Lipid preparations of amphotericin for the treatment of fungal infections
12
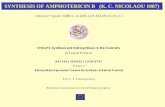
Correspondence EVALUATION OF LEPTIN PROTEIN LEVELS IN PATIENTS WITH COOLEY’S ANAEMIA Endocrine disorders related to toxic effects of iron overload, such as short stature, delayed puberty and hypogonadism, represent major problems in both adolescent and adult thalassaemic patients. It has been suggested that gonadal dysfunction in these patients might be characterized mainly by a neuroendocrine dysfunction resulting in impaired hypothalaemic releasing hormone production, which is inadequate for proper pituitary stimulation (Kattamis & Kattamis, 1995). Pulsatile gonadotrophin releasing hor- mone (GnRH) treatment seems to re-establish, at least partially, the correct pituitary–gonadal function. Leptin, a recently discovered adipocyte-derived hormone, acts primarily at the hypothalamus, where it has effects on appetite, energy expenditure and the neuroendocrine axes. Leptin-deficient mice exhibit a complex phenotype which includes hypogonadism, impaired sexual maturation and infertility due to hypothalamic–pituitary hormone failure (Flier & Maratos-Flier, 1998). Exogenous leptin allows the recovery of the reproductive function. Recently, a related man and woman with congenital leptin deficiency have been described. Both showed hypogonadism (i.e. small penis and testis, primary amenorrhoea, respectively) of hypothalamic origin, suggesting that leptin not only controls body mass but may also be necessary to initiate human puberty (Strobel et al, 1998). To evaluate leptin levels in thalassaemic patients, blood samples were collected after an overnight fast from 162 patients with Cooley’s anaemia, 78 males (age: mean 19 6 7 years, range 5–39) and 84 females (age: mean 20 6 12 years, range 6–41) and from 138 normal subjects, matched for gender, age and body mass index (BMI). Leptin was measured by a commercial radioimmunoassay (Linco Research Inc., St Louis, Mo.). BMI was calculated as weight (kg) divided by height (m) squared. Mean leptin concentration was 2·69 6 1·23 ng/ml in thalassaemic males; this value appeared to be significantly lower (P < 0·0005) than in controls (6·86 6 2·71 ng/ml). Although thalassaemic females also had lower leptin levels (6·37 6 2·9 ng/ml) than matched normal subjects (9·37 6 5·2 ng/ml), the differences were not significant (P < 0·05). Furthermore, the physiologically positive BMI/ leptinaemia relationship, consistently found in normal and obese subjects, disappeared in thalassaemic males and was present, but lacked statistical significance in females (Fig 1). Therefore the adipocytes of thalassaemic patients seem unable to maintain adequate leptin production. The lack of any association between circulating leptin and body fat has already been observed in elderly subjects (Moller et al, 1998). Iron deposition studies in animal models have demonstrated that, although absent in the dermis, iron is well represented in subcutaneous layer adipocytes and that iron ions can seriously inhibit adipocyte activity (Youson & Sargent, 1984; Rejholcova et al, 1988). The differences between genders cannot be explained by an unequal iron overload (males, ferritin mean: 2·200 6 0·945 mg/l; females, ferritin mean: 1·938 6 0·848 mg/l; P < 0·1), but could be the consequence of the physiologically different extension of the target organ (i.e. more subcutaneous adipose tissue in women). These results suggest that adipose tissue dysfunction can be considered as one of the endocrinopathies affecting thalassaemic patients. The consequent low leptin levels might play a role in the neuroendocrine dysfunctions reported in these patients. 1 Department of Paediatrics, E MANUELE Second University of Napoli, M IRAGLIA DEL G IUDICE 1 Napoli, S ILVERIO P ERROTTA * 2 Centro Microcitemie, M ARIA T ERESA C ARBONE * Ospedale Cardarelli, C LAUDIA C ALABRO ` * Napoli, and L UIGI E SPOSITO * 3 29 o Divisione di Pediatria, C ARLO D E ROSA 2 Settore Microcitemie, A NNA S AVIANO 3 Ospedale Cardarelli, ROSARIO D I T ORO * Napoli, Italy L AURA P ERRONE * REFERENCES Flier, J.S., & Maratos-Flier, E. (1998) Obesity and the hypo- thalamus: novel peptides for new pathways. Cell, 92, 437–440. British Journal of Haematology , 1999, 105, 839–850 839 q 1999 Blackwell Science Ltd Fig 1. Correlation between body mass index (BMI) and serum leptin concentration in 70 normal females (line 1: r ¼ 0·60; P < 0·0005), in 68 normal males (line 2: r ¼ 0·53; P < 0·001), in 84 thalassaemic females (line 3: r ¼ 0·25, P > 0·05) and in 78 thalassaemic males (line 4: r ¼¹0·064, P > 0·25).
-
Upload
jayesh-mehta -
Category
Documents
-
view
216 -
download
2
Transcript of Lipid preparations of amphotericin for the treatment of fungal infections

Correspondence
EVALUATION OF LEPTIN PROTEIN LEVELS IN PATIENTS WITH COOLEY’S ANAEMIA
Endocrine disorders related to toxic effects of iron overload,such as short stature, delayed puberty and hypogonadism,represent major problems in both adolescent and adultthalassaemic patients. It has been suggested that gonadaldysfunction in these patients might be characterized mainlyby a neuroendocrine dysfunction resulting in impairedhypothalaemic releasing hormone production, which isinadequate for proper pituitary stimulation (Kattamis &Kattamis, 1995). Pulsatile gonadotrophin releasing hor-mone (GnRH) treatment seems to re-establish, at leastpartially, the correct pituitary–gonadal function.
Leptin, a recently discovered adipocyte-derived hormone,acts primarily at the hypothalamus, where it has effects onappetite, energy expenditure and the neuroendocrine axes.Leptin-deficient mice exhibit a complex phenotype whichincludes hypogonadism, impaired sexual maturation andinfertility due to hypothalamic–pituitary hormone failure(Flier & Maratos-Flier, 1998). Exogenous leptin allows therecovery of the reproductive function. Recently, a relatedman and woman with congenital leptin deficiency have beendescribed. Both showed hypogonadism (i.e. small penis andtestis, primary amenorrhoea, respectively) of hypothalamicorigin, suggesting that leptin not only controls body massbut may also be necessary to initiate human puberty (Strobelet al, 1998).
To evaluate leptin levels in thalassaemic patients, bloodsamples were collected after an overnight fast from 162patients with Cooley’s anaemia, 78 males (age: mean 19 6 7years, range 5–39) and 84 females (age: mean 20 6 12years, range 6–41) and from 138 normal subjects, matchedfor gender, age and body mass index (BMI). Leptin wasmeasured by a commercial radioimmunoassay (Linco
Research Inc., St Louis, Mo.). BMI was calculated as weight(kg) divided by height (m) squared.
Mean leptin concentration was 2·69 6 1·23 ng/ml inthalassaemic males; this value appeared to be significantlylower (P <0·0005) than in controls (6·86 6 2·71 ng/ml).Although thalassaemic females also had lower leptinlevels (6·37 6 2·9 ng/ml) than matched normal subjects(9·37 6 5·2 ng/ml), the differences were not significant(P<0·05). Furthermore, the physiologically positive BMI/leptinaemia relationship, consistently found in normal andobese subjects, disappeared in thalassaemic males and waspresent, but lacked statistical significance in females (Fig 1).Therefore the adipocytes of thalassaemic patients seemunable to maintain adequate leptin production. The lack ofany association between circulating leptin and body fat hasalready been observed in elderly subjects (Moller et al, 1998).Iron deposition studies in animal models have demonstratedthat, although absent in the dermis, iron is well representedin subcutaneous layer adipocytes and that iron ions canseriously inhibit adipocyte activity (Youson & Sargent, 1984;Rejholcova et al, 1988). The differences between genderscannot be explained by an unequal iron overload(males, ferritin mean: 2·200 6 0·945 mg/l; females, ferritinmean: 1·938 6 0·848 mg/l; P <0·1), but could be theconsequence of the physiologically different extension ofthe target organ (i.e. more subcutaneous adipose tissue inwomen).
These results suggest that adipose tissue dysfunction canbe considered as one of the endocrinopathies affectingthalassaemic patients. The consequent low leptin levelsmight play a role in the neuroendocrine dysfunctionsreported in these patients.
1Department of Paediatrics, E M A N U E L E
Second University of Napoli, M I R A G L I A D E L G I U D I C E1
Napoli, S I LV E R I O P E R RO T TA *2Centro Microcitemie, M A R I A T E R E S A C A R B O N E *Ospedale Cardarelli, C L AU D I A C A L A B RO *Napoli, and L U I G I E S P O S I T O *329o Divisione di Pediatria, C A R L O D E RO S A
2
Settore Microcitemie, A N NA S AV I A N O3
Ospedale Cardarelli, RO S A R I O D I T O RO *Napoli, Italy L AU R A P E R RO N E *
REFERENCES
Flier, J.S., & Maratos-Flier, E. (1998) Obesity and the hypo-thalamus: novel peptides for new pathways. Cell, 92, 437–440.
