
K. Shimatani/ K-H Symposium/ October 22-23, 20011 What Impact Will Globalization Have on Bridging...
25
K. Shimatani/ K-H Symposium/ October 22-23, 2001 1 What Impact Will Globalization Have on Bridging Studies Katsuyoshi Shimatani J-Clin, Pfizer
-
Upload
tavion-murley -
Category
Documents
-
view
216 -
download
3
Transcript of K. Shimatani/ K-H Symposium/ October 22-23, 20011 What Impact Will Globalization Have on Bridging...

K. Shimatani/ K-H Symposium/ October 22-23, 2001 1
What Impact Will Globalization Have on Bridging Studies
Katsuyoshi Shimatani
J-Clin, Pfizer
K. Shimatani/ K-H Symposium/ October 22-23, 2001 2
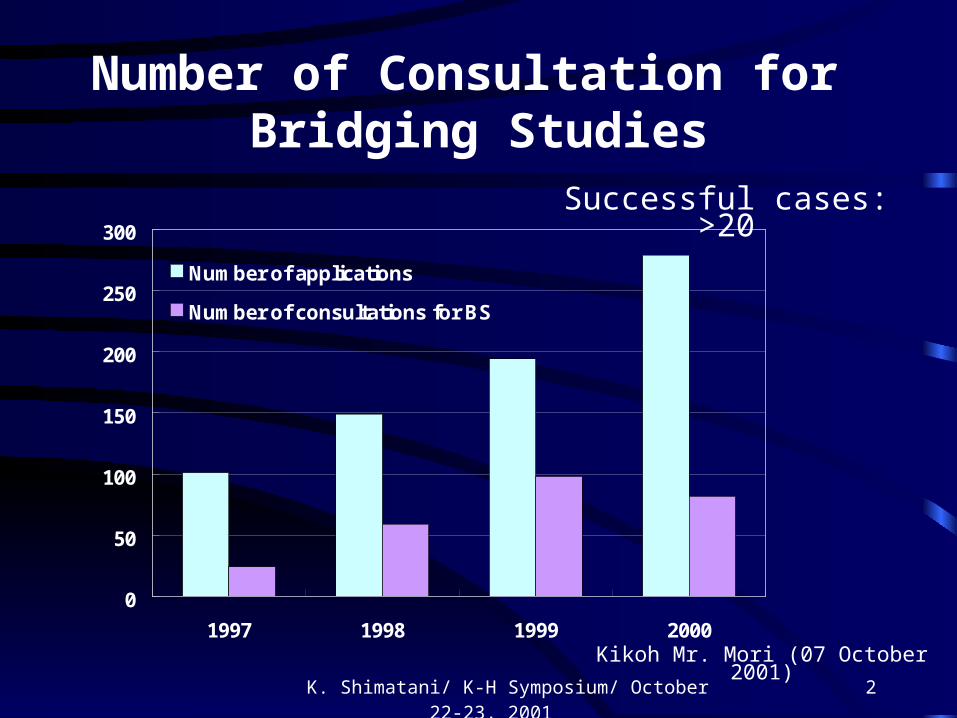
Number of Consultation for Bridging Studies
Kikoh Mr. Mori (07 October 2001)
Successful cases: >20
0
50
100
150
200
250
300
1997 1998 1999 2000
Number of applications
Number of consultations for BS

