J. N. WALTON: MUSCULAR DYSTROPHY1344 23 May 1964 Craniopagus Twins-Franklin MDICALJOURNAL the time....
6
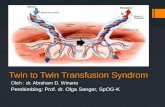
BRmIsH MEDICAL JOURNAL 23 May 1964 J. N. WALTON: MUSCULAR DYSTROPHY FIG. 1.-Focal musce-;fibre necrosis and phagocytosis in a female carrier of the Duchenne-type dystrophy. (H. and E. x 220.) . Wl E _ II E_; FIG. 2.-An area of abortive regeneration in a female carrier; the small fibre to the left of centre is basophilic and contains several large vesicular nuclei with prominent nucleoli. (H. and E. x220.) FIG. 3.-Electron micrograph, X 15,550, transverse section of muscle FIG. 4.-Electron micrograph, X 19,430, of muscle section from patient outained by biopsy from patient with muscular dystrophy of Duchenne with muscular dystrophy of Duchenne type, showing excessive numbers type. There is widespread loss of myofilaments with disorganization of of bodies, provisionally identified as lysosomes, lying between the myo- mitochondria and of the sarcotubular system. (From Pearce, 1964.) fibrils. (From Pearce, 1964.) A=Myofibrils. B=Z-band. C=Sarco- A = Relatively normal nmyofilaments. B = Area of myofilament loss. C= tubule. D = Lysosomes. E = Mitochondrion. Mitochondria. D = Collagen fibrils outside the sarcolemma. E =Sarco- lemma. F = Sarcotubule. FIG. 5.-Normal myoblasts; adult mouse muscle; phase contrast. (From FIG. 6.-A myoblast, presumed to be dystrophic; explant from a Pearce, 1964.) dystrophic mouse of the Bar Harbor strain; phase contrast. (From Pearce, 1964.) on 5 February 2020 by guest. Protected by copyright. http://www.bmj.com/ Br Med J: first published as 10.1136/bmj.1.5394.1336-a on 23 May 1964. Downloaded from
Transcript of J. N. WALTON: MUSCULAR DYSTROPHY1344 23 May 1964 Craniopagus Twins-Franklin MDICALJOURNAL the time....

BRmIsHMEDICAL JOURNAL23 May 1964
J. N. WALTON: MUSCULAR DYSTROPHY
FIG. 1.-Focal musce-;fibre necrosis and phagocytosis in a female carrierof the Duchenne-type dystrophy. (H. and E. x 220.)
.Wl E _ II E_;
FIG. 2.-An area of abortive regeneration in a female carrier; the smallfibre to the left of centre is basophilic and contains several large vesicular
nuclei with prominent nucleoli. (H. and E. x220.)
FIG. 3.-Electron micrograph, X 15,550, transverse section of muscle FIG. 4.-Electron micrograph, X 19,430, of muscle section from patientoutained by biopsy from patient with muscular dystrophy of Duchenne with muscular dystrophy of Duchenne type, showing excessive numberstype. There is widespread loss of myofilaments with disorganization of of bodies, provisionally identified as lysosomes, lying between the myo-mitochondria and of the sarcotubular system. (From Pearce, 1964.) fibrils. (From Pearce, 1964.) A=Myofibrils. B=Z-band. C=Sarco-A= Relatively normal nmyofilaments. B= Area of myofilament loss. C= tubule. D= Lysosomes. E= Mitochondrion.Mitochondria. D= Collagen fibrils outside the sarcolemma. E =Sarco-
lemma. F= Sarcotubule.
FIG. 5.-Normal myoblasts; adult mouse muscle; phase contrast. (From FIG. 6.-A myoblast, presumed to be dystrophic; explant from aPearce, 1964.) dystrophic mouse of the Bar Harbor strain; phase contrast. (From
Pearce, 1964.)
on 5 February 2020 by guest. P
rotected by copyright.http://w
ww
.bmj.com
/B
r Med J: first published as 10.1136/bm
j.1.5394.1336-a on 23 May 1964. D
ownloaded from

1344 23 May 1964 Craniopagus Twins-Franklin MDICAL JOURNAL
the time. Twin C had a precordial systolic murmur which hasnot persisted, Twin D a cleft of soft and part of hard palate. Atseven months Twin C had two left-sided fits associated withrespiratory infections. Despite phenobarbitone, fits had recurred.Twin C, who survived separation, was estimated at 17 months tohave a development level corresponding to 8 months. At a monthunder 3 years she weighs 28 lb. 12 oz. (13 kg.). She can situnaided for a time, rocks back and forth, crows and gurgles, saysmum and dad, can hold a toy in the right hand and takes, someinterest in her surroundings. She has a left spastic hemiplegia.