British Journal of Haematology, 1999, 105, 839–850
839q 1999 Blackwell Science Ltd
Fig 1. Correlation between body mass index (BMI) and serum leptinconcentration in 70 normal females (line 1: r ¼ 0·60; P<0·0005),in 68 normal males (line 2: r ¼ 0·53; P<0·001), in 84 thalassaemicfemales (line 3: r ¼ 0·25, P>0·05) and in 78 thalassaemic males(line 4: r ¼¹0·064, P>0·25).

Kattamis, C.A. & Kattamis, A.C. (1995) Management of thalasse-mias: growth and development, hormone substitution, vitaminsupplementation, and vaccination. Seminars in Hematology, 32,269–279.
Moller, N., O’Brien, P. & Nair, K.S. (1998) Disruption of therelationship between fat content and leptin levels with aging inhumans. Journal of Clinical Endocrinology and Metabolism, 83, 931–934.
Rejholcova, M., Wilhelm, J. & Svoboda, P. (1998) Lipid peroxidationinhibits norepinephrine-stimulated lipolysis in rat adipocytes:
reduction of beta-adrenoceptor number. Biophysical andBiochemical Research Communications, 150, 802–810.
Strobel, A., Issad, T., Camoin, L., Ozata, M. & Strosberg, A.D. (1998)A leptin missense mutation associated with hypogonadism andmorbid obesity. Nature Genetics, 18, 213–215.
Youson, J.H. & Sargent, P.A. (1984) Iron deposition in theintegument of lampreys. Anatomical Record, 209, 461–468.
Keywords: Cooley’s anaemia, leptin, thalassaemia.
INDOLENT COURSE AS PRESENTATION IN T-PROLYMPHOCYTIC LEUKAEMIA
We read with interest the paper by Garand et al (1998)relating to the clinical course of T-prolymphocytic leukaemia(T-PLL). Although T-PLL has typically been considered anaggressive disease with fatal course and short survival(Matutes et al, 1991; Hoyer et al, 1995), their data supportthe existence of two patient populations: one with an initialrapidly progressive clinical course and another with aninitial indolent phase that progressed to an aggressive stageafter a variable period. We have recently observed twopatients with T-PLL presenting this biphasic evolution.
The first patient was an asymptomatic 53-year-old manwith isolated stable lymphocytosis (leucocytes 10 × 109/lwith 53% prolymphocytes, Hb 15·2 g/dl, platelets152 × 109/l). Lymphocytes expressed a post-thymicimmunophenotype: TdT¹, CD2þ, CD3þ, CD5þ, CD7(i)þ,CD1a¹, and CD4þ CD8¹. Bone marrow was infiltratedwith 15% prolymphocytes. After an asymptomatic clinicalcourse of 18 months with stable leucocytosis, the patientdeveloped B symptoms, peripheral lymphadenopathies,hepatosplenomegaly, and papular skin lesions. Leucocytosisincreased rapidly to 75 × 109/l with 82% prolymphocytes.Bone marrow biopsy demonstrated infiltration by 83% ofprolymphocytes. Biopsies of a peripheral adenopathy andskin showed infiltration by prolymphocytes. Despitevarious different chemotherapy combinations (including20-deoxycoformycin), the disease progressed and the patientdied 24 months from the diagnosis.
The second patient was an 86-year-old man whopresented with malaise. The physical examination wasnormal. Laboratory data were unremarkable except forleucocytosis of 12·5 × 109/l with 75% prolymphocytes.Lymphocytes expressed a post-thymic immunophenotypeand were also CD4þ CD8¹. The patient did not receivetreatment. After 13 months he developed lymphadenopathy,hepatosplenomegaly and rapidly increasing leucocytosis(173 × 109/l with 96% prolymphocytes). Bone marrowbiopsy revealed infiltration by 68% of prolymphocytes.Chemotherapy with chlorambucil and prednisone wasstarted, but the patient died due to disease progression 21months from the diagnosis.
Our cases confirm that a silent indolent course mayprecede some cases of T-PLL. In both patients, after an initialindolent phase of 18 and 13 months respectively, the disease
rapidly progressed to an aggressive form characterized byB symptoms, liver and spleen enlargement, lymphadeno-pathies, skin lesions and rapidly increasing leucocytosis.Response to treatment was very poor, and the mediansurvival after progression was short, 6 and 8 monthsrespectively.
We agree with Garand et al (1998) who proposed that,although T-PLL generally has a rapidly aggressive course, ina significant number of patients the disease may present abiphasic evolution with an initial stable clinical coursepreceding the invariably fatal progression. We believe thatthe identification of this subgroup of patients would be ofgreat clinical value in order to assay therapeutic strategiesfor increasing the duration of the stable phase, because oncethe disease transforms into an aggressive stage, therapeuticresults are discouraging.
Department of Haematology, E VA D O M I N G O -D O M E N E C H
Hospital Duran i Reynals, E VA G O N Z A L E Z -B A RC A
Institut Catala d’Oncologia, A N T O N I O S A L A R
Ciutat Sanitaria i A L I C I A D O M I N G O C L A RO S
Universitaria de Bellvitge, A L B E RT G R A N E N A
Hospitalet de LLobregat,Barcelona, Spain
REFERENCES
Garand, R., Goasguen, J., Brizard, A., Buisine, J., Carpentier, A.,Claisse, J.F., Duchayne, E., Lagrange, M., Segonds, C., Troussard,X. & Flandrin, G. (1998) Indolent course as a relatively frequentpresentation in T-prolymphocytic leukaemia. British Journal ofHaematology, 103, 488–495.
Hoyer, J.D.. Ross, C.W., Li, C.Y., Witzing, T.E., Gascoyne, R.D.,Dewald, G.W. & Hanson, C.A. (1995) True T-cell chroniclymphocytic leukemia: a morphologic and immunophenotypicstudy of 25 cases. Blood, 86, 1163–1169.
Matutes, E., Brito-Babapulle, V., Swansbury, V., Ellis, J., Morilla, R.,Dearden, C., Sempere, A. & Catovsky, D. (1991) Clinical andlaboratory features of 78 cases of T-prolymphocytic leukemia.Blood, 78, 3269–3274.
Keywords: T-prolymphocytic leukaemia, indolent course,leucocytosis.
840 Correspondence
q 1999 Blackwell Science Ltd, British Journal of Haematology 105: 839–850

CHRONIC HEPATITIS C VIRUS INFECTION AND PRIMARY CUTANEOUS B-CELL LYMPHOMA
Primary cutaneous B-cell lymphoma (CBCL) comprises 10–25% of all primary cutaneous lymphomas (Willemze et al,1997). The possibility of an infectious origin of CBCL hasbeen suggested, but the agents so far implicated, such as theEpstein-Barr virus, human T-lymphocyte virus-1, humanherpesvirus 8 and Borrelia burgdorferi, could account foronly a proportion of cases of CBCL.
There is growing evidence that hepatitis C virus (HCV)is involved in the pathogenesis of certain B-cell lympho-proliferative disorders, including type II mixed cryo-globulinaemia and, possibly, monoclonal gammopathiesand non-Hodgkin’s lymphoma (NHL) (Pioltelli et al, 1996;De Vita et al, 1997; Luppi et al, 1998). No information is sofar available on the possible association between HCVinfection and CBCL. To address this issue, we haveexamined 34 consecutive patients with CBCL amongthose attending the Department of Dermatology of theUniversity of Milan, Italy, between January 1989 andAugust 1998. There were 21 males and 13 females, with amedian age of 52 years (range 29–83). The diagnosis ofCBCL was based on clinical, histopathological and immuno-phenotypic criteria, according to the classification forprimary cutaneous lymphomas of the European Organisa-tion for Research and Therapy of Cancer (EORTC) (Willemzeet al, 1997). 32 patients (94%) had follicle centre celllymphoma, one had immunocytoma/marginal B-cell lym-phoma and one had plasmacytoma. Complete staging wasnegative for extracutaneous localizations of the disease andall patients were treated by surgery and/or radiotherapyand interferon (IFN)-a. Most of them showed severalcutaneous relapses. Four patients with follicle centre celllymphoma showed dissemination to extracutaneous sitesincluding lymph nodes (two cases) and bone marrow (twocases), 6 months to 3 years after diagnosis. These patientswere treated by cyclophosphamide, epirubicin, vincristineand prednisolone (CEOP) chemotherapy; however, thelast two cases (bone marrow relapses in absence ofany cutaneous lesions) died after the second cycle ofpolychemotherapy.
Anti-HCV antibodies were determined by a third-genera-tion enzyme immunoassay, and confirmed by a recombi-nant immunoblot assay (both supplied by Ortho DiagnosticSystems, Raritan, N.J., U.S.A.). Of the 34 patients withCBCL, only one patient (3%) had a confirmed anti-HCVreactivity; the serum HCV RNA tested positive by RT-PCR(Amplicor HCV kit, Roche Molecular Systems, Basel,Switzerland). Hence, the frequency of HCV infection wassubstantially lower than that previously reported amongpatients with non-cutaneous B-cell NHL in Milan (20%)(Pioltelli et al, 1996), and was comparable to that observedin the general population (3·2%) of the same geographicarea (Bellentani et al, 1994).
