J. Perinat. Med. Computer prediction of neonatal ...
12
110 Takemura et al, Computer prediction of neonatal conditions J. Perinat. Med. 2 (1974) 110 Computer prediction of neonatal conditions by sampled data analyses of the fetal heart rate and the scalp blood during labor H. Takemura, H. Fujimoto Department of Obstetrics and Gynecology, Osaka University Medical School, Osaka, Japan Shionogi Pharmaceutical Company, Computer Center, Osaka, Japan Received January 12, 1973. Accepted December 18, 1973. One of the most important pieces of Information that an obstetrician can get, äs feedback in the attendance of childbirths, is the expected neonatal condition äs represented by the AP GAR score [1]. To evaluate the quality of labor monitoring, some guidance is needed during the course of labor. This cannot be achieved without such type of Information äs that which is usu- ally called a controlled variable in control en- gineering. Although its essential significance äs to the later development of the baby's body and mind is somewhat controversial, a colla- borative study reported by DRÄGE, KENNEDY, BERENDES, SCHWARZ and WEISS [3] has clearly demonstrated that the lower the points of the AP GAR score, the higher the incidence of neuro- logical abnormalities at one year of age. It is also commonly known that the high mortality and morbidity rates are in the low AP GAR score group. Hence, in order to establish a mathematical formula for predicting the AP GAR scores at both one and five minutes after birth from several fetal parameters minimizing any possibility of personal, subjectively biased judgments, two different types of Computer prediction Systems have been developed. One is discriminant analysis of fetal variables to differentiate between the normal infants with an APGAR score of 8 or more and the depressed infants with a score of 7 or less. The other is partial regression ana- lysis of fetal variables to construct a linear Curriculum vitae HARUMI FUJIMOTO, B. S. Born in Saitama, Japan on April 24, 1924, he graduated from Tokyo University of Education in 1965 with the degree of B. S., majoring Mathematics in the School of Science. Presently he is wor- king äs a system analyst in Shionogi Computing Center, Shionogi Research Laboratory, Osaka, Japan. regression function of APGAR scores using a set of data which were individüally given at each stage of labor. 1. Materials and methods More than one hundred cases who were ad- mitted at Yale New Haven Medical Center, were continuously monitored by electronic means äs well äs by fetal scalp blood analysis during the year 1966—67. Only the data of the cases with complete sets of Information such äs fetal blood pH, PO 2 , PCO 2 , actual base excess (BE), the level of basal fetal heart rate (BFHR) and the incidences of late and variable fetal heart rate decelerations (%UPI & % CORD) during twenty minutes at each stage of labor, were processed by an electronic digital Computer FACOM 270—20*. * Fuji Electric Co., Japan. J. Perinat, Med. 2 (1974)
Transcript of J. Perinat. Med. Computer prediction of neonatal ...

110 Takemura et al, Computer prediction of neonatal conditions
J. Perinat. Med.2 (1974) 110
Computer prediction of neonatal conditions by sampleddata analyses of the fetal heart rate and the scalp bloodduring labor
H. Takemura, H. Fujimoto
Department of Obstetrics and Gynecology, Osaka University Medical School,Osaka, Japan
Shionogi Pharmaceutical Company, Computer Center, Osaka, Japan
Received January 12, 1973. Accepted December 18, 1973.
One of the most important pieces of Informationthat an obstetrician can get, äs feedback in theattendance of childbirths, is the expected neonatalcondition äs represented by the AP GAR score [1].To evaluate the quality of labor monitoring,some guidance is needed during the courseof labor. This cannot be achieved withoutsuch type of Information äs that which is usu-ally called a controlled variable in control en-gineering. Although its essential significance ästo the later development of the baby's bodyand mind is somewhat controversial, a colla-borative study reported by DRÄGE, KENNEDY,BERENDES, SCHWARZ and WEISS [3] has clearlydemonstrated that the lower the points of theAP GAR score, the higher the incidence of neuro-logical abnormalities at one year of age. It is alsocommonly known that the high mortality andmorbidity rates are in the low AP GAR scoregroup. Hence, in order to establish a mathematicalformula for predicting the AP GAR scores at bothone and five minutes after birth from severalfetal parameters minimizing any possibility ofpersonal, subjectively biased judgments, twodifferent types of Computer prediction Systemshave been developed. One is discriminantanalysis of fetal variables to differentiate betweenthe normal infants with an APGAR score of 8 ormore and the depressed infants with a score of7 or less. The other is partial regression ana-lysis of fetal variables to construct a linear
Curriculum vitae
HARUMI FUJIMOTO, B. S.Born in Saitama, Japan onApril 24, 1924, he graduatedfrom Tokyo University ofEducation in 1965 with thedegree of B. S., majoringMathematics in the School ofScience. Presently he is wor-king äs a system analyst inShionogi Computing Center,Shionogi Research Laboratory,Osaka, Japan.
regression function of APGAR scores using a setof data which were individüally given at eachstage of labor.
1. Materials and methodsMore than one hundred cases who were ad-mitted at Yale New Haven Medical Center, werecontinuously monitored by electronic means äswell äs by fetal scalp blood analysis during theyear 1966—67. Only the data of the cases withcomplete sets of Information such äs fetal bloodpH, PO2, PCO2, actual base excess (BE), thelevel of basal fetal heart rate (BFHR) and theincidences of late and variable fetal heart ratedecelerations (%UPI & % CORD) during twentyminutes at each stage of labor, were processed byan electronic digital Computer FACOM 270—20*.* Fuji Electric Co., Japan.
J. Perinat, Med. 2 (1974)

Takemura et al., Computer prcdiction of neonatal conditions 111
delivery
CDST AG E 3-4-5cm
CD-6-7cm
CD=8-9cm
earlyund
täteund
1min.Apgar
score
5min.Apgar
score
LABORCOURSE
Pl
PC
B
BF
U
CO
T
\
£
E
HR
Pl_
RD
t
/
-4
t
r
r
t
f
-
/
t
'
-f
f
r
t
'
/
f
t
r
t
f
f
t
'
t
r
1
,
r
\' 1c
f£
l·i
0 1) £! l"1 il1 (
1 11 1i %
0)5
|̂
j
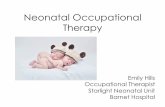
Fig. 1. Design of a sampled data prediction System for neonatal conditions based upon a set of seven fetal parametersat a given stage of childbirth.
