – a package of HIV prevention, care, support and treatment for mothers, children and their families.

• The total population calculated for 1 March 2001 was 1,027,015,247, making the 2001 census the first to count more than a billion Indians.
http://www.censusindia.net/results/resultsmain.html
• The population had risen by 21.34% compared to the 1991 total.
http://www.censusindia.net/results/
• Although India occupies only 2.4% of the world's land area, it supports over 17.5% of the world's population 1.13 billion people.
• 31.8% of Indians are younger than 15 years of age.
• As per the 2001 census, 72.22% of the people live in more than 550,000 villages, and the remainder in more than 2000 towns and cities.

• Till September 2004, around 633,108 doctors were registered with different State Medical Councils of India.
• This implies 1 doctor for 1622 persons (or 61 doctors per 100,000 populations) as against 1 doctor per 182 persons and 401 persons in the United States and Australia respectively.

Serving the reproductive needs of
Half a Billion
Women

The Possible solutions
• Strengthen capacity
• Increase the number of providers
Capacity

The Place of Private Health Care
• India spends less than 1 percent of its GDP on health.
• Only Pakistan spends less among its South Asian neighbors.
• Sri Lanka and Bhutan which are poorer than India spend 6 percent and 10 percent respectively of their GDP on health.
Gross underutilization of ‘free’ care
• In general, in India people depend more on the private sector for health care than they do on the public sector.
• The private health sector in India is one of the largest in the world: 80 percent of all qualified doctors, 75 percent of dispensaries and 60 percent of hospitals in India belong to the private sector
Narayan et al, 2003.
• According to the NFHS II, only 23.5 percent of urban residents and 30.6 percent of rural residents choose to visit a government health facility as their main source of health care services.

Increase the number of providers

What has changed?
• Technology
• Demography
• Development of cadres of non physician providers
• Physician perception
“The terms “non-physician” and “mid-level providers” refer to a broad range of non-physician health workers, including midwives, nurses, clinical officers, physician assistants and paramedics, among others, whose training and responsibilities differ from one country to another, but who are involved in the provision of reproductive health care or primary health care services”
WHO 2003.
Who will be the “increased” providers…

FOGSI’s position on the inclusion of MLP’s
• Acknowledging the problem
• The gap between the number of providers needed and the providers available
• Defining the MLP’s
• Setting standards for training
• Taking cognizance of the legal scenario

FOGSI is committed to…
• To introduce or change policies to facilitate MLPs to provide care after receiving adequate training
• To capacity build the MLPs for ensuring continued and sustainable services towards maintaining the quality of care and services.
• To provide MLPs with sufficient educational materials.
• To ensure availability of up to date operational guidelines for the MLPs to act as a quick reference.
• To ensure that the MLPs also promote and recognise the reproductive and sexual rights of women.
The way forward….
• Safe and Effective Technology is available.• The problem is reaching it to those who need it the
most• Inadequate and Inequitable access • Increase access by increasing the number of service
providers and build good quality capacity• Partnerships with the government, NGO’s and other
stakeholders.

• The problem of HIV and MTCT
• The problem of resources.
• Management
• The role of pharmacists
• Role of partnerships
Issues for us…
• Universal Precautions
• MTCT
• Contraception and HIV
• PEP
• Abortion and HIV
• Infertility and HIV

The UN PMTCT response
1. Primary prevention interventions within services related to reproductive health
2. Appropriate counseling and support to women living with HIV to enable them make an informed decision about their future reproductive life, with special attention to preventing unintended pregnancies.
3. HIV testing be integrated in maternal child health units where ARVs are provided to prevent infection being passed on to their babies and also the woman’ s own health; and adequate counseling is provided on the best feeding option for the baby.
4. Better integration of HIV care, treatment and support for women found to be positive and their families.
2003

HIV Infection in pregnancy
• Informed universal screening– interventions can reduce maternal-to-child
transmission from 25-30% to less than 2%
• Confidentiality and disclosure
• Antenatal monitoring and advise
• Screening for fetal abnormalities
• Look for complications of therapy.

