Liver anatomy and physiology medicine
73
LIVER ODESSA BACUD - TIANGCO, MD
-
Upload
robin-hesita-tolentino -
Category
Documents
-
view
59 -
download
5
description
Liver anatomy and physiology medicine parts and functions
Transcript of Liver anatomy and physiology medicine

7/17/2019 Liver anatomy and physiology medicine
http://slidepdf.com/reader/full/liver-anatomy-and-physiology-medicine 1/73
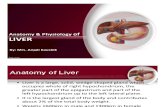
LIVER
ODESSA BACUD
-
TIANGCO, MD

7/17/2019 Liver anatomy and physiology medicine
http://slidepdf.com/reader/full/liver-anatomy-and-physiology-medicine 2/73
ANATOMY

7/17/2019 Liver anatomy and physiology medicine
http://slidepdf.com/reader/full/liver-anatomy-and-physiology-medicine 3/73

7/17/2019 Liver anatomy and physiology medicine
http://slidepdf.com/reader/full/liver-anatomy-and-physiology-medicine 4/73

7/17/2019 Liver anatomy and physiology medicine
http://slidepdf.com/reader/full/liver-anatomy-and-physiology-medicine 5/73
ANATOMY

7/17/2019 Liver anatomy and physiology medicine
http://slidepdf.com/reader/full/liver-anatomy-and-physiology-medicine 6/73

7/17/2019 Liver anatomy and physiology medicine
http://slidepdf.com/reader/full/liver-anatomy-and-physiology-medicine 7/73
HEPATIC VEIN
● Small
short
hepaticveins

7/17/2019 Liver anatomy and physiology medicine
http://slidepdf.com/reader/full/liver-anatomy-and-physiology-medicine 8/73
HEPATIC ARTERY
● Replacedhepatic
artery
● Accessoryhepatic
artery

7/17/2019 Liver anatomy and physiology medicine
http://slidepdf.com/reader/full/liver-anatomy-and-physiology-medicine 9/73
PORTAL VEIN

7/17/2019 Liver anatomy and physiology medicine
http://slidepdf.com/reader/full/liver-anatomy-and-physiology-medicine 10/73
PORTAL VEIN●
75%● Posterior to the
bile duct & hepatic
artery
● valveless
● 3-5 mm Hg

7/17/2019 Liver anatomy and physiology medicine
http://slidepdf.com/reader/full/liver-anatomy-and-physiology-medicine 11/73
BILIARY SYSTEM

7/17/2019 Liver anatomy and physiology medicine
http://slidepdf.com/reader/full/liver-anatomy-and-physiology-medicine 12/73
LYMPHATICS & INNERVATION
● Spaces of Disse & clefts of Mall → sub-Glissonian
&periportal → cisterna chyli
● Vagus nerve & celiac plexus
●
C3 & C4

7/17/2019 Liver anatomy and physiology medicine
http://slidepdf.com/reader/full/liver-anatomy-and-physiology-medicine 13/73
LIVER LOBE

7/17/2019 Liver anatomy and physiology medicine
http://slidepdf.com/reader/full/liver-anatomy-and-physiology-medicine 14/73

7/17/2019 Liver anatomy and physiology medicine
http://slidepdf.com/reader/full/liver-anatomy-and-physiology-medicine 15/73
● Coagulation
factors
● Plasma proteins-
eg. albumin
● Glucose
● Lipoproteins
● Triglyceride
PHYSIOLOGY:SYNTHETIC FUNCTIONS
● Cholesterol →
● Bile salt

7/17/2019 Liver anatomy and physiology medicine
http://slidepdf.com/reader/full/liver-anatomy-and-physiology-medicine 16/73
BILIRUBIN METABOLISM
uncojugated

7/17/2019 Liver anatomy and physiology medicine
http://slidepdf.com/reader/full/liver-anatomy-and-physiology-medicine 17/73
BILIRUBIN METABOLISM
uncojugated

