J_Neurotrauma_submission_16-APR-2014
28
For Peer Review Only/Not for Distribution Journal of Neurotrauma: http://mc.manuscriptcentral.com/neurotrauma Prospective Examination of the Effects of Combat-related Mild Traumatic Brain Injury: Does Blast mTBI History Matter? Journal: Journal of Neurotrauma Manuscript ID: Draft Manuscript Type: Regular Manuscript Date Submitted by the Author: n/a Complete List of Authors: Kontos, Anthony; University of Pittsburgh, Orthopaedic Surgery ELbin, RJ; University of Arkansas, Office for Sport Concussion Research Kotwal, Russ; Joint Trauma System, US Army Institute of Surgical Research Lutz, Robert; U.S. Army Special Operations Command, Kane, Shawn; U.S. Army Special Operations Command, Forsten, Robert; 121st Combat Support Hospital, US Army Medical Activity, Collins, Michael; University of Pittsburgh, Orthopaedic Surgery Keywords: ADULT BRAIN INJURY, HEAD TRAUMA , MILITARY INJURY, TRAUMATIC BRAIN INJURY, PROSPECTIVE STUDY Mary Ann Liebert, Inc, 140 Huguenot Street, New Rochelle, NY 10801 Journal of Neurotrauma
-
Upload
robert-forsten -
Category
Documents
-
view
7 -
download
0
Transcript of J_Neurotrauma_submission_16-APR-2014

For Peer Review O
nly/Not for Distribution
Journal of Neurotrauma: http://mc.manuscriptcentral.com/neurotrauma
Prospective Examination of the Effects of Combat-related
Mild Traumatic Brain Injury: Does Blast mTBI History Matter?
Journal: Journal of Neurotrauma
Manuscript ID: Draft
Manuscript Type: Regular Manuscript
Date Submitted by the Author: n/a
Complete List of Authors: Kontos, Anthony; University of Pittsburgh, Orthopaedic Surgery ELbin, RJ; University of Arkansas, Office for Sport Concussion Research Kotwal, Russ; Joint Trauma System, US Army Institute of Surgical Research Lutz, Robert; U.S. Army Special Operations Command, Kane, Shawn; U.S. Army Special Operations Command, Forsten, Robert; 121st Combat Support Hospital, US Army Medical Activity, Collins, Michael; University of Pittsburgh, Orthopaedic Surgery
Keywords: ADULT BRAIN INJURY, HEAD TRAUMA , MILITARY INJURY, TRAUMATIC BRAIN INJURY, PROSPECTIVE STUDY
Mary Ann Liebert, Inc, 140 Huguenot Street, New Rochelle, NY 10801
Journal of Neurotrauma

For Peer Review O
nly/Not for Distribution mTBI and Blast History
1
Prospective Examination of the Effects of Combat-related Mild Traumatic Brain
Injury: Does Blast mTBI History Matter?
Anthony P. Kontos, Ph.D.,1 R.J. Elbin Ph.D.,
2 Russ S. Kotwal, M.D., M.P.H.,
3 Robert H.
Lutz, M.D.,4 Shawn Kane, M.D.,
4 Peter J. Benson, M.D.
4, Robert D. Forsten, D.O.,
5
Michael W. Collins, Ph.D.1
1 – The University of Pittsburgh Medical College Sports Medicine Concussion Program,
Pittsburgh, PA
2 – University of Arkansas, Office for Sport Concussion Research, Fayetteville, AR
3 - Joint Trauma System, US Army Institute of Surgical Research, San Antonio, TX
4 – U.S. Army Special Operations Command, Fort Bragg, NC
5 – 121st Combat Support Hospital, US Army Medical Activity- Korea, Seoul, South
Korea
Corresponding Author: Anthony P. Kontos, Ph.D., Assistant Research Director,
UPMC Sports Medicine Concussion Program, Associate Professor Department of
Orthopaedic Surgery, University of Pittsburgh School of Medicine, 3200 South Water
Street, Pittsburgh, PA 15203, (412) 432-3725, [email protected].
Total Word Count: 3,836
Page 1 of 27
Mary Ann Liebert, Inc, 140 Huguenot Street, New Rochelle, NY 10801
Journal of Neurotrauma
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review O
nly/Not for Distribution mTBI and Blast History
2
Abstract
The effects of mild traumatic brain injury (mTBI) have received significant attention
since the beginning of the conflicts in Afghanistan and Iraq. Surprisingly, little is known
about the temporal nature of neurocognitive impairment, mTBI and post-traumatic stress
(PTS) symptoms following combat-related mTBI. It is also unclear as to the role that
blast exposure history has on mTBI and PTS impairments and symptoms. The purpose of
this study was to examine prospectively the effects of mTBI on neurocognitive
performance, and mTBI and PTS symptoms among US Army Special Operations
Command (USASOC) personnel; and to study the influence of previous history of blast
mTBI on these effects. Eighty USASOC personnel with (n=19) and without (n=61) a
history of blast-related mTBI completed the military version of the Immediate Post-
Concussion Assessment Cognitive Test (ImPACT), Post Concussion Symptom Scale
(PCSS), and the PTSD Checklist (PCL) at baseline, as well as 1-7 days and 8-20 days
following a combat-related mTBI. Results indicated that verbal memory (p=.002) and
processing speed (p=.003) scores were significantly lower and mTBI symptoms (p=.001)
were significantly higher at 1-7 days post-injury compared to both baseline and 8-20 days
post-injury. Post-traumatic stress remained stable across the three time periods.
Participants with a history of blast mTBI demonstrated lower verbal memory at 1-7 days
post mTBI compared to participants without a history of blast mTBI (p=.02). Decreases
in neurocognitive performance and increased mTBI symptoms are evident 1-7 days
following combat-related mTBI, and a history of blast-related mTBI may influence these
effects.
