Issues in Pain Management: The Patient with Chronic Low Back Pain Robin Hamill-Ruth.
59
Issues in Pain Management: The Patient with Chronic Low Back Pain Robin Hamill-Ruth
-
Upload
ralph-miles -
Category
Documents
-
view
220 -
download
5
Transcript of Issues in Pain Management: The Patient with Chronic Low Back Pain Robin Hamill-Ruth.

Issues in Pain Management:
The Patient with
Chronic Low Back Pain
Robin Hamill-Ruth

Chronic Low Back Pain
• Demographics• Anatomy• Evaluation• Management Options
– Medical– Adjunctive therapies– Interventional
• Case Reports


Chronic LBP: Demographics
• 80% of Americans experience LBP at some point during their lifetime.
• Annual prevalence of LBP about 30%• Most common cause of disability under age 45• Accounts for 12.5% of all sick days (Frank, 1993)
• Second most common reason for visits to MD (Hart, 1995)
• 5th leading cause of hospital admission (Taylor, 1994)

Chronic LBP: Demographics
• Each year, 3-4% of population is temporarily disabled, 1% of working age population is permanently, totally disabled
• Annual cost to US in 1980 estimated at 85 million dollars/year
• Between 1971 and 1981, # disabled grew 14 times the rate of population growth
• Prevalence rising with increasing age up to 65 years after which it declines

Chronic LBP: The Good News?
• Recovery from LBP– 60-70% recover by 6 weeks– 80-90% improve by 12 weeks– Recovery after 12 weeks is “slow and uncertain”– Those with isolated LBP recover more quickly
than those with sciatica– non-work related back symptoms cause less lost
time from work than work related symptoms



Differential Dx of LBP and Sciatica• Sacroiliitis, SI dysfunction• Piriformis syndrome• Iliolumbar syndrome• Quadratus lumborum syndrome• Trochanteric bursitis• Ischiogluteal bursitis• Facet syndrome• Meralgia paresthetica• Fibromyositis/Fibromyalgia• GI, GU, Vascular, Intraabdominal

Assessment: History
• S = site
• C = character
• R = radiation
• O = onset• D = discriminating features
(time course, what aggravates, what relieves, etc)

Confounding Conditions
• Depression, grief
• Confusion, memory deficits
• Medical conditions– ASCVD, DM, Obesity, CRF, COPD, Sleep apnea
• Psycho-socio-economics• money• transportation• other responsibilities• litigation, disability worker’s comp issues
“Quantifying” Pain
• Assessment– VAS (verbal, visual)
• pain• sleep• mood• function
– Draw your pain– Self, significant other report– Pain scales, inventories




History 2
• Past medications including dose, response, why stopped
• Past interventions and therapies
• Current meds, allergies
• Past med history
• ROS
• Social, work history

Physical Exam
• General
• Spine visual, palpation, percussion
• Posture, gait, movement during change in position
• Neuro (sensation, strength, tone, reflexes)
• ROM, flexibility
• Provacative maneuvers (eg. SLR, distracted SLR, Patrick’s, facet loading)
• Abdomen, chest, vascular, adjacent joints

Waddell’s Signs: Nonorganic Pathology
1.Nonanatomic tenderness
2.Simulation test (axial loading)
3.Distraction sign (eg. SLR v. DSLR)
4.Regional sensory or motor disturbance (stocking distrib, diffuse motor weakness)
5.Overreaction
3+ positive => poor outcome to spine surgery

Radiologic Evaluation
• Plain Films
• MRI
• CT
• CT Myelogram
• Discogram
• Angio- and venograms

Goals of Therapy• Educate the patient
– differential diagnosis
– management options
– realistic goals, pacing
• Address sleep dysfunction
• Manage depression• Improve function physically, emotionally,
socially
• Decrease pain

Pharmacologic Options• Acetaminophen
– Beware of other sources, toxic doses, other hepatotoxic agents
• Anti-inflammatory Agents: Nonspecific – Piroxicam, Indocin, Ketorolac
– Naproxen
– Ibuprofen
– Diclofenac, Nabumetone
• Cox II specific agents– Rofecoxib, Celecoxib, Parecoxib, Etoricoxib,
Valdecoxib, etc
NSAIDs
• Advantages: – antiinflammatory, analgesic, limited
sedation, non-addicting, +cheap, available OTC
• Concerns: – available OTC in multiple preps, GI effects,
renal and hepatic toxicity, platelet effects, fluid retention

