Mag. Herbert Maier Platelet Function Testing PFA-100 ® System Clinical Indications.
28
Mag. Herbert Maier Platelet Function Testing PFA-100 ® System Clinical Indications
Transcript of Mag. Herbert Maier Platelet Function Testing PFA-100 ® System Clinical Indications.

Mag. Herbert Maier
Platelet Function Testing
PFA-100® System
Clinical Indications

HM 2
Overview of the PFA-100® Test System
Overview
Introduction
Overview of the Test System
Test Principle
Intended Use and Clinical Performance
PFA-100® compared to Bleeding Time
VWD and DDAVP
Acetyl Salicylic Acid (ASA, Aspirin® - Bayer)
Use of PFA in:
Pre-surgical screening and Bleeding Risk management
Risk Stratification of CVD patients
Transfusion medicine

HM 3
PFA-100® Platelet Function Analyzer
Trigger solution container
Soft keys
LCD screen
Built-In Printer
Carousel
Cassette
Test Cartridge

HM 4
PFA-100® Test Principle
before after
apertureØ150 µM
cup
Platelet plug
Filter+
epinephrineor ADP
flash membrane
800 µl blood
capillaryØ 200 µM
collagen
p = -40 mBar

HM 5
high shear rate>5000 /s
high shear rate>5000 /s
PFA-100® Test Principle
PFA-100®
capillary 200µm
Epinephrine or
ADP membrane with
platelet
von Willebrand Factor
erythrocyte
FLOW
collagen coating
To: Poujol, Nurden, Paponneau, et al.
In Vivo Haemostasis
lumen
fibrinogen
platelet
collagen fibrils
erythrocyte
von Willebrand Factor
endothelial cell
HM 6
Simulates in-vivo conditions; high shear such as
present in small arteries (CVD)
High shear increases the sensitivity to vWF
abnormalities
Assesses the effect of anti-platelet agents under
physiological conditions*
*also recommendation of subcommittee on Biorheology - ISTH 1999
PFA-100® Test Principle - summary

HM 7
Col/EpiCol/ADP
3.8% (129mM) buffered Sodium citrate;90% Central Interval (sec)**: 85 - 165 71 -
118
** : data based on testing of 127 samples with normal platelet function in Germany
** Dade® PFA-100® System Package Insert
Expected Normal Ranges
Expected Values

HM 8
Comparison of the PFA-100® with skin Bleeding Time test
To : Mammen, Comp, Gosselin, et al..
0
1
0 1
Sen
siti
vity
1 - Specificity
PFA-100 ®
Bleeding Time test
PFA-100®
Area Under Curve 0.98 0.70Error 0.01 0.04
Bleeding Time test
Populations:
206 normals176 abnormals
PFA-100® Clinical Performance

HM 9
Sensitivity of PFA-100® System for Platelet Dysfunction
* with Dade® PFA-100® Col/Epi Cartridge (based on meta-analysis of 15 studies)
E.J. Favoloro. Haemophilia 2001; 7:170-179
GT
Cases
Sensitivity (%)
BSS SPD
Sensitivity for Platelet Dysfunction
14
100%
HPS ASA
2
100%
16
75%
11
91%
127
95%
Overall sensitivity for platelet disorders: 91%

HM 10
Sensitivity of PFA-100® System for vWD
1
Cases
Sensitivity (%)
2A 2B
Sensitivity for von Willebrand Disease Type
174*
88%
2M 3 Acquired
33
100%
36
92%
12
100%
31
100%
8/8
100%
Overall sensitivity for VWD: 92%

