Louis Appleby Professor of Psychiatry University of Manchester Chair, National Suicide Prevention...
33
Louis Appleby Professor of Psychiatry University of Manchester Chair, National Suicide Prevention Advisory Group Department of Health
-
Upload
calvin-wiggins -
Category
Documents
-
view
216 -
download
1
Transcript of Louis Appleby Professor of Psychiatry University of Manchester Chair, National Suicide Prevention...

Louis Appleby Professor of Psychiatry
University of Manchester
Chair, National Suicide Prevention Advisory Group
Department of Health

National Suicide Prevention Strategy: Six actions
• Reduce risk in high risk groups • Tailor approaches to improve mental health in
specific groups• Reduce access to the means of suicide • Provide better information and support to those
bereaved or affected by suicide • Support media in delivering sensitive approaches
to suicide• Support research, data collection and monitoring

Suicide rates, England 1994-2012
Age standardised death rate per 100,000 population
Source: ONS
3-year average

Suicide rates by age and gender, England 2012
Source: ONS

Suicide in young men
0
5
10
15
20
25
30
1973 1978 1983 1988 1993 1998 2003 2008
Age standardised death rateper 100,000 population
Males 20-34
Persons, All Ages
Three-year average rate, plotted against final year of average
Males 35-49
Source: ONS
2010

UK(1996-2012)
England(1996-2012)
Wales(1996-2012)
Scotland(1997-2012)
N. Ireland(1997-2012)
N N N N N
Generalpopulation
100,329 78,170 5,475 13,235 3,449
In contact withservices
26,216(26%)
20,300(26%)
1,260(23%)
3,705(28%)
951(28%)
National Confidential Inquiry: suicides

Patient suicides: age and gender profile
7%
18%
27%
22%
14%
7%
5%7%
14%
22%23%
18%
10%7%
0
500
1000
1500
2000
2500
Under 25 25-34 35-44 45-54 55-64 65-74 75+
Nu
mb
er o
f p
atie
nts
Age-group
Male Female
ENGLAND_SUICIDE (2002-2012)© National Confidential Inquiry into Suicide and Homicide by People with Mental Illness. All rights reserved.Not to be reproduced in whole or part without the permission of the copyright holder.

2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 20120
200
400
600
800
1000
1200
1400
1250 1256
13171277
1123 1139
1209
11541227
1215
771
1272
Estimated Confirmed
Year
Nu
mb
er
of
pa
tie
nts
130713061242761234
Patient suicide - England
ENGLAND_SUICIDE (2002-2012)© National Confidential Inquiry into Suicide and Homicide by People with Mental Illness. All rights reserved.Not to be reproduced in whole or part without the permission of the copyright holder.

ENGLAND_SUICIDE (2002-2012)© National Confidential Inquiry into Suicide and Homicide by People with Mental Illness. All rights reserved.Not to be reproduced in whole or part without the permission of the copyright holder.
Patient suicide method - England
2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 20120
100
200
300
400
500
600
700
456 456
515487
456 472
549
479
584556
615
336345
379
339
272281 289
328 326
372
332
198 210182 192
206 198 198217
182160
144
Hanging/strangulation Self-poisoning Jumping/multiple injuries
Year
Nu
mb
er o
f p
atie
nts

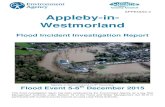
Patient suicides: primary diagnosis by gender
ENGLAND_SUICIDE (2002-2012)© National Confidential Inquiry into Suicide and Homicide by People with Mental Illness. All rights reserved.Not to be reproduced in whole or part without the permission of the copyright holder.

Living circumstances: patient suicides
Alone 5768 (46%)
With parent(s)1435 (11%)
With spouse/partner (with or without
children)3793 (30%)
With children only555 (4%)
Other shared (e.g. friends)
651 (5%)
Prison/YOI70 (1%)
Other specified310 (2%)
ENGLAND_SUICIDE (2002-2012)© National Confidential Inquiry into Suicide and Homicide by People with Mental Illness. All rights reserved.Not to be reproduced in whole or part without the permission of the copyright holder.

