LGS Foundation 2016 Conference - Friday Morning
76
-
Upload
lgs-foundation -
Category
Healthcare
-
view
390 -
download
0
Transcript of LGS Foundation 2016 Conference - Friday Morning


Therapies for LGS
Part One
Pharmacological
Angus A Wilfong, MD Baylor College of Medicine
Texas Children’s Hospital
4th International Family & Professional Conference on LGS

Research Funding NINDS
Moody Foundation
Novartis
Acorda
Eisai
Pfizer
UCB
Lundbeck
GW Pharma
Publication Royalties Up-To-Date
Disclosures

Treatment of Epilepsy 2016 Antiepileptic drugs (AEDs) - >30!
Epilepsy surgery
Resective
Ablative
Disconnection
Ketogenic diet
Neurostimulation
Vagus Nerve Stimulation (VNS)
Responsive Neurostimulation (NeuroPace®)
Deep Brain Stimulation (DBS)
Goals of Epilepsy Therapy
Maximize quality of life
Having as few seizures as possible
Having as few adverse effects from
therapy as possible
Minimize the impact of the “epileptic
encephalopathy”
Due to a combination of the underlying cause
for the LGS, the seizure burden, and the drugs

Basic Principles of Epilepsy Therapy
Important considerations in choosing the first or the
next best medication to use:
Efficacy – target most disruptive/dangerous seizure type
Safety and tolerability - ?need for safety monitoring labs
Consider comorbidities – weight, mood, behavior
Formulation – liquid, tablets, chewable tablets, dispersible
tablets, capsules, sprinkle capsules, extended release
tablets/capsules, intravenous solutions
Route – orally, G-tube
Number of times per day
Taste
Cost - insurance coverage, copays

Adverse Effects and Tolerability
Safety AE’s (idiosyncratic) – 1st month
hypersensitivity reactions (rash)
Stevens-Johnson syndrome
Toxic Epidermal Necrolysis (TENS)
liver failure
bone marrow failure (aplastic anemia)
pancreatitis
glaucoma
As a class of medication, FDA considers all AEDs
to have an increased risk for suicidal ideation

Dose-Related AE’s (treatment emergent) Depend upon dose, rate of titration, other drugs on board
sleepy/drowsy/dizzy/double vision (CNS AE’s)
cognitive/behavioral effects
GI effects/weight changes
sleep changes
cosmetic changes
endocrine changes
kidney stones
bone demineralization
ataxia/peripheral neuropathy
Adverse Effects and Tolerability

Basic Principles of Epilepsy Therapy
Use scientifically proven therapies first (“on label” for LGS)
valproic acid
felbamate
topiramate
lamotrigine
rufinamide
clobazam
Attempt to wean off a current AED while adding or shortly
after adding a new AED – try to limit current therapies to
only 2-3 AEDs at a time
Be aware of drug-to-drug interactions between different
AEDs and other therapies – anxiety, stimulants (ADD),
behavior (neuroleptics), antihistamines

Treating LGS is Difficult
There are typically multiple seizure types, and it is
not uncommon for one AED to work for only one
seizure type
Seizures in LGS are much more likely to be
refractory to AEDs than the general epilepsy
population
General epilepsy population – 30-40% intractable
LGS population – 80-90% intractable and typically have
life-long epilepsy
High comorbid rates of intellectual disability and
behavior disorders

Treatment goals for epilepsy
Kwan P, et al. Epilepsia 2009; doi: 10.1111/j.1528-1167.2009.02397.x Gilliam F. Neurology 2002;58:s9-s19. Wheless JW. Neurostimulation Therapy for Epilepsy. In: Wheless JW, Willmore LJ, Brumback RA, eds. Advanced Therapy in Epilepsy. Hamilton, Ontario: BC Decker, Inc. 2008. Faught E, et al. Epilepsia 2009;50(3):501-509.
AED Trial 1 Monotherapy
Treatment Goal
• Seizure freedom
Treatment Goal
• Maximize quality of life
• Optimize Long-term seizure control
• Minimize AED side effects
• Maximize adherence
AED Trial 2 Monotherapy
or Polytherapy
Newly Diagnosed Refractory Epilepsy
Epilepsy Surgery
EEG/video monitoring
VNS Therapy
AEDs (Polytherapy)
Ketogenic Diet