HIV Infection in PregnancyHIV Infection in Pregnancy General Principles of ARV TherapyGeneral Principles of ARV Therapy
Nucleoside/nucleotide reverse transcriptase inhibitors • reduce the growth of HIV• Inhibit prolongation of DNA chain insert false nucleotide• Zidovudine, lamivudine
Non nucleoside reverse transcriptase inhibitors• keep HIV from making copies of itself• Bind directly to reverse transcriptase preventing activity• Nevirapine, efavirenz
Protease inhibitors• prevent HIV from being formed • Inhibit cleavage of viral packaging prior to viral release• Indinavir, saquinavir mesylate, nelfinar mesylate
Livingstone, Curr Wom Health Rep, 2:245, 2002

How many antiretrovirals?
Single drug therapy Polydrug therapy
Better safety profile Can be continued as long term therapy
Efficacious against MTCT – CS may be offered
Reduces viral load to nearly nil – CS not required
Simplicity Effective for advanced disease
Rs 7,000 to 8,500 Rs 21,000 to 24,000 plus

Single dose nevirapine
• The simplest of all PMTCT drug regimens was tested in the HIVNET 012 trial, which took place in Uganda between 1997 and 1999.
• This study found that a single dose of nevirapine given to the mother at the onset of labour and to the baby after delivery roughly halved the rate of HIV transmission.6 7
• As it is given only once to the mother and baby, single dose nevirapine is relatively cheap and easy to administer.
• Since 2000, many thousands of babies in resource-poor countries have benefited from this simple intervention, which has been the mainstay of many PMTCT programmes.
Connor et al, NEJM 331(18), 3 November 1994Guay et al, The Lancet 354(9181), 4 September 1999

When is single dose nevirapine appropriate?
• Because of concerns about drug resistance and relatively low effectiveness, there is now general agreement that single dose nevirapine should be used only when no alternative PMTCT drug regimen is available. Whenever possible, women should receive a combination of drugs to prevent HIV resistance problems and to decrease MTCT rates even further.
• Nevirapine, however, is still the only single dose drug available to prevent MTCT.

Optimize Labor Care
• Late rupture of membranes
• Avoid invasive procedures such as fetal electrodes, scalp blood sampling
• Avoid traumatic or instrumental delivery
• Vaginal lavage with chlorhexidine is not efficacious
• Elective LSCS– With effective ART it may have a limited role.
• Breast Feeding– If she takes no preventive drugs and breastfeeds
then the chance of her baby becoming infected is around 20-45%.

Post Delivery Care
• Antibiotics, wound care, analgesics and discharge as per routine
• If the mother chooses to breast feed, teach and support her
• If the mother opts not to breast feed, suppress lactation

Child’s Serostatus
• Child is HIV positive if :– PCR is positive at any time after birth– ELISA test is positive after 18 months age
• ELISA positive before 18 months does not mean that baby is infected
• Timing of transmission by timing of PCR positivity: < 48 hours : antenatal 48 hours to 7 days : intrapartum > 7 days : postnatal transmission

Contraception
• Condoms should be used even if the couple is using other methods
• Hormonal methods are suitable for pregnancy prevention
• In asymptomatic HIV positive patients, IUCD is not contraindicated, but is best avoided

PEP

What is PEP?
• The term “Post-exposure prophylaxis” or PEP refers to the prophylactic use of antiretrovirals to prevent establishment of HIV infection after an occupational exposure to HIV
Types of occupational exposures• Percutaneous
– Needle stick– Sharps injury
• Mucocutaneous
• Contact with skin which is abraded, chapped, inflamed or an open wound
• Direct contact with concentrated HIV in a laboratory
• Isolated skin exposure
Risk of Transmission of Different Viruses Following Accidental Needle Injury
• Hepatitis B virus 6-30%
• Hepatitis C virus 1.8%
• HumanImmunodeficiency Virus 0.3%

