Kaleidoscope Out of Home Care Clinic- Evolution with the new NSW health Pathways Prepared by: Dr...
31
Kaleidoscope Out of Home Care Clinic- Evolution with the new NSW health Pathways Prepared by: Dr Anne Piper John Hunter Children’s Hospital Kaleidoscope in Greater Newcastle 20 th August 2012
-
Upload
martina-burke -
Category
Documents
-
view
224 -
download
1
Transcript of Kaleidoscope Out of Home Care Clinic- Evolution with the new NSW health Pathways Prepared by: Dr...

Kaleidoscope Out of Home Care Clinic- Evolution with the new NSW health Pathways
Prepared by:
Dr Anne Piper
John Hunter Children’s Hospital
Kaleidoscope in Greater Newcastle
20th August 2012
2
Kaleidoscope OOHC clinic• Commenced as a pilot in Newcastle 2005 with
the aim of offering comprehensive health assessments to children entering long term out of home care who are on interim or final orders.
• Initial referrals accepted from one Community Service Centre and Newcastle Centacare.
• Later referrals accepted from 3 Newcastle Community Service Centres
• Referrals sent directly from CS and criteria that they had not had a recent paediatric assessment nor a regular Paediatrician
• Initial referrals not screened• Early Clinic primarily Paediatrician and
Paediatric Nurse, 87 Paediatrician only

Kaleidoscope clinic
• Goal of the clinic was not only to provide a thorough health and developmental assessment but collation of a large range of health information into a report format, that can then be used to inform the ongoing health care of the child.
• The clinic did not aim to replicate services that were already in place or to take over the ongoing care of children already linked into services or medical care
• If children were being referred to Kaleidoscope for a specific reason or service- it was not appropriate to divert those referrals to the out of home care clinic
4
Early phase
• Initial operational issues with inappropriate referrals• During pilot phase no strict criteria• Many children had been in care for years with kinship
carers and regular GPs• 15 were attending Christian or Private schools• Caseworkers referred children not in care• Referrals screened more closely after the initial few
months• Regular visits to CSC to speak to staff• Approximately 50 referrals rejected 2005 -2010
• Initially follow up appointments offered- ceased – Not always the appropriate service– Paediatric review not always required-
better use of resources to see GP for ongoing care- and referral as appropriate
– Follow up limited capacity of the clinic to accept new referrals

6
Review of criteria following the pilot phase
Based on experiences, a new referral criteria was developed:
• Child has recently been placed in care < 12 months
• The child did not have a regular paediatrician nor has had a paediatric medical assessment in the last 12 months
• The child must be under the parental responsibility of the Minister
• The child is aged 0-12 years (occasional referrals of older children will be considered)
• The child is not in kinship care (occasional referrals may be considered after discussion)

Clinic changes
• From 2009- for training, and to ensure the clinic was not cancelled when Paediatrician unavailable, Paediatric Registrar/fellow allocated to the clinic.
• Re-allocation of staff to the clinic from the Hospital Acute Child Protection Team.
• Child Protection Team psychologist assigned to the clinic
• Child Protection clinical nurse role expanded- greater role in the clinic.

Prioritised pathways- from 2009
• Developed for Speech and language – normal referral pathways – but children in OOHC prioritised
• Developed within existing resources• Dental assessments- prioritised• Normal referral pathways for all other
services, including mental health

9
Present clinic Processes and Resources
• Multidisciplinary screening:– Minimum Paediatrician or Paediatric
Registrar, with Psychologist & Nurse– Health assessment and examination– Clinical interview and Structured play
• 60-90 minutes face to face per child• Pre- assessment:
– Intake processes– Information gathering
• Post- assessment:– Report writing, Referral letters / calls– Feedback to Community Services and
recommendations re follow-up• Total time cost: Minimum 4 hours per child
required
The new OOHC pathway- a time of change
• From 1st September 2010, with the commencement of the OOHC pathway- referrals for all children in the greater Newcastle area were forwarded via the OOHC pathway to the clinic for triaging.
• Referral sent on new referral form developed by NSW Health working group.
• Baseline 2a- GP or Early Childhood nurse assessment (depending on age) unless ‘exempt’
• If required- child then to be seen for a ‘comprehensive assessment’ 2b
What is a comprehensive assessment?
RACP recommendations for children entering OOHC
1.Medical history 6.Development2.Family history 7. Mental health3.Immunisation status 8. Hearing check4.Examination 9. Vision check5. Growth status 10. Dental check
No one health professional can undertake all of theseCannot be achieved by a GP primary screen- and not even
by a Paediatrician assessmentNot achievable in one day
Changes with the new Pathway
• Prior to the new pathway- all referrals sent directly to the clinic from Community Services.
• Initially no referrals received by the clinic for several weeks while processes streamlined.
• Request from Clinic staff that all referrals, whether it was judged prior that they did not fit our criteria for ‘comprehensive’, be forwarded for intake and for statistics purposes.