Pre-operative studies of behaviour showed that each twin reactedas a separate individual. One slept with the other awake orsucking a bottle or crying. Pulse, temperature, respiration, haemo-globin values differed. Electroencephalograms by Dr. G. Pampiglionerevealed independence of cerebral activity, including induction ofsleep and appropriate changes in the one given thiopentone byinjection. That the other was unaffected suggested no markedarterial communication.The post-operative course of both survivors was stormy and
difficult. Skin coverage has been made complete, and in neitherhas there been any evidence of destruction of the grafted freeze-dried dura mater. A series of plastic helmets of increasing sizehas protected the brains from further damage.
Conclusion
The paediatrician's part in the management and treatment ofcraniopagus twins is described together with brief case recordsof two pairs of such twins. If the object of the endeavour isto separate pairs of conjoined twins, the team that has onesurvivor from each of two pairs has scored a real success. Butif the object is regarded as restoring people who have met astrange fate to a normal happy family life, these cases aredisappointing.
It is a pleasure to record the untiring work during the longmonths of Dr. Seymour Mason, Dr. Kenneth Hugh-Jones, and thehouse-physicians to the children's department at St. Bartholomew'sHospital, as well as the devotion of Sister Joan Clark, Miss B.Franklin, and the nursing staff.
REFERENCES
Franklin, A. W. (1960). Lancet, 1, 1065.- Tomkinson, J. S., and Williams, E. R. (1958). Ibid., 2, 683.Kenny, A. (1961). Daily Express, October 20.
Muscular Dystrophy: Some Recent Advances in Knowledge*
JOHN N. WALTON,+ M.D., F.R.C.P.
[WITH SPECIAL PLATE]
Brit. med. J., 1964, 1, 1344-1348
Genetic Research
Duchenne-type Muscular Dystrophy
Evidence in favour of a sex-linked or X-linked recessiveinheritance of this variety of muscular dystrophy in themajority of families comes, first, from a study of typicalpedigrees (Stevenson, 1953; Walton, 1955, 1956c); secondly,from the fact that affected males have been born of the samefemale but of different fathers (Walton, 1956c); thirdly, fromthe finding of a family in which there was a suggestion ofcrossing-over between this variety of dystrophy and red-greencolour-blindness (Philip, Walton, and Smith, 1956); and,fourthly, from the fact that the disease has been described intypical form in a " female " suffering from Turner's syndrome(ovarian agenesis) who was presumed to have an XO chromo-some constitution (Walton, 1956c). Although, as Boyer andFainer (1963) point out, none of these findings is absolutelyconclusive, nevertheless the evidence in support of sex-linkedrecessive inheritance of these cases would seem to be con-vincing even though no linkage has yet been demonstratedbetween this form of dystrophy and haemophilia or the newlydescribed Xg blood group. With the collaboration of Dr.Race we have examined a number of families and have foundno such linkage. An analysis of pedigrees has, however,amply confirmed that in a small proportion of families thereare affected females as well as affected males; this and otherevidence clearly indicates that the disease may sometimes beproduced by an autosomal recessive gene (Lapiy and de
Grouchy, 1954; Kloepfer and Talley, 1958; Dubowitz, 1960;Jackson and Carey, 1961).Chung and Morton (1959) give reasons for suggesting that,
whereas a considerable number of cases of muscular dystrophyof the Duchenne type arise as a result of a gene mutation,there are others in which the disease may be truly sporadic-that is, it may be due to manifestation in the heterozygote.Hence there is evidence to suggest that there can be funda-mental genetic heterogeneity among cases of clinically similarmuscular dystrophy. As Nirenberg (1963) has pointed out,intracellular transmission of abnormally coded D.N.A. infor-mation occurs within the cell when R.N.A. carries the codeinto metabolic steps which terminate in a quantitative orqualitative alteration of a particular enzyme. Metabolic path-ways associated with the expression of various specific genesoften overlap and in turn may cause an overlap in clinicalstigmata. We shall not be able to understand similarities anddifferences between neuromuscular entities which dependupon different genes until we understand the details of suchoverlap. Chung and Morton (1959) and Morton, Chung, andPeters (1963) have also given cogent reasons for suggesting thatalthough many cases of limb-girdle muscular dystrophy areclearly the results of an autosomal recessive gene and thephenotype appears in the homozygote, there are others whichare truly sporadic and are presumed to be due to expressionin the heterozygote.Of more direct practical importance are recent studies
carried out on female carriers of the sex-linked recessive generesponsible for most cases of the Duchenne-type dystrophy.Aebi, Richterich, Colombo, and Rossi (1962), Hughes (1963),and Pearce, Pennington, and Walton (1964c) have found thatover 70% of such female carriers can be identified by meansof serum creatine kinase estimation. Dreyfus, Schapira,
* Conclusion of the Goulstonian Lecture delivered to the Royal Collegeof Physicians of London on 20 January 1964. The first part waspublished last week.
t Neurologist, Regional Neurological Centre, Newcastle General Hospital;Physician in Neurology, Royal Victoria Infirmary, Newcastle uponTyne.