What Is The Risk?
Occupational
Percutaneous 0.3%
Mucous membrane 0.09%
Sexual transmission 0.018% to 3%
Mother to child 25%
Infected blood products 95%
Antiviral therapy 1998; 3 (Suppl 4): 45-47

Factors Influencing Risk
• Depth of injury
• Size and type of needle
• Device visibly contaminated with blood
• Procedure involving a needle placed in artery or vein
• Use of zidovudine
• Source patient’s viral load

How To Reduce Risk?
• Number of procedures
• Double gloves
• Gowns, facemasks, goggles. Care during procedures where splattering of blood is anticipated
• Use of impervious needle-disposal containers
• Transport of samples in sealed containers
• Universal precautions
Antiseptics effective against HIV
• Undiluted Savlon solution
• Chlorhexidine
• 2% glutaraldehyde
• Household bleach
• Formalin 4%
• Povidone iodine 2%
• IPA, ethanol 70%
• Dettol solution – no effect

Treatment Of Exposure - Immediate Measures
• Use of soap and water to wash any wound or skin
• Flush exposed mucous membrane with water
• Report to the concerned authority
• Counselling
• Antiretroviral therapy

General Guidelines For PEP
• Therapy should be recommended after exposure
• Therapy should be initiated as soon as possible, preferably within hours of exposure
• 2- and 3-drug regimens, based on level of risk
• Source patient’s HIV status unknown, decide on a case-to-case basis
• Follow up counseling and HIV testing using ELISA periodically for at least 6 months (baseline, 6 weeks, 12 weeks and 6 months)
• Potential benefits should be weighed against potential risks

Zidovudine 300 mg + lamivudine 150 mg (Duovir* 1 tab) bid OrTenofovir disoproxil fumarate 300 mg + emtricitabine 200mg (Tenvir –EM 1 tab) od
OrTenofovir disoproxil fumarate 300 mg (Tenvir) od + lamivudine 150mg bid or 300mg od (Lamivir)
Alternative:Stavudine 30/40 mg + lamivudine 150 mg (Lamivir-S 30/40 1 tab) bidOr Didanosine 250/400mg (Dinex-EC) od + lamivudine 150mg bid or 300mg od (Lamivir)
* Drugs listed are those available in India
Basic regimen (28 days)*

Expanded regimen (28 days)*
Basic regimen plus:
Preferred:• Lopinavir 200 mg/ritonavir 50 mg (Lopimune 2 tabs) bid
Alternative:• Atazanavir 400mg od• If used with TDF: atazanavir 300mg od and ritonavir 100mg (Ritomune 1 tab)
bid Or• Indinavir 800 mg (Indivan 2 caps) and ritonavir 100 mg (Ritomune 1tab) bid
or Indinavir 800mg (2 caps) tidOr • Saquinavir 1000mg ( Maximune 2 tabs bid ) and ritonavir 100 mg (Ritomune
1 tab) bid Or• Nelfinavir 750 mg (Nelvir 3 tabs) tidOr• Efavirenz 600 mg (Efavir-600 1 tab) od at bedtime
* Drugs listed are those available in India
Enfuvirtide (90 mg (1 ml) twice daily by subcutaneous injection) to be used only with expert consultation

Follow up of exposed cases
• Baseline HIV testing• Follow up testing at 6 weeks, 3 months and 6 months by
ELISA• Role of HIV DNA PCR – unclear. If done must be
confirmed by ELISA

• More and more patients with HIV infection continue to seek treatment
• Greater number of needlestick injuries are expected to occur
• The risk of HIV transmission is extremely small
• The availability of PEP should not preclude taking universal precautions
PEP

