LECTURA FISIOPATOLOGIA AINES

of 18
-
Upload
kari-chaynasc -
Category
Documents
-
view
221 -
download
0
description
La fisiopatológica de los aines y su utilización.
Transcript of LECTURA FISIOPATOLOGIA AINES
-
14/7/2015 NSAIDs:Mechanismofaction
http://www.uptodate.com/contents/nsaidsmechanismofaction?topicKey=RHEUM%2F7989&elapsedTimeMs=0&source=search_result&searchTerm=aine 1/18
OfficialreprintfromUpToDate www.uptodate.com2015UpToDate
AuthorDanielHSolomon,MD,MPH
SectionEditorDanielEFurst,MD
DeputyEditorPaulLRomain,MD
NSAIDs:Mechanismofaction
Alltopicsareupdatedasnewevidencebecomesavailableandourpeerreviewprocessiscomplete.Literaturereviewcurrentthrough:Jun2015.|Thistopiclastupdated:Nov20,2014.
INTRODUCTIONMorethan17,000,000Americansusevariousnonsteroidalantiinflammatorydrugs(NSAIDs)onadailybasis,makingthisclassofdrugsoneofthemostcommonlyusedintheworld.TheCentersforDiseaseControlintheUnitedStatespredictsthat,withtheagingofthepopulation,therewillbeasignificantincreaseintheprevalenceofpainfuldegenerativeandinflammatoryrheumaticconditions,leadingtoaparallelincreaseintheuseofNSAIDs.
HISTORYSodiumsalicylate,discoveredin1763,wasthefirstnonsteroidalantiinflammatorydrug(NSAID).Gastrointestinaltoxicity(particularlydyspepsia)associatedwiththeuseofacetylsalicylicacid(ASA)ledtotheintroductionofphenylbutazone,anindoleaceticacidderivative,intheearly1950sthiswasthefirstnonsalicylateNSAIDdevelopedforuseinpatientswithinflammatoryconditions.Phenylbutazoneisaweakprostaglandinsynthetaseinhibitorthatalsoinducesuricosuria.Itwasshowntobeausefulagentinpatientswithankylosingspondylitisandgout.Concernsrelatedtobonemarrowtoxicity,particularlyinwomenovertheageof60,haveessentiallyeliminatedtheuseofthisdrug.
Indomethacin,anotherindoleaceticacidderivative,wasdevelopedinthe1960sasasubstituteforphenylbutazone.ThefollowingyearswitnessedthedevelopmentofmoreandmoreNSAIDsinanefforttoenhancepatientcompliance(bydecreasingtheabsolutenumberofpillsandfrequencywithwhichtheyaretakeneachday),reducetoxicity,andincreasetheantiinflammatoryeffect.
PHARMACOLOGYTherearenowatleast20differentnonsteroidalantiinflammatorydrugs(NSAIDs),fromsixmajorclassesdeterminedbytheirchemicalstructures,availableforuseintheUnitedStates.Thesedrugsdifferintheirdose,druginteractions,andsomesideeffects.Acomparisonofthedrugs,organizedbychemicalgrouping,ispresentedinthetable(table1).Druginteractionsandsideeffectsarediscussedseparately.(See'Druginteractions'belowand"NonselectiveNSAIDs:Adversecardiovasculareffects"and"NonselectiveNSAIDs:Overviewofadverseeffects".)
PharmacokineticsMostNSAIDsareabsorbedcompletely,havenegligiblefirstpasshepaticmetabolism,aretightlyboundtoserumproteins,andhavesmallvolumesofdistribution.NSAIDsundergohepatictransformationsvariouslybyCYP2C8,2C9,2C19and/orglucuronidation.HalflivesoftheNSAIDsvarybutingeneralcanbedividedinto"shortacting"(lessthansixhours,includingibuprofen,diclofenac,ketoprofenandindomethacin)and"longacting"(morethansixhours,includingnaproxen,celecoxib,meloxicam,nabumetoneandpiroxicam).Patientswithhypoalbuminemia(due,forexample,tocirrhosisoractiverheumatoidarthritis)mayhaveahigherfreeserumconcentrationofthedrug.
AssessmentoftoxicityandtherapeuticresponsetoagivenNSAIDmusttakeintoaccountthetimeneededtoreachthesteadystateplasmaconcentration(roughlyequaltothreetofivehalflivesofthedrug).ThepathogenesisofsymptomaticpepticulcerdiseasecausedbyexposuretoNSAIDsismainlyaconsequenceofsystemic(postabsorptive)inhibitionofgastrointestinal(GI)mucosalcyclooxygenase(COX)activity.(See"NSAIDs(includingaspirin):Pathogenesisofgastroduodenaltoxicity".)
ThechoiceofoneNSAIDoveranothershouldconsiderpatientspecificriskfactorsfortoxicityandthewayinwhichthedrugismetabolized.Inolderpatients,forexample,thepossiblebenefitofincreasedcompliancewithlongeractingdrugsisprobablyoffsetbytheenhancedincidenceofgastrointestinaltoxicityassociatedwithprominententerohepaticcirculationofactivemetabolites.NSAIDswithashorthalflifeandnoenterohepatic
-
14/7/2015 NSAIDs:Mechanismofaction
http://www.uptodate.com/contents/nsaidsmechanismofaction?topicKey=RHEUM%2F7989&elapsedTimeMs=0&source=search_result&searchTerm=aine 2/18
circulationmaybethebestchoicesforolderdebilitatedpatients,althoughanyuseofNSAIDswouldgenerallybeavoidedinsuchpatientsbecauseoftheirpotentialtoxicityinthispopulation.Inaddition,allagentsshouldbeusedatthelowesteffectivedose.
DruginteractionsNSAIDscaninteractwithnumerousdrugs.Theseincludeanticoagulants,antiplateletagents,antihypertensives,calcineurininhibitors(cyclosporineandtacrolimus),digoxin,diuretics,glucocorticoids,lithium,selectiveserotoninreuptakeinhibitors(SSRIs),methotrexate(MTX),andothermedications.TheinteractionofNSAIDswithMTXgenerallyrequiresavoidanceofNSAIDuseinpatientsreceivingantineoplasticdoses,whilebothmaybeusedconcurrentlywithstandardMTXmonitoringapproachesinpatientsreceivinglowdoseMTX(eg,forthetreatmentofrheumatologicdisorders)[1].(See"Useofmethotrexateinthetreatmentofrheumatoidarthritis".)