Key Words: mTBI, blast, PTSD, neurocognitive, military
Page 2 of 27
Mary Ann Liebert, Inc, 140 Huguenot Street, New Rochelle, NY 10801
Journal of Neurotrauma
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review O
nly/Not for Distribution mTBI and Blast History
3
Introduction
Mild traumatic brain injury (mTBI) is a signature injury sustained by military
personnel during the conflicts in Afghanistan and Iraq1 and accounts for 76% of all brain
injuries reported from 2001 – 2011 in US military personnel (http://www.dvbic.org/TBI-
Numbers.aspx). The estimated lifetime prevalence rate of mTBI among military
personnel is 19.5%.2 However, in spite of these data and due in part to logistic challenges
in combat environments, few studies have assessed the immediate effects of combat-
related mTBI in military personnel. Moreover, Kontos et al.3 reported that combat-related
mTBI exposure was associated with residual neurocognitive impairment and increases in
post-traumatic stress (PTS) symptoms and clinical levels of post-traumatic stress disorder
(PTSD). In addition, the decreases in neurocognitive function and increased PTS
symptoms reported in Kontos et al.3 were further exacerbated by the number of previous
exposures to combat-related mTBI (i.e., dose response). Further investigation of these
relationships is warranted as there is a need to develop a better understanding of the
mTBI and PTS symptoms and cognitive impairments immediately following combat-
related mTBI, and factors that may influence these outcomes in military personnel.
The primary mechanisms of mTBI in military personnel involve blast, blunt, and
blast-blunt combination injuries resulting from exposure to improvised explosive devices
(IEDs), falls, and motor vehicle collisions.4 Blast-related injuries are classified into
primary, secondary, tertiary, and quaternary blast injury types and are more prevalent as
an mTBI mechanism.5,6 Primary blast injuries involve exposure to high-force blast waves
that produce mechanical projectiles (i.e., missile fragments) and secondary blast injury
results in military personnel being forcefully thrown following exposure. Tertiary blast
Page 3 of 27
Mary Ann Liebert, Inc, 140 Huguenot Street, New Rochelle, NY 10801
Journal of Neurotrauma
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review O
nly/Not for Distribution mTBI and Blast History
4
injuries involve collapsing debris, and exposure to fires and noxious fumes are examples
of quaternary blast injury types.6,7 Blunt mTBI results from falls and motor vehicle
collisions that produce acceleration-deceleration forces to the head. Blast-blunt
combination injuries involve both blast and blunt mechanisms.
The signs and symptoms of mTBI include headache, dizziness, fatigue,
inattention, depression, imbalance, memory dysfunction, and slowed reaction time.1,8,9
Within one week of injury the majority of mTBI symptoms cluster into a primary
cognitive-migraine-fatigue symptom factor with additional and less pronounced somatic,
affective, and sleep factors.10 The mTBI symptoms that persist beyond one week post-
injury cluster into more distinct emotional, migraine/somatic, cognitive, and sleep
factors.11 The symptom presentations observed in military personnel with mTBI are
similar to the sequelae documented in athletes with sport-related mTBI.12 If mismanaged,
these impairments may lead to prolonged impairment, with recent reports showing that
the prevalence of chronic mTBI symptoms ranges from 15 to 30%.13 Moreover, PTS
symptoms that commonly overlap with mTBI symptoms occur in up to 40% of U.S.
military personnel who have had mTBI.14 Baseline levels of PTS symptoms are higher
for military personnel with previous exposure to blast-related mTBI.3 These findings
stress the importance of proper assessment and management of mTBI in military
personnel, and continued investigation of the effects of exposure to mTBI.
Despite the potential deleterious effects of the aforementioned impairments and
symptoms on combat performance and quality of life, the majority of military personnel
with mTBI underestimate the seriousness of this injury and do not seek medical
attention.15 Similar to military personnel, many athletes also minimize and avoid
Page 4 of 27
Mary Ann Liebert, Inc, 140 Huguenot Street, New Rochelle, NY 10801
Journal of Neurotrauma
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review O
nly/Not for Distribution mTBI and Blast History
5
reporting mTBI symptoms to medical professionals.16 Due to potential self-report
limitations and shortcomings of relying on subjective reports (e.g., inaccurate symptom
reporting) more objective assessments for mTBI are often employed. Computerized
neurocognitive testing (e.g., Automated Neuropsychological Assessment Metrics
[ANAM]; military version of the Immediate Post-concussion Assessment and Cognitive
Test [ImPACT]) is one tool that provides more objective data on the effects of mTBI in
military personnel.
Although computerized neurocognitive testing has been used in the military for
over a decade, little is known about the acute (i.e., 24-72 hours) and sub-acute (i.e., 3-21
days) cognitive effects of mTBI when assessed in the combat environment. Kelly and
colleagues17 compared the cognitive performance of soldiers with mTBI to healthy and
injured controls within 72 hours post-injury using the ANAM battery. They reported that
soldiers with mTBI demonstrated significant decreases in performance on simple reaction
time, procedural reaction time, and code substitution, compared to both control groups.
Although this was the first study to document the acute (i.e., within 72 hours of injury)
cognitive effects of combat-related mTBI among military personnel, these data were
limited to a small sample of cases (N= 34) that included only post-injury assessments.17
Moreover, the researchers did not assess the effects of mTBI beyond the 72 hour time
period. These researchers also did not examine potential differences in post-mTBI
neurocognitive performance between blast and blunt mechanisms of injury or the
influence of mTBI history on subsequent post-mTBI cognitive performance. Previous
research3 has documented that a history of blast-related mTBI is associated with worse
baseline performance on visual memory and reaction time than a history of blunt mTBI
Page 5 of 27
Mary Ann Liebert, Inc, 140 Huguenot Street, New Rochelle, NY 10801
Journal of Neurotrauma
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review O
nly/Not for Distribution mTBI and Blast History
6
or no history of mTBI. In addition, these researchers reported that individuals with prior
exposure to blast-related mTBI demonstrated increased PTS symptoms. However, little is
known about the interaction between mTBI history and current mTBI on cognitive
impairments, symptoms and PTS following subsequent mTBI in military personnel.
