KEPILEPSY Presentation
39
1
description
levetiracetam data sheet
Transcript of KEPILEPSY Presentation

1

2
Defining Epilepsy: Epilepsy is a general term used for a group of disorders that cause disturbances in electrical signaling in the brain. The brain is a highly complex electrical system, powered by roughly 80 pulses of energy per second. An epileptic seizure occurs when these energy pulses come much more rapidly-as many as 500 per second for a short time-due to an electrical abnormality in the brain.
Epilepsy

3
Epilepsy
This brief electrical surge can happen in just a small area of the brain, or it can affect the whole brain. Depending on the part of the brain that is affected, the surge of electrical energy can cause: Changes in a person's sensations or
state of consciousness. Uncontrolled movements of certain
parts of the body or of the whole body.

4
There are numerous types of seizures, which fall into two broad categories: Generalized seizures and Partial seizures.
Generalized seizures affect the whole brain and cause a loss of consciousness.
Partial seizures initially affect only part of the brain, and consciousness may or may not be affected.
Not all seizures are alike:

5
Types of Seizures1- Tonic-clonic seizures:
This is the type of seizure (tonic-clonic seizure) most people associate with epilepsy.
A generalized tonic-clonic seizure often begins without warning.
It involves a sudden stiffness of the body, followed by muscle contractions or jerking motions.

6
Types of Seizures2- Absence Seizures:
Absence seizures often occur in young children and are commonly mistaken for daydreaming. An absence seizure involves a brief disruption of consciousness—lasting from a few seconds to about half a minute.

7
Types of Seizures3- Atonic Seizures:
This may result in the dropping of the head or a limb, or lead a student to fall to the ground. There also may be a brief loss of consciousness, because the patient may fall to the ground, there is a risk of injury.
Sometimes known as a "drop attack," atonic seizures cause a sudden loss of muscle tone.

8
Types of Seizures4- Myoclonic Seizures:
Myoclonic seizures are one of the most common types of seizures, typically affecting children and young adults. A Myoclonic seizure involves a sudden contraction of muscles and can appear as a jerk of one or both arms or sometimes the head. Myoclonic seizures may cause just a single jerk or several jerking movements.

9
Types of Seizures5- Simple Partial Seizures:
In this type of seizure (simple partial seizure), an electrical disturbance starts in one half (or hemisphere) of the brain, so the patient may experience symptoms like twitching, numbness, dizziness, or disturbances to their senses.

10
Types of Seizures6- Complex Partial Seizures:
Like a partial seizure, a complex partial seizure starts in one hemisphere of the brain, and can spread to areas that involve consciousness.
When there is an altered state of consciousness at the onset of the event, the patient may experience a change in awareness and may seem confused.
A common symptom is tugging at clothing; the patient may seem conscious but it is important to remember that he or she is completely unaware of their actions.

11
Types of Seizures6- Complex Partial Seizures:

12
What Can Trigger A Seizure? Different things can trigger seizures in people with epilepsy. Seizures can be triggered by many factors, including:- Missing a dose of medication - Tiredness - Missing meals - Taking illicit drugs - Increased stress level - Flashing lights - Drinking alcohol - Overheating or overexertion (hyperthermia)

13
What is KEPILEPSY® (Levetiracetam)?
KEPILEPSY® (Levetiracetam) does not inhibit or induce hepatic enzymes to produce clinically relevant interactions.
KEPILEPSY® (Levetiracetam) is not appreciably protein-bound, nor does it affect the protein binding of other drugs. Thus, because of its minimal protein binding and lack of hepatic metabolism, the risk of drug interactions is very low.

14
Renal ImpairmentDosage should be reduced in patients with impaired renal function receiving KEPILEPSY® (Levetiracetam) according to the table below:
Group Creatinine clearance(ml/min)
Dosage and frequency
Normal > 80 500 to 1,500 mg twice dailyMild 50-79 500 to 1,000 mg twice dailyModerate 30-49 250 to 750 mg twice dailySevere < 30 250 to 500 mg twice dailyEnd-stage renal disease patientsundergoing dialysis (A 750 mg loading dose is recommended on the first day of treatment with KEPILEPSY® )
- 500 to 1,000 mg once daily (Following dialysis, a 250 to 500 mg supplemental dose is recommended)

15
Hepatic Impairment No dose adjustment is needed for patients with hepatic impairment receiving KEPILEPSY® (Levetiracetam).
Pediatric Patients The body weight adjusted apparent clearance of KEPILEPSY® (Levetiracetam) was approximately 40% higher than in adults.
Starting dose: 10 mg/kg twice daily Maximum dose: 30 mg/kg twice daily

