
Long-term effect of surgical/non-surgical treatment of periodontal … articles/LR131/Lindhe... ·...
12
Journal of Clinical Periodonlology 1984: 11: 448-458 Key words: Flaque conirol - sculiii^/rool planing - modified Widman flap - probing deplh - allachmenl level. Accepted for publication August 3, 1983 Long-term effect of surgical/non-surgical treatment of periodontal disease J. LINDHE', E. WESTFELT', S. NYMAN', S. S. Socransky" AND A. D. HAFFAJEE^ 'Department of Periodontology, School of Dentistry, University of Gothenburg, Gothenburg, Sweden "Department of Periodontology, Forsyth Dental Center, Boston, USA Abstract. The present investigation describes the effect of periodontal therapy in a group of patients who, following active treatment, were monitored over a 5-year period. One aim of the study was to analyze the role played by the patients' self-performed plaque control in preventing recurrent periodontitis. In addition, probing depth and attachment level alterations were studied separately for sites with initial probing depths of ^4 mm which were treated initially by either surgical or non-surgical procedures. Following active treatment (surgical/non-surgical), the patients were maintained on a plaque control regimen for 6 months, which included professional tooth cleaning once every 2 weeks. During the subsequent 18 months, the interval between the recall appointments was extended to 12 weeks and included prophylaxis as well as oral hygiene instruction. Following the 24-month examination, the interval between the recall appointments was further extended, now to 4-6 months. In addition, the maintenance program was restricted to oral hygiene instruction and professional, supragingival tooth cleaning, but further subgingival instrumentation was avoided. Clinical examinations including assessments of the oral hygiene, the gingival conditions, the probing depths and the attachment levels were performed at Baseline and after 24 and 60 months alter completion of active therapy. Assessments of plaque and gingivitis were repeated annually. The results of the examinations showed that the patients' standard of self-maintained oral hygiene had a decisive influence on the long-term effect of treatment. Patients who during the 5 years of monitoring consistently had a high frequency of plaque-free tooth surfaces showed little evidence of recurrent periodontal disease, while patients who had a low frequency of plaque-free tooth surfaces had a high frequency of sites showing additional loss of attachment. The present findings demonstrated that sites with an initial pocket depth exceeding 3 mm responded equally well to non-surgical and surgical treatments. This statement is based on probing depth and attachment level data from sites which were free of plaque at the 6-, 12-, 24-, 36-, 48- and 60-month reexaminations. It is suggested that the critical determinant in periodontal therapy is not the technique (surgical or non-surgical) that is used for the elimination of the subgingival infection, but the quahty of the debridement of the root surface. Several long-term trials have demonstrated that al. 1979, Nytnan & Lindhe 1979, Pihlstrometal- treatment of periodontal disease including 1981, 1983, Ramfjord et al. 1982). Axelsson & measures such as self-performed plaque con- Lindhe (1981) demonstrated the significance of trol, professional debridement and surgical the quality of the maintenance care program for management of periodontal pockets, may be the long-term success of periodontal therapy in successful in establishing healthy gingivae and a study of 90 patients with advanced peri- preventing further loss of supporting tissues, odontal disease. After active therapy, the sub- provided the patients are recalled on a regular jects were either maintained at the utiiversity basis for maintenance therapy (e.g. Knowles et clinic in a meticulous plaque control program
Transcript of Long-term effect of surgical/non-surgical treatment of periodontal … articles/LR131/Lindhe... ·...

Journal of Clinical Periodonlology 1984: 11: 448-458
Key words: Flaque conirol - sculiii^/rool planing - modified Widman flap - probing deplh - allachmenl level.
Accepted for publication August 3, 1983
Long-term effect of surgical/non-surgicaltreatment of periodontal disease
J. LINDHE', E. WESTFELT', S. NYMAN', S. S. Socransky" AND A. D. HAFFAJEE^
'Department of Periodontology, School of Dentistry, University of Gothenburg, Gothenburg, Sweden"Department of Periodontology, Forsyth Dental Center, Boston, USA
Abstract. The present investigation describes the effect of periodontal therapy in a group of patientswho, following active treatment, were monitored over a 5-year period. One aim of the study was toanalyze the role played by the patients' self-performed plaque control in preventing recurrentperiodontitis. In addition, probing depth and attachment level alterations were studied separately forsites with initial probing depths of ^ 4 mm which were treated initially by either surgical or non-surgicalprocedures.
Following active treatment (surgical/non-surgical), the patients were maintained on a plaque controlregimen for 6 months, which included professional tooth cleaning once every 2 weeks. During thesubsequent 18 months, the interval between the recall appointments was extended to 12 weeks andincluded prophylaxis as well as oral hygiene instruction. Following the 24-month examination, theinterval between the recall appointments was further extended, now to 4-6 months. In addition, themaintenance program was restricted to oral hygiene instruction and professional, supragingival toothcleaning, but further subgingival instrumentation was avoided. Clinical examinations includingassessments of the oral hygiene, the gingival conditions, the probing depths and the attachment levelswere performed at Baseline and after 24 and 60 months alter completion of active therapy. Assessmentsof plaque and gingivitis were repeated annually.
The results of the examinations showed that the patients' standard of self-maintained oral hygiene hada decisive influence on the long-term effect of treatment. Patients who during the 5 years of monitoringconsistently had a high frequency of plaque-free tooth surfaces showed little evidence of recurrentperiodontal disease, while patients who had a low frequency of plaque-free tooth surfaces had a highfrequency of sites showing additional loss of attachment. The present findings demonstrated that siteswith an initial pocket depth exceeding 3 mm responded equally well to non-surgical and surgicaltreatments. This statement is based on probing depth and attachment level data from sites which werefree of plaque at the 6-, 12-, 24-, 36-, 48- and 60-month reexaminations. It is suggested that the criticaldeterminant in periodontal therapy is not the technique (surgical or non-surgical) that is used for theelimination of the subgingival infection, but the quahty of the debridement of the root surface.