The primary purpose of the current study was to examine prospectively the effects
of mTBI on neurocognitive performance, and mTBI and PTS symptoms among US Army
Special Operations Command (USASOC) personnel. A secondary purpose of the study
was to examine the role of history of blast mTBI on the above outcomes. We
hypothesized that cognitive impairments and symptoms would be evident following
mTBI and that a history of blast mTBI would worsen these outcomes.
Materials and Methods
Participants and Design
A prospective, repeated measures design involving assessments of neurocognitive
performance, mTBI and PTS symptoms was conducted between December 2009 and
March 2012. A total of 276 USASOC personnel (Age, M = 28.68 years, SD = 6.40) with
a diagnosed mTBI were included in the initial sample for this study. The majority of the
sample was currently deployed (80%, n= 220) and male (99%, n= 273). Individuals were
excluded from the study if they had a history of diagnosed moderate to severe TBI, brain
surgery, major psychiatric disorder, or neurological disorder. In addition, participants
were included only if reliable data were available for mechanism of injury and previously
diagnosed mTBI history. Finally, participants were included if they completed the
measures described below at baseline (pre-injury), and 1-7 and 8-20 days post-injury
Page 6 of 27
Mary Ann Liebert, Inc, 140 Huguenot Street, New Rochelle, NY 10801
Journal of Neurotrauma
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review O
nly/Not for Distribution mTBI and Blast History
7
intervals. The resulting sample of 80 all male participants represented a total response
rate of 28% of the original sample of 276 USASOC personnel.
Definition of mTBI
For the current study, a diagnosed mTBI involved presentation with signs (e.g.,
loss of consciousness, disorientation/confusion, amnesia) and symptoms (e.g., dizziness,
headache) of an mTBI with confirmatory diagnoses through follow-up clinical
assessments by USASOC medical personnel. All injuries in the current study were
characterized by Glasgow Coma Scale (GCS) scores of 15 with no abnormal findings on
structural imaging (i.e. CT Scan, MRI).
Instrumentation
Neurocognitive Performance, mTBI Symptoms, and PTS Symptoms
A military version of the Immediate Post-Concussion Assessment Cognitive Test
(ImPACT) was used to assess neurocognitive performance. The military version of this
test also comprises the following sections: 1) demographics, 2) the Post-concussion
Symptom Scale (PCSS), and 3) post-traumatic stress disorder (PTSD Checklist: PCL).
The neurocognitive assessment is comprised of six subtests: 1) verbal memory, 2) design
memory, 3) X’s and O’s, 4) symbol matching, 5) color matching, and 6) three letter
memory. The six neurocognitive subtests are collapsed into four composite scores
including verbal memory, visual memory, visual motor processing speed, and reaction
time (RT). Demographic data include age, sex, migraine history, deployment status,
testing location, military rank, and military occupational specialty. The PCSS contains 22
self-report symptoms rated on a 0 (none) to 6 (severe) point Likert scale. The PCL
encompasses 17 items and requires individuals to indicate on a scale of 1 (not at all) to 5
Page 7 of 27
Mary Ann Liebert, Inc, 140 Huguenot Street, New Rochelle, NY 10801
Journal of Neurotrauma
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review O
nly/Not for Distribution mTBI and Blast History
8
(extremely) how much each item bothered them during the past month. The PCL yields a
PTSD symptom score that ranges from 17-85. Clinical PTSD cut-offs for the PCL were
set at 28 or higher, per current guidelines for recent veterans of combat in Afghanistan
and Iraq.18-20
Procedures
This study was approved by both the University of Pittsburgh and Womack Army
Medical Center institutional review boards for human subject research. Each participant
individually completed the web-based military version of the PCSS, PCL, and military
ImPACT tests at baseline and approximately 1-7 and 8-21 days post injury.
Data Analysis
Descriptive analyses were conducted to describe the sample and mechanism of
mTBI (e.g., blunt or blast/combination) for participants. The sample was divided into two
mutually exclusive groups based on history of medically diagnosed mTBI since joining
USASOC: 1) history of blast mTBI, or 2) no blast mTBI history. It is important to note
that some participants in the no blast mTBI history group may have had previous
exposure to blunt mTBI. A series of 2 (blast mTBI history) x 3 (time) repeated measures
ANOVAs with Bonferroni correction for multiple comparisons were used to compare
changes in neurocognitive performance, mTBI symptoms and PTS symptoms from
baseline to 1-7 and 8-20 days post-injury. The independent variables were history of
diagnosed blast mTBI and time (baseline, 1-7 days, and 8-21 days post injury).
Dependent variables were scores on the ImPACT composites (verbal and visual memory,
processing speed, and reaction time), total PCSS, and total PCL symptom scores. Data
were analyzed using SPSS Version 20 (IBM).
Page 8 of 27
Mary Ann Liebert, Inc, 140 Huguenot Street, New Rochelle, NY 10801
Journal of Neurotrauma
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review O
nly/Not for Distribution mTBI and Blast History
9
Results
Descriptive Data and mTBI Mechanisms and Previous mTBI Exposure among USASOC
Personnel
A summary of descriptive demographic data for the blast mTBI history and no
history groups as well as the total sample is provided in Table 1. The results of a series of
independent samples t-tests and chi-square analyses (mTBI mechanism, history of
medical diagnosed blunt mTBI) supported significant differences between the blast mTBI
history groups on age (t= -2.25, p=.03) and height (t= -2.28, p=.03). The blast mTBI
history group was slightly older (31.05 +/- 7.07 yrs) and taller (180.61 +/- 5.86cm) than
the no history group (27.54 +/- 5.57 yrs; 176.59 +/- 6.95 cm). The breakdown of mTBI
mechanisms was as follows: 29% (23/80)- blunt mTBI, 21% (17/80)- blast/combination
mTBI. The mTBI mechanisms for 50% (40/80) of the injuries in this sample were
unknown/undocumented. One-third (26/80) of the sample reported a history of at least
one medically diagnosed blunt mTBI and 24% (19/80) reported a history of at least one
medically diagnosed blast/combination mTBI.