Tab. I. The number of subjects studied in this report.
stage 3-First Stage
-5 6—7 8—9Second Stageearly late
No. 47 22 12 14 58
The number of cases computed is shown inTab. LAs shown in Fig. l, a course of labor was devidedinto five stages; the early first stage where cer-vical dilatation was 3—4—5 cm, the middle firststage of 6—7 cm, the late first of 8—9 cm,the early second stage, and the late secondstage which was the last twenty minutes justbefore delivery. At each stage the quantitativedata for processing were obtained during aperiod of twenty minutes. Several measurementsof fetal blood, analysed for pH with an ASTRUPpH-meter and for PO2 and PCO2 with a micro ILmeter during the twenty minutes were all aver-aged to get a set of sampled data at a given stagefor processing. Actual base excess (BE) wascalculated with the SIGGAARD-ANDERSEN align-ment nomogram [8] from the averaged values ofpH, PCO2 and hemoglobin concentration. Thebasal fetal heart rate (BFHR äs an initial value offetal heart rate just before each contraction) was
also averaged äs all uterine contractions during thetwenty minutes to get the level of BFHR at thatstage. The parameters in the pattern of late FHRdeceleration (UPI) and that of variable one(CORD) were both represented by the ratio oftheir incidence or appearance over the number ofcontractions during the twenty minutes. TheIdentification of the FHR patterns was onlypossible visually [4], APGAR scores at one andfive minutes after birth were correlated with aset of values of seven fetal parameters mentionedabove, at each stage of labor, in order to get apredictive solution by both discriminant analysisand partial regression analysis.
2. Results2.1 Discriminant analysisA Computing flow chart for predictive discri-mination between the vigorous infants who areassumed to have 8 or more APGAR score and thedepressed one of 7 or less at one and five minutesafter birth, in any stage of labor, is shown inFig. 2. The sets of data that were provided to theComputer (from forty-seven patients at the earlyfirst stage) are given in Tab. II. The discriminantfunctions at all the five stages for both one andfive minutes APGAR scores, which thus obtained,are summarized in Fig. 3.
J. Pcrinat. Mcd. 2 (1974)

112 Takemura et aL, Computer prediction of neonatal conditions
Tab. II. Examples of complete set data of forty-seven fetuses at the early first stage of labor with 3—4—5 cm cervicaldilatation.
No.
123456789
1011121314151617181920212223242526272829303132333435363738394041424344454647
CaseNo.
21242526282930313233363738394041444648495053565760616264717273747578808182838488929396979899
100
ActualAPGAR s.
9.009.009.008.001.009.009.008.009.007.00
10.009.008.008.007.009.008.001.009.008.009.009.002.006.005.007.009.005.009.008.008.009.006.008.003.002.009.009.008.003.009.008.009.009.009.007.009.00
pH
7.317.317.287.217.267.357.287.237.327.267.317.277.297.317.267.297.017.267.287.297.297.267.327.317.217.277.377.317.267.257.287.287.337.307.307.267.317.287.297.317.257.317.337.297.297.337.21
P02
15.0021.9924.0024.3916.6920.0023.0013.9925.0020.5018.5020.5021.1920.5012.7920.2912.7916.7915.5021.9915.0017.5011.4918.9910.3925.0016.0019.6914.6917.1923.6918.2925.0016.4918.0010.7920.2922.2914.6921.2920.5019.4920.2921.9920.2924.4920.00
PC02
41.0044.5043.2950.0056.0042.5051.7956.5051.2956.5050.0049.6944.7945.2953.6946.8959.2949.6952.2942.0047.5049.0054.0049.0054.5942.5042.2941.5044.6955.5042.6950.5942.0043.0047.6946.6952.7942.2946.2947.0046.1941.0049.5045.0946.0042.5935.50
BE
-̂ .79—3.69—6.00—4.79—3.19—1.89—2.69-4.69
0.00—3.09—1.29—3.79—4.39—3.19—3.09-̂ .19
—17.09—5.00—3.19—5.29—3.39—5.50
0.50—1.59—6.59—6.79—0.09—5.79—6.79—4.39—6.00—3.29—3.24—4.79—3.00—6.29
0.29—6.09—3.39—2.79—6.69-4.89
0.00—4.39—4.00—2.89—6.19
MeanBFHR
155.00169.99140.00140.00180.00140.00140.00150.00144.99135.00150.00150.00130.00130.00144.99144.99105.00144.99155.00130.00160.00160.00144.99140.00160.00140.00150.00135.00150.00150.00130.00150.00173.00140.00135.00110.00150.00150.00130.00130.00150.00169.99164.99130.00140.00155.00164.99
%UPIpercont.
1.000.710.180.140.600.000.000.830.000.280.000.000,000.270.620.000.660.120.250.000.000.600.250.001.000.000.120.620.180.200.000.000.000.000.000.420.120.000.000.000.070.000.000.000.140.000.50
%CORDpercont.
1.000.280.450.420.001.000.000.500.330.420.000.000.290.450.500.090.330.620.250.000.370.200.000.660.660.300.620.000.450.460.370.000.140.530.900.000.750.500.000.530.350.330.290.420.710.000.60
J. Pcrinat. Med. 2 (1974)

Takemura et al., Computer prediction of neonatal conditions 113
K number of variableN(1): sample size from population 1N(2): sample size from population 2
AP: pfobability that an observationcomes from population 1
AQ: probability that an observationcomes from population 2
V (i. j): covariance matrixA(i.j): mean of X(j) of sample«
from population iC(i.j):the cost of misclaesification
X(i): observation. i-1.—,K
10
clear A.V
YES
if the sample is from population 1.A(1 . j )*-A(1 . j )+X(j)
if the sample is from population 2.
i-1. - .K i-1 .-.K
.1.···. K j — 1.—.K
0.
I.
TL.
ET,
IV.
V.
VI.
Fig. 2. Computing flow chart for discriminant analysis ofthe neonatal conditions based upon several fetal parameters.
The functions are constructed so äs to have apositive value if the infant is to be vigorous andto have a negative one if it is to be depressed. Thecorrect and false discriminations of neonatal
ApGAR
SC0RE
B A
D
abnormal< critical·value
—* normal
A Parameterat A Stage
DIAGNOSTIC PROBABILITY OF LABOR MONITORING
Relative Differential Probability for Correct Diagnosis(A+C)/(A+B+C+D) -, S-B= (A+B)/(A+B+C+D) ~ x - A+B
Probability for Correct Dia^nosis = A+B+C+Dn
Detectability for The Depressed -.