InteractionsmayoccurduetoNSAIDrelatedreductioninrenalperfusionoradditivehemorrhagictoxicity.Furthermore,someNSAIDsmodestlyinhibitCYP2C9(ibuprofen,ketoprofen,flurbiprofen,indomethacin,diclofenac,meloxicam)orCYP2C8/2D6(celecoxib)and/orglucuronidation,whichmayincreaseconcentrationsofdrugshighlydependentonthesepathwaysforclearance.Theeffectsofsomeinteractionsarelistedbelow.(SeeLexiInteractprogramincludedwithUpToDateforadditionalinformation,includingsuggestionsformanagement,andtocheckforotherpotentialinteractions.)
AngiotensinconvertingenzymeinhibitorsNSAIDsmayattenuatetheefficacyofangiotensinconvertingenzymeinhibitorsbyblockingvasodilatorandnatriureticprostaglandinsandpotentiatinghyperkalemia.(See"MajorsideeffectsofangiotensinconvertingenzymeinhibitorsandangiotensinIIreceptorblockers",sectionon'Hyperkalemia'.)
LowdoseaspirinThecardioprotectiveeffectoflowdoseaspirinmaybenegatedbycertainNSAIDs.(See"NonselectiveNSAIDs:Adversecardiovasculareffects",sectionon'Patientstakingaspirinforprevention'.)
ThemorelimitedgastrointestinaltoxicityofCOX2selectiveagentscomparedwithnonselectiveNSAIDsmaybeoffsetbyconcurrentuseoflowdoseaspirin.(See"OverviewofselectiveCOX2inhibitors".)
GlucocorticoidsTheriskofpepticulcerdiseaseincreasessignificantlywhenglucocorticoidsareusedincombinationwithanNSAID,comparedwiththeuseofeitheralone.(See"Majorsideeffectsofsystemicglucocorticoids",sectionon'Gastrointestinaltract'.)
SSRIsTheuseofselectiveserotoninreuptakeinhibitorsincombinationwithNSAIDsisassociatedwithanincreasedriskofgastroduodenaltoxicitycomparedwiththeuseofdrugsfromeitherclassalone.(See"NSAIDs(includingaspirin):Pathogenesisofgastroduodenaltoxicity",sectionon'Riskofgastrointestinalcomplications'.)
WarfarinNSAIDscanincreasetheriskofbleedinginvitaminKantagonisttreatedpatientsbymultiplemechanismsincludinggastrointestinaltoxicity,increaseintheInternationalNormalizedRatio(INR),andinterferencewithplateletfunction.(See"BiologyofwarfarinandmodulatorsofINRcontrol".)
MECHANISMOFACTIONThereisaclearindividualvariationinresponsetononsteroidalantiinflammatorydrugs(NSAIDs)somepatientsseemtorespondbettertoonedrugthantoothers.PharmacodynamicsoftheindividualNSAIDs,includingtheirbiochemicalandphysiologicaleffectsandtheirmechanismsofaction,maybeveryimportantinpredictingtheultimateclinicalresponseanddrugefficacy.Bycomparison,pharmacokineticdifferencesacrossNSAIDs,includingdifferencesinabsorption,distribution,anddifferentialmetabolism,areprobablynotsignificantinthiscontext.Theriskofadverseeventsalsoseemstobevariableamongindividualdrugsandpatientsthesedifferencesinadverseeventriskhavebeenascribedtodifferencesinpharmacokinetics,includingabsorption,distribution,andmetabolism.Inaddition,numerousmechanismsofactionhavebeenascribedtotheNSAIDs.
CyclooxygenaseinhibitionTheprimaryeffectofNSAIDsistoinhibitcyclooxygenase(prostaglandinsynthase),therebyimpairingtheultimatetransformationofarachidonicacidtoprostaglandins,prostacyclin,andthromboxanes(figure1)[2].TheextentofenzymeinhibitionvariesamongthedifferentNSAIDS,althoughthere
-
14/7/2015 NSAIDs:Mechanismofaction
http://www.uptodate.com/contents/nsaidsmechanismofaction?topicKey=RHEUM%2F7989&elapsedTimeMs=0&source=search_result&searchTerm=aine 3/18
arenostudiesrelatingthedegreeofcyclooxygenaseinhibitionwithantiinflammatoryefficacyinindividualpatients[3,4].
COXenzymesTworelatedisoformsofthecyclooxygenase(COX)enzymehavebeendescribed[5,6]:COX1(PGHS1)andCOX2(PGHS2).TheCOX1andCOX2isoformspossess60percenthomologyinthoseaminoacidsequencesapparentlyconservedforcatalysisofarachidonicacid[711].AsplicevariantderivedfromtheCOX1genehasbeendescribedasCOX3.Therelevanceofthisisoformisstillunclear[12].Thereareimportantdifferencesintheregulationandexpressionoftheseenzymesinvarioustissues:
Thus,differencesintheeffectivenesswithwhichaparticularNSAIDinhibitsanisoformofcyclooxygenasemayaffectbothitsactivityandtoxicity.TheefficacyandsafetyofselectiveCOX2inhibitorsarediscussedindetailseparately.(See"OverviewofselectiveCOX2inhibitors".)
TheeffectofCOX2inhibitiononinflammationisnotcompletelyunderstood:
SomeolderNSAIDsarealsorelativelyselectivefortheCOX2receptoratlowdoses.Nabumetone,forexample,
COX1isexpressedinmosttissuesbutvariably.Itisdescribedasa"housekeeping"enzyme,regulatingnormalcellularprocesses(suchasgastriccytoprotection,vascularhomeostasis,plateletaggregation,andkidneyfunction),andisstimulatedbyhormonesorgrowthfactors.
COX2isusuallyundetectableinmosttissuesitsexpressionisincreasedduringstatesofinflammation,orexperimentallyinresponsetomitogenicstimuli.Asanexample,growthfactors,phorbolesters,andinterleukin1stimulatetheexpressionofCOX2infibroblasts,whileendotoxinservesthesamefunctioninmonocytes/macrophages[6,13].COX2isconstitutivelyexpressedinthebrain,inthekidney,inbone,andprobablyinthefemalereproductivesystem[14].
AnotherdistinguishingcharacteristicofCOX2isthatitsexpressionisinhibitedbyglucocorticoids[15].Thisobservationmaycontributetothesignificantantiinflammatoryeffectsoftheglucocorticoids.
COX3appearstobeexpressedatahighlevelinthecentralnervoussystemwithtranscriptsforthissplicevariantaccountingfor5percentofCOXmRNAitisalsofoundintheheart[12,16].
COX2knockoutmiceareassusceptibletoinflammationasintactmice[17,18].Paradoxically,COX1knockoutmiceshowlessulcerationaftertheadministrationofindomethacinthanintactmiceeventhoughtheirgastricprostaglandinE2levelsarereducedby99percent[19].
