Japanese Pediatric Acupuncture
18
V aus: Birch, Shonishin: Japanese Pediatric Acupuncture (ISBN 9783131500618) © 2011 Georg Thieme Verlag Foreword Traditional East Asian Medicine (TEAM) boasts a rich variety of literary genres. The medical dis- course (yi lun 醫論), the case record (yi an醫案), and the modern textbook are just a few of the most prominent styles of TEAM writing today. Stephen Birch’s Shonishin: Japanese Pediatric Acupuncture certainly qualifies as a textbook, and it is to some extent a medical discourse and a collection of case records. But it also belongs to another venerable genre of the TEAM literature that is still in its infancy in the West. In many ways, this is a “clinical insights” memoir. An entire generation of TEAM practitioners in the West have now fully matured as master clini- cians. With 30 or more years’ experience in adapt- ing this medicine to practice in the West, this gen- eration has begun sharing their clinical insights with the rest of us. The present volume is a rich and very personal expression of this process of trans- mission by an eminent member of this generation. In this, it also represents the full blossoming of sho- nishin’s development and assimilation into TEAM in the West. It is ample evidence that we have truly made this medicine our own. As much and perhaps more than any other speci- alty of TEAM practice, shonishin rewards knack over theory. It is easy to learn but difficult to truly master. Each practitioner must ultimately “get” the tech- nique in his or her hands. A skilled teacher, how- ever, knows how to effectively communicate that knack to others. Steve brings the sensibilities of a professionally trained clinical researcher to the task of unpacking the shonishin practice with consum- mate skill. This is evident in both his writing and in the DVD that accompanies the text. The two media combine to bring the techniques vividly to life. Children are remarkably responsive to thera- peutic influence, making them much more prone to overtreatment than their adult counterparts. Though questions of optimal therapeutic dosage are familiar territory for all experienced clinicians, Steve has thought this issue out and articulated it with an unprecedented depth and clarity. The clini- cal ramifications of his dosing model extend far beyond pediatrics and into medical practice as a whole, almost regardless of the modality being used. Nowhere in clinical practice is the demand for fluid adaptability to changing circumstances more pressing than in pediatrics. Steve discusses this often unspoken aspect of the therapeutic encounter as the “dance of treatment. ” Once again, one’s sen- sitivity to optimum dosing lies at the heart of the matter. It is a dance that embraces moment-to- moment decisions concerning which technique to use, what tool to administer that technique with, precisely how much of that technique to adminis- ter, and with what degree of force. Then too, it is a dance largely choreographed by a squirming, some- times squawking partner, and one typically over- seen by a pensive parent hovering in the wings. The themes of therapeutic dose and the fluid dance of treatment run throughout the text. A brief glance at the table of contents reveals the compre- hensive discussions of pediatric needling tech- niques, and expositions on individual diseases ac- companied by prescriptive treatment strategies requisite for a textbook on a pediatric specialty. But the entire book is constructed around case examples. Many of these are from Steve’s own prac- tice illustrating his personal approach to both the topic at hand, and its relationship to the dose and the dance. Many other case records are those of col- leagues, illustrating a variety of creative approaches to treatment. It is a technique that is best trans- mitted within the context of specific examples as opposed to theoretical abstractions, though both are necessary for a full understanding In some ways, shonishin isn’t much to look at. It is an unassuming technique that can easily leave one wondering how a bit of stroking, a little tap- ping, and perhaps even a touch of tickling could have any real therapeutic value. Yet experienced shonishin practitioners know how almost miracu- lously effective it can be. It can work where biome- dical, naturopathic, and other TEAM modalities have fallen short and it combines easily with all of them. In this book, Steve has shown us what a potent tool of efficacy and a thing of beauty the sho- nishin dance can be. Charles Chace Boulder, Colorado
Transcript of Japanese Pediatric Acupuncture

Thieme-VerlagFrau Kurz
Sommer-DruckFeuchtwangen
Birch:Shonishin
WN026347/01/01TN 150061
11.5.2011Birch_Titelei
V
aus: Birch, Shonishin: Japanese Pediatric Acupuncture (ISBN 9783131500618) © 2011 Georg Thieme Verlag
Foreword
Traditional East Asian Medicine (TEAM) boasts arich variety of literary genres. The medical dis-course (yi lun醫論), the case record (yi an醫案), andthe modern textbook are just a few of the mostprominent styles of TEAM writing today. StephenBirch’s Shonishin: Japanese Pediatric Acupuncturecertainly qualifies as a textbook, and it is to someextent a medical discourse and a collection of caserecords. But it also belongs to another venerablegenre of the TEAM literature that is still in itsinfancy in theWest. In many ways, this is a “clinicalinsights”memoir.
An entire generation of TEAM practitioners inthe West have now fully matured as master clini-cians. With 30 or more years’ experience in adapt-ing this medicine to practice in the West, this gen-eration has begun sharing their clinical insightswith the rest of us. The present volume is a rich andvery personal expression of this process of trans-mission by an eminent member of this generation.In this, it also represents the full blossoming of sho-nishin’s development and assimilation intoTEAM inthe West. It is ample evidence that we have trulymade this medicine our own.
Asmuch and perhapsmore than any other speci-alty of TEAM practice, shonishin rewards knack overtheory. It is easy to learn but difficult to trulymaster.Each practitioner must ultimately “get” the tech-nique in his or her hands. A skilled teacher, how-ever, knows how to effectively communicate thatknack to others. Steve brings the sensibilities of aprofessionally trained clinical researcher to the taskof unpacking the shonishin practice with consum-mate skill. This is evident in both his writing and inthe DVD that accompanies the text. The two mediacombine to bring the techniques vividly to life.
Children are remarkably responsive to thera-peutic influence, making them much more proneto overtreatment than their adult counterparts.Though questions of optimal therapeutic dosageare familiar territory for all experienced clinicians,Steve has thought this issue out and articulated itwith an unprecedented depth and clarity. The clini-cal ramifications of his dosing model extend farbeyond pediatrics and into medical practice as awhole, almost regardless of themodality being used.
Nowhere in clinical practice is the demand forfluid adaptability to changing circumstances morepressing than in pediatrics. Steve discusses thisoften unspoken aspect of the therapeutic encounteras the “dance of treatment.” Once again, one’s sen-sitivity to optimum dosing lies at the heart of thematter. It is a dance that embraces moment-to-moment decisions concerning which technique touse, what tool to administer that technique with,precisely how much of that technique to adminis-ter, and with what degree of force. Then too, it is adance largely choreographed by a squirming, some-times squawking partner, and one typically over-seen by a pensive parent hovering in thewings.
The themes of therapeutic dose and the fluiddance of treatment run throughout the text. A briefglance at the table of contents reveals the compre-hensive discussions of pediatric needling tech-niques, and expositions on individual diseases ac-companied by prescriptive treatment strategiesrequisite for a textbook on a pediatric specialty.
But the entire book is constructed around caseexamples. Many of these are from Steve’s own prac-tice illustrating his personal approach to both thetopic at hand, and its relationship to the dose andthe dance. Many other case records are those of col-leagues, illustrating a variety of creative approachesto treatment. It is a technique that is best trans-mitted within the context of specific examples asopposed to theoretical abstractions, though bothare necessary for a full understanding
In some ways, shonishin isn’t much to look at. Itis an unassuming technique that can easily leaveone wondering how a bit of stroking, a little tap-ping, and perhaps even a touch of tickling couldhave any real therapeutic value. Yet experiencedshonishin practitioners know how almost miracu-lously effective it can be. It can work where biome-dical, naturopathic, and other TEAM modalitieshave fallen short and it combines easily with all ofthem. In this book, Steve has shown us what apotent tool of efficacy and a thing of beauty the sho-nishin dance can be.
