
LGS Foundation 2016 Conference - Friday Afternoon
66
-
Upload
lgs-foundation -
Category
Healthcare
-
view
229 -
download
0
Transcript of LGS Foundation 2016 Conference - Friday Afternoon


Lennox-Gastaut Foundation: Denver April 29, 2016
• Comorbid Neurocognitive Aspects of Lennox-Gastaut Syndrome: Understanding why this type of epilepsy affects development
• Michael G. Chez MD
• Director of Epilepsy Program
• Sutter Neuroscience Institute
• Sacramento CA
History
• William G. Lennox 1884–1960
• Henri Gastaut 1915-1995
• Defined EEG and Clinical Abnormalities of this disease
• LGS clinically described syndrome is actually spectrum of causes

Defining LGS
• Incidence: estimate 2:100,000 0.002%
• Approximately 4% of Children with epilepsy
• 20 % prior Infantile Spasms of West Syndrome

Clinical Facts • Age of onset typically after age 2
• Can be normal development before onset
• 80-90% cognitive decline(Doose form may be milder)
• May rarely start in adolescence or adult
• Mortality rate ranges from 3% to 7%

Clinical Manifestations
• Seizure Onset may be sudden and progress rapidly if not prior seizure history (i.e. prior infantile spasms)
• Spectrum of Causes
• Idiopathic 30%
• Lesional 70%
• Syndrome
• Genetics

IMPORTANT FACT
• ONSET: Mostly age 2-6 years, typically before age 4
• Overlaps peak ability for the brain to make language
• Overlaps frontal temporal myelination period and pruning
• Refractive to Standard AEDs typically

TONIC SEIZURE LGS

EEG Pattern LGS

Lennox Gastaut Syndrome
• Clinical seizure types:
• Generalized grand mal, atypical prolonged absence, myoclonic, tonic, and drop seizures
• Can have hundreds per day
• Difficult to control
• Treatment often not effective

Syndromes that can show Lennox-Gastaut that have autism features
• Syndromes: trisomy 13, Angelmann’s, Aicardi Syndrome, Retts, Tuberous Sclerosis, 20% prior West Syndrome(Infantile Spasms),Cri de Chat, Shank 2,3 (Phelan McDermitt), and others
• Isolated chromosomal abnormalities; Chromosomal duplication/deletions with abnormalities that overlap autism 15q31.33 XP22.33 CATNP2, 7q36, 7q21, PCDH19 CDLK5, TCBD1 among many others
• Channelopathies SCN1A, SCN2A GABR3 KCNq2, Ca channelopathies among others
• Lissencephaly and other migrational genetic abnormalities
• Degenerative Conditions like Battens may mimic

LGS Syndrome
• Cognitive Disability: a main concern
• 80-90% cognitive disability
• 80-90% some autistic symptoms; especially early onset and language not developed; Dravet’s and others
• ADHD behavioral hyperactivity, impulsivity 50%

Autism and LGS Genes
• Much in common
• Overlap of both conditions
• Often synaptic or membrane receptor issues
• Inflammation issues similar in both
• Often same age onset
• Can have some of these genes and no epilepsy

LGS and Autism
• Autism is a clinical diagnosis
• Certain core Social Language and Stereotypical Behaviors
• Any early childhood language delay may lead to behavioral problems and may mimic autism
• Early onset epilepsy effects are on language and thalamocortical and prefrontal connections; autism has similar regions affected

What Happens?
• Absence seizures can disrupt prefrontal and thalamocortical connections/tracts
• Research shows this with imaging
• Attention deficits can be seen with Absence Seizures
• Many factors in evolution cognitive and physiological issues and subsequent behavioral and clinical outcomes

Neurocognition in Epilepsy
• Age of onset
• Seizure type/EEG pattern/Duration/Severity
• Treatments
• Educational and Emotional factors
• Comorbid factors: Lesion, Infection, Inflammation, Hypoxia, Injury, Surgery

Neurocognitivie Deficits in Epilepsy
• Earlier onset affect pathways associated with corresponding development
• Infancy more occipital parietal posterior temporal
• Can disrupt sensory motor coordination visual motor and language understanding
• fMRI correlation with atypical speech localization in medical literature

Neurocognition and Epilepsy
• Multiple research papers point to pre-existing deficits before seizure onset in school age children
• Even treated typcial Childhood Absence Epilepsy (CAE) shows different frontal cortical connections

Cognition and Epilepsy
• Rasmussens Syndrome: Hemispherectomy
• Good example of early brain plasticity
• Can be good thing as functions can still move to the other hemisphere if operate before age 5 may still be able to walk etc.
• However early plasticity also effected by multiple issues and not as firmly developed as memory loss say as adolescent or adult in typical temporal lobe epilepsy

Neurocognition in LGS
• Age 2-5: peak language and specialization and improvement of early frontal lobe executive function and motor coordination
• Frequency of interictal discharges can make difference in noticable effect of epileptic activity on attention (> 20 interictal spikes/hr)
• Frontal lobes and extra-temporal regions affected in early childhood epilepsy like LGS

