
Jeannie Randles RN Grad cert wound care PG Cert &PG Dip Primary Health.
29
WOUND ASSESSMENT USING TIME 2013 Jeannie Randles RN Grad cert wound care PG Cert &PG Dip Primary Health
-
Upload
anabel-owens -
Category
Documents
-
view
215 -
download
2
Transcript of Jeannie Randles RN Grad cert wound care PG Cert &PG Dip Primary Health.
WOUND ASSESSMENT USING TIME 2013
Jeannie Randles RNGrad cert wound care
PG Cert &PG Dip Primary Health
Assess whole patient not hole in the patient
outline
documentation Wound healing process Chronic wounds Wound assessment using TIME

Documentation !!!
Assess wound assessment
forms and notes Re assess Read previous
documentation Care plan (up to date
and clear) Outcomes (up to date
and appropriate) If its not written it
didn’t happen!!!!

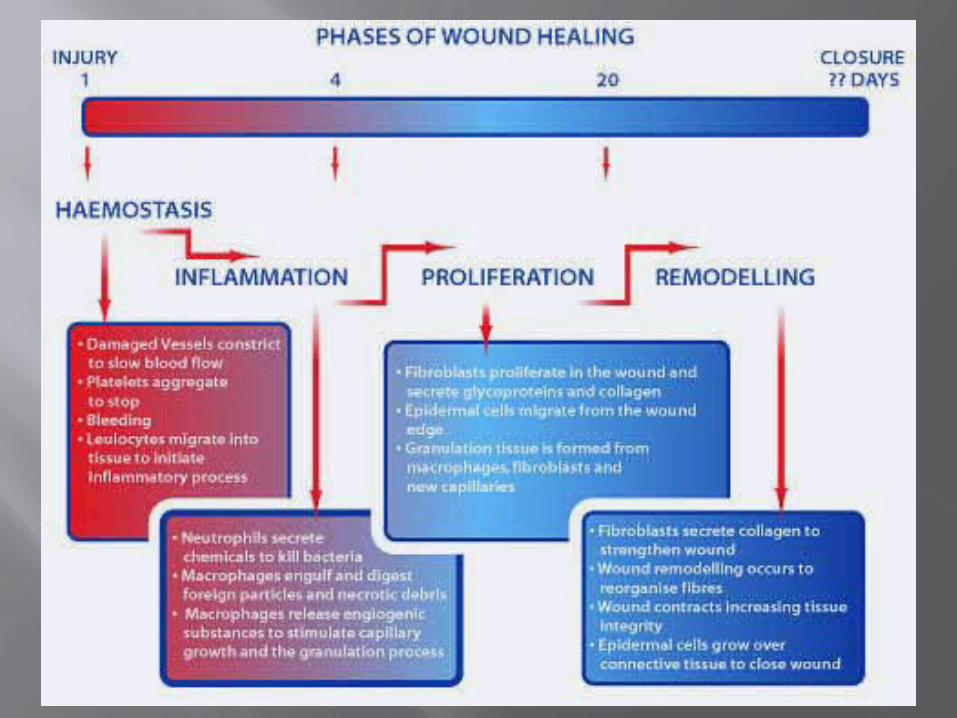
Wound healing process
cascade of events Haemostasis Inflammation Proliferation Remodelling
Not always in order

haemostasis
Arrest bleeding Vasoconstriction Compression of
injured vessels Platelet activation Fibrin production Clot formation

Inflammation
Vasodilation Leukocyte supplant
platelets White cells
predominant for 1st three days
Monocytes become macrophages and debride the wound

proliferation
Fibroblasts migrate from wound margins Generate cytokines, growth factors,
collagen Capillary loops form(angiogenesis) Inflammation reduces

