Malaysia
70
MALAYSIA 1. PRATAP KARPAYAH 2. GIRLAND MUANZA 3. NIK FATIMAH AZ ZAHARA 4. MENAHA MOHANASUNDARRAM 5. TUAN MUHAMMAD HANIF
Transcript of Malaysia

MALAYSIA 1. PRATAP KARPAYAH 2. GIRLAND MUANZA
3. NIK FATIMAH AZ ZAHARA4. MENAHA MOHANASUNDARRAM
5. TUAN MUHAMMAD HANIF

GENERAL SOCIAL-ECONOMIC
CHARACTERISTICS OF RESIDENTIAL LIFE IN
MALAYSIA

GOVERNMENT STRUCTURE AND POLITICAL REGIME IN MALAYSIA Government of Malaysia refers to the Federal Government or national government authority based in the federal territories of Kuala Lumpur, and the federal executive based in Putrajaya. Malaysia is a federation of 13 states operating within a constitutional monarchy under the Westminster parliamentary system and is categorised as a representative democracy. The federal government of Malaysia adheres to and is created by the Federal Constitution of Malaysia, the supreme law of the land.The federal government adopts the principle of separation of powers and has three branches: executive, legislature and judiciary.
The state governments in Malaysia also have their respective executive and legislative bodies. The judicial system in Malaysia is a federalised court system operating uniformly throughout the country.
GENERAL SOCIAL-ECONOMIC CHARACTERISTICS OF RESIDENTIAL LIFE


ADMINISTRATIVE AND TERRITORIAL SUBDIVISIONS
• - The states and federal territories of Malaysia are the principal administrative divisions of Malaysia.
• - Malaysia is a federation comprising thirteen states (Negeri) and three federal territories (Wilayah Persekutuan).
• -Eleven states and two federal territories are located on the Malay Peninsula, collectively called Peninsular Malaysia (Semenanjung Malaysia) or West Malaysia.
• -Two states are on the island of Borneo, and the remaining one federal territory consists of islands offshore of Borneo; they are collectively referred to as East Malaysia or Malaysian Borneo.

CLIMATIC AND GEOGRAPHIC PECULIARITIES
Malaysia weather benefits from a tropical climate with high temperatures and high humidty throughout the year. Daytime temperatures rise above 30°C (86°F) year-round and night-time temperatures rarely drop below 20°C (68°F).
Geography and climate
Malaysia is situated in central South-East Asia, bordering Thailand in the north, with Singapore to the south and Indonesia to the south and west. It is composed of Peninsular Malaysia and the states of Sabah and Sarawak on the north coast of the island of Borneo, 650 to 950km (404 to 600 miles) across the South China Sea.
Peninsular Malaysia is an area of forested mountain ranges running north-south. The coastline extends nearly 1,900km (1,200 miles). The west coast consists of mangrove swamps and mudflats which separate into bays and inlets. In the west, the plains have been cleared and cultivated, while the unsheltered east coast consists of tranquil beaches backed by dense jungle.
Malaysian Borneo, Sarawak has flat landforms and, in some places, swampy coastal plains with rivers penetrating the jungle-covered hills and mountains of the interior. Sabah has a narrow coastal plain which gives way to mountains and jungle. Mount Kinabalu, at 4,094m (13,432ft), is the highest peak in Malaysia.

GENERAL ECONOMIC GROWTH & THE PREDOMINANT TYPE
OF PRODUCTION (INDUSTRIAL AND AGRICULTURAL PRODUCTION)
Malaysia has a newly industrialised market economy, which is relatively open and state-oriented.
The economy of Malaysia is the third largest in Southeast Asia. As one of three countries that control the Strait of Malacca, international trade plays a large role in Malaysia's economy.
Agricultural Sector
Agriculture is now a minor sector of the Malaysian economy, accounting for 7.1% of Malaysia's GDP in 2014 and employing 11.1% of Malaysia's labour force, in 1960s when agriculture accounted for 37% of Malaysia's GDP and employed 66.2% of the labour force.
The crops grown by the agricultural sector has also significantly shifted from food crops like paddy and coconut to industrial crops like palm oil and rubber.
Industry sector
- Malaysia's industrial sector accounts for 36.8%,
over a third of the country's GDP in 2014, and
employs 36% of the labour force in 2012.
The industrial sector mostly contributed by the Electronics industry, Automotive industry and Construction industry.

