
Lake Stevens School District · Lake Stevens School District ... free of charge, when you need...
12
Lake Stevens School District Student Enrollment Registration Checklist The following registration items must be completed in order to register your child with Lake Stevens School District. Student Registration Form Copy of Birth Certificate (proof of age and legal name) Proof of Guardianship (if student lives with adult other than parent) Proof of Residence (i.e. property tax statement, utility bill, lease or rental agreement) Home Language Survey Release of Information Form Certificate of Immunization Status (CIS Form) All dates must be transferred to the CIS form, including signature and date by guardian. Q&A with additional information is also available on the district website under “Health Services.” Student Emergency Contact/Alert Form Student Health History Form If your child has a life-threatening condition (i.e. asthma, diabetes, anaphylaxis, seizure, hemophilia) you must contact your school nurse for an appropriate care plan. These documents are also available on the district website under Health Services. Student Residency Questionnaire (McKinney-Vento) Electronic Information Systems Consent Form www.lkstevens.wednet.edu Rev 1/2018
Transcript of Lake Stevens School District · Lake Stevens School District ... free of charge, when you need...

Lake Stevens School District Student Enrollment Registration Checklist
The following registration items must be completed in order to register your child with Lake Stevens School District.
Student Registration Form
Copy of Birth Certificate (proof of age and legal name)
Proof of Guardianship (if student lives with adult other than parent)
Proof of Residence (i.e. property tax statement, utility bill, lease or rental agreement)
Home Language Survey
Release of Information Form
Certificate of Immunization Status (CIS Form) All dates must be transferred to the CIS form, including signature and date by guardian. Q&A with additional information is also available on the district website under “Health Services.”
Student Emergency Contact/Alert Form
Student Health History Form If your child has a life-threatening condition (i.e. asthma, diabetes, anaphylaxis, seizure, hemophilia) you must contact your school nurse for an appropriate care plan. These documents are also available on the district website under Health Services.
Student Residency Questionnaire (McKinney-Vento)
Electronic Information Systems Consent Form
www.lkstevens.wednet.edu Rev 1/2018

LAKE STEVENS STUDENT REGISTRATION FORM SCHOOL DISTRICT
Date: _________________________
OFFICE USE ONLY
Staff Initials Student ID: Entry Date: Legal Name Verified? Birth Cert Other Legal Doc
LSSD District Resident? Yes No Non-Resident Home District: Verified Waiver? Yes No
Has your child or a sibling ever been registered in the Lake Stevens School District? Yes No If yes, which school?
STU
DEN
T IN
FO STUDENT NAME
Birthdate (Month/Day/Year)
/ /
Birth Certificate? Yes No
Legal LAST Name
Gender Male
Female Migrant? Yes No
Grade
Date Entered USA: (Month/Day/Year)
/ /
Legal FIRST Name Legal MIDDLE Name
Birthplace (City, State, County, Country)
Military Family—Student has a parent/guardian who is a member of the: Active Duty Armed Forces Reserves of the Armed Forces Washington National Guard More than one parent/guardian is a member of any of the above
PR
IMA
RY
HO
USE
HO
LD
SEC
ON
D H
OU
SEH
OLD
PRIMARY PARENT/GUARDIAN INFORMATION (Household where student resides the majority of the time) Legal Parent/Guardian #1 Last Name
Primary Phone Please check if confidential (will not be published) Second Phone Third Phone ( ) ( ) ( ) Home Work Mobile Home Work Mobile Home Work Mobile Email
Relation to Student: Father Mother Guardian Other:
First Name
Parent/Guardian #2 Last Name First Name
Email Second Phone Third Phone ( ) ( ) Home Work Mobile Home Work Mobile
Relation to Student: Father Mother Guardian Stepmother Stepfather Other:
Resident Street Address Apt # City State Zip
Mailing Address (If different From above) Apt # PO Box City State Zip
SECOND HOUSEHOLD INFORMATION (Student does not primarily reside at this residence) Parent/Guardian #1 Last Name
Primary Phone Please check if confidential (will not be published) Second Phone Third Phone ( ) ( ) ( ) Home Work Mobile Home Work Mobile Home Work Mobile Email
Relation to Student: Father Mother Guardian Other:
First Name
Parent/Guardian #2 Last Name First Name
Email: Second Phone Third Phone ( ) ( ) Home Work Mobile Home Work Mobile
Relation to Student: Father Mother Guardian Stepmother Stepfather Other: Resident Address Street Apt City State Zip
Mailing Address (If different From above) Apt # PO Box City State Zip
PLEASE LIST OTHER SIBLINGS CURRENTLY ATTENDING LAKE STEVENS SCHOOL DISTRICT
Last Name First Name School Grade
Lake Stevens School District Student Registration Form Revised: 2/26/2016

STU
DEN
T H
ISTO
RY
Name of school student last attended ______________________________ District _________________________ City_________________________ State ________
Has your child ever been retained? Yes No If yes, at what grade level(s)? _________________________
Has your child ever received services in any of the following programs? Check all applicable programs.