Cognition in Early Childhood
• Excitable cortex with increased synapses and glutaminergic transmission that allows plasticity and learning can also abnormally form and spread epileptic connectivity
• Inflammation affects cytokine levels and may affect or prune connections
• LGS constant atypical slow spike wave imagine its effect on regions of brain being discussed

Early LGS and Cognition
• Subcortical Connections affect emotional and attention
• Absence and partial complex seizures in childhood show decreased instead of increasing thalmic left sided volume compared to controls and orbitofrontal gyri smaller less asymmetric than controls ( Left > right side)
• Correlation to behavior and attention emotional decision making
• Language arcuate fasciculus may be affected change language self-awareness

Neurocognition and LGS
• If preschool affected functions delayed
• Triggers poor start grade school
• Success in first grade associated with high school class rank
• As children age pruning occurs at adolescence
• Depending on frequency seizures and generalized or focal spikes this will vary
• As age, patients can develop more focal seizures as well

Head trauma in LGS
• New evidence repeated concussion or head injury may increase inflammation and subcortical connectivity may be damaged
• Add this to epilepsy effects discussed
• Patients with drop attacks often fall but sleepiness or vomiting or headache or dizziness ataxia may goe unnoticed in this LGS population
• Need to be more aware of this additional factor

Conceptualizing Lennox–Gastaut syndrome as a secondary network epilepsy John S. Archer1,2,3*, Aaron E. L. Warren1, Graeme D. Jackson1,2,3 and David F. Abbott1,2
• epileptic activity is expressed through large-scale
brain networks, particularly the attention and default-mode networks.
• Cortical lesions, when present, appear to chronically interact with these networks to produce network instability rather than triggering each individual epileptic discharge.
• LGS can be considered as “secondary” network epilepsy because the epileptic manifestations of the disorder reflect the networks being driven, rather than the specific initiating process
THALAMIC ROLE LGS
• generalized nature of epileptic discharges and seizures has led many to postulate that the thalamus may be a key initiator of epileptic activity in LGS.
• Recordings from the thalamus during generalized epileptic discharges of LGS confirm that the thalamus is involved
• EEG–functional magnetic resonance imaging (fMRI) studies have shown thalamic involvement during SSW and generalized spike-and-wave
• thalamus is probably acting as a synchronizer and amplifier, rather than initiator.

LGS Pattterns fMRI: PFS and SSW

LGS Tonic Seizure

Symptomatic (Lesional)LGS
• This occurs in 60-70%
• Brain injury of focal or multifocal spikes may evolve early in development into LGS pattern
• Some may be predisposed vs remaining focal issue
• Thalamic involvement may spread or synchronize connections for this pattern change
• Removal of focal lesion can still lead to repair and control of epilepsy and improved function

Treating Neurocognitive Comorbidity
• Affects attention language frontal lobe issues and subcortical regions in LGS
• Can offer help by following: 1. Early treatment Seizures
• 2. treat comorbid issues attention and behavior
• 3, prevent further injury
• 4. identify focal lesion or onset issues-possible surgery

Hope For Neurocognitive Deficits
• Correct Diagnosis of Epilepsy and Cause
• Intervene with appropriate treatment for symptoms that are comorbid
• Early speech OT PT and ABA type therapies are important
• Prevent head injury
• Identify EEG and Genetic or lesional issues

LGS Treatments
• Pharmaceutical: Avoid most sodium channel drugs • Felbamate; Lamictal; Topiramate; Rufinamide; Clobazam • More broad spectrum agents • Consider ACTH or steroids; high dose benzodiazepines especially in
lesional or idiopathic non-genetic cases; other immune therapy; stem cell future
• Nutritional: Ketogenic Issues
• Surgical Options

LGS Syndrome
• Some Lesional may actually be surgical candidates if pre-2 yr or early onset was focal.
• Often not go back to original onset diagnosis
• Need to be aggressive with these patients both diagnostic testing and with reviewing prior tests and treatments

Case Examples
• Following individual cases may give insight how to get better results for some cases
• Examples of focal lesional
• Genetic
• response to high dose valium or acth to reestablish focal surgical site