Adjuvant Medications: Steroids
• Steroids– Oral, injection, topical, iontophoresis– 3 doses of depo prep over 4-6 weeks, 4 mo. holiday– Concerns:
• Adrenal suppression• Effect on glucose (DM), sodium excretion
(HTN, CHF)• Osteoporosis• Altered wound healing, immunity

Adjuvant Medications
• Antidepressants– TCAs (elavil, doxepin, nortrip): v. low dose
• sleep, anti-neuropathic effect• ataxia, orthostasis, constipation
– Trazodone• low dose, primarily for sleep
– SSRIs (Paxil, Prozac)– SNRIs (Effexor)

Adjuvant Medications• Anticonvulsants
– Pro: Neuropathic pain: lancinating, burning– Con: Ataxia, sedation, confusion (esp elderly)
• Drugs– Carbamazepine (Tegretol)– Gabapentin (Neurontin)– Lamotrigine (Lamictal)– Topiramate (Topomax)– Trileptal, etc– Clonazepam

Medications: Tramadol
• Tramadol (Ultram)– opiate effects– serotonergic effects– Max dose: 400 mg/day
• Problems– Lowered seizure threshold– Increased risk of seizures with TCA > SSRI– ? non-addicting

Adjuvant Medications
• Muscle Relaxants– Muscle spasm (acute strain/sprain,
fibromyalgia)– Spasticity due to denervation (baclofen,
dantrolene)– Secondary effects:
– Sleep, anxiolysis– anti-neuropathic effect (baclofen)

Adjuvant Medications
• Topical agents– NSAID preparations– Capsaicin– Lidoderm– Cica-care type skin covers– Commercial OTC preps

Medications: Opiates
• Chronic Opiate Therapy– Trial of short-acting medication ??
• Darvocet• Hydrocodone (Vicodin, Lortab)• Oxycodone (Roxicodone, Percocet, Tylox)• Hydromorphone (Dilaudid)• Morphine (MSIR, Roxanol)• Hydromorphone (Dilaudid)

Medications: Opiates• Chronic Opiate Therapy
– Long-acting Agents• Methadone• Morphine SR (MS Contin, Kadian,
Oramorph SR)• Oxycondone SR (Oxycontin)• Fentanyl Patch (Duragesic)• Hydromorphone SR (Dilaudid SR in
future)
Adjuvant Therapies
• Education
• Weight loss
• Exercise, Yoga
• Heat, cold, elevation, rest
• Massage, TENS
• Physical Therapy – strengthening, mobility, aquatics, low impact
aerobics

Psychologic Therapy
• Counseling– Pain counseling– Grief, depression– Pacing strategies– Appropriate goal setting
• Self-regulation techniques
– Self-hypnosis– Relaxation training– Biofeedback

Interventional Techniques• Advantages:
– “One shot”
– Simple
– Low risk
• Disadvantages– Positioning, technical difficulties
– Cost
– Cumulative steroid doses
– Anticoagulation?

Interventional Techniques
• Trigger Point Injections• Joint Injections (steroid, hyaluronate)• Epidural Steroid Injections
– translaminar vs. transforaminal• Medial Branch Nerve Blocks, Denervation• Implantable Spinal Cord Stims, Intrathecal
Pumps• Intradiscal Electrothermal Therapy (IDET)• Vertebroplasty