AEDs 2016 1) phenobarbital
• All generic
2) phenytoin Dilantin®/Cerebyx®
3) mysoline Primidone®
4) ethosuximide Zarontin®
5) carbamazepine Tegretol®/Carbatrol®
6) valproate Depakene®/Depakote®/
Depakote-ER®/Depacon®
7) felbamate
• Felbatol®
8) gabapentin
• Neurontin®
9) lamotrigine
• Lamictal®/Lamictal-XR®
10) topiramate
• Topamax®/Trokendi-XR®/
Qudexy-XR®
11) tiagabine
• Gabitril®
12) oxcarbazepine
• Trileptal®/Oxtellar-XR®
13) levetiracetam
• Keppra®/Keppra-XR®/
Spirtam®
14) zonisamide
• Zonegran®
15) pregabalin
• Lyrica®
16) rufinamide
• Banzel®
17) lacosamide
• Vimpat®
18) vigabatrin
• Sabril®
19) clobazam
• Onfi®
21) eslicarbazepine
• Aptiom®
20) ezogabine
• Potiga®
22) perampanel
• Fycompa®
23) brivaracetam • Briviact®

Adjunctive/bridge therapies
clonazepam – Klonopin®
clorazepate – Tranxene®
Rescue therapies – clusters of seizures or
prolonged seizures
clonazepam - Klonopin®
clorazepate – Tranxene®
lorazepam – Ativan®
diazepam - Valium®
rectal diazepam - Diastat®
nasal midazolam – Versed® Note: Diastat® is FDA approved for treatment of cluster seizures only and
intranasal Versed® is not FDA approved to treat clusters of seizures or
prolonged seizures
Adjunctive and Rescue AEDs
clusters
prolonged

phenobarbital, primidone, phenytoin, carbamazepine
Increase cholesterol and triglycerides
Many drug-to-drug interactions due to induction of hepatic
CYP-450 system
Impair bone metabolism leading to osteoporosis – need
supplementation with Vitamin D and Calcium
Impair hormone metabolism – irregular menses
Sodium channel meds tend to be less effective for LGS
phenytoin, carbamazepine, oxcarbazepine, eslicarbazepine
AEDs more likely to aggravate behavior disorders
phenobarbital, levetiracetam, perampanel
AEDs to Avoid if Possible

Valproic Acid (VPA) Depakene®/Depakote®/Depakote-ER®/Depacon®
First broad-spectrum AED to US market 1978 – FDA approved
Formulations (generic and brand name)
Liquid (three times daily)
Capsules (three times daily) and sprinkle capsules (twice daily)
Tablets (twice daily)
Extended release tablets (once daily)
Intravenous solution (three to four times daily)
Generally considered the “gold standard” for treatment of LGS
Safety issues are liver toxicity (idiosyncratic and dose-related),
pancreatitis (idiosyncratic), thrombocytopenia (dose-related)
Generally requires safety monitoring for CBC and liver function
studies

Valproic Acid (VPA) Tolerability issues are weight gain, hair loss, hormonal
changes
Behavior – tends to be well tolerated – mood stabilizer.
Approved by FDA to treat migraine headaches
Able to “load” orally or IV and get started quickly
Can be used for status epilepticus
Drug-to-drug interactions
lamotrigine – VPA impairs lamotrigine metabolism, so must
decrease dose if adding VPA
rufinamide – VPA impairs rufinamide metabolism and levels may
increase
felbamate – impairs VPA metabolism and levels may increase
cannabidiol (CBD) – impairs VPA metabolism and levels may
increase

Felbamate (FBM) Felbatol®
Arrived US market 1993 – FDA approved for LGS
Formulations (generic and brand name)
Liquid (three times daily)
Tablets (three times daily)
Generally considered one of the most potent of all AEDs
Safety issues are liver toxicity (idiosyncratic and dose-related)
and aplastic anemia (idiosyncratic) – Black Box from FDA
Requires very close safety monitoring for CBC and liver function
studies – initially every 1-2 weeks and then monthly for several
months
Adults are at higher risk – youngest death 14 years old
All life-threatening toxicity occurred within first year of therapy