Several long-term trials have demonstrated that al. 1979, Nytnan & Lindhe 1979, Pihlstrometal-
treatment of periodontal disease including 1981, 1983, Ramfjord et al. 1982). Axelsson &
measures such as self-performed plaque con- Lindhe (1981) demonstrated the significance of
trol, professional debridement and surgical the quality of the maintenance care program for
management of periodontal pockets, may be the long-term success of periodontal therapy in
successful in establishing healthy gingivae and a study of 90 patients with advanced peri-
preventing further loss of supporting tissues, odontal disease. After active therapy, the sub-
provided the patients are recalled on a regular jects were either maintained at the utiiversity
basis for maintenance therapy (e.g. Knowles et clinic in a meticulous plaque control program

LONG-TERM EFFECT OF PERIODONTAL THERAPY 449
(recall group) or sent back to the referringdentists for maintenance therapy (non-recallgroup). The follow-up examinations performed3 and 6 years after the completion of activetreatment revealed that the recall group patientshad maintained excellent oral hygiene and hadno additional loss of attachment. The patientsof the non-recall group had a high frequency of(i) plaque harboring tooth surfaces, (ii) gingivalUnits which bled on probing and (iii) sites whichshowed additional loss of attachment. It waseoncluded that the patients' standard of self-Performed oral hygiene was the determiningfactor for success or failure in the long-termmaintenance of periodontal health. This con-'̂ ept, however, has been questioned by, e.g.Ramfjord et al. (1982) and Morrison et al.('982), who monitored 78 patients for 8 yearsfollowing active therapy. The maintenancetreatment included professional supra- and sub-gingival debridement every 3 months. Theauthors concluded "with professional toothcleaning ... the pocket reduction and clinicalattachment level gained by therapy can be"iiaintained without significant effect from vari-ations in personal oral hygiene" ... "Severity ofrecurrent gingivitis ... does not appear to haveany significant impact on recurrence of pocketdepth or maintenance of clinical attachmentlevels".
The first aim of the present study was to'tirther analyze the role played by the patients'Self-performed plaque control in preventingrecurrent periodontal disease.
In a recent publication (Lindhe et al. 1982),the effect of one surgical and one non-surgical
of treatment was studied in 15 patientsmoderately advanced periodontal disease,
'n these patients, tooth debridement was car-ried out in conjunction with the modified"idman flap procedure (Ramfjord and Nissie' ' 4 ) in 2 jaw quadrants, while in the contra-ateral jaw quadrants treatment was restricted° scaling and root planing. The patients who,
'ollowing treatment, were enrolled in a meticu-ous plaque control program were re-examined
6, 12 and 24 months after the completion ofactive therapy. The results of the re-examina-tions revealed that scaling and root planingused alone (non-surgery group) were equallyeffective as their use in combination with theflap procedure (surgery group) in establishingclinically healthy gingiva and in preventingfurther loss of attachment. It was also demon-strated, however, that the degree of pocketdepth reduction was more pronounced fol-lowing surgery than following a treatmentrestricted to subgingival instrumentation. Con-sequently, the frequency of sites with probingdepths exceeding 4 mm after treatment washigher in the non-surgery group than in thesurgery group. Waerhaug (1978) claimed thatroot surfaces adjacent to pockets exceeding 3mm in depth are extremely difficult to properlydebride by subgingival scaling. He also sug-gested (i) that immediately following such in-complete debridement, the gingiva at clinicalinspection may appear in good health, but (ii)that eventually the remaining subgingival mi-crobiota will proliferate and additional attach-ment loss result. Furthermore, Waerhaug(1978)stated that the predictability of a certain treat-ment procedure cannot be established in lessthan 3 to 5 years, and that only a few clinicaltrials fulfill these requirements. It is not clearwhether Waerhaug's concerns are justified, butif they are, it seemed essential that the patientsdescribed in our previous publication (Lindheet al. 1982) should be monitored for up to 5years in order to determine the rate of relapse ofdisease in sites which prior to active therapy haddeep pockets.
The second aim of the present study was toassess the periodontal conditions of this groupof patients 5 years after completion of activetreatment with special emphasis on sites withinitial pocket depth > 3 mm.
Material and Methods
This investigation included 15 subjects, 32-57years of age (mean age 47.9 years) selected at
450 LINDHE, WESTFELT, NYMAN, SOCRANSKY AND HAFFAJEE
random from the patients referred to the De-partment of Periodontology, University ofGothenburg, for treatment of periodontal dis-ease. Following a Baseline exarnination, allpatients were subjected to treatment utilizing asplit mouth design. On one side of the mouthscaling and root planing were performed inconjunction with a modified Widman flapprocedure (MWF-group) while the contralater-al quadrants were treated by subgingival scalingand root planing (RPL-group).