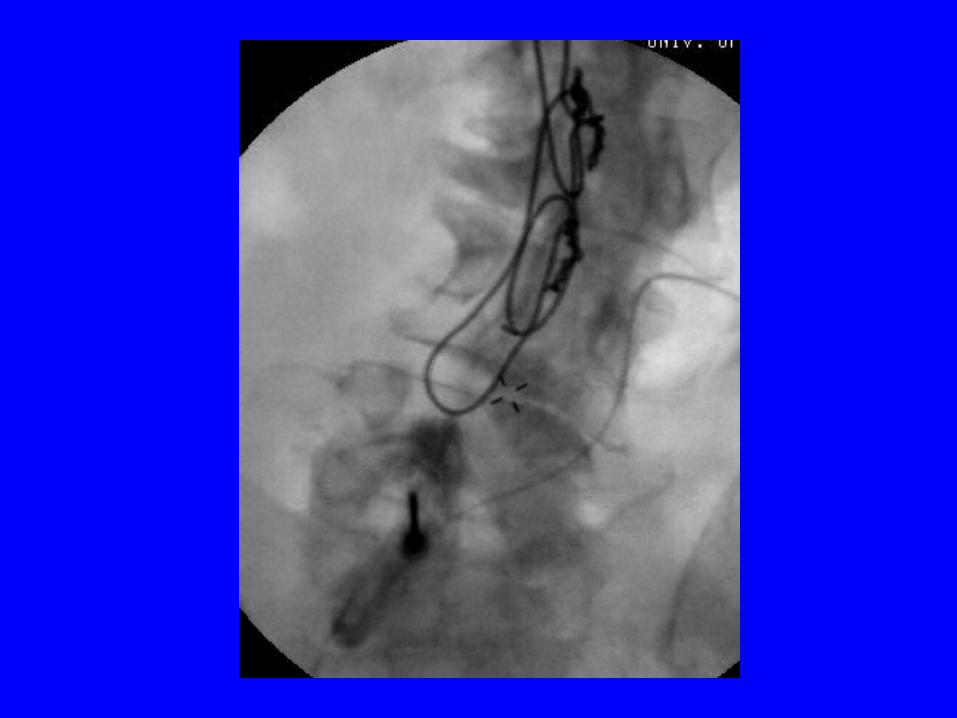
Sacroiliac Joint Injection
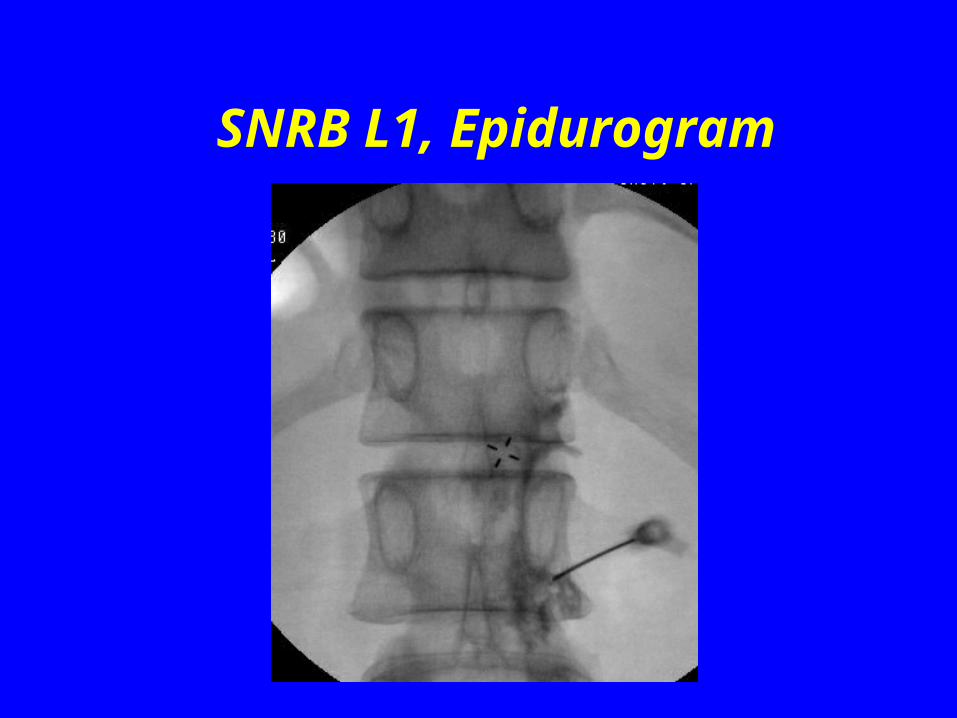
SNRB L1, Epidurogram
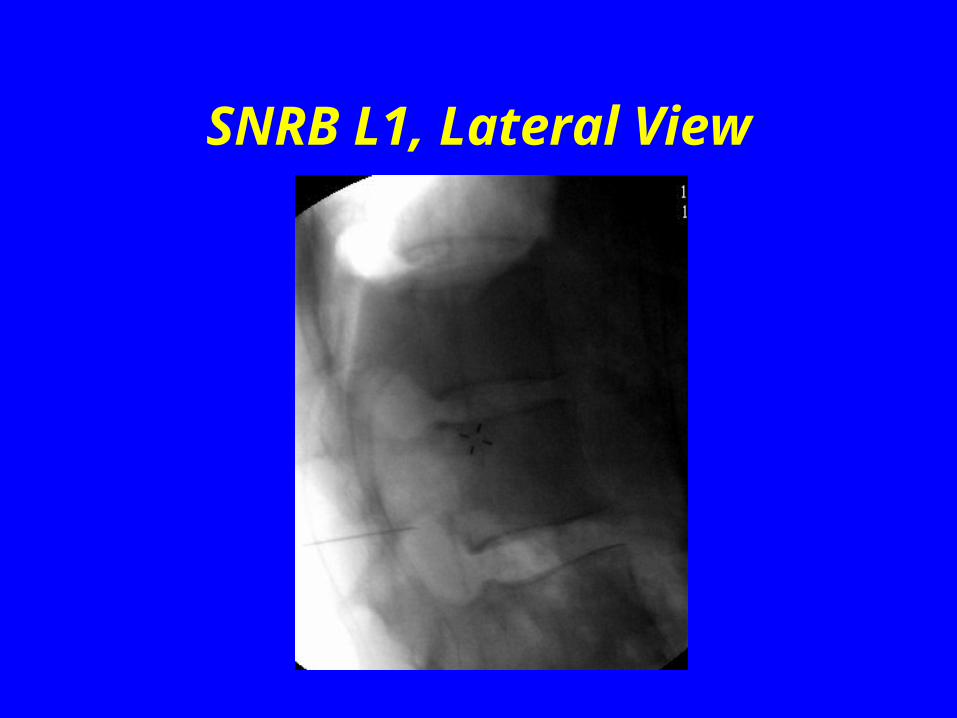
SNRB L1, Lateral View