Felbamate (FBM) Tolerability issues are weight loss (may be severe) and
insomnia (may be severe)
Behavior – tends to be an activator and brightens children up
and can lift some of the “encephalopathy”
Able to get started fairly quickly
Drug-to-drug interactions
Many drug interactions as is both an inducer and an
inhibitor in the P450 system
Tends to result in higher serum levels of carbamazepine,
phenytoin, and valproic acid

Lamotrigine (LTG) Lamictal®/Lamictal-XR®
Arrived US market 1994 – FDA approved for LGS
Formulations (generic and brand name)
Tablets (twice daily)
Chewable tablets and orally disintegrating tablets (twice daily)
Extended release tablets (once daily)
Broad spectrum AED with efficacy for most seizure types –
tends to be particularly effective for absence seizures, but may
aggravate myoclonic seizures
Safety issues are allergic hypersensitivity reactions (rash) –
Black Box warning from FDA for Stevens-Johnson syndrome
and Toxic Epidermal Necrolysis
Risk factors include age (children>adults), rate of titration (slower
is safer), starting dose (lower is safer), and VPA (increases risk)

Lamotrigine (LTG) Tolerability issues are dizziness/double vision, insomnia (may
be severe), and rarely aseptic meningitis with headaches
Behavior – tends to be an activator and brightens children up
and can lift some of the “encephalopathy”. Approved by FDA to
treat depression in Bipolar disease
Never able to get started quickly and takes the longest of any
AED to reach therapeutic target dosage
Drug-to-drug interactions
Most import interaction is with valproic acid that impairs
LTG metabolism and requires lowering the dosage
Few other drug interactions as is only a mild P450 inducer,
other strong inducers will lower levels and may require a
higher dosage

Topiramate (TPM) Topamax®/Trokendi-XR®/Qudexy-XR®
Arrived US market 1996 – FDA approved for LGS
Formulations (generic and brand name)
Tablets (twice daily)
Sprinkle capsules (twice daily)
Extended release sprinkle capsules (once daily)
Broad spectrum AED with efficacy for most seizure types,
except for absence seizures
Safety issues are kidney stones, metabolic acidosis, and acute
glaucoma
Requires safety monitoring blood work for acidosis

Topiramate (TPM) Tolerability issues are cognitive slowing, weight loss and
paresthesias (numbness and tingling – orange juice helps)
Behavior – overall, behavior neutral.
Approved by FDA to treat migraine headaches
Not usually able to start quickly due to cognitive effects
Drug-to-drug interactions
Few significant drug interactions and none with other AEDs

Levetiracetam (LVT) Keppra®/Keppra-XR®/Spirtam®(first drug made with 3D printing)
Arrived US market 1999 – NOT FDA approved for LGS
Formulations (generic and brand name)
Liquid (twice daily)
Tablets (twice daily)
Extended release tablets (once daily)
Intravenous solution (twice daily)
Orally disintegrating tablets (twice daily)
Broad spectrum AED with particular efficacy for myoclonic
seizures and little efficacy absence seizures
Safety issues are related to effects on behavior with aggression
No safety monitoring blood work is needed

Levetiracetam (LVT) Tolerability issues are mostly related to adverse effects on
behavior with aggression and agitation
Behavior – negative and can be severe
Able to “load” orally or IV and can start quickly
Drug-to-drug interactions
No significant drug interactions and none with other AEDs

Zonisamide (ZNS) Zonegran®
Arrived US market 2000 – NOT FDA approved for LGS
Formulations (generic and brand name)
Capsules (once daily)
Broad spectrum AED with similar efficacy as topiramate,
except works for atypical absence seizures
Safety issues similar to topiramate with kidney stones and
metabolic acidosis, but no acute glaucoma
Requires safety monitoring blood work for acidosis

Zonisamide (ZNS) Tolerability issues are similar to topiramate with cognitive
slowing and weight loss, but no paresthesia
Behavior – overall, behavior neutral
Not usually able to start quickly due to cognitive effects
Drug-to-drug interactions
Few significant drug interactions and none with other AEDs