POPULATION STATISTICS

POPULATION SIZE AND RESIDENTIAL DENSITY
Census 2010 revealed that the total population of Malaysia was 28.3 million, compared with 23.3 million in 2000. This gives an average annual population growth rate of 2.0 per cent for the period 2000-2010. The rate was lower compared to that of 2.6 per cent during 1991-2000. The state with the highest growth rate for the period 2000-2010 was W. P. Putrajaya (17.8%), followed by Selangor (2.7%), Melaka (2.6%) and Sabah (2.1%). Among the states which experienced lower growth rate were Terengganu (1.4%), Perak (1.4%), W. P. Labuan (1.3%) and Perlis (1.2%).


POPULATION SIZE AND RESIDENTIAL DENSITY
Population density of Malaysia stood at 86 persons per square kilometer in 2010 compared with 71 persons in 2000.
Unlike the population distribution, the population density revealed a different picture.
Selangor being the most populous state was only ranked fifth in terms of population density with 674 persons per square kilometer.
Among the most densely populated states were W. P. Kuala Lumpur (6,891 persons), Pulau Pinang (1,490 persons) and W. P. Putrajaya (1,478 persons).

POPULATION DISTRIBUTION
Population distribution by state indicated that Selangor was the most populous state (5.46 million), followed by Johor (3.35 million) and Sabah (3.21 million).
The population share of these states to the total population of Malaysia was 42.4 per cent. The least populated states were W. P. Putrajaya (72,413) and W .P. Labuan (86,908).

RELIGION IN MALAYSIA
Malaysia is a multicultural and multiconfessional country.
As of the 2010 Population and Housing Census,
61.3 percent of the population practices Islam 19.8 percent Buddhism 9.2 percent Christianity 6.3 percent Hinduism 1.3 percent Chinese
The remainder is accounted for by other faiths, including, Animism,, Folk religion, Sikhism and other belief systems.

MALAYSIA: LANGUAGES AND ETHNIC GROUPS
LanguagesBahasa Malaysia (official), English, Chinese (Cantonese, Mandarin, Hokkien, Hakka, Hainan, Foochow), Tamil, Telugu, Malayalam, Panjabi, Thai
Note: in East Malaysia there are \several indigenous languages; most widely spoken are Iban and Kadazan
Ethnic groupsMalay 50.1%, Chinese 22.6%, indigenous 11.8%, Indian 6.7%, other 0.7%, non-citizens 8.2% (2010 est.)

AGE-SEXUAL COMPOSITION OF THE POPULATION
This entry provides the distribution of the population according to age.
Information is included by sex and age group (0-14 years, 15-64 years, 65 years and over).
The age structure of a population affects a nation's key socioeconomic issues.
Countries with young populations (high percentage under age 15) need to invest more in schools, while countries with older populations (high percentage ages 65 and over) need to invest more in the health sector
Age structure:
0-14 years: 28.8% (male 4,456,033/female 4,206,727)
15-24 years: 16.9% (male 2,580,486/female 2,511,579)
25-54 years: 41.2% (male 6,277,694/female 6,114,312)
55-64 years: 7.6% (male 1,163,861/female 1,122,746)
65 years and over: 5.5% (male 777,338/female 862,577) (2014 est.)

AGE PYRAMID

GROWTH OF MALAYSIA POPULATION.
Malaysia’s population has been growing, with forecasts that it will continue to grow –
The size of households is getting smaller . In 1970 there was an average of 5.5 people per household or, to put it another way, there were about 182 households for every 1,000 people.
By 2020 the forecast is that the average will be 4 people, or 250 households for every 1,000 people.
The number of households is therefore increasing at a faster rate than the growth of the population. This unalterable demographic fact is what is one of the drivers for housing demand.