These results were in part unexpected, since HCV-relatedB-cell NHL cases present some similarities with CBCL,including a low-grade clinical behaviour and a histologicsubtype generally consistent with follicle centre cell and
marginal zone lymphoma (Luppi et al, 1998). Moreover, theyfrequently have an extranodal localization at the onset(De Vita et al, 1997). However, it should be noted thatthe extranodal sites of oncogenesis in HCV-related B-cellNHL are preferably the target organs of HCV infection(De Vita et al, 1997), and that HCV is not related tothe pathogenesis of gastric lymphomas of the mucosa-associated lymphoid tissue (MALT) type (Tkoub et al, 1998).Thus, our data further strengthen the current opinionthat CBCL represents a distinctive group among B-cell NHLs.Furthermore, they support the hypothesis that CBCLand MALT-type lymphomas, besides having similarfeatures at the histological and clinical levels (Willemzeet al, 1997), might also have common aetiopathogeneticmechanisms.
Centro Trasfusionale e di DA N I E L E P R AT I
Immunologia dei Trapianti A L B E RT O Z A N E L L A
and Divisione di Ematologia, C L AU D I A D E M AT T E I
IRCCS Ospedale Maggiore E L E N A FA R M A
di Milano, and C A R L A B O S C H E T T I
*Istituto di Scienze Dermatologiche G I RO L A M O S I RC H I A
IRCCS Ospedale Maggiore- L U I G I A V E N E G O N I *Universita degli Studi di Milano, E M I L I O B E RT I *
Milano, Italy
REFERENCES
Bellentani, S., Tiribelli, C., Saccoccio, G., Sodde, M., Fratti, N.,De Martin, C., Cristianini, C., and the Dionysos Study Group(1994) Prevalence of chronic liver disease in the generalpopulation of Northern Italy: the Dionysos study. Hepatology, 20,1442–1449.
De Vita, S., Sacco, C., Sansonno, D., Gloghini, A., Dammacco, F.,Crovatto, M., Santini, G., Dolcetti, R., Boiocchi, M., Carbone, A.& Zagonel, V. (1997) Characterization of overt B-celllymphomas in patients with hepatitis C virus infection. Blood,90, 776–782.
Luppi, M., Longo, G., Ferrari, M.G., Barozzi, P., Marasca, R.,Morselli, M., Valenti, C., Mascia, T., Vandelli, L., Vallisa, D.,Cavanna, L. & Torelli, G. (1998) Clinico-pathological character-ization of hepatitis C virus-related B-cell non-Hodgkin’s lympho-mas without symptomatic cryoglobulinemia. Annals of Oncology,9, 495–498.
Pioltelli, P., Zehender, G., Monti, G., Monteverde, A. & Galli, M.(1996) HCV and non-Hodgkin lymphoma. Lancet, 347, 624–625.
Tkoub, E.M., Haioun, C., Pawlotsky, J.M., Dhumeaux, D. &Delchier, J.C. (1998) Chronic hepatitis C virus and gastric MALTlymphoma. Blood, 91, 360.
Willemze, A., Kerl, H., Sterry, W., Berti, E., Cerroni, L., Chimenti, S.,Diaz-Perez, J.L., Geerts, M.L., Goos, M., Knobler, R., Ralfkiaer, E.,Santucci, M., Smith, N., Wechsler, J., van Vloten, W.A. &Meijer, C.J.L.M. (1997) EORTC classification for primary cuta-neous lymphomas: a proposal from the cutaneous lymphomastudy group of the European Organisation for Research andTreatment of Cancer. Blood, 90, 354–371.
Keywords: hepatitis C virus, cutaneous B-cell lymphoma.
841Correspondence
q 1999 Blackwell Science Ltd, British Journal of Haematology 105: 839–850

BUDD-CHIARI SYNDROME ASSOCIATED WITH HOMOZYGOUS FACTOR V LEIDEN MUTATION
We read with interest the article by Leebeek et al (1998)describing a patient with Budd-Chiari syndrome (BCS) andportal and mesenteric vein thrombosis who was homozygousfor factor V Leiden (FVL) mutation and was successfullytreated by transjugular porto-systemic stent (TIPS) place-ment followed by local thrombolytic treatment. In recentyears, BCS has been associated with FVL mutation, and mostof the cases were found to be heterozygous (Mahmoud et al,1997; Das et al, 1998; Mohanty et al, 1998).
Recently a 22-year-old unmarried north Indian (Punjabi)female was referred to our hospital with insidious onsetabdominal distension of 4 months duration and reducedurinary output. Examination revealed hepatomegaly (2 cmbelow right costal margin), a minimally palpable spleen,ascites and umbilical hernia. Liver function tests werenormal. The patient had a past history of jaundice at theage of 6 years. Hepatic ultrasonography revealed nodularhepatomegaly with heterogenous echotexture. Hepatic veinswere occluded and the inferior vena cava was narrowed inthe retrohepatic area. Intrahepatic comma-shaped collat-erals were seen in both right and left lobes. Caudate lobehypertrophy and ascites was also noted. The patient is beingtreated symptomatically. An ultrasound showed features ofliver cirrhosis with thrombosis of the hepatic veins, amesoatrial shunt/liver transplantation is contemplated inthe patient.
A thrombophilia screen showed normal protein C andprotein S levels and negative lupus anticoagulant screen.DNA analysis was carried out with MnI1 digestion of theamplified factor V DNA fragment and a homozygous patternwas obtained. Analysis of the four polymorphisms in exon 13of the factor V gene was done (Cox et al, 1996). A 637 bpsegment of exon 13 was amplified by the polymerase chainreaction and digested with either Hinf1 or Taq1, revealingpolymorphisms at positions 2298 (T/C), 2325 (C/T), 2391(G/A) and 2833 (A/T) of the factor V gene. Our case with thehomozygous FVL mutation showed the CTAA/CTAA haplotype.
FVL mutation has been documented to be present in theindigenous population of north India with an allelefrequency of 1·9% (Garewal et al, 1997). An association ofBCS and FVL mutation has been noted in Indian patients(Das et al, 1998; Mohanty et al, 1998). However, to the best
of our knowledge, this case is the first case of FVL mutationin the homozygous state from India. Two other cases havebeen associated with BCS and homozygous FVL mutation inthe literature (Leebeek et al, 1998; Mahmoud et al, 1997).The haplotype of this case is the one significantly associatedwith FVL mutation in the European populations (Cos et al,1996). This case supports the theory that the FVL mutationarose from a single mutational event arising in a singleCaucasoid ancestor, which spread to the Caucasoid sub-populations, including Europeans, Jews, Arabians and Indians.Haplotypic analysis of more homozygous individuals for theFVL mutation from India is required to resolve the issue ofwhether the mutation exists due to a founder effect or as aresult of an independent spontaneous mutation.
Departments of Haematology and G U R J E E WA N G A R E WA L
*Hepatology, R E E N A DA S
Education and Research, YO G E S H C H AW L A *Chandigarh-160 012, India R. K. D H I M A N *
REFERENCES
Cos, M.J., Rees, D.C., Martinson, J.J. & Clegg, J.B. (1996) Evidence fora single origin of factor V Leiden. British Journal of Haematology,92, 1022–1025.
Das, R., Garewal, G., Chawla, Y. & Dhiman, R.K.. (1998) Prevalenceof the factor V Leiden mutation in portal and hepatic veinthrombosis. Gut, 41, 147.
Garewal, G., Das, R. & Trehan, U. (1997) Factor V Leiden: prevalencein the indigenous population and cases of thrombosis in northIndia. British Journal of Haematology, 97, 940.
Leebeek, F.W.G., Lameris, J.S., van Buuren, H.R., Gomez, E.,Madretsma, S. & Sonneveld, P. (1998) Budd-Chiari syndrome,portal vein and mesenteric vein thrombosis in a patienthomozygous for factor V Leiden mutation treated by TIPS andthrombolysis. British Journal of Haematology, 102, 929–931.
Mahmoud, A.E.A., Elias, E., Beauchamp, N. & Wilde, J.T. (1997)Prevalence of the factor V Leiden mutation in hepatic and portalvein thrombosis. Gut, 40, 798–800.
Mohanty, D., Shetty, S., Narayana, T.S. & Abraham, P. (1998) FactorV Leiden mutation and Budd-Chiari syndrome. Blood, 92, 1838–1839.
Keywords: factor V Leiden, Budd-Chiari syndrome.
THE COMMON HAEMOCHROMATOSIS MUTATION DOES NOT INCREASE THE RISK OF THROMBOSISIN PATIENTS WITH FACTOR V LEIDEN
A recent report suggested an association between hetero-zygosity for the common hereditary haemochromatosismutation in the Hfe gene (C282Y) and the factor V Leidenmutation in patients with thrombosis (Xie et al, 1998). Wehave failed to find such an association in a similar study of aU.K. thrombophilic cohort.