Role and responsibilities of the clinic given the new referral pathways? The dilemma• Whether tertiary role?• Primary or secondary tier?• Discussion re referral criteria?• Loosening of criteria re kinship carers• Decision that no changes to criteria until other
pathways for children to have health assessments

Dilemmasfor clinic staff at intake
How do we decide that the primary screen (2a) was adequate• Which children should just have a GP screen
vs comprehensive assessment• Discussion re implementing screening tools-
prior to and during the clinic.• Previously no formal screening or
assessment tools used in the primary screen-or in clinic
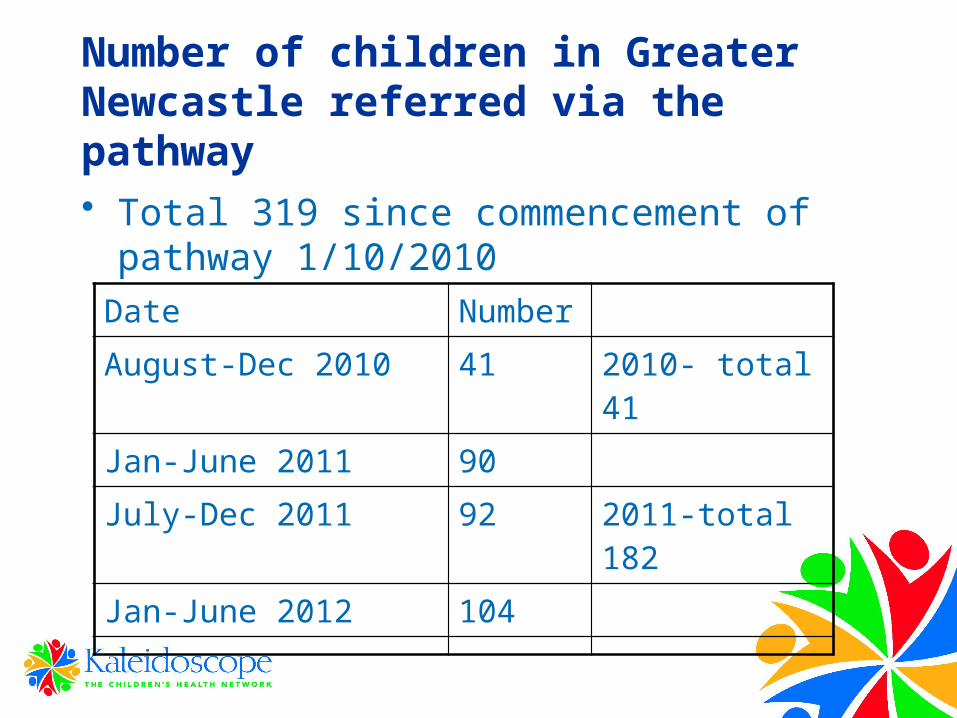
Date Number
August-Dec 2010 41 2010- total 41
Jan-June 2011 90
July-Dec 2011 92 2011-total 182
Jan-June 2012 104
Number of children in Greater Newcastle referred via the pathway
• Total 319 since commencement of pathway 1/10/2010

Greater numbers of referralsdue to
• All children entering care being referred via the pathway
• Larger geographical area- whole of greater Newcastle
• Children assumed into care at birth now referred and accepted by the clinic- unless having Paediatric Follow up
• Loosening of kinship care criteria- now 53% of children seen

Number of children seen in OOHC clinic since 2005- 367 total
• 2005- 18• 2006- 24• 2007- 31• 2008- 40• 2009- 56 (Registrar allocated to clinic)• 2010- 62• 2011- 85- additional clinic added• 2012- 49 Jan- August

0102030405060708090
June-
Dec2005
2007 2009 2011
Number seen

Ages of children seen in the clinic
Year <1 year 1-5 years
5-12 years
>12 years
2005-2006
1 14 20 7
2010 5 27 26 2 0
2011 21 31 29 3
2012 12 21 15 1