COX2mayhaveantiinflammatoryproperties.Usingananimalmodelofinflammationandcarrageenininducedpleurisy,onestudyshowedthatmaximalCOX2expressioncoincidedwithinflammatoryresolutionandwasassociatedwithminimalprostaglandinE2synthesis[20].
HumanTlymphocytesexpresstheCOX2isoenzymewhereitmayservearoleinboththeearlyandlateeventsofTcellactivation,suchastheproductionofinterleukin2,tumornecrosisfactoralpha,andinterferongamma[21].
AlthoughselectiveCOX2inhibitionmayproducelessgastrictoxicity,therehasbeenconcernthatCOX2inhibitioncoulddelayhealingofgastricerosionsorulcersandmayenhanceinjuryinaninflamedtissue,asinanexperimentalmodelofcolitis[2224].TheseobservationsmayhaveclinicalimportanceinpatientswithinflammatoryboweldiseaseinwhomnonselectiveNSAIDscanexacerbatethedisease.(See"Clinicalmanifestations,diagnosis,andprognosisofulcerativecolitisinadults".)
Aclinicallysignificantdelayinhealingofulcerswasnotobservedintheclinicaltrialsofcelecoxib.However,approximately40percentofthepatientsincludedinthetrialswererequiredtobefreeofulcerspriortostudyentry.Thus,theeffectofcelecoxibonulcerhealinginpatientswithpreexistingulcerdiseasehasnotbeenwellestablished.
-
14/7/2015 NSAIDs:Mechanismofaction
http://www.uptodate.com/contents/nsaidsmechanismofaction?topicKey=RHEUM%2F7989&elapsedTimeMs=0&source=search_result&searchTerm=aine 4/18
appearstobeamoreeffectiveinhibitorinsomeexperimentalsystemsofCOX2thanCOX1[25].EtodolacalsoinhibitstheCOX2isoformmorethanCOX1(10to1ratio)[26,27].
FurtherdiscussionrelatingtoCOX2inhibitorsispresentedelsewhere.(See"OverviewofselectiveCOX2inhibitors".)
StudieswithsalicylatesSalicylatesbarelyinhibitthecyclooxygenaseenzymeinpurecellfreeenzymesystems,and,incellmembranesystems,theireffectsarenotmeasurable.However,inahumanwholecellsystem,theyareverypotentinhibitorsofbothCOX1andCOX2,withthelatterinducibleformbeingmoresensitivetotheeffectsofthedrugthantheconstitutiveenzyme[28].Althoughthenonacetylatedsalicylatesarenotgoodprostaglandinsynthesisinhibitorsinvitro,clinicalstudieshaveshownthatthesedrugs(suchassalsalate)maybeaseffectiveasotherNSAIDsinpatientswithRA[29].
Theeffectsofacetylsalicylicacid(ASA)onCOX2activityareverydifferentfromtheeffectsonCOX1[30].AcetylatedCOX1andCOX2cannotformtheintermediateproductsofprostaglandinsynthesis.However,acetylatedCOX2retainsthecapacitytoalterarachidonicacidtoform15RHETE,whileacetylatedCOX1doesnot.15RHETEhasunknownbiochemicaleffects,butitmaybeimportantasamodulatorofproliferationsinceitisaproductofaninducibleenzymeduringstatesofinflammation[30].Thiseffectonproliferationmayhaveseveralinterestingramifications,includingtheuseofaspirinforthepreventionofcoloncancer(See'Apoptosis'belowand"NSAIDs(includingaspirin):Roleinpreventionofcolorectalcancer".)
StudieswithtopicalNSAIDsSeveralNSAIDsarenowavailableastopicalformulations.Thereisreasonableevidencethattheseagentsareeffectivecomparedwithplaceboforseveralchronicpainfulconditions,includingosteoarthritis[31].Moreover,therearedatademonstratingthattheseagentsareabsorbedandpenetratelocaltissuesintheareaofapplication[32].TopicalapplicationofNSAIDslimitssystemicabsorption[32]andtheassociatedsideeffectsanddruginteractions[33].
NonprostaglandinmediatedeffectsAlthoughaspirin(theonlyacetylatedNSAID)isnotthoughttohaveeffectsotherthanthoserelatedtoinhibitionofprostaglandinsynthesis,severalnonprostaglandinmediatedmechanismsofactionhavebeenpostulatedtoexplaintheactionsofthenonacetylatedsalicylatestheseobservationsmayalsoapply,toavaryingdegree,tothenonsalicylateNSAIDs[3,4].
Theroleofthesenonprostaglandinmediatedprocessesinclinicalinflammationremainsunclear.DespitethefactthatnonacetylatedsalicylateshaveshownequalantiinflammatoryefficacywhencomparedwithASAinpatientswithrheumatoidarthritis(RA)[35],thereisnoclearevidencethatcyclooxygenaseinhibitionisnotachievedatthedosesofdrugrequiredtoachieveanantiinflammatoryresponse[3,4,36].
NSAIDShavealsobeendemonstratedinvitrotoinhibitNFkappaBdependenttranscription,leadingtoinhibitionofinduciblenitricoxidesynthetase(iNOS)[37].Nitricoxidesynthetase,onceinducedbycytokinesandotherproinflammatorymediators,producesNOinlargeamounts,therebyleadingtoincreasedinflammation(includingvasocongestion,cytotoxicity,andvascularpermeability)[38].TherapeuticlevelsofaspirininhibitexpressionofiNOSandthesubsequentproductionofnitriteinvitro[37].Sodiumsalicylateandindomethacinhavenosucheffectsatpharmacologicdoses,althoughatsuprapharmacologicdosages,sodiumsalicylatealsoinhibitsnitriteproduction[37].
TheinhibitionofNFkappaBbysalicylatesmayberesponsibleforthecapacityofsalicylsalicylate(salsalate)to
SomeoftheseeffectsappeartoberelatedtothephysicochemicalpropertyofNSAIDsthatenablesthemtoinsertintobiologicalmembranesanddisruptimportantinteractionsnecessaryforcellfunction(eg,transmembraneaniontransport,oxidativephosphorylation,anduptakeofarachidonate).
NeutrophilfunctionisinhibitedbynonacetylatedsalicylatesandothernonsalicylateNSAIDsinvitro.Asanexample,NSAIDsinterferewiththeneutrophilendothelialcelladherencethatiscriticalfortheabilitytorespondtoinflammation.NSAIDsdecreasetheexpressionofLselectin,whichremovesacrucialstepinthemigrationofgranulocytestositesofinflammation[34].