Charles ChaceBoulder, Colorado
Contents
Section 1 Overview and History
1 Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
2 History and Theory . . . . . . . . . . . . . . . . . . . . . . . 6Kanmushisho (疳虫証) orKannomushisho (疳の虫証) . . . . . . . . . . . . . . . . 11ShonishinToday . . . . . . . . . . . . . . . . . . . . . . . . . . 12
Section 2 Treatment Principles and Tools ofTreatment
3 General Considerations in the Treatment ofChildren . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17
4 AModel for Judging the Dosage Needs ofPatients . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19The Therapeutic Dose—AConceptual Model . 19The Sensitive Patient . . . . . . . . . . . . . . . . . . . . . . 20Explanations of Increased Sensitivity . . . . . . . . 21
5 Assessing Changes, Recognizing andCorrecting Problems of Overdose . . . . . . . . . 24Reactions to Over-treatment . . . . . . . . . . . . . . . 24Modifying Treatment Methods to Regulatethe Dose of Treatment and Deliver TreatmentSuccessfully . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27Final Thoughts on the Issue of Regulating theDose of Treatment . . . . . . . . . . . . . . . . . . . . . . . . 28
6 Basic ShonishinTreatment Tools . . . . . . . . . . . 29Tools Used for Tapping . . . . . . . . . . . . . . . . . . . . 29Tools Used for Stroking/Rubbing . . . . . . . . . . . 32Tools Used for Pressing . . . . . . . . . . . . . . . . . . . . 35Tools Used for Scratching . . . . . . . . . . . . . . . . . . 35Needle Sets . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 39Most Recommended Tools . . . . . . . . . . . . . . . . . 41Care of the Tools . . . . . . . . . . . . . . . . . . . . . . . . . 41Disposable Tools . . . . . . . . . . . . . . . . . . . . . . . . . 41Treatment Applications . . . . . . . . . . . . . . . . . . . 42Monitoring and Assessing Treatment Effects . 42
Section 3 Root Treatment Approaches andTechniques
7 The Core TreatmentModel . . . . . . . . . . . . . . . 45Precautions and Contraindications of the CoreNon-pattern-based Root Treatment . . . . . . . . . 45Techniques for Basic Treatment . . . . . . . . . . . . 46Preferences, Styles, and Approaches . . . . . . . . 50
8 Home Treatment and Parental Participation 52Goals . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 52Precautions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 53The Basic Method . . . . . . . . . . . . . . . . . . . . . . . . . 53
9 Pattern-based Root Treatment:MeridianTherapy Applied to Adults . . . . . . . 55Basic Theories of MeridianTherapy . . . . . . . . . . 55MeridianTherapy Treatment Principles . . . . . . 57MeridianTherapy Diagnostic Methods andPatterns . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 57MeridianTherapy Treatment and TreatmentTechniques . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 58
10 Pattern-based Root Treatment:MeridianTherapy Applied to Children . . . . . 61Diagnosis to Select the Primary Pattern inChildren . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 61Diagnosis to Select Additional Steps of RootTreatment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 62Modifying Point Selection for Treatment ofthe Primary Patterns . . . . . . . . . . . . . . . . . . . . . . 62TreatmentMethods in MeridianTherapy . . . . . 63Treatment Technique with Spring-loadedTeishin . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 64Point Location of MainTreatment Points . . . . . 65Five Phase Correspondences and ClinicalPractice . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 66Assessing Treatment Effectiveness . . . . . . . . . . 67
Thieme-VerlagFrau Kurz
Sommer-DruckFeuchtwangen
Birch:Shonishin
WN026347/01/01TN 150061
11.5.2011Birch_Titelei
X
aus: Birch, Shonishin: Japanese Pediatric Acupuncture (ISBN 9783131500618) © 2011 Georg Thieme Verlag

Section 4 Symptomatic Treatment Approachesand Techniques
11 Needling . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 71Needle Types . . . . . . . . . . . . . . . . . . . . . . . . . . . . 71Needle Sensations and Timing of the Needling 72Needle Insertion . . . . . . . . . . . . . . . . . . . . . . . . . . 74
12 Dermal Needles and Associated Techniques 76Ryu—Press-spheres, Empishin—Press-tackNeedles, and Hinaishin—Intra-dermalNeedles . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 76Selecting between Use of Intra-dermalNeedles, Press-tack Needles, andPress-spheres . . . . . . . . . . . . . . . . . . . . . . . . . . . . 77Precautions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 77Application of Press-spheres, Press-tackNeedles, and Intra-dermal Needles . . . . . . . . . . 79
13 Moxa:Okyu (DirectMoxa) and Chinetsukyu(WarmMoxa) . . . . . . . . . . . . . . . . . . . . . . . . . . . 80Okyu—The Physiology of Direct Moxa . . . . . . . 81Chinetsukyu—WarmMoxa . . . . . . . . . . . . . . . . . 83
14 Kyukaku—Cupping . . . . . . . . . . . . . . . . . . . . . . . 84
15 Shiraku—Bloodletting (Jing Points andVascular Spiders) . . . . . . . . . . . . . . . . . . . . . . . . 85Jing Point Bloodletting . . . . . . . . . . . . . . . . . . . . . 85Vascular Spider Bloodletting . . . . . . . . . . . . . . . 86
16 Point Location—Location of Extra Points forSymptomatic Treatment . . . . . . . . . . . . . . . . . 88Josen . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 88Uranaitei . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 88Shitsumin . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 88Asthma Shu Point . . . . . . . . . . . . . . . . . . . . . . . . . 88“Stop Coughing” Point . . . . . . . . . . . . . . . . . . . . 89Lateral Pigen Point . . . . . . . . . . . . . . . . . . . . . . . . 89Moving LR-1 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 89
Section 5 Treatment of Specific Problems/Diseases
17 Introduction to the Treatment of SpecificProblems/Diseases . . . . . . . . . . . . . . . . . . . . . . 93How to Use these Treatment Chapters . . . . . . 95Putting Your Treatment Together into aSystem . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 95Sources Used in the TreatmentChapters of this Book . . . . . . . . . . . . . . . . . . . . . 99
18 Respiratory Problems . . . . . . . . . . . . . . . . . . . 101Asthma . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 101Additional Respiratory Conditions . . . . . . . . . 113
19 Skin Disease . . . . . . . . . . . . . . . . . . . . . . . . . . . . 115Eczema . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 115Atopic Dermatitis . . . . . . . . . . . . . . . . . . . . . . . . 127Urticaria . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 131
20 Digestive Problems . . . . . . . . . . . . . . . . . . . . . 134Constipation . . . . . . . . . . . . . . . . . . . . . . . . . . . . 134Diarrhea . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 139Abdominal Pain . . . . . . . . . . . . . . . . . . . . . . . . . 143Stomach Problems . . . . . . . . . . . . . . . . . . . . . . . 146Additional Digestive Problems . . . . . . . . . . . . 151
21 Behavioral, Emotional, or Sleep Problems 153Kanmushisho—the Cranky Child . . . . . . . . . . . 153Stress . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 162Further Emotional/BehavioralProblems . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 163
22 Urinary Disturbances . . . . . . . . . . . . . . . . . . . 164General Approach for Patients with UrinaryProblems . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 168Most Likely Pattern-based Root Diagnosis . . . 168Typical Non-pattern-based Root Treatment . 169Recommendations for SymptomaticTreatment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 169Integrating the Pattern-based and CoreNon-pattern-based Root Treatments withNeedling and Moxa SymptomaticTreatments . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 170Other Considerations . . . . . . . . . . . . . . . . . . . . 172Further Case Histories . . . . . . . . . . . . . . . . . . . . 172
23 Ear and Nose Problems . . . . . . . . . . . . . . . . . . 177Otitis Media—Ear Infections . . . . . . . . . . . . . . . 177Nasal Congestion . . . . . . . . . . . . . . . . . . . . . . . . 183Sinusitis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 188
24 Developmental Problems . . . . . . . . . . . . . . . 190General Approach for the Treatment ofChildren with Developmental Problems . . . . 191Most Likely Pattern-based Root Diagnosis . . . 191Typical Non-pattern-based Root Treatment . 192Recommendations for SymptomaticTreatment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 192Other Considerations . . . . . . . . . . . . . . . . . . . . 193Further Case Histories . . . . . . . . . . . . . . . . . . . . 193
Thieme-VerlagFrau Kurz
Sommer-DruckFeuchtwangen
Birch:Shonishin
WN026347/01/01TN 150061
11.5.2011Birch_Titelei
Contents XI
aus: Birch, Shonishin: Japanese Pediatric Acupuncture (ISBN 9783131500618) © 2011 Georg Thieme Verlag
25 Weak Constitution . . . . . . . . . . . . . . . . . . . . . 203The LungWeak Constitution Patient . . . . . . . 204The SpleenWeak Constitution Patient . . . . . . 204The KidneyWeak Constitution Patient . . . . . 204The LiverWeak Constitution Patient . . . . . . . 204General Approach for Patients withWeakConstitution . . . . . . . . . . . . . . . . . . . . . . . . . . . . 205Goals of Treatment . . . . . . . . . . . . . . . . . . . . . . 206Root Treatment for the LungWeakConstitutionType . . . . . . . . . . . . . . . . . . . . . . . . 206Root Treatment for the SpleenWeakConstitutionType . . . . . . . . . . . . . . . . . . . . . . . . 207Root Treatment for the KidneyWeakConstitutionType . . . . . . . . . . . . . . . . . . . . . . . . 207Root Treatment for the LiverWeakConstitutionType . . . . . . . . . . . . . . . . . . . . . . . . 208Further Case Histories . . . . . . . . . . . . . . . . . . . . 209
26 Recurrent Infections . . . . . . . . . . . . . . . . . . . . 218Recurrent Respiratory Tract Infections . . . . . . 218Candida Albicans Infection . . . . . . . . . . . . . . . . 227
27 Improving Vitality . . . . . . . . . . . . . . . . . . . . . . 230Goals of Treatment in Complicated Cases . . . 234General Approach to Improve Vitality . . . . . . 234Typical Non-pattern-based RootTreatment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 235Other Supportive Treatments . . . . . . . . . . . . . 235Other Considerations . . . . . . . . . . . . . . . . . . . . 235Further Case History . . . . . . . . . . . . . . . . . . . . . 236
28 Recommendations for Treatment of Otherand Less Commonly Seen Problems . . . . . . 238The Child with Fever . . . . . . . . . . . . . . . . . . . . . 238Teething Problems . . . . . . . . . . . . . . . . . . . . . . 240Infectious Diseases . . . . . . . . . . . . . . . . . . . . . . 240Tonsillitis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 241Mumps . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 241Nervous Conditions . . . . . . . . . . . . . . . . . . . . . . 242Neurological Conditions . . . . . . . . . . . . . . . . . . 242Kidney Diseases . . . . . . . . . . . . . . . . . . . . . . . . . 244Postnatal Lethargy with Lack ofSucking Reflex . . . . . . . . . . . . . . . . . . . . . . . . . . 244Surgical Conditions . . . . . . . . . . . . . . . . . . . . . . 245
29 Combining TreatmentMethods . . . . . . . . . . 246
Appendix . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 251
Glossary of ShonishinTerminology . . . . . . . . . . . 252
Additional Information . . . . . . . . . . . . . . . . . . . . . 254Treatment Equipment . . . . . . . . . . . . . . . . . . . . 254Educational . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 254
Bibliography . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 255
Index . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 257
Thieme-VerlagFrau Kurz
Sommer-DruckFeuchtwangen
Birch:Shonishin
WN026347/01/01TN 150061
11.5.2011Birch_Titelei
XII Contents
aus: Birch, Shonishin: Japanese Pediatric Acupuncture (ISBN 9783131500618) © 2011 Georg Thieme Verlag
stand that the practitioners of that time wouldhave had the same or greater problems than wehave today, trying to insert needles into emotional,frightened, unhappy, resistant, and restless,movingchildren. Why do I say greater problems? Becauseneedle technology was not at all as it is today, andthe needles available in the 1600s were signifi-cantly thicker and had a rougher surface than whatis available now. Nobody enjoys treating childrenwhen they are crying, screaming, resisting, andfighting with you. Thus, it is easy to understandwhy the developers of shonishin would have beenkeen to look for a different approach, so that theycould treat children more comfortably, and thechild would remain calmer and parents lessstressed. The motivations for developing the sys-tem are, I think, quite clear.