MALAYSIA: POPULATION, URBANIZATION, EMIGRATION.
Median age total: 27.7 years male: 27.4 years female: 27.9 years (2014 est.)
Population growth rate 1.47% (2014 est.)Birth rate 20.06 births/1,000 population
(2014 est.)Death rate 5 deaths/1,000 population (2014
est.)Net migration rate -0.34 migrant(s)/1,000
population note: does not reflect net flow of an unknown number of illegal immigrants from other countries in the region (2014 est.)
Urbanization urban population: 72.8% of total population (2011) rate of urbanization: 2.49% annual rate of change (2010-15 est.)

CHARACTERISTIC OF THE POPULATION’S
HEALTH IN MALAYSIA

1. MORBIDITY AND INJURIES
The Institute for Public Health conducted the National Health and Morbidity Survey, NHMS in 2011. NHMS has been started since 1986.NHMS has been conducted for the fourth time in 2011

A. GENERAL INCIDENCE RATE OF THE POPULATION
COMMUNICABLE DISEASE
TB MALARIADYSENTARYMEASLES HEPATITIS
• NONCOMMUNICABLE DISEASE – HYPERTENSION– CANCER– DENGUE FEVER– OCCUPATONAL
INJURIES– STD– HIV

COMMUNICABLE DISEASES
Malaria has decreased markedly with better surveillance and prompt treatment.
TB is slightly increase possibly attributed to the increase in influx of immigrant workers into the country. These workers mostly originated from poor developing countries in the region.
Dysentery is decrease, might be attributed to improvement of water supply and basic hygiene.
Immunizable diseases shows decreasing in incidence due to wide coverage of immunization. The decline in Hepatitis B incidence may be attributed to the introduction of the National Hepatitis B immunization.

NON-COMMUNICABLE-
is increase in rates due to rapid economic growth. For example diseases such as cardiovascular diseases and nutrition.
HYPERTENSION incidence rate that showed a decline, incidence of cardiovascular disease rose by more than a 100%. Nutritional problems were reflected by increasing trends of obesity, protein malnutrition and by underweight births.
MALIGNANT CANCEr incidence rate had been reported to rise in 1997 compared to 1990.
DENGUE AND DENGUE HAEMORRHAGIC There had been a markedly tremendous increase in the incidence rate of this disease over a span of 7 years due to housing estates and construction sites.
WORK-RELATED ACCIDENTS AND OCCUPATIONAL INJURIES were also observed to have increased.
SEXUALLY TRANSMITTED DISEASES (SYPHILIS AND GONORRHEA) had shown a decline in incidence Rates.
HIV/AIDS were not reported prior to 1986. However, since then there has been an alarming increase in incidence of both HIV infections and AIDS.

DIABETES MELLITUS 15.2% (2.6 million) of adults 18 years and above have diabetes 7.2% are known to have diabetes 8.0% are previously undiagnosed with diabetes.
HYPERTENSION 32.7% (5.8 million) of adults 18 years and above have hypertension 12.8% are known to have hypertension 19.8% are previously undiagnosed with hypertension
HYPERCHOLESTEROLEMIA 35.1% (6.2 million) of adults 18 years and above have hypercholesterolemia 8.4% are known to have hypercholesterolemia 26.6% are previously undiagnosed with hypercholesterolemia

B. GENERAL PREVALENCE RATE OF THE POPULATION

D. INFECTIOUS MORBIDITY RATES
1. MEASLES 2. MALARIA 3. HIV/AIDS4. TB

MEASLESMeasles immunization which was introduced later in 1982.
By 1985, the immunization coverage with single dose of live attenuated vaccine at 9 months of age improved rapidly from 34.6% in 1986 to more than 85% in the late 1990s.
After 1987, the incidence of measles declined rapidly, falling from 33/100,000 population in 1987 to 2/100,000 population in 1998.

MALARIA• Every patient presenting at
the clinic with fever has screened for malaria.
• And from 1980, such efforts have produced a steep decline in the number of reported cases of malaria.
• The incidence then leveled off until the late 1990s when another drop in incidence occurred.
• Since 2000, the incidence has stabilized at the incidence rate of between 26 to 55/100,000 population

HIV/AIDSThe increasing prevalenceof HIV in Malaysia has yet to abate since the first reported cases in 1986.
The adult prevalence of HIV in Malaysia is presently at 0.5% .
There was three virtual peaks in 1992, 1996 and 2002, denoting that the source of transmissions is localized and continual.
Around 79% of HIV cases and 65.4% of AIDS cases in Malaysia are within the age group of 20 – 39 years

TUBERCULOSISIn 1990, there were only 6 cases of TB co-infection with HIV cases reported among the 10,873 TB cases.
The number had escalated to 933 cases or 6.5% of the total number of 14,389.
There is a sudden and shocking increase of 187 cases (25%) when compared to the 2001 report.