Detectability for The Vi^orous - -
Accuracy äs for The Depressed = ·
Accuracy äs for The Vigorous
Probability of Detection and Accuracy for The Depressed
= JE x IV = pcn X · C
c
Fig. 4. Definition of diagnostic probabilities in the pre-diction of neonatal conditions by a critical value of asingle fetal variable at each stage of labor. (DRDN:Diagnostic Reliability for Depressed Neonates)
condition by this means are summed up in Fig. 5,äs the number of cases in four categories, A, B,C and D which are shown in Fig. 4. A is thegroup of the correct diagnosis^ "to be vigorous",
STAGE
APGAR
CD=3-4-5 cm
=+ 78.854( )+ 0.050947(+ 4.6733( )- 1.0476( )- 2.6332( )+ 0.18275( )- 0.11629( )-598.03
CD=6-7 cm CD=8-9cm
=+ 808.32( )+ 0.21270(+ 36.132( )- 12.150( )+ 1.1389( )+ 2.2132( )- 0.94897(-6125.6
=- 48.214( )+ 7.0428( )+ 1.9029( )+ 2.0091 ( )- 13.702( )+ 2.7870( )- 1.8864( )+360.30
early und
=- 62.068( )- 2.2719( )+ 0.86729( )+ 0.93979( )- 6.6476( )+ 0.31681 ( )- 0.96749( )+469.34
late und
+ 3.8094(pH)- 0.37797(p02/10)+ 0.53180(pC02/10)- 0.32041 (BE)-l· 4.5486(BFHR/100)-H 0.27096(%UPIX10)+ 0.17362(%CORDX10)-41.074
APGAR
'+ 23.344( )- 0.94380( )+ 0.8001 2( }- 0.21 998( )- 5.00000( )+ 0.1 601 1( )- 0.0791 56( )-166.24
=- 1610.0( )- 7.61 74( )- 90.465( )+ 23.61 2( )- 15.995( )
0.8781 2( )+ 0.79376( )+12298.0
- 74.872( )+ 3.7620( )- 0.27992(+ 0.63242(- 30.116( )+ 0.59645(~ 1.1538( )+ 588.75
=-f 9.4500(pH)- 1.4188(p02/10)-f- 1.1950(pC02/10)- 0.53702(BE)-r- 3.9903(BFHR/100)•f 0.042273(%UPIX10)- 0.092590(%CORDX10)-82.039
Fig. 3. A pair of discriminant functions for the APGAR scores at l and 5 minutes after birth based upon a set of sevenfetal parameters at a given stage of childbirth.
J. Pcrinat. Mcd. 2 (1974)

114 Takemura et al., Computer prediction of neonatal conditions
CD=3-4-5cm 6-7 cm 8-9 cm early Hnd 'ate und
A iPGAR
1 min.
11
8
23
5
3
3
15
1
0
3
9
0
1
5
7
1
10
11
'33
4
Pred.
APGAR5 min.
11
3
30
3
Pred.
17 11 48
Fig. 5. The results o£ a number of cases äs predicted by the set of discriminant functions äs described in Fig. 3, utilizingseven fetal parameters, pH,PO2, PCO2, actual base excess, basal FHR, %UPI, and %CORD at a stage.
K: numuber of dependent variable
Y: dependent variable
X(i): independent variable =1.···.
V(i.j):covariance matrix of X
COE(i): regression coefficient.
clear SYX AN.COEV. SM. SYY. SY. NS
AN<-AN+1SY«-SY+YSYY<-SYY+YXY
SYX(i)<-SYX(i)+Y*X(i)
JLSYX(i)«-SYX(i)-SM(i)* SY/AN
Matrix InversionV<-V '
COE(i)«-COE(i)+V(i.j)*SYX(j)j=1.-, Ki = 1. · · · . K
OutputCOE(i)
Fig. 6. Computing flow chart for partial regression analysisof APGAR scores at l and 5 minutes, respectively, usingseveral fetal parameters.
and D is the newborns incorrectly diagnosed äs"to be vigorous" although, actually, they weredepressed.
2.2 Partial regression analysisFig. 6 is an example o£ a Computing flow chart _ , .for obtaining a regressional equation for APGARscores at both one and five minutes after birthby partial regression analysis from the data at ceach stage of labor. The same sets of completedata of seven fetal parameters äs in Tab. II wereused for the regression in forty-seven cases at theearly first stage. The equations, thus obtained,predicting the APGAR scores at both one andfive minutes after birth are shown in Fig. 7.Some of the estimated APGAR scores are com-pared with actual ones in Tab. III.The correlations between the actual APGARscore (ordinate) and the predicted one (abscissa) 'are plotted on graphs äs shown in a pair ofexamples of Fig. 8. Then, the accuracy of theprediction was again tested by the f our categories'representation äs shown in the number of casesof Fig. 9.