LGS SYNDROME
• Case Examples: Case 1
• Patient with focal onset seizures left temporal lobe
• Had 2 surgeries but seizures than spread and became LGS
• Failed all combinations typical medications
• Reassess videa EEG and treatment
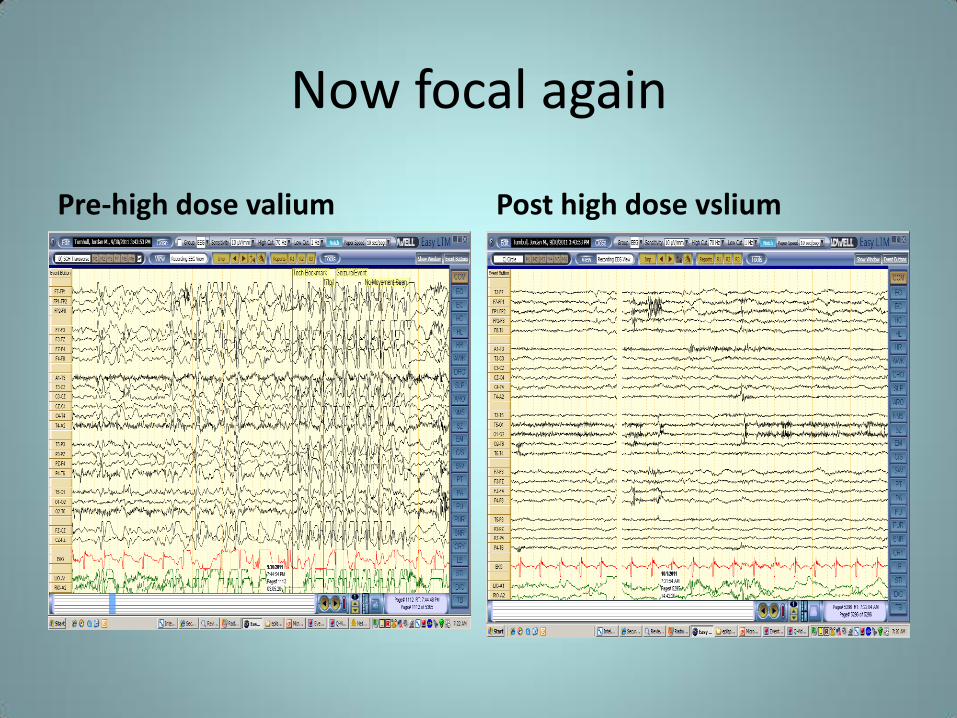
Now focal again
Pre-high dose valium Post high dose vslium

Case 2
• Patient with autistic decline LGS after neonatal stroke from infection/shock
• Cognitive delays
• EEG with atypical absence generalized seizures and CSWS and slow spike wave activity
• Actually focal frontal case surgical option?
• Seizure free since 2011 laser ablation

JP sleep pre-vimpat/ keppra added to Depakote

MEG Left MEG Right
R L
A P
L
EEG
R L
R
MEG 7/29/11
MRI 7/20/11 Patient after localization with treatment MEG

Case 3
• 4 year old PDD-NOS
• Seizures with atypical absence and drops
• Never diagnosed
• LGS varient
• Shows genetic abnormality on microarray

JP 7q21.3 copy deletion post-depakote/pre-felbatol/clobazam

JP Chromosome 7q21.3 deletion post-felbatol and clobazam July 2011 at 8 weeks
Future Options
• Individual Genetic options • May guide better response to certain
pharmaceutical options • Fenfluramine/ CBD/ Ganaxolone/ Rationale
Polytherapy • Immune Modulation • DBS • Laser Ablation/Resection of lesions • Possible neuroregenerative options: Stem Cell • Computer brain technology growth
Conclusions • Neurocognitive effect of LGS makes sense
• Research explains many interactions and potential interventions
• Treat clinical phenotype as needed: treat ADHD ABA therapy speech OT PT Frontal lobe issues
• Be aggressive with epilepsy early and with work up genetics and imaging and monitor EEG with treatment
• Advocate and be proactive: Discuss and find appropriate team approach










National resources for individuals with LGS
Jenni Wolfenbarger, MPH
JoyfulJourneyMom.com

Introduction

Wish Granting Organizations
Make A Wish Foundation
Dream Factory
Dream Foundation
Sunshine Foundation
Kids Wish Network
Jason’s Dream for Kids

Medical Equipment/Therapies
Wheelchairs 4 Kids
Grotto Humanitarian Foundation
United Healthcare Children’s Foundation
MY GYM Challenged America
Aubrey Rose Foundation
Project Mend
Gia Nicole Angel Foundation
Building Blocks for Kids

Resources for Epilepsy
The Danny Did Foundation
Chelsea Hutchinson Foundation
TJ Joy Memorial Fund
Paws with a Cause
J Kiffin Penry Patient Travel Assistance Fund
Clinical Trial Patient Assistance Fund (Epilepsy Foundation)
Respite care funds through some local Epilepsy Foundation affiliates

Camps/Respite
Deliver the Dream
The Center for Courageous Kids
Paul Newman Camps
David’s Refuge

Grants for Medical Travel
First Hand Foundation
Angel Flight
The Carrie Premsagar Foundation

Free Services and Gifts
Santa’s Little Hackers
Feel Better Friends
Ween Dream
Peach’s Neet Feet
Tiny Superheroes
Icing Smiles
Special Spaces
Sharing the Weight

Non-profits and Companies working together
Encourage companies to research grants for their products
Ex:Koolway Sports and grant foundations working together to serve families

~Jessie Doyle
I think the hardest part of having a child with a delay of any kind is the fight:
The fight for services. The fight for people to understand who
your child is and what they need. The fight for knowledge, because
knowledge is power. And the quiet fight you have within yourself wondering if you’ve left no
stone unturned.

Thank You!



