Given this kind of motivation it is still necessaryto understand how this approach developed bybriefly discussing historical trends within the lar-ger context of Traditional East Asian Medicine, orTEAM for short. The term “TEAM” refers to all thosetherapies and approaches that arose in East Asiaand were strongly influenced by the early Chinesemedicine qi-based theory of systematic correspon-dence. It thus includes diverse practices such asherbal medicine, acupuncture, moxibustion, cup-ping, bloodletting, and massage (Birch and Felt1999). TEAM started in China, and evolved thereinto many different strands and approaches. After
spreading to neighboring countries such as Japan,Korea, and Vietnam, adaptations and new interpre-tations emerged from those countries. Today TEAMembraces themultitude of practice styles and treat-ment approaches that can be found throughoutChina, Taiwan, Japan, Korea, and their offshootsoutside Asia, such as in Europe, the United States,and Australasia (Birch and Felt 1999). The com-monly used system of Traditional ChineseMedicineor TCM is a subset of the larger field of TEAM, repre-senting a unique and broad inclusion and combina-tion of historical andmodernmethods and ideas.
Historically in Japan, medical texts were writtenin Chinese, thus literate medical practitioners inJapan read Chinese source texts in order to getinformation about medical practice. At the timethat shonishin was developed (17th century) therewere many texts and traditions of medical practiceavailable to a literate practitioner. The first specia-lized pediatric texts in China and thus in Japanwere, however, exclusively herbal medicine texts(Gu 1989). Given the fear that can be encounteredusing acupuncture on children, it is not surprisingthat the trend in China might be toward using her-bal medicines rather than acupuncture in pedia-trics. This does not mean that acupuncture, moxi-bustion, massage and so on were not also used, butthe dominant trend in Chinese pediatric treat-ments has been herbal medicine. The evidence forthis is in many modern TCM texts on pediatrics
Thieme-VerlagFrau Kurz
Sommer-DruckFeuchtwangen
Birch:Shonishin
WN026347/01/01TN 150061
11.5.2011Birch_Umbruch
2 History and Theory 7
aus: Birch, Shonishin: Japanese Pediatric Acupuncture (ISBN 9783131500618) © 2011 Georg Thieme Verlag
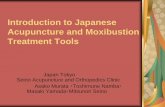
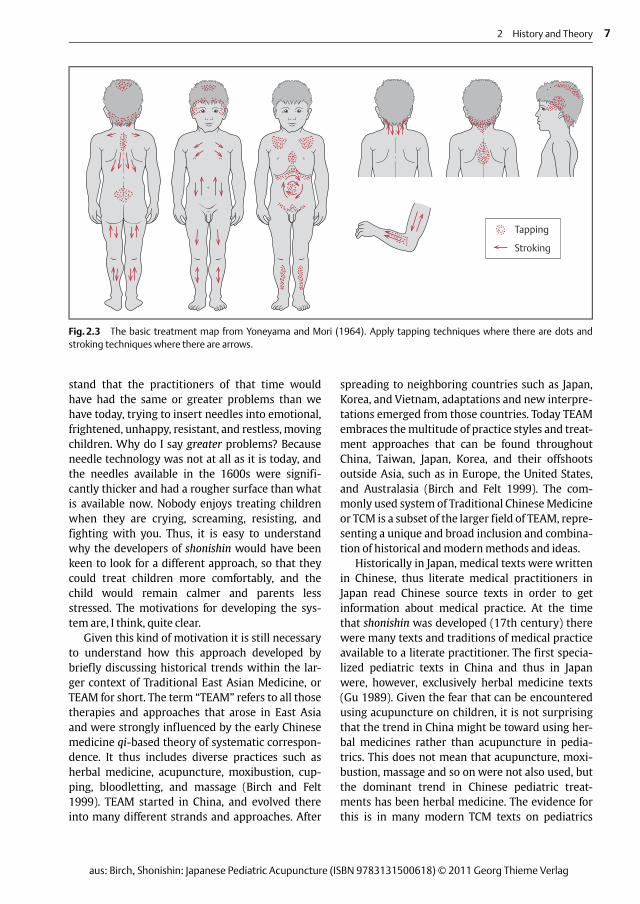
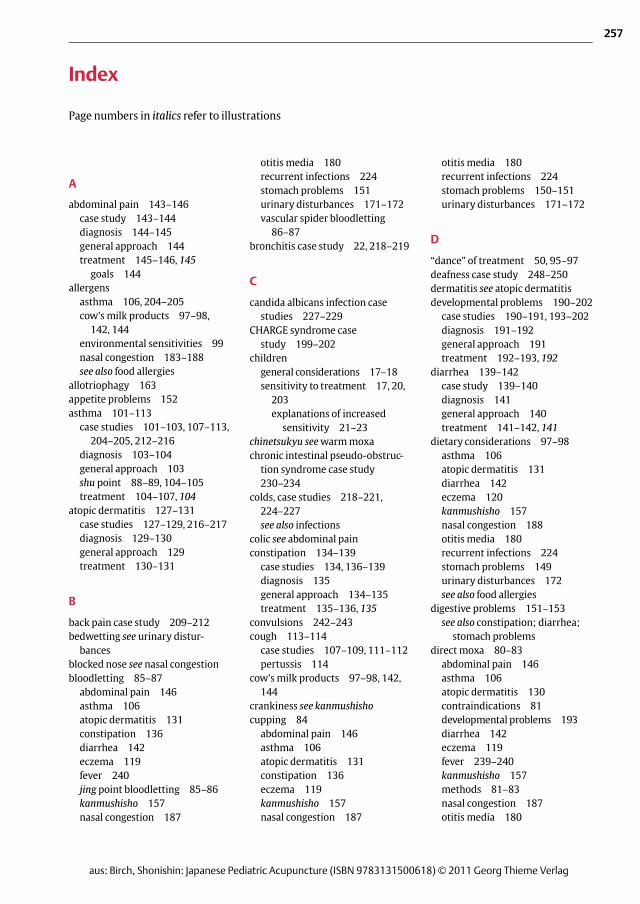
Tapping
Stroking
Fig.2.3 The basic treatment map from Yoneyama and Mori (1964). Apply tapping techniques where there are dots andstroking techniques where there are arrows.
4 AModel for Judging the Dosage Needs of Patients
The Therapeutic Dose—AConceptualModel
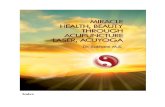
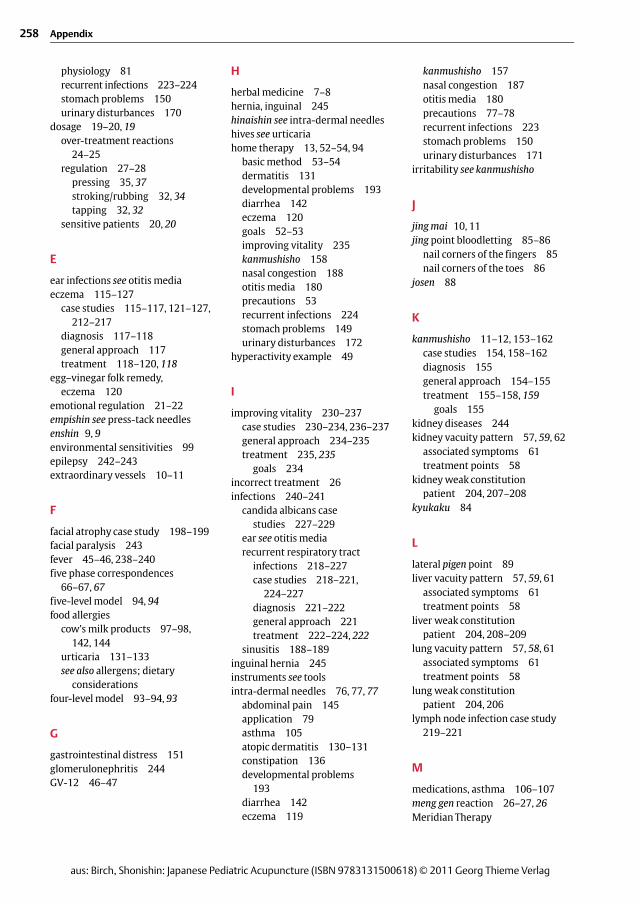
In mainstream medicine, it is generally well under-stood that there is an optimal dosage range for aparticular drug to be effective. The concentration ofthe drug in the blood should lie roughly betweentwo values for it to be effective. Below the lowervalue, the drug is less effective or ineffective andabove the upper value the drug is in too high a con-centration and can cause unwanted side-effects orlead to overdose of treatment. This general idea isquantitatively based, where the optimal dose rangeis often based on body mass and the upper andlower dose ranges are numerical values. But it ispossible to extend this idea to a more qualitativeillustration of dosage needs. I say that it is qualita-tive since we have no laboratory value to measure.We can make qualitative estimates of need only.The following ideas are extensions of explanationsthat Yoshio Manaka made about dose of treatment,in relation to intensity of stimulation delivered(Manaka, Itaya, and Birch 1995, pp.118–119).
When a therapy reaches the therapeutic dosethreshold (TDT), it starts to have its expected thera-peutic effects. If the dose of the treatment builds uptoomuch so that it crosses themaximum therapeu-tic dose (MTD), the patient may start to experienceunwanted side-effects due to over-treatment.