Rufinamide (RFM) Banzel®
Arrived US market 2008 – FDA approved for LGS
Formulations (brand name only)
Liquid (twice daily)
Tablets (twice daily)
Broad spectrum AED with efficacy for most generalized seizure
types, except for absence seizures
Safety issues are cardiac arrhythmias and cannot use if have
familial short-QT syndrome
Must obtain ECG before taking

Rufinamide (RFM) Tolerability issues are dizziness, sleepiness, GI upset
Behavior – tends to be relatively behavior neutral
Not usually able to start quickly due to dizzy/sedative effects
Drug-to-drug interactions
valproic acid impairs rufinamide metabolism and serum
levels may rise
Few other drug interactions as is only a very mild P450
inducer and inhibitor

Clobazam (CLB) Onfi®
Arrived US market 2011 (most of rest of world in early 1980’s)
FDA approved for LGS
Formulations (brand name only)
Liquid (once or twice daily)
Tablets (once or twice daily)
Broad spectrum AED with efficacy for most generalized seizure
types, except for absence seizures
Safety issues are related to it being a benzodiazepine (broadly
in same category as diazepam – Valium®)
Marked sedative effects if combined with other sedating
medications or alcohol

Clobazam (CLB) Tolerability issues are similar to, but less severe than other
benzodiazepines with cognitive slowing, sedation, and drooling
Behavior – overall, behavior neutral, but some children may
become agitated and aggressive
Not usually able to start quickly due to cognitive and sedative
effects
Drug-to-drug interactions
cannabidiol (CBD) – impairs clobazam metabolism and levels may
increase substantially
Few other significant drug interactions and none with other AEDs

Medical Marijuana

Courtesy of Fernando Stein MD

Interest in several neurologic conditions – pain,
spasticity, epilepsy
Fervor in epilepsy community based upon report of
child with Dravet syndrome (CNN – Charlotte’s Web)
Cannabis contains >80 cannabinoids
THC - tetrahydrocannabinol
CBD – cannabidiol
Thought to have no abuse potential and to have anti-
seizure properties
Basic science suggested efficacy in animal models
Several States have approved Medical Marijuana
First worldwide clinical trial completed in Dravet
syndrome and ongoing in LGS
Medical Marijuana

Conclusions There are a number of safe and effective
medications available for the management of
seizures associated with LGS
Management should focus on maximizing quality
of life – as few seizures and as few adverse
effects as possible
Nonpharmacologic treatments should be
considered early if medications are not working,
especially curative ones if possible
Exciting and innovative new medical and surgical
treatments are rapidly emerging

Thank-you!


Non-pharmacologic Therapies for LGS
Scott Demarest MD Assistant Professor, Departments of Pediatrics and Neurology University of Colorado School of Medicine Children's Hospital Colorado

Disclosures
My epilepsy genetics research is supported by NIH funding through a K12 mechanism.
No conflicts of interest
I want to thank Drs. Kelly Knupp and Anup Patel who have provided me with some of these slides
Objectives
• Where do non-pharmacologic therapies fit into epilepsy treatment and LGS?
• What kinds of therapies are these?
• What are the advantages of one therapy over another?
• What is on the Horizon?

Goals of Epilepsy Treatment
According to the Epilepsy Foundation, the goal of all epilepsy treatment is to:
Prevent further seizures Avoid side effects Make it possible for people to lead active lives
When Epilepsy is intractable specific treatment goals should drive care!

Intractable Epilepsy Treatment Goals
We always want less seizures and less side effects…
But
These two goals often are in conflict.
Patients and families should define SPECIFIC treatment goals with their neurologist to help prioritize and balance treatment and side effects.