E. SELECTED CHRONIC DISEASES RATES

F. SUBSTANCE ABUSE DISORDERS: ALCOHOL
Among the current drinkers, the consumption prevalence was highest in • urban areas (9.0%, 95% Cl:
7.8,10.3), • males (12.1%, 95% Cl: 10.8,
13.7), other Bumiputras (21.6%, 95% Cl: 17.6, 26.3),
• age group between 25-29 years old (10.9%, 95% Cl: 8.7, 13.6),
• singles (12.2%, 95% Cl: 10.2,14.4),
• those with tertiary education (10.9%, 95% Cl: 9.1, 13.1),
Findings from NHMS 2015 showed a reduction in the prevalence of current drinkers in Malaysia as compared to findings from NHMS 2011.

TOBACCOOverall, the prevalence of current smoker was 22.8% (95%CI: 21.9, 23.8). There was a slight reduction from 23.1% reported in 2011.
It was estimatedthat nearly five million Malaysians aged 15 years and above smoked. The prevalence was highest in Sabah, followed by Kedah and Pahang.
The proportion of current smokers was 30 times higher among males compared to females (43.0%, 95%CI: 41.4, 44.6 vs 1.4%, 95%CI: 1.1, 1.8)
Significantly higher prevalence of tobacco use was observed among respondents in rural areas (27.9%, 95%CI: 26.3, 29.6), as compared to urban areas (21.2%, 95%CI: 20.1, 22.4).
Lower proportion of current smokers was observed among the 15-19 years old age group at 13.2% (95%CI: 11.5,15.2) and peaked at 35-39 years old age group at 17.4% (95%CI:15.3,19.7).
Approximately a quarter of Malays (24.7%, 95%CI: 23.6, 25.9) and other Bumiputras (25.8%,95%CI: 23.4, 28.4) were current smokers and their prevalence were remarkably higher than Chinese (14.2%, 95%CI: 12.7, 15.9) and Indians (16.5%, 95%CI: 14.0, 19.4).

G. INJURIESHOME INJURY (CHILDREN AND ELDERLY)
8.2% (0.1 million) of children below 7 years experienced home injury 5.3% (0.1 million) of elderly 60 years and above experienced home injury

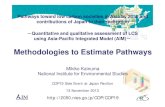
Cause-specific and age-specific incidence rates of disabilityThe disability incidence rate for a given year is the proportion of the exposed
population at the beginning of that year who become newly entitledExample : The modified male disability age-adjusted incidence rate equation to
disability benefits during the year.
DIMt = DIMtTR +1.47dimt-1 −0.63dimt-2 + εt
DIMt -male disability incidence rate in year t; DIMt
TR - male disability incidence rate from the TR04II in year t; dimt -deviation of the male disability incidence rate from the TR04II male disability incidence rate in year εt -random error in year t
2. DISABILITY

Distribution of disabled persons by groups
Male Disability Incidence Rate Calendar Years 1970-2003
Female Disability Incidence Rate, Calendar Years 1970-2003

CURRENT GOVERMENT PROGRAMS OF THE
ASSISTANCE AND SUPPORT OF DISABLED PERSONS1. Disabled Persons Policy System
Objective StatementOKU policy set following four objectives:1. Provide recognition and acceptance of the principle that people with disabilities have the same rights and opportunities for full participation in society.2. Ensure that disabled people enjoy the same rights, opportunities and equal access under the law of the country.3. Eliminate discrimination against any person by reason of incapacity, 4. Educate and raise public awareness about the rights of disabled people.