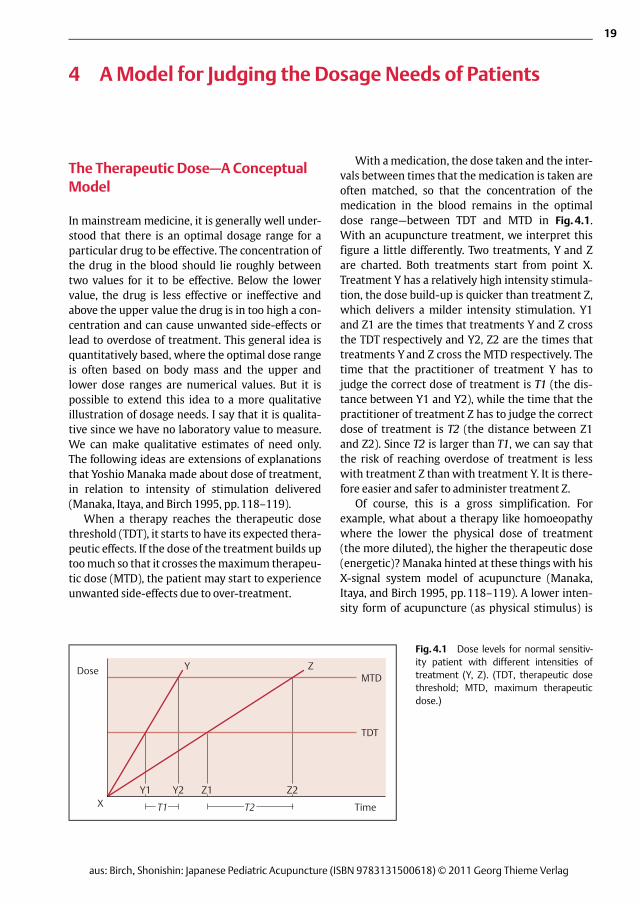
With amedication, the dose taken and the inter-vals between times that the medication is taken areoften matched, so that the concentration of themedication in the blood remains in the optimaldose range—between TDT and MTD in Fig.4.1.With an acupuncture treatment, we interpret thisfigure a little differently. Two treatments, Y and Zare charted. Both treatments start from point X.Treatment Y has a relatively high intensity stimula-tion, the dose build-up is quicker than treatment Z,which delivers a milder intensity stimulation. Y1and Z1 are the times that treatments Y and Z crossthe TDT respectively and Y2, Z2 are the times thattreatments Y and Z cross the MTD respectively. Thetime that the practitioner of treatment Y has tojudge the correct dose of treatment is T1 (the dis-tance between Y1 and Y2), while the time that thepractitioner of treatment Z has to judge the correctdose of treatment is T2 (the distance between Z1and Z2). Since T2 is larger than T1, we can say thatthe risk of reaching overdose of treatment is lesswith treatment Z than with treatment Y. It is there-fore easier and safer to administer treatment Z.
Of course, this is a gross simplification. Forexample, what about a therapy like homoeopathywhere the lower the physical dose of treatment(the more diluted), the higher the therapeutic dose(energetic)? Manaka hinted at these things with hisX-signal system model of acupuncture (Manaka,Itaya, and Birch 1995, pp.118–119). A lower inten-sity form of acupuncture (as physical stimulus) is
Thieme-VerlagFrau Kurz
Sommer-DruckFeuchtwangen
Birch:Shonishin
WN026347/01/01TN 150061
11.5.2011Birch_Umbruch
19
aus: Birch, Shonishin: Japanese Pediatric Acupuncture (ISBN 9783131500618) © 2011 Georg Thieme Verlag
Dose
XY1 Y2 Z1 Z2
T1 T2
MTD
TDT
Y Z
Time
Fig.4.1 Dose levels for normal sensitiv-ity patient with different intensities oftreatment (Y, Z). (TDT, therapeutic dosethreshold; MTD, maximum therapeuticdose.)

to give less (point held slightly retracted) or more(point held slightly protruding) stimulation. Youthen tap the region you are working on the esti-mated number of times required, additionally modi-fying the weight of the tap.The dose is thus adjustedaccording to the scale outlined inTable 6.1.
It is generally a good idea to briefly apply tap-ping with the instrument on yourself, for exampleon the back of the hand. This allows you to quicklysee how it feels, andwhether your attempt to adjustdose through how you hold and tap matches thelevel you are attempting to use on the child. Whenit matches you can immediately go on to applyingthe technique on the child. If not, you can readjustwhat you are doing.
Tools Used for Stroking/Rubbing
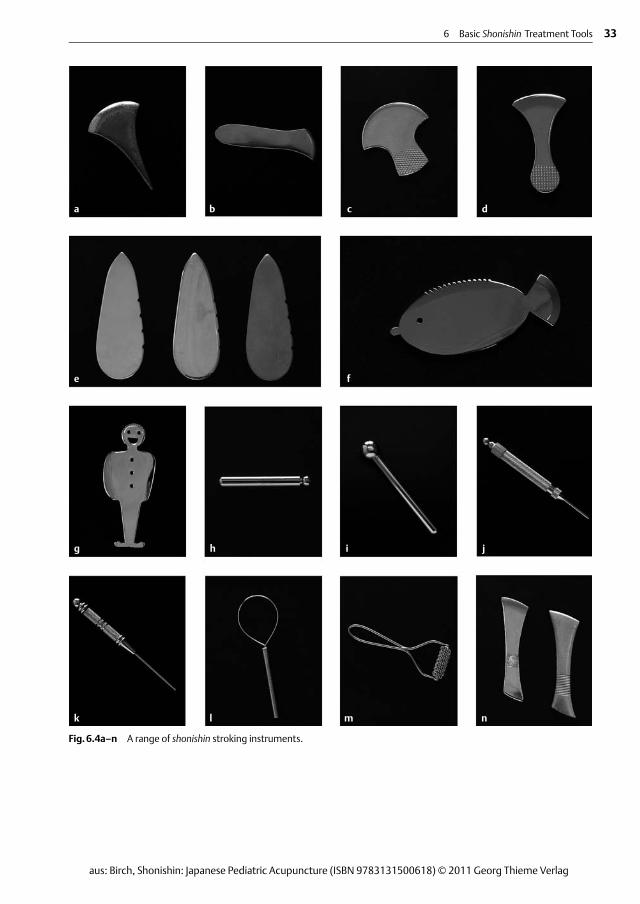
Figure 6.4 shows the range of tools used for apply-ing stroking or rubbing techniques. Figure 6.5shows the tools that are usually easy to obtain fromsuppliers and which the author has found easy touse.
The tools used for stroking or rubbing come intwo varieties. The first (Fig.6.5a), which is used forstroking or rubbing, has a rounded ball-like surface.The second (Fig.6.5f) has an elongated flatter sur-face that is either rounded or straight and smooth,both of which are used only for stroking. I use theterm rubbing to refer to a back and forth rubbing ofthe skin surface, while stroking is applied in a singledirection. This is an important distinction since,based on the treatment principles outlined above,it is useful to apply stroking only in a downwarddirection, as this helps direct the qi in this direction.In babies and small children this is often a veryhelpful tactic.
Like the tapping tools, it is often helpful to keepthe instrument out of view of the child, in whichcase it should be held within the right hand (ifright-handed). On the accompanying ➤DVD var-ious examples are given of how to hold theseinstruments for stroking. The➤DVD shows how tohold them so that as one strokes or rubs with themthey are out of viewof the patient.
How one holds the instrument and whichinstrument one uses can apply different doses tothe regionworked on. For example, when using therounded ball instrument, allowing the roundedend to protrude slightly out from the surface of thepalm can apply an increased dose. Holding the fin-gers of the stroking hand in such a way that theinstrument is cushioned within them, and thenstroking with both fingers and instrument canapply a lower dose. This is illustrated on the accom-panying➤DVD.
If using the flat surface instrument such as thechokishin, strokingwith the long, flat surface gener-ally gives a little more stimulation and thus higherdose than stroking with the narrower rounded end.
After estimating the amount of stimulation youwant to apply you should hold the instrument so asto give less or more stimulation. You then stroke orrub the region you areworking onwith the numberof required strokes, additionally modifying theweight of the contact. The dose is thus adjustedaccording to the scale inTable 6.2.
Thieme-VerlagFrau Kurz
Sommer-DruckFeuchtwangen
Birch:Shonishin
WN026347/01/01TN 150061
11.5.2011Birch_Umbruch
32 Section 2 Treatment Principles and Tools of Treatment
aus: Birch, Shonishin: Japanese Pediatric Acupuncture (ISBN 9783131500618) © 2011 Georg Thieme Verlag
Table 6.1 Dose regulation with tapping technique
Dose/Factor Location of pointed end Number of taps* Weight of tapping
Higher dose Point held level with or slightly protrudingbeyond end of finger and thumb
More Slightly more
Lower dose Point held slightly behind the level of thefinger and thumb
Fewer Less, barely touchingthe skin
* The number of taps on a body area will also vary depending on whether one is using only the tappingmethod for the root treatment,using only a little additional tapping along with the rubbing methods for the root treatment, or whether one is targeting symptoms andtapping a whole area or a single acupoint.
Thieme-VerlagFrau Kurz
Sommer-DruckFeuchtwangen
Birch:Shonishin
WN026347/01/01TN 150061
11.5.2011Birch_Umbruch
6 Basic Shonishin Treatment Tools 33
aus: Birch, Shonishin: Japanese Pediatric Acupuncture (ISBN 9783131500618) © 2011 Georg Thieme Verlag
a b c d
e f
g h i j
k l m n
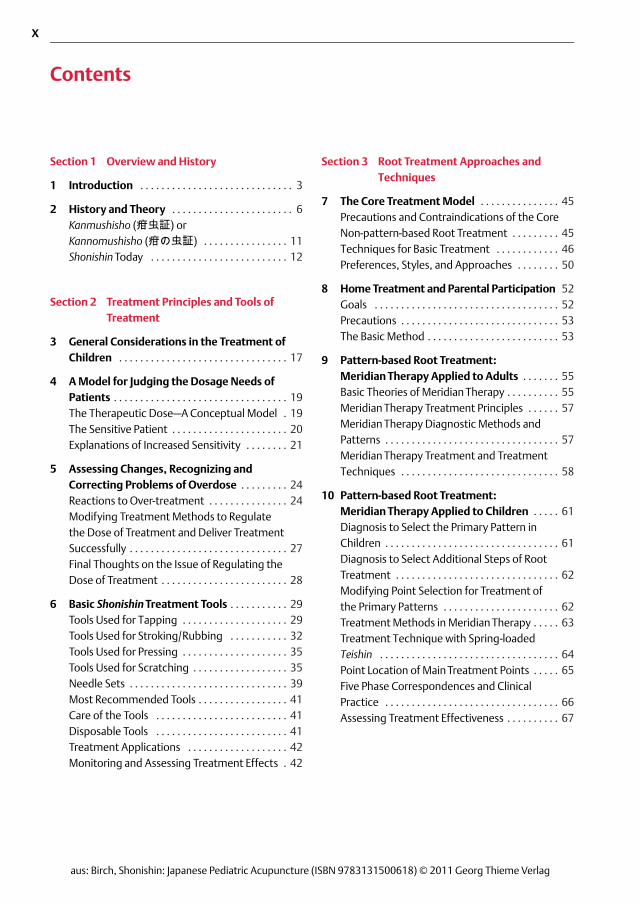
Fig.6.4a–n A range of shonishin stroking instruments.