-
14/7/2015 NSAIDs:Mechanismofaction
http://www.uptodate.com/contents/nsaidsmechanismofaction?topicKey=RHEUM%2F7989&elapsedTimeMs=0&source=search_result&searchTerm=aine 5/18
reducelevelsofHbA andtoimproveothermarkersofglycemiccontrolinpatientswithtype2diabetessuchstudieswerebased,inpart,ontheobservationthatNFkappaBisactivatedbyobesityandpromotesinsulinresistanceandriskfortype2diabetesandcardiovasculardisease[39].
ApoptosisAnoveleffectofNSAIDshasbeendescribedinvolvingprostaglandininhibition.Prostaglandinsinhibitapoptosis(programmedcelldeath)invivoNSAIDs,therefore,establishamorenormalcellcycleintheinflammatorystateviainhibitionofprostaglandinsynthesis[40].Animportantextensionoftheseobservationsmaybetheassociationbetweentheuseofaspirin,andperhapsotherNSAIDs,andareducedriskofcolorectalcancer.(See"NSAIDs(includingaspirin):Roleinpreventionofcolorectalcancer".)
Themechanismofthisprotectiveeffectcannotbeentirelyattributedtoinhibitionofprostaglandinsynthesis.Thetwoprerequisitesforthedevelopmentofcancerareproliferationandtheinhibitionofapoptosis.Onestudyfoundthatsulindacdecreasedthesizeofadenomatouspolypsinpatientswithfamilialadenomatouspolyposisbyincreasingapoptosisratherthanalteringproliferation[41].Cellproliferationwasstudiedviaimmunohistochemistryforcellnuclearantigeninagroupof22patientsrandomizedtoeithersulindac(150mgtwicedaily)orplacebo.Althoughsulindaccausedasignificantdecreaseinpolypsizeandnumberafterthreemonths,therewasnosignificantchangeincytokineticvariablesorcellcycledistribution.However,thesubdiploidapoptoticfractionwasincreasedsignificantlyinthepatientstreatedwithsulindac(31versus10percentatbaseline).Celecoxibhasalsobeenshowntoreducethedevelopmentofadenomasinpatientswithfamilialadenomatouspolyposisandinpatientswithsporadicadenomatouspolyps[4244].
INFORMATIONFORPATIENTSUpToDateofferstwotypesofpatienteducationmaterials,TheBasicsandBeyondtheBasics.TheBasicspatienteducationpiecesarewritteninplainlanguage,atthe5 to6 gradereadinglevel,andtheyanswerthefourorfivekeyquestionsapatientmighthaveaboutagivencondition.Thesearticlesarebestforpatientswhowantageneraloverviewandwhoprefershort,easytoreadmaterials.BeyondtheBasicspatienteducationpiecesarelonger,moresophisticated,andmoredetailed.Thesearticlesarewrittenatthe10 to12 gradereadinglevelandarebestforpatientswhowantindepthinformationandarecomfortablewithsomemedicaljargon.
Herearethepatienteducationarticlesthatarerelevanttothistopic.Weencourageyoutoprintoremailthesetopicstoyourpatients.(Youcanalsolocatepatienteducationarticlesonavarietyofsubjectsbysearchingonpatientinfoandthekeyword(s)ofinterest.)
SUMMARY
1c
th th
th th
BeyondtheBasicstopics(see"Patientinformation:Nonsteroidalantiinflammatorydrugs(NSAIDs)(BeyondtheBasics)")
Allnonsteroidalantiinflammatorydrugs(NSAIDs)areabsorbedcompletely,havenegligiblefirstpasshepaticmetabolism,aretightlyboundtoalbumin,andhavesmallvolumesofdistribution.HalflivesoftheNSAIDsvarybut,ingeneral,canbedividedinto"short"(lessthansixhours)and"long"(morethansixhours)actingdrugs.Patientswithhypoalbuminemia(due,forexample,tocirrhosisoractiverheumatoidarthritis)mayhaveahigherfreeserumconcentrationofthedrug.(See'Pharmacology'above.)
AssessmentoftoxicityandtherapeuticresponsetoagivenNSAIDmusttakeintoaccountthetimeneededtoreachthesteadystateplasmaconcentration(roughlyequaltothreetofivehalflivesofthedrug).Toxicity(eg,gastroduodenal)mayvarybasedupontheextentofenterohepaticcirculation,sincethisdefinesthelengthoftimeadrugcomesintodirectcontactwiththegastrointestinalmucosa.ThespecificchoiceofoneNSAIDoveranothershouldtakeintoconsiderationtheriskfactorsfortoxiceventsthatindividualpatientspossessandthewayinwhichthedrugismetabolized.NSAIDswithashorthalflifeandnoenterohepaticcirculationmaybethebestchoicesforolderdebilitatedpatients.Allagentsshouldbeusedatthelowesteffectivedose.(See'Pharmacology'above.)
ThereisindividualvariationinresponsetoNSAIDssomepatientsseemtorespondbettertoonedrugthan
-
14/7/2015 NSAIDs:Mechanismofaction
http://www.uptodate.com/contents/nsaidsmechanismofaction?topicKey=RHEUM%2F7989&elapsedTimeMs=0&source=search_result&searchTerm=aine 6/18
UseofUpToDateissubjecttotheSubscriptionandLicenseAgreement.
REFERENCES
1. ColebatchAN,MarksJL,EdwardsCJ.Safetyofnonsteroidalantiinflammatorydrugs,includingaspirinandparacetamol(acetaminophen)inpeoplereceivingmethotrexateforinflammatoryarthritis(rheumatoidarthritis,ankylosingspondylitis,psoriaticarthritis,otherspondyloarthritis).CochraneDatabaseSystRev2011:CD008872.
2. VaneJR.Inhibitionofprostaglandinsynthesisasamechanismofactionforaspirinlikedrugs.NatNewBiol1971231:232.
3. BrooksPM,DayRO.Nonsteroidalantiinflammatorydrugsdifferencesandsimilarities.NEnglJMed1991
toothers,whichmayinpartberelatedtopharmacodynamics,includingbiochemicalandphysiologicaleffectsandmechanismsofaction.Theriskofadverseeventsalsovariesamongindividualdrugsandpatientsthesedifferencesinadverseeventriskhavebeenascribedtodifferencesinpharmacokinetics,includingabsorption,distribution,andmetabolism.(See'Mechanismofaction'above.)
TheprimaryeffectofNSAIDsistoinhibitcyclooxygenase(prostaglandinsynthase),therebyimpairingtheultimatetransformationofarachidonicacidtoprostaglandins,prostacyclin,andthromboxanes.TheextentofenzymeinhibitionvariesamongthedifferentNSAIDS,althoughtherearenostudiesrelatingthedegreeofcyclooxygenaseinhibitionwithantiinflammatoryefficacyinindividualpatients.(See'Cyclooxygenaseinhibition'above.)