Medications Are Still the Mainstay of Treatment
Basic principals
• Use a single drug whenever possible
(or as few as possible)
• Start low and go slow
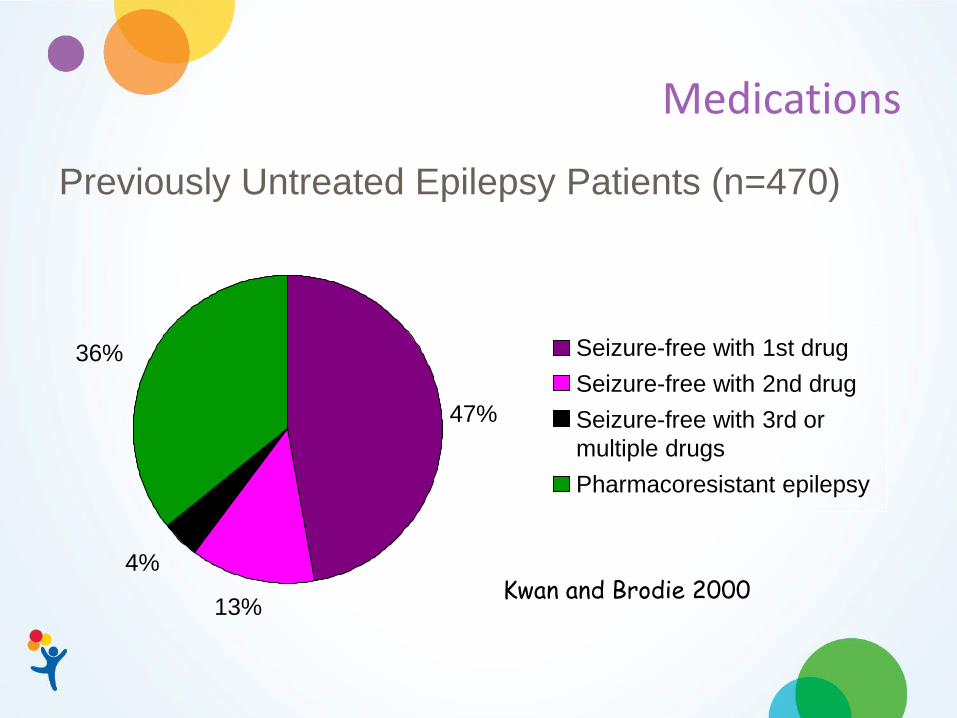
Medications
13%
4%
36%
47%
Seizure-free with 1st drug
Seizure-free with 2nd drug
Seizure-free with 3rd or
multiple drugs
Pharmacoresistant epilepsy
Kwan and Brodie 2000
Previously Untreated Epilepsy Patients (n=470)

Medications
13%
4%
36%
47%
Seizure-free with 1st drug
Seizure-free with 2nd drug
Seizure-free with 3rd or
multiple drugs
Pharmacoresistant epilepsy
Kwan and Brodie 2000
Previously Untreated Epilepsy Patients (n=470)

Medications
13%
4%
36%
47%
Seizure-free with 1st drug
Seizure-free with 2nd drug
Seizure-free with 3rd or
multiple drugs
Pharmacoresistant epilepsy
Kwan and Brodie 2000
Most LGS Patients Meds are not working well enough.
What else can we try?

Medications
13%
4%
36%
47%
Seizure-free with 1st drug
Seizure-free with 2nd drug
Seizure-free with 3rd or
multiple drugs
Pharmacoresistant epilepsy
Kwan and Brodie 2000
≠ Better

There are a lot of Meds
Older Medications
(1st Generation)
Generic Name Year Introduced Trade
Name
Bromides 1857 —
Phenobarbital 1912 Luminal®
Phenytoin Sodium 1956 Dilantin®
Ethosuximide 1960 Zarontin®
Diazepam 1963 Valium®
Carbamazepine 1968 Tegretol®
Lorazepam 1977 Ativan®
Valproic acid 1978 Depakene®
Divalproex sodium 1983 Depakote®
Carbamazepine 1986 Epitol®
Diazepam 1997 Diastat®
Carbamazepine 1997 Carbatrol®
Phenytoin Sodium 1998 Phenytek®
Newer Medications
(2nd & 3rd Generation)
Generic Name FDA Approval Trade
Name
Felbamate 1993 Felbatol®
Gabapentin 1993 Neurontin®
Lamotrigine 1994 Lamictal®
Topiramate 1996 Topamax®
Tiagabine 1997 Gabitril®
Levetiracetam 1999 Keppra®
Oxcarbazepine 2000 Trileptal®
Zonisamide 2000 Zonegran®
Pregabalin 2005 Lyrica®
Rufinamide 2007 Banzel ®
Lacosamide 2008 Vimpat ®
Vigabatrin 2009 Sabril ®
Clobazam 2011 Onfi ®
Esogabine 2012 Potiga ®
Preampanel 2013 Fycompa®
Eslicarbazepine 2013 Aptiom®
But is there something else to try?
So what do we do if meds aren’t working?
We think about:
• Surgery
• VNS
• Ketogenic diet