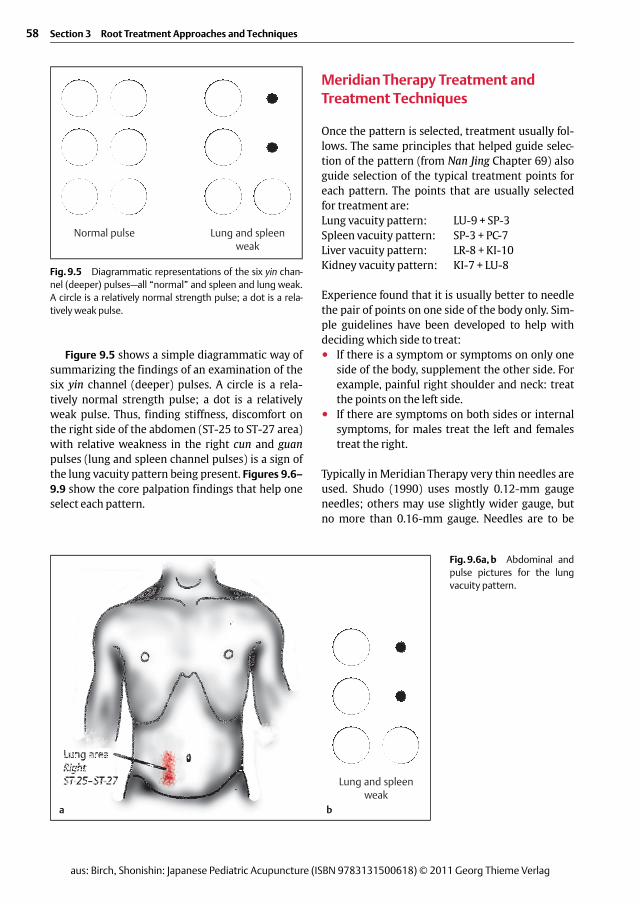
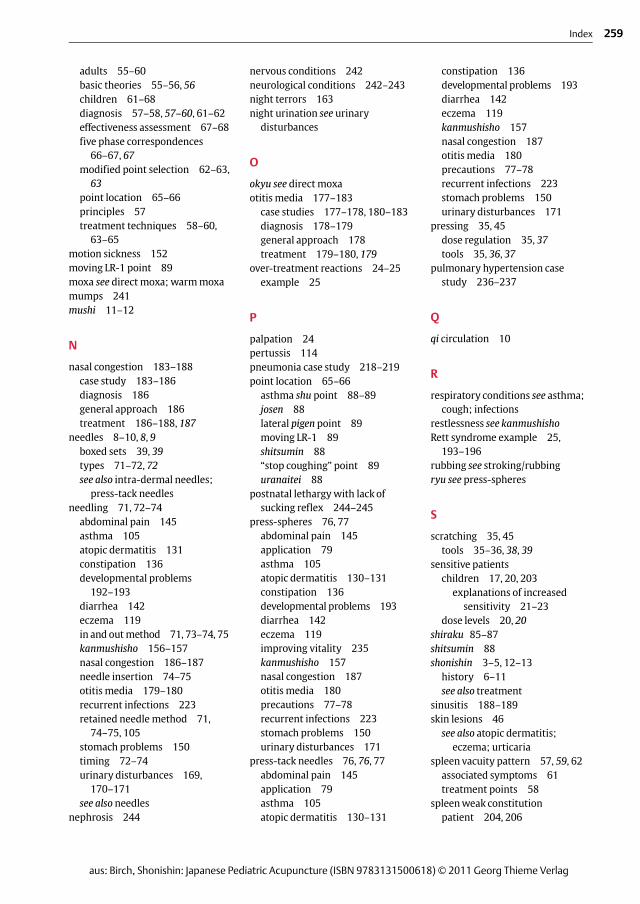
Figure 9.5 shows a simple diagrammatic way ofsummarizing the findings of an examination of thesix yin channel (deeper) pulses. A circle is a rela-tively normal strength pulse; a dot is a relativelyweak pulse. Thus, finding stiffness, discomfort onthe right side of the abdomen (ST-25 to ST-27 area)with relative weakness in the right cun and guanpulses (lung and spleen channel pulses) is a sign ofthe lung vacuity pattern being present. Figures 9.6–9.9 show the core palpation findings that help oneselect each pattern.
MeridianTherapy Treatment andTreatment Techniques
Once the pattern is selected, treatment usually fol-lows. The same principles that helped guide selec-tion of the pattern (from Nan Jing Chapter 69) alsoguide selection of the typical treatment points foreach pattern. The points that are usually selectedfor treatment are:Lung vacuity pattern: LU-9 + SP-3Spleen vacuity pattern: SP-3 + PC-7Liver vacuity pattern: LR-8 + KI-10Kidney vacuity pattern: KI-7 + LU-8
Experience found that it is usually better to needlethe pair of points on one side of the body only. Sim-ple guidelines have been developed to help withdeciding which side to treat:● If there is a symptom or symptoms on only one
side of the body, supplement the other side. Forexample, painful right shoulder and neck: treatthe points on the left side.
● If there are symptoms on both sides or internalsymptoms, for males treat the left and femalestreat the right.
Typically in Meridian Therapy very thin needles areused. Shudo (1990) uses mostly 0.12-mm gaugeneedles; others may use slightly wider gauge, butno more than 0.16-mm gauge. Needles are to be
Thieme-VerlagFrau Kurz
Sommer-DruckFeuchtwangen
Birch:Shonishin
WN026347/01/01TN 150061
11.5.2011Birch_Umbruch
58 Section 3 Root Treatment Approaches and Techniques
aus: Birch, Shonishin: Japanese Pediatric Acupuncture (ISBN 9783131500618) © 2011 Georg Thieme Verlag
Normal pulse Lung and spleenweak
Fig.9.5 Diagrammatic representations of the six yin chan-nel (deeper) pulses—all “normal” and spleen and lung weak.A circle is a relatively normal strength pulse; a dot is a rela-tively weak pulse.
Fig.9.6a,b Abdominal andpulse pictures for the lungvacuity pattern.
a b
Lung and spleenweak

18 Respiratory Problems
Asthma
Asthma is a serious condition that can be life threat-ening. Most children with asthma we treat are ondaily medication to prevent asthma attacks, andoften additional medication to help calm down orstop attacks once they begin. Those with milderasthma conditions may be taking the asthmamedi-cation only with signs of impending symptoms.Some patients will present with asthmalike symp-toms (wheezing, difficulty breathing, chroniccough) due to other conditions such as croup orbronchitis. If these conditions are chronic, the childmay have been prescribed asthma medications tohelp with the difficult breathing or chronic cough.Sometimes parents turn up with their child statingthat their child has asthma for which they receiveasthmamedications, but it is actually amore severeform of something like croup with some of thesame symptoms of asthma (wheezing, difficultybreathing). Occasionally, you may find some confu-sion around the actual diagnosis of the conditionthat the child has. In this subsection I describe thetreatment of asthma and discuss some additionalproblems that canmanifest with asthma symptomssuch as croup.1
Case 1Gilbert, Boy Age 27Months
Main complaints: He had been coughing daily for along time. The condition had been diagnosed as asth-ma for which he had been prescribed the daily use of
a steroid inhaler. He had a tendency to catch coldeasily, the cold triggering worsening of the asthmasymptoms, especially the coughing. His sleep waspoor as he was wokenmany nights by the coughing.
History: He was born 6 weeks premature and was inhospital for the first 10 days of life. It was felt that hiscondition was probably a result of being born prema-ture.
Diagnosis: From the symptoms and the pulse (rightpulse weaker than left), I diagnosed him as having thelung vacuity pattern.
Treatment: I discussed with the mother how to testfor cow’s milk sensitivity (see Chapter 17) and sheagreed to start this as soon as possible.
Tapping with the herabari was applied on the head,GV-12 area, neck area, and a little on the back.
Stroking with an enshin was applied down thearms, legs, and abdomen.
Using a teishin, supplementation was applied to leftLU-9 and SP-5, draining to right LR-3 and left TB-5.
Still using the teishin, light stroking was also applieddown the back.
Press-spheres were left on left BL-13 and the “stopcoughing” points on the elbows.
Second visit—7 days later
No coughing at all this week. The coughing hadstopped immediately after treatment. As a result ofthe dramatic change, his mother had stopped givinghim the inhaler, so that he had not used it at all thisweek. However, his sleep was not so good and he hadwoken in a badmood several mornings.
Treatment: I spoke to the mother about the wisdomof simply stopping the use of the inhaler and that sheshould at least consult with the prescribing doctor.She agreed to consider this.
Tapping with the herabari was applied to GV-20,the neck, GV-12, LU-1, and occipital regions.
Stroking with an enshin was applied down thearms, legs, and abdomen.
Thieme-VerlagFrau Kurz
Sommer-DruckFeuchtwangen
Birch:Shonishin
WN026347/01/01TN 150061
11.5.2011Birch_Umbruch
101
aus: Birch, Shonishin: Japanese Pediatric Acupuncture (ISBN 9783131500618) © 2011 Georg Thieme Verlag
1 A number of similarly manifesting conditions are covered invarious chapters in this book. Here I discuss “asthma” withindications for treatment of asthmalike manifestations ofsomething like “croup.” On pages 113f I discuss a number ofother respiratory conditions, which can also include similarmanifestations of signs and symptoms. In chapters 25 and 26 Ialso discuss treatment of underlying conditions that can pre-dispose towards these problems.