Changes in Neurocognitive Performance, Symptoms, and Post-Traumatic Stress
Symptoms Across Time
The results from a series of 2 diagnosed history of blast mTBI group (none, blast
mTBI history) x 3 time periods (baseline, 1-7 and 8-20 days) repeated measures
ANOVAs revealed significance within subjects main effect for time on verbal memory (F
[2, 77]= 6.71, p= .002), processing speed (F [2, 77]= 6.19, p= .003) and mTBI symptoms
(F [2, 77]= 14.28, p= .001). A summary of the main effect for time on neurocognitive
performance, mTBI symptoms and PTS symptoms is presented in Table 1. Specifically,
Page 9 of 27
Mary Ann Liebert, Inc, 140 Huguenot Street, New Rochelle, NY 10801
Journal of Neurotrauma
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review O
nly/Not for Distribution mTBI and Blast History
10
the results indicated that verbal memory and processing speed scores were significantly
lower and mTBI symptoms were significantly higher at 1-7 days post-injury compared to
both baseline and 8-20 days post-injury. Although visual memory and reaction time were
not statistically lower at 1-7 days post-injury compared to baseline and 8-20 days post-
injury, the results did support a clinically meaningful trend across these time periods.
Post-traumatic stress symptoms remained constant across the three time periods.
Interaction between Diagnosed Blast mTBI History and Time on Neurocognitive
Performance, mTBI Symptoms, and PTS Symptoms
The results from a series of 2 diagnosed history of blast mTBI group (none, blast
mTBI history) x 3 time periods (baseline, 1-7 and 8-20 days) repeated measures
ANOVAs supported one interaction between a history of diagnosed blast mTBI and time
on verbal memory (F [2, 77]= 4.08, p=.02). A summary of the results for these analyses
is presented in Table 3. Specifically, verbal memory scores were lower at 1-7 days and 8-
20 days post injury than baseline for the diagnosed history of blast mTBI group but not
for the no history of blast mTBI group (see Figure 1). There were non-significant, but
clinically relevant trends for lower performance on visual memory, processing speed, and
reaction time and higher mTBI symptoms at 1-7 days post-injury compared to baseline
for the diagnosed history of blast mTBI group compared to the no blast mTBI history
group. However, there were no such trends for PTS symptoms, which remained
essentially stable across each of the three time points (see Table 3).
Page 10 of 27
Mary Ann Liebert, Inc, 140 Huguenot Street, New Rochelle, NY 10801
Journal of Neurotrauma
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review O
nly/Not for Distribution mTBI and Blast History
11
Discussion
Overview of Key Findings
In the current study we prospectively examined changes in neurocognitive
performance, mTBI and PTS symptoms from baseline to 1-7 and 8-20 days post-injury
among USASOC personnel who sustained a mTBI. We also investigated the role that
previous history of blast mTBI had on subsequent neurocognitive outcomes and mTBI
and PTS symptom reports. There were several key findings in this study: 1) decreases in
neurocognitive performance (i.e., verbal memory, processing speed) and increases in
mTBI symptoms were detected during the first 7 days following mTBI in USASOC
personnel; 2) PTS symptoms remained stable from baseline to 20 days post-injury; and 3)
USASOC personnel with a prior history of blast mTBI demonstrated worse
neurocognitive performance during the first week following mTBI on verbal memory
compared to those without history of blast mTBI. These findings provide partial support
for our hypotheses and demonstrate the effects of mTBI on neurocognitive performance
and symptom reports in USASOC personnel. These findings also underscore the
importance of the role of previous exposure to blast mTBI on subsequent mTBI outcomes.
General Discussion
The current findings support and extend previous research that has examined the
adverse effects of mTBI on cognitive performance and symptom reports in military
populations. In a small sample of military personnel (n = 34) assessed within 72 hours of
mTBI, Kelly et al.17 documented significant changes in simple and procedural reaction
time, code substitution, and matching compared to non-injured, matched controls.
However, Kelly and colleagues17 did not measure these outcomes beyond the initial 72
Page 11 of 27
Mary Ann Liebert, Inc, 140 Huguenot Street, New Rochelle, NY 10801
Journal of Neurotrauma
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review O
nly/Not for Distribution mTBI and Blast History
12
hour acute period following mTBI. The current study extended the previous study and
demonstrated decreased neurocognitive performance up to 7 days post injury, with a
return to pre-injury neurocognitive performance and mTBI symptoms within 8 - 20 days.
This return to pre-injury levels at 8-20 days provides some evidence that the current
clinical practice guidelines implemented by USASOC medical personnel for assessing
and managing mTBI are effective in reducing the long term effects of this injury.
Statistical decreases in neurocognitive performance within the first week
following mTBI were supported for verbal memory and processing speed, but not for
visual memory and reaction time. Although not statistically significant, performance on
visual memory and reaction time was lower at 1-7 days post-injury compared to baseline
levels. It is important to note that these statistically non-significant trends may still be
clinically relevant, as they support a general decline in neurocognitive performance in the
first week following injury.
In addition to the neurocognitive findings, as expected, total mTBI symptoms
were significantly higher compared to baseline at 1-7 days post-injury, but were not
significantly elevated at 8-20 days post injury. In contrast to this increase in mTBI
symptoms, PTS symptom scores remained stable from baseline to both post-injury time
intervals. This finding suggests that some of the initial effects of mTBI previously
attributed to PTS among military personnel, may in fact, be a direct result of the mTBI
instead. Given the purposeful selection for resiliency among USASOC personnel, the
changes associated with PTS may not manifest at all, may manifest later in the process or
only after multiple exposures to potential PTS-inducing stimuli, such as mTBI in this
sample. Resiliency has been reported to be a moderator of stress associated with military
Page 12 of 27
Mary Ann Liebert, Inc, 140 Huguenot Street, New Rochelle, NY 10801
Journal of Neurotrauma
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review O
nly/Not for Distribution mTBI and Blast History
13
deployment,21 and “highly cohesive” military units with strong social support are
reported to be more resilient to high combat exposure as well as depression and PTS.22
Given the short period of time after mTBI exposure (no more than 20 days) in the current
study, PTS symptoms in this population may not manifest for months to years following
blast exposure as documented in previous research.15 Extricating PTS from mTBI-
particularly in the early phases of the injury- is further complicated by the number of
overlapping symptoms of both PTS and mTBI.23 Given this potential overlap between
symptoms of PTS and mTBI and previous findings, the lack of increased PTS symptom
reports following mTBI requires additional study and should be interpreted cautiously
secondary to the chronic course of both PTS and mTBI.
