Jess ctev
43
FUNCTIONAL OUTCOME IN THE MANAGEMENT OF RECURRENT,RESISTANT AND NEGLECTED CASES OF CTEV TREATED BY JESS Dr.MADA DAVIS PG STUDENT MCH,TVPM
-
Upload
sitanshubarik -
Category
Health & Medicine
-
view
642 -
download
7
Transcript of Jess ctev

FUNCTIONAL OUTCOME IN THE MANAGEMENT OF
RECURRENT,RESISTANT AND NEGLECTED CASES OF CTEV
TREATED BY JESS
Dr.MADA DAVIS
PG STUDENT
MCH,TVPM


INTRODUCTION
• Idiopathic club foot is one of the oldest and commonest congenital deformity of mankind, ever since man has adopted the erect posture.
• It occurs in variable severity and some of the mobile feet are corrected well with manipulation and stretching. Nearly half the feet are rigid and do not show full correction with, conservative management.

• In this study the patients were operated and followed by Dr. B.B. Joshi’s method of controlled differential distraction. The study includes 15 patients (18 foot) which were treated by the principles of controlled differential distraction.








Lateral film with the foot held in maximal dorsi-flexionTalocalcaneal angle(A) - normal range 25-50º abnormal if <25º

AIMS AND OBJECTIVES
• To assess the efficacy of differential distraction as a method of treatment in CTEV.
• To evaluate various technical problems, complications of techniques and to suggest ways to overcome them.
• To find out applicability in relapsed and neglected CTEV.
• To work out the cost effectiveness of this method v/s surgery.
• To critically assess the results based on clinical and radiological findings.
• To draw clear cut indication and contra-indication of this method and to evaluate various merits and demerits of differential distraction method.

MATERIALS AND METHODS
• This study includes 15 patients (with 18 feet) with old, recurrent and resistant cases of clubfoot deformities treated by Joshi's external stabilizing system, at Medical college Hospital attached to Medical College, Thiruvananthapuram.
• Average follow-up was of 24 weeks (ranging from 16-36 weeks). There were 11 male and 4 female patients. The age at the time of operation ranged from 5 months to 5 years.

MATERIALS AND METHODS
• Complete clinical and radiological assessment of each foot was made and deformity combination was laid down in each foot as per the criteira given by George. W.Simons.
• The time taken for correction by distraction ranged from 4 weeks to 10 weeks with an average of 6 weeks. The fixator frame was further retained for 1 ½ months.

MATERIALS AND METHODS
• All patients had preoperative talocalcaneal index measured on X-ray. Post-operatively, after the removal of the fixator talocalcaneal index was measured.
• The results were assessed on findings of clinical appearance of the feet, mobility of the joints, functional activity and the radiological assessment. Results were
classified into two groups - satisfactory / unsatisfactory

OBSERVATION AND ANALYSIS
• Sex Ratio : In this study out of 15 cases, 11 were males and 4 females. The sex ratio being 2.75:1
• Laterality : Out of 15 cases 7 were bilateral and 8 were unilateral.
• Family history : No cases had a family history. No history of twins in the series. In 4 cases there is history of consanguinous marriage.
• Age at surgery : Age of the patient at the time of surgery varied from 5 months to 5 years.
• Duration of the follow up : In this study, the duration of follow up ranges from 3 months to 18 months . Average period of follow up was 6 months.

MALE AND FEMALE RATIO
Total no of cases
Total no of feet
Male FemaleMale :
Female ratio
15 18 11 4 2.75:1
11
4
0
2
4
6
8
10
12
Male Female

UNILATERAL / BILATERAL
Total No of cases
Unilateral Bilateral Ratio
Rt. Lt.
15 8 4 3 4:1

AGE DISTRIBUTION
Age group (in years) No of casesPercentag
eNo. of feet
4 months – 3 years 13 86.67 16 feet
3 year – 5 year 2 13.33 2 feet
13
2
4 months - 3 years 3 years - 5 year Slice 3

PREVIOUS PROCEDURE
Previous Procedures No.of casesPercentag
e
Postero Medial Release 2 13.33
Serial Casting 7 46.67
None 6 40.0
2
7
6
0
1
2
3
4
5
6
7
Postero medial release Serial Casting Non

DURATION OF DISTRACTION
Maximum Minimum Average
8 weeks 6 weeks 7 weeks

RESULTSThe results were graded as satisfactory or unsatisfactory depending upon SIMONS CRITERIA (1985)
S.No Satisfactory Unsatisfactory
1 Symptoms NoneMinimal to moderate
pain with activity
2Appearance of
hindfootNormal to mild deformity
Moderate to significant residual
deformity
3. Forefoot adduction Mild Severe
4.Functional weakness
of triceps suraeNone or mild
Cannot support weight on toes
5.Range of motion at
ankle
Dorsiflexion greater than 10o , plantar flexion
greater than 15o
Dorsiflexion less than 10o, plantar flexion
less than 15o.
6.Range of motion at
subtalar jointPresent Nil
7. Additional treatmentNone, cast or minor
surgery
Freq. treatment with cast or major
surgery.
8. Complications Minor Major
Radiologically, the talocalcaneal angle in stress or weight bearing AP & lateral views should be more than 150 to call a result to be satisfactory.