Using a teishin supplementation was applied to leftLU-9 and SP-5, draining to right LR-5 and TB-5.
Press-spheres were left on right BL-13 and the “stopcoughing” points on the elbows.
Third visit—5 days later
He woke on this day with a cold at 5.30a.m. withsymptoms of coughing. He was still coughing, butwith signs of improvement. He had diarrhea over theweekend as well.
Treatment: Tapping with a herabari was applied toGV-20, ST-12 region, neck region, LU-1, GV-12, andLI-4.
Stroking with an enshin was applied down thearms, legs, back, and abdomen.
Using a teishin, supplementation was applied to leftLU-9 and SP-3, draining to right LR-3.
Press-spheres were left bilaterally on the asthmashu points and GV-12.
Fourth visit—2 weeks later
His cough was much better, but he was still coughinga little in the early morning.
Treatment: Tapping with the herabari was applied toGV-20, ST-12 region, GV-12, and LI-4.
Stroking with an enshin was applied down thearms, legs, back, and abdomen.
Using a teishin, supplementation was applied toright LU-9 and SP-3, draining to left LR-3.
Press-spheres were left on bilateral asthma shupoints and behind shen men on the back of the leftear.
Fifth visit—1 week later
The cough wasmuch better again, but he had startedcoughing a little more 2 days before this visit.
Treatment: Tapping with the herabari was applied tothe head, ST-12 region, occipital region, LU-1.
Stroking with an enshin was applied down thearms, legs, back, and abdomen.
Using a teishin, supplementation was applied to leftLU-9 and SP-3, draining to right LR-3.
Press-spheres were left bilaterally on the asthmashu points and behind shen men on the back of theleft ear.
Sixth visit—13 days later
The cough had again improved, but he had startedcoughing a little more in the early morning with acold that started 1 day before this visit.
Treatment: Tapping with the herabari was applied toGV-20, ST-12 region, LU-1, GV-12, LI-4, and LI-11.
Stroking with an enshin was applied down thearms, legs, back, and abdomen.
Using a teishin, supplementation was applied to leftLU-9 and SP-3, draining to right LR-3.
Press-spheres were left bilateral on BL-13 andbehind shen men on the back of the left ear.
Seventh visit—2 weeks later
No symptoms of coughing and his condition was over-all much improved. There were no sleep distur-bances.
Treatment: Tapping with the herabari was applied toGV-20, ST-12 region, GV-12, LI-4, and LI-11.
Stroking with an enshin was applied down thearms, legs, back, and abdomen.
Using a teishin, supplementation was applied to leftLU-9 and SP-3, draining to right LR-3 and left SI-7.
Press-spheres were left on GV-12 and behind shenmen on the back of the left ear.
Eighth visit—22 days later
On holiday he started with a lung infection and wasprescribed antibiotics. He fully recovered and had hadno coughing before or since then. This was a signifi-cant milestone, since any time he had got sick like thisbefore his cough had severely worsened. This time,he had no coughing!
Treatment: Tapping with the herabari was applied toGV-20, the neck region, GV-12, and LI-4.
Stroking with an enshin was applied down thearms, legs, back, and abdomen.
Using a teishin, supplementation was applied to leftLU-9 and SP-3, draining to right LR-3.
Press-spheres were left on GV-12 and behind shenmen on the back of the left ear.
Treatment finished as the family moved away. In thefinal discussions with his mother she revealed thatshe had not talked to the doctor who had prescribedthe inhaler. She had always kept it with her, but since
Thieme-VerlagFrau Kurz
Sommer-DruckFeuchtwangen
Birch:Shonishin
WN026347/01/01TN 150061
11.5.2011Birch_Umbruch
102 Section 5 Treatment of Specific Problems/Diseases
aus: Birch, Shonishin: Japanese Pediatric Acupuncture (ISBN 9783131500618) © 2011 Georg Thieme Verlag

23 Ear and Nose Problems
Otitis Media—Ear Infections
The following case of recurrent ear infections is of ayoung boy who came for treatment before I hadlearned Meridian Therapy sufficiently well to applyit on children. Thus, besides some simple sympto-matic treatment, the principle treatment was thecore non-pattern-based root treatment that is typi-cal of the shonishin system. This case is selected asit is typical of what happenswhen treating childrenwith recurrent ear infections. Of course, treatmentdoes not always work as well and smoothly as this,hence more detailed treatment options are alsogiven below, but Mike was the first of a number of3–6-year-old children that I treated for recurrentinfections as Mike’s parents were in a position toget theword out and refer other children.
Case 1Mike, Boy Age 3½ Years
Main complaints: Mike came for treatment havingjust completed a round of antibiotics for infections inboth ears. The right ear had, as usual, been muchworse than the left ear. Over the last 10 months hehad had many ear infections. With each, the doctoreventually prescribed antibiotics, which would clearup the episode, but within 2 weeks of completing theantibiotics another infection would start, sometimesonly in the right ear, but often in both. The problemhad started initially from catching a bad cold and hav-ing it progress to the ears, but since then, while sev-eral episodes of ear infection had arisen from catch-ing cold, many had not. He had been very disruptedby this process as the pain would often be bad andwould disturb sleep, energy, and the rest of thefamily. The antibiotics disturbed his digestion a bit,with some episodes of loose stools and some epi-sodes of constipation. The parents were interested intrying something different, as it was clear that theproblemwas not going away; rather, it was being sup-pressed by each round of antibiotics. The doctor hadrecently said that if this kept up Mike would probably
have to have ear tubes placed to help prevent furtherproblems. The parents were looking for a treatmentto break the cycle of infections. Other than the prob-lem of recurrent ear infections Mike was healthy andall other systems were unremarkable.
Assessment: Palpation revealed hard painful areasbelow each ear extending downward from TB-17, theright being more hard and uncomfortable than theleft. The occipital border was also stiff, especiallyaround GB-12.
Treatment: On this first visit I decided to apply a sho-nishin core treatment with light stroking and sometargeted tapping.
Light stroking with an enshin was applied down thearms (three yang channels), legs (stomach, gallblad-der, and bladder channels), down the back, across theshoulders, chest, and down the abdomen (stomachchannel).
Light tapping was applied above and behind bothears, and over the reactive regions below the ears andover the occipital region, especially around GB-12.
Press-spheres were placed at GV-12 and on themost reactive point within the reactive regions beloweach ear.
I discussed with the parents that it would be idealto give treatment more than once a week to increasethe chances of preventing recurrence of the infec-tions, but they told me as working parents they weretoo busy to be able to do this. So I told them I wouldfigure out what to do about it.
Second visit—1 week later
Mike was doing well, there were no signs of ear infec-tion, nothing to report.
Treatment: A very slightly increased dose of thesame treatment as given on the first occasion wasapplied.
I then proceeded to explain to the parents how todo the light stroking and tapping treatment at a lowdose each day: stroking down the same areas on thearms, legs, back, shoulders, and tapping on the areasaround the ears and GB-12 region.
Thieme-VerlagFrau Kurz
Sommer-DruckFeuchtwangen
Birch:Shonishin
WN026347/01/01TN 150061
11.5.2011Birch_Umbruch
177
aus: Birch, Shonishin: Japanese Pediatric Acupuncture (ISBN 9783131500618) © 2011 Georg Thieme Verlag
Third visit—1 week later
Mike was still fine, with no sign of an infection. Thehome treatments had been going well and tookabout 2–3minutes each day.
Treatment: The same treatment as given on the firstoccasionwas applied.
Fourth visit—1 week later
Still nothing to report, Mike had no symptoms. Hometreatment was going well.
Treatment: The same treatment as given on the firstoccasionwas applied.
I also scheduled Mike to come back in 2 weeks tostretch out treatments while the parents continueddoing daily home treatment.
Fifth visit—2 weeks later
Still nothing to report, Mike had no symptoms. Hometreatment was going well.
Treatment: The same treatment as given on the firstoccasionwas applied.
Sixth visit—2 weeks later
Still nothing to report, Mike had no symptoms. Hometreatment was going well.
Treatment: The same treatment as given on the firstoccasionwas applied.
We now extended treatment to every 4 weeks.
Seventh visit—4 weeks later
Still nothing to report, Mike had no symptoms. Hehad caught cold and for the first time it did not trig-ger an ear infection and he recovered from the coldquickly.
Treatment: The same treatment as given on the firstoccasionwas applied.
Eighth visit—4 weeks later
Still nothing to report, Mike had no symptoms. Hometreatment was going well.
Treatment: The same treatment as given on the firstoccasionwas applied.
After this we stopped treatment. Mike had had nosign of an ear infection for about 4 months; it lookedlike we had broken the cycle. The parents were stillapplying the simple home treatment regularly butwithout the press-spheres. They agreed to call fortreatment should Mike start an ear infection. Atanother 4-month follow-up conversation, Mike wasstill fine. He seemed to catch cold less often thanbefore and had no sign of any further ear infections.His parents referred many other children with earinfections for treatment.
General Approach for the Treatment ofOtitis Media
Our aim is to improve the overall condition of thechild so he or she has better resistance to infectionsand treat to deal with the local manifestations thatadditionally make the child susceptible to ear infec-tions. Changing the overall condition of the childcan be accomplished with just the use of the basiccore shonishin treatment or the pattern-based roottreatment, but it generally works better if youapply a combination of these two treatment ap-proaches.
Most Likely Pattern-based Root Diagnosis
If the recurrent ear infections arise from catchingcold repeatedly, the typical pattern to be treated isthe lung vacuity pattern. If the ear infections ariseindependently of catching cold, this could be due tolung vacuity pattern or kidney vacuity pattern. Ifthe child is young and the pulse and other signs fordistinguishing the pattern are not clear, one needsother signs to distinguish them. If the hands tend tobe cold, it is likely to be a lung vacuity pattern andone should start treating this. Having generally stiffshoulders is also a sign of lung vacuity type. How-ever, if the feet tend to get cold easily (but not thehands) this is more likely to be a kidney vacuity pat-tern. You may also notice some small temperaturevariations on the abdomen to support the choice ofkidney pattern, such as slightly cooler below thenavel compared with above the navel. Also, if theear infections have triggered changes in hearing,you can suspect the kidney vacuity pattern.