Tworelatedisoformsofthecyclooxygenase(COX)enzymehavebeendescribed:COX1(PGHS1)andCOX2(PGHS2).TheCOX1andCOX2isoformspossess60percenthomologyinthoseaminoacidsequencesapparentlyconservedforcatalysisofarachidonicacid.AsplicevariantderivedfromtheCOX1genehasbeendescribedasCOX3.Therelevanceofthisisoformisstillunclear.Thereareimportantdifferencesintheregulationandexpressionoftheseenzymesinvarioustissues.(See'COXenzymes'above.)
COX1isexpressedinmosttissuesbutvariably.Itisdescribedasa"housekeeping"enzyme,regulatingnormalcellularprocesses(suchasgastriccytoprotection,vascularhomeostasis,plateletaggregation,andkidneyfunction)andisstimulatedbyhormonesorgrowthfactors.COX2isusuallyundetectableinmosttissuesitsexpressionisincreasedduringstatesofinflammation,orexperimentallyinresponsetomitogenicstimuli.COX2isconstitutivelyexpressedinthebrain,inthekidney,inbone,andprobablyinthefemalereproductivesystemtheexpressionofCOX2isinhibitedbyglucocorticoids.DifferencesintheeffectivenesswithwhichaparticularNSAIDinhibitsanisoformofcyclooxygenasemayaffectbothitsactivityandtoxicity.(See'COXenzymes'above.)
Salicylatesbarelyinhibitthecyclooxygenaseenzymeinpurecellfreeenzymesystems,and,incellmembranesystems,theireffectsarenotmeasurable.However,inahumanwholecellsystem,theyareverypotentinhibitorsofbothCOX1andCOX2,withthelatterinducibleformbeingmoresensitivetotheeffectsofthedrugthantheconstitutiveenzyme.Althoughthenonacetylatedsalicylatesarenotgoodprostaglandinsynthesisinhibitorsinvitro,clinicalstudieshaveshownthatthesedrugs(suchassalsalate)maybeaseffectiveasotherNSAIDsinpatientswithrheumatoidarthritis(RA).(See'Studieswithsalicylates'above.)
Severalnonprostaglandinmediatedmechanismsofactionhavebeenpostulatedtoexplaintheactionsofthenonacetylatedsalicylatestheseobservationsmayalsoapply,toavaryingdegree,tothenonsalicylateNSAIDs.Theseincludedisruptionofinteractionsnecessaryforcellfunctionthroughactionsincellmembranesandinhibitionofneutrophilfunction,includingendothelialcelladherence,bynonacetylatedsalicylatesandothernonsalicylateNSAIDsinvitro.NSAIDShavealsobeendemonstratedinvitrotoinhibitNFkappaBdependenttranscription,leadingtoinhibitionofinduciblenitricoxidesynthetase(iNOS).(See'Nonprostaglandinmediatedeffects'above.)
-
14/7/2015 NSAIDs:Mechanismofaction
http://www.uptodate.com/contents/nsaidsmechanismofaction?topicKey=RHEUM%2F7989&elapsedTimeMs=0&source=search_result&searchTerm=aine 7/18
324:1716.4. AbramsonSB,WeissmannG.Themechanismsofactionofnonsteroidalantiinflammatorydrugs.Arthritis
Rheum198932:1.5. MeadeEA,SmithWL,DeWittDL.Differentialinhibitionofprostaglandinendoperoxidesynthase
(cyclooxygenase)isozymesbyaspirinandothernonsteroidalantiinflammatorydrugs.JBiolChem1993268:6610.
6. DeWittDL,MeadeEA,SmithWL.PGHsynthaseisoenzymeselectivity:thepotentialforsafernonsteroidalantiinflammatorydrugs.AmJMed199395:40S.
7. DeWittDL,elHarithEA,KraemerSA,etal.Theaspirinandhemebindingsitesofovineandmurineprostaglandinendoperoxidesynthases.JBiolChem1990265:5192.
8. ShimokawaT,SmithWL.Prostaglandinendoperoxidesynthase.Theaspirinacetylationregion.JBiolChem1992267:12387.
9. ShimokawaT,SmithWL.Essentialhistidinesofprostaglandinendoperoxidesynthase.His309isinvolvedinhemebinding.JBiolChem1991266:6168.
10. ShimokawaT,KulmaczRJ,DeWittDL,SmithWL.Tyrosine385ofprostaglandinendoperoxidesynthaseisrequiredforcyclooxygenasecatalysis.JBiolChem1990265:20073.
11. TohH.ProstaglandinendoperoxidesynthasecontainsanEGFlikedomain.FEBSLett1989258:317.12. ChandrasekharanNV,DaiH,RoosKL,etal.COX3,acyclooxygenase1variantinhibitedby
acetaminophenandotheranalgesic/antipyreticdrugs:cloning,structure,andexpression.ProcNatlAcadSciUSA200299:13926.
13. LeeSH,SoyoolaE,ChanmugamP,etal.Selectiveexpressionofmitogeninduciblecyclooxygenaseinmacrophagesstimulatedwithlipopolysaccharide.JBiolChem1992267:25934.
14. DuboisRN,AbramsonSB,CroffordL,etal.Cyclooxygenaseinbiologyanddisease.FASEBJ199812:1063.
15. O'BanionMK,WinnVD,YoungDA.cDNAcloningandfunctionalactivityofaglucocorticoidregulatedinflammatorycyclooxygenase.ProcNatlAcadSciUSA199289:4888.
16. SchwabJM,SchluesenerHJ,LauferS.COX3:justanotherCOXorthesolitaryelusivetargetofparacetamol?Lancet2003361:981.
17. MorhamSG,LangenbachR,LoftinCD,etal.Prostaglandinsynthase2genedisruptioncausessevererenalpathologyinthemouse.Cell199583:473.
18. DinchukJE,CarBD,FochtRJ,etal.RenalabnormalitiesandanalteredinflammatoryresponseinmicelackingcyclooxygenaseII.Nature1995378:406.
19. LangenbachR,MorhamSG,TianoHF,etal.Prostaglandinsynthase1genedisruptioninmicereducesarachidonicacidinducedinflammationandindomethacininducedgastriculceration.Cell199583:483.
20. GilroyDW,ColvilleNashPR,WillisD,etal.Induciblecyclooxygenasemayhaveantiinflammatoryproperties.NatMed19995:698.
21. IiguezMA,PunznC,FresnoM.Inductionofcyclooxygenase2onactivatedTlymphocytes:regulationofTcellactivationbycyclooxygenase2inhibitors.JImmunol1999163:111.