Following active treatment, the patients weremaintained for 6 months on a plaque controlregimen which involved professional tooth clea-ning once every 2 weeks (Axelsson & Lindhe,1974). For the next 18 months, the intervalbetween the recall appointtnents was extendedto 3 months. At Baseline and at the recall visits
6, 12 and 24 months after the completion ofactive treattnent, the patients were exatminedwith regard to oral hygiene (Plaque Index,Silness & Loe 1964), gingival conditions (Ging-ivaf Index, Loe & Silness 1963), probing depthsand clinical attachtnent levels. Afl tooth sur-faces and gingival units were included in theexatninations. For a detailed description of theoverall treatment and the examination proce-dures, the reader is referred to Lindhe et al.(1982),
Following the 24-month examination, theinterval between the recall appointments wasextended to 4-6 tnonths. In addition, the tnain-tenance program was restricted to oral hygieneinstruction and professional, supragingivaftooth cleaning, but further subgingival instru-mentation was avoided. 36, 48 and 60 tnonths
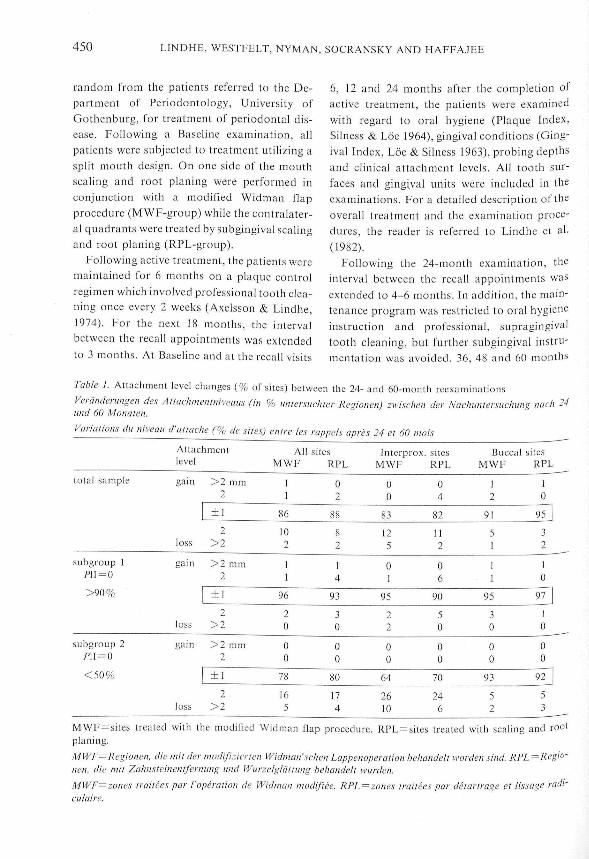
Table I. Attachment level changes (% of sites) between the 24- and 60-month reexaminations
yeranderungen des Atlachmenlniveaus (in % unlersucliter Regionen) zwischen der Naelnmtersue.und 60 Monaien.
Variations du niveau d'allache (% dc sites) entre les rappels apres 24 et 60 inois
Attaehmentlevel
All sitesMWF RPL
Interprox. sitesMWF RPL
Buccal sitesMWF RPL
total sample
subgroup 1pn=o
>90%
subgroup 2pn=o<50%
gain
loss
gain
loss
gain
loss
^ 2 mm2
±1
2>2
>2 mm2
±1
2>2
>2 mm2
+ f2
>2
1f
86
102
f1
96
20
00
78
165
02
88
82
14
93
30
00
80
174
00
83
125
01
95
to
to
00
64
2610
04
82
112
06
90
50
00
70
246
12
91
51
I1
95
30
00
93
52
10
95
32
10
97 1f
0
0
0
92
5
MWF = sites treated with the modified Widman flap procedure. RPL = sites treated with scaling and rootplaning.
MWF=Regionen. die mil der modifiziencn Widman'schen Lappenoperation hehandeli worden sind. RPL =Regio-nen. die mit Zahnsteinentfernung und Wurzelglattung behandelt wurden.
MWF=zones traitees par I'operation de Widman mcdifiec. RPL—zones traitees par delartrage et lissage raiH-ciilaire.

LONG-TERM EFFECT OF PERIODONTAL THERAPY 451
Table 2. Probing depth changes (% of sites) between Baseline and the 60-month reexamination for sites withwitial probing depth 5^4 mm
jerattderungen der Sondierungsliefe (in % untersuchter Regionett) zwischen der Ausgangsunlersuchung (base-'"c) und der Nachuntersuchung ttaeh 60 Monaten an Regionen mit einer initialen Sondierungsliefe von ̂ 4 mtnattations de la profondeur au sondage (% de site.s) entre I'examen initial et le rappclapres 60 mois. pour les poches
profondeur initiate '^4 mm
total sample
subgroup 11̂1 = 0
>90%
subgroup 2/'1I = O
<50%
_^
Probing depth
reduced
increased
reduced
increased
reduced
increased
>2 mm2
+ 1
2>2
>2 mm2
+ 1
2>2
>2 mm2
+ 1
2>2
All sitesMWF
3727
34
11
5633
11
00
1915
61
to t
o
RPL
3125
43
10
5034
16
00
2118
57
30
Interprox,MWF
3622
40
11
5530
15
00
2210
63
13
sitesRPL
2822
49
10
4736
18
00
18II
68
30
ee Table 1
"/-,' sietie Tab. I.
=/-.• cf. Tableau I.
alter active treatment, the quality of the pa-
' 'ents' self-performed plaque control was as-
sessed. At the termination of the study, 60
'Months after aetive treatment, a final examina-
tion was performed and included the same
P'lrameters as assessed at Baseline.
The present study describes changes which
Occurred between Baseline and the 60-month
••s-examination as well as between the 24-month
^nd the 60-month re-examinations. The data
'neluded represent the I 1 patients who took
part in the entire 5-year study. The 4 patients
*h Were excluded received restorative therapy
the 24-month examination which pre-
the insertion of the stent used for
' 'ttachment level measurements.