HM 11
Fressinaud et al. British Journal of Haematology 1999;106(3):777-783.
Correction of Primary Hemostasis in vWD patients
VWD patient management with DDAVP
HM 12
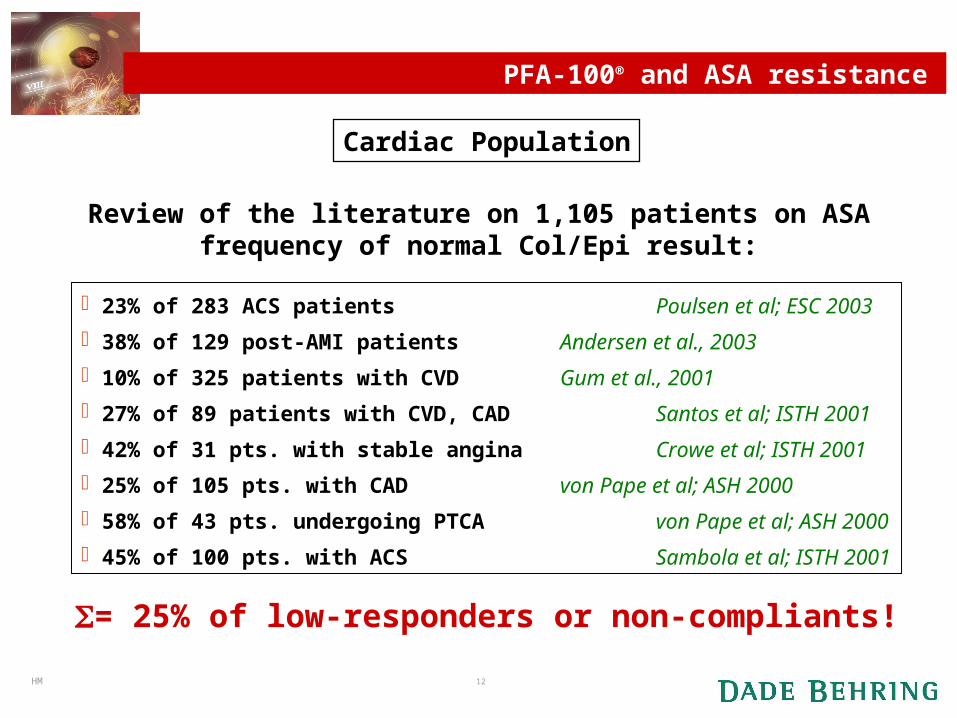
23% of 283 ACS patients Poulsen et al; ESC 2003
38% of 129 post-AMI patients Andersen et al., 2003
10% of 325 patients with CVD Gum et al., 2001
27% of 89 patients with CVD, CAD Santos et al; ISTH 2001
42% of 31 pts. with stable angina Crowe et al; ISTH 2001
25% of 105 pts. with CAD von Pape et al; ASH 2000
58% of 43 pts. undergoing PTCA von Pape et al; ASH 2000
45% of 100 pts. with ACS Sambola et al; ISTH 2001
= 25% of low-responders or non-compliants!
Review of the literature on 1,105 patients on ASAfrequency of normal Col/Epi result:
Cardiac Population
PFA-100® and ASA resistance

HM 13
• 33% of 118 cerebral ischemia patients Hanswillemenke et al; GTH 2002
• 37% of 129 cerebrovascular patients Alberts et al., 2004
• 23% of 53 cerebrovascular patients Grundmann et al., 2003
= 33% of low-responders or non-compliants!
Review of the literature on 300 patients on ASAfrequency of normal Col/Epi result:
Stroke Population
PFA-100® and ASA resistance

HM 14
There is a correlation between ASA non-responsiveness measured by PFA-100® and
clinical events!
Patients with AMI had 38% ASA non-responders compared to 18% for non
AMI patients
Poulsen et al., 2003
The event rates was 36% in the post-AMI group of ASA non-reponders,
compared to 24% for the responders
Andersen et al., 2003
Patients with recurrent cerebral ischemia attacks had 30% ASA non
responders, compared to 15% for patients with stable clinic
Hanswillemenke et al; GTH 2002
Symptomatic cerebral ischemia patients had 34% ASA non-responders,
compared to 0% for the asymptomatic group
Grundmann et al., 2003
Review of the literature on 552 patients with clinical data
PFA-100® and ASA resistance

HM 15
Conclusion: aspirin non-responders
Poor response to aspirin has been found in
1. Acute coronary syndromes, where it predicted deaths2. Late venous graft occlusion after bypass3. Recurrent TIA
ACS patients with aspirin home therapy could also profit from additional aspirin infusion (Fuchs & Jilma)