K. Shimatani/ K-H Symposium/ October 22-23, 2001 3
Drug Approved Through the Use of Overseas Data (1)
Indication of Drug Date of Approval Overseas Data forErectile dysfunction January 1999 EvaluationAlzheimer's disease October 1999 Evaluation
Influenza December 1999 ReferenceDepression, Panic disorders August 2000 Reference
Allergy August 2000 EvaluationBreast cancer December 2000 Evaluation
Influenza December 2000 EvaluationBreast cancer April 2001 Reference
Bronchial asthma June 2001 ReferenceMigraine June 2001 Evaluation
(NCE)
K. Shimatani/ K-H Symposium/ October 22-23, 2001 4
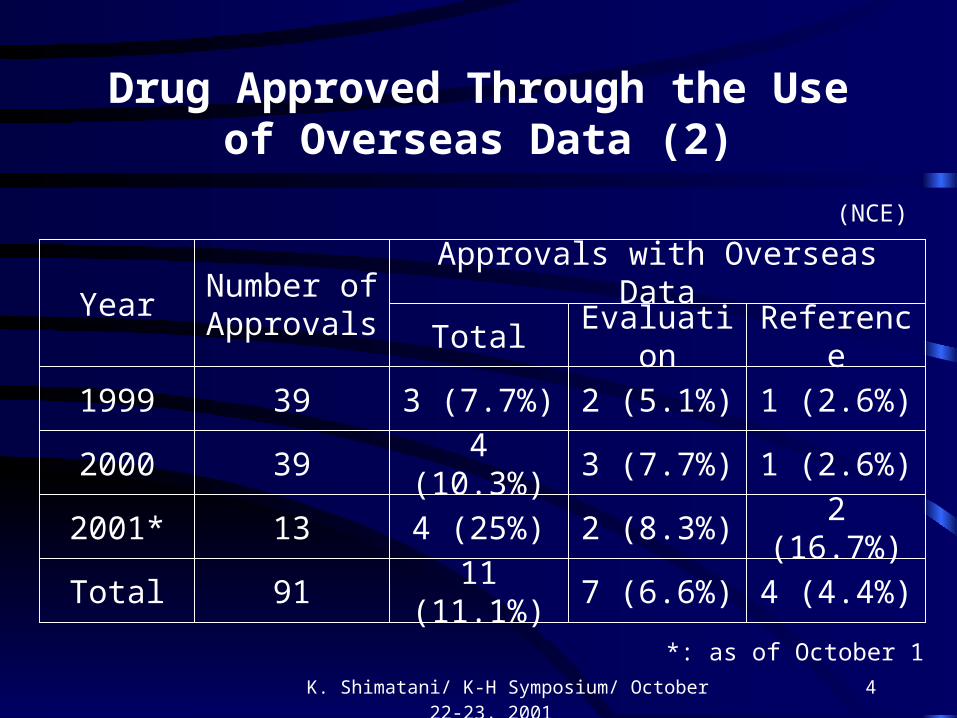
Drug Approved Through the Use of Overseas Data (2)
(NCE)
YearNumber of Approvals
Approvals with Overseas Data
Evaluation ReferenceTotal
1999 39 3 (7.7%) 2 (5.1%) 1 (2.6%)
2000 39 4 (10.3%) 3 (7.7%) 1 (2.6%)
2001* 13 4 (25%) 2 (8.3%) 2 (16.7%)
Total 91 11 (11.1%) 7 (6.6%) 4 (4.4%)
*: as of October 1

K. Shimatani/ K-H Symposium/ October 22-23, 2001 5
Were the objectives of the bridging study achieved?
Was study duplication minimized?
Studies not done in Japan for CCDPPhase II: 1
Phase III: 5
Long term study: 3
Special study: 3
K. Shimatani/ K-H Symposium/ October 22-23, 2001 6
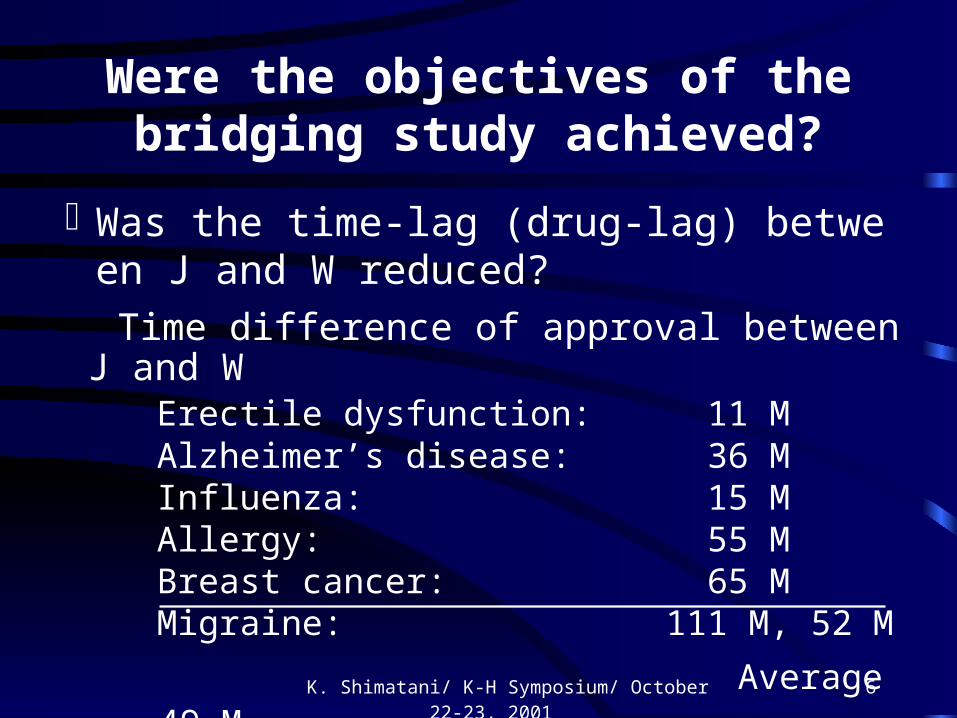
Were the objectives of the bridging study achieved?
Was the time-lag (drug-lag) between J and W reduced?
Time difference of approval between J and WErectile dysfunction: 11 MAlzheimer’s disease: 36 MInfluenza: 15 MAllergy: 55 MBreast cancer: 65 MMigraine: 111 M, 52 M
Average 49 M
K. Shimatani/ K-H Symposium/ October 22-23, 2001 7
Observations in Bridging Studies (1)
Are 20 successful consultations and 11 approval drugs in 3 years sufficient numbers?
The drug-lag has shortened but has not disappeared
“Bridging” is broadly defined Would it be better to define bridging more narrowly?
Most of the drugs that have been approved are ones that meet special medical needs