Special Education/IEP for: ________________________ 504 Plan for: __________________________ OT/PT Fine/Gross Motor Highly Capable
ELL Speech/Language Title 1/LAP Services Behavior Services Counseling (inside/outside school), Social Skills (i.e. Friendship Group)
Does your child have any past, current, or pending disciplinary actions or any history of violent behavior? Yes No Date ______________________________
Is your child presently on suspension or expulsion from another school? Yes No If yes, reason __________________________________________________
Do you work or reside on Federal Land? Yes No
Is there a joint-custody or parenting plan in effect? Yes No
Is there a restraining order against anyone pertaining to your student? Yes No (If yes, most recent certified legal papers must be on file with the
School). Restraining order is against Name(s)___________________________________________________________________________________________________
Ethnicity and Race School districts in Washington State are required to report student data by ethnicity and race categories to the state’s Office of Superintendent of Public Instruction. Ethnicity and race categories used in our district are the same as used in all Washington school districts. They are set by the federal government, the Washington State Legislature, and the state Superintendent of Public Instruction.
Please complete BOTH sections below: 1. Is your child of Hispanic or Latino origin?
No, my child is not Hispanic or Latino
Yes, my Child is Hispanic or Latino - (Check all that apply): Cuban Puerto Rican South American Dominican Mexican/Mexican American/Chicano Latin American Spaniard Central American Other Hispanic/Latino
2. What race do you consider your child? (Check at least one selection).
African American or Black Thai Colville Samish White or Caucasian Vietnamese Cowlitz Sauk-Suiattle Asian Indian Other Asian Hoh Shoalwater Bay Cambodian Native Hawaiian Jamestown S’Klallam Skokomish Chinese Fijian Kalispel Snoqualmie Filipino Guamanian or Chamorro Lower Elwa Klallam Spokane Hmong Mariana Islander Lummi Squaix Island Indonesian Melanesian Makah Stillaguamish Japanese Micronesian Muckleshoot Suquamish Korean Samoan Nisqually Swinomish Laotian Tongan Nooksack Tulalip Malaysian Other Pacific Islander Port Gamble S’Klallam Yakama Pakistani Alaska Native Puyallup Other Washington Indian Singaporean Chehalis Quileute Tribe
Taiwanese Quinault Other American Indian/Alaska Native
RESIDENCE VERIFICATION Please provide the information requested below so that we may legally enroll your child in the Lake Stevens School District. Lake Stevens School District may ONLY enroll students whose Parent(s) or Guardian(s) reside within school district boundaries, unless an Inter-district Transfer form has been ACCEPTED by our district prior to enrollment. Residency verification is a parent responsibility and falsification of information provided on this document will be grounds for immediate cancellation of enrollment.
In order to verify the address listed (on the front page of this form), we require one of the following be provided for review upon initial registration or at any time during enrollment when a home address changes).
Property Tax Statement Utility Bill (must show parent/guardian name, address < 30 days old) Rent Receipt(s) Residential Building Permit (with completion date) Lease or Rental Agreement (specifying date of occupancy within 30 days)
REL
EASE
A
UTH
OR
IZA
TIO
N Please Check Yes or No
Emergency Medical Authorization – In the event parent/guardian cannot be reached, I authorize school authorities to obtain emergency care for my child. Yes No
Student Release – In the event parent/guardian cannot be reached, I authorize school authorities to release my child to the persons designated on my child’s Emergency Contacts form. Yes No
“I declare under penalty of perjury under the laws of the State of Washington that the foregoing is true and correct. I understand that falsification of information to achieve enrollment or assignment may be cause for revocation of the student’s enrollment in Lake Stevens School District.”
Legal Parent/ Guardian Signature __________________________________________________ Date _____________
Lake Stevens School District Student Registration Form Revised: 2/26/2016

English/November 2016
Office of Superintendent of Public Instruction (OSPI)
Home Language Survey
The Home Language Survey is given to all students enrolling in Washington schools.
Student Name: Grade: Date:
Parent/Guardian Name Parent/Guardian Signature
Right to Translation and All parents have the right to information about their child’s Interpretation Services education in a language they understand. Indicate your language preference so
we can provide an interpreter or 1. In what language(s) would your family prefer to communicate translated documents, free of with the school? charge, when you need them. __________________________________
Eligibility for Language
Development Support
Information about the student’s
language helps us identify students
who qualify for support to develop
the language skills necessary for
success in school. Testing may be
necessary to determine if language
supports are needed.