22. MizunoH,SakamotoC,MatsudaK,etal.Inductionofcyclooxygenase2ingastricmucosallesionsanditsinhibitionbythespecificantagonistdelayshealinginmice.Gastroenterology1997112:387.
23. ReuterBK,AsfahaS,BuretA,etal.Exacerbationofinflammationassociatedcolonicinjuryinratthroughinhibitionofcyclooxygenase2.JClinInvest199698:2076.
24. NewberryRD,StensonWF,LorenzRG.Cyclooxygenase2dependentarachidonicacidmetabolitesareessentialmodulatorsoftheintestinalimmuneresponsetodietaryantigen.NatMed19995:900.
25. RothSH.NSAIDgastropathy.Anewunderstanding.ArchInternMed1996156:1623.26. PatrignaniP,PanaraMR,GrecoA,etal.Biochemicalandpharmacologicalcharacterizationofthe
cyclooxygenaseactivityofhumanbloodprostaglandinendoperoxidesynthases.JPharmacolExpTher1994271:1705.
27. GlaserK,SungML,O'NeillK,etal.EtodolacselectivelyinhibitshumanprostaglandinG/Hsynthase2(PGHS2)versushumanPGHS1.EurJPharmacol1995281:107.
28. MitchellJA,AkarasereenontP,ThiemermannC,etal.Selectivityofnonsteroidalantiinflammatorydrugsas
-
14/7/2015 NSAIDs:Mechanismofaction
http://www.uptodate.com/contents/nsaidsmechanismofaction?topicKey=RHEUM%2F7989&elapsedTimeMs=0&source=search_result&searchTerm=aine 8/18
inhibitorsofconstitutiveandinduciblecyclooxygenase.ProcNatlAcadSciUSA199390:11693.29. BombardierC,PelosoPM,GoldsmithCH.Salsalate,anonacetylatedsalicylate,isasefficaciousas
diclofenacinpatientswithrheumatoidarthritis.SalsalateDiclofenacStudyGroup.JRheumatol199522:617.
30. MarcusAJ.Aspirinasprophylaxisagainstcolorectalcancer.NEnglJMed1995333:656.31. RothSH,ShainhouseJZ.Efficacyandsafetyofatopicaldiclofenacsolution(pennsaid)inthetreatmentof
primaryosteoarthritisoftheknee:arandomized,doubleblind,vehiclecontrolledclinicaltrial.ArchInternMed2004164:2017.
32. HaroutiunianS,DrennanDA,LipmanAG.TopicalNSAIDtherapyformusculoskeletalpain.PainMed201011:535.
33. MakrisUE,KohlerMJ,FraenkelL.Adverseeffectsoftopicalnonsteroidalantiinflammatorydrugsinolderadultswithosteoarthritis:asystematicliteraturereview.JRheumatol201037:1236.
34. DazGonzlezF,GonzlezAlvaroI,CampaneroMR,etal.PreventionofinvitroneutrophilendothelialattachmentthroughsheddingofLselectinbynonsteroidalantiinflammatorydrugs.JClinInvest199595:1756.
35. Doestheacetylgroupofaspirincontributetotheantiinflammatoryefficacyofsalicylicacidinthetreatmentofrheumatoidarthritis?TheMulticenterSalsalate/AspirinComparisonStudyGroup.JRheumatol198916:321.
36. StevensonDD,HoughamAJ,SchrankPJ,etal.Salsalatecrosssensitivityinaspirinsensitivepatientswithasthma.JAllergyClinImmunol199086:749.
37. AminAR,VyasP,AtturM,etal.Themodeofactionofaspirinlikedrugs:effectoninduciblenitricoxidesynthase.ProcNatlAcadSciUSA199592:7926.
38. HawkeyCJ.Futuretreatmentsforarthritis:newNSAIDs,NONSAIDs,ornoNSAIDs?Gastroenterology1995109:614.
39. GoldfineAB,FonsecaV,JablonskiKA,etal.Theeffectsofsalsalateonglycemiccontrolinpatientswithtype2diabetes:arandomizedtrial.AnnInternMed2010152:346.
40. LuX,XieW,ReedD,etal.Nonsteroidalantiinflammatorydrugscauseapoptosisandinducecyclooxygenasesinchickenembryofibroblasts.ProcNatlAcadSciUSA199592:7961.
41. PasrichaPJ,BediA,O'ConnorK,etal.Theeffectsofsulindaconcolorectalproliferationandapoptosisinfamilialadenomatouspolyposis.Gastroenterology1995109:994.
42. LynchPM,AyersGD,HawkE,etal.Thesafetyandefficacyofcelecoxibinchildrenwithfamilialadenomatouspolyposis.AmJGastroenterol2010105:1437.
43. ArberN,EagleCJ,SpicakJ,etal.Celecoxibforthepreventionofcolorectaladenomatouspolyps.NEnglJMed2006355:885.
44. BertagnolliMM,EagleCJ,ZauberAG,etal.Celecoxibforthepreventionofsporadiccolorectaladenomas.NEnglJMed2006355:873.
Topic7989Version12.0
-
14/7/2015 NSAIDs:Mechanismofaction
http://www.uptodate.com/contents/nsaidsmechanismofaction?topicKey=RHEUM%2F7989&elapsedTimeMs=0&source=search_result&searchTerm=aine 9/18
GRAPHICS
Orallyavailablenonopioidanalgesicandnonsteroidalantiinflammatorydrugs(NSAIDs):Usualdosingforadultswithpainorinflammation
Drug
Optionalinitialloadingdose
Usualanalgesic
dose(oral)
Maximumdoseper
day(mg)
Selectedcharacteristicsand
roleintherapy
Paraaminophenolderivative
Acetaminophen*(paracetamol,APAP)
None 325to650mgevery4to6hours,or
1000mgevery6hoursuptothreetimesperday
3000mg Effectivefornoninflammatorypainmaybeopioidsparing.Doses
-
14/7/2015 NSAIDs:Mechanismofaction
http://www.uptodate.com/contents/nsaidsmechanismofaction?topicKey=RHEUM%2F7989&elapsedTimeMs=0&source=search_result&searchTerm=aine 10/18
NSAIDagents
AppliestoallnonselectiveNSAIDs:Effectivefortreatmentofacuteandchronicpainfulandinflammatoryconditions.Maydecreaseopioidrequirements.ShorttomoderateactingNSAIDs(eg,naproxen,ibuprofen)arepreferredformostpatients.Doseandagerelatedriskofgastropathy.Maycauseorworsenrenalimpairment.NonselectiveNSAIDsreversiblyinhibitplateletfunctioningandcanaltercardioprotectiveeffectsofaspirin.AvoidNSAIDsinpatientswithrenalinsufficiency(CrCl
-
14/7/2015 NSAIDs:Mechanismofaction
http://www.uptodate.com/contents/nsaidsmechanismofaction?topicKey=RHEUM%2F7989&elapsedTimeMs=0&source=search_result&searchTerm=aine 11/18
cholinemagnesiumtrisalicylateandsalsalate2000mg.Relativelyslowonset.500mgdoseofdiflunisalhasacomparableanalgesiceffectwith650mgacetaminophenoraspirin.