Abortion in women living with HIV
No woman is required to build the world
by destroying herself.
~ Rabbi Sofer ~

Almost all abortion-related deaths are preventable
When abortion is performed by qualified people using correct techniques in sanitary conditions, it is one of the safest medical procedures

Reproductive Health Strategy
• Safe sex practices and monogamous relationship
• Pap smear screening
• Prevention of unwanted pregnancy– Condom use– Hormonal contraception or IUD
• Termination of unwanted pregnancy

Do women with HIV seek abortion?
• Nowrosjee Wadia Maternity Hospital– Study period 1993 to 2003
– Number of patients tested: 116031
– Number of patients HIV positive : 1508 (1.31%)
– Number of HIV positive patients undergoing MTP : 76 (4.35%)
• Reasons for low MTP rates– Opt to continue pregnancy
– Late registration and testing

Reproductive rights
• Same rights and privileges as any other woman
• Pregnancy termination is permitted under the same provisions as per the MTP Act
• Decisions about pregnancy continuation or termination are based on unbiased, non-directive counseling

Medical factors influencing the MTP decision
• Women on HAART especially if Efavirenz
(Category D) is part of the regimen
• Co-morbidity that may endanger maternal life

Medical agents after one year in INDIA
• More than 1 million tablets of Mifepristone from a single company
Data from Zydus Cadila

Market Growth % of Mife - Miso
0 20 40 60 80 100 120
Dec'04
Dec'05
Nov' 06
% Growth
Misoprostol
Mifepristone
ORG MARG DataCourtesy Sun Pharma

“A revolution without a rebellion”
Chris Sutton

Medical abortion : legal aspects
• 7 weeks of pregnancy
• Ultrasound not necessary
• Valid consent– Without coercion or undue influence– Minors
• Back up facilities at a recognized MTP center; should also be equipped to manage biomedical waste effectively

The “informal” sector
• While 60% of chemists were aware of mifepristone, only 35% of outlets stocked the drug.
• Chemists reported an average of two customers per week for mifepristone and four customers per week for misoprostol.
• Chemists said 90% of sales were to non-physicians and that the majority of customers were men.
• Most sales were reported to be to those carrying a prescription, but over-the-counter sales were also reported in a small number of cases.
Ganatra Bela, Manning Vinoj, Pallipamulla Suranjeen Prasad, 2005, Ipas, New Delhi, India.

Medical abortion : regimen till 9 weeks pregnancy
• 200 mg Mifepristone
• 48 hours later 400 micrograms of Misoprostol vaginally
• Follow up after 15 days to ensure completeness

Additional measures
• No evidence of drug interactions between either drug and HAART
• Adding antibiotics ? – Evidence of lower genital tract infection– Prolonged bleeding (>7days)– Low CD4 count
• Pain relief– Spasmolytics (Tramadol)– Avoid NSAIDs especially if low platelet count associated
with HIV

Instructions to patient
• Disposal of sanitary pads in a safe manner– No evidence of environmental HIV transmission – Report if heavy bleeding, pain, fever, no bleeding
in first 48 hours after Misoprostol
• Avoid intercourse

Medical v/s Surgical Abortion
• Advantages– Surgical and anesthesia risk minimized– Demedicalization– Privacy
• Disadvantages– More number of visits– Available only till 7 weeks of pregnancy
• Disposal of biomedical waste should not be a consideration

Post abortion counseling
• Medical abortion is not – A alternative to contraception– An “over-the-counter” abortion
• Discuss sexual health issues and reinforce the reproductive health strategy

Infertility and HIV
• For couples discordant for HIV infection who wish to conceive, appropriate advice should be given to optimise the chance of conception while minimising the risk of sexual transmission.
• In vitro fertilisation (IVF) is now considered to be ethically acceptable for couples with subfertility.
Infertility and HIV
• Where a woman who is HIV negative has an HIV-positive partner, the risk of transmission to the woman, estimated as approximately 1:500 per sexual act, can be reduced by limiting sexual intercourse to around the time of ovulation.
• For HIV discordant couples where the woman is HIV positive, the couple should be advised on how to perform artificial insemination at the time of ovulation

Infertility and HIV
To date there have been no seroconversions in women inseminated with washed sperm.