Results
The results are presented for (i) the entire
sample, (ii) patients who had maintained an
excellent standard of oral hygiene during the 5-
year period; PlI = 0>90% at each re-examina-
tion (subgroup I) and (iii) patients who failed
to maintain a proper standard of oral hygiene;
/'1I = O<5O% at each re-examination (sub-
group 2).
The changes in the clinical attachment level
which occuiTed between the 24- and60-montli re-
examinations are presented in Table I. For the
total sample, the attachment level remained
unchanged in 86-88% of the sites. Gain of
attachment of 2 mm or more occurred in 2% of

452 LINDHE, WESTFELT, NYMAN, SOCRANSKY AND HAFFAJEE
the sites during this time period while 10-f2%of the sites exhibited attachment loss amount-ing to ^ 2 mm. No obvious difference withrespect to attachment level alteration was foundbetween the 2 treatrnent groups (MWF andRPL) but loss of attachment was more preva-lent at interproximal than at buccaf surfaces.The patients of subgroup 1 exhibited loss ofattachment (^2 mm) in only few sites (2-3%),while rnore than 95% of the sites remainedunchanged or gained clinical attachment level.There were no differences between the 2 treat-ment groups or between interproxitnal andbuccal sites. In contrast, the patients of sub-group 2 had no sites with gain of attachment,but attachment foss of > 2 mtn was found inabout 20%' of the sites. This attachtnent loss
occurred most frequently in the interproxitnalareas.
Tables 2 and 3 summarize probing depth andattachment level alterations during the periodbetween the Baseline examination and the 60-month reexaminalion in sites with a probingdepth exceeding 3 mm at Baseline. A reductionof probing depth of 2 mm or more occurred in55-65% of sites in the total patient sample(Table 2). Only 1-2% of sites showed increasedprobing depth values in cornparison to theBaseline data. About 85% of the initially deeppockets (^4 mm) in the patients of Subgroup 1were reduced in depth, the tnajority of them bymore than 2 tntn. Such a reduction of theprobing depth in initially deep pockets was lessprevalent in the patients of subgroup 2. Hovv-
Table 3. Attachment level changes (% of sites) between Baseline and the 60-month reexamination for siteswith initial probing depth 3J4 mm
Veranderungen des Attachtnentnivcaus (in % unlersucliter Regionen) zwisehen der Ausgaiigsuntersuehung (base-line) und der Naclmntersuclnmg nach 60 Monaten an Regionen mit einer initialcn Sondierungsliefe von ^4 /«'"Variations de niveau d'attache (% de sites) entre I'examen initial et le rappcl apres 60 mois. pour les pochesd'lme profondeur initiate '^4 mtn
total sample
subgroup 1P1I = O
>90%
subgroup 2P\\ = Q
<50%
MWF; RPLMWE: RPL:MWE RPL:
Attachmentlevel
gain
loss
gain
foss
gain
loss
see Table f
siehe Tab. I.
cf. Tableau L
>2 mm2
+ f
2
>2
>2 mtn2
+ f
2>2
>2 mm2
±1
2>2
All sitesMWF
38
71
134
313
75
70
55
69
146
RPL
412
77
42
417
11
20
69
78
33
Interprox.MWF
48
71
115
413
76
60
66
64
167
sitesRPL
413
"142
4f8
75
30
310
79 153

LONG-TERM EFFECT OF PERIODONTAL THERAPY 453
Tabte 4. Probing depth changes (% of sites) between the 24- and 60-month reexamination for sites withprobing depth 5=4 mm at the 24-month reexamination
^eratiderung dtr Sottdierungstiefe (in % untersuchter Regionen) zwisctien der Naclntntersuctutttg nach 24 und 60Monaten an Regionen tnit einer Sondierungstiefe von '5^4 mm bei der Nachuntersuchung nach 24 MonatenSatiations de ta profondeur au sottdage (% dc sites) entre tes rappets apres 24 et 60 tnois, pour tes poetics0 une profondeur '^4 mttt tors du rappet apres 24 tnois
total sample
subgroup 1fli=o
>90%
subgroup 2fli=o
<50%
Probing depth
reduced
increased
reduced
increased
reduced
increased
> 2 mm2
l-l-
2>2
>2 mm2
±1
2>2
>2 mm2
±12
>2
MWF
07
76
143
010
87
30
05
50
369
All sitesRPL
19
84
51
320
74
30
06
79
123
InterproxMWF
06
76
134
06
89
60
05
55
3010
sitesRPL
011
82
51
022
74
40
06
77
133
MWF; RPL; see Table 1,MWF: RPL: .sietie Tab. I.
MWF, RPL: cf Tat3teau I.
probing depth remained unaltered in
about 60% of the sites in this group.