Seventy-five unrelated subjects, all of whom were hetero-zygous for factor V Leiden and had a personal history of
venous thrombosis, and 120 unrelated control subjects, 75of whom were age and sex matched to the patients, werestudied. Two control subjects were heterozygous for thefactor V Leiden allele. DNA samples from all subjects wereanalysed for the presence of the G to A transition atnucleotide 845 of the Hfe gene that results in the C282Ysubstitution as previously described (Jouanolle et al, 1996).The frequency of C282Y carriership (defined as either
842 Correspondence
q 1999 Blackwell Science Ltd, British Journal of Haematology 105: 839–850

heterozygosity or homozygosity for the mutation) was 20%(allele frequency 0·11, 95% CI 0·06–0·16) among thepatients compared to 14·2% (allele frequency 0·08, 95% CI0·05–0·11) in the control group, but this difference was notstatistically significant (Table I).
Our results failed to show an association between factor VLeiden and the C282Y mutation and contrast with those ofXie et al (1998). This may reflect the different approachesused in the two studies to derive the frequency of C282Ycarriership in the general population. Although our studyselected control subjects from the same ethnic and geo-graphic background as the patients, Xie et al (1998) basedtheir approximate 6% prevalence in the Canadian popula-tion on the frequencies previously obtained in two controlgroups composed of Caucasian subjects of either Breton(carrier frequency 5·8%) or undisclosed (carrier frequency6·4%) origin (Jouanolle et al, 1996; Feder et al, 1996). Theprevalence of the C282Y mutation varies widely betweenpopulations. Thus, although the mutation is apparentlyabsent from African, Asian and Australasian populations(Merryweather-Clarke et al, 1997), two studies in the U.K.and France found the frequency of C282Y carriership in thenormal population to be 17% and 17·5% respectively (Williset al, 1997; Jezequel et al, 1998). Given these differences ingeographic distribution of the C282Y mutation, we believethe approach adopted by Xie et al (1998) to approximatethe prevalence of the C282Y mutation in their general
population is inappropriate and that it is of criticalimportance when performing studies such as these to use acontrol population from the same geographic and ethnicbackground as the patients.
Division of Molecular S A N JAY B A N Y P E R S A D
and Genetic Medicine, M A RT I NA E. DA LY
University of Sheffield, M I C H A E L M A K R I S
Royal Hallamshire Hospital,Sheffield
REFERENCES
Feder, J.N., Gnirke, A., Thomas, W., Tsuchihashi, Z., Ruddy, D.A.,Basava, A., Dormishian, F., Domingo, R., Jr, Ellis, M.C., Fullan, A.,Hinton, L.M., Jones, N.L., Kimmel, B.E., Kronmal, G.S., Lauer, P.,Lee, V.K., Loeb, D.B., Mapa, F.A., McClellan, E., Myer, N.D., Mintier,G.A., Moeller, N., Moore, T., Morikang, E., Prass, C.E., Quintana,L., Starnes, S.M., Schatzman, R.C., Brunke, K.J., Drayna, D.T.,Risch, N., Bacon, B.R. & Wolff, R.K. (1996) A novel MHC class I-like gene is mutated in patients with hereditary haemochromatosis.Nature Genetics, 13, 399–408.
Jezequel, P., Bargain, M., Lellouche, F., Geffroy, F. & Dorval, I. (1998)Allele frequencies of hereditary haemochromatosis gene mutationsin a local population of west Brittany. Human Genetics, 102, 332–333.
Jouanolle, A.M., Gandon, G., Jezequel, P., Blayau, M., Campion, M.L.,Mosser, J., Fergelot, P., Chauvel, B., Bouric, P., Carn, G., Andrieux,N., Gicquel, I., Le Gall,, Y.-V. & David, V. (1996) Haemochromatosisand HLA-H. (Letter). Nature Genetics, 14, 251–252.
Merryweather-Clarke, A.T., Pointon, J.J., Shearman, J.D. & Robson,K.J.H. (1997) Global prevalence of putative haemochromatosismutations. Journal of Medical Genetics, 34, 275–278.
Willis, G., Jennings, B.A., Goodman, E., Fellows, I.W. & Wimperis, J.Z.(1997) A high prevalence of HLA-H 845A mutations inhemochromatosis patients and the normal population in easternEngland. Blood Cells, Molecules and Diseases, 23, 288–291.
Xie, Y.-G., Lillicrap, D.P. & Taylor, S.A.M. (1998) An associationbetween the common hereditary hemochromatosis mutation andthe factor V Leiden allele in a population with thrombosis. (Letter).Blood, 92, 1461–1462.
Keywords: factor V Leiden, haemochromatosis mutation,thrombosis.
SPLENIC IRRADIATION AS MANAGEMENT OF ITP
The management of haematological diseases in Jehovah’switnesses is usually complicated. We recently cared for apatient with severe chronic idiopathic thrombocytopenicpurpura (ITP) in whom splenectomy was deemed necessaryto control his disease (Okerbloom et al, 1996). Based on twoprevious articles (Calverley et al, 1992; Caulier et al, 1995)reporting good results with splenic irradiation in patientseither old or with contraindications for surgery, we decidedto use radiation therapy as a means of preparing a riskycandidate for a splenectomy.
A 23-year-old man, a Jehovah’s witness, was admitted inFebruary 1998 with a relapse of chronic ITP. The patient hadthe first episode at age 12 and it did not recur until
November 1997, when he developed purpura, petechiaeand mucusal bleeding with a platelet count of 3 × 109/l. Hewas placed on steroids which produced no rise in theplatelet count. A week later a pulse of intravenous globulin(IVIgG) was given with an excellent response lasting 5weeks, but falling precipitously to 1 × 109/l with recurrenceof the bleeding diathesis. This prompted the current crisis,when he was treated with prednisone 120 mg and a 5 dcourse of IVIgG (see Fig 1, week 11), the latter beingrepeated 3 weeks later and followed by a 4 d course ofdexamethasone 40 mg. Because the patients platelet counthad been 10 × 109/l for 4 weeks, with the maximal responseafter 6 weeks of full therapy of 18 × 109/l, and as minor
843Correspondence
q 1999 Blackwell Science Ltd, British Journal of Haematology 105: 839–850
Table I. Hfe G845A genotypes in thrombophilic patients with factorV Leiden and control subjects.
Hfe G845A genotype
GG (%) AG (%) AA (%) Total
Cases 60 (80.0) 14 (18.7) 1 (1.3) 75Controls 103 (85.8) 15 (12.5) 2 (1.7) 120
P ¼ NS.

bleeding diathesis still persisted, we felt splenectomy wasindicated.
Surgery was considered too risky for someone refusingblood component replacement and taking the reportedexperiences on patients with unacceptable surgical risksinto account, splenic irradiation was carried out. A totaldose of 15 Gy was administered over 5 consecutive days(300 cGy/d via two, anterior and posterior opposite fields).One week later the platelet count was 110 × 109/l andsplenectomy was uneventfully carried out after anotherweek. Three weeks later the platelet count had further risento 420 × 109/l and has remained stable around this levelwithout any other treatment, for the ensuing 10 months.
Splenic radiation has been used as an alternative tosplenectomy in patients with corticosteroid-resistant immunethrombocytopenia and contraindications to surgery. In thecombined series (Calverley et al, 1992; Caulier et al, 1995),9/21 patients (47%) had good early responses with a rise inthe platelet count >50 × 109/l, which can be considered as arelatively safe threshold for this type of surgical intervention.Most responses lasted for >6 months.
Low-dose splenic irradiation has not been associated withacute or long-term side-effects, since the radiation toleranceof the kidney and colon are well above the doses used, buta proportion of patients in whom splenectomy wassubsequently required had varying degrees of adhesion
formation between the spleen and the surrounding tissues atlaparotomy (Calverly et al, 1992).
The radiation dose has varied widely. Calverley et al (1992)predominantly used a 600 cGy total dose, in six doses over 3weeks without renal shielding, whereas Caulier et al (1995)used 1500 cGy in 5 weeks (2-weekly 150 cGy doses),shielding the left kidney but leaving 20–25% of the splenicvolume undertreated.
It is worth noting the speed of the platelet response: in ourpatient, 7 d after the start of radiotherapy the platelet counthad increased from 18 to 110 × 109/l. Likewise, responseswere observed as early as 4 weeks from the start ofradiotherapy (Calverley et al, 1992). It is also worthmentioning that using radiation as an immediate preoperativetreatment, one should avoid adhesion formation between thespleen and the surrounding tissues found when splenectomyis performed later (in 3/6; Calverley et al, 1992).
In high-risk situations such as the one we report, a shortcourse of splenic radiation can rapidly increase the plateletfound to safe levels, and thus reduce the risks associated withsplenectomy.