7/17/2019 Liver anatomy and physiology medicine
http://slidepdf.com/reader/full/liver-anatomy-and-physiology-medicine 18/73
BILIRUBIN METABOLISM
conjugated

7/17/2019 Liver anatomy and physiology medicine
http://slidepdf.com/reader/full/liver-anatomy-and-physiology-medicine 19/73
BILE
● Bile
● 85% water
● 10% bile salts
● 3% mucus & pigments
● 1% fats
● 0.7% inorganic salts
● BILE ACIDS
● Primary : cholic &
chenodeoxycholic
● Secondary : deoxycholic& lithocholic

7/17/2019 Liver anatomy and physiology medicine
http://slidepdf.com/reader/full/liver-anatomy-and-physiology-medicine 20/73
BILE & ENTEROHEPATIC
CIRCULATION
500-1000ML/24H

7/17/2019 Liver anatomy and physiology medicine
http://slidepdf.com/reader/full/liver-anatomy-and-physiology-medicine 21/73
LIVER FUNCTION TESTS

7/17/2019 Liver anatomy and physiology medicine
http://slidepdf.com/reader/full/liver-anatomy-and-physiology-medicine 22/73
● PARENCHYMAL- AST, ALT
●
BILIARY - Alkaline phosphatase
● SYNTHETIC - INR, factors V & VII, bilirubin,
albumin

7/17/2019 Liver anatomy and physiology medicine
http://slidepdf.com/reader/full/liver-anatomy-and-physiology-medicine 23/73

7/17/2019 Liver anatomy and physiology medicine
http://slidepdf.com/reader/full/liver-anatomy-and-physiology-medicine 24/73
RADIOLOGIC EVALUATION OF THE
LIVER

7/17/2019 Liver anatomy and physiology medicine
http://slidepdf.com/reader/full/liver-anatomy-and-physiology-medicine 25/73
ULTRASOUND
●
Economical● Screen for HCC
● Biliary tract stones
● Intrahepatic biliary
ductal dilation

7/17/2019 Liver anatomy and physiology medicine
http://slidepdf.com/reader/full/liver-anatomy-and-physiology-medicine 26/73
ULTRASOUND
● Microbubblecontrast
● Doppler UTZ
● laparoscopic
● IOUS- gold standard
to detect number,extent & blood vessel
association of tumors

7/17/2019 Liver anatomy and physiology medicine
http://slidepdf.com/reader/full/liver-anatomy-and-physiology-medicine 27/73
COMPUTED TOMOGRAPHY SCANS
● Highly sensitive
●
Dual- & triple-phase IV contrast
● 3-D

7/17/2019 Liver anatomy and physiology medicine
http://slidepdf.com/reader/full/liver-anatomy-and-physiology-medicine 28/73
COMPUTED TOMOGRAPHY SCANS
● PRE-OPERATIVE
EVALUATION-
inflow & outflow
of hepatic bloodvessel
● -Liver volume
● Primary vs.
metastatic

7/17/2019 Liver anatomy and physiology medicine
http://slidepdf.com/reader/full/liver-anatomy-and-physiology-medicine 29/73
MAGNETIC RESONANCE IMAGING
● Less sensitive at spatial discrimination
● More sensitive for detecting early HCC &
distinguishing HCC for macroregenerativenodules
● Contrast- cystic vs. Hemangioma
● MRC

7/17/2019 Liver anatomy and physiology medicine
http://slidepdf.com/reader/full/liver-anatomy-and-physiology-medicine 30/73
● PET Scan
F-flurodeoxyglycose
●
Angiography ● Hepatic arterial chemoembolization
● Percutaneous biopsy
● Diagnostic laparoscopy

7/17/2019 Liver anatomy and physiology medicine
http://slidepdf.com/reader/full/liver-anatomy-and-physiology-medicine 31/73
LIVER FAILURE

7/17/2019 Liver anatomy and physiology medicine
http://slidepdf.com/reader/full/liver-anatomy-and-physiology-medicine 32/73
● Hepatic insufficiency---> encephalopathy