on 5 February 2020 by guest. P
rotected by copyright.http://w
ww
.bmj.com
/B
r Med J: first published as 10.1136/bm
j.1.5394.1336-a on 23 May 1964. D
ownloaded from

Schapira, and Demos (1961) detected 23 out of 26 carriersusing estimations of serum creatine kinase and measurementsof circulation time. More recently still, van den Bosch(1963) and Barwick (1963) have indicated that minor electro-myographic abnormalities suggestive of a myopathy may alsobe detected in carriers, and Emery (1963) and Pearson,Fowler, and Wright (1963) have demonstrated that there maybe minor clinical abnormalities such as minimal muscularwasting and pseudohypertrophy of the calves in a number ofcarrier females who are apparently unaffected clinically(Fig. A).
BRITISHMEDICAL JOURNAL 1345
of research, but would like simply to mention briefly some
of the techniques that are being utilized in the hope ofdetermining the nature of the fundamental pathologicalprocess. The principal methods of attack are by means
of the biochemical and histochemical study of muscle-biopsy samples; by investigation of the morphology of thedisease process with the aid of the electron microscope andby means of tissue culture and interference microscopy; and,finally, by electrophysiological studies of muscle-fibre andmembrane potentials. A considerable impetus to research hasfollowed the discovery of forms of hereditary musculardystrophy occurring in mice of the Bar Harbor strain(Michelson, Russell, and Harman, 1955) and in chickens(Julian and Asmundson, 1960), but although the disease pro-
cesses in these animals are clearly dystrophic it is impossible as
yet to say whether results obtained with such experimentalmaterial can necessarily be relied upon in studying the humandisease.
Biochemistry
Since the early observation that patients with musculardystrophy excreted excessive quantities of creatine in theurine (Levene and Kriszteller, 1909) a vast amount of bio-chemical work has been carried out and the concentration ofmany organic and inorganic compounds within dystrophicmuscle has been compared with that in normal muscle. Inthe table I have summarized from Dreyfus and Schapira
Variations in Constituents of Muscle Tissue in Muscular Dystrophy
Constituent
FIG. A.-Pseudohypertrophy of the calves in themother of two sons who were suffering from muscu-lar dystrophy of the Duchenne type. Her serumcreatine kinase was 54 units, amply confirming that
she was a carrier.
Dubowitz (1963) and Pearce, Pearce, and Walton (1964)have found definite histological abnormalities in musclebiopsies obtained from a series of carrier females (SpecialPlate, Figs. 1 and 2). These observations all give consider-able support to the Lyon hypothesis (Lyon, 1961, 1962) thatin a proportion of cells of the female one X-chromosome maybe inactivated. The evidence strongly suggests that in carrierfemales a proportion of the muscle cells are in fact dystrophicbut that usually this proportion is not large enough to giverise to clinically obvious weakness. Nevertheless, the methodsoutlined are of considerable value in the detection of carriers,and hence are useful for the purpose of genetic counselling.It is likely that within the next year or two methods of carrierdetection will become even more reliable.
Fundamental Research and the Pathogenesis. of the Disease
It is my firm belief that an effective treatment for pro-gressive muscular dystrophy will be discovered only when thefundamental biochemical defect or defects responsible for themuscular wasting which occurs as a result of the disease pro-cess are also discovered. Indeed, it seems that now we areable to detect preclinical cases of dystrophy, particularly ofthe Duchenne type, the correct time to attack the disease pro-cess would be at this stage before clinical weakness super-venes. I have not the time to describe fully modern methods
Change Constituent Change
Glycogen . . Decrease Respiratory enzymes:Lactic acid .. .. Succinic dehydrogenase Decrease
,, oxidase ..Glycogenolytic enzymes: Cytochrome ,, .. ,
Phosphorylase , , FumaraseAldolase .. .. AconitasePhosphoglucomutase .. ,, Cytochrome C ,HexokinaseLactic dehydrogenase .. Increase Protein compoundsTotal glycogenolysis Decrease Collagen .Increase
Myosin .DecreasePhosphorus compounds and Myoglobin . .other organics :TransaminasesATPCreatine phosphokinase Proteolytic enzymes IncreaseHexose phosphate .. IncreasePhosphocreatine .. Decrease Inorganic compounds:Creatine .. .. Potassium .. DecreaseCarnosine .. .. Sodium .Increase
Chloride.P04Iron .. Decrease
* From Pearson (1963).