Cannabidiol – lets get this out of the way
This is non-pharma but still a drug
(Actually ~200 drugs if taking an artisanal preparation)
This is not something I recommend, but I do have many patients taking it.
There is time devoted to this on Sunday

Resective Surgery The first thing I think about
Most patients are not candidates for resection… But focal lesions in the brain or large lesions mostly on one side of the brain can cause LGS (or an LGS-like syndrome) and those patients may be a surgical candidates (PMID – 25284034). This is important to think about as surgery in this setting is a potential cure for epilepsy. These surgeries are a big deal and usually are either a hemispherectomy or multilobar surgery (though not always).

Then what?
Can consider:
• Ketogenic diet
• VNS
• Corpus Callosotomy

The Ketogenic Diet
• High fat, low carb, enough protein diet
• This can be done in patients with or without a Gtube (formula based or through food)
• Requires the guidance of a dietician
• This diet switches the brain to using fats for an energy source instead of sugar
We don’t really understand why this works…

Ketogenic Diet
Approximately 50% of patients with LGS respond to the KD with a >50% reduction in seizures and some patients (23%) may achieve a >90% reduction (Retrospective – PMID 22443637) Patients usually admitted to start diet Some places have patients fast prior to starting diet Should give it a 3 months trial Re-evaluate after 1-2 years on treatment

Potential Side Effects of the KD
Constipation (Drink lots of water)
Vomiting
Abdominal pain
Decreased energy
High cholesterol
Kidney stones (Drink lots of water)
Slower growth potential (Probably not if being monitored appropriately)

Other Dietary Therapies
Modified Adkins diet
Low-Glycemic index diet
Less restriction
Not been well studied in LGS patients
Could be good options for some to consider
Vitamins and Supplements
Vitamin B6 and/or folinic (not folic) acid used for infants who have a deficiency of this vitamin as a cause for their seizures
•This is usually the result of specific genetic changes
Other vitamins not clinically proven to help

Vagus Nerve Stimulator
The VNS Therapy System consists of
an implanted pacemaker-like
generator and nerve stimulation
electrodes, which deliver
intermittent stimulation to the
patient’s left vagus nerve that sends
signals to the brain

Vagus Nerve Stimulator
It is used as add on treatment for drug-resistant epilepsy (including patients with LGS) who are not suitable candidates for resective surgery 50% of LGS patients respond to VNS therapy, with at least a >50% reduction in seizures Response may improve over time Appears best for drop attack (atonic) seizures Recent American Academy of Neurology (AAN) guideline recommends that VNS be considered for patients with LGS

VNS may be considered for seizures in children, for LGS-associated seizures
Seizure detection by change in heart rate for activation (Aspire SD)
Longer battery life (now available)
Vagal Nerve Stimulator (VNS)
VNS – Side Effects
Site infection
During stimulation: (Typically resolves if turned off) Hoarseness
Drooling
Cough
Voice alteration
6-23% of patients had worsening behavior or hyperactivity