7/17/2019 Liver anatomy and physiology medicine
http://slidepdf.com/reader/full/liver-anatomy-and-physiology-medicine 33/73
● ACUTE
● Rapid massive loss of hepatocyte functional mass
without pre-existing liver disease
● CHRONIC
● Viral hepatitis, metabolic diseases, alochol abuse,
toxins
● Ongoing & progressive hepatocyte necrosis →
fibrosis & regeneration→ cirrhosis

7/17/2019 Liver anatomy and physiology medicine
http://slidepdf.com/reader/full/liver-anatomy-and-physiology-medicine 34/73
ACUTE LIVER FAILURE
● Development of encephalopathy within 26
weeks of onset of any hepatic symptom
● Fulminant Hepatic Failure
● Subfulminant Hepatic Failure

7/17/2019 Liver anatomy and physiology medicine
http://slidepdf.com/reader/full/liver-anatomy-and-physiology-medicine 35/73
ACUTE LIVER FAILURE
● Etiology
● Acetaminophen overdose
● Viral hepatitis
● Other drug toxicities
● 20% will survive--> N liver function

7/17/2019 Liver anatomy and physiology medicine
http://slidepdf.com/reader/full/liver-anatomy-and-physiology-medicine 36/73
HEPATIC ENCEPHALOPATHY

7/17/2019 Liver anatomy and physiology medicine
http://slidepdf.com/reader/full/liver-anatomy-and-physiology-medicine 37/73
ACUTE LIVER FAILURE
● Treatment
● Supportive care/Medical Management
● LIVER TRANSPLANT – 60% survival rate

7/17/2019 Liver anatomy and physiology medicine
http://slidepdf.com/reader/full/liver-anatomy-and-physiology-medicine 38/73
CRITERIA FOR SELECTION OF PATIENTS MOST LIKELY TO BENEFIT FROM
LIVER TRANSPLANTATION
● ACETAMINOPHEN TOXICITY
● PH< 7.3 regardless of grade of encephalopathy
● PT > 100 sec (INR >6.5) & creatinine > 300
umol/L (in patients with grade 3-4
encephalopathy
● VIRAL HEPATITIS/DRUG REACTION
● PT > 100 sec (INR >6.5 regardless of grade of
encephalopathy)
● or....

7/17/2019 Liver anatomy and physiology medicine
http://slidepdf.com/reader/full/liver-anatomy-and-physiology-medicine 39/73
CRITERIA FOR SELECTION OF PATIENTS MOST LIKELY TO BENEFIT FROM
LIVER TRANSPLANTATION
●
VIRAL HEPATITIS/DRUG REACTION ● Any 3 of the following regardless of the grade of
encephalopathy)
●
1. age <11 & >40● 2. duration of jaundice before the onset of
encephalopathy> 7 days
● 3. cause : non-HepA, non-HepB, halothane
hepatitis, idiosyncratic drug reaction
● 4. PT > 50 sec (INR > 3.5)
● 5. serum bilirubin > 300 umol/L (> 17.5 mg/dl)

7/17/2019 Liver anatomy and physiology medicine
http://slidepdf.com/reader/full/liver-anatomy-and-physiology-medicine 40/73
CHRONIC LIVER FAILURE
CIRRHOSIS

7/17/2019 Liver anatomy and physiology medicine
http://slidepdf.com/reader/full/liver-anatomy-and-physiology-medicine 41/73
CIRRHOSIS
● Hepatic fibrosis
● Nodular regeneration
● Etiology
● Pathogenesis
● Clinical manifestations

7/17/2019 Liver anatomy and physiology medicine
http://slidepdf.com/reader/full/liver-anatomy-and-physiology-medicine 42/73
CIRRHOSIS
Cirrhosis & portal hypertension negativeimpact on the outcomes of nontransplant
surgical procedures

7/17/2019 Liver anatomy and physiology medicine
http://slidepdf.com/reader/full/liver-anatomy-and-physiology-medicine 43/73
ULTRASOUND