16
KEPILEPSY® (Levetiracetam) is not recommended for use in children below 4 years of age due to insufficient data on safety and efficacy.
Infants and children less than 4 years:
Elderly (from 65 years and old)
Adjustment of the dose is recommended in elderly patients with compromised renal function

17
Daily DosageAdd-on Therapy
Adults and adolescents from 16 years of age weighing 50 kg or more
The initial therapeutic dose is 500 mg twice daily. This dose can be started on the first day of treatment. Depending upon the clinical response and tolerance, the daily dose can be increased up to 1,500 mg twice daily. Dose changes can be made in 500 mg twice daily increases or decreases every two to four weeks.

18
Mode of Action of KEPILEPSY®
KEPILEPSY® the First Synaptic Vesicle 2 A (SV2A) Ligand For the Treatment of Epilepsy.

19
Mode of Action of KEPILEPSY®
KEPILEPSY® has a specific brain binding site (SV2A) which is a presynaptic protein located on the synaptic vesicles. This action is involved in the regulation of vesicle exocytosis, leading to altering in the epileptic firing. KEPILEPSY® bioavailability is 100%, which ensures rapid onset of action.

20
Mode of Action of KEPILEPSY®
SV2AKEPILEPSY® Levetiracetam
KEPILEPSY® (Levetiracetam) binds to a synaptic vesicle protein SV2A, leading to impede (modulate or regulate) nerve conduction across synapses.

21
Different Strengths of KEPILEPSY®

22
1- Doumbia-Ouattara M, Bourel-Ponchel E, Le Moing AG, Querne L, Delignières A, de Broca A, Berquin P. [Experience with levetiracetam in the treatment of childhood refractory epilepsy]. Arch Pediatr. 2012 Jan;19(1):3-8.
INTRODUCTION: In young children presenting drug-resistant epilepsy, the number of approved antiepileptic drugs is limited. Levetiracetam (LEV) is one of the most recent antiepileptic drugs (AED) introduced on the market and data on its effectiveness and tolerance in children are scarce.
PATIENTS AND METHODS: The objective of this retrospective study was to report our experience with the use of levetiracetam as an adjuvant therapy in a population of 42 children presenting a drug-resistant epilepsy. The study was conducted over a 5-year-period (from 1 January 2004 to 30 June 2007).

23
1- Doumbia-Ouattara M, Bourel-Ponchel E, Le Moing AG, Querne L, Delignières A, de Broca A, Berquin P. [Experience with levetiracetam in the treatment of childhood refractory epilepsy]. Arch Pediatr. 2012 Jan;19(1):3-8.
RESULTS: The patients' mean age was 10.8 years (range, 2.1-19 years). The mean duration of epilepsy was 6.6 years (range, 1.5-19 years). After the administration of Levetiracetam, 10 patients (24%) became seizure-free and 16 (38%) had more than 50% seizure reduction. A reduction of less than 50% was observed in 13 patients (31%).
Seizure free More than 50 % seizure reduction
Less than 50 % seizure reduction
0
10
20
30
40
24%
38%31%% of
patients achieved

24
1- Doumbia-Ouattara M, Bourel-Ponchel E, Le Moing AG, Querne L, Delignières A, de Broca A, Berquin P. [Experience with levetiracetam in the treatment of childhood refractory epilepsy]. Arch Pediatr. 2012 Jan;19(1):3-8.
The effectiveness of Levetiracetam was similar in partial and generalized epilepsy.
Levetiracetam was well tolerated by these patients.
CONCLUSION: This study confirms the effectiveness and tolerance of LEV used as an adjuvant therapy in children presenting drug-resistant epilepsy, particularly in the very young ones.

25
2- Delanty N, Jones J, Tonner F. Adjunctive levetiracetam in children, adolescents, and adults with primary generalized seizures: open label, noncomparative, multicenter, long-term follow-up study. Epilepsia. 2012 Jan;53(1):111-9.
PURPOSE: To evaluate the long-term efficacy and tolerability of adjunctive levetiracetam (LEV) in patients with uncontrolled idiopathic generalized epilepsy (IGE).
METHODS: This phase III, open-label, long-term, follow-up study (N167; NCT00150748) enrolled patients (4 to <65 years) with primary generalized seizures (tonic-clonic, myoclonic, absence). Patients received adjunctive LEV at individualized doses (1,000-4,000 mg/day; 20-80 mg/kg/day for children/adolescents weighing <50 kg). Efficacy results are reported for all seizure types [intention-to-treat (ITT) population, N = 217] and subpopulations with tonic-clonic (n = 152), myoclonic (n = 121), and/or absence (n = 70) seizures at baseline.