(1962) and from Pearson ((1963) the biochemical abnormalitiesobserved in this disease. Considerable work has also beencarried out upon the nature of the myoglobin which is present
in dystrophic muscle. Perkoff, Hill, and Tyler (1962) havefound an abnormal pattern of myoglobin in childhoodmuscular dystrophy, as have Whorton, Hudgins, andConners (1961), but the significance of these observations inrelation to the nature of the dystrophic process remainsobscure and other protein studies directed particularly towardsestimations of actin and myosin concentrations in dystrophicmuscle have been disappointing. My colleague Dr.Pennington has demonstrated an increased concentration ofcathepsins, of acid phosphatase, and of 5-nucleotidase indystrophic muscle, but the increased concentration of theseenzymes may well be simply the result of tissue breakdown.Whereas it has been recognized for some considerable time
that such enzymes as aldolase and creatine kinase leak fromthe diseased muscle cell into the serum, and that this leakageis presumed to be due to a defect in the muscle-fibre mem-
brane, the concentration of these and other enzymes whichbehave similarly in dystrophic muscle is reduced to onlyabout 80% of the normal. Pennington (1962), however, found
23 May 1964 Muscular Dystrophy-Walton
on 5 February 2020 by guest. P
rotected by copyright.http://w
ww
.bmj.com
/B
r Med J: first published as 10.1136/bm
j.1.5394.1336-a on 23 May 1964. D
ownloaded from

that adenylic deaminase was reduced to about a third of thenormal value in both dystrophic mice and in human patientswith muscular dystrophy of the Duchenne type. This is themost striking reduction in enzyme content of dystrophicmuscle yet discovered, but its significance is obscure, as thefunction of this enzyme in muscle is not yet understood.McArdle (1963) has suggested that it is of importance to studyphospholipids within muscle in view of the importance ofthese compounds in the formation and integrity of the muscle-fibre membrane; recently my colleague Dr. Pennington hasbegun certain studies of phospholipid synthesis in muscle usingthin-layer chromatography and a technique whereby 14C-labelled phosphorylcholine is incorporated into lipid in mouse
skeletal muscle, but this work is still in its preliminary stages.
Also of considerable interest is a recent finding that invarious mammalian species, including man, lactic dehydro-genase exists in five electrophoretically distinct molecularvarieties in nearly all tissues, and that, in contrast to normaladult muscle which contains a preponderance of LD4 andLD5 isoenzymes, some patients with dystrophy lack LD5completely and have lesser quantities of LD4 (Wieme andHerpol, 1962; Dreyfus, Demos, Schapira, and Schapira,1962; Pearson, 1963). Further studies of this type will beawaited with considerable interest, and it seems plain that theincreasing volume of biochemical research now being carriedout is likely to be fruitful.
Histochemistry
Considerable interest was aroused by the suggestion ofBourne and Golarz (1959) that dystrophy might be due to a
primary proliferation of connective tissue in dystrophicmuscle; they demonstrated excessive activity of 5-nucleotidasein muscle biopsy samples. Subsequently, however (Golarzand Bourne, 1963), they have somewhat modified these earlierviews, and others (Dubowitz and Pearse, 1961; Engel, 1962)have failed to confirm their findings. Whereas histochemistryhas revealed that there are at least two types of muscle fibrein normal human muscle, one being rich in phosphorylase andthe other rich in oxidative enzymes (Dubowitz and Pearse,1961), there is no evidence that either of these fibre types is
specifically involved by the dystrophic process. Recently, too,A. G. E. Pearse (1963) has made the interesting suggestionthat monoamine oxidase, which is an important componentof the sarcotubular system concerned with the conduction ofthe electrical impulse into the interior of the muscle cell, maybe reduced in amount in cases of muscular dystrophy, butthis is a preliminary observation which as yet requires verymuch further study.
Electron Microscopy
As yet ultrastructural studies of diseased muscle are in theirinfancy. Following upon the important work of Huxley(1957) and others, Price (1963) has confirmed that the viewsexpressed about the ultrastructure of the muscle fibre whichwere based upon the examination of rabbit muscle can alsobe applied to man. At last the significance of the pattern oforganization in normal skeletal muscle which the electronmicroscope has revealed is being clarified. To date studies ofdystrophic muscle with this technique have not revealed anyspecific changes. Van Breemen (1960), Pearce (1963, 1964),and Mair (1963) have confirmed that disintegration andfragmentation of myofibrils and myofilaments may occur
(Special Plate, Fig. 3), but neither the actin nor the myosin
appears to be specifically involved and there is apparently no
selective damage to any single part of the sarcomere. Themitochondria and sarcotubular elements are also damaged,but the changes are not very different from those observed
BRITISHMEDICAL JOURNAL
in patients with other forms of myopathy such as polymyositisand even steroid myopathy. On the other hand, Pearce (1963,1964) has drawn particular attention to the excessive concen-
tration of vesicular bodies, provisionally identified as lyso-somes (Special Plate, Fig. 4), in dystrophic muscle. Incollaboration with Pennington (unpublished observations) hehas found that these bodies contain proteolytic enzymes suchas cathepsins and acid phosphatase; they may simply bepresent in a scavenging role. It is to be hoped (Pearson, 1963)that electron microscopical studies of muscle obtained frompreclinical cases of muscular dystrophy may help to identifythe earliest structural changes which occur in this disease.