HM 16
Acesal Tbl., 500 mg Acesal-Calcium, 250 mgAcetylin Tbl., 500 mg Acetylsalicylsäure 500 PB, 500 mgAcetylsalicylsäure Tbl. Michallik, 500 mg Alacetan N Tbl., 250 mgAlka-Seltzer Brausetbl., 325 mg Antineuralgie Tbl. Scheurich, 250 mgAsasantin Tbl., 330 mg Aspirin Tbl., 500 mg, 300 mg, 100 mgAspirin direkt Kautbl., 500 mg Aspirin plus C Brausetbl., 400 mgAspirin protect, 100 und 300 mg Aspisol Amp., 500 mgAspro Tbl., 320 mg ASS-AbZ Tbl.ASS Bonfal Infarktschutz Tbl., 75 mg ASS 100/500 Hexal Tbl.ASS dura Tbl., 500 mg ASS Kreuz, 500 Tbl.ASS 100 Tbl. Lichtenstein ASS light 100 AzupharmaASS Kombi ratiopharm Brausetbl., 300 mg ASS mini Tbl., von CT, 50 mgASS ratiopharm Tbl., 100, 300, 500 mg ASS +C Braustbl. 500 mgASS Stada 100/500 Tbl.-Boxazin plus C Br.-tbl., 500mg ASS opt. Tbl., 500 mg
Boxonal Tbl., 210 mg CC-ASS-500 Tbl., 500 mg
CC-Cor Tbl., 30 mg CC-forte Tbl., 250 mgCebion Erkältungsbrausetbl., 50 mg Chephapyrin N Tbl., 250 mgCoffalon Tbl., 200 mg (Calicylamid) Coffetylin Tbl., 450 mg
Contradol Pastillen-Dolomo TN Tbl., 250 mg Dolviran N Tbl., 500 mgDoppel-Spalt compact Tbl., 500 mg Dorocoff-ASS plus Tbl., 400 mg
ASA-containing Medication in Germany (1)
(Koscnielny, personal communication)
*All medications are listed registered trade marks from various companies

HM 17
Gelonida NA supp. für Ki/Erw., 125 mg/500 mg Glutidal Tbl., 400 mg (Salicylamid)Godamed 100/500 Tbl., 100 /500 mg Godasal Tbl., 500 mg-HA-Tbl.N., 250 mgHerz ASS ratiopharm 50/100 Tbl., 50 mg/ 100 mg Hermes ASS plus Tbl., 400 mg
Malinert Tbl., 325 mg Melabon K Tbl., 250 mgMelanbon+C Brausetbl., 500 mg Menostabil-ASS Tbl.Mentopin Vit. C+ASS Brausetbl., 500 mg Micristin Tbl., 500 mgMiniasal Tbl., 30 mg Neuralgin Tbl., 250 mgNeuranidal Tbl., 300 mg Neuranidal Duo Brausetbl., 400 mgOrtoton Plus Tbl., 400 mg Pono-ASS Kaps. Praecineural Tbl., 350 mg und supp. 500 mg Pyracil N Tbl.Quadronal ASS comp. Tbl., 460 mg Ring N Tbl., 300 mgRio-Josipyrin N Tbl., 250 mg Romigal ASS 500 Tbl., 500 mg
Santasal N Tbl., 500 mg Spalt ASS Tbl., 600 mgSpalt A+P Tbl., 300 mg Spalt plus Tbl., 250 mg
Temagin ASS 600 Tbl., 600 mg Temagin PAC Tbl., 250 mgTempil N Kaps., 250 mg Thomapyrin Tbl., 250 mgThomapyrin C Brausetbl., 300 mg Togal Tbl., 250 mgTogal Kopfschmerzbrause + Vit.C, 500 mg Togal ASS Tbl., 400 mg
Werodon-ASS Tbl.
ASA-containing Medication in Germany (2)
(Koscnielny, personal communication)
*All medications are listed registered trade marks from various companies