7/17/2019 Liver anatomy and physiology medicine
http://slidepdf.com/reader/full/liver-anatomy-and-physiology-medicine 44/73
ULTRASOUND
● Coarsened
echotexture
● Enlarged Left lobe

7/17/2019 Liver anatomy and physiology medicine
http://slidepdf.com/reader/full/liver-anatomy-and-physiology-medicine 45/73
COMPUTED TOMOGRAPHY SCANS
6
CHILD TURCOTTE PUGH CLASSIFICATION

7/17/2019 Liver anatomy and physiology medicine
http://slidepdf.com/reader/full/liver-anatomy-and-physiology-medicine 46/73
CHILD-TURCOTTE-PUGH CLASSIFICATION
CHILD TURCOTTE PUGH

7/17/2019 Liver anatomy and physiology medicine
http://slidepdf.com/reader/full/liver-anatomy-and-physiology-medicine 47/73
CHILD-TURCOTTE-PUGH
CLASSIFICATION

7/17/2019 Liver anatomy and physiology medicine
http://slidepdf.com/reader/full/liver-anatomy-and-physiology-medicine 48/73
PORTAL HYPERTENSION

7/17/2019 Liver anatomy and physiology medicine
http://slidepdf.com/reader/full/liver-anatomy-and-physiology-medicine 49/73
PORTAL HYPERTENSION
●
WHVP or direct portal venous pressure that is>5 mmHg greater than the inferior vena cava(IVC) pressure,
●
a splenic pressure of >15 mmHg,● or a portal venous pressure measured at
surgery of >20 mmHg
●
● A portal pressure of >12 mmHg is necessary for
varices to form and subsequently bleed.

7/17/2019 Liver anatomy and physiology medicine
http://slidepdf.com/reader/full/liver-anatomy-and-physiology-medicine 50/73
Etiology
Pathophysiology

7/17/2019 Liver anatomy and physiology medicine
http://slidepdf.com/reader/full/liver-anatomy-and-physiology-medicine 51/73
Pathophysiology
Cli i l if t ti

7/17/2019 Liver anatomy and physiology medicine
http://slidepdf.com/reader/full/liver-anatomy-and-physiology-medicine 52/73
Clinical manifestations

7/17/2019 Liver anatomy and physiology medicine
http://slidepdf.com/reader/full/liver-anatomy-and-physiology-medicine 53/73
Clinical manifestations
● Cruveilhier-Baumgarten murmur
● Veins of Retzes- retroperitoneal

7/17/2019 Liver anatomy and physiology medicine
http://slidepdf.com/reader/full/liver-anatomy-and-physiology-medicine 54/73
SURGICAL CONCERNS
● Encephalopathy
●
Ascites
● Variceal bleeding
VARICEAL BLEEDING

7/17/2019 Liver anatomy and physiology medicine
http://slidepdf.com/reader/full/liver-anatomy-and-physiology-medicine 55/73
VARICEAL BLEEDINGPrevention of bleeding
●
improvement of liver function (i.e., abstention fromalcohol),
● avoidance of aspirin and NSAIDs,
● propranolol or nadolol (nonselective beta blockers)
● prophylactic endoscopic variceal ligation (EVL)-
– medium to large varices,
– every 1 to 2 weeks until obliteration,
● Esophagogastroduodenoscopy (EGD) 1 to 3 monthslater
● Surveillance EGD every 6 months

7/17/2019 Liver anatomy and physiology medicine
http://slidepdf.com/reader/full/liver-anatomy-and-physiology-medicine 56/73
VARICEAL BLEEDINGManagement of bleeding
● ICU for resuscitation
● Blood resuscitation to a hemoglobin level of ~ 8 g/dL. Overreplacment of
packed red blood cells and the overzealous administration of saline →
rebleeding and increased mortality.
● fresh-frozen plasma and platelets
● short-term prophylactic antibiotics : ceftriaxone 1 g/day IV is often given.
● Vasopressin, administered IV at a dose of 0.2 to 0.8 units/min,
● Somatostatin and its analogue octreotide (initial bolus of 50 g IV followed bycontinuous infusion of 50 g/h) also cause splanchnic vasoconstriction.
● EGD & EVL
Even when aggressive pharmacologic and endoscopic therapies are