2.3 Comparisons between the two Computertechniques
According to the definition of probability of ,correct diagnosis (PCD) äs (A + C)/(A + B + '
J. Perinat. Med. 2 (1974)

Takemura et al., Computer prediction of neonatal conditions 115
STAGE 00=3-4-5 cm CO-6-7cm CD-8-9 cm
-57.190242(AI)+ 0.13237703(81)- 034952788(01)- 0.75636481(01)+ 0.029290606(EI)- 0.5931 1087(FI)'+ 0.90530631(01)+ 7.4680851
5--25.91 591 6(AI)-f 0.034134722(81)- 0.16556578(01)+ 0.3456413(01)+ 0.0054327945(61)- 0.94582967(F1)+ 0.66506851(61)+ 8.5744680
AI -pH- 7.2902 123B I-pOa- 18.925529CI=pCOa- 47.972336D I-BE+4.1 234036E I-BFHR-1 46.63829FI-%UPI- 0.21 163995G I=-%CORD -0.3666801 2
H-84.920758(AD)·*· 0.1 1824057(8 Π )-f 0,71923496(0 Π )- 1.0496064(00)+ 0.014433495(ΕΠ)- 2.8628641 (FD)-H 0.1 9212870(0 Π )+ 7.6363636
+ 47.21 4978(ΑΠ)-f 0.0591 17744(ΒΠ)+ 035035301 (CD)- 0.66235943(0 Π)+ 0.020527066(EO)- 1.6034803(FD)+ 0.42703847(60)+ 8.6818181
AD-pH-7.2813630ΒΠ-ρΟί-1 7.677270Cn=pCOj -46.736358Dfl-BE+5.1 227269E Π-BFHR- 152,600000Fn«=%UPI-0.34818640Gn*=%CORD -0.43944969
+26.101913(AO)+ 0.026506836(801)+ 0.13161483(CD1)- 0.44784275(001)- 001 2771 252(EOI)- 3.5171248(FOI)+ 2.2212651(601)+ 7.7500000
+ 9.2879630(Affl)- 0.038835328(801)+ 0.030798652(001)- 0.21765830(001)+ 0.00753 18463(E ffl )- 2.0152945(F01)+ 0.4088 2846(G ffl )+ 8.9166666
AOI=pH-7.2683328801 -pOj-1 6.958332C 01 =pCO>- 47.31 6663Dffl-BE+6.1083330E D -BFHR- 154.1 6666F DI =% UPI -0.3 1627886GID-%CORD-0.520436i
earty Dnd
-44.563751 (AN)+ 0.26802575(BW)- 0.34332828(CN)+ 0.605 35095(0 IV)- 0.0035335822(EW)- 0.37129498(FW)-f 3.6278252(GW)+ 66428571
+ 0.27197726(AW)+ 0.0043037027(BW)- 0.069672665(0W)+ 0.068284043(DN)-f 0.0056399830(EN)- 0.38603877(FW)+ 1.2457307(0 W)-f 8.6428571
A p/=pH-7.2814281BW»pOa-16.621427CW«pCOa-47.114280DIV «=BE+5.4 642854E IV=BFHR-147.14285FW-%UPI-0.41656874
late Und
-40.465144(AV)+ 0.16502163(BV)- 0.21460333(CV)+ 0.75342546(DV)- 0.030099188(EV)- 2.0408312(FV)- 0 34620959(GV)+ 7.500000
-47.629169(AV)+ 0.053045685(BV)- 0 29220040(CV)+ 0.87152588(DV)- 0.023061280(EV)- 0.059476791 (FV)+ 0.19240421 (GV)+ 8.6379310
AV=|
CV*DV*EV=FV·
'pH-7.2646548'pOi-15.086203'pCC-2-50.112064'BE+5.1931031=BFHR-143.62068=%UPI-0.46783039'%CORD-0.67467240
Fig. 7. A pair of partial regression functions for l and 5 minutes' APGAR scores based upon a set of seven fetalParameters at a given stage of childbirth.
101min. Apgar Score
(13) .
(3)
10oro
87
5 min. Apgar Score
(0)
(6)
0 7 8 10 0 7 8 10pred. pred.
Fig. 8. A pair of examples of a correlogram between the estimation by the two partial regression functions at theearly first stage of labor and the actual APGAR cores at l and 5 minutes after birth.
CD==3-4-5cm 6-7cm 8-9cm early lind late Und
A 1PGAR
1 min.
HGAR5 min.
13
10
0
0
21
3
Pred.
41
6
5
4
1
1
13
0
19
1
13
11
30
4
Pred.
12 12 50
i Fig. 9. Prediction of APGAR scores with partial regression functions s described in Fig. 7, using the seven fetal para-meters pH, PO2, PCO2, actual BE, mean BFHR, %UPI, and %CORD at a stage.
J. Pcrinat. Med. 2 (1974)

116 Takemura et al., Computer prediction of neonatal conditions
Tab. III. Examples of predicted APGAR scores by partialregression analysis.
Gase Actual EstimatedNo. APGAR s. APGAR s.
60 5.00000 6.3898961 7.00000 8.6514962 9.00000 7.3846864 5.00000 5.9724771 9.00000 7.4089772 8.00000 6.9242673 8.00000 8.2107074 9.00000 7.0231075 6.00000 8.9180978 8.00000 7.3574780 3.00000 7.4555681 2.00000 4.8423582 9.00000 8.1309583 9.00000 8.7885284 8.00000 6.8162088 3.00000 7.2426892 9.00000 8.2773193 8.00000 8.4991296 9.00000 8.0198297 9.00000 7.8336198 9.00000 8.0633799 7.00000 8.22959
100 9.00000 8.03133
C + D) in the four groups shown in Fig. 4, thediagnostic probabilities o£ these two techniquesat each s tage are compared with APGAR scores atone and five minutes. The diagnostic reliabilityfor the depressed neonates (DRDN), which isdefined äs C/(C + D) C/(B + D) is the prob-
äbility to satisfy necessary äs well äs sufficientconditions for the diagfiosis of the depressedinfants, is also compared. Both the above, PCDand DRDN, are calculated from the numbers inFig. 5 and Fig. 9 and are summarized in Tab. 4.
3, CommentThe Computer, often called an artificial brain, hasopened a new era in techniques, replacing thehuman brain by electronic logic and memorydevices. Astronomical, weather and economicaltrend predictions are based upon certain logicalprocessing of up-to-däte Information which maybe vastly complicated and yet analyzable bystatistical means. Prediction of fetal outcome atbirth is quite a similar Situation although it is alsovery complicated and it is difficult to believe inthe continuity of the fetus in utero to the ex-trauterine neonate. Too many unpredictableinterferences can occur during such a shortperiod of time. It is hardly possible to imaginethat such a dynamic unpredictability of childbirthcan be overcome by logical or rational judgmentsusing various kinds of measurements or infor-p
mation. How much is contributed to this problemby Computer techniques. The preliminary resultsin this report are seemingly not so satisfying. Ifthe probäbility Of correct diagnosis (PCD) byComputer techniques is compared with that bythe simple pH criterion [2, 6, 7] in the samegroup of subjects, the percentages are not so
Tab. IV. Comparison between diagnostic probäbility —I (PCD) and —VI (DRDN) for correct discrimination o£ neonatalconditions in four categories' diagnoses by a pair of Computer predictions (DFA and PRÄ) based upon 7 fetal parameters(Fig. 5 und Fig. 9) and that of a single fetal criterion that if the pH is less than 7.20 the infant will be depressed (Fig. 10).
/D\FW
B-n
Stage
APGAR
PCD%DRDN%
PCD%DRDN%
PCD%DRDN%
CD=3-
1 min
66.025.9
66.033.5
70.20.0
-4— 5cm
5min
70.210.7
87.30.0
85.10.0
CD =1 min
81.837.5
77.344.4
86.425.0
6 — 7cm
5min
86.440.0
90.925.0
95.550.0
CD =
1 min
100.0100.0
91.775.0
75.033.3
8— 9cm
5 min
—
100.00.0
66.70.0
Early
1 min
85,769.5
78.666.7
64.316.7
Und5 min
86.766.7
85.70.0
78.60.0
Late1 min
75.928.4
70.733.6
75.818.5
lind
5min
89.735.6
89.716.0
82.88.9
DFA: discrimination function analysis, PRÄ: partial regression analysisPCD: probäbility for correct diagnosis (A + C)/(A + B + C + D)DRDN: diagnostic reliability for depressed neonates C/(C + D) X C/(B + C)
J. Perinat. Med. 2 (1974) \

Takcmura et al., Computer prediction of neonatal conditions 117
A 3PGAR1 min.