(Registrar: Profile tab,2. What language did your child learn first? Language & Native Language) __________________________________
3. What language does your child use the most at home? (Registrar: Profile tab, Home __________________________________ Language)
4. What is the primary language used in the home, regardless of (Registrar: Family tab, Home Language)the language spoken by your child?
__________________________________
5. Has your child received English language development support
in a previous school? Yes___ No___ Don’t Know___
Prior Education
Your responses about your child’s
birth country and previous
education:
Give us information about the
knowledge and skills your child is
bringing to school.
May enable the school district to
receive additional federal funding
to provide support to your child.
This form is not used to identify
students’ immigration status.
6. In what country was your child born? ___________________
7. Has your child ever received formal education outside of the
United States? (Kindergarten – 12th grade) ____Yes ____No
If yes: Number of months: ______________
Language of instruction: ______________
8. When did your child first attend a school in the United States? (Kindergarten – 12th grade)
_______________________
Month Day Year
Thank you for providing the information needed on the Home Language Survey. Contact your school
district if you have further questions about this form or about services available at your child’s school.
Note to district: This form is available in multiple languages on http://www.k12.wa.us/MigrantBilingual/HomeLanguage.aspx. A response that includes a language other than English to question #2 OR question #3 triggers English language proficiency placement testing. Responses to questions #1 or #4 of a language other than English could prompt further conversation with the family to ensure that #2 and #3 were clearly understood. ”Formal education” in #7 does not include refugee camps or other unaccredited educational programs for children.
Forms and Translated Material from the Bilingual Education Office of the Office of Superintendent of Public Instruction are licensed under a Creative
Commons Attribution 4.0 International License.

Dear Lake Stevens Families:
The mission of Lake Stevens School District is to help students become contributing members of society and lifelong learners. We are proud of our students—they are doing remarkable things, and we love to tell their stories and highlight their successes. One of the ways we do this is through the sharing of photos, videos and classwork. This information is shared internally, throughout the community, in presentations, online and with the media for television, newspaper and radio coverage.
Most information about our students is confidential and cannot be made public without the consent of parents/guardians. However, the Federal Family Educational Rights and Privacy Act (FERPA) allows each student’s “directory information” to be released without specific consent from parents. Directory information, which is generally not considered harmful or an invasion of privacy if released, includes: the student’s name, photograph, address, telephone number, date and place of birth, dates of attendance, participation in officially recognized sports and activities, weight and height of members of athletic teams, diplomas and awards received and the most recent previous school attended.
Lake Stevens School District (LSSD) will release directory information upon request to law enforcement and Child Protective Services without the consent of parents. LSSD does not release directory information for commercial use.
If you do not want directory information released about your child, please complete section A on the next page. The choices made on this form will remain on your student’s record as long as he/she is enrolled in Lake Stevens School District, or until a new form is submitted. You have the right to make changes to this form at any time. If no form is on file, permission for the release of directory information is granted. For more information, please review Board Policy 5230: Student Records.
Additionally, the Federal Elementary and Secondary Education Act requires high schools to provide military recruiters and higher education institutions with a list of student names, addresses and phone numbers. Parents have the right to request that their child’s name be omitted from that list. If you do not want directory information released to military or college recruiters, please complete section B on the next page.
For questions or more information, contact the district’s Communications Department at 425-335-1501.
Warm Regards,
Amy Beth Cook, Ed.D. Superintendent Lake Stevens School District

Request to Restrict Release of Information
If you do not want directory information released about your child, or if you do not want information about your child released to military or college recruiters, complete this form and return it to your child’s school. A separate form must be completed for each child. If this form is not returned, your permission to release information is implied. This form supersedes any prior permissions or restrictions. If your preferences change, you are responsible for completing a new form and submitting it to your child’s school.
SECTION A: Directory Information and Student Images Directory information is defined as the student’s name, address, telephone number, photograph, date and place of birth, dates of attendance, participation in officially recognized activities and sports, weight and height of members of athletic teams, diplomas and awards received and the most recent previous school attended. This information can only be released to state and federal education agencies; state and local officials; organizations conducting studies for educational agencies for the purpose of improving education; persons and agencies in connection with an emergency to protect the health and safety of the student or other persons.
Do not release any of my student’s information to other institutions except where required by law.
By marking the box above, you have restricted the release of all directory information about your child—including his or her name and photo in school and district publications. This includes the yearbook, school newsletters, graduation/honor roll lists, athletic programs or PTA materials. Please note that Lake Stevens School District will still release directory information, upon request, to law enforcement and Child Protective Services.