Previous research has supported the relationship between mTBI symptoms and
PTSD symptoms,24 but many of these studies focus on chronic mTBI and PTSD
symptom reporting.25-27
Little is known regarding the acute PTS symptom presentation
and its relationship to acute mTBI symptoms, as measured in the current study. There
may be a bias among USASOC personnel to minimize PTS symptoms in the days and/or
weeks following mTBI due to the fear of the consequences of a behavioral health referral
(e.g., being withheld from active duty/combat), stigma associated with reporting PTS
symptoms, and the potential for receiving a PTSD diagnosis.28 The time course of PTS
and mTBI symptom reporting warrants additional study in order to better understand the
temporal nature of how these symptoms emerge and develop following mTBI and if a
history of blast mTBI influences the development of PTSD.
In the current study, USASOC personnel with a history of blast mTBI performed
worse on verbal memory one week following mTBI compared to those without a history
Page 13 of 27
Mary Ann Liebert, Inc, 140 Huguenot Street, New Rochelle, NY 10801
Journal of Neurotrauma
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review O
nly/Not for Distribution mTBI and Blast History
14
of blast mTBI. This finding is consistent with previous research by Kontos et al.,3 which
reported that a history of blast mTBI was associated with lower baseline neurocognitive
performance. However, there were no differences on verbal memory in the current
sample at baseline; only at 1-7 days post-injury. Therefore, a history of previous blast
mTBI may amplify the initial effects of subsequent mTBIs. It is noteworthy that the
verbal memory scores of individuals with a history of previous exposure to blast mTBI
returned to pre-injury levels by 8-20 days. This finding indicates that although personnel
with a history of blast mTBI may experience more significant initial impairment
following a subsequent mTBI, with proper clinical management their impairments are
short-lived. However, if these potentially at-risk personnel are returned to active duty too
early when they are still suffering from the effects of this injury, these initial effects may
be prolonged or worsened.
There were no differences between history of previous exposure to blast mTBI
groups on current mTBI and PTS symptoms. This finding is in contrast to the residual
effects on mTBI and PTS symptoms reported by Kontos and colleagues.3 One reason for
this finding is that USASOC personnel may deny or minimize their PTS symptoms in
order to remain active with their units and avoid potential stigma associated with PTSD
in the military. Alternately, USASOC personnel may lack insight into their PTS
symptoms in the period immediately following exposure to mTBI. In the current study,
we did not differentiate among levels of exposure to previous blast mTBIs. Moving
forward, researchers should examine the potential interaction between history of previous
exposure to blast mTBI and current mTBI mechanism on outcomes. In so doing,
Page 14 of 27
Mary Ann Liebert, Inc, 140 Huguenot Street, New Rochelle, NY 10801
Journal of Neurotrauma
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review O
nly/Not for Distribution mTBI and Blast History
15
researchers may be able to determine if these previous exposures to blast mTBI
compound the effects of subsequent blast/combo and blunt mTBIs, equally.
Limitations
As with any research, there were some limitations to the current study. Due to the
inherent challenges in obtaining complete and accurate medical records during active
combat environments there was a low overall response rate (29%, 80/276) from among
all USASOC personnel who met initial inclusion criteria. We were able to obtain reliable
information for only 50% of the current mTBI mechanisms (e.g., blast/combo, blunt).
Blast sensor data were unavailable in this study. Therefore, the amount of force at impact
whether previous or current, blunt or blast, could not be measured and incorporated into
our analyses. Consequently, we were unable to examine potential differences in
outcomes based on current mTBI mechanism or the interaction between current
mechanism and a history of previous exposure to blast mTBI. The use of self-reported
PTS and mTBI symptom data are limited in that they rely on subjective reporting. Also,
we assumed that respondents were honest and accurate in their responses. The entire
sample was comprised of males, which limits the generalizability of the current findings
to male military personnel only. As such, the sex differences in recovery outcomes
following mTBI in civilian sport populations reported by researchers29,30
could not be
examined in the current study sample. Finally, the study sample was delimited to
USASOC personnel, who represent a selective sub-sample that may not be generalizable
to the overall US Army and US Military populations.
Implications
Page 15 of 27
Mary Ann Liebert, Inc, 140 Huguenot Street, New Rochelle, NY 10801
Journal of Neurotrauma
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review O
nly/Not for Distribution mTBI and Blast History
16
Neurocognitive impairment and symptoms were detected on average up to one-
week in USASOC personnel following mTBI. We believe that computerized
neurocognitive testing can be a useful tool for medical providers use as part of a
comprehensive mTBI post-injury assessment to guide return to full duty and participation
in follow on combat operations. Neurocognitive data, in combination with information
about balance, vestibular, oculomotor and other assessments, can help inform better
clinical decision-making and identify personnel who are potentially at-risk, but do not
report symptoms. Additionally, these data can be used to better inform military leaders
regarding the impact of such events on personnel, and to promote conservative
management strategies and adherence to clinical practice guidelines as warranted.
Based on the current findings, military medical professionals should consider the
history of previous exposure to blast mTBI when evaluating patients who have incurred a
subsequent mTBI. For sustained combat operations- as evidenced by nearly 13 years of
conflict- a risk benefit analysis may be warranted as military leaders consider the
repetitive use of the same personnel from a relatively small all-volunteer force to conduct
frequent missions involving likely exposure to mTBI mechanisms. Potential multiple
exposures to blast forces and other mTBI mechanisms may result in adverse, residual
long-term health implications for these at-risk military personnel.