Tissue Culture
Geiger and Garvin (1957) first suggested that the growthpattern in vitro of muscle obtained from muscular-dystrophypatients was different from that of normal adult human muscle,but Herrmann (1961) was unable to confirm these findingsand pointed to the difficulty of culturing adult human muscle.Pearce (1963, 1964) has described a technique of tissue cultureapplicable to adult normal mouse muscle and to dystrophicmouse muscle. He has found that on making small crushlesions in the muscle of such mice a typical histological pictureof regeneration was seen after five days. If such an area ofmuscle was excised and explanted there was a profuse pro-
duction of myoblasts in explants obtained both from normalmice and from dystrophic mice. 111e compared the explantsobtained from six dystrophic and six normal adult mice andfound certain distinctive differences. The nuclei of myoblastsfrom dystrophic cultures often contained only one or twonucleoli whereas the nuclei of normal myoblasts generallypossessed three (Special Plate, Figs. 5 and 6) or more.
Multinucleate myoblasts were found to be less common indystrophic cultures than in the normal, and non-striatedmuscle straps containing many nuclei were observed incultures from normal muscle but never in those fromdystrophic muscle. There was also an irregularity of themargins of those myoblasts which were presumed to bedystrophic. These findings strongly suggested that the musclecells in dystrophic animals were abnormal at an early stageof development.Ross (1964) has begun a study of the nuclei of normal and
dystrophic myoblasts using the interference microscope. Hehas shown that at the point when myoblasts fuse there is a
considerable reduction in the volume of individual nucleoliwithin the nuclei of the cells engaged in this activity. Hesuggests that this process of fusion involves considerablemetabolic activity which may temporarily lead to a depletionof the R.N.A. reserves in the nucleus. His preliminaryobservations, which will require confirmation, upon dystrophicmyoblasts, suggest that these contain significantly smalleramounts of nucleolar material than do normal myoblasts andthat they fail to fuse. Clearly much further work on tissueculture requires to be done before the significance of thesefindings can be elucidated, but despite the serious technicaldifficulties it seems likely that this method will be useful inthe investigation of the dystrophic process.
Electrophysiological Studies
It is now well established that by means of the insertion ofmicro-electrodes into individual muscle cells in vitro and invivo it is possible to make accurate recordings of muscle-membrane potentials both in animals and in man (Johns,
1958; Elmqvist, Johns, and Thesleff, 1960; Creutzfeldt,Abbott, Fowler, and Pearson, 1963). Johns (1963) has sum-
marized the differences between end-plate potentials recordedby this method and the muscle-action potential itself.
1346 23 May 1964 Muscular Dystrophy-Walton
on 5 February 2020 by guest. P
rotected by copyright.http://w
ww
.bmj.com
/B
r Med J: first published as 10.1136/bm
j.1.5394.1336-a on 23 May 1964. D
ownloaded from

23 May 1964 Muscular Dystrophy-Walton BoUff 1347
Important observations upon the phenomenon of myotoniahave already been made. Creutzfeldt et al. (1963) havedemonstrated a consistent reduction in membrane potential inpatients with hyperkalaemic periodic paralysis, many of whomalso show myotonia, and, as Johns has indicated, there is apossibility that the irritability of myotonic muscle may be dueto a partial state of depolarization of the fibre membrane. Onthe other hand, in goats suffering from myotonia, Bryant(1962) has demonstrated that the resting membrane potentialis normal but that small induced depolarizations may initiatetrains of repetitive action potentials.Lenman (1963) has found that the resting membrane poten-
tial recorded from the muscle of dystrophic mice of the BarHarbor strain is consistently about 10-20% lower than innormal mice. These results have been confirmed byMcComas and Mossawy (1963) in my department; theyrecorded from 255 fibres in normal mice (mdan 83.0 mV) andfrom 225 in dystrophic mice (mean 76.0 mV) and there wasmuch greater variation between individual fibres in thedystrophic animals (Fig. B). The further application of thistechnique to the study of muscular dystrophy and of myotoniain both man and animals will be likely to yield information ofmuch value. In particular, it will be important to study thepropagation of the electrical impulse along the muscle-fibremembrane which is probably damaged by the dystrophic pro-cess. It should also be possible to study the inward spreadof excitation from the membrane to the myofibril, a processin which the sarcotubular system is undoubtedly of greatimportance. These studies are as yet in their infancy, but arelikely to contribute a great deal to our understanding of thebehaviour of the muscle cell in health and disease.
NORMAL. 255 fibresMe4n=8350. S.E.- '02SmV
I0
60 70 80 90
z 20 DYSTROPiIC, 225 fibresMeens760. S.E.-044mV
00
060 70 so 90
RESTING POTENTIAL (MV)FIG. B.-Comparison of the membrane potentials recordedwith intracellular micro-electrodes in normal adult mice(above) and adult dystrophic mice (below) of the Bar
Harbor strain (McComas and Mossawy, 1963).