7/17/2019 Liver anatomy and physiology medicine
http://slidepdf.com/reader/full/liver-anatomy-and-physiology-medicine 57/73
Even when aggressive pharmacologic and endoscopic therapies are
initiated and these treatment options are maximized, 10 to 20% of
patients with variceal bleeding will continue to bleed. Shunt therapy,
with either surgical shunts or TIPS, has been shown to control
refractory variceal bleeding in >90% of treated individuals. Shuntsurgery usually is considered only in patients with preserved hepatic
function (i.e., CTP class A); TIPS is used in patients with
decompensated liver disease (i.e., CTP class B or C). However, the use
of these treatment options is dependent on local expertise.
Balloon tamponade using a Sengstaken-Blakemore tube will control
refractory variceal bleeding in >80% of patients. However, its
application is limited due to the potential for complications, whichinclude aspiration and esophageal perforation. Therefore, use of a
Sengstaken-Blakemore tube should be limited to short-term therapy
(<24 hours) in those patients awaiting definitive care.
TRANSJUGULAR INTRAHEPATIC

7/17/2019 Liver anatomy and physiology medicine
http://slidepdf.com/reader/full/liver-anatomy-and-physiology-medicine 58/73
TRANSJUGULAR INTRAHEPATIC
PORTOSYSTEMIC SHUNT● Control variceal bleeding in
>90% refractory to medical
treatment
● Complications : bleeding,
infection, renal failure,
decreased hepatic function,
hepatic encephalopathy

7/17/2019 Liver anatomy and physiology medicine
http://slidepdf.com/reader/full/liver-anatomy-and-physiology-medicine 59/73
PORTOCAVAL SHUNT
Eck fistula
● high incidence of
hepatic
encephalopathy
● decreased liver
function
●
makes subsequenthepatic transplantation
much more technically
difficult

7/17/2019 Liver anatomy and physiology medicine
http://slidepdf.com/reader/full/liver-anatomy-and-physiology-medicine 60/73
MESOCAVAL SHUNT
● technically easier
● does not adversely
affect subsequent
hepatictransplantation.
● higher incidence of
shunt thrombosis and
rebleeding

7/17/2019 Liver anatomy and physiology medicine
http://slidepdf.com/reader/full/liver-anatomy-and-physiology-medicine 61/73
DISTAL SPLENORENAL (WARREN)
● Used most often
● lower rate of hepatic
encephalopathy and
decompensation,
● not interfering with
subsequent hepatic
transplantation

7/17/2019 Liver anatomy and physiology medicine
http://slidepdf.com/reader/full/liver-anatomy-and-physiology-medicine 62/73
DISTAL SPLENORENAL (WARREN)
● Used most often
● lower rate of hepatic
encephalopathy and
decompensation,
● not interfering with
subsequent hepatic
transplantation

7/17/2019 Liver anatomy and physiology medicine
http://slidepdf.com/reader/full/liver-anatomy-and-physiology-medicine 63/73
SUGIURA PROCEDURE
● In patients withextrahepatic portal
vein thrombosis
and refractoryvariceal bleeding

7/17/2019 Liver anatomy and physiology medicine
http://slidepdf.com/reader/full/liver-anatomy-and-physiology-medicine 64/73
BENIGN SOLID LIVER TUMORS

7/17/2019 Liver anatomy and physiology medicine
http://slidepdf.com/reader/full/liver-anatomy-and-physiology-medicine 65/73
CYSTIC DISEASES OF THE LIVER

7/17/2019 Liver anatomy and physiology medicine
http://slidepdf.com/reader/full/liver-anatomy-and-physiology-medicine 66/73
● Congenital cysts
● Biliary cystadenoma
●
Polycystic liver disease● Caroli's disease