K. Shimatani/ K-H Symposium/ October 22-23, 2001 8
Observations in Bridging Studies (2)
Dosage differences
There are no set results for determining dosage in bridging studies
Should dose response studies be conducted using the same dosage range as that used in the West, or a dosage range that is one step lower?
Japan is said to use lower dosages than the West, but is it really that the dosages are scientifically low, or is this simply a matter of culture/ custom?
K. Shimatani/ K-H Symposium/ October 22-23, 2001 9
Observations in Bridging Studies (3)
Bridging is intended to mainly pursue similarity only, but has it been possible to adequately obtain the information required for Japanese prescribers and patients?
Is it necessary to re-confirm efficacy of the drugs in Japanese?
There are a lot of cases in which extrinsic factors have been a bigger problem than intrinsic factors

K. Shimatani/ K-H Symposium/ October 22-23, 2001 10
Observations in Bridging Studies (4)
There are therapeutic areas for which bridging is difficult
The use of placebo in psychiatry
It is necessary to have a large sample size in order to calculate the true end points in CV area
Conducting only 1 bridging study is very risky. Depending on the therapeutic area, reproducibility may be low. Wise way to use overseas data should be considered in order to reduce duplication

K. Shimatani/ K-H Symposium/ October 22-23, 2001 11
Bridging Study Benefits
1. Drugs for which it would be difficult to obtain approval based only on the Japanese data have been approved through the use of overseas data
2. The duplication of clinical data has been minimized through the use of overseas data
3. The time required for development has been reduced
With the introduction of the new GCP
4. The quality of Japanese clinical studies has improved
5. Awareness of clinical studies has improved among investigators, sponsors, and others
K. Shimatani/ K-H Symposium/ October 22-23, 2001 12
Bridging Study Transitions
Retrospective bridging
The bridging of similar aspects based on studies already
conducted or underway in the West and Japan
Prospective bridging
The design and conduction of new studies in Japan that
are similar to studies already conducted in the West
Advanced bridging
The design and conduction of new studies in both the
West and Japan for the purpose of bridging
K. Shimatani/ K-H Symposium/ October 22-23, 2001 13
Future options of clinical trials under Globalization
1. Advanced bridging studies
2. Global studies

K. Shimatani/ K-H Symposium/ October 22-23, 2001 14
Advanced Bridging Studies (1)
( 1 ) Protocols of overseas studies should be designed aiming to bridge Japanese studies.
Japan must input to overseas protocols.

K. Shimatani/ K-H Symposium/ October 22-23, 2001 15
Advanced Bridging Studies (2)
( 2 ) Even if Japan start later, the NDAs can be simultaneous
West
Japan Phase I Phase II Phase III
Phase I Phase II
Simultaneous NDA
This strategy could be applied for the therapeutic
areas: No difference in medical practices End points already validated (precedent) Easy to get consistent results
K. Shimatani/ K-H Symposium/ October 22-23, 2001 16
Global StudiesWhy Global Studies?1) ICH recommend to avoid redundancy of clinical studies
which have been already done in overseas
However, MHLW/ Japanese prescribers need to see Japanese data
Global studies Simultaneous NDA
2) There are difficult areas to conduct clinical studies in Japan
Small patient population (cancer and others) Mega-trial (cardiac events, bone fracture) Difficult to have consistent result (psychiatry and others)

K. Shimatani/ K-H Symposium/ October 22-23, 2001 17
Points to be discussedin Global studies
Speed and Quality
Sample size
Similarity
Dosage
Study design
Medical practice

K. Shimatani/ K-H Symposium/ October 22-23, 2001 18
Speed and Quality
Has the Japanese clinical trialenvironment improved?
Collaboration with Asian Countries
YES, but…….