Attaehment level alterations in sites with
initial probing depths of ^ 4 mm are sum-
marized in Table 3. More sites lost attachrnent
•n the patients of subgroup 2 (20% and 6%)
than in the individuals of subgroup I (7% and
•^%). Gain of attachment occurred more fre-
"luently in the patients of subgroup 1 than in
subgroup 2,
Alterations of probing depths and clinical
attachment levels //; the interval belweett 24 and
'^'^ tnonihs for sites where the probing depthExceeded 3 mm at the 24-month re-examination'̂•e presented in Tables 4 and 5. For the total
Sample, the probing depth remained unchanged
in about 75-85% of the sites (Table 4) and theattaehment level unaltered in about 85 % (Table5). Reduction of the probing depth and gain ofthe clinical attachment occurred mainly in thegroup of patients who maintained a high stan-dard of oral hygiene (subgroup 1), while furtherincrease of the probing depth was found pre-dominantly in patients who failed to exerciseproper plaque control measures. In this lattergroup of patients, (subgroup 2), no sites ex-hibited attachment gain but a further loss ofattachment (5=2 mm) occurred in 36% of theinitially MWF-treated sites and in 18% of thesites treated with scaling and root planing(Table 5),

454 LINDHE, WESTEELT, NYMAN, SOCRANSKY AND HAEEAJEE
Discussion
The present investigation demonstrated that thepatients' standard of oral hygiene evidently hada decisive influence on the long-term result oftreatment of periodontal disease. Thus, patientswho, during the 5 years of monitoring, con-sistently had a high frequency of plaque-freetooth surfaces showed virtually no signs ofrecurrent gingivitis, increased probing depth oradditional loss of attachment. Patients with alow frequency of plaque-free tooth surfaces hada higher frequency of sites showing inflamma-tion and additional loss of attachment. Thisobservation is in close agreement with findingsreported previously (e.g. Rosling et al. 1976 a, b,Nyman et al. 1977, Poison & Heijl 1978,Axelsson & Lindhe 1981) and emphasizes that
in the absence of plaque, inflammatory peri-odontal disease fails to recur. Our data, how-ever, seem to be at variance with results re-ported by Pihlstrom et al. (1981, 1983) whomonitored patients during a 4-6/2 year periodafter active therapy. The authors concluded: "mspite of initial intensive oral hygiene instructionand reinforcement at regular intervals, thesupragingival plaque index did not vary frompretreatment levels ... In spite of this, ... pocketdepth was reduced, attachment level maintain-ed or increased and inflammation reduced overthe 4-year titne interval". The findings reportedhere also fail to corroborate data recentlyreported by Ramfjord et al. (1982). They studiedthe "role of personal plaque control in peri-odontal maintenance care" by annual assess-tnent of pocket depth and attachment level
Table 5. Attachment level changes (% of sites) between the 24- and 60-month reexamination for sites with.probing depth 3=4 mm at the 24-month reexaminationVeranderungen des Attachmentniveaus (in % untersuchter Regionen) zwischen der Nachunlersuchung nach 24 und60 Monaten an Regionen mil einer Sondierungstiefe von '^4 mm bei der Nachuntersuehung nach 24 MonatenVariations du niveau d'attache (% de sites) entre les rappels apres 24 et 60 mois, pour les poches d'uneprofondeur '^4 mm tors du rappet apres 24 mois
total sample
subgroup 1P\\ = 0
>90%
subgroup 2P\l = (i
<50%
MWF; RPL
MWF: RPL;
MWr, RPL:
Attachmentlevel
gain
loss
gain
loss
gain
loss
see Table 1.
siehe Tab. 1.
cf. Tableau I.
>2 mm2
±1
2>2
> 2 mm2
+ 1
2> 2
> 2 mm2
l-l-
2>2
All sitesMWE
20
84
95
30
93
30
00
64
1818
RPL
27
85
70
314
80
30
00
82
180
Interprox.MWE
00
85
106
00
94
60
00
67
1419
sitesRPL
18
84
70
015
8 . 140
00
83
170

LONG-TERM EFFECT OF PERIODONTAL THERAPY 455
alterations in patients who, over an 8-yearperiod, were recalled every 3 months for profes-sional prophylaxis. The 78 patients were divid-ed into 2 main subgroups; one group withplaque score >1.92 (PDI Index, Ramfjord1959, 1967) and another with plaque scored1-92. A second grouping of the patients was alsotindertaken: "the 25% of patients with thehighest plaque scores in one group and the 25 %W:th the lowest scores in another group". Thefigures presented by Ramfjord et al. (1982)reveal that, during the first years after activetreatment, attachment loss in shallow pocketsWas significantly less and attachment gain indeep pockets significantly greater in those 25%ol the patients who had the lowest plaque score('51.32) in comparison to those who had highscores (5s2.58). The difference between thegroups, however, tended to be decreased withincreasing observation time. The grouping ofthe sample was based on oral hygiene deter-niinations made 12 months following activetreatment, and the plaque assessments were notsubsequently repeated. The disappearance ofthe differences in pocket depth and attachmentlevel between the various subsamples may havet>een an effect of a gradually deteriorating oralhygiene in the initially low plaque score group,
an assumption would be in agreementfindings reported by Nyman et al. (1975),
Rosling et al. (1976a) and Nyman et al. (1977)Which showed that in patients who, followingactive therapy, were not maintained in a well-supervised oral hygiene program, the plaqueScores with time gradually returned to pretreat-rnent levels. Furthermore, the data from thepresent study demonstrated that in patients inWhom, after the 24-month examination, thesupragingival plaque control was not appro-priate, the probing depth was increased andadditional attachment loss occurred.
Results reported by Lindhe et al. (1983) froma Series of long-term follow-up examinations of5 adult subjects with untreated periodontal'sease, revealed that disease failed to progress
"1 sites devoid of plaque, while additional
attachment loss occasionally occurred in siteswith plaque infection and inflammation. It wasalso observed that during the 6-year period ofmonitoring: (i) 33 of the untreated patientsshowed no sign of disease progression; (ii) morethan 50% of all attachment loss discovered inthe entire sample took place in 4 patients. Theseobservations make it reasonable to question thevalidity of grouping patients in different cate-gories based on individual mean Plaque Indexscores. Rather, the probing depth and attach-ment level alterations should be evaluated inrelation to sites which, during the entire periodof monitoring (or at all reexaminations), areconsistently devoid of or harbor plaque. A moredetailed analysis of the present data revealedthat practically all sites which, at the 6-, 12-, 24-,36-, 48- and 60-month examinations receivedPlaque Index score 0, were not exposed toincreased probing depth or additional attach-ment loss. In contrast, a large number (but farfrom all) of those sites which consistentlyharbored visible amounts of plaque (PlaqueIndex score 2) exhibited increased probingdepth and loss of attachment.