Conclusions
I have been able to do little more than to sketch in outlinesome of the clinical features of the principal varieties of humanmuscular dystrophy and to mention only a few of the recentadvances in knowledge. Unquestionably some of these havebeen of great practical importance. Of particular value is theintroduction of the serum creatine kinase as a routine diag-nostic test for clinical and preclinical muscular dystrophy andin the identification of female carriers of the gene respon-sible for the most severe form of dystrophy-namely, theDuchenne variety which affects young boys. Of even greater
importance, however, are the fundamental research techniquesnow being utilized in the hope of elucidating the nature ofthe dystrophic process. Many theories have been adduced toexplain why the muscles waste, and there are still a greatmany unanswered questions. One of these, which may befundamental, is that we have as yet no explanation why thedisease process is so curiously selective, particularly in itsearly stages, affecting some muscles and sparing others. Thesuggestion has been made that those most liable to be affectedare the muscles firsi developed in embryonic life, but thissuggestion has not been substantiated.The recent attempt by Das Gupta (1963) to see whether
phasic and tonic motor units are present in man and whetherone of these is selectively involved in the dystrophic processhas been unsuccessful, and as yet little information is avail-able on how individual muscles vary in enzyme constitution.It may be that there is some specific biochemical reason,depending perhaps upon differential concentrations of enzymes,which explains the selective nature of the dystrophic process.Clearly, therefore, in attempting to increase our understand-ing of the disease we must compare not only the differentforms of muscular dystrophy but also different muscles, bothin normal individuals and in sufferers. Denny-Brown's (1951)suggestion that dystrophy might be due to an inability of themuscle cell to regenerate cannot be the whole story, sinceWalton and Adams (1956) and others have shown thatregenerative phenomena are commonly observed in dystrophicmuscle, even though such regeneration appears to be singu-larly ineffective, a finding whicn is confirmed to some extentby the results to date of tissue culture. It seems probablethat the dystrophic process will eventually prove to be due tothe absence of one or more enzymes within the muscle cell,but despite the clinical, pathological, and biochemical simi-larities between the various forms of muscular dystrophy it ispossible that the biochemical processes concerned in each ofthese may be different, and it is even possible that each of theclinical subtypes may not always be determined by the samegene at the same locus. Clearly, therefore, a multitude ofproblems have yet to be surmounted, but one can, I think,conclude that the climate of research which has developedwithin the last few years has modified, at least to some extent,the attitude of despair previously so prevalent. The increasingvolume of investigative work now being carried out in manyparts of the world must surely give hope that before manyyears have passed the cause or causes of this tragic diseasewill be identified, and that when that time comes there maybe some prospect of developing an effective treatment.
My colleagues and I are grateful to the Muscular DystrophyAssociation of America, Inc., the Muscular Dystrophy Associationof Canada, and to the Muscular Dystrophy Group of Great Britainfor financial support, and I am indebted to Miss R. Allan forsecretarial assistance.
REFERENCES
Adams, R. D., Denny-Brown, D., and Pearson, C. (1953). Diseases ofMuscle. Hoeber, New York.
Aebi, U., Richterich, R., Colombo, J. P., and Rossi, E. (1962). Enzymol.biol. clin. (Basel), 1, 61.
Banker, B. Q., Victor, M., and Adams, R. D. (1957). Brain, 80, 319.Barwick, D. D. (1963). In Research in Muscular Dystrophy, p. 10.
Pitman, London.- Newell, D. J., and Walton, J. N. (1963). Neurology (Minneap.), 13,
12.Osselton, J. W., and Walton, J. N. (1962). Presented to the E.E.G.
Society, November 1962.and Walton, J. N. (1963). Amer. 7. Med., 35, 646.
Batten, F. E. (1909). Quart. 7. Med., 3, 313.- and Gibb, H. P. (1909). Brain, 32, 187.
Becker, P. E. (1953). Dystrophia Musculorum Progressiva. Thieme,Stuttgart.(1957). Acta genet. (Basel), 7, 303.and Kiener, F. (1955). Z. Neurol., 193, 427.
on 5 February 2020 by guest. P
rotected by copyright.http://w
ww
.bmj.com
/B
r Med J: first published as 10.1136/bm
j.1.5394.1336-a on 23 May 1964. D
ownloaded from

1348 23 May 1964 Muscular Dystrophy-WaltonBourne, GC. H., and Golarz, M. N. (1959). Nature (Lond.), 183, 1741.Boyer, S. H., and Fainer, D. C. (1963). Amer. 7. AMed., 35, 622.Bryant, S. H. (1962). Fed. Proc., 21, 312.Buchtbal, F. (1962). Wid Neurol., 3, 16.Chung, C, S., and Morton, N. E. (1959). Amer. 7. hum. Genet., 11, 339.Creutzfeldt, 0. D., Abbott, B. C., Fowler, W. M., and Pearson, C. M.