Haematology and Radiotherapy Services, M. C A L L I S
Hospital Vall d’Hebron, C. PA L A C I O S
Barcelona, Spain A. L O P E Z
J. G I R A LT
A. J U L I A
REFERENCES
Calverly, D.C., Jones, G.W., Kelton, J.G. (1992) Splenic radiation forcorticosteroid-resistant immune thrombocytopenia. Annals ofInternal Medicine, 116, 977–981.
Caulier, M.T., Darloy, F., Rose, Ch., Camier, G., Morel, P., Bauters, F. &Fenaux, P. (1995) Splenic irradiation for chronic autoinmunethrombocytopenic purpura in patients with contraindications tosplenectomy. British Journal of Haematology, 91, 208–211.
Okerbloom, J.A., Regan, D.H. & Warrier, I. (1996) Idiophaticthrombocytopenic purpura: a practice guideline developed byexplicit methods for the American Society of Hematology. Blood,88, 3–40.
Keywords: thrombocytopenic purpura, Jehovah’s witness,splenic irradiation, splenectomy.
MUTATION OF THE WT1 GENE IN MYELODYSPLASTIC SYNDROMEAND ACUTE MYELOID LEUKAEMIA POST MYELODYSPLASTIC SYNDROME
Myelodysplastic syndrome (MDS) comprises a heterogenousgroup of haematological disorders that are regarded aspreleukaemic stages. Patients with MDS frequently exhibitprogressive increases in blast counts in bone marrow,showing a transition to acute myeloid leukaemia (AML)post MDS. Cancer is considered to develop during theacquisition of multiple genetic events responsible formalignant transformation. The WT1 gene was cloned as a
candidate of tumour suppressor gene for Wilms tumour (Callet al, 1990). The gene is located at chromosome band 11p13and allelic loss has been reported within this region in Wilmstumour. The gene encodes a zinc finger transcriptional factor,that either activates or represses transcription. The WT1 gene ismutated in about 10% of patients with Wilms tumour.
A mutation of the WT1 gene in leukaemia was firstreported in a Wilms tumour survivor with WAGR syndrome
844 Correspondence
q 1999 Blackwell Science Ltd, British Journal of Haematology 105: 839–850
Fig 1. Clinical course of a patient with refractory ITP.

(Wilms tumour, aniridia, genitourinary abnormalities, andmental retardation) (Pritchard-Jones et al, 1994). The samegroup of investigators also reported that WT1 mutationswere detected in four of 36 patients with sporadic acuteleukaemias. They found that mutations were observed inAML and biphenotypic leukaemia but were rare in acutelymphoblastic leukaemia (King-Underwood & Pritchard-Jones, 1998). Mutations of the WT1 gene may be involvednot only in acute leukaemia but also in MDS.
We analysed mutations of the WT1 gene in 28 patientswith MDS and AML post MDS, using polymerase chainreaction–single-strand conformation polymorphism analy-sis (PCR-SSCP). PCR-SSCP analysis was performed withinexons 7–10, those containing four zinc finger regions of theWT1 gene, since mutations have been reported in these zincfinger regions (Little et al, 1992). Mobility shifts weredetected in one patient with AML post MDS. Sequenceanalysis was subsequently performed, and a missensemutation CGG to TGG, converting Arg to Trp at codon394 was identified. This mutation was identical to one thatwas reported as a germ-line mutation in a patient withDenys-Drash syndrome, a triad of genital malformation,nephrotic syndrome, and Wilms tumour (Coppes et al,1992). Our patient did not have genital malformations or afamily history of Denys-Drash syndrome. To test thepossibility of a germ-line mutation, an autopsy sample ofliver tissue from the same patient was analysed. Normallymigrating bands were observed in the sample, indicating themobility shifts were due to an acquired change. The samemutation was also found in a patient with acute undiffer-entiated leukaemia (King-Underwood & Prichard-Jones,
1998) and may play a role in the development of theseleukaemias.
Department of Haematology, NA O K I M O R I
Tokyo Women’s Medical University, M I C H I KO O K A DA *Tokyo, and T O S H I KO M O T O J I
*Chromosome Laboratory, H I D E A K I M I Z O G U C H I
Shiseikai Dai-ni Hospital,Tokyo, Japan
REFERENCES
Call, K.M., Glaser, T., Ito, C.Y., Buckler, A.J., Pelletier, J., Haber, D.A.,Rose, E.A., Kral, A., Yeger, H., Lewis, W.H., Jones, H. & Housman,D.E. (1990) Isolation and characterization of a zinc fingerpolypeptide gene at the human chromosome 11 Wilms’ tumorlocus. Cell, 60, 509–520.
Coppes, M.J., Liefers, G.J., Higuchi, M., Zinn, A.B., Balfe, J.W. &Williams, B.R.G. (1992) Inherited WT1 mutation in Denys-Drashsyndrome. Cancer Research, 52, 6125–6128.
King-Underwood, L. & Pritchard-Jones, K. (1998) Wilms’ tumor(WT1) gene mutations occur mainly in acute myeloid leukemiaand may confer drug resistance. Blood, 91, 2961–2968.
Little, M.H., Prosser, J., Condie, A.C., Smith, P.J., Heyningen, V.V. &Hastie, N.D. (1992) Zinc finger point mutations within the WT1gene in Wilms tumor patients. Proceedings of the National Academyof Sciences of the United States of America, 89, 4791–4795.
Pritchard-Jones, K., Renshaw, L. & King-Underwood, L. (1994) TheWilms tumour (WT1) gene is mutated in a secondary leukaemiain a WAGR patient. Human Molecular Genetics, 3, 1633–1637.
Keywords: myelodysplastic syndrome, leukaemia, WT1gene, mutation.
LIPID PREPARATIONS OF AMPHOTERICIN FOR THE TREATMENT OF FUNGAL INFECTIONS
Two recent papers on treatment of fungal infectionspublished in the British Journal of Haematology, one reviewingantifungal therapy in immunocompromised patients(Richardson & Kokki, 1998) and the other retrospectivelycomparing amphotericin B lipid complex (Abelcet, ABLC)with liposomal amphotericin (AmBisome) in haematologicalmalignancies (Clark et al, 1998), deserve detailed comments.Significant lacunae in the data provided and incompletediscussion in both papers make AmBisome appear to be asuperior product in the absence of any persuasive data tothat effect.
Richardson & Kokki (1998)This review article contained some sweeping statements onAmBisome which were not substantiated with supportingliterature and omitted important information aboutAbelcet.
The licensed dose of AmBisome for the treatment ofconfirmed fungal infections in the U.K. as well as the U.S.A. is3–5 mg/kg according to the package inserts. The three ‘key’studies cited by the authors in support of AmBisome(Ringden et al, 1991; Chopra et al, 1992; Mills et al,
1994), two of which actually overlap (all the patientsincluded in Chopra et al (1992) were also included in Millset al (1994)), used AmBisome at doses of 3 mg/kg.
The evidence supporting the use of AniBisome at doses<3 mg/kg in invasive aspergillosis is very limited. Richardson& Kokki (1998) quoted a recently published EORTC study(Ellis et al, 1998) to support their conclusion that 1 and4 mg/kg AmBisome were equally effective in the therapy ofaspergillosis. In the EORTC study, out of 87 evaluable patients,only 20 had microbiologically confirmed aspergillosis. Threeof the eight patients receiving 1 mg/kg AmBisome and 7/12patients receiving 4 mg/kg AmBisome responded. Results inthese small numbers of patients cannot be interpreted asevidence showing equal efficacy for the two doses ofAmBisome. Therefore Richardson & Kokki’s recommendationof 1–3 mg/kg of AmBisome in invasive aspergillosis had nofactual basis and must be considered somewhat irresponsibleconsidering the fact that inadequate antifungal therapyimpairs the chances of recovery from a potentially fatalinvasive fungal infection. It may be cheaper to use 1–2 mg/kg AmBisome initially (cf. the significantly higher cost of3–5 mg/kg AmBisome in comparison with 5 mg/kg Abelcet),
845Correspondence
q 1999 Blackwell Science Ltd, British Journal of Haematology 105: 839–850

perhaps to get a foot through the door, but there is noevidence that this is in the patient’s best interest.
The authors claim that AmBisome has immunomodulat-ing action which enhances effector cell function againstfungal cells but quote no data to support this statement.They also went on to say that studies on AmBisomelocalization at infection sites and its local action are ‘wellaccepted’ without providing any citations, again leaving anincorrect impression on uncritical readers that AmBisomehas a mechanism of action that is superior to the other lipid-based amphotericin preparations.
The authors did not quote the only prospective random-ized study which has compared any lipid preparation ofamphotericin at all (Abelcet) with conventional ampho-tericin B in patients with a proven fungal infection(candidiasis). In this study 5 mg/kg Abelcet was as effectiveas 0·6–1 mg/kg conventional amphotericin (Anaissie et al,1995) and significantly less nephrotoxic (Luke & Boyle,1998). Additionally, in the small number of patients infectedwith multiple Candida species the response rate to Abelcetwas 50% compared with 0% for conventional amphotericin(P ¼ 0·05; Fisher’s exact test).