Corpus Callosotomy
Cuts the connection between the two sides of the brain

Corpus Callosotomy
There have been a few small studies: • 60-90% - >50% reduction in seizures • 50-75% - >90% • 10-15% seizure free
PMIDs – 2401256, 24912732, 16499762, 25284034
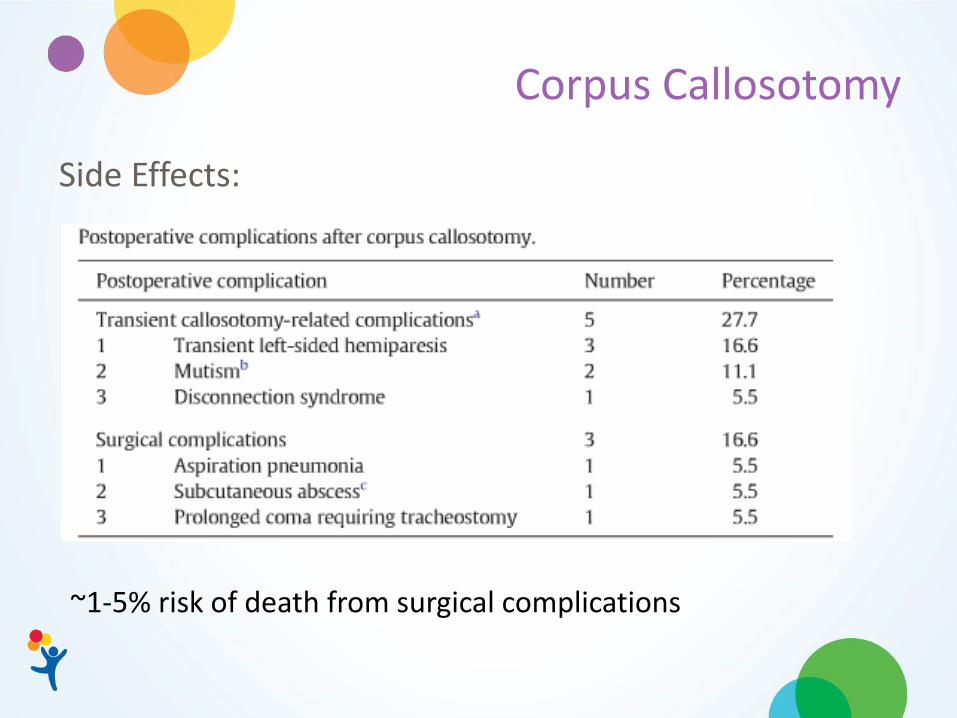
Corpus Callosotomy
Side Effects:
~1-5% risk of death from surgical complications

Corpus Callosotomy vs VNS
CC is better for Atonic • 80% vs 55% - >50% reduction in Atonic seizures • 70% vs 26% - >75% reduction in Atonic seizures BUT otherwise no difference in efficacy for other seizure types
***You can do one after the other and there is continued *** improvement in seizures
PMID – 23068970, 26979179
Those are the mainstays…
but what else is there?

CNS implanted device that would recognize seizure activity and activate signal to stop it Potentially more benefit for patients with bilateral mesial temporal sclerosis or other focal epilepsies Not clear how helpful this will be for LGS Recently FDA approved Not currently approved for children
Responsive NeuroStimulation (RNS)

Steroids
• Prednisone and ACTH have been used
• There are many small studies that are not high quality
• Potentially dangerous side effects
What do we do about the relapse rate???
PMID: 17951084

Steroids
PMID: 26086765

Intravenous Immunoglobulin (IVIG)
PMID: 17521345

IVIG and Steroids
There are many small LOW quality studies that have interesting and somewhat promising results.
These treatments are invasive and can be dangerous
(and are expensive – ACTH and IVIG)
We need HIGH quality randomized
control trials!

A note on personalized medicine
Probably ~20-40% of patients with LGS are due to genetic causes
• There are numerous genes
• DNM1, CDKL5, STXBP1, GABRB3, HDAC4, ALG13, SCN1A, SCN2A, SCN8A… to name a few
The goal is genetic cause specific treatments for epilepsies like LGS that target the underlying problem
This is just getting started
but this will be a real thing 5-10 years from now

Quick review: My approach
You have to try a few meds first but if that does not work:
1. Think about resective surgery (only chance for cure)
2. What seizure type is the biggest problem?
VNS vs ketogenic diet vs Corpus Callosotomy
3. Can try ALL or some of these…

Quick review: My approach
Now we are off the beaten path:
• Steroids
• IVIG
There are logistical barriers in many cases AND There are important side effects to consider

Throughout the Journey
We often are trying new medications between some of these options
Be careful to make one change at a time so you know what helps or hurts!
I keep looking for the cause if it is not known. This is becoming more and more likely to impact treatment.
Never stop advocating for our kids!
We can make things better!!

Thank You
I think we are taking questions at the end