(1963). Electroenceph. cdin. Neurophysiol., 15, 508.Das Gupta, A. (1963). In Research in Muscular Dystrophy, p. 256.
Pitman, London.Denny-Brown, D. (1951). 7. Neuropath. exp. Neurol., 10, 94.Dowben, R. M. (1963). New Engl. 7. Med., 268, 912.Dreyfus, J. C., Demos, J., Schapira, F., and Schapira, G. (1962). C.R.
Acad. Sci. (Paris), 254, 4384.and Schapira, F. (1958). Ann. N.Y. Acad. Sci., 75, 235.
and Demos, J. (1961). 2nd Int. Congr. Hum. Genet.,Rome, p. 80.
Dubowitz, V. (1960). Brain, 83, 432.(1963). 7. Neurol. Neurosurg. Psychiat., 26, 322.
- and Pearse, A. G. E. (1961). 7. Path. Bact., 81, 365.Duchenne, G. B. (1868). Arch. gin. Mid., 11, 5, 179, 305, 421, 552.Ebashi, S., Toyokura, Y., Momoi, H., and Sugita, H. (1959). 7. Biochem.
(Tokyo), 46, 103.Elmqvist, D., Johns, T. R., and Thesleff, S. (1960). 7. Physiol. (Lond.),
154, 602.Emery, A. E. H. (1963). Lancet, 1, 1126.Engel, W. K. (1962). Neurology (Minneap.), 12, 778.- Foster, J. B., Hughes, B. P., Huxley, H. E., and Mahler, R. (1961).
Brain, 84, 167.Erb, W. (1884). Dtsch. Arch. klin. Med., 34, 467.Evans, J. H., and Baker, R. W. R. (1957). Brain, 80, 557.Fuchs, E. (1890). Arch. Ophthal., 36, 234.Geiger, R. S., and Garvin, J. S. (1957). 7. Neuropath. exp. Neurol., 16,
532.Gilliatt, R. W. (1962). Brit. med. 7., 2, 1073.Gglarz, M. N., and Bourne, G. H. (1963). Muscular Dystrophy in Man
and Animals, Chap. 3. Karger, Basel.Gowers, W. R. (1902). Brit. med. 7., 2, 89.Gresham, G. A., and Cruickshank, J. G. (1960). 7. Neuropath. exp.
Neurol., 19, 342.Herrmann, H. (1961). Res. Publ. Ass. nerv. ment. Dis., 38, 697.Hughes, B. P. (1963). In Research in Muscular Dystrophy, p. 167.
Pitman, London.Hutchinson, J. (1879). Med.-Chir. Trans., 62, 307.Huxley, H. &B (1957). 7. biophys. biochem. Cytol., 3, 631.Jackson, C. E., and Carey, J. H. (1961). Pediatrics, 28, 77.Johns, R. J. (1958). Res. Publ. Ass. nerv. ment. Dis., 38, 704.- (1963). Amer. 7. Med., 35, 611.
Julian, L. M., and Asmundson, V. S. (1960). Anat. Rec., 136, 218.Keevil, T. (1953). Bull. Hist. Med., 27, 201.Kiloh, L. G., and Nevin, S. (1951). Brain, 74, 115.Kloepfer, H. W., and Talley, C. (1958). Ann. hum. Genet., 22, 138.Kugelberg, E., and Petersen, I. (1949). 7. Neurol. Neurosurg. Psychiat.,
12, 268.Lamy, M., and de Grouchy, J. (1954). 7. Ginit. hum., 3, 219.Landouzy, L., and Dejerine, J. (1884). C.R. Acad. Sci. (Paris), 98, 53.Lenman, 1. A. (1963). In Research in Muscular Dystrophy, p. 230.
Pitman, London.Levene, P. A., and Kriszteller, L. (1909). Amer. 7. Physiol., 24, 45.Leyden, E. (1876). Klinik der Ruchenmarks-Krankheiten, vol. 2, p. 531.
Hirschwald, Berlin.Lyon, M. F. (1961). Nature (Lond.), 190, 372.- (1962). Amer. 7. hum. Genet., 14, 135.McArdle, B. (1963). In Research in Muscular Dystrophy, p. 145.
Pitman, London.McComas, A. J., and Mossawy, S. J. (1963). Unpublished observations.Mair, W. G. P. (1963). In Research in Muscular Dystrophy, p. 112.
Pitman, London.Meryon, E. (1852). Med.-chir. Trans., 35, 72.Michelson, A. M., Russell, E. S., and Harman, P. J. (1955). Proc. Nat.
Acad. Sci. (Wash.), 41, 1079.Mbbius, P. J. (1879). Samml. klin. Vortr., 171, 1505.