The authors mentioned ‘anecdotal’ and ‘limited’ informa-tion on Abelcet, but did not quote the study of Wingard(1997) which provided details of the efficacy of Abelcet inpresumed and confirmed fungal infections in 95 bonemarrow transplant recipients. Another report showing theefficacy of lower doses of Abelcet in confirmed fungalinfections was also not cited (Walsh et al, 1997) where2·5 mg/kg Abelcet was administered daily for 6 weeks to sixpaediatric cancer patients with hepatosplenic candidiasisand response was seen in all five evaluable patients.
A large multi-centre series containing 556 patients(Walsh et al, 1998), including the patients reported byWingard (1997), has provided more data on the efficacy ofAbelcet in fungal infections: among the 291 mycologicallyconfirmed cases evaluable for therapeutic response there wasa complete or partial response to ABLC in 57%, including42% of 130 aspergillosis cases, 67% of 42 disseminatedcandidiasis cases, 71% of 24 zygomycosis cases, and 82% of11 patients with fusariosis.
Richardson & Kokki (1998) also reported tissue penetra-tion data (higher lung concentrations of amphotericin withAbelcet) in one Abelcet-treated patient but did not providethe reference (Janoff et al, 1993) which would have enabledthe readers to judge the issue for themselves. There are alsoconsistent experimental data suggesting selective pulmonaryconcentration of amphotericin with Abelcet (Olsen et al,1991; Wasan et al, 1990) because of its larger molecular size(Mehta, 1997; Hunt et al, 1979). This is in contrast topoor pulmonary concentrations achieved with AmBisome(Ringden et al, 1991; Heinemann et al, 1998), which, as hasbeen speculated by Ringden et al (1991), may be responsiblefor poor mycologic response in AmBisome-treated patientswith pulmonary aspergillosis.
Clark et al (1998)The data provided in this study did not support the authors’primary contention that AmBisome at the median dose of
1·9 mg/kg and Abelcet at the median dose of 4·8 mg/kgresulted in a clinically similar outcome because of smallpatient numbers as well as lack of some importantinformation.
Although the absolute neutrophil counts (ANC) at thecommencement of therapy in the two groups were notsignificantly different, it was immediately obvious that theproportion of neutropenic (ANC <0·5 × 109/l) patients inthe Abelcet group (median ANC 0·3) was greater than thatin the AmBisome group (median ANC 0·6). This disparitywas likely to be even greater amongst patients with proveninfection where the median ANC in the Abelcet group was0·1 × 109/l compared with 2·1 × 109/l in the AmBisomegroup. Similarly, amongst patients who did not respond themedian ANC at the time of cessation of therapy was0·3 × 109/l in the Abelcet group (failure in the setting ofneutropenia) compared with 1·5 × 109/l in the AmBisomegroup (failure despite lack of neutropenia).
Lack of neutropenia at the commencement of therapy andrecovery from neutropenia facilitates a successful outcome:in our study (Mehta et al, 1997), 17/20 Abelcet coursesadministered with ANC >0·5 × 109/l resulted in a responsecompared with 18/33 courses with ANC <0·5 × 109/l(P ¼ 0·07, Fisher’s exact test). The authors must providenumbers which allow comparison of the proportion ofneutropenic patients in each group. It is possible thatAmBisome was apparently efficacious only because of higherneutrophil counts or that Abelcet was equally effectivedespite a greater proportion of neutropenic patients.
Although the median AmBisome dose used was modest(1·9 mg/kg for suspected infections and 2·1 mg/kg forproven infections), the highest AmBisome dose used was4 mg/kg for each indication. The authors should haveprovided details of drug doses received by responders andnon-responders, overall as well as separately for suspectedand proven infections. If the AmBisome doses received byresponding patients were generally higher than the medianof the whole group, it would again undermine the maincontention of the paper that low-dose AmBisome isequivalent to full-dose Abelcet.
The paper mentioned, in four separate places, thatthere were ‘non-significantly increased levels of immuno-suppression’ in AmBisome-treated patients. Details ofimmunosuppression should have been provided because,although corticosteroid, Campath and antilymphocyteglobulin administration would certainly interfere with thetreatment of fungal infections, I am not sure that thesame holds true for cyclosporine as a single agent or fordonor leucocyte infusions. If non-significant differences wereto be highlighted, it should have been noted that 62% ofAbelcet-treated proven infections were treated successfullycompared with only 42% of AmBisome-treated proveninfections.
Although infusion-related toxicity was significantlyhigher with Abelcet, discontinuation of therapy due toadverse events was necessary in only one of 36 patientscompared with none of 32 AmBisome-treated patients(P ¼ 0·5; Fisher’s exact test). This was in keeping withdiscontinuation rates observed by others (Mehta et al, 1997;
846 Correspondence
q 1999 Blackwell Science Ltd, British Journal of Haematology 105: 839–850

Walsh et al, 1998), and was in marked contrast to a recentanecdotal report in which Abelcet apparently had to bediscontinued in 74% of 17 patients due to unusual side-effects (Ringden et al, 1998).
Abelcet has generally been used at the licensed dose of5 mg/kg. The dosing approach to AmBisome has beenlaissez-faire: there is often a tendency to use the drug at dosesthat are much lower than the licensed doses (doses for whichthere is limited or no supporting data in the literature)because of its prohibitive cost (Stewart et al, 1995). The doseis then increased gradually when there is failure to respond.Failure of therapy under these circumstances is thenattributed to the usual lack of success in treating fungalinfections rather than to any shortcomings in drug dosing.There are data to suggest that lower doses of Abelcet, onthe limited occasions that the drug has been reported to beused as such doses, were also effective (Walsh et al, 1997;vide supra).
Thus, in contrast to the impression the two papers appearto leave, there are no data to suggest that AmBisome issuperior to Abelcet on a mg-equivalent basis. There aretheoretical tissue distribution advantages in using Abelcet,which is significantly less expensive than AmBisome.
Myeloma and Transplantation JAY E S H M E H TA
Research Center,University of Arkansas for
Medical Sciences,4301 West Markham, Slot 508,Little Rock, AR 72205,U.S.A.
REFERENCES
Anaissie, E.J., White, M., Uzun, 0., Singer, 0., Bodey, G.P., Azarnia, N.,Lopez-Berestein, G. & Matzke, D. (1995) Amphotericin B lipidcomplex (ABLC) vs amphotericin B (AMB) for treatment ofhematogenous and invasive candidiasis: a prospective, ran-domized, multicenter trial. Proceedings of the 35th InterscienceConference on Antimicrobial Agents and Chemotherapy, SanFrancisco, p. 330 (abstract LM21).
Chopra, R., Fielding, A. & Goldstone, A.H. (1992) Successfultreatment of fungal infections in neutropenic patients withliposomal amphotericin (AmBisome): a report on 40 cases froma single centre. Leukemia and Lymphoma, 7, (Suppl.), 73–77.
Clark, A.D., McKendrick, S., Tansey, R.L., Franklin, I.M. & Chopra, R.(1998) A comparative analysis of lipid-complexed and liposomalamphotericin B preparations in haematological oncology. BritishJournal of Haematology, 103, 198–204.
Ellis, M., Spence, D., de Pauw, B., Meunier, E., Marinus, A.,Collette, L., Sylvester, R., Meis, L., Boogaerts, M., Selleslag, D.,Krcmery, V., von Sinner, W., MacDonald, R., Doven, C. &Vandercam, B. (1998) An EORTC international multicenterrandomized trial (EORTC number 19923) comparing two dosagesof liposomal amphotericin B for treatment of invasive aspergillosis.Clinical Infectious Diseases, 27, 1406–1412.
Heinemann, V., Sturm, A., Jehn, U., Wachholz, K., Holler, E. &Kolb, H.J. (1998) Tissue concentration and organ distribution ofliposomal amphotericin (AmBisome). Bone Marrow Transplanta-tion, 21, (Suppl.1), S150.
Hunt, C.A., Rustum, Y.M., Mayhew, E. & Papahadjopoulos, D. (1979)Retention of cytosine arabinoside in mouse lung followingintravenous administration in liposomes of different size. DrugMetabolism and Disposal, 7, 124–128.
Janoff, A.S., Perkins, W.R., Saleton, S.L. & Swenson, C.E. (1993)Amphotericin B lipid complex (ABLC): a molecular rationale forthe attenuation of amphotericin B related toxicities. Journal ofLiposome Research, 3, 451–472.
Luke, R.G. & Boyle, J.A. (1998) Renal effects of amphotericin B lipidcomplex. American Journal of Kidney Diseases, 31, 780–785.
Mehta, J. (1997) Do variations in molecular structure affect theclinical efficacy and safety of lipid-based amphotericin B prepara-tions? Leukemia Research, 21, 183–188.
Mehta, J., Kelsey, S., Chu, R., Powles, R., Hazel, D., Riley, U., Evans, C.,Newland, A., Treleaven, J. & Singhal, S. (1997) Amphotericin Blipid complex (ABLC) for the treatment of confirmed or presumedfungal infections in immunocompromised patients with hemato-logic malignancies. Bone Marrow Transplantation, 20, 39–43.