The district uses student images and school work in a variety of ways, including Lake Schools; the district calendar; local newspapers; professional development materials; brochures; flyers; school newsletters; and on its website and social media to promote student achievement and build school spirit. The district and its schools also produce videos highlighting student successes. In addition, media often visit schools to capture events and activities.
Exception: If you would like your child’s name and photo to be included in school and district publications and in information shared with the media, mark the box below.
I agree to allow my child’s name and photograph to be included in school and district publications and in information shared with the media.
Note: If you mark both boxes, directory information will not be released to other institutions, but your child’s name and photo/likeness may be published inside and outside of the district.
SECTION B: Recruitment The United States military requests and is entitled to the names, telephone numbers and addresses of middle and high school students unless the parent/guardian restricts release of the information. Additionally, secondary schools often host college fairs and campus visits where students’ names, telephone numbers and addresses are shared with the higher education institution.
Do not release my student’s information to military recruiters.
Do not release my student’s information to college recruiters.
Name of student (please print) Name of parent or guardian (please print)
Date Parent/guardian signature
March 2016

Certificate of Immunization Status (CIS)
For Kindergarten-12th Grade / Child Care Entry
Please print. See back for instructions on how to fill out this form or get it printed from the Washington Immunization Information System.
Office Use Only: Reviewed by: Date:
Signed Cert. of Exemption on file? Yes No
Child’s Last Name: First Name: Middle Initial: Birthdate (MM/DD/YY): Sex:
____________________________________________________________________________________________________________________________________________________
I give permission to my child’s school to share immunization information with the Immunization Information System to help the school maintain my child’s school record.
______________________________________________________________ Parent/Guardian Signature Required Date
I certify that the information provided on this form is correct and verifiable.
______________________________________________________________ Parent/Guardian Signature Required Date
♦ Required for School and Child Care/Preschool Date Date Date Date Date Date ● Required Only for Child Care/Preschool MM/DD/YY MM/DD/YY MM/DD/YY MM/DD/YY MM/DD/YY MM/DD/YY
Documentation of Disease Immunity Healthcare provider use only
Required Vaccines for School or Child Care Entry
♦ DTaP, DT (Diphtheria, Tetanus, Pertussis)
♦ Tdap (Tetanus, Diphtheria, Pertussis)
♦ Td (Tetanus, Diphtheria)
♦ Hepatitis B 2-dose schedule used between ages 11-15
● Hib ( Haemophilus influenzae type b)
♦ IPV / OPV (Polio)
♦ MMR (Measles, Mumps, Rubella)
● PCV / PPSV (Pneumococcal)
♦ Varicella (Chickenpox) History of disease verified by IIS
Recommended Vaccines (Not Required for School or Child Care Entry)
Flu (Influenza)
Hepatitis A
HPV (Human Papillomavirus)
MCV, MPSV (Meningococcal)
MenB (Meningococcal)
Rotavirus
If the child named in this CIS has a history of Varicella (Chickenpox) or can show immunity by blood test (titer) it MUST be verified by a healthcare provider
I certify that the child named on this CIS has:
a verified history of Varicella (Chickenpox).
laboratory evidence of immunity (titer) to disease(s) marked below. Lab report(s) for titers MUST also be attached.
Diphtheria Mumps Other: Hepatitis A Polio __________
Hepatitis B Rubella __________
Hib Tetanus
Measles Varicella
Licensed healthcare provider signature Date (MD, DO, ND, PA, ARNP)
Printed Name

Instructions for completing the Certificate of Immunization Status (CIS): printing it from the Immunization Information System (IIS) or filling it in by hand.
To print with immunization information filled in: Ask if your healthcare provider’s office enters immunizations into the WA Immunization Information System (Washington’s statewide database). If they do, ask them to print the CIS from the IIS and your child’s immunization information will fill in automatically. You can also print a CIS at home by signing up and logging into MyIR at https://wa.myir.net. If your provider doesn’t use the IIS, email or call the Department of Health to get a copy of your child’s CIS: [email protected] or 1-866-397-0337.
To fill out the form by hand: #1 Print your child’s name, birthdate, sex, and sign your name where indicated on page one. #2 Vaccine information: Write the date of each vaccine dose received in the date columns (as MM/DD/YY). If your child receives a combination vaccine (one shot that protects against
several diseases), use the Reference Guide below to record each vaccine correctly. For example, record Pediarix under Diphtheria, Tetanus, Pertussis as DTaP, Hepatitis B as Hep B, and Polio as IPV.