2. 1Malaysia People’s Aid (BR1M 2.0) System
Is a part of Government effort to ease burden of disabled people and lower income group in Malaysia.
3. Special Needs School for disabled students
- Malaysia offers early intervention programmes for children with special needs and mainstream children, catering to their individual development and growth.
CURRENT GOVERNMENT PROGRAMS OF THE ASSISTANCE AND SUPPORT OF DISABLED
PERSONS


ORGANIZATION OF THE HEALTH
SERVICE SYSTEM IN MALAYSIA

A. MODEL OF A HEALTH SERVICE SYSTEM
A. State sources of health service financing
GNP to the public health care services: 3.8% (2008), 4.6% (2009), 4.4% (2010).Public health services is almost free, only charged in certain services (outpatient – RM1 / 0.33USD; inpatient – max RM500 / USD 166.67 for non gov. servants).Private health services require payments, or co-payments with private health insurance coverage.
B. System of medical insurance Private insurance is voluntarily purchased by individuals.- Charged based on the health
status, type of insurance and level if coverage of insurance.
Occupational insurance- In the private sectors who earns
less than RM3000 a month are protected by the Employee's Social Security Act 1969 (ESSA 1969).
- They are covered under two insurance schemes; Employees' Injury Scheme and Invalidity Pension Scheme


PRIVATE MEDICAL INSTITUTIONS. PAID MEDICAL SERVICE FORMSMalaysia has a widespread system of health care. Healthcare in Malaysia is divided into user-charged private sector and subsidised public sector.
Government / public hospitals - 151 MOH hospitals (2013)
Government clinics (health centres, rural / community clinics, maternal and child health clinics, mobile clinics, dental clinics, mobile dental clinics) - about 5300 (2008)
Private hospitals and medical centers - ~130 (2013)
Private practitioner clinics - ~6k-7k private clinics owned by doctors, registered with Malaysian Medical Council).
Some private hospitals are established as charitable institutions.
Private insurance is voluntarily purchased by individuals, who pay different premiums depending on the type of health insurance and level of coverage.
Examples of non profitable organizations: MERCY Malaysia, UNICEF Malaysia.
Public sectorPrivate sector

MEDICAL INSTITUTIONSGovernment Medical Institutions
The main public health provider is MOH that provides primary care, secondary care and tertiary care.
An open-door policy in regard to general outpatient services and hospital admissions has been practiced by the public health sector.
Access to specialist services is nonetheless controlled through a national system of referral.
Specialist services are available at designated hospitals.
Private Medical Institution
Private health providers - “complement”.
Private hospitals exist in a variety of sizes. Newly built private hospitals are equipped with large, ultramodern and lavish medical technology.
Private general practitioners' clinics - convenient medical service.
The private facilities are monitored and regulated (implementation of Private Health Care Facilities and Services Act 1998) by the Malaysian government to ensure quality service and cost control. It expresses specific requirements for facility standards and the assurance of quality services in accordance with the National Quality Assurance Programme.
The expense of utilizing health services at private facilities (represented by their user fees) is higher than at public facilities.

MALARIA – TRENDS AND PATTERN
Malaysia has achieved major success in virtually eliminating malaria from urban and other densely populated areas.

MALARIA – ERADICATION PROGRAMS
Vector –Borne Diseases Control Programme and Strategies
At the national level, the Vector-Borne Diseases Control Programme (VBDCP) is a dedicated section under the Disease Control Division of the Public Health Department, MOH.The specific objectives of the national malaria control programs are
- to reduce malaria morbidity and mortality- to prevent re-establishment of malaria in areas with no
indigenous cases

TUBERCULOSIS – TRENDS AND PATTERN

TUBERCULOSIS – ERADICATION PROGRAMS
Strategies - BCG vaccination for all newborn babies- Screening of symptomatic cases and high-risk
groups, including mandatory screening of foreign workers and HIV patients in prisons and drug rehabilitation centers
- Raising awareness of the disease through mass media
- Training health staff about the disease- Conducting research relating TB epidemiology and
treatment outcomes, including national TB prevalence study and a multi drug resistance survey.