Mills, W., Chopra, R., Linch, D.C. & Goldstone, A.H. (1994)Liposomal amphotericin B in the treatment of fungal infectionsin neutropenic patients: a single-centre experience of 133 episodesin 116 patients. British Journal of Haematology, 86, 754–760.
Olsen, S.J., Swerdel, M.R., Blue, B., Clark, J.M. & Bonner, D.P. (1991)Tissue distribution of amphotericin B lipid complex in laboratoryanimals. Journal of Pharmacy and Pharmacology, 43, 831–835.
Richardson, M.D. & Kokki, M.H. (1998) Antifungal therapy in ‘bonemarrow failure.’ British Journal of Haematology, 100, 619–628.
Ringden, O., Jønsson, V., Hansen, M., Tollemar, J. & Jacobsen, N.(1998) Severe and common side effects of amphotericin B lipidcomplex (Abelcet). Bone Marrow Transplantation, 22, 733–734.
Ringden, O., Meunier, E., Tollemar, L., Ricci, R., Tura, S., Kuse, E.,Viviani, M.A., Gorin, N.C., Klastersky, J., Fenaux, R., Prentice, H.G.& Ksionski, G. (1991) Efficacy of amphotericin B encapsulated inliposomes (AmBisome) in the treatment of invasive fungalinfections in immunocompromised patients. Journal of Antimicro-bial Chemotherapy, 28, (Suppl. B), 73–82.
Stewart, A., Powles, R., Hewetson, M., Antrum, J., Richardson, C. &Mehta, J. (1995) Costs of antifungal prophylaxis after bonemarrow transplantation: a model comparing oral fluconazole,liposomal amphotericin and oral polyenes as prophylaxis againstoropharyngeal infections. PharmacoEconomics, 8, 350–361.
Walsh, T.J., Hiemenz, J.W., Seibel, N.L., Perfect, J.R., Horwith, G.,Lee, L., Silber, L.L., DiNubile, M.J., Reboli, A., Bow, E., Lister, J. &Anaissie, E.J. (1998) Amphotericin B lipid complex for invasivefungal infections: analysis of safety and efficacy in 556 cases.Clinical Infectious Diseases, 26, 1383–1396.
Walsh, T.J., Whitcomb, P., Piscitelli, S., Figg, W.D., Hill, S.,Chanock, S.J., Jarosinski, R., Gupta, R. & Pizzo, P.A. (1997)Safety, tolerance, and pharmacokinetics of amphotericin B lipidcomplex in children with hepatosplenic candidiasis. AntimicrobialAgents and Chemotherapy, 41, 1944–1948.
Wasan, K.M., Vadiei, K., Lopez-Berestein, G. & Luke, D.R. (1990)Pharmacokinetics, tissue distribution, and toxicity of free andliposomal amphotericin B in diabetic rats. Journal of InfectiousDiseases, 161, 562–566.
Wingard, J.R. (1997) Efficacy of amphotericin B lipid complexinjection (ABLC) in bone marrow transplant recipients with life-threatening systemic mycoses. Bone Marrow Transplantation, 19,343–347.
The comments by Dr Mehta concerning our review includesome erroneous information and he appears to havemisinterpreted, misquoted or invented parts of our review
847Correspondence
q 1999 Blackwell Science Ltd, British Journal of Haematology 105: 839–850

of the treatment of fungal infections, compiled in 1997 andpublished in March 1998 (Richardson & Kokki, 1998). Wewelcome the opportunity to reply. His thesis appears to bethat cost considerations should encourage the use of Abelceton the grounds that there are no data to suggest lower dosesof AmBisome, which would be cost-comparable, are aseffective as Abelcet in the treatment of confirmed fungalinfections. We do not agree with this.
The first and most obvious error in Dr Mehta’s letter is hisclaim that the licensed dose for AmBisome in the U.K. is3–5 mg/kg. The data sheet actually states: ‘Therapy forsystemic and/or deep mycoses is usually instituted at a dailydose of 1·0 mg/kg of body weight, and increased stepwise to3·0 mg/kg, as required.’ This recommendation was based onthe key studies to which Dr Mehta refers. In Mills et al (1994)the median dose of AmBisome administered was 1684 mgfor a median of 12 d. This equates to almost exactly 2 mg/kg/d for an average 70 kg patient. Ringden et al (1991) quoted amedian daily dose for proven and presumed invasive mycosesof 2·4 mg/kg in their series. The 3 mg/kg/d dose that DrMehta suggests for these studies is therefore incorrect.Ringden et al (1991) specifically included in their Materialsand Methods section the statement: ‘Dosing was begun at0·5 or 1·0 mg/kg, and the dose was then increased in a step-wise fashion.’
Dr Mehta then proceeds to mention the work of Ellis et al(1998) and suggests that the response rate of patients withproven invasive aspergillosis (IA) to AmBisome at 4 mg/kg/dappeared to be better than 1 mg/kg/d. We did not quote thatpaper because it was published after our review, but wewould suggest that the results are very equivocal. On the onehand, the overall clinical response in both probable andproven IA was encouraging at both dose levels: 26/41 (64%)in the 1 mg/kg arm and 22/46 (48%) in the 4 mg/kg arm.The radiological response rates were very similar. Theresponse rates in the 20 patients with proven IA were alsoencouraging, at 38% in the 1 mg/kg cohort and 58% in the4 mg/kg cohort. On the other hand, there was a trendtowards a better outcome among proven cases of IA in thehigher dose group, compounded by generally a worseprognosis among the patients in that dose group. Onemight therefore conclude that 1 mg/kg of AmBisome is aneffective dose in IA but 4 mg/kg could be better, though theevidence was not definitive.
The response rates in Ellis et al (1998) are in line withother reported efficacy rates for AmBisome and arecomparable with the 55/130 responses (42%) reported forAbelcet at 5 mg/kg by Walsh et al (1998) in their study. Aswith Ellis et al (1998), we did not cover the papers fromWalsh et al (1997, 1998) because they had not beenpublished at the time of our review was prepared. Dr Mehtamoves on to make the alarming accusation that our‘recommendation of 1–3 mg/kg of AmBisome in invasiveaspergillosis has no factual basis and must be consideredsomewhat irresponsible.’ This we refute totally. What weactually said was: ‘It is usual to begin treatment withAmBisome with a dose of 1·0–3·0 mg/kg, or even higher’,which is a statement of fact and in no way irresponsible.Again, we have been grossly misquoted. What Dr Mehta has
highlighted is that there is some considerable debate aboutthe most appropriate dosing of AmBisome, whilst there ismuch less known about Abelcet. The reason is simple. Thereare very little reliable data regarding Abelcet at doses below5 mg/kg and the tolerance of the agent above 5 mg/kg isextremely poor. This gives clinicians little option.
AmBisome, however, is very different. As indicated,there exists good clinical data, corroborated by preclinicaldata, that doses from 1 mg/kg/d are effective in thetreatment of mycoses. Several reports have been publishedof the use of AmBisome up to 15 mg/kg/d. This tends tosuggest that the available dose range for AmBisome is verywide indeed and has led to different authors suggestingdifferent options, based on their own experience and guidancefrom the literature. Far from being a criticism of AmBisome,this can only be seen as one of the product’s strengths.
Dr Mehta is incorrect to say that the study of Anaissie et al(1995), which has not been published in a peer-reviewedjournal and therefore not easily reviewed in detail, is the onlyprospective randomized study to have compared any lipidformulation of amphotericin with the conventional drug inpatients with a proven fungal infection. A recent randomizedcomparison of AmBisome at 5 mg/kg/d with conventionalamphotericin B at 1 mg/kg/d in the treatment of IA(Leenders et al, 1998) suggested that AmBisome wassignificantly better in terms of response at day 14 andoverall mortality, adjusted for malignancy status. Even atthis high dose, the safety profile of AmBisome, in terms ofnephrotoxicity, was superior to that of the conventionaldrug. We thank Dr Mehta for bringing the Wingard (1997)report to our attention, which certainly adds to ourunderstanding of Abelcet and its use.
Dr Mehta’s acceptance and understanding of the tissuedistribution of AmBisome and Abelcet is also of concern. Thepathogenesis of invasive fungal infection and pharmaco-kinetics of lipid formulations of amphotericin B in experi-mental models are very different from that seen in humans.Moreover, an independent review of the Ringden et al (1991)paper, concerning tissue levels in three patients, not one,makes a very definite statement: ‘Substantial amounts ofdrug [AmBisome] were recovered in kidney and lung tissue’(Coukell & Brogden, 1998). These levels were far high thanthe minimum inhibitory concentration against all fungalpathogens.
We thank Dr Mehta for giving us the opportunityto update and clarify his understanding of our review.It is hoped that our appraisal of the most recentliterature outlined here in the context of his letterreinforce the recommendations that we made in the originalreview.