Morton, N. E., and Chung, C. S. (1959). Amer. 7. hum. Genet., 11, 360.- - and Peters, H. A. (1963). Muscular Dystrophy in Man and
Animals, Chap. 8, edited by G. H. Bourne and M. N. Golarz.Karger, Basel.
Nirenberg, M. W. (1963). Sci. Amer., 208, 80.Oppenheim, H. (1900). Mschr. Psychiat. Neurol., 8, 232.Pearce, G. W. (1963). In Research in Muscular Dystrophy, p. 75. Pit-
man, London.- (1964). In Disorders of Voluntary Muscle, Chap. 9, edited by J. N.
Walton. Churchill, London.- Pearce, J. M. S., and Walton, J. N. (1964). In preparation.- and Walton, J. N. (1962). 7. Path. Bact., 83, 535.
Pearce, J. M. S., Pennington1 R. J., and Walton, J. N. (1964a). 7.Neurol. Neurosurg. Psychzat., 27, 1.
- (1964b). Ibid., 27, 96.(1964c). Ibid. In press.
Pearsel A. G. E. (1963). In Research in Muscular Dystrophy, p. 189.Pitman, London.
Pearson, C. M. (1957). New Engl. 7. Med., 256, 1069.(1962). Brain, 85, 109.(1963). Amer. 7. Med., 35, 632.
- Fowler, W. M., and Wright, S. W. (1963). Proc. Nat. Acad. Sci.(Wash.), 50, 24
Pennington, R. J. (1962). Proc. Ass. cdin. Biochem., 2, 17.Perkoff, G. T., Hill, R. L., and Tyler, F. H. (1962). 7. cdin. Invest., 41,
1391.Perlstein, M. A., Gibbs, F. A., Gibbs, E. L., and Stein, M.D. (1960).
7. Amer. med. Ass., 173, 1329.Philip, U., Walton, J. N., and Smith, C. A. B. (1956). Ann. hum. Genet.,31, 155.Price, H. M. (1963). Amer. 7. Med., 33, 589.Ross, K. F. A. (1964). Quart. 7. micr. Sci. In press.- and Schapira, G. (1962). Biochemistry of Hereditary Myopathies,
p. 146. Thomas, Springfield, Illinois.Shy, G. M., Engel, W. K., Somers, J. E., and Wanks, T. (1963). Brain,
86, 793.- and Magee, K. R. (1956). Brain, 79, 610.Sibley, J. A., and Lehninger, A. L. (1949). 7. biol. Chem., 117, 859.Steinert, H. (1909). Dtsch. Z. Nervenheilk., 37, 58.Stevenson, A. C. (1953). Ann. Eugen. (Lond.), 18, 50.Thomson, W. H. S., and Guest, K. E. (1963). 7. Neurol. Neurosurg.
Psychiat., 26, 111.- Leyburn, P., and Walton, J. N. (1960). Brit. med. 7., 2, 1276.Turner, J. W. A. (1940). Brain, 63, 163.
(1949). Ibid., 72, 25.and Lees, F. (1962). Ibid., 85, 733.
Tyler, F. H., and Wintrobe, M. M. (1950). Ann. intern. Med., 32, 72.Van Breemen, V. L. (1960). Amer. 7. Path., 37, 333.van den Bosch, J. (1963). In Research in Muscular Dystrophy, p. 23.
Pitman, London.Walton, J. N. (1952). 7. Neurol. Neurosurg. Psychiat., 15, 219.- (1955). Ann. hum. Genet., 20, 1.
(1956a). 7. Neurol. Neurosurg. Psychiat., 19, 106.(1956b). Lancet, 1, 1023.(1956c). Ann. hum. Genet., 21, 40.
- (1957). 7. Neurol. Neurosurg. Psychiat., 20, 144.(1961). Res. Publ. Ass. nerv. ment. Dis., 38, 378.(1963). In Muscular Dystrophy in Man and Animals, Chap. 7,
edited by G. H. Bourne and M. N. Golarz. Karger, Basel.(1964). In Disorders of Voluntary Muscle, Chap. 11, edited by
J. N. Walton. Churchill, London.- and Adams, R. D. (1956). 7. Path. Bact., 72, 273.-- (1958). Polymyositis. Livingstone, Edinburgh.and Natrrass, F. J. (1954). Brain, 77, 169.
Wayne, H. L., and Browne-Mayers, A. N. (1959). Dis. nerv. Syst., 20,288.
Welander, L. (1951). Acta med. scand., Suppl. No. 265, p. 1.- (1957). Acta Genet. (Basel), 7, 321.
Whorton, C. M., Hudgins, P. C., and Conners, J. J. (1961). New Engl,7. Med., 265, 1242.
Wieme, R. J., and Herpol, J. E. (1962). Nature (Lond.), 194, 287.
on 5 February 2020 by guest. P
rotected by copyright.http://w
ww
.bmj.com
/B
r Med J: first published as 10.1136/bm
j.1.5394.1336-a on 23 May 1964. D
ownloaded from