LEPROSYIn order to protect the inhabitants from being infected by leprosy, enacted draconian laws to forcibility isolate those suffering from the disease of leprosy from the other inhabitants.These unfortunate human beings treated more as sub-humans were forcibility isolated into very remote camps in the deep jungle in placesThe Malaysian Leprosy Relief Association (MaLRA) was founded by The late Senator Tan Sri T H Tan in 1959.Objectives of this association & what MaLRA does?
To assist in the prevention, treatment and control of leprosy with a view of its ultimate eradication by:
- assisting and encouraging leprosy patients to seek early treatments;- looking after the welfare of leprosy patients and dependants during
isolation and treatment;- rehabilitating cured leprosy patients;- combating prejudice against the disease of leprosy;- making every effort to eradicate the disease of leprosy.

B. THE MANAGEMENT OF A HEALTH SERVICE SYSTEM

ORGANIZATION OF HOS PITAL CARE TO URBAN POPULATION
KINDS OF MEDICAL AIDIn Malaysia, there are non MoH hospitals and 4 types of hospitals under MoH:
District Hospital : 100-200 bedsState General Hospital : 500 – 1500 bedsNational Referral Center
is the highest level of hospital in hierarchy. Has 2800 beds and situated in KL receives referral from all over the country eg: neurosurgery
Special Institutions present 7 institutions providing service for specific diseaseThey are:
National TB CenterHospital for Leprosy5 mental hospitals



• Structure of Urban Hospitals• Administrative
division• Reception/Registration• Emergency
Department• Outpatient
department• Pharmacy• Medico-diagnostic • Department• Specialized and • Rehabilitative
Units• Reanimation and
Operative• Units• Pathological Units
• District and State Hospital provide outpatient and inpatient care by both specialist and non-specialist MOs in: General Surgery Pediatrics Medicine Obgn Psychiatry
• Hospitals can also be divided into Specialized Hospitals Nonspecialized Hospital
• These hospitals are classified such based on the fact whether present or not any Specialist working at the Hospitals

INDICES OF PROVISION OF THE POPULATION WITH HOSPITAL BEDS (PER 10 000 PERSONS)
Is the availability of number of beds to 10000 populationProvision of Population with Hospital Beds in Malaysia: 19 beds for 10000 inhabitantsMalaysia ranked at the 100th position while Russia is at 3rd position with 105 beds according to World Health Statistics by WHO

FREQUENCY OF HOSPITALISATION
(PER 1000 PERSONS)Frequency of Hospitalization in Malaysia is: 74 per 1000 inhabitants which is lesser compared with Russia (190 for 1000 inhabitants)
The percentage of the population admitted to MOH hospitals varied significantly for various states. Perlis and Negeri Sembilan had the highest percentage of admissions with 10.5% and 9.9% respectively while the lowest percentages were found in Kedah and Penang with 1.3% and 1.4% respectively.

AVERAGE DURATION OF THE PATIENT STAY IN HOSPITAL
The Average Length Of Stay In Hospitals (ALOS) is one measure of the efficiency with which hospital resources are used
This refers to the number of days (with an overnight stay) that patients spend in an acute-care inpatient institution.It is generally measured by dividing the total number of days stayed by all patients in acute-care inpatient institutions during a year by the number of admissions or discharges.The ALOS in Malaysia In MoH Institutes 3.23 days In Private Hospitals is 3.37 days
The state of Perlis had the longest ALOS of 3.70 days, versus the shortest ALOS of 2.30 days in Johor.

HOSPITAL LETHALITY AND OTHER INDICATORS OF HOSPITAL ACTIVITY
ICU Mortality in MoH hospitals: 21.5%
In-hospital mortality rates in MoH hospitals: 29.5%
Work Loading of Medical personnel 1 Doctor for 791
inhabitants 1 Nurse for 387 inhabitants
Overall Bed Occupancy Rate (BOR) for MoH hospitals is 68.63%
Bed Turnover: 59 Patients To 1 Bed in Average

D.ORGANIZATION OF MEDICAL CARE TO RURAL POPULATION
Population with difficulties to medical access:Orang Asli and PenansEstate Workers People on small islands
Two notable programme for in improving access to care for rural population.Flying doctor services970 location in Sarawak, 51 location in Sabah and KelantanAverage patient attendences range from 75,000 – 90,000 per year including 300- 400 emergency medical evacuation cases.MOH mobile health teams193 mobile health teams outreach services to remote population in 2008.
“Telemedicine” is a programme for rural population to get access with medical specialists. It is reported that 90% of rural population now have access to a doctor , with health clinics every 5km.