CD - 3-4
1
0
•6cm
33
13
6-7cr
0
1
n
18
3
8-9c
2
2
m
7
1
early
0
1
nd
8
5
late II
4
5
nd
39
10
Fred.
A iPGAR5 min.
1
0
40
6
Fred.
20 11 46
Fig. 10. Discrimination of neonatal conditions by a single fetal pH criterion, i. e. if thc fetal capillary blood's pHis lower than 7.20, then the Jnfant is expected to be depressed. The subjects are the same äs computed for Fig. 5and Fig. 9, äs described in Tab. 1.
much higher in the former than the latter evenafter such complicated processing of the manyParameters (Fig. 10 and Tab. IV). The possiblereasons for this are äs follows:1. The probability for correct diagnosis (PCD)is quite dependent upon the percentage incidenceof vigorous babies among the total number ofcases, and it is fairly difficult to achieve a markedincrease in it by any means.2. The number of the cases f ed into the Computeris too small and the distribution of the datadeviates too much f rom the GAUSsian distributionto have a good resolution.3. The processed data sampled during twentyminutes at a given stage are not sufficient enoughto clarify the pathogenesis of fetal and neonataldepression. For example, during the samplingperiod of twenty minutes acute depression of thefetus due to interrupted umbilical circulation [5]just several minutes before birth cannot always bereflected in the averaged value of fetal parameters.In fact about one third of the cases of neonataldepression in our series can be ascribed to suchacute depression.Sampled data have definite shortcomings. Sam-pling of fetal blood can never be done contin-uously in present circumstances, so that thecontinuous monitoring of FHR is quite in-formative in that sense. However, even withsuch sampled Information in the blood the fetal
pH has great diagnostic significance betterthan any other parameters äs seen in the highachievement in PCD (DP-I) by the single pHcriterion of Tab. IV. The fact that the largestcoefficient was found in the pH term in all theequations of Fig. 3 and Fig. 7 is also quite con-vincing. Therefore, sampled data of fetal bloodmay never be considered äs perfect Informationbut are still quite important for clinical judgment.The continuous data provided by FHRmonitoring is not a decisive factor but rathera screening aid to complement the decisionwhen, and in what case, to take a fetal bloodspecimen from the presenting part. In that sensethe sampled data System described here wasrepresented by an averaged value of each para-meter during a sampling period of twentyminutes. This timing was rather random be-cause a stage of labor for data sampling wasdefined according to the cervical dilatation. Inother aspects, however, it is a clinically meaning-ful Situation because of the fact that it is notalways possible to monitor all childbirths fromthe beginning to the end. In practice obstetriciansfrequently face the Situation where they have tomake a decision to deliver a fetus, through thevagina or by cesarean section, just on a limitedamount of Information.Sometimes it is rather dangerous to sit at amonotonous monitoring desk, because we fre-
J. Perinat. Med. 2 (1974)

118 Takemura et al., Computer prediction of neonatal conditions
quently become accustomed to seeing slight ab-normal findings and hence we lose a sense ofgood timing that would allow us a decisiveaction. Analog data are easily overlooked evenwith the slightest but definite abnormalities, sothat quantification of the analog Signals should bean obligatory process for human pattern recogni-tion. Also the digitized data loses some Infor-mation, if it is done by certain limited number ofsamplings. Both the analog and the digital dataprocessings should be useful. In fact äs describedpreviously, the continuous monitoring of FHRis the way to detect fetal distress at the earliestpossible time. This produces, however, manyfalse positive results in otherwise vigorousinfants. On the contrary, the pH of fetal bloodis quite a decisive parameter in predicting adefinitely depressed infant if it is truly lower thannormal, although it is rather late to have a realdecrease of pH value in the fetal blood.If we turn our eyes from the task of screeningnormal babies out of the depressed who shouldbe detected äs early and äs accurately äs possible,it is astonishing that the diagnostic reliabilityfor the depressed neonate (DRDN) in Tab. IV isvery much improved by both Computer tech-niques, surpassing the results of single parameterprediction by means of fetal pH. The variousmerits of seven fetal parameters all seem to becontributing to these results, which are en-couraging enough for us to revise the mathe-matical models upon which we have processedthe data. More extensive data should be accu-
SummaryIn order to avoid subjectively biased judgment, two Com-puter prediction Systems for l and 5 minutes' APGARscores have been developed on the basis of multi-variableanalysis of fetal data. One uses discriminant analysis todifferentiate the depressed infant of APGAR 7 or less fromthe normal of 8 or more, the other is partial regression ana-lysis to estimate the APGAR score itself by a regressionfunction derived from a set of fetal variables at each stageof labor. More than one hundred cases were monitoredcontinuously by electronic äs well äs biochemical means atYale New Haven Medical Center in 1966—67, but onlycases with complete sets of Information (such äs fetalcapillary blood pH, PO2, PCO2, actual base excess (BE), thelevel of basal fetal heart rate (BFHR) and the percentageincidences of late and variable FHR decelerations over anumber of uterine contractions (%UPI and %CORD),during a sampling period of twenty minutes at each stage of
mulated from a larger population. The type ofdistribution of data and %he correlation betweenthem should be rechecked. The time course ofeach fetal parameter during the five stages inutero can be informative in the prediction, eventhough it is unrealistic to expect to get a füll setof Information at every stage of labor, in allindividuals. Hence^ if we can add some defectivedata by statistically reasonable Interpolation by aComputer we shall be able to produce a markedincrease in the number of processable cases withbetter prediction in the future.