26
2- Delanty N, Jones J, Tonner F. Adjunctive levetiracetam in children, adolescents, and adults with primary generalized seizures: open label, noncomparative, multicenter, long-term follow-up study. Epilepsia. 2012 Jan;53(1):111-9.
KEY FINDINGS: One hundred twenty-five (57.6%) of 217 patients were still receiving treatment at the end of the study. Mean (standard deviation, SD) LEV dose was 2,917.5 (562.9) mg/day. Median (Q1-Q3) exposure to LEV was 2.1 (1.5-2.8) years, and the maximum duration was 4.6 years. Most patients were taking one (124/217, 57.1%) or ≥2 (92/217, 42.4%) concomitant antiepileptic drugs (AEDs).
Seizure freedom of ≥6 months (all seizure types; primary efficacy end point) was achieved by 122 (56.2%) of 217 patients, and 49 (22.6%) of 217 patients had complete seizure freedom. Seizure freedom of ≥6 months from tonic-clonic, myoclonic, and absence seizures was achieved by 95 (62.5%) of 152, 75 (62.0%) of 121, and 44 (62.9%) of 70 patients, respectively. Mean (SD) maximum seizure freedom duration was 371.7 (352.4) days.

27
2- Delanty N, Jones J, Tonner F. Adjunctive levetiracetam in children, adolescents, and adults with primary generalized seizures: open label, noncomparative, multicenter, long-term follow-up study. Epilepsia. 2012 Jan;53(1):111-9.
All seizure types (n=217)
Tonic-clonic seizures ()152
Myoclonic seizures (n=121)
Absence seizure (n=70)
52
54
56
58
60
62
64 57% 63% 62% 63%
% of patients with seizure free (interval ≥ 6 months)

28
2- Delanty N, Jones J, Tonner F. Adjunctive levetiracetam in children, adolescents, and adults with primary generalized seizures: open label, noncomparative, multicenter, long-term follow-up study. Epilepsia. 2012 Jan;53(1):111-9.
Conclusion: Adjunctive LEV (range 1,000-4,000 mg/day) demonstrated efficacy as a long-term treatment for primary generalized seizures in children, adolescents, and adults with IGE, and was well tolerated.

29
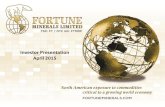
3- Werhahn KJ, Klimpe S, Balkaya S, Trinka E, Krämer G. The safety and efficacy of add-on levetiracetam in elderly patients with focal epilepsy: a one-year observational study. Seizure. 2011 May;20(4):305-11. Epub 2011 Jan 22.
PURPOSE: The long-term safety and efficacy of levetiracetam (LEV) was evaluated as add-on therapy in focal epilepsy patients (n=491) aged at least 65 years who failed at least one monotherapy.
METHODS: Patients (n=491) with focal epilepsy treated with at least one antiepileptic drug in monotherapy with insufficient seizure control were included in this prospective open-label study. The recommended LEV dose range was 1000-3000 mg per day. Follow-up visits were done approximately after 3, 6 and 12 months. Safety and efficacy was analysed based on all patients who received LEV (safety population, n=491) and all patients who were seen at all visits and completed the trial (per protocol population, n=364).

30
3- Werhahn KJ, Klimpe S, Balkaya S, Trinka E, Krämer G. The safety and efficacy of add-on levetiracetam in elderly patients with focal epilepsy: a one-year observational study. Seizure. 2011 May;20(4):305-11. Epub 2011 Jan 22.
RESULTS: Patients (53% men, median age 71 years) had a total of 97 adverse events (AEs) reported in 53 patients. The most common AEs were fatigue and restlessness (9.7% each of all AEs). A total of 35 serious AEs occurred in 19 patients (3.9% of the safety population), all but one unrelated to the study medication. Mean monthly seizure frequency dropped significantly from 7.0 (SD 8.7, range 1-85, median 4) at baseline to 1.7 (SD 2.9, range 0-29, median 1) at 3 month, 1.2 (SD 2.6, range 0-30, median 0) at 6, and 1.4 (SD 6.6, range 0-99, median 0) at 12 months, corresponding to a reduction of 75.7%, 82.9%, and 80.0% relative to baseline. Seizure freedom was reported by 42%, 57.7%, and 58% of patients during the previous period at 3, 6 and 12 months follow-up, respectively.