Conclusion
In conclusion, the present study demonstrated that neurocognitive deficits in
verbal memory and processing speed and an increase in reported mTBI symptoms
following mTBI in USASOC personnel are evident in the first week, but resolve within 8
– 20 days following injury. However, these increases were not observed for PTS
Page 16 of 27
Mary Ann Liebert, Inc, 140 Huguenot Street, New Rochelle, NY 10801
Journal of Neurotrauma
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review O
nly/Not for Distribution mTBI and Blast History
17
symptoms, which remained stable and low from baseline through 8-20 days post-injury.
Importantly, a history of exposure to previous blast mTBI appears to exacerbate initial
impairment and symptoms following a subsequent mTBI exposure. As such, clinicians
should identify these at-risk personnel for more conservative and targeted clinical
management to mitigate the effects of previous history of exposure to blast mTBI on
subsequent mTBIs. However, the current findings suggest that personnel with a previous
history of exposure to blast mTBI recovered to pre-injury neurocognitive and symptom
levels by 8-20 days, similar to personnel with no history of blast mTBI. Therefore,
current clinical practice guidelines for managing this injury implemented by USASOC
medical personnel may be helping to improve outcomes even in these at-risk personnel.
Author Disclosure Statement
Dr. Collins owns a 10% share in ImPACT Applications, Inc. With regard to the study
data, Dr. Collins was not involved in data collection, entry or analysis; he was only
involved in data interpretation.
Disclaimer
This research was funded by the U.S. Special Operations Command Biomedical
Initiatives Steering Committee. The views expressed herein are those of the author(s) and
do not reflect the official policy of the Department of the Army, Department of Defense,
or the U.S. Government. Citations of commercial products or organizations do not
constitute an official DoD endorsement or approval of the products or services of these
organizations. This report was approved for public release by the U.S. Army Special
Operations Command Operational Security Office and Public Affairs Office on April,15,
2014, and the U.S. Army Medical Department Public Affairs Office on April 15, 2014.
Page 17 of 27
Mary Ann Liebert, Inc, 140 Huguenot Street, New Rochelle, NY 10801
Journal of Neurotrauma
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review O
nly/Not for Distribution mTBI and Blast History
18
Page 18 of 27
Mary Ann Liebert, Inc, 140 Huguenot Street, New Rochelle, NY 10801
Journal of Neurotrauma
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review O
nly/Not for Distribution mTBI and Blast History
19
References
1. Warden, D. (2006). Military TBI during the Iraq and Afghanistan wars. J Head
Trauma Rehab 21, 398-402.
2. Tanielian, T., Jaycox, J.H. (2008). Invisible wounds of war: psychological and
cognitive injuries, their consequences, and services to assist recovery. RAND. Santa
Monica, CA.
3. Kontos, A.P., Kotwal, R.S., Elbin, R.J., Lutz, R.H., Forsten, R.D., Benson, P.J.,
Guskiewicz, K.M. (2013). Residual effects of combat-related mild traumatic brain
injury. J. Neurotrauma 30, 680-686.
4. Murray, C.K., Reynolds, J.C., Schroeder, J.M., Harrison, M.B., Evans, O.M.,
Hospenthal, D.R. (2005). Spectrum of care provided at an echelon II Medical Unit
during Operation Iraqi Freedom. Mil Med 170, 516-520.
5. Krainin, B.M., Forsten, R.D., Kotwal, R.S., Lutz, R.H., Guskiewicz, K.M. (2011).
Mild traumatic brain injury literature review and proposed changes to classification.
J Spec Oper Med 11, 38-47.
6. DePalma, R.G., Burris, D.G., Champion, H.R., Hodgson, M.J. (2005). Blast
injuries. New Engl J Med 352, 1335-1342.
7. Taber, K.H., Warden, D.L., Hurley, R.A. (2006). Blast-related traumatic brain
injury: what is known? J Clin Neuropsych Clin N 18, 141-145.
8. Fear, N.T., Jones, E., Groom, M., Greenberg, N., Hull, L., Hodgetts, T.J., Wessely,
S. (2009). Symptoms of post-concussional syndrome are non-specifically related to
Page 19 of 27
Mary Ann Liebert, Inc, 140 Huguenot Street, New Rochelle, NY 10801
Journal of Neurotrauma
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review O
nly/Not for Distribution mTBI and Blast History
20
mild traumatic brain injury in UK Armed Forces personnel on return from
deployment in Iraq: an analysis of self-reported data. Psychol Med 39, 1379-1387.
9. Levin, H.S., Wilde, E., Troyanskaya, M., Petersen, N.J., Scheibel, R., Newsome,
M., Radaideh, M., Wu, T., Yallampalli, R., Chu, Z., Li, X. (2010). Diffusion tensor
imaging of mild to moderate blast-related traumatic brain injury and its sequelae. J
Neurotrauma 27, 683-694.
10. Kontos, A.P., Elbin, R.J., Schatz, P., Covassin, T., Henry, L., Pardini, J., Collins,
M.W. (2012). A revised factor structure for the post-concussion symptom scale:
baseline and postconcussion factors. Am J Sports Med 40, 2375-2384.
11. Pardini, J., Stump, J.E., Lovell, M., Collins, M.W., Moritz, K., Fu, F.H. (2004). The
post concussion symptom scale (PCSS): a factor analysis [abstract]. Brit J Sports Med
38, 661 - 662.
12. Eskridge, S.L., Macera, C.A., Galarneau, M.R., Holbrook, T.L., Woodruff, S.I.,
MacGregor, A.J., Morton, D.J., Shaffer, R.A. (2013). Influence of combat blast-related
mild traumatic brain injury acute symptoms on mental health and service discharge
outcomes. J Neurotrauma 30, 1391-1407.
13. Vanderploeg, R.D., Curtiss, G., Luis, C.A., Salazar, A.M. (2007). Long-term
morbidities following self-reported mild traumatic brain injury. J Clin Exp
Neurpsychol 29, 585-598.