Department of Bacteriology M A L C O L M D. R I C H A R D S O N
and Immunology,Haartman Institute,University of Helsinki
Department of Infectious M A A R I T H. KO K K I
Disease Epidemiology,National Public Health Institute,Helsinki
848 Correspondence
q 1999 Blackwell Science Ltd, British Journal of Haematology 105: 839–850

REFERENCES
Annaissie, E.J., White, M., Uzun, O., Singer, O., Bodey, G.P.,Azarnia, N., Lopez-Berestein, G. & Matzke, D. (1995) Ampho-tericin B lipid complex (ABLC) vs amphotericin B (AMB) fortreatment of hematogenous and invasive candidiasis: a pro-spective, randomized, multicenter trial. Proceedings of the 35thInterscience Conference on Antimicrobial Agents and Chemotherapy,San Francisco, p. 330 (abstract LM21).
Coukell, A.J. & Brogden, R.N. (1998) Liposomal amphotericin B:therapeutic use in the management of fungal infections andvisceral leishmaniasis. Drugs, 55, 585–612.
Ellis, M., Spence, D., de Pauw, B., Meunier, F., Marinus, A., Collette, L.,Sylvester, R., Meis, J., Boogaerts, M., Selleslag, D., Krcmery, V., vonSinner, W., MacDonald, P., Doven, C. & Vandercam, B. (1998) AnEORTC international multicenter randomized trial (EORTCnumber 19923) comparing two dosages of liposomal ampho-tericin B for treatment of invasive aspergillosis. Clinical InfectiousDiseases, 27, 1406–1412.
Leenders, A.C.A.P., Daenen, S., Jansen, R.L.H., Hop, W.C.J.,Lowenberg, B., Wiljermans, P.W., Cornelissen, J., Herbrecht, R.,van der Lelie, H., Hoogsteden, H.C., Verbrugh, H.A. & de Marie, S.(1998) Liposomal amphotericin B compared with amphotericin Bdeoxycholate in the treatment of documented and suspectedneutropenia-associated invasive fungal infections. British Journalof Haematology, 103, 205–212.
Mills, W., Chopra, R., Linch, D.C. & Goldstone, A.H. (1994)Liposomal amphotericin B in the treatment of fungal infectionsin neutropenic patients: a single-centre experience of 133 episodesin 116 patients. British Journal of Haematology, 86, 754–759.
Richardson, M.D. & Kokki, M.H. (1998) Antifungal therapy in ‘bonemarrow failure’. British Journal of Haematology, 100, 619–628.
Ringden, O., Meunier, F., Tollemar, J., Ricci, P., Tura, S., Kuse, E.,Viviani, M.A., Gorin, N.C., Klastersky, J., Fenaux, P., Prentice, H.G.& Ksionski, G. (1991) Efficacy of amphotericin B encapsulated inliposomes (AmBisome) in the treatment of invasive fungalinfections in immunocompromised patients. Journal of Antimicro-bial Chemotherapy, 28, (Suppl. B), 73–82.
Walsh, T.J., Hiemenz, J.W., Seibel, N.L., Perfect, J.R., Horwith, G.,Lee, L., Silber, J.L., DiNubile, M.J., Reboli, A., Bow, E., Lister, J. &Anaissie, E.J. (1998) Amphotericin B lipid complex for invasivefungal infections: analysis of safety and efficacy in 556 cases.Clinical Infectious Diseases, 26, 1383–1396.
Walsh, T.J., Whitcomb, P., Pitcitelli, S., Figg, W.D., Hill, S.,Chanock, S.J., Jarsinski, P., Gupta, R. & Pizzo, P.A. (1997) Safety,tolerance, and pharmacokinetics of amphotericin B lipid complexin children with hepatosplenic candidiasis. Antimicrobial Agentsand Chemotherapy, 41, 1944–1948.
Wingard, J.R. (1997) Efficacy of amphotericin B lipid complexinjection (ABLC) in bone marrow transplant recipients with life-threatening systemic mycoses. Bone Marrow Transplantation, 19,343–347.
We would like to respond to Dr Mehta’s comments. Our paper(Clark et al, 1998) was the first comparison of liposomal andlipid complexed amphotericin B preparations in haemato-logical oncology. We did not find a statistically significantdifference in clinical outcome in patients treated with amedian dose of 1·9 mg/kg/d of AmBisome when comparedwith Abelcet at a median dose of 4–8 mg/kg/d in the contextof BMT/PBSCT or high-dose chemotherapy. We accept thatabsence of evidence is not evidence of absence of effect insmall studies, as discussed by Altman & Bland (1995). Wemade comments on dosages and outcomes overall which
were broadly in line with trials comparing either preparationto conventional amphotericin B (Hiemenz & Walsh, 1996).At the time we pointed out that subgroup analysis was notpossible and here again would caution against extrapolatingoverall figures to subgroups with very small numbers ofpatients such as those with proven infections. We agree withDr Mehta that neutropenia is a major predisposing factor forfungal infection and persistence is an adverse prognosticindicator. If there was a statistically significant difference inoverall ANC or the proportion of patients with ANC<0·5 × 109/l it would influence outcome. In our study thedifferences in median values of ANC did not translatethemselves into a statistical difference in neutrophil counts atcommencement or cessation of therapy in any comparativegroup due to the very wide confidence intervals. Thepropositions of patients in each group with ANC<0·5 × 109/l are shown in Table I. There was no statisticaldifference between the proportions of patients who wereneutropenic overall or in any subgroup between patientswho received either drug. Taking proven infection as anexample using Fisher’s exact test P ¼ 0·32, the odds ratio,expressing the likelihood of neutropenia in Abelcet patientscompared to AmBisome patients was 4·0 but the 95%confidence interval was 0·44–36·7. In other words Abelcetpatients may be anywhere from half as likely to 36 times aslikely to be neutropenic. The overall odds ratio was 1·56(0·57, 4·25). In a small study with limited statistical power,trends may be important and warrant analysis in largerstudies, as Dr Mehta has pointed out for ANC. Comments weremade about levels of pharmacological immunosuppression inthe context of the paper in all but one instance occurredjuxtaposed to comments highlighting non-significantdifferences in neutrophil counts, disease status, APACHEscores and predicted mortality.
Drug dosages are shown in Table II. As can be seen, drugdoses were not significantly higher in the respondingpatients treated with either preparation.
Prior to publication of our paper no comparativeinformation existed on efficacy of these lipid-associatedpreparations. We accept that the study was limited by its
849Correspondence
q 1999 Blackwell Science Ltd, British Journal of Haematology 105: 839–850
Table I. The numbers of patients in each group with ANC<0·5 × 109/l at commencement and cessation of therapy. Nostatistical differences were found using chi-square or Fisher’s exacttests. Odds ratios were not informative due to wide confidenceintervals.
AmBisome Abelcet(no. patients (no. patientswith ANC with ANC<0·5 × 109/l) <0·5 × 109/l)
Commence- Cessation Commence- Cessationment ment
Overall 15/31 7/31 19/32 6/32Proven 3/7 2/7 6/8 2/8Responders 9/22 3/22 14/25 2/25Non-responders 6/9 4/9 5/7 4/7

size. Indeed we perceived that possibly the most importantrole of the paper was to stimulate debate and lead to large-scale, prospective, randomized, directly comparative trials withthe statistical power to delineate differences between outcomein patients treated with lipid-associated amphotericin Bpreparations. Ideally a national registry of BMT/PBSCT patientsundergoing treatment with lipid-associated amphotericinpreparations should be established. This would enable alarger analysis to be made of the current experience beinggained with these agents and provide information necessaryto design an appropriate randomized study.
Academic Transfusion Medicine Unit, A N D R E W C L A R K
Department of Medicine, I A N M. F R A N K L I N
University of Glasgow,Royal Infirmary,Glasgow G31 2ER
REFERENCES
Altman, D.G. & Bland, J.M. (1995) Absence of evidence is notevidence of absence. British Medical Journal, 311, 485.
Clark, A.D., McKendrick, S., Tansey, P.J., Franklin, I.M. & Chopra, R.(1998) A comparative analysis of lipid complexed and liposomalamphotericin B preparations in haematological oncology. BritishJournal of Haematology, 103, 198–204.
Hiemenz, J.W. & Walsh, T.J. (1996) Lipid formulations of ampho-tericin B: recent progress and future directions. Clinical InfectiousDiseases, 22, (Suppl. 2), S133–S144.
Keywords: Abelcet, AmBisome, amphotericin B lipid complex,liposomal amphotericin.
850 Correspondence
q 1999 Blackwell Science Ltd, British Journal of Haematology 105: 839–850
Table II. Drug doses received by responders and non-responders.
Abelcet AmBisome
RespondersTotal patients 25 22Total dose (mg), median (range) 4150 (1250–10150) 1250 (450–4900)Days (d), median (range) 14 (4–42) 10 (4–39)Daily dose (mg/kg/d), median (range) 4·8 (1·84–5·76) 1·9 (0·7–2·3)
Non-respondersTotal patients 7 9Total dose (mg), median (range) 6150 (2000–12070) 1000 (200–3350)Days (d), median (range) 20 (7–42) 8 (4–28)Daily dose (mg/kg/d), median (range) 4·81 (2·6–5·3) 2·1 (0·7–4)