#3 History of Varicella Disease: If your child had chickenpox (varicella) disease and not the vaccine, a health care provider must verify chickenpox disease to meet school requirements.
If your healthcare provider can verify that your child had chickenpox, ask your provider to check the box in the Documentation of Disease Immunity section and sign the form. If school staff access the IIS and see verification that your child had chickenpox, they will check the box under Varicella in the vaccines section.
#4 Documentation of Disease Immunity: If your child can show positive immunity by blood test (titer) and has not had the vaccine, have your healthcare provider check the boxes for the appropriate disease in the Documentation of Disease Immunity box, and sign and date the form. You must provide lab reports with this CIS.
Reference guide for vaccine abbreviations in alphabetical order For updated list, visit https://fortress.wa.gov/doh/cpir/iweb/homepage/completelistofvaccinenames.pdf Abbreviations
Full Vaccine Name
Abbreviations Full Vaccine
Name Abbreviations
Full Vaccine Name
Abbreviations Full Vaccine
Name Abbreviations Full Vaccine Name
DT Diphtheria, Tetanus Hep A Hepatitis A MCV / MCV4 Meningococcal Conjugate Vaccine
OPV Oral Poliovirus Vaccine
Tdap Tetanus, Diphtheria, acellular Pertussis
DTaP Diphtheria, Tetanus, acellular Pertussis
Hep B Hepatitis B MenB Meningococcal B PCV / PCV7 / PCV13
Pneumococcal Conjugate Vaccine
VAR / VZV Varicella
DTP Diphtheria, Tetanus, Pertussis
Hib Haemophilus influenzae type b
MPSV / MPSV4 Meningococcal Polysaccharide Vaccine
PPSV / PPV23 Pneumococcal Polysaccharide Vaccine
Flu (IIV) Influenza HPV (2vHPV / 4vHPV / 9vHPV)
Human Papillomavirus
MMR Measles, Mumps, Rubella
Rota (RV1 / RV5) Rotavirus
HBIG Hepatitis B Immune Globulin
IPV Inactivated Poliovirus Vaccine
MMRV Measles, Mumps, Rubella with Varicella
Td Tetanus, Diphtheria
Reference guide for vaccine trade tames in alphabetical order For updated list, visit https://fortress.wa.gov/doh/cpir/iweb/homepage/completelistofvaccinenames.pdf Trade Name Vaccine Trade Name Vaccine Trade Name Vaccine Trade Name Vaccine Trade Name Vaccine
ActHIB® Hib Fluarix® Flu Havrix® Hep A Menveo® Meningococcal Rotarix® Rotavirus (RV1)
Adacel® Tdap Flucelvax® Flu Hiberix® Hib Pediarix® DTaP + Hep B + IPV
RotaTeq® Rotavirus (RV5)
Afluria® Flu FluLaval® Flu HibTITER® Hib PedvaxHIB® Hib Tenivac® Td
Bexsero® MenB FluMist® Flu Ipol® IPV Pentacel® DTaP + Hib + IPV Trumenba® MenB
Boostrix® Tdap Fluvirin® Flu Infanrix® DTaP Pneumovax® PPSV Twinrix® Hep A + Hep B
Cervarix® 2vHPV Fluzone® Flu Kinrix® DTaP + IPV Prevnar® PCV Vaqta® Hep A
Daptacel® DTaP Gardasil® 4vHPV Menactra® MCV or MCV4 ProQuad® MMR + Varicella Varivax® Varicella
Engerix-B® Hep B Gardasil® 9 9vHPV Menomune® MPSV4 Recombivax HB® Hep B
If you have a disability and need this document in another format, please call 1-800-525-0127 (TDD/TTY call 711). DOH 348-013 December 2016

ELC HK GW HC HL MP SL SC LSMS NLMS CMHS LSHS
NEW STUDENT EMERGENCY CONTACTS/ALERTS SCHOOL YEAR:
Student Name: Grade: Birth Date:
Parent/Guardian Name(s):
SCHOOL CLOSURE EMERGENCY PROCEDURE
In the event of school closure during the school day (power outage, heavy falling snow, etc.), the school will
first attempt to call the parent(s) at the phone numbers provided on your student’s registration form. Please
ensure that you have provided numbers where we may reach you during daytime hours. If your child is
medically fragile, make arrangements for your child’s medical needs at school and have an emergency plan in
place. You will need to make additional contact with the school nurse for those arrangements.
AUTHORIZED EMERGENCY & RELEASE CONTACTS (Please List Contacts in Order of Preference)
In the event that a parent/guardian cannot be reached, please provide up to four additional contacts that are
authorized to pick up your student from school.