HM 18
PFA-100® in Preoperative Screening
The Berlin Experience* - Set Up
During 2000, 5649 patients, filled in a questionnaire dedicated to bleeding observations
• Results pos.resp. pred.value
– prolonged bleeding 5.7% 8.2%
– high frequency of “blue spots” 5.1% 65.4%
– NSAID’s 3.6% 83.9%
– Menorrhagia 4,5%
• All patients were tested with a panel of screening tests:Platelet Count, APTT, PT, PFA-100 (Col/Epi and Col/ADP)
Patients, with a positive bleeding history (11.2%), were tested with two additional tests; BT (Surgicutt®), VWF:Ag.
* Koscielny J, et al. Clin Appl Thrombosis/Hemostasis 2004; 10(3): 195-204
HM 19
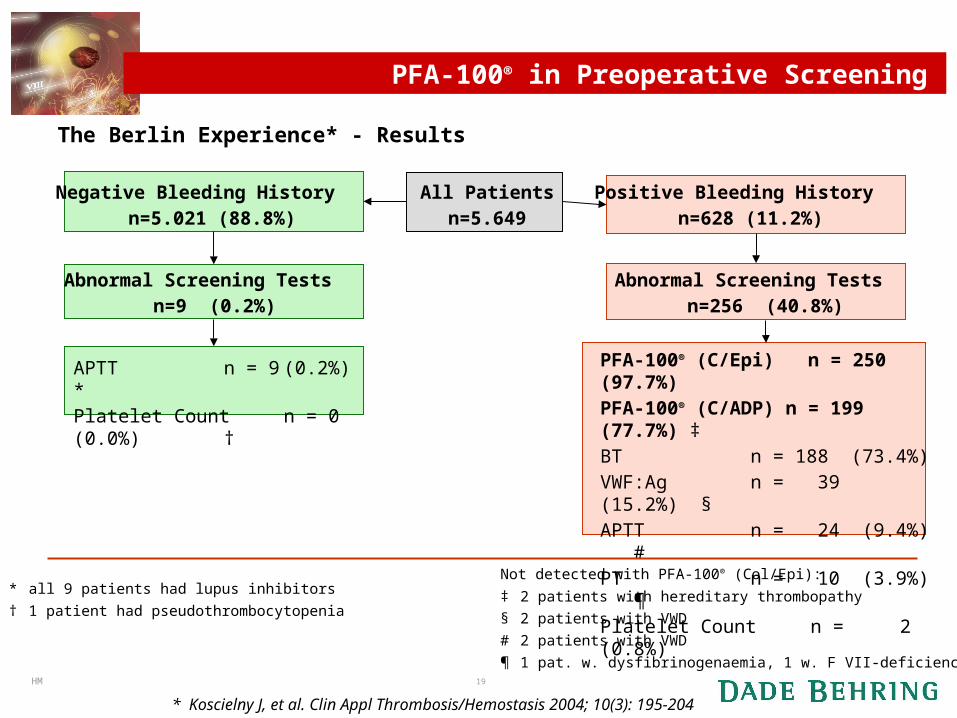
PFA-100® in Preoperative Screening
The Berlin Experience* - Results
* Koscielny J, et al. Clin Appl Thrombosis/Hemostasis 2004; 10(3): 195-204
All Patientsn=5.649
Negative Bleeding History n=5.021 (88.8%)
Abnormal Screening Tests n=9 (0.2%)
Positive Bleeding History n=628 (11.2%)
PFA-100® (C/Epi) n = 250 (97.7%) PFA-100® (C/ADP) n = 199 (77.7%) ‡BT n = 188 (73.4%)VWF:Ag n = 39 (15.2%) §APTT n = 24 (9.4%) #PT n = 10 (3.9%) ¶Platelet Count n = 2 (0.8%)
APTT n = 9 (0.2%) *Platelet Count n = 0 (0.0%) †
* all 9 patients had lupus inhibitors
† 1 patient had pseudothrombocytopenia
Not detected with PFA-100® (Col/Epi):
‡ 2 patients with hereditary thrombopathy
§ 2 patients with VWD
# 2 patients with VWD
¶ 1 pat. w. dysfibrinogenaemia, 1 w. F VII-deficiency
Abnormal Screening Tests n=256 (40.8%)
HM 20
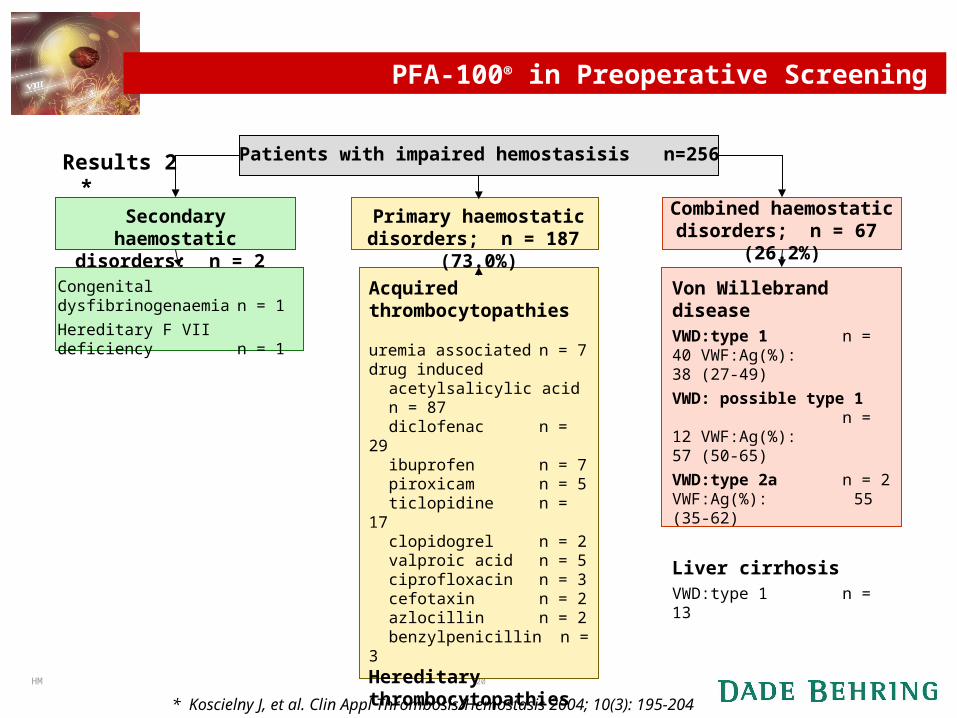