Selective Nerve Root Block: AP View

SNRB: Lateral View

S1 Selective Transforaminal Block

Epidural Steroid Injection

Epidural Steroid Injection
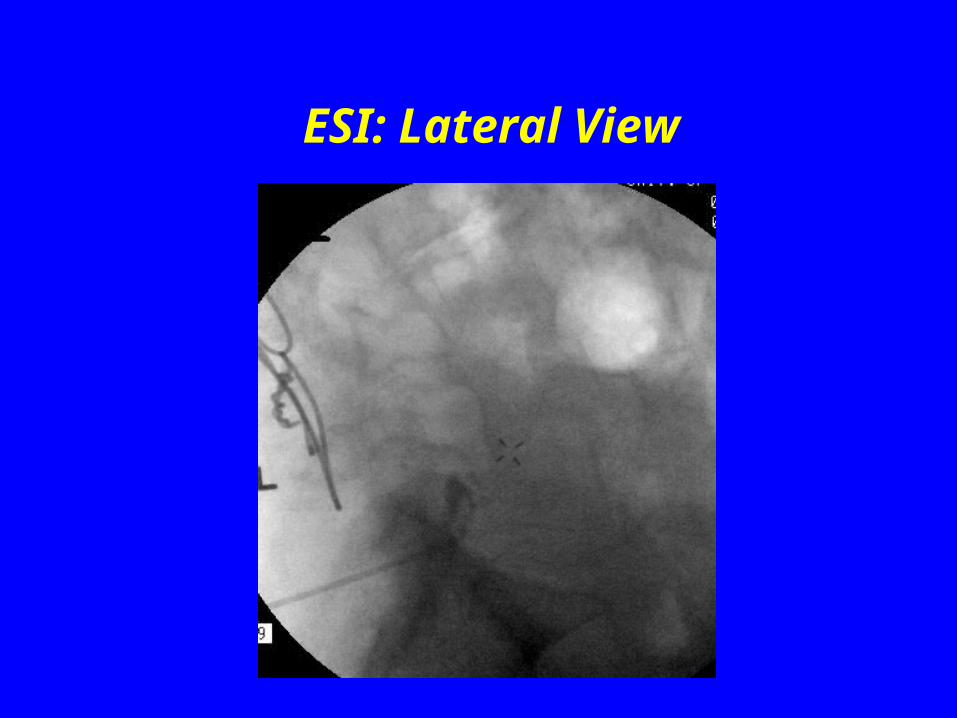
ESI: Lateral View