My child can only be released from school with a parent/guardian OR the following individuals:
1) Phone ( ) Relationship Family Friend
Daycare Neighbor
2) Phone ( ) Relationship Family Friend
Daycare Neighbor
3) Phone ( ) Relationship Family Friend
Daycare Neighbor
4) Phone ( ) Relationship Family Friend
Daycare Neighbor
CRITICAL ALERTS
Please list any non medical critical alerts that the school should be aware of concerning your child. Alert
information is shared with school staff on a “need to know basis” only and is considered confidential. It is the
parent’s responsibility to alert the school with critical information. Please be specific. Medical alerts need to
be recorded on the student health history form, not in this section.
LEGAL RESTRICTIONS/NO CONTACT/RESTRAINING ORDERS
Are there any legal restrictions in place regarding your student? Yes No
Restrictions are against: Name(s)
If YES, the most recent certified
legal papers must be on file
with the school.
Parent/Guardian Signature: Date:
New Student Emergency Contacts/Alerts 2/1/2013
__________________________________________________
__________________
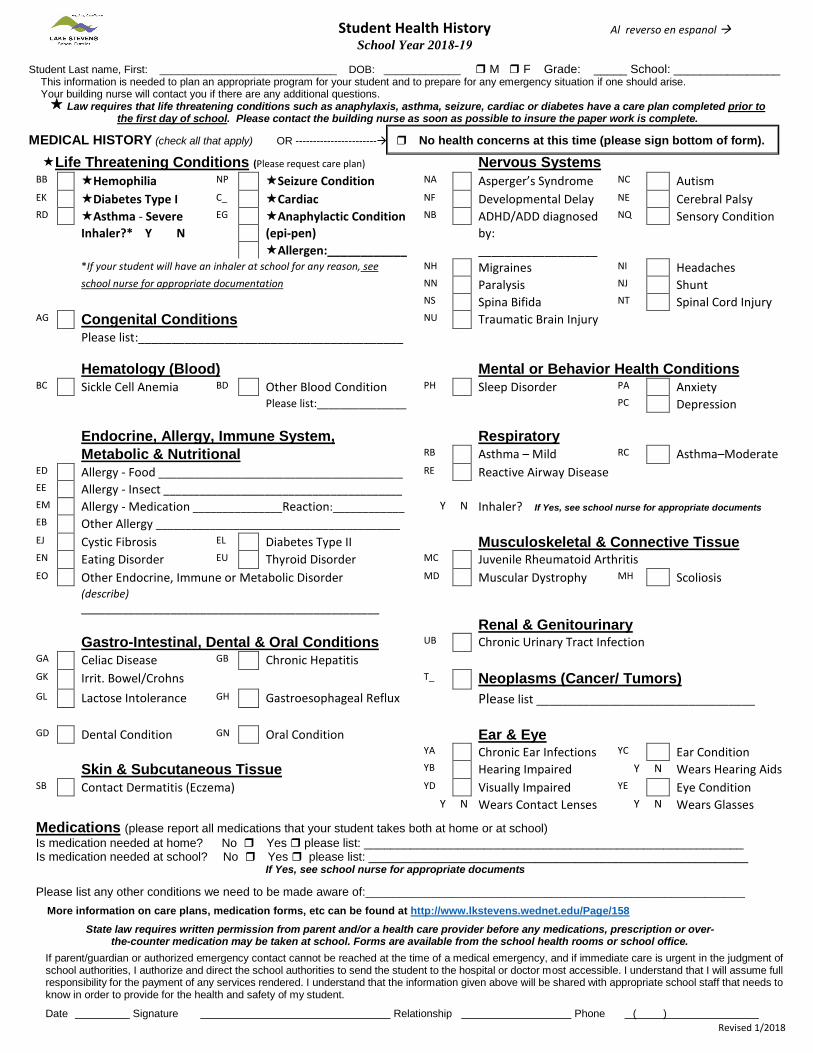
Student Health History Al reverso en espanol School Year 2018-19
Student Last name, First: ______________________________ DOB: _____________ M F Grade: _____ School: ________________ This information is needed to plan an appropriate program for your student and to prepare for any emergency situation if one should arise. Your building nurse will contact you if there are any additional questions. Law requires that life threatening conditions such as anaphylaxis, asthma, seizure, cardiac or diabetes have a care plan completed prior to
the first day of school. Please contact the building nurse as soon as possible to insure the paper work is complete.
MEDICAL HISTORY (check all that apply) OR ----------------------- No health concerns at this time (please sign bottom of form).