The patients described in this study werefollowing the Baseline examination subjected totreatment of periodontal disease which in 2 jawquadrants was limited to subgingival scalingand root planing while the root surfaces in thecontralateral jaw quadrants were debrided aftersurgical flap elevation. A separate analysis wasperformed regarding the effect of treatment ofsites which at the Baseline examination hadprobing depths exceeding 3 mm. This was donebecause it has been suggested (Waerhaug 1978)that it is difficult or impossible by non-surgicaltherapy to properly debride root surfaces ad-jacent to deep pockets. The present findings,however, clearly demonstrate that sites with aninitial pocket depth exceeding 3 mm respondedequally well to the non-surgical as to the surgi-cal mode of treatment. This statement is basedon probing depth and attachment level datafrom sites which were free from plaque (PlaqueIndex score = 0) at all re-examinations. Our
456 LINDHE, WESTFELT, NYMAN, SOCRANSKY AND HAEFAJEE
findings are consistent with those of Listgartenet al. (1978) who treated pocketsSs 5 mm by sub-gingival scaling and plaque control. Clinical,microbiological and histological assessmentsperformed 8 and 25 weeks after active therapyrevealed that all treated sites showed no supra-gingival plaque accumulation and that properhealing had occurred. In many respects, ourfindings also agree with Pihlstrom et al. (1983)who showed that non-surgical treatment ofmoderately advanced to advanced periodontaldisease was equally as effective as surgicaltreatment with respect to probing depth reduc-tion and attachment level gain as assessed 6/2years after initial therapy. The data reported inthe present study as well as in publications byBadersten et al. (1981, 1984), Hill et al. (1981),Pihlstrom et al. (1983) should not be interpretedas suggesting that surgical exposure of deeppockets is a superfluous component of peri-odontal therapy. Obviously, however, the crit-ical determinant in periodontal therapy is notthe technique/;cr if that is used for the elimina-tion of the subgingival infection but that de-bridement of the root surface is properly per-formed.
The initial healing response of the peri-odontal tissues following surgical and non-surgical treatment of moderately advancedperiodontal disease was recently studied in 15human subjects by Lindhe et al. (1982). It wasfound that both methods of treatment resultedin some loss of clinical attachment in shallowpockets, while gain of clinical attachment con-sistently occurred in deep pockets. In fact, thedeeper the initial pocket depth was, the morepronounced was the clinical attachment gain.Similar findings have also been reported byother investigators (e.g. Knowles et al. 1979.Pihlstrom et al. 1981, 1983, Hill et al. 1981,Badersten et al. 1984). Recent studies in animalsand humans have demonstrated that followingtraditional therapy, significant gain of con-nective tissue attachment fails to occur on a rootsurface deprived of its periodontal ligamenttissue (Frank etal. 1974, Caton et al. 1980, Cole
et al. 1980, Nyman et al. 1981, Froum et al.1982). This fact must be considered when datadescribing gain of attachment following thera-py are reported in clinical trials. Since the at-tachment level in a clinical examination isdetermined by the use of a periodontal probe, itis likely that attachment gain following treat-ment simply reflects a decreased ability of theinstrument to identify the apical portion of thedento-gingival epithelium (Listgarten 1980). Inorther words, gain of clinical attachment indeep pockets should be regarded as the result ofthe disappearance of the inllammatory cellinfiltrate in the gingiva and increased amountsof collagen in the previous lesion.
Acknowledgement
This investigation was supported by a grantfrom NIDR (Nil) No. DE 0489.