Salsalate 1500mg 750to1000mgevery8to12hours
3000mg
Propionicacids(phenylpropionicacid)
Naproxen* 500mg(naproxenbase)
550mg(naproxensodium)
250to500mgevery12hours(naproxenbase)
275to550mgevery12hours(naproxensodium)
1250mgacute,1000mgchronic(naproxenbase)
1375mgacute,1100mgchronic(naproxensodium)
AgoodchoicefortreatmentofacuteorchronicpainandinflammationinmostpatientsifNSAIDtherapyisindicated.Highdoses(eg,500mgtwicedaily)mayhavelesscardiovasculartoxicitythancomparabledosesofotherNSAIDs.Forthetreatmentofrheumatologicdisorders,totaldailydosemaybeincreasedtoamaximumof1500mgbase(1650mgnaproxensodium)whenneeded.Naproxensodiumhasmorerapidabsorptionandonsetofeffectthannaproxenbase.
Ibuprofen* 1600mg 400mgevery4to6hours
3200mg(acute),2400mg(chronic)
200to400mgdosehasacomparableanalgesiceffectwith650mgacetaminophenoraspirin.Shortdurationofeffect.Usefulalternativetonaproxeninpatientswithoutcardiovascularrisks.
Ketoprofen 100mg 50mgevery6hoursor75mgevery8hours
300mg 25mgdosehasacomparableanalgesiceffectto400mgibuprofen.
-
14/7/2015 NSAIDs:Mechanismofaction
http://www.uptodate.com/contents/nsaidsmechanismofaction?topicKey=RHEUM%2F7989&elapsedTimeMs=0&source=search_result&searchTerm=aine 12/18
Shortdurationofeffect.
Flurbiprofen 100mg 50to100mgevery6to12hours
300mg Lozengepreparationavailableinsomecountries.
Oxaprozin None 1200mgoncedaily
26mg/kgupto1800mg(whicheverislower)
Longdurationofeffect.
Aceticacids(pyranoindoleaceticacid)
Diclofenac 75or100mg
50mgevery8hours
150mg
Approvedmaximumdailydoseinsomecountriesis100mg
Diclofenacisalsoavailableasatopicalpatch,solution,andgelfortreatmentofmusculoskeletalpainandosteoarthritisofsuperficialjoints,whichmaybeusefulincombinationwithorasanalternativetosystemicNSAIDs.RefertoUpToDatereviewofinitialtreatmentofosteoarthritisandseparatetable.InteractswithdrugsthatarestronginhibitorsorinducersofCYP2C9drugmetabolismuseLexiInteracttodeterminespecificinteractions.
Etodolac 400to600mg
Immediaterelease:200to400mgevery6to8hours
Extendedrelease:400to1000mgoncedaily
Immediaterelease:1000mg
Extendedrelease:1200mg
RelativelyCOX2selectiveatlowertotaldailydoseof600to800mg.200mgdosehasacomparableanalgesiceffectwith400mgofibuprofen.
Indomethacin 75mg Immediaterelease:25to50mgevery8to12hours
Controlledrelease:75
150mg Usefulfortreatmentofacutegoutandspecifictypesofheadache.Potentinhibitoryeffectsonrenalprostaglandinsynthesis.Morefrequently
-
14/7/2015 NSAIDs:Mechanismofaction
http://www.uptodate.com/contents/nsaidsmechanismofaction?topicKey=RHEUM%2F7989&elapsedTimeMs=0&source=search_result&searchTerm=aine 13/18
mgonceortwicedaily
associatedwithCNSsideeffects(eg,headache)comparedwithotherNSAIDs.Carefullyselectandmonitorpatientstoreduceriskofrenalandcardiovasculartoxicities.
Tolmetin 600mg 400to600mgevery8hours
1800mg
Sulindac 300mg 150to200mgevery12hours
400mg Morefrequentlyassociatedwithhepaticinflammation(idiosyncraticorwithfeaturesofhypersensitivity)comparedwithotherNSAIDs.SulindacmetabolitesimplicatedintheformationofrenalcalculirefertotopicreviewofnonselectiveNSAIDadverseeffects.Prescribingshouldbelimitedtospecialistswithexperienceintreatmentofchronicpainandinflammation.
Oxicams(enolicacids)
Meloxicam 7.5mg 7.5to15mgoncedaily
15mg Longdurationofeffectslowonset.RelativelyCOX2selectiveandminimaleffectonplateletfunctionatlowertotaldailydoseof7.5mg.Rarelyassociatedwithseriouscutaneousallergicreactions,includingStevensJohnsonsyndrome.
Piroxicam 10mg 10to20mgoncedaily
20mg Alongactingoptionfortreatmentofchronicpainandinflammationpoorly
-
14/7/2015 NSAIDs:Mechanismofaction
http://www.uptodate.com/contents/nsaidsmechanismofaction?topicKey=RHEUM%2F7989&elapsedTimeMs=0&source=search_result&searchTerm=aine 14/18
responsivetootherNSAIDs.Dailydoses20mgincreaseriskofseriousGIcomplications.Concurrentpharmacologicgastroprotectionissuggested.Rarelyassociatedwithseriouscutaneousallergicreactions,includingStevensJohnsonsyndrome.Prescribingshouldbelimitedtospecialistswithexperienceintreatmentofchronicpainandinflammation.
Fenamates(anthranilicacids)
Meclofenamate(meclofenamicacid)
150mg 50mgevery4to6hours
400mg AlternateNSAIDchoicefortreatmentofacuteorchronicpain,inflammation,anddysmenorrhea.AppearstobeassociatedwithhigherincidenceofGIdisturbance(includingdiarrhea)comparedwithothernonselectiveNSAIDs.
Mefenamicacid
500mg 250mgevery6hours
1000mg AlternateNSAIDchoicefortreatmentofacutepainanddysmenorrhea.Durationofusenottoexceedsevendays(acutepain)orthreedays(dysmenorrhea).Antiinflammatoryefficacyiscomparativelylow.Notindicatedfortreatmentofchronicpainorinflammation.