Thieme-VerlagFrau Kurz
Sommer-DruckFeuchtwangen
Birch:Shonishin
WN026347/01/01TN 150061
11.5.2011Birch_Umbruch
178 Section 5 Treatment of Specific Problems/Diseases
aus: Birch, Shonishin: Japanese Pediatric Acupuncture (ISBN 9783131500618) © 2011 Georg Thieme Verlag
For the lung vacuity pattern supplement LU-9and SP-3. If the ear infection has arisen out of catch-ing cold and there are still signs of the cold, such ascough, congested lungs, and alternating fever-chills,try treating themetal jing-river points LU-8 and SP-5instead. If the child has a fever with the ear infec-tion, you need to check the temperature. If 37.8°Cor higher, the core non-pattern-based root treat-ment is contraindicated. In this case try using theying-spring points for the lung vacuity pattern,LU-10 and SP-2. For the kidney vacuity pattern sup-plement KI-7 and LU-8. If with fever, try the ying-spring points KI-2 and LU-10.
Case 2 below illustrates an alternative strategyfor treating the relevant acupoints, using a verylight stroking along the flow of the channels overthe target acupoints for supplementation, and lightstroking against the flow of the channel over thetarget acupoint for draining.
Typical Non-pattern-based Root Treatment
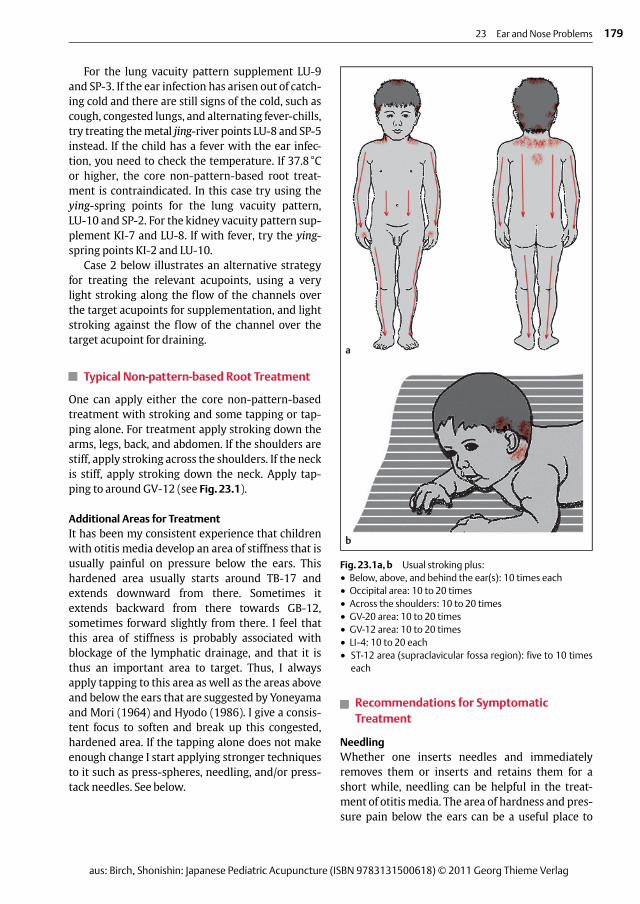
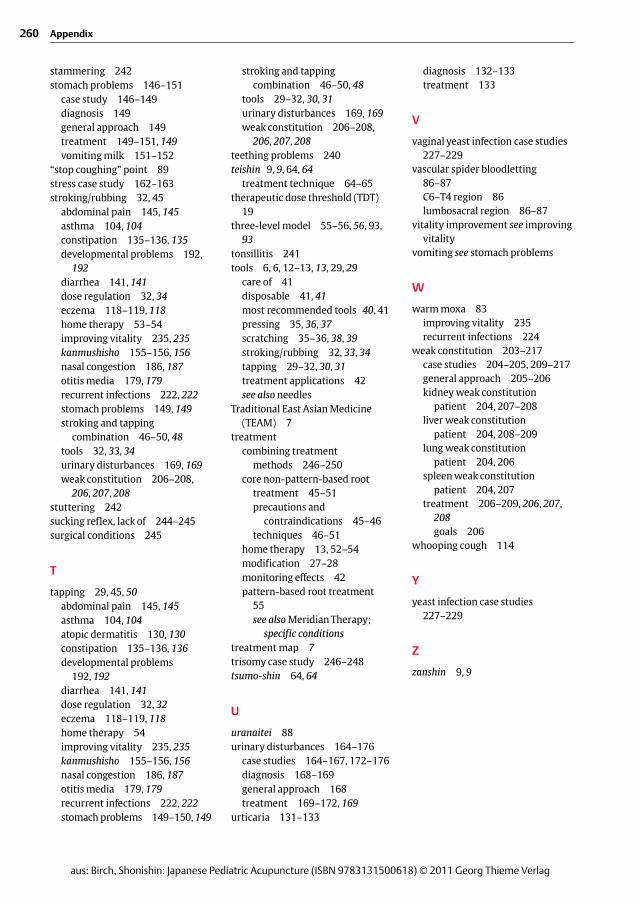
One can apply either the core non-pattern-basedtreatment with stroking and some tapping or tap-ping alone. For treatment apply stroking down thearms, legs, back, and abdomen. If the shoulders arestiff, apply stroking across the shoulders. If the neckis stiff, apply stroking down the neck. Apply tap-ping to around GV-12 (see Fig.23.1).
Additional Areas for TreatmentIt has been my consistent experience that childrenwith otitis media develop an area of stiffness that isusually painful on pressure below the ears. Thishardened area usually starts around TB-17 andextends downward from there. Sometimes itextends backward from there towards GB-12,sometimes forward slightly from there. I feel thatthis area of stiffness is probably associated withblockage of the lymphatic drainage, and that it isthus an important area to target. Thus, I alwaysapply tapping to this area as well as the areas aboveand below the ears that are suggested by Yoneyamaand Mori (1964) and Hyodo (1986). I give a consis-tent focus to soften and break up this congested,hardened area. If the tapping alone does not makeenough change I start applying stronger techniquesto it such as press-spheres, needling, and/or press-tack needles. See below.
Recommendations for SymptomaticTreatment
NeedlingWhether one inserts needles and immediatelyremoves them or inserts and retains them for ashort while, needling can be helpful in the treat-ment of otitis media. The area of hardness and pres-sure pain below the ears can be a useful place to
Thieme-VerlagFrau Kurz
Sommer-DruckFeuchtwangen
Birch:Shonishin
WN026347/01/01TN 150061
11.5.2011Birch_Umbruch
23 Ear and Nose Problems 179
aus: Birch, Shonishin: Japanese Pediatric Acupuncture (ISBN 9783131500618) © 2011 Georg Thieme Verlag
a
b
Fig.23.1a,b Usual stroking plus:● Below, above, and behind the ear(s): 10 times each● Occipital area: 10 to 20 times● Across the shoulders: 10 to 20 times● GV-20 area: 10 to 20 times● GV-12 area: 10 to 20 times● LI-4: 10 to 20 each● ST-12 area (supraclavicular fossa region): five to 10 times
each
Thieme-VerlagFrau Kurz
Sommer-DruckFeuchtwangen
Birch:Shonishin
WN026347/01/01TN 150061
11.5.2011Birch_Umbruch
257
aus: Birch, Shonishin: Japanese Pediatric Acupuncture (ISBN 9783131500618) © 2011 Georg Thieme Verlag
Index
Page numbers in italics refer to illustrations
A
abdominal pain 143–146case study 143–144diagnosis 144–145general approach 144treatment 145–146, 145
goals 144allergens
asthma 106, 204–205cow’s milk products 97–98,
142, 144environmental sensitivities 99nasal congestion 183–188see also food allergies
allotriophagy 163appetite problems 152asthma 101–113
case studies 101–103, 107–113,204–205, 212–216
diagnosis 103–104general approach 103shu point 88–89, 104–105treatment 104–107, 104
atopic dermatitis 127–131case studies 127–129, 216–217diagnosis 129–130general approach 129treatment 130–131
B
back pain case study 209–212bedwetting see urinary distur-
bancesblocked nose see nasal congestionbloodletting 85–87
abdominal pain 146asthma 106atopic dermatitis 131constipation 136diarrhea 142eczema 119fever 240jing point bloodletting 85–86kanmushisho 157nasal congestion 187
otitis media 180recurrent infections 224stomach problems 151urinary disturbances 171–172vascular spider bloodletting
86–87bronchitis case study 22, 218–219
C
candida albicans infection casestudies 227–229
CHARGE syndrome casestudy 199–202
childrengeneral considerations 17–18sensitivity to treatment 17, 20,
203explanations of increased
sensitivity 21–23chinetsukyu seewarmmoxachronic intestinal pseudo-obstruc-
tion syndrome case study230–234
colds, case studies 218–221,224–227see also infections
colic see abdominal painconstipation 134–139
case studies 134, 136–139diagnosis 135general approach 134–135treatment 135–136, 135
convulsions 242–243cough 113–114
case studies 107–109, 111–112pertussis 114
cow’s milk products 97–98, 142,144
crankiness see kanmushishocupping 84
abdominal pain 146asthma 106atopic dermatitis 131constipation 136eczema 119kanmushisho 157nasal congestion 187
otitis media 180recurrent infections 224stomach problems 150–151urinary disturbances 171–172
D
“dance” of treatment 50, 95–97deafness case study 248–250dermatitis see atopic dermatitisdevelopmental problems 190–202
case studies 190–191, 193–202diagnosis 191–192general approach 191treatment 192–193, 192
diarrhea 139–142case study 139–140diagnosis 141general approach 140treatment 141–142, 141
dietary considerations 97–98asthma 106atopic dermatitis 131diarrhea 142eczema 120kanmushisho 157nasal congestion 188otitis media 180recurrent infections 224stomach problems 149urinary disturbances 172see also food allergies
digestive problems 151–153see also constipation; diarrhea;
stomach problemsdirect moxa 80–83
abdominal pain 146asthma 106atopic dermatitis 130contraindications 81developmental problems 193diarrhea 142eczema 119fever 239–240kanmushisho 157methods 81–83nasal congestion 187otitis media 180
Thieme-VerlagFrau Kurz
Sommer-DruckFeuchtwangen
Birch:Shonishin
WN026347/01/01TN 150061
11.5.2011Birch_Umbruch
258 Appendix
aus: Birch, Shonishin: Japanese Pediatric Acupuncture (ISBN 9783131500618) © 2011 Georg Thieme Verlag
physiology 81recurrent infections 223–224stomach problems 150urinary disturbances 170
dosage 19–20, 19over-treatment reactions
24–25regulation 27–28
pressing 35, 37stroking/rubbing 32, 34tapping 32, 32
sensitive patients 20, 20
E
ear infections see otitis mediaeczema 115–127
case studies 115–117, 121–127,212–217
diagnosis 117–118general approach 117treatment 118–120, 118
egg–vinegar folk remedy,eczema 120
emotional regulation 21–22empishin see press-tack needlesenshin 9, 9environmental sensitivities 99epilepsy 242–243extraordinary vessels 10–11
F
facial atrophy case study 198–199facial paralysis 243fever 45–46, 238–240five phase correspondences
66–67, 67five-level model 94, 94food allergies
cow’s milk products 97–98,142, 144
urticaria 131–133see also allergens; dietary
considerationsfour-level model 93–94, 93
G
gastrointestinal distress 151glomerulonephritis 244GV-12 46–47
H
herbal medicine 7–8hernia, inguinal 245hinaishin see intra-dermal needleshives see urticariahome therapy 13, 52–54, 94