4. Conclusions1. Two Computer prediction Systems of fetaloutcome in terms of l and 5 min. APGAR scoresbased upon complete sets of seven fetal parameters1. e., pH, PO2, PCQ2, actual BE, mean BFHR,%UPI and %CORD which were sampled at eachstage of labor (early, middle, late Ist stage, earlyand late lind stage) have been developed, usingthe data of biochemically. and electronicallymonitored childbirths at the Yale New HavenMedical Center.2. Neither Computer techniques, discriminantanalysis or partial regression analysis, couldachieve a marked increase in the PCD (probabilityfor correct diagnosis) over the results of a singlepH criterion, but they did greatly improve theDRDN (diagnostic reliability for the depressedneonate), which encourages us in the furtherautomatic monitoring of childbirths.
labor, were provided for computation äs shown in Tab. I.A course of labor was divided into five stages, namely theearly first stage of 3—4—5 cm cervical dilation, the middlefirst stage of 6—7 cm, the late first stage of 8—9 cm, theearly second stage, and the late second stage which was 'the last twenty minutes just before delivery. Several times'measurements of fetal blood pH were made with anASTRÜP pH-meter. The PÖ2 and PCOg were measured bya micro IL meter during the sampling period of twentyminutes and were averaged to give a set of data for onecase at each stage. Base excess was calcülated from theSIGGAARD-ANDERSEN alignment nomogram. The level ofthe BFHR was also an averaged value of the basal FHR ·during all uterine contractions during the twenty minutes lof continuous recording. Such sampled data from the ifetus is not complete monitoring but is, nevertheless, in >'lpractice, quite important, because the obstetrician often has
J. Perinat. Med. 2 (1974) $

Takcmura et al., Computer prediction of neonatal conditions 119
to make a dccision äs to dclivcr a fetus vaginally or ab-dominally on a relatively limitcd amount of Information.Some examples of such data for computation are shownin Tab. II. The respective discriminant functions for oneand five minutes' APGAR scores, at any one of the fivcstages, are summarized in Fig. 3 so äs to give a positivevalue if the fetus is to be born vigorous and a negativeone if depressed.
According to correlograms between the Computer pre-diction and the actual outcome shown in Fig. 4, the numberof cases of correct or false diagnosis are summed up inFig. 5. The probability for correct diagnosis [PCD =(A + Q/(A + B + C + D) in Fig. 4] is about 85 percent äs shown in Tab. IV.
Another computation was carried out to get partial re-gression functions (Fig. 7) in order to predict one and fiveminutes' APGAR scores themselves, äs shown by theexamples in Tab. 3. The probability for correct diagnosis bythese equations is once again evaluated by the number ofcases of correct and false discrimination and shows 70—90%accuracy and is therefore similar to the results obtainedby discriminant analysis. However, äs Tab. IV clearlyshows, these probabilities for correct diagnosis are littlebetter than the achievement of the simplest, single pHdiscrimination, which states that if the fetal capillary bloodpH is greater than or equal to 7.20, the baby should not bedepressed. This poor result, even by computation, can beascribed to several factors:
1. The percentage of vigorous infants among all the casesstudicd was too high to achieve a marked increase inthe probability for correct diagnosis (PCD).
2. The number of cases was too small especially in thedepressed and deviates too much from the GAussiandistribution.
3. The sampled and averaged data in a twenty minuteperiod of a given stage did not providc precise enoughinformation.
However, these methods demonstrate the great significanceof the fetal blood pH. This is shown by the pH term, whichhas the largest coefficient value in any of the equationsnot only of the discriminant functions but also of thepartial regression functions. On the other hand when weconsider the diagnostic reliability for the depressedneonate [DRDN = C/(C + D) X C/(B + C) in Fig. 4],it is surprising that the two Computer techniques havemade such improved probabilities äs high äs 30—70%in contrast to the single pH judgments which have, onaverage, a DRDN of about 25% (including many zeros atvarious stages, Tab. IV). These diffcrences should meangrcat improvement in the clinical management of verysick fetuses, because detection of the depressed infants äsearly äs possible and äs accurately äs possible is the majortask of fetal diagnosis during labor. The various merits ofseven fetal parameters all seem to be contributing to theseimproved results. Hence we are sufficiently encouraged toaccumulate more data and to revise our mathematicalmodels upon which we have processed the data.
Keywords: Computer prediction, APGAR score, fetal heart rate, fetal capillary blood, discriminant analysis, partial re-gression analysis, diagnostic probabilities.
ZusammenfassungComputervorhersage des NeugeborenenzustandesUm subjektive Einflüsse auszuschließen, wurden auf derGrundlage einer Vielfaktorenanalyse der fetalen Meßdatenzwei Computer-Vorhersagesysteme für den l- und 5-Minuten APGAR-Wert entwickelt. Das eine benützt dieDiskriminanzanalyse zur Unterscheidung des deprimiertenKindes mit einem APGAR von 7 oder weniger von demnormalen mit einem APGAR von 8 oder mehr. Das anderebenützt die partielle Regressionsanalyse, wobei der APGAR-Wert selbst geschätzt wird, als Regression einer Funktion,die sich von einem ganzen Satz fetaler Variabler in deneinzelnen Stadien der Geburt ableitet. Über 100 Fällewurden am Yale New Haven Medical Center in der Zeitvon 1966—1967 kontinuierlich sowohl elektronisch alsauch biochemisch überwacht. Aber nur Fälle mit einemvollständigen Satz an Informationen (nämlich pH, PO2,PCO2 und aktueller Basen Exzess im fetalen Kapillar-Blut,die basale Herzfrequenz des Feten, und prozentuale An-gaben über Spättiefs und variable Tiefs der fetalen Herz-töne bezogen auf die Zahl der Wehen) und zwar »über eine20-Minuten-Phase für jedes Stadium der Geburt wurden fürdie Computer-Auswertung verwendet wie dies in Tab. Igezeigt wird. Der Geburtsverlauf wurde in 5 Phasen einge-teilt, nämlich die frühe Eröffnungsperiode bei einer Zer-vixdilatation von 3—4—5cm, die mittlere Eröffnungs-periode bei einer Zervixdilatation von 6—7 cm, die späte