Nonacidic(naphthylalkanone)
Nabumetone 1000mg 500to750mgevery8to12hours
2000mg Moderatedurationofeffectslowonset.RelativelyCOX2
-
14/7/2015 NSAIDs:Mechanismofaction
http://www.uptodate.com/contents/nsaidsmechanismofaction?topicKey=RHEUM%2F7989&elapsedTimeMs=0&source=search_result&searchTerm=aine 15/18
or1000to1500mgoncedaily
selectiveatlowertotaldailydoseof1000mgorless.Minimaleffectonplateletfunctionattotaldailydoseof1000mgorless.
SelectiveCOX2inhibitors
Celecoxib 400mg 200mgdailyor100mgevery12hours
400mg RelativereductioninGItoxicitycomparedwithnonselectiveNSAIDs.Noeffectonplateletfunction.CardiovascularandrenalrisksaredoserelatedandappearsimilartothoseofnonselectiveNSAIDs.Patientswithindicationsforcardioprotectionrequireaspirinsupplementindividualsmayrequireconcurrentgastroprotection.
Etoricoxib(notavailableinUnitedStates)
None 30to60mgoncedaily
60mg(chronicpainandinflammation)
120mg(acutepainforuptoeightdays)
Maybeassociatedwithmorefrequentandseveredoserelatedcardiovasculareffects(eg,hypertension)comparedwithnonselectiveandotherCOX2selectiveNSAIDs.Otherwise,risksandbenefitsaswithcelecoxib(seeabove).
GI:gastrointestinalINR:internationalnormalizedratioCNS:centralnervoussystemCYP450:cytochromeP450OTC:overthecounter,availablewithoutprescriptionCrCl:creatinineclearanceCOX2:cyclooxygenaseisoform2NSAID:nonsteroidalantiinflammatorydrugSSRIs:selectiveserotoninreuptakeinhibitors.*AvailablewithoutaprescriptionintheUnitedStates.AlistofCYP450inducingdrugsisavailableseparatelyinUpToDate.NSAIDsmayinteractwithaspirin,warfarin,methotrexate,antihypertensives,serotoninreuptakeinhibitorantidepressants(eg,SSRIs,cyclicantidepressants,venlafaxine),andotherdrugs.Forspecificinteractions,usetheLexiInteractprogramincludedwithUpToDate.RefertotheUpToDatetopiconthecardiovasculareffectsofnonselectiveNSAIDs.Foradditionalinformationongastroprotectivestrategies,includingselectiveCOX2inhibitorsandotheroptions,refertotheUpToDatetopicsontheoverviewofselectiveCOX2inhibitorsandonNSAIDs(includingaspirin)andtheprimarypreventionofgastroduodenaltoxicity.
-
14/7/2015 NSAIDs:Mechanismofaction
http://www.uptodate.com/contents/nsaidsmechanismofaction?topicKey=RHEUM%2F7989&elapsedTimeMs=0&source=search_result&searchTerm=aine 16/18
Preparedwithdatafrom:1. Anon.Drugsforpain.TreatmentguidelinesfromtheMedicalLetter2013.11:31.2. CastellsagueJ,RieraGuardiaN,CalingaertB,etal.IndividualNSAIDsanduppergastrointestinal
complications:Asystematicreview.DrugSaf201235:1127.3. LexicompOnline.Copyright19782015Lexicomp,Inc.AllRightsReserved.
Graphic70067Version34.0
-
14/7/2015 NSAIDs:Mechanismofaction
http://www.uptodate.com/contents/nsaidsmechanismofaction?topicKey=RHEUM%2F7989&elapsedTimeMs=0&source=search_result&searchTerm=aine 17/18
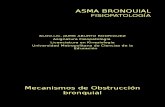
Prostaglandinandthromboxanesynthesis
Schematicrepresentationofprostaglanginsynthesispathwayswithenzymesthatcatalyzespecificreactions.Ofnote,plateletsonlyexpresscyclooxygenase(COX)1.RefertoUpToDatetopicsonnonsteroidalantiinflammatorydrugs,antiplateletdrugs,cyclooxygenaseinhibitors,andspecificdiseasestatesforfurtherdetails.
PG:prostaglandinTx:thromboxane.
Graphic66146Version7.0
-
14/7/2015 NSAIDs:Mechanismofaction
http://www.uptodate.com/contents/nsaidsmechanismofaction?topicKey=RHEUM%2F7989&elapsedTimeMs=0&source=search_result&searchTerm=aine 18/18
Disclosures:DanielHSolomon,MD,MPHGrant/Research/ClinicalTrialSupport:Amgen[osteoporosis].GrantSupport:Lilly[RA]Pfizer[RA]AstraZeneca[gout].TrialExec.Committee:Pfizer[NSAID(celecoxib)].DanielEFurst,MDGrant/Research/ClinicalTrialSupport:AbbVie[RA,IBD,PMS,PsA(adalimumab)]Actelion[SSc(bosentan,macitentan)]Amgen[RA,IBP,AS,PsA(etanercept)]BMS[RA,SSc(abatacept)]Gilead[SSc(ambresentan)]GSKNIHNovartisPfizer[SSc(sildenafil)]Roche/Genentech[RA,IBD,AS,SSc(rituxan,tocilizumab)]UCB[RA,IBD,AS(certolizumab)].Speaker'sBureau:AbbVie[RA,IBD,PMS,PsA(adalimumab)]Actelion[SSc(bosentan,macitentan)]UCB[RA,IBD,AS(certolizumab)].Consultant/AdvisoryBoards:AbbVie[RA,IBD,PMS,PsA(adalimumab)]Actelion[SSc(bosentan,macitentan)]Amgen[RA,IBP,AS,PsA(etanercept)]BMS[RA,SSc(abatacept)]Cytori[labtestadvisory]Gilead[SSc(ambresentan)]GSKNIHNovartisPfizer[SSc(sildenafil)]Janssen[RA,IBD(infliximab)]NIHNovartisPfizer[SSc(sildenafil)]Roche/Genentech[RA,IBD,AS,SSc(rituxan,tocilizumab)]UCB[RA,IBD,AS(certolizumab)].PaulLRomain,MDNothingtodisclose.Contributordisclosuresarereviewedforconflictsofinterestbytheeditorialgroup.Whenfound,theseareaddressedbyvettingthroughamultilevelreviewprocess,andthroughrequirementsforreferencestobeprovidedtosupportthecontent.AppropriatelyreferencedcontentisrequiredofallauthorsandmustconformtoUpToDatestandardsofevidence.Conflictofinterestpolicy
Disclosures


