7/17/2019 Liver anatomy and physiology medicine
http://slidepdf.com/reader/full/liver-anatomy-and-physiology-medicine 67/73
LIVER INFECTIONS

7/17/2019 Liver anatomy and physiology medicine
http://slidepdf.com/reader/full/liver-anatomy-and-physiology-medicine 68/73
● Pyogenic liver abscess
● Amoebic liver abscess
●
Hydatid Disease● Ascariasis
● Schistosomiasis
● Viral hepatitis
● The most common source of liver abscess is the biliary tree in
patients with cholecystitis choledocholithiasis or cholangitis

7/17/2019 Liver anatomy and physiology medicine
http://slidepdf.com/reader/full/liver-anatomy-and-physiology-medicine 69/73
patients with cholecystitis, choledocholithiasis, or cholangitis
● Less common sources include other intra-abdominal processes,
such as appendicitis or diverticulitis, and hematogenous spread from
sources such as an infected heart valve or the oral cavity a the
vascular route is associated with multiple abscesses
● The right hepatic lobe is affected more than twice as frequently as
the left, due to vascular anatomy
● Aspiration of abscess fluid and subsequent culture guide antibiotic
choice
● Failure to culture pathogenic organism(s) may be due to prior
antibiotic treatment or inadequate anaerobic culture
● Treatment includes antibiotics and often either percutaneous or
surgical drainage/debridement, depending on the size, number, and
complexity of the abscess(es)
● Less common sources include other intra-abdominal processes such as

7/17/2019 Liver anatomy and physiology medicine
http://slidepdf.com/reader/full/liver-anatomy-and-physiology-medicine 70/73
● Less common sources include other intra abdominal processes, such as
appendicitis or diverticulitis, and hematogenous spread from sources such as an
infected heart valve or the oral cavity
●
Amebic liver abscess should be considered in endemic areas or patients whohave been to the tropics
● Fungal microabscesses are seen primarily in patients with compromised
immune systems
● Rarely, liver abscess may be due to trauma, secondary infection from an
amebic abscess or a necrotic malignant hepatic tumor, or direct extension from
local structures
● Common pathogens include Streptococcus spp., Escherichia coli, Klebsiella,
and Bacteroides spp. Polymicrobial infections occur in 15% to 20% of patients;
approximately the same percentage have multiple abscesses
●

7/17/2019 Liver anatomy and physiology medicine
http://slidepdf.com/reader/full/liver-anatomy-and-physiology-medicine 71/73
● Amebic liver abscess follows vascular spread of Entamoeba histolytica
from the colon in patients with the intestinal infection amebiasis. Amebic
abscesses may be very large; they contain aspirate with 'anchovy-sauce'
color and consistency
● Liver abscess in a child suggests immunocompromise
● A single abscess is the most common presentation; spread to the liver via
the vascular route is associated with multiple abscesses
● The right hepatic lobe is affected more than twice as frequently as the
left, due to vascular anatomy
● Aspiration of abscess fluid and subsequent culture guide antibiotic
choice
● Failure to culture pathogenic organism(s) may be due to prior antibiotictreatment or inadequate anaerobic culture
● Treatment includes antibiotics and often either percutaneous or surgical
drainage/debridement, depending on the size, number, and complexity of
the abscess(es)

7/17/2019 Liver anatomy and physiology medicine
http://slidepdf.com/reader/full/liver-anatomy-and-physiology-medicine 72/73
MALIGNANT LIVER TUMORS

7/17/2019 Liver anatomy and physiology medicine
http://slidepdf.com/reader/full/liver-anatomy-and-physiology-medicine 73/73
●
3rd most common cancer mortality
● Risk factors : Hep B, Hep C, Cirrhosis, aflatoxins, flukes
● Inc serum AFP in 55-95%
● Resection if :
● Single lesion < 5 cm, up to 3 lesions each < 3 cm
● Childs A & B
● No portal hypertension
● Tumor recurrence : 70% at 5 years