E. THE MAIN PRINCIPLES OF EMERGENCY CARE ORGANIZATION
Managed by paramedics and 90% of clinics are equipped with ambulances.Strengthening capacity to respond to increasing numbers of accidents and emerge ncies requires standardizing clinical treatment, referral protocols and providing better equipment.Ambulance services in Malaysia are provided by Ministry of health, Red Crescent, St. Johns’ Amulance, Civil Defence Department.National emergency call center network directs emergency callls, arangges communications between hospital emergency departments, organize telemedicine and has mobile medical teams.

F. THE SYSTEM OF PROTECTION OF MOTHERHOOD AND CHILDHOOD
Child Act 2001Core principles are non-discrimination, best interest od child, the right to life, survival and development of the childRepealed Juvenile Courts Act 1947 , Women and Girls Protection Act 1973, and Child Protection Acy 1991 Setting up Child Protection Teams and Child Activity Centres at district and state levels for children at risk or vulnerable children to all forms of exploitation and abuse.Provides Court of Children which is child-friendly taking into account the mental and emotional maturity of a child.

FAMILY PLANNING
With the launching of the National Planning Program in conjunction with the First Malaysia Plan in 1966, family planning became an official policy.
The aim: To improve maternal and child health & decelerating the rate of population growth from 3% in 1966 to 2% in 1985 by setting targets to increase the number of family planning acceptors
The National Family Planning Board was established to plan, execute and coordinate all family planning activities in the country.
The program began with the provision of clinical contraceptive services mainly in the urban areas.
Subsequently, the National Program was expanded to the rural areas through the integration of family planning with primary health care services of the Ministry of Health in the early 1970s.


MATERNAL AND CHILD HEALTH INDICATORS
The 8th Millennium Developement Goals (MDG) for the world include reducing child mortality and improving meternal health. Malaysia has reduced differentials in maternal and child mortality between Bumiputera and other ethnic groups and among states through more equitable social and economic development and better health services.



It is Government's responsibility to protect and advance the interests of society & includes the delivery of high-quality health care.
The ultimate goal of achieving high quality of care will require strong partnerships among federal, state, and local governments and the private sector.
The Malaysian health care system requires doctors to perform a compulsory three years service with public hospitals to ensure that the manpower in these hospitals is maintained.
Doctors are required to perform 4 years including 2 years of housemanship and 2 years government service with public hospitals throughout the nation, ensuring adequate coverage of medical needs for the general population.
Foreign doctors are encouraged to apply for employment in Malaysia, especially if they are qualified to a higher level.
CONCLUSION

ANNUAL REPORT MALAYSIAN MINISTRY OF HEALTH 2012 HEALTH INFORMATICS CENTRE, PLANNING AND
DEVELOPMENT DIVISION, MINISTRY OF HEALTH MALAYSIA HEALTH AT A GLANCE ASIA/PACIFIC 2012, WHO HEALTH INFORMATICS CENTRE, MINISTRY OF HEALTH
MALAYSIA MALAYSIA HEALTHPLAN 2008, MINISTRY OF HEALTH
MALAYSIA 10TH MALAYSIA PLAN - 1CARE FOR 1MALAYSIA, MINISTRY
OF HEALTH MALAYSIA
BIBLIOGRAPHY

Although the quantity rather than quality of health services has been the focus historically in developing countries, evidence suggests that quality of care (or the lack of it) must be at the center of every discussion about better health.
Quality comprises three elements: 1. Structure refers to stable, material characteristics (infrastructure, tools,
technology) and the resources of the organizations that provide care and the financing of care (levels of funding, staffing, payment schemes, incentives).
2. Process is the interaction between caregivers and patients during which structural inputs from the health care system are transformed into health outcomes.
3. Outcomes can be measured in terms of health status, deaths, or disability-adjusted life years—a measure that encompasses the morbidity and mortality of patients or groups of patients. Outcomes also include patient satisfaction or patient responsiveness to the health care system (WHO 2000).
SUGGESTION