31
3- Werhahn KJ, Klimpe S, Balkaya S, Trinka E, Krämer G. The safety and efficacy of add-on levetiracetam in elderly patients with focal epilepsy: a one-year observational study. Seizure. 2011 May;20(4):305-11. Epub 2011 Jan 22.
After 3 months After 6 months After 12 months0
10
20
30
40
50
60
42%
57% 58%
% of patients achieved seizure free

32
3- Werhahn KJ, Klimpe S, Balkaya S, Trinka E, Krämer G. The safety and efficacy of add-on levetiracetam in elderly patients with focal epilepsy: a one-year observational study. Seizure. 2011 May;20(4):305-11.
CONCLUSIONS: Add-on treatment with Levetiracetam in elderly patients with focal epilepsy was safe and efficient. Levetiracetam might be considered as a suitable drug in the elderly.

33
4- Lyseng-Williamson KA. Levetiracetam: a review of its use in epilepsy. Drugs. 2011 Mar 5;71(4):489-514
Levetiracetam is an established second-generation antiepileptic drug (AED). Worldwide, levetiracetam is most commonly approved as adjunctive treatment of partial onset seizures with or without secondary generalization; other approved indications include monotherapy treatment of partial onset seizures with or without secondary generalization, and adjunctive treatment of myoclonic seizures associated with juvenile myoclonic epilepsy and primary generalized tonic-clonic (GTC) seizures associated with idiopathic generalized epilepsy.
Levetiracetam has a novel structure and unique mechanisms of action. Unlike other AEDs, the mechanisms of action of levetiracetam appear to involve neuronal binding to synaptic vesicle protein 2A, inhibiting calcium release from intraneuronal stores, opposing the activity of negative modulators of GABA- and glycin-gated currents and inhibiting excessive synchronized activity between neurons.

34
In addition, levetiracetam inhibits N-type calcium channels. Levetiracetam is associated with rapid and complete absorption, high oral bioavailability, minimal metabolism that consists of hydrolysis of the acetamide group, and primarily renal elimination.
It lacks cytochrome P450 isoenzyme-inducing potential and is not associated with clinically significant pharmacokinetic interactions with other drugs, including other AEDs. The efficacy of oral immediate-release levetiracetam in controlling seizures has been established in numerous randomized, double-blind, controlled, multicentre trials in patients with epilepsy. Adjunctive levetiracetam reduced the frequency of seizures in paediatric and adult patients with refractory partial onset seizures to a significantly greater extent than placebo.
Monotherapy with levetiracetam was noninferior to that with carbamazepine controlled release in controlling seizures in patients with newly diagnosed partial onset seizures.
4- Lyseng-Williamson KA. Levetiracetam: a review of its use in epilepsy. Drugs. 2011 Mar 5;71(4):489-514

35
Levetiracetam also provided seizure control relative to placebo as adjunctive therapy in patients with idiopathic generalized epilepsy with myoclonic seizures or GTC seizures.
In addition, patients receiving oral levetiracetam showed improvements in measures of health-related quality of life relative to those receiving placebo.
Although treatment-emergent adverse events were commonly reported in the clinical trials of levetiracetam, the overall proportion of patients who experienced at least one treatment-emergent adverse event was broadly similar in the levetiracetam and placebo treatment groups, with most events being mild to moderate in severity. Levetiracetam is not associated with cognitive impairment or drug-induced weight gain.
4- Lyseng-Williamson KA. Levetiracetam: a review of its use in epilepsy. Drugs. 2011 Mar 5;71(4):489-514

36
KEPILEPSY® Key Points
KEPILEPSY® offer to the doctor & patient all what they need from an antiepileptic drug.
KEPILEPSY® (Levetiracetam) FDA approved.
KEPILEPSY® has a unique mode of action.
KEPILEPSY® has a rapid onset of action.
KEPILEPSY® unlike other anti-epileptic drugs has an ideal pharmacokinetics expected of an antiepileptic drug.

37
KEPILEPSY® Key PointsKEPILEPSY® can be administrated with or without food.
KEPILEPSY® no drug-drug interaction with other drugs due to its low protein binding.
KEPILEPSY® no need for dose adjustment in patients with liver impairment.
KEPILEPSY® broad spectrum antiepileptic drug.
KEPILEPSY® proven efficacy in the treatment of variety of seizures types.
KEPILEPSY® proven efficacy as monotherapy or adjunctive therapy against a variety of seizure types.

38
KEPILEPSY® Key PointsKEPILEPSY® show sustained stable efficacy and well tolerated in patients with different types of seizures during 5 years follow up.
KEPILEPSY® available in many strengths (250, 500, 750 & 1000 mg /tab. – Syrup 500 mg / 5 ml)

39