Eröffnungsperiode bei 8—9 cm, die frühe und die späteAustreibungsperiode; letztere umfaßte die letzten 20 Mi-nuten vor der Entbindung. Mehrfach wurden Messungendes fetalen Blut-pH mit einem AsTRUP-Gerät durchgeführt.PO2 und PCO2 wurden mit einem Micro-IL-Meßgerätwährend der 20-Minuten-Phasen gemessen, und ein Mittel-wert errechnet, um für jeden Fall zu jedem Stadium einenSatz an Meßdaten zu erhalten. Der Basen-Exzess wurdenach dem SiGGAARD-ANDERSEN-Nomogramm ermittelt.Die Höhe der Basalherzfrequenz des Feten war ebenfallsein gemittelter Wert der basalen fetalen Herzfrequenzwährend der Wehen innerhalb der 20-Minuten-Phasen, diekontinuierlich registriert wurden. Die so stichprobenartiggewonnenen Meßdaten des Feten bedeuten keine voll-ständige kontinuierliche Überwachung, sind aber dennochin der Praxis von großer Bedeutung, da der Geburtshelferoft mit einer relativ begrenzten Anzahl von Informationenentscheiden muß, ob die Entbindung auf vaginalem oderabdominalem Wege zu Ende zu führen ist. Einige Bei-spiele solcher Meßdaten für die Computerauswertung sindin Tab. II dargestellt. Die entsprechenden Diskriminanz-Funktionen für den l-Minuten und 5-Minuten APGAR-Wert während jeder der 5 Geburtsphasen sind in Fig. 3zusammengestellt, wobei sich ein positiver Wert ergibt,wenn der Fetus in einem lebensfrischen und ein negativer,wenn er in einem deprimierten Zustand geboren werden
J. Perinat. Mcd. 2 (1974)

120 Takemura et al., Computer prediction o£ neonatal conditions
wird. Entsprechend der Gegenüberstellung der Computer-vorhersage und dem tatsächlichen Ergebnis wie es in Fig. 4dargestellt ist, sind die Fallzahlen der korrekten und derfalschen Diagnosen in Fig. 5 zusammengestellt. Die Wahr-scheinlichkeit der richtigen Diagnose liegt bei etwa 85%wie es in der Tab. IV gezeigt wird. Ein anderes Computer-auswertungssystem wurde zur Ermittlung partieller Re-gressionsfunktionen verwendet um die 1-Minuten und5-Minuten-ApGAR-Werte selber vorherzusagen, wie an-hand von Beispielen in der Tab. III dargestellt ist. DieWahrscheinlichkeit der richtigen Diagnose bei diesemRechengang wurde ebenfalls durch die Gegenüberstellungder Zahl der Fälle richtiger und falscher Einschätzung er-mittelt; sie zeigt eine Genauigkeit von 70—90% und istdamit vergleichbar mit den Ergebnissen die durch dieDiskriminanzanalyse erzielt wurden. Die Wahrscheinlich-keit der richtigen Diagnose aber ist, wie Tab. IV klar dar-legt, größer als wenn man sie von einer einfachen einzelnenpH-Bestimmung ableiten würde, was die Feststellung zu-läßt, daß bei einem fetalen kapillaren Blut-pH von 7,20 und
, \ höher das Neugeborene nicht deprimiert sein wird.Dieses spärliche Ergebnis der Computerauswertung kannverschiedenen Faktoren zugeschrieben werden:1. Der Prozentsatz der lebensfrischen Kinder unter den
untersuchten Fällen war zu hoch, um einen deutlichenAnstieg über den Normalprozentsatz zu erzielen.
2. Die Fallzahl war zu klein und streut zu sehr über dieGAUsssche Verteilung hinaus.
3. Die innerhalb von 20-Minuten-Phasen für jede Ge-burtsphase gewonnenen, fund gemittelten Meßdatenlieferten nicht genügend Informationen. Dennochzeigen diese Methoden die große Bedeutung des fetalenBlut-pH. Dies ist dargestellt am pH-Wert, der dengrößten Koeffizienten in allen Rechengängen hat, nichtnur bei der Diskriminanz-Funktion sondern auch beider partiellen Regressionsfunktion.
Wenn wir andererseits die diagnostische Zuverlässigkeitbezüglich des deprimierten Neugeborenen betrachten, soist es verwunderlich, daß die beiden Computertechnikendie Wahrscheinlichkeit auf 30—70% erhöhten. Demgegen-über beträgt die Wahrscheinlichkeit einer korrekten Vor-hersage bei alleiniger Beurteilung durch eine Einzel-pH-Messung durchschnittlich etwa 25% (Tab. IV). Diese Unter-schiede können eine bedeutende Verbesserung bedeutenfür die klinische Betreuung sehr kranker Feten, denn diemöglichst frühe und möglichst genaue Erkennung desdeprimierten Kindes ist die vorrangige Aufgabe der fetalenDiagnostik unter der Geburt. Die sieben verschiedenstenfetalen Parameter scheinen alle zu diesen verbesserten Er-gebnissen beizutragen. Von daher sind wir ausreichend er-mutigt, weiteres Material zusammenzutragen und unseremathematischen Modelle zu überarbeiten, mit denen wirdie Meßdaten ausgewertet haben.
Schlüsselwörter: Computervorhersage, ApGAR-Wert, fetale Herzfrequenz, fetales Kapillarblut, Diskriminazanalyse,partielle Regressionsanalyse, diagnostische Wahrscheinlichkeiten.
ResumSPrediction par ordinateur de Petat du nouveau-negräce ä Fanalyse d'informations sur le rythme car-diaque foetal et le sang capillaire au cours du travailAfin d'eviter les jugements subjectifs et partiaux, deuxsystemes de prediction, par ordinateur, ont ete etablis pourles index d'ApGAR ä l et 5 minutes par des methodes d'analyse de variables multiples a partir d'informations ob-jectives sur le foetus.L'une est une analyse discriminante permettant dedistinguer les nouveau-nes deprimes avec un APGARegal ou inferieur ä 7 de ceux qui sont normaux avec unAPGAR egal ou superieur a 8. L'autre est une analyse deregression partielle permettant d'evaluer l'index d'APGAR lui-meme par une fonction de regression calculeea partir d'un ensemble de variables foetales ä chaque stadedu travail.Parmi les cent cas avec surveillance continue par moyenselectroniques et biochimiques au Centre Hospitalier deTUniversite de Yale en 1966 et 1967, seuls les cas avec unensemble d'informations complet (pH, PO2, PCO2, exces debase (B. E.), niveau de rythme cardiaque foetal de base(B. F. H. R.), et pourcentage de d6celerations tradives etvariables par rapport au nombre de contractions uterines(%UPI et %CORD) pendant une periode de vingt minutesau cours du travail, ont ete utilises pour les calculs comme
le montre le Tab. I. Le travail a ete divise en cinq stades:dilatation cervicale de 3—A—5 cm, 6—7 cm, 8—9 cm, stadede debut d'expulsion et les 20 minutes precedant l'ac-couchement. Si plusieurs mesures du pH sanguin foetal parl'appareil d'AsTRUp et de la PO2 et la PCO2 par une me-thode de micro-mesure etaient pratiquees dans chaqueperiode de 20 minutes, on faisait la rnoyenne des resultatsobtenus pour avoir un ensemble de donnees a chaquestade.L'exces de base a ete calcule sur le graphique de SIGGAARD-ANDERSEN. Le rythme cardiaque foetal de base a ete obtenuen faisant la moyenne des rythmes de base (B. F. H. R.)pendant 20 minutes. Les informations obtenues sur lefoetus ne suffisent pas pour realiser une surveillance com-plete. Elles sont cependant tout-ä-fait importantes pouraider ä porter un jugement en clinique parce qu'en pratiquel'obstotricien doit souvent prendre la decision d'extraire lefoetus par voie vaginale ou abdominale sur un nombrelimite d'informations.Le Tab. II montre des exemples de donnees utilisables pourles calculs. Dans la premifcre etude, les fonctions discrimi-nantes ont ete con$ues de teile sorte qu'on obtienne unchiffre positif si le nouveau-ne est vigoureux, et nogatifs'il est deprime comme on Fa resume Fig. 3 pour chacun descinq stades et pour les index d'ApGAR une minute et cinq,;:minutes respectivement.