Zusammenfassung
Langzeilejfckte clunirgischey bziv. nichl-clururgischcrBehandliing der ParodontiiisDie voi'liegende Studie beschreibt die Effekte paro-dontaler Therapie bei einer Probandengruppe, dienach der aktiven Behandlung 5 Jahre lang regel-massig iiberwacht wurde. Eines der Ziele dieser Studiewar die Analyse der Rolle, die die vom Patieiitenselbst vorgenommene Plaquekontrolle bei der Rezi-divprophylaxe der Parodontitis spielt. Daruberhin-aus wurden die Sondierungstiefen und die Attacli-mentniveaus separat in solchen Regionen mit initialenTaschentiefen von ^ 4 mm studiert, die urspriinglichentweder mit chirurgischen oder nicht-chirurgisclienMethoden behandelt worden waren. Nach der aktivenBehandlungsphase (cliirurgisch oder nicht-chir-urgisch) wurde die Plaquekontrolle 6 Monate langiiberwacht und 1-maljedezweiie Wocheprofessionel-le Zahnreinigung angeordnei. Wahrend der dannfolgenden 18 Monate wurden die Intervalle zwischenden Einbestellungen zur Nachsorge auf 12 Wochenerweiiert und die Nachsorge tjeinhaliete sowohl pro-phylaktischc Behandlung als auch Hygieneinsiruk-tion. Naeh einer 24 Monaien andauernden Unier-suchungsfolge wurden die Intervalle zwischen denNachsorge-Einbesiellungen dann bis auf 6 Monateerweiieri. Das Nachsorgeprogramm wurde nun auiorale Hygieneinstruktion und professionelle supra-gingivale Zahnreinigung reduziert - subgingivale Be-handlung mii Zahnsteininsirumenien wurde vei-

LONG-TERM EFFECT OF PERIODONTAL THERAPY 457
n. Die klinische Unteisuchung mit der Be-wertung der oralen Hygiene, dergingivalen Situation,sowie der Messung der Sondierutigstiefe und des At-tachmentniveaus (Niveau des Epithelansatzes), wur-de anlasslich der Ausgangsuntersuchung und 24 undw Monate nach der Beendigungderaktiven Therapie^orgenommen. Die Bewertung der Plaque-und Ging-ivitissituation wurde dann jahrlich wiederholt. DieNachuntersuchungsergebnisse zeigten, dass der vomPatienten selbst aufrechterhaltene Standard der ora-len Hygiene entscheidenden Einfluss auf den Lang-zeiteffekt der Behandlung hatte. Bei Patienten, beidenen wahrend der 5-jahrigen Uberwachung einandauerndes holies Vorkommen plaquefreier Zahn-oberflachen registrierl worden war, wurden kaumRezidive der Parodontalkrankheit gesehen, wahrend°£i Patienten mit geringerem Vorkommen plaque-ireier Zahnoberflachen, haufig Regionen mit weiter-gehendem Attachmentverlust angetroffen wurden.Die vorliegenden Resultate zeigen, dass Regionen mitantanglich tieferen Taschentiefen als 3 mm gunstigauf sowohl die nicht-chirurgischen als auch die chir-Wgisehen Behandlungen reagierten. Diese Feststel-lung wird aufgrund der Beobachtung der Taschen-tiefen und der vorligeneden Daten uber das Attacli-mentniveau in solchen Regionen getroffen, die bei derNachuntersuchung nach 6-, 12-, 24-, 36-, 48- und 60Wonaten plaquefrei waren.
Es erscheint wahrscheinlich, dass die kritischcDeterminante parodontaler Therapie nicht in dcrBehandltmgstechnik (chirurgisch oder nicht-chirur-gisch) zu suchen ist, die eine Elimination der sub-gingivalen Infektion ermoglicht, sondern in der Qua-'itat der Debrisenti'ernung von der Wurzeloberfliiche.
Resume
poraison enwe les effels a long lerme dit irailememrgical et non-chirurgical de la maladieparodontale
presente etude decrit I'effet de la therapie paro-chez un groupe de patients ayant subi un
'raitement actif, suivi ensuite durant 5 ans. L'un des"uts de l'etude, etait d'analyser l'influence du eontroie"c plaque exerce par le patient sur la prevention de laParodontite recurrente. De plus, les variations deProfondeur au sondage et de niveau d'attache dans lesPoches d'une profondeur initiale > 4 mm traitees'^hirurgicalement ou non ont cte enregistrees separe-nient.
•^Pres le traitement actif, chirurgical ou non, lesPatients ont ete soumis durant 6 mois a un eontroie deplaque comprenant un nettoyageprofessionnel toutes^̂ 2 semaines. Pendant les 18 mois suivants, les'̂ ''Ppels ont eu lieu toutes les 12 semaines et com-Poriaieni prevention et instruction en hygiene buc-^ale. Deux ans apres le traitement, les rappels espacesa 4-6 mois ne comportaient plus qu'un detartrage
sus-gingival et tme instruction en hygiene buccale.L'indice de plaque, I'indice gingival, les profondeursau sondage et les niveaux d'attache ont ete enregistresa I'examen initial, et 24 et 60 mois apres le traitementactif. Les indices de plaque et de gencive ont etereleves annuellement.
Les resultats indiquent que le degre d'hygienebuccale maintenu par le patient a une influencemarquante sur le succes du traitement a long terme.Les poches parodontales > 3 mm etaient traitees avecle meme succes par la chirurgie ou une approcheconservatrice. Ces constatations sont basees sur lesmesurcs effectuees dans des sites sans plaque lors desrappels apres 6, 12, 24, 36, 48 et 60 mois. Le facteurdeterminant de la therapie parodontale ne seraitdone pas la technique utilisee (chirurgicale ou non)pour climiner I'inflammation sous-gingivale mais laqualite du lissage radiculaire.
References
Axelsson, P. & Lindhe, .1. (1974) The effect of apreventive programme on dental plaque, gingivitisand caries in schoolchildren. Results after one andtwo years. .lournal of Clinical Periodontology I,126-138.
Axelsson, P. & Lindhe, J. (1981) The significance ofmaintenance care in the treatment of periodontaldisease. Journal of Clinical Feriodontologv 8, 281-295.
Badersten, A., Nilveus, R. & Egelberg, J. (1981) Ef-fect of nonsurgical periodontal therapy. I. Moder-ately advanced periodontitis. Journal of CliniealFeriodontology 8, 57-72.
Badersten, A., Nilveus, R. & Egelberg, J. (1984) Ef-fect of nonsurgical periodontal therapy. II. Severe-ly advanced periodontitis. Journal of Clinical Ferio-dotology, 11, 63-76.
Caton, J., Nyman, S. & Zander, H. (1980) Histome-tric evaluation of periodontal surgery. IL Connect-ive tissue attachment levels after four regenerativeprocedures. Journal of Clinieal Feriodoniologv 7,224-231.
Cole, R. T., Crigger, M., Bogle, G., Egelberg, J. &Selvig, K. A. (1980) Conneetive tissue regenerationto periodontally diseased teeth. Journal of Feriod-ontal Research 15, 1-9.