Life Threatening Conditions (Please request care plan) BB
EK
RD
AG
BC
ED
EE
EM
EB
EJ
EN
EO
GA
GK
GL
GD
SB
Hemophilia NP Seizure Condition Diabetes Type I C_ Cardiac
EGAsthma - Severe Anaphylactic Condition Inhaler?* Y N (epi-pen)
Allergen:____________ *If your student will have an inhaler at school for any reason, see school nurse for appropriate documentation
Congenital Conditions Please list:________________________________________
Hematology (Blood) BDSickle Cell Anemia Other Blood Condition
Please list:_______________
Endocrine, Allergy, Immune System, Metabolic & Nutritional Allergy - Food _________________________________________ Allergy - Insect ________________________________________ Allergy - Medication _______________Reaction:____________ Other Allergy _________________________________________ Cystic Fibrosis EL Diabetes Type II Eating Disorder EU Thyroid Disorder Other Endocrine, Immune or Metabolic Disorder (describe)
Gastro-Intestinal, Dental & Oral Conditions GBCeliac Disease Chronic Hepatitis
Irrit. Bowel/Crohns Lactose Intolerance GH Gastroesophageal Reflux
GNDental Condition Oral Condition
Skin & Subcutaneous Tissue Contact Dermatitis (Eczema)
NA
NF
NB
NH
NN
NS
NU
PH
RB
RE
Y N
MC
MD
UB
T_
YA
YB
YD
Y N
Nervous Systems Asperger’s Syndrome NC Autism Developmental Delay NE Cerebral Palsy ADHD/ADD diagnosed NQ Sensory Condition by:
Migraines NI Headaches Paralysis NJ Shunt Spina Bifida NT Spinal Cord Injury Traumatic Brain Injury
Mental or Behavior Health Conditions Sleep Disorder PA Anxiety
PC Depression
Respiratory RCAsthma – Mild Asthma–Moderate
Reactive Airway Disease
Inhaler? If Yes, see school nurse for appropriate documents
Musculoskeletal & Connective Tissue Juvenile Rheumatoid Arthritis Muscular Dystrophy MH
Renal & Genitourinary Chronic Urinary Tract Infection
Scoliosis
Neoplasms (Cancer/ Tumors) Please list _________________________________
Ear & Eye Chronic Ear Infections YC Ear Condition Hearing Impaired Y N Wears Hearing Aids Visually Impaired YE Eye Condition Wears Contact Lenses Y N Wears Glasses
Medications (please report all medications that your student takes both at home or at school) Is medication needed at home? No Yes please list: _________________________________________________________ Is medication needed at school? No Yes please list: _________________________________________________________
If Yes, see school nurse for appropriate documents
Please list any other conditions we need to be made aware of:_________________________________________________________ More information on care plans, medication forms, etc can be found at http://www.lkstevens.wednet.edu/Page/158
State law requires written permission from parent and/or a health care provider before any medications, prescription or over-the-counter medication may be taken at school. Forms are available from the school health rooms or school office.
If parent/guardian or authorized emergency contact cannot be reached at the time of a medical emergency, and if immediate care is urgent in the judgment of school authorities, I authorize and direct the school authorities to send the student to the hospital or doctor most accessible. I understand that I will assume full responsibility for the payment of any services rendered. I understand that the information given above will be shared with appropriate school staff that needs to know in order to provide for the health and safety of my student.
Date Signature Relationship Phone ( ) Revised 1/2018
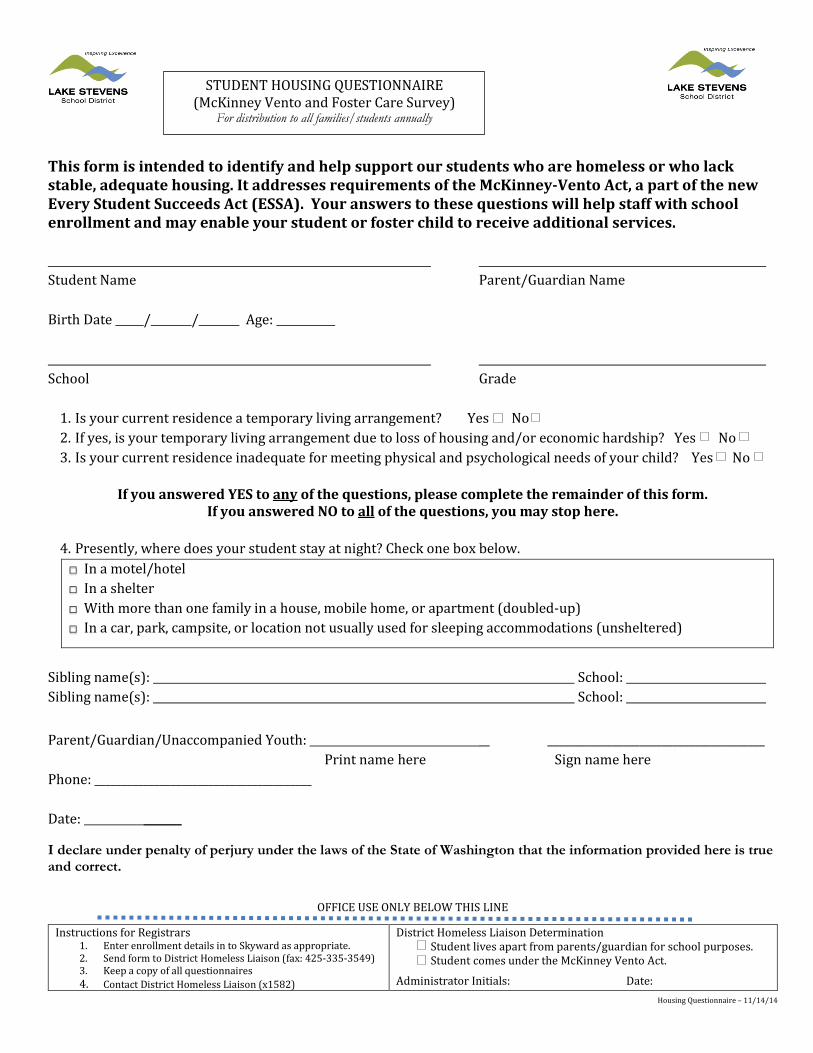
STUDENT HOUSING QUESTIONNAIRE (McKinney Vento and Foster Care Survey)
For distribution to all families/students annually