PFA-100® in Preoperative Screening
Results 2 *
* Koscielny J, et al. Clin Appl Thrombosis/Hemostasis 2004; 10(3): 195-204
Patients with impaired hemostasisis n=256
Secondary haemostatic disorders; n = 2 (0.8%)
Congenital dysfibrinogenaemian = 1
Hereditary F VII deficiency n = 1
Combined haemostatic disorders; n = 67 (26.2%)
Von Willebrand disease
VWD:type 1 n = 40 VWF:Ag(%): 38 (27-49)
VWD: possible type 1 n = 12 VWF:Ag(%): 57 (50-65)
VWD:type 2a n = 2 VWF:Ag(%): 55 (35-62)
Liver cirrhosisVWD:type 1 n = 13
Acquired thrombocytopathiesuremia associated n = 7drug induced
acetylsalicylic acid n = 87diclofenac n = 29ibuprofen n = 7piroxicam n = 5ticlopidine n = 17clopidogrel n = 2valproic acid n = 5ciprofloxacin n = 3cefotaxin n = 2azlocillin n = 2benzylpenicillin n = 3
Hereditary thrombocytopathiesGlanzmann Thromb. n = 1Bernard-Soulier S. n = 1Secretion Defects n = 16
Primary haemostatic disorders; n = 187 (73.0%)
HM 21
PFA-100® in Preoperative Screening
Conclusions*
The vast majority of these patients could not be identified by routine screening for PT, APTT and Platelet Count
250 of these patients (256) are detected with the PFA-100® (Col/Epi)
A combination of all tests, without PFA-100® would miss up to 30% of the patients at risk for bleeding!
The PFA-100® (Col/Epi) demonstrated a PPV of 81.8% and NPV of 93.4% for impaired hemostasis
The PFA-100® system is clearly superior to the bleeding time.
* Koscielny J, et al. Clin Appl Thrombosis/Hemostasis 2004; 10(3): 195-204