Timing of last contact: patient suicides
18%
32%
22%
13%14%
0
500
1000
1500
2000
2500
3000
3500
4000
4500
< 24 hours 1-7 days 1-4 weeks 5-13 weeks More than 13weeks
Nu
mb
er o
f p
atie
nts
ENGLAND_SUICIDE (2002-2012)© National Confidential Inquiry into Suicide and Homicide by People with Mental Illness. All rights reserved.Not to be reproduced in whole or part without the permission of the copyright holder.

Mental health teams’ estimation of suicide risk at last contact: patient suicides
12%
48%
31%
9%
28%
58%
12%
2%0
1000
2000
3000
4000
5000
6000
7000
8000
No risk Low Moderate High
Nu
mb
er o
f pat
ien
ts
Suicide risk
Long-term risk Immediate risk
ENGLAND_SUICIDE (2002-2012)© National Confidential Inquiry into Suicide and Homicide by People with Mental Illness. All rights reserved.Not to be reproduced in whole or part without the permission of the copyright holder.

UK(1996-2012)
N
England(1996-2012)
N
Wales(1996-2012)
N
Scotland(1997-2012)
N
N. Ireland(1997-2012)
N
Generalpopulation
10,974 8,959 416 1,329 270
In contact withservices
1,133(10%)
866(10%)
44(11%)
191(14%)
32(12%)
Homicide convictions
UK_HOMICIDE © National Confidential Inquiry into Suicide and Homicide by People with Mental Illness. All rights reserved.Not to be reproduced in whole or part without the permission of the copyright holder.

Primary diagnosis of patient homicides (based on Inquiry questionnaire data)
ENGLAND_HOMICIDE (2002-2012)© National Confidential Inquiry into Suicide and Homicide by People with Mental Illness. All rights reserved.Not to be reproduced in whole or part without the permission of the copyright holder.
Other
Personality disorder
Drug dependence/misuse
Alcohol dependence/misuse
Affective disorder
Schizophrenia and other delusional disorders
0 20 40 60 80 100 120 140 160 180
11%
16%
16%
13%
13%
30%
Number of patients

Secondary diagnosis of patient homicides (based on Inquiry questionnaire data)
ENGLAND_HOMICIDE (2002-2012)© National Confidential Inquiry into Suicide and Homicide by People with Mental Illness. All rights reserved.Not to be reproduced in whole or part without the permission of the copyright holder.
Other
Dementia
Anxiety/phobia/panic disorder/OCD
ADHD/conduct disorder
Pervasive development disorder/autistic
Learning disability
Organic disorder
Adjustment disorder/reaction
Personality disorder
Drug dependence/misuse
Alcohol dependence/misuse
Affective disorder
0 20 40 60 80 100 120
1%
1%
5%
1%
1%
1%
1%
4%
17%
30%
25%
17%
Number of patients

Mental health teams’ estimation of risk of violence at last contact: patient homicides
ENGLAND_HOMICIDE (2002-2012)© National Confidential Inquiry into Suicide and Homicide by People with Mental Illness. All rights reserved.Not to be reproduced in whole or part without the permission of the copyright holder.
No risk Low Moderate High0
50
100
150
200
250
33%
38%
22%
7%
48%
42%
8%
1%
Long-term risk
Immediate risk
Risk of violence
Nu
mb
er o
f p
atie
nts

ENGLAND_HOMICIDE (2002-2012)© National Confidential Inquiry into Suicide and Homicide by People with Mental Illness. All rights reserved.Not to be reproduced in whole or part without the permission of the copyright holder.
2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 20120
10
20
30
40
50
60
70
80
44
7064
72 74
53
66
38 37 36
22
59
71
44 4347
44
Estimated Confirmed
Year of conviction
Num
ber o
f pati
ents
Patient homicide - England

• Study of “low risk paradox”
• Case note review of 81 patient suicides/homicides
• Conclusion: risk management should be individual to patient

Patient suicide: number of mental health in-patients; number who died by hanging/strangulation on the ward
ENGLAND_SUICIDE (2002-2012)© National Confidential Inquiry into Suicide and Homicide by People with Mental Illness. All rights reserved.Not to be reproduced in whole or part without the permission of the copyright holder.
2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 20120
20
40
60
80
100
120
140
160
180
200
165
183
162155
142
122
106 103
8983
50
36
46
3428 31
20 2028 23
14 15
In-patient suicide Hanging/strangulation on the ward
Year
Nu
mb
er o
f p
atie
nts