Frank, R., Fiore-Donno, G., Cimasoni, G. & Matter,J. (1974) Ultrastructural study of epithelial andeonnective gingival reattachment in man. Journalof Feriodontology 45, 626-635.
Froum, S. J., Coran, M., Thaller, B., Kushner, L.,Seopp, 1. W. & Stahl, S. S. (1982) Periodontal heal-ing following open debridement flap procedures. I.Clinical assessment of soft tissue and osseous re-pair. Journal of Feriodontology 53, 8-14.
Hill, R. W., Ramfjord, S. P., Morrison, E. C , Apple-

458 LINDHE, WESTFELT, NYMAN, SOCRANSKY AND HAEFAJEE
berry, E. A., Caffesse, R. G., Kerry, G. J. & Nissle,R. R. (1981) four types of periodonial treatmentcompared over two years. .Journal of Periodonlol-ogy 52, 655-662.
Knowles, J. W., Burgett, F. G., Nissfe, R. R., Shicf<,R. A. Morrison, E. C. & Ramfjord, S. P. (1979) Re-sults of periodonial treatment related to pocketdepth and attachment level. Eight years. Journal ofPeriodotmlogy 50, 225-233.
Lindhe, } . , Haffajee, A. D. & Socransky, S. S. (1983)Progression of periodonial disease in adufi subjectsin ihe absence of periodoniaf iherapy. Journal ofClinical Periodontology 10, 433-442.
Lindhe, J., Wesifeli, E., Nyman, S., Socransky, S. S.,HeijI, L. & Bratihall, G. (1982) Healing followingsurgical/non-surgical treatment of periodonial dis-ease. Journal of Clinical Periodontology 9, 115-128.
Lisigarten, M. A. (1980) Periodontal probing: Whatdoes it mfAw'l Journal of Clinical Periodontology 7,165-176.
Listgarten, M. A., Lindhe, J. & Hcllden, L. (1978)Effect of teiracycline and/or scaling on humanperiodontaf disease. Journal of Clinical Periodonto-logy 5, 2A(,-21\.
Loe, H. & Silness, J. (1963) Periodonial disease inpregnancy. I. Prevalence and severity. Acta Odont-ologiea Scandinavica 21, 533-551.
Morrison, E. C , Ramfjord, S. P., Burgeii, F. G.,Nissle, R. R. & Shick, R. A. (1982) The significanceof gingivitis during the mainienance phase ofperiodontal treatment. Journal of Periodontoloaiy53,31-34.
Nyman, S. & Lindhe, J. (1979) A longitudinal studyof combined periodontal and prosiheiic treaimeniof paiienis with advanced periodonial disease.Journal of Periodontology 4, 163-169.
Nyman, S., Lindhe, J. & Karring, T. (1981) Healingfollowing surgical treatment and root deminerali-zaiion in monkeys wiih periodontal disease. Jour-nal of Clinical Periodontology 8, 249-258.
Nyman, S., Lindhe, J. & Roshng, B. (1977) Peri-odontal surgery in plaque-infected dentitions../our-iicd of Clinical Periodontology 4, 240-249.
Nyman, S., Rosling, B. & Lindhe, J. (1975) Effectof professional tooth cleaning on healing after peri-odontal surgery. Journal of Clinical Periodontologv2, 80-86.
Pihisirom, B. L., Oriiz-Campos, C. & McHugh, R. B.
(1981) A randomized four-year study of periodont-al therapy. Journal of Periodontology 52, 227-242.
Pihlstrom, B. L., McHugh, R. B., Oliphant, T. H. &Ortiz-Campos, C. (1983) Comparison of surgicaland non-surgical treatment of periodontal disease.Journal of Clinical PeriodontologylO, 524-541.
Poison, A. M. & Heijl, L. (1978) Osseous repair ininfrabony periodonial defects. Journal of ClinicalPeriodontology 5, 13-23.
Ramfjord, S. P. (1959) Indices for prevalence andincidence of periodontal disease. Journal of Pert-odontology 30, 51-59.
Ramfjord, S. P. (1967) The periodonial disease index(PDI). Journal of Periodontology 38, 602-610.
Ramfjord, S. P., Morrison, E. C , Burgeii, F. G.,Nissle, R. R., Shick, R. A., Zann, G. J. & Know-les, J. W. (1982) Oral hygiene and mainienance ofperiodonial suppori. Journal of Periodontology 53,26-30.
Ramfjord, S. P. & Nissle, R. R. (1974) The modifiedWidman flap. Journal of Periodontology 45, 601-607.
Rosling, B., Nyman, S. & Lindhe, J. (1976a) Theeffeci of sysiemaiic plaque control on bone regene-ration in infrabony pockets. Journal of ClinicalPeriodontology 3, 38-53.
Rosling, B., Nyman, S., Lindhe, J. & Jern, B. (1976b)The healing poieniial of ihe periodonial iissues fol-lowing differeni iechniqucs of periodonial surgeryin plaque-free dentitions. A 2-year clinical study.Journal of Clinical Periodontology 3, 233-250.
Silness, .1. & Loe, H. (1964) Periodontal disease inpregnancy. 11. Correlation between oral hygie"^and periodontal condition. Acta Odontologicu.Scandinavica 22, 121-135.
Waerhaug. J. (1978) Healing of the dento-epithelialjunction following subgingival plaque control. I-As observed in human biopsy material. Journiil "Jt'eriodontology 49, 1-8.
Address;
Elisabet WestfeltDepartment of PeriodontologySchool of DentistryUniversity of GoteborgBox 33070S-40033 GoteborgSweden



