14. Hoge, C.W., McGurk, D., Thomas, J.L., Cox, A.L., Engel, C.C., Castro, C.A. (2008).
Mild traumatic brain injury in U.S. Soldiers returning from Iraq. New Engl J Med 358,
453-463.
Page 20 of 27
Mary Ann Liebert, Inc, 140 Huguenot Street, New Rochelle, NY 10801
Journal of Neurotrauma
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review O
nly/Not for Distribution mTBI and Blast History
21
15. Lange, R.T., Brickell, T.A., French, L.M., Merritt, V.C., Bhagwat, A., Pancholi, S.,
Iverson, G.L. (2012). Neuropsychological outcome from uncomplicated mild,
complicated mild, and moderate traumatic brain injury in US military personnel.
Arch Clin Neuropsychol 27, 480-494.
16. McCrea, M., Hammeke, T., Olsen, G., Leo, P., Guskiewicz, K. (2004).
Unreported concussion in high school football players: implications for prevention.
Clin J Sports Med 14, 13-17.
17. Kelly, M.P., Coldren, R.L., Parish, R.V., Dretsch, M.N., Russell, M.L. (2012).
Assessment of acute concussion in the combat environment. Arch Clin Neuropsychol
27, 375-388.
18. Kennedy, J.E., Leal, F.O., Lewis, J.D., Cullen, M.A., Amador, R.R. (2010).
Posttraumatic stress symptoms in OIF/OEF service members with blast-related and
non-blast-related mild TBI. NeuroRehabilitation 26, 223-231.
19. McDonald, S.D., Calhoun, P.S. (2010). The diagnostic accuracy of the PTSD
checklist: a critical review. Clin Psychol Rev 30, 976-987.
20. Tiet, Q.Q., Schutte, K.K., Leyva, Y.E. (2013). Diagnostic accuracy of brief PTSD
screening instruments in military veterans. J Subst Abuse Treat 45, 134-142.
21. Dolan, C.A., Adler, A.B. (2006). Military hardiness as a buffer of psychological
health on return from deployment. Mil Med 171, 93-98.
22. Phillips, C.J., Leardmann, C.A., Gumbs, G.R., Smith, B. (2010). Risk factors for
posttraumatic stress disorder among deployed US male marines. BMC Psychiatry 10,
52.
Page 21 of 27
Mary Ann Liebert, Inc, 140 Huguenot Street, New Rochelle, NY 10801
Journal of Neurotrauma
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review O
nly/Not for Distribution mTBI and Blast History
22
23. Stein, M.B., McAllister, T.W. (2009). Exploring the convergence of
posttraumatic stress disorder and mild traumatic brain injury. Am J Psychiatry 166,
768-776.
24. Schneiderman, A.I., Braver, E.R., Kang, H.K. (2008). Understanding sequelae
of injury mechanisms and mild traumatic brain injury incurred during the conflicts
in Iraq and Afghanistan: persistent postconcussive symptoms and posttraumatic
stress disorder. Am J Epidemiol 167, 1446-1452.
25. Lange, R.T., Brickell, T.A., Ivins, B., Vanderploeg, R.D., French, L.M. (2013).
Variable, not always persistent, postconcussion symptoms after mild TBI in U.S.
military service members: a five-year cross-sectional outcome study. J Neurotrauma
30, 958-969.
26. Vasterling, J.J., Brailey, K., Proctor, S.P., Kane, R., Heeren, T., Franz, M. (2012).
Neuropsychological outcomes of mild traumatic brain injury, post-traumatic stress
disorder and depression in Iraq-deployed US Army soldiers. Brit J of Sports Med 201,
186-192.
27. Dolan, S., Martindale, S., Robinson, J., Kimbrel, N.A., Meyer, E.C., Kruse, M.I.,
Morissette, S.B., Young, K.A., Gulliver, S.B. (2012). Neuropsychological sequelae of
PTSD and TBI following war deployment among OEF/OIF veterans. Neuropsychol
Rev 22, 21-34.
28. Mittal, D., Drummond, K.L., Blevins, D., Curran, G., Corrigan, P., Sullivan, G.
(2013). Stigma associated with PTSD: perceptions of treatment seeking combat
veterans. Psychiatr Rehabil J 36, 86-92.
Page 22 of 27
Mary Ann Liebert, Inc, 140 Huguenot Street, New Rochelle, NY 10801
Journal of Neurotrauma
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review O
nly/Not for Distribution mTBI and Blast History
23
29. Covassin, T., Schatz, P., Swanik, C.B. (2007). Sex differences in
neuropsychological function and post-concussion symptoms of concussed collegiate
athletes. Neurosurgery 61, 345-350.
30. Broshek, D.K., Kaushik, T., Freeman, J.R., Erlanger, D., Webbe, F., Barth, J.T.
(2005). Sex differences in outcome following sports-related concussion. J Neurosurg
102, 856-863.
Page 23 of 27
Mary Ann Liebert, Inc, 140 Huguenot Street, New Rochelle, NY 10801
Journal of Neurotrauma
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review O
nly/Not for DistributionTable 1. Summary of Demographic Data, mTBI Mechanism, and History of Medically
Diagnosed Blast mTBI.