Infertility and HIV
• IVF is now considered ethically acceptable in view of vertical transmission rates of less than 2% and increased life expectancy for parents taking HAART.
• HIV positive men with low sperm counts may be offered intracytoplasmic sperm injection following sperm washing.

Life is not about how
many breaths you take
but about moments
that take your breath away
Will Smith in Hitch

• The problem of HIV and MTCT
• The problem of resources.
• Management
• The role of pharmacists
• Role of partnerships
Role of the Pharmacist
• Review prescriptions• Recommend changes to regimen• Monitor adherence to treatment• Remove barriers to treatment• Manage adverse effects• Monitor drug interactions• Pharmacovigilance• Manage drug supply

Adherence- Strategies
• Encourage clients to bring ARVs at each visit to the Pharmacy –
• Encourage clients not to take any over-the-counter medications-
• Counseled on how to take ARVs correctly- timing of doses, with or without meals
• Emphasize the importance of taking ARVs- suppression of HIV
Adherence- Strategies
• Do pill counts• Provide pill boxes ( supplied by drug companies): • Relate possible side effects• Liaise with multidisciplinary team members if a
problem arises e.g. drowsiness, shift worker. May warrant change in regimen.
• Encourage support of family member or friend.• Be a very good listener.

Pharmacovigilance
• To detect unknown adverse reactions and interactions
• To detect increases of frequency of (known) adverse reactions
• To identify risk factors/mechanisms underlying adverse reactions
Managing Drug Supply
• To ensure adequate and continuous supply of ARVs
• To prevent stock outs
• To liaise with local Pharmaceutical companies
• Inventory control, including reducing expired stock

• The problem of HIV and MTCT
• The problem of resources.
• Management
• The role of pharmacists
• Role of partnerships

“Let us not underestimate the
Problem,But let us also not
overestimate our capability to do something about it.”
Barrack Obama
24 / 11/ 2008

• The overall objective is to increase the contribution of HCP Associations to national MNCH plans through a strengthened participation in policy and programme development and an increased alignment of activities to the national targets regarding the achievement of MDGs 4 and 5 (reducing child mortality by 2/3 and maternal mortality by ¾ by 2015).


Task 1: Selection of Priority Actions
• Advocacy
• Planning
• Human Resources
• Organizational Strengthening
• Quality Improvement

Project management Committee
• Chairman: Praful Sheth.
• Nominated Focal Point: Jaydeep Tank.
• Members– 2 Representatives from each association.
• Rotate each meeting through the associations.

AdvocacyTask 1 • (a) Problems associated with advocacy and why is it a top priority.
– No coherent and integrated strategy.– All stakeholders do not have an equal voice. – Health planning is not done by professionals.
• (b) How will capacity building in this activity contribute to achievement of MDGs 4 and 5?
– Self evident and as below
• (c) Who will benefit most and how?
– Strengthen maternal – perinatal, neonatal and child health in the community as well as facility.
– Integrated and continued care.

Quality ImprovementTask 1 • (a) Problems associated with Quality Improvement and why is it a top priority.
– Quality in public health sector needs urgent attention. – Unregulated health care. – Practical standards for different settings. – Quality as a culture does not exist in health care training
• (b) How will capacity building in this activity contribute to achievement of MDGs 4 and 5?
– Self evident and as below
• (c) Who will benefit most and how?
– Strengthen maternal – perinatal, neonatal and child health in the community as well as facility.
– Integrated and continued care.

The trouble with so many of us
is that we underestimate
the power of simplicity.
We tend to mistake
movement for achievement.
~ Robert Stuberg ~