HM 22
PFA-100® in Preoperative Screening
Recommendations*
For patients needing a pre-surgical work-up, a test panel without the PFA-100® (Col/Epi) is insufficient.
Patients with increased risk for bleeding complications can be identified using a standardized questionnaire and a test panel comprised of PFA-100® (Col/Epi), VWF-Ag, PT and APTT.
The PFA-100® (col/Epi) is important also for assessing the therapeutic efficacy of drugs such as aspirin and desmopressin acetate (DDAVP)
* Koscielny J, et al. Clin Appl Thrombosis/Hemostasis 2004; 10(3): 195-204

HM 23
Preoperative management of patients with impaired hemostasis
The Berlin Experience* - Results
The administration of DDAVP led to a correction of platelet dysfunction in 229 of the 254 patients treated (90.2%).
In patients with corrected impaired hemostasis the number of blood transfusions was non-significantly lower (9.4% vs. 12.2%; p = 0.202), than in patients without impaired hemostasis.
In a retrospective group of patients with non-corrected impaired hemostasis, the number of blood transfusions was significantly higher (89.3% vs. 11.3%; p < 0.001) than in patients without impaired hemostasis.
* Koscielny J, et al. Clin Appl Thrombosis/Hemostasis 2004; 10(2): 155-166

HM 24
Preoperative management of patients with impaired hemostasis
0
20
40
60
80
100
1999 retrospective 2000 prospective
Results * Retrospective study n=5102
Prospective studyn=5649
Corrected Impaired
n=256
Non-corrected normalsn=5393
transfusedn=24 (9,4%)
transfusedn=660 (12,2%)
Non-corrected Impairedn=317
Non-corrected normals
n=4785transfused
n=283 (89,3%)transfused
n=541 (11,3%)
Tra
nsf
use
d (
%)
p < 0.001
p = 0.202
Elective operations
* Koscielny J, et al. Clin Appl Thrombosis/Hemostasis 2004; 10(2): 155-166

HM 25
Platelet Function in Patients with Acute MI*
Set-up
Patients with acute chest pain or symptoms suggestive of acute coronary
syndromes (n=216) were prospectively examined at an emergency unit.
Results
COL/ADP-CT was significantly shorter in MI patients, than in other patient
groups (unstable angina, stable coronary artery disease), or controls.
Furthermore, COL/ADP-CT and COL/EPI–CT at presentation were
independent predictors of myocardial damage as measured by CK-MB or
TnT.
Patients with MI whose COL/ADP-CT values fell in the first quartile had
3-fold higher CK-MB and TnT levels than those in the fourth quartile.
* Frossard M, et al. Circulation. 2004;110:1392-1397

HM 26
Potential applications for PFA-100 in transfusion medicine
Quality control of platelet concentrates
– Collection (van der Boehlen et al. 2001, Feuring et al. 2001)– Storage (Beck et al. 2002, Borzini et al. 1999)– Cryo-Preservation (Borzini et al. 1999, 2000)
Therapeutic monitoring (e.g. DDAVP)
» Eriksson et al. Vox Sang 1996
Peri-operative transfusion management
– Platelet concentrates (Raman et al. 2001)

HM 27
Conclusion
INDICATIONS FOR PFA-100
BLEEDING Screening for VWD and platelet dysfunction Transfusion medicine: donor screening, transfusion efficacy Menorrhagia: screening for platelet defect / VWD Surgery: patients with high risk for platelet dysfunction or vWD
THROMBOSIS Detection of aspirin non-responsiveness and platelet hyperactivity

HM 28
The End
Thank you for your attention!Thank you for your attention!
Any Questions???