Results
• Equinus at the ankle : The feet showed well corrected mobile ankle joints. The post – operative range of motion at the ankle was an average of 40o, with 25o of plantar flexion and 15o of dorsiflexion.
• Fore foot adduction :This was assessed clinically and radiologically. Out of 18 feet, 4 feet showed varus deformity of less than 10o.
• Hind foot varus : All but one patient had a good correction of heel varus.

RADIOLOGICAL FINDINGS The talo-calcaneal index was measured both preoperatively and post operatively. The findings are shown below.
Average pre-operative
Average Post –operative
Normal values
A.P. 13o 20o 25-40
Lateral 20o 35o 25-50o
T.C. Index 33o 55o >40o
Radiologically, the talocalcaneal angle in stress or weight bearing AP and lateral views should be more than 15o to call a result to be satisfactory.

ASSESSMENT OF RESULTS • The results were assessed according to George Simons criteria. They are
classified into Satisfactory (Excellent, Good and Fair) and Unsatisfactory (Poor). In our series we had 14 satisfactory and 1 unsatisfactory result.
Excellent : Clinically and radiologically 100% correction Clinical appearance of foot normal
Good : Foot clinically normal70% radiological correction
Fair : Clinically one deformity partially persisting Radiological correction between 50-70%
Poor : Clinically foot doesn’t appear to be normal. Radiological correction less than 50%.
Satisfactory (Excellent, Good, Fair)Unsatisfactory (Poor)

PRE OPERATIVE XRAY OF 9 MNTH OLD CHILD

POST OPERATIVE XRAY OF THE SAME CHILD

POST OPERATIVE XRAY

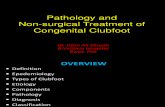
PRE OP PICTURE OF 9 MNTH OLD CHILD

POST OP PICTURE SHOWING CORRECTION OF DEFORMITIES

PRE OP PICTURE OF ONE YR OLD SHOWING EQUINUS VARUS AND ADDUCTION

POST OP PICTURE SHOWING CORRECTION OF DEFORMITIES

PRE OP PICTURE-NOTE FORE FOOT ADDUCTION

NOTE CORRECTION OF FOREFOOT ADDUCTION

DISCUSSION
The results of the present series can be discussed under the following headings.
1. Age at Operation :– We compared the results of surgery done at younger age to
those done at older age. In our series, operation performed in the age group 5 months – 2 years, the results were good. In the older age group of 3-5 years, the results were fair.
2. Variety of club feet :– In the recurrent varieties, application of the technique of
differential distraction appears to be sound and in resistant varieties the results of differential distraction is superior to any other technique.

3. Forefoot adduction:40% of children in our series had clinical residual forefoot adduction but, all had pliable metatarsals and adductors which required nothing other than an orthotic device.

POST OPERATIVE CLINICO RADIOLOGICAL RESULTS
Result No. of Cases Percentage
Satisfactory 14 93.33
Unsatisfactory 1 6.67
Satisfactory - Excellent, Good, Fair.Unsatisfactory - Poor.

Complications associated with JESS Distractor
• Contamination of the assembly with urine and faeces.
• Temporary edema of the foot.
• Supericial pin tract infection.
• Flexion contracture of the toes.

TECHNICAL PROBLEMS OF DIFFERENTIAL DISTRACTION :
• As we used indigenously made link joints and distractors, mechanical problems with link joints were the main time consuming factor during the surgery. But later, all the problems were overcome and average time for surgery was 1 hour.
• In younger age groups, 4 mm distractors with 1 mm pitch are well and good. But in higher age group, 6 mm distractors with 1.86 mm pitch are required. Daily distraction of 1.86 mm is not tolerated by children. Thus rate of distraction has to be maintained at 1 mm daily.
• Passing the distal metatarsal K wires.

TECHNICAL PROBLEMS OF DIFFERENTIAL DISTRACTION :
– Skin necrosis at the sole – foot plate interface : This could be overcome by regular cleaning with antiseptics.
– Patient compliance : In almost all the cases the child was very much irritable towards the end of the treatment.
– The anterior stabilization rod needs to be refitted every two weeks to accommodate the equinus correction.
– Over-stretching of the skin over the medial and posterior aspect of the foot in severely deformed club foot showed signs of necrosis during the distraction phase which had to be overcome by stopping the distraction for 2-3 days.

CONCLUSION
• From this study it could be concluded that
JESS is an excellent technique in the management of recurrent, resistant and neglected cases of CTEV especially when it is done at an early age.

THANK YOU