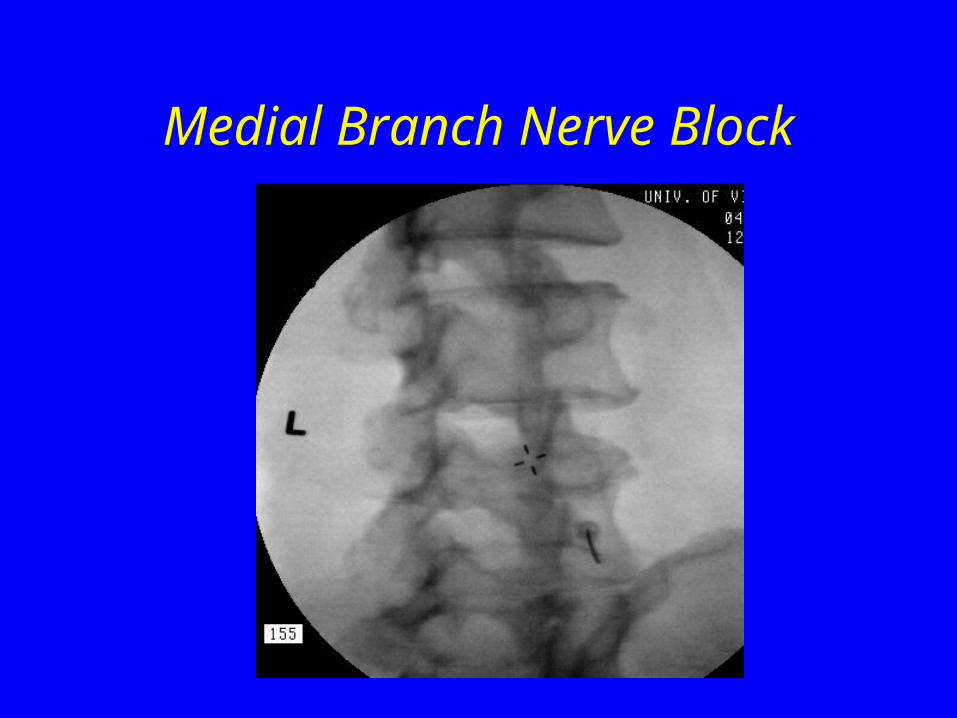
Medial Branch Nerve Block

Medial Branch Nerve Block
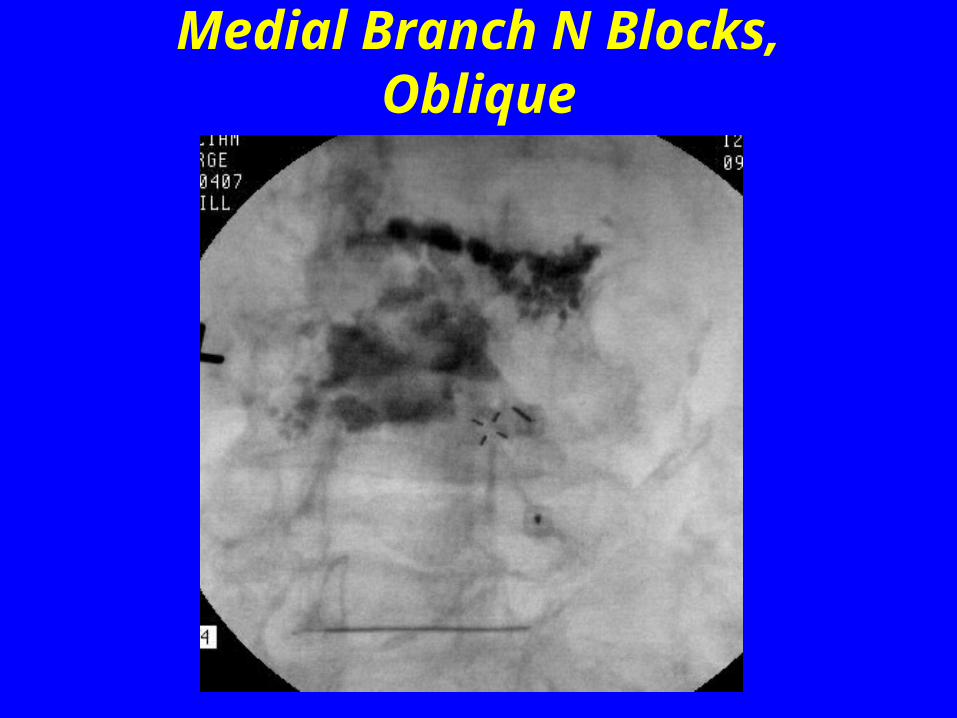
Medial Branch N Blocks, Oblique