In-patient suicides – care factors
• less likely to be detained under MHA (OR=0.43)
• more likely to be off ward without agreement (OR=13.07)
Source: Hunt et al, Psych Med, 2007

2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 20120
50
100
150
200
250
59
71
108
153
156
177190
223
185 185
149
165
183
162 155
142 122
106103
8983
50
CR/HT In-patient
Year
Nu
mb
er o
f p
atie
nts
Suicide under CR/HT and in-patient care - England
ENGLAND_SUICIDE (2002-2012)© National Confidential Inquiry into Suicide and Homicide by People with Mental Illness. All rights reserved.Not to be reproduced in whole or part without the permission of the copyright holder.

Suicide under crisis resolution/home treatment teams
• 140 suicides per year (England 2003-11)
• Rate higher than among in-patients(14.6 per 10,000 CR/HT episodes vs. 8.8 per 10,000 admissions)
• Increase from 80 per year (2003-04) to 163 (2010-11)
• Rate has fallen
• 44% lived alone; 49% adverse life events; 34% died <3 months discharge
SOURCE: NCI data, Lancet Psychiatry (2014)

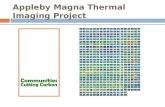
Suicides per week following discharge, England
ENGLAND_SUICIDE (2002-2012)© National Confidential Inquiry into Suicide and Homicide by People with Mental Illness. All rights reserved.Not to be reproduced in whole or part without the permission of the copyright holder.
1 2 3 4 5 6 7 8 9 10 11 12 130
50
100
150
200
250
300
350
400 380
292
253
207 199
161147
134 137122 113 111 123
Weeks between discharge and suicide (Week 1 = First week following discharge)
Nu
mb
er
of
pa
tie
nts

Suicide within two weeks of hospital discharge
• Case-control study 100 post-discharge suicides and 100 living controls (England 2004-06)
• Independent risk factors:
self-harmmale gender aged ≥ 40last admission <7 daysadverse life eventsco-morbid psychiatric illness
• Under CPA protective
SOURCE: NCI data, Psychiatric Services (2013)

Mental health teams contact with relatives after suicide: patient suicides
None3674 (32%)
Letter862 (8%)
Discussion (face to face or
telephone)6859 (60%)
Other78 (1%)
ENGLAND_SUICIDE (2002-2012)© National Confidential Inquiry into Suicide and Homicide by People with Mental Illness. All rights reserved.Not to be reproduced in whole or part without the permission of the copyright holder.

Patients as victims of homicide
• 1,496 victims (England & Wales, 2003-05)
• 90 (6%) patient victims
• 29/90 killed by fellow patient (7 with schizophrenia)
• 21/29 both victim and offender at the same NHS Trust
• Alcohol/drug misuse and previous violence common among patient victims and perpetrators
SOURCE: NCI data, Lancet Psychiatry (2014)

Key service recommendations
Removal of ligature points
Assertive outreach
24-hour crisis team
7-day follow-up
Non-compliance
Dual diagnosis
Criminal justice sharing
Multi-disciplinary review
Training in suicide risk management
Safety First, 200112 Steps to a Safer Service

Do safety measures reduce suicide rates?
Patient suicide rate per 10,000
*
* = significant difference p<0.05
Source: National Confidential Inquiry, Lancet, 2012

Suicide rates in target groups
Recommendation Target group % fall in suicide
Ligature points In-patients 24%
Assertive outreach ‘Non-compliant’ community patients 32%
Assertive outreach ‘Missed appointment’ community patients 11%
24-hour crisis team In-patients 29%
7-day follow-up Patients within 3 months of discharge 21%
Non-compliance ‘Non-compliant’ policy community patients 25%
Source: National Confidential Inquiry, Lancet, 2012

Patient suicide: the impact of service changes

Safety priorities for MH care
• Support for patients facing financial problems
• Review use of crisis resolution/home treatment
• Care plan & early follow-up post-hospital discharge
• Continue focus on ward environment
• Maintain specialised community teams: AO, dual diagnosis
• Multidisciplinary review after incidents

www.medicine.manchester.ac.uk
Follow us on twitter
@NCISH_UK
Follow us on Facebook