J. Perinat. Med. 2 (1974) j
l

Takcmura et al., Computer prediction of neonatal conditions 121
Lcs quatre catogories diffarentes du tableau de corrdlationentre les valeurs predites et reelles sont montrees Fig. 4.Le nombre de cas avec diagnostic exact ou faux est prcsenteFig. 5. La probabilite d'un diagnostic exact (PCD =«A + C»/«A + B + C + D»), c'est-i-dire le nombre decas dans lesquels Tetat du foetus (doprime ou non) estpredit correctement est de l'ordre de 85% en moyenneavec leslimitcs de 66% et 100% (Tab. IV).On a utilise le mSme ensemble de donnoes pour un autrecalcul, celui des fonctions de rogression partielle (Fig. 7)afin de prddire les Index d'ApGAR l et 5 minutes a chaquestade du travail sous forme digitale, tels qu'on le montreTab. III. Les probabilites de donner un diagnostic exact(P. C. D.) a partir de ces equations sont calculoes pour lespatientes ayant eu par Tetude discriminante des prddictionsexactes ou erronees. Le calcul donne des resultats identiques,pour 70 a 90% a ceux de l'etude discriminante (Tab. 4).Cependant, comme il est ddmontro clairement tab. 4, cesprobabilites de diagnostic exact ne sont guere meil-leures que celles obtenues par l'emploi du pH seule-ment, ce qui signifie que si le pH du sang capillairefoetal est superieur ou egal a 7,20, le nouveau-ne nedevrait pas etre άέρπτηέ et vice-versa. Ce resultat peutetre impute a plusierus facteurs:1°) Le pourcentage d'enfants vigoureux est trop elevo
pour qu'on puisse atteindre un niveau superieur,2°) Le nombre de patientes est trop petit et trop dovie par
rapport a la distribution de GAUSS, et,
3°) Les donnees que Γόη a mesuroes et dont on a fait lamoyenne en 20 minutes pour un certain stade nepeuvent pas apporter suffisamment d'informations.
Mais par n'importe quelle voie on peut domontrer la hautevaleur diagnostique du pH sanguin foetal meme par lecoefficient έίενέ obtenu pour le pH dans chacune desoquations, non seulement dans les fonctions discriminantesmais aussi dans les fonctions de regression partielle (Fig.3 et 7).Par ailleurs, si nous examinons la fiabilito du diagnostic(DRDN =5 C/«C + D» X C/«B + C») dans le cas denouveau-nos doprimos, en ce qui concerne les conditions^cessaires mais aussi s ffisantes pour dotecter Petat dedepression aussit t que possible et aussi exactement quepossible, il est surprenant d'avoir une el£vation des pro-babilitas de l'ordre de 30 a 70% environ par les deux me-thodes de calcul sur le simple pH qui reprosente environ25% de probabilites mais avec nombreux zoros a difforentsstades (Tab. 4). Ces difforences pourraient se traduire par uneimportante amolioration dans l'attitude pratique, en Cli-nique, pour les foetus en tres mauvais etat, puisque c'estchez ces derniers que se posent les problemes diagnostiquesmajeurs. Les differentes valeurs des sept paramatres foetauxsemblent toutes jouer un role dans les resultats, qui sontassez encourageants pour que d'autres donnees soientreunies et que Γόη tente de verifier les methodes de calculutilisees pour le traitement de nos informations.
Mots-cles: Prediction par ordinateur, index d'ApGAR, rythme cardiaque foetal, sang capillaire foetal, analyse discrimi-nante, analyse par regression partielle, probabilites diagnostiques.
AcknowledgementsThe clinical parts of this work were carried out when one of the authors was at Yale University School of Medicine s aFULBRIGHT research fellow from the U. S. Department of State and s a JAMES-HUDSON-BROWN Memorial postdoctoralfellow from Yale during 1966—67. The authors express sincerest thanks to Prof. K. KURACHI of Osaka University MedicalSchool and to Prof. E. J. QUILLIGAN and Dr. E. H. HON of University Southern California for their consistent en-couragement of this work.
Bibliography[1] APGAR, V.: The newborn (APGAR) scoring System.
Pediatric Clinic of North America 13 (1966) 645[2] BEARD, R. W., E. D. MORRIS: Fetal and maternal
acid-base balance during normal labour. J. Obstet.Gynaec. Brit. Cwlth. 72 (1965) 496
[3] DR GE, T. S., C. KENNEDY, H. BERENDES, B. K.SCHWARZ, W. WEISS : The APGAR score s an index ofinfant morbidity. Develop. Med. Child. Neurol. 8(1966) 141
[4] HON, E. H.: Detection of fetal distress. Fifth WorldCongress of Gynaecology and Obstetrics. In: WOOD, C.:Fifth World Congress of Gynaec. & Obstet. Butter-worths, Sydney 1967
[5] HON, E. H., A. F. KHAZIN: Biochemical studies of thefetus. Obst. & Gynec. 33 (1969) 219
[6] KUBLI, F.: Fetale Gefahrenzust nde und ihre Diagnose.Thieme, Stuttgart 1966
[7] SALING, E.: Das Kind im Bereich der Geburtshilfe.Thieme, Stuttgart 1966
[8] SIGGAARD-ANDERSEN, O.: The Acid-base Status of theBlood. Williams & Wilkins, Baltimore 1966
[9] TAKEMURA, H.: Optimization in discriminating pre-diction of APGAR scores by a fixed criterion of fetalParameters, pH, PO2, PCO2, BE, actual BE, basal FHR,%UPI, and %CORD (submitted for publication)
Hikaru Takemura, M. D.Department of Obstetrics & GynecologyOsaka University Medical Schooll—2, Dojimahamadori 3-chomeFukushima-ku, Osaka/Japan
J. Perinnt. Med. 2 (1974)