This form is intended to identify and help support our students who are homeless or who lack stable, adequate housing. It addresses requirements of the McKinney-Vento Act, a part of the new Every Student Succeeds Act (ESSA). Your answers to these questions will help staff with school enrollment and may enable your student or foster child to receive additional services.
Student Name Parent/Guardian Name
Birth Date / / Age:
School Grade
1. Is your current residence a temporary living arrangement? Yes No 2. If yes, is your temporary living arrangement due to loss of housing and/or economic hardship? Yes No 3. Is your current residence inadequate for meeting physical and psychological needs of your child? Yes No
If you answered YES to any of the questions, please complete the remainder of this form. If you answered NO to all of the questions, you may stop here.
4. Presently, where does your student stay at night? Check one box below.
□ In a car, park, campsite, or location not usually used for sleeping accommodations (unsheltered)
□ In a motel/hotel □ In a shelter □ With more than one family in a house, mobile home, or apartment (doubled-up)
Sibling name(s): School: Sibling name(s): School:
Parent/Guardian/Unaccompanied Youth: __ ________________________________________ Print name here Sign name here
Phone: ________________________________________
Date: _______
I declare under penalty of perjury under the laws of the State of Washington that the information provided here is trueand correct.
OFFICE USE ONLY BELOW THIS LINE
Instructions for Registrars1. Enter enrollment details in to Skyward as appropriate. 2. Send form to District Homeless Liaison (fax: 425-335-3549) 3. Keep a copy of all questionnaires 4. Contact District Homeless Liaison (x1582)
District Homeless Liaison Determination Student lives apart from parents/guardian for school purposes.Student comes under the McKinney Vento Act.
Administrator Initials: Date: Housing Questionnaire – 11/14/14

___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
_____________________________________
_____________________________________
_____________________________________
_____________________________________
_____________________________________
_____________________________________
Electronic Information System (Networks)
Individual User Access Informed Consent Form
for Parent and Student
In consideration for the privilege of using the network and in consideration for having access to the public networks, I hereby release Lake Stevens School District, Washington School Information Processing Cooperative, and other intermediary providers, if any, and operators, and any institutions with which they are affiliated from including, without limitation, the type of damage identified in the Lake Stevens School District’s Acceptable Use Guidelines. Further, my child and I agree to abide by the District’s policy and procedures for electronic information systems, which we have reviewed and understand, and we acknowledge that failure to comply with the policy and procedures may result in revocation of network use privileges. My child and I acknowledge and agree that Lake Stevens School District has the right to review, edit, or remove any materials installed, used, stored, or distributed on or through the network or the District’s system and we hereby waive any right or privacy which my child or I may otherwise have into such material.
Signature of Student
Printed Name of Student
Date Signed
Student ID #
Student Birthdate
School / Campus
Signature of Parent/Guardian (required if user is under age 18)
Printed Name of Parent/Guardian
Date Signed
Address – City/State/Zip
Phone Number
Student Grade Level
*Students over eighteen do not need a parent’s signature.


