Medial Branch N Block, AP

Implantable Therapies
• Spinal Cord Stimulator– Fairly focal pain, eg. Single extremity
radiculopathy, ischemia, neuropathic or sympathetically-maintained pain
• Intrathecal Pump– Refractory pain or intolerance to adequate
dosage of medications– longevity > 3-6 months– opiates, local anesthetic, baclofen, clonidine

When and Whom to Refer
• Possible procedural answer• NSAIDs, PT, low dose opiates,• Intolerance of multiple medications• Not responding to simple interventions• Significant psycho-social issues impeding function• Concerns with polypharmacy, possible abuse issues• You want another opinion, you’re uncomfortable • Patient wants another opinion
Osteoarthritis: Case Report• 82 yo female referred for implantation of intrathecal
pump for refractory LBP
• Xrays: severe DJD, stenosis
• Pt (and husband) reports worst time is sleeping. Inspite of PE, films, feels she functions just fine during the day.
– On Coumadin, Cox II agents -> inadequate relief.
– Percocet qhs only lasts 2 hours
– Recommendations: Methadone 5 mg. PO qhs with acetaminophen, PRN
• Result: Both she and her husband slept much better, both satisfied with regimen.

Arthritis: Case Report• 78 yo male with long hx steroid dependent RA,
with osteoporosis, compression fractures, degenerative disc disease and facet arthropathy.
• Presents with acute compression fracture T12, bilat. T 12 radiculopathy, secondary muscle spasm and marked LBP due to facet arthropathy.
• Effectively bedridden. History complicated by severe peripheral neuropathy, problems with ataxia and frequent falls. Also has PHN R flank, low abdomen.

Arthritis: Case Report, cont.
• Amitriptyline 10 qhs--good pain relief, sleep; increased falls
• Oxycodone--constipation, sedation• Methadone--good pain relief but severe
constipation, lethargy• Low dose gabapentin caused increased ataxia,
falls, confusion • Ultram was actually tolerated well with partial
relief.

Arthritis: Case Report, Interventions• Vertebroplasty of T12 gave some relief of back
pain, but patient fell several days later, which led to vertebroplasty at T11
• Bilateral T12 SNRBs done x2 with steroid for persistent radicular pain with some improvement
• Lumbar diagnositic facets gave good temporary relief so did radiofrequency ablation of medial branch nerves
• Trigger point injections in paraspinous muscles gave excellent relief

Arthritis: Case Report, Conclusion
• Lidoderm to flank/abdomen for PHN• Physical therapy improved mobility, endurance.
– Pt given walker for stability– Home exercise program, +/- compliance– TENS for myofascial component added
• Pain, sleep improved. Back at work. Falls improved with elimination of multiple medication.
• Effexor added recently for further mood modulation.• Recommended counseling re. Grief, loss of previous level
of function. Declined by patient.

Adjuvant Medications/Treatments
• Glucosamine/Chondroitin
• Hyaluronate preparations (Synvisc)
• Iontophoresis
• TENS
• Orthotic devices