Types of wound healing
Primary intention – surgical closure, minimises connective tissue deposition, resulting in rapid healing
Secondary intention – wounds that are left open and heal by deposition of connective tissue resulting in increased scar formation
Tertiary (delayed primary) – delayed closure of wounds complicated by infection.
Chronic wounds
• “Chronic wounds are wounds that fail to progress through an orderly and timely sequence of repair”
• Often stay in inflammatory stage or move between stages
http://www.worldwidewounds.com/2004/october/Enoch-Part2/Alternative-Enpoints-To-Healing.html Last Modified: Thursday, 21-Oct-2004 15:19:52 BST
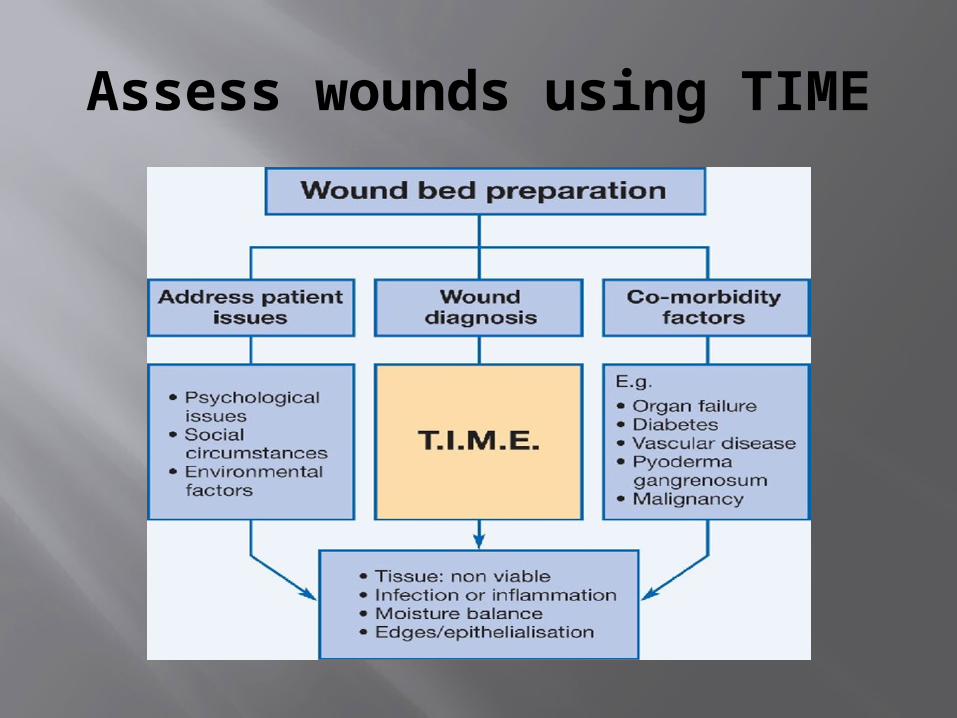
Assess wounds using TIME
TIME
T is for tissue Slough Granulation, healthy or dull/friable Epithelial islands Necrotic tissue Tendon or bone exposed Describe tissue seen in detail and in %’s

slough

granulation

Epithelial islands

Necrotic tissue

Tendon exposed
Inflammation/infection
I is for inflammation or infection
↑ erythema ↑ exudates ↑ pain ↑ wound size ↑ malodour Delay in healing
Tissue becomes friable
↑slough Undermining Bridging pocketing

Infected

Moisture balance
Ideal wound healing environment is moist, not wet and not dry (some exceptions apply)
Describe exudates i.e. amount, colour, odour
Describe effect of exudates i.e. maceration, desiccation
Frequency of dressing changes and condition of dressings at changes i.e. saturated or dry

Macerated

Desiccated
Edges/epethelialisation
E is for edges/epethelialisation Rolled Epethelialising Punched out Sloped Undermining
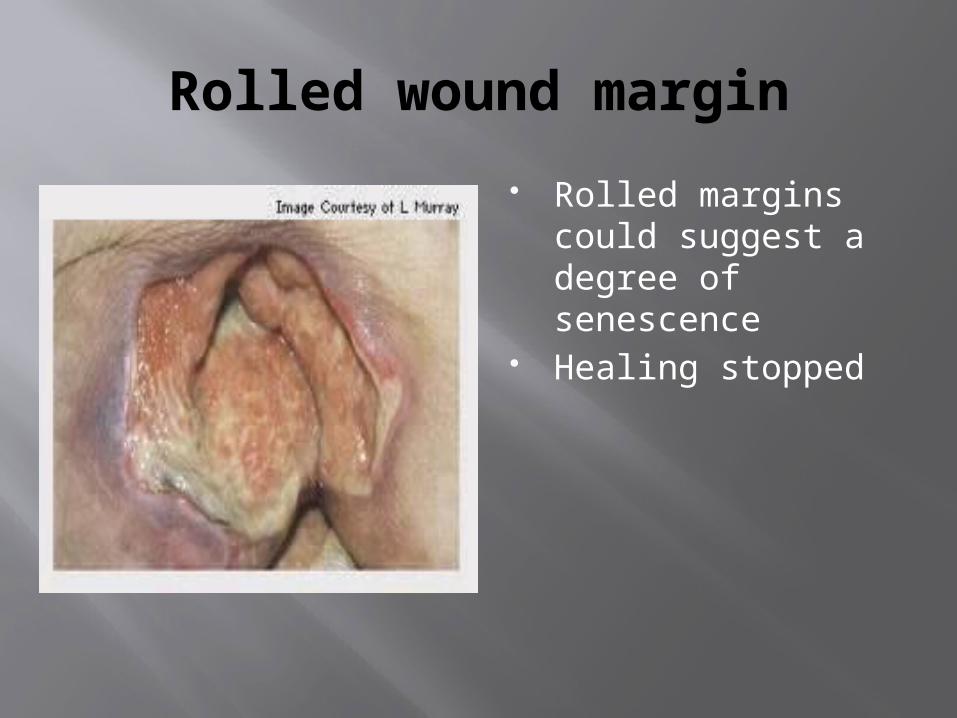
Rolled wound margin
Rolled margins could suggest a degree of senescence
Healing stopped

Epethelialising

Punched out

Irregular shaped wound margins
Conclusion
Wounds are dynamic and need constant re assessment
Excellent wound care follows excellent wound assessment
Clear documentation is a crucial component of wound assessment
Excellent wound assessment involves the whole of the patient and not just the hole in the patient


