basic method 53–54dermatitis 131developmental problems 193diarrhea 142eczema 120goals 52–53improving vitality 235kanmushisho 158nasal congestion 188otitis media 180precautions 53recurrent infections 224stomach problems 149urinary disturbances 172
hyperactivity example 49
I
improving vitality 230–237case studies 230–234, 236–237general approach 234–235treatment 235, 235
goals 234incorrect treatment 26infections 240–241
candida albicans casestudies 227–229
ear see otitis mediarecurrent respiratory tract
infections 218–227case studies 218–221,
224–227diagnosis 221–222general approach 221treatment 222–224, 222
sinusitis 188–189inguinal hernia 245instruments see toolsintra-dermal needles 76, 77, 77
abdominal pain 145application 79asthma 105atopic dermatitis 130–131constipation 136developmental problems
193diarrhea 142eczema 119
kanmushisho 157nasal congestion 187otitis media 180precautions 77–78recurrent infections 223stomach problems 150urinary disturbances 171
irritability see kanmushisho
J
jingmai 10, 11jing point bloodletting 85–86
nail corners of the fingers 85nail corners of the toes 86
josen 88
K
kanmushisho 11–12, 153–162case studies 154, 158–162diagnosis 155general approach 154–155treatment 155–158, 159
goals 155kidney diseases 244kidney vacuity pattern 57, 59, 62
associated symptoms 61treatment points 58
kidneyweak constitutionpatient 204, 207–208
kyukaku 84
L
lateral pigen point 89liver vacuity pattern 57, 59, 61
associated symptoms 61treatment points 58
liver weak constitutionpatient 204, 208–209
lung vacuity pattern 57, 58, 61associated symptoms 61treatment points 58
lung weak constitutionpatient 204, 206
lymph node infection case study219–221
M
medications, asthma 106–107meng gen reaction 26–27, 26MeridianTherapy
Thieme-VerlagFrau Kurz
Sommer-DruckFeuchtwangen
Birch:Shonishin
WN026347/01/01TN 150061
11.5.2011Birch_Umbruch
Index 259
aus: Birch, Shonishin: Japanese Pediatric Acupuncture (ISBN 9783131500618) © 2011 Georg Thieme Verlag
adults 55–60basic theories 55–56, 56children 61–68diagnosis 57–58, 57–60, 61–62effectiveness assessment 67–68five phase correspondences
66–67, 67modified point selection 62–63,
63point location 65–66principles 57treatment techniques 58–60,
63–65motion sickness 152moving LR-1 point 89moxa see direct moxa; warmmoxamumps 241mushi 11–12
N
nasal congestion 183–188case study 183–186diagnosis 186general approach 186treatment 186–188, 187
needles 8–10, 8, 9boxed sets 39, 39types 71–72, 72see also intra-dermal needles;
press-tack needlesneedling 71, 72–74
abdominal pain 145asthma 105atopic dermatitis 131constipation 136developmental problems
192–193diarrhea 142eczema 119in and outmethod 71, 73–74, 75kanmushisho 156–157nasal congestion 186–187needle insertion 74–75otitis media 179–180recurrent infections 223retained needlemethod 71,
74–75, 105stomach problems 150timing 72–74urinary disturbances 169,
170–171see also needles
nephrosis 244
nervous conditions 242neurological conditions 242–243night terrors 163night urination see urinary
disturbances
O
okyu see direct moxaotitis media 177–183
case studies 177–178, 180–183diagnosis 178–179general approach 178treatment 179–180, 179
over-treatment reactions 24–25example 25
P
palpation 24pertussis 114pneumonia case study 218–219point location 65–66
asthma shu point 88–89josen 88lateral pigen point 89moving LR-1 89shitsumin 88“stop coughing” point 89uranaitei 88
postnatal lethargywith lackofsucking reflex 244–245
press-spheres 76, 77abdominal pain 145application 79asthma 105atopic dermatitis 130–131constipation 136developmental problems 193diarrhea 142eczema 119improving vitality 235kanmushisho 157nasal congestion 187otitis media 180precautions 77–78recurrent infections 223stomach problems 150urinary disturbances 171
press-tack needles 76, 76, 77abdominal pain 145application 79asthma 105atopic dermatitis 130–131
constipation 136developmental problems 193diarrhea 142eczema 119kanmushisho 157nasal congestion 187otitis media 180precautions 77–78recurrent infections 223stomach problems 150urinary disturbances 171
pressing 35, 45dose regulation 35, 37tools 35, 36, 37
pulmonary hypertension casestudy 236–237
Q
qi circulation 10
R
respiratory conditions see asthma;cough; infections
restlessness see kanmushishoRett syndrome example 25,
193–196rubbing see stroking/rubbingryu see press-spheres
S
scratching 35, 45tools 35–36, 38, 39
sensitive patientschildren 17, 20, 203
explanations of increasedsensitivity 21–23
dose levels 20, 20shiraku 85–87shitsumin 88shonishin 3–5, 12–13
history 6–11see also treatment
sinusitis 188–189skin lesions 46
see also atopic dermatitis;eczema; urticaria
spleen vacuity pattern 57, 59, 62associated symptoms 61treatment points 58
spleenweak constitutionpatient 204, 206
Thieme-VerlagFrau Kurz
Sommer-DruckFeuchtwangen
Birch:Shonishin
WN026347/01/01TN 150061
11.5.2011Birch_Umbruch
260 Appendix
aus: Birch, Shonishin: Japanese Pediatric Acupuncture (ISBN 9783131500618) © 2011 Georg Thieme Verlag
stammering 242stomach problems 146–151
case study 146–149diagnosis 149general approach 149treatment 149–151, 149vomitingmilk 151–152
“stop coughing” point 89stress case study 162–163stroking/rubbing 32, 45
abdominal pain 145, 145asthma 104, 104constipation 135–136, 135developmental problems 192,
192diarrhea 141, 141dose regulation 32, 34eczema 118–119, 118home therapy 53–54improving vitality 235, 235kanmushisho 155–156, 156nasal congestion 186, 187otitis media 179, 179recurrent infections 222, 222stomach problems 149, 149stroking and tapping
combination 46–50, 48tools 32, 33, 34urinary disturbances 169, 169weak constitution 206–208,
206, 207, 208stuttering 242sucking reflex, lack of 244–245surgical conditions 245
T
tapping 29, 45, 50abdominal pain 145, 145asthma 104, 104atopic dermatitis 130, 130constipation 135–136, 136developmental problems
192, 192diarrhea 141, 141dose regulation 32, 32eczema 118–119, 118home therapy 54improving vitality 235, 235kanmushisho 155–156, 156nasal congestion 186, 187otitis media 179, 179recurrent infections 222, 222stomach problems 149–150, 149
stroking and tappingcombination 46–50, 48
tools 29–32, 30, 31urinary disturbances 169, 169weak constitution 206–208,
206, 207, 208teething problems 240teishin 9, 9, 64, 64
treatment technique 64–65therapeutic dose threshold (TDT)
19three-level model 55–56, 56, 93,
93tonsillitis 241tools 6, 6, 12–13, 13, 29, 29
care of 41disposable 41, 41most recommended tools 40, 41pressing 35, 36, 37scratching 35–36, 38, 39stroking/rubbing 32, 33, 34tapping 29–32, 30, 31treatment applications 42see also needles
Traditional East AsianMedicine(TEAM) 7
treatmentcombining treatment
methods 246–250core non-pattern-based root
treatment 45–51precautions and
contraindications 45–46techniques 46–51
home therapy 13, 52–54modification 27–28monitoring effects 42pattern-based root treatment
55see alsoMeridianTherapy;
specific conditionstreatment map 7trisomy case study 246–248tsumo-shin 64, 64
U
uranaitei 88urinary disturbances 164–176
case studies 164–167, 172–176diagnosis 168–169general approach 168treatment 169–172, 169
urticaria 131–133
diagnosis 132–133treatment 133
V
vaginal yeast infection case studies227–229
vascular spider bloodletting86–87C6–T4 region 86lumbosacral region 86–87
vitality improvement see improvingvitality
vomiting see stomach problems
W
warmmoxa 83improving vitality 235recurrent infections 224
weak constitution 203–217case studies 204–205, 209–217general approach 205–206kidneyweak constitution
patient 204, 207–208liver weak constitution
patient 204, 208–209lung weak constitution
patient 204, 206spleenweak constitution
patient 204, 207treatment 206–209, 206, 207,
208goals 206
whooping cough 114
Y
yeast infection case studies227–229
Z
zanshin 9, 9