K. Shimatani/ K-H Symposium/ October 22-23, 2001 19
0
50
100
150
200
250
Sep
-99
Oct
-99
Nov
-99
Dec
-99
Jan
-00
Feb
-00
Mar
-00
Ap
r-0
0
May
-00
Jun
-00
Jul-
00
Au
g-0
0
Sep
-00
Oct
-00
Target No of pts
Actual No. of pts
No of sits (drug shipment)
Collaboration with SMO
K. Shimatani/ K-H Symposium/ October 22-23, 2001 20
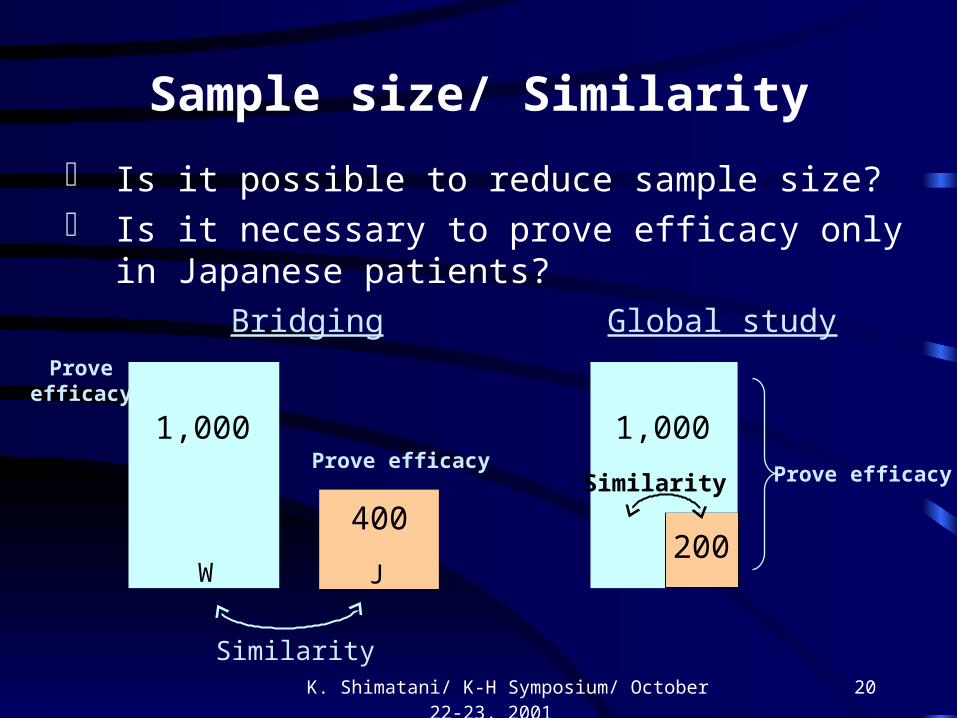
Sample size/ Similarity
Is it possible to reduce sample size? Is it necessary to prove efficacy only in Japanese
patients?
Bridging Global study
1,000
200400
1,000
W J
Similarity
Prove efficacy
Proveefficacy
Prove efficacySimilarity
K. Shimatani/ K-H Symposium/ October 22-23, 2001 21
Similarity

K. Shimatani/ K-H Symposium/ October 22-23, 2001 22
Dosage
From PK profile
West L M H
Japan option 1 L M H
option 2 l L M
option 3 conduct Phase IIa

K. Shimatani/ K-H Symposium/ October 22-23, 2001 23
Study design/ Medical practice
To allow some flexibility in designing of protocol in
order to satisfy with local needs
- Diagnosis- Diagnosis - Primary endpoints- Primary endpoints
- Severity- Severity - Secondary endpoints- Secondary endpoints
- Demography- Demography - Dosage- Dosage

K. Shimatani/ K-H Symposium/ October 22-23, 2001 24
Bridging studies minimize the duplication of studies and increase the chances of approval
Summary (1)
Differences in extrinsic factors are more important than intrinsic factors in bridging studies

K. Shimatani/ K-H Symposium/ October 22-23, 2001 25
Summary (2)
As an important alternative to bridging studies, we should think to conduct global studies. In particular, we should be aggressive in looking into this for therapeutic areas in which clinical studies are difficult to conduct in Japan alone. In such cases, we should be flexible in choosing sample sizes and protocol designs that will allow both the global objectives as well as the local objectives to be achieved.
We need to explore options that would allow us to collaborate with other countries in Asia when conducting global studies


