Time in care when seen in our clinic
Year Time in care
2005 (June-Dec)
2010 (Jan-Sept)
2011- 2012
10m-11 years (mean 5 years
1m-2 years (m= 5.8 m)
All < 12 months
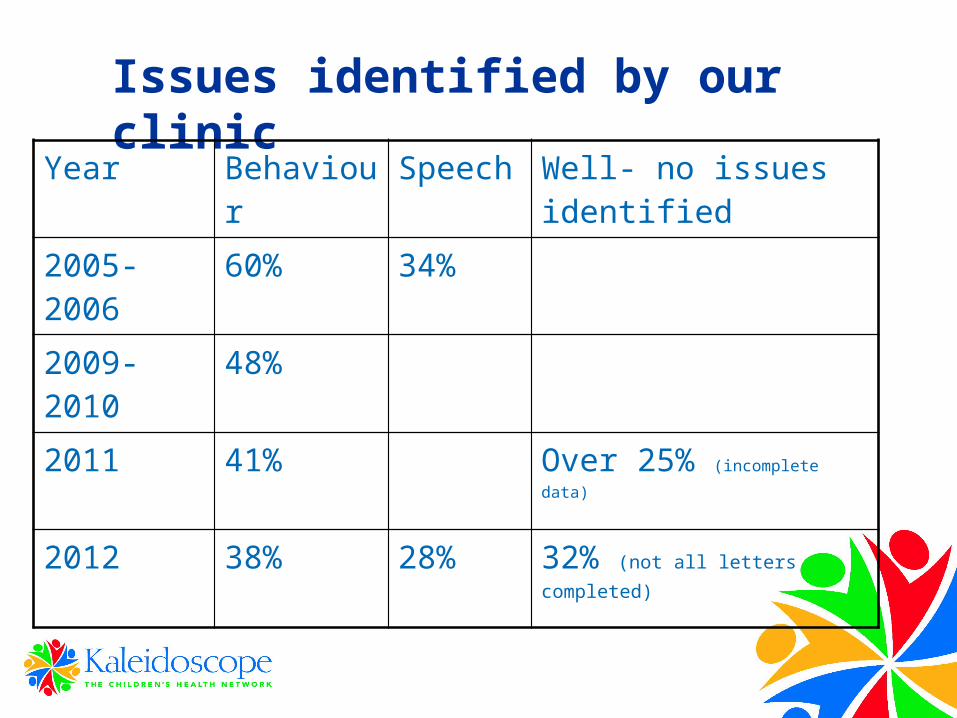
Issues identified by our clinicYear Behaviour Speech Well- no issues
identified
2005-2006 60% 34%
2009-2010 48%
2011 41% Over 25% (incomplete data)
2012 38% 28% 32% (not all letters completed)

Referrals rejected since new pathway
• >106 definitely declined by the clinic• Reasons
– out of area– Already well linked into services or already have
an appointment elsewhere– In care of biological parents with PR to Minister– > 12 years of age-advise more appropriate for
Youth Health team
Advantages of the new pathway
• Dental –organised at intake- priority rating- now likely to happen after primary screening
• Hearing – previously OOHC intake- now health case manager to arrange
• Vision- advised in clinic- but often arranged prior to clinic
• Information gathering by OOHC intake worker- request for birth records, determine if referral suitable for pathway, immunisation records
Ongoing challenges for clinic staff
• Carers not wishing to attend- or understanding why they should attend
• Aboriginal kinship carers- high non-attendance rate- need to target aboriginal carers in culturally appropriate manner
• Behaviour/mental health- require ongoing assessment and management- clinic unable to provide this
• Inability to offer ongoing review has led to criticism when this is already an issue that concerns staff
• Ongoing review would mean inability to see as many new patients- and not an efficient use of resources
• Currently many children followed up by Paediatrician in" General Paediatric’ clinic

GP involvement
• GP referral now requested- as no ongoing review offered in clinic and unable to take over day-to-day medical care.
• Most children should have had a GP visit prior- primary screen, immunisations etc
• Allows Medicare billing by Paediatrician, and letter to be sent to the GP
• Advised that if further Paediatric review required- should be arranged by the GP to the appropriate service/clinician
• Paediatric review to be based on clinical need- rather than to ‘complete forms

Comprehensive ‘one-stop shop’ vs priority pathways
• Pros- One day multidisciplinary comprehensive assessment- means all assessments completed on one day- and fewer appointments to attend.
• Cons-Not all children need allied health multidisciplinary assessment- not an efficient use of staff time, especially when no issues or fail to attend.
• Appointments too long for most children and families- can affect quality of the assessment.
• Not all have developmental concerns• Generally Paediatrician clinical assessment adequate
for developmental assessments of under 2s. • Some children and carers appear overwhelmed by
number of people in the room

Future directions
• Clinic unable to meet demand of growing number of referrals, with current resources and no additional funding from OOHC pathway to the existing clink/service
• Utilisation of new health case manager position to screen which children require comprehensive/Paediatric assessment.
• ASQ and SDQ screening questionnaires sent and scored by health case manager as part of primary assessment.
• More detailed primary assessment carried out by health case manager.

Future directions
• Health case manager will monitor 0-5 case plan every 6 months- until 5 years of age
• 6-17 years – every 12 months to ensure recommendations are followed through
• GP CAFHN review 6 monthly- until 5 years• 12 monthly until 17 years (GP)• Refer as appropriate if Paed review required• CAFHN nurse visit can also count as primary
health screen (instead of health case manager)

The future
• Future- closer linkage with HCM ensuring more efficient planning for our service
• (Of note- over 25% of children not identified with any issues in our ‘comprehensive’ review)– Which children would benefit from assessment in our Clinic– Which staff need to be present – Ensuring the recommendations are followed through– Ongoing data collection to determine if our assessments are
making a difference for the children

• Questions??
Thank you to
The Kaleidoscope OOHC Clinic team• Margaret Ryan, Clinical Nurse Specialist• Elisha Stanton- Child Protection team Psychologist• Lynette Visiou- Administration
Acknowledgements for their assistance• Karen Kemp- HNELHD OOHC coordinator• OOHC Intake officer Amanda Kenneth• Health Case Manager Julie McBride