Measures
History of Medically
Diagnosed Blast
mTBI (n= 19)
M (SD)
No History
(n= 61)
M (SD)
Total Sample
(N= 80)
M (SD)
Age* 31.05 (7.07) 27.54 (5.57)
Height (cm)* 180.61 (5.86) 176.59 (6.95)
Weight (kg) 86.56 (10.68) 82.11 (9.79)
# (%) # (%) # (%)
mTBI Mechanism
Blunt
Blast/Combination
Undocumented
4 (21%)
6 (32%)
9 (49%)
19 (31%)
11 (18%)
31 (51%)
23 (29%)
17 (21%)
40 (50%)
History of Blunt
mTBI
4 (21%) 22 (36%) 26 (33%)
Page 24 of 27
Mary Ann Liebert, Inc, 140 Huguenot Street, New Rochelle, NY 10801
Journal of Neurotrauma
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review O
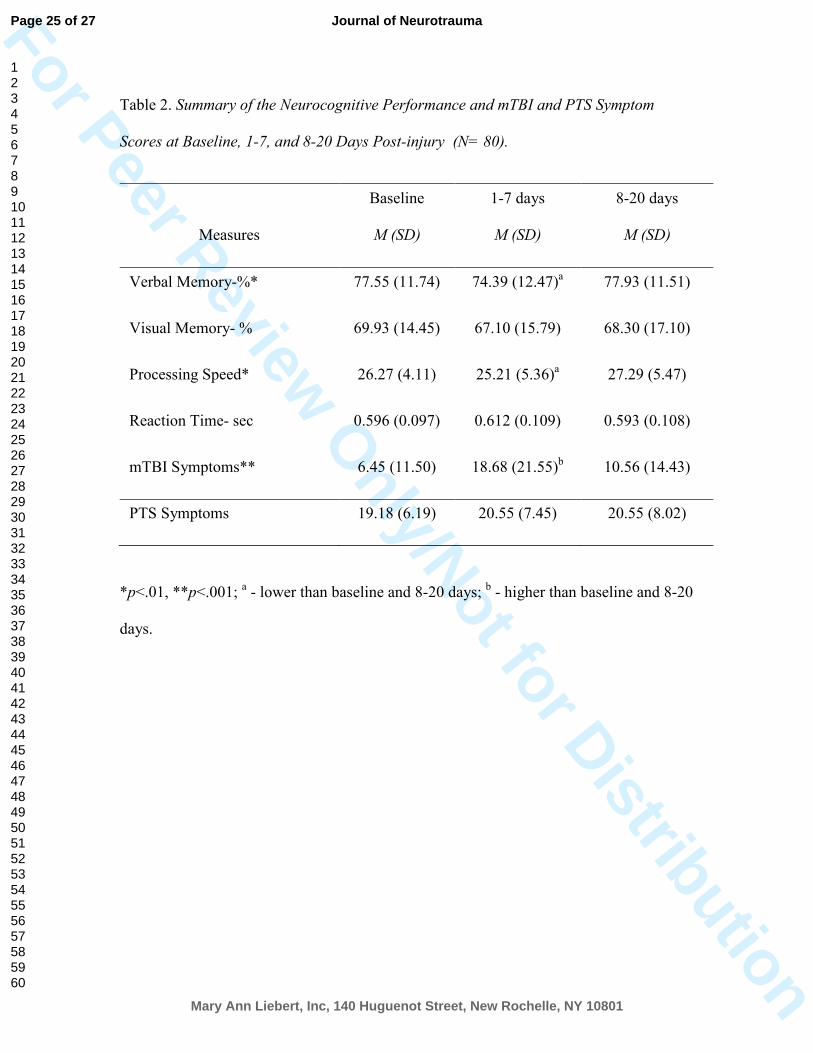
nly/Not for DistributionTable 2. Summary of the Neurocognitive Performance and mTBI and PTS Symptom
Scores at Baseline, 1-7, and 8-20 Days Post-injury (N= 80).
*p<.01, **p<.001; a - lower than baseline and 8-20 days;
b - higher than baseline and 8-20
days.
Measures
Baseline
M (SD)
1-7 days
M (SD)
8-20 days
M (SD)
Verbal Memory-%* 77.55 (11.74) 74.39 (12.47)a 77.93 (11.51)
Visual Memory- % 69.93 (14.45) 67.10 (15.79) 68.30 (17.10)
Processing Speed* 26.27 (4.11) 25.21 (5.36)a 27.29 (5.47)
Reaction Time- sec 0.596 (0.097) 0.612 (0.109) 0.593 (0.108)
mTBI Symptoms** 6.45 (11.50) 18.68 (21.55)b 10.56 (14.43)
PTS Symptoms 19.18 (6.19) 20.55 (7.45) 20.55 (8.02)
Page 25 of 27
Mary Ann Liebert, Inc, 140 Huguenot Street, New Rochelle, NY 10801
Journal of Neurotrauma
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review O
nly/Not for DistributionTable 3. Summary of the Interaction between Diagnosed History of Blast mTBI and Time
on Neurocognitive Performance, mTBI and PTS Symptoms (N= 80).
*p<.05
Measures/Groups
Baseline
M (SD)
1-7 days
M (SD)
8-20 days
M (SD)
Verbal Memory-%*
History of Blast mTBI
No History
80.92 (7.05)
77.55 (11.74)
70.25 (16.27)
75.67 (10.87)
76.70 (13.22)
78.31 (11.01)
Visual Memory- %
History of Blast mTBI
No History
69.96 (14.09)
69.93 (14.68)
66.36 (13.32)
67.33 (16.58)
64.93 (16.93)
69.35 (17.16)
Processing Speed
History of Blast mTBI
No History
26.12 (4.09)
26.32 (4.15)
23.02 (4.89)
25.90 (5.35)
26.35 (4.36)
27.58 (5.72)
Reaction Time- sec
History of Blast mTBI
No History
0.577 (0.068)
0.602 (0.104)
0.635 (0.069)
0.604 (0.118)
0.605 (0.093)
0.589 (0.113)
mTBI Symptoms
History of Blast mTBI
No History
6.53 (9.78)
6.43 (12.03)
24.11 (22.66)
16.98 (21.09)
9.11 (10.23)
11.02 (15.56)
PTS Symptoms
History of Blast mTBI
No History
18.21 (3.18)
19.48 (6.86)
20.84 (6.34)
20.46 (7.81)
20.36 (8.26)
20.61 (8.01)
Page 26 of 27
Mary Ann Liebert, Inc, 140 Huguenot Street, New Rochelle, NY 10801
Journal of Neurotrauma
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review O
nly/Not for Distribution
254x190mm (72 x 72 DPI)
Page 27 of 27
Mary Ann Liebert, Inc, 140 Huguenot Street, New Rochelle, NY 10801
Journal of Neurotrauma
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960