
Isokinetic Muscle Strength in Long-Term IDDM Patients in - Diabetes
6
Isokinetic Muscle Strength in Long-Term IDDM Patients in Relation to Diabetic Complications Henning Andersen, Per L. Poulsen, Carl E. Mogensen, and Johannes Jakobsen The isokinetic muscle strength in 56 IDDM patients with >20 years of diabetes duration and in their individually sex-, age-, weight-, and height-matched control subjects was assessed. Peak torque of foot dorsal and plantar flexion and knee and wrist extension and flexion was measured. The neuropathic condition was assessed by a neurological disability score, a neuropathy symptom score, nerve conduction studies, and quantitative sensory examination. All results were summed to obtain a neu- ropathy rank-sum score for each patient. According to their renal albumin excretion, the patients were classi- fied to have normo-, micro-, or macroalbuminuria. In addition, according to their retinal status, patients were classified as having no, simple, or proliferative retinopa- thy. The IDDM patients had a 21% reduction of muscle strength of both ankle dorsal ( P < l x 10~ 4 ) and plantar flexors (P < 0.01), compared with control subjects. A 16% reduction of knee extensors (P < 0.005) and a 17% reduction of knee flexors (P < 0.01) was found. In contrast, muscle strength in wrist flexors and extensors was not significantly reduced (10 and 11%, respectively [NS]). In patients with the most severe weakness, muscle strength of the calf muscles was only 50% of the expected performance. Correlations were found between the neu- ropathy rank-sum score and the muscle strength of ankle dorsal (r = -0.66, P < 1 x 10~ 7 ) and plantar flexors (r = -0.51, P < 0.0005), knee extensors (r = -0.51, P < 0.0005) and flexors (r = -0.44, P < 0.005), and wrist flexors (r = —0.41, P < 0.005). No correlation was found for wrist extensors (r = 0). Neither were there any relationships between muscle strength at the ankle and knee and the degree of albuminuria or retinopathy. In conclusion, motor performance is substantially impaired in long-term EDDM patients, and the weakness is related to the presence of neuropathy but not to albuminuria or retinopathy per se. Diabetes 45:440-445, 1996 P olyneuropathy is a common complication of diabe- tes and may result in sensory, autonomic, and motor disturbances (1). The manifestations range from subclinical alterations in nerve function to disabling dysfunctions such as pain, foot ulcers, walking instability, and frequent injuries from falling (2,3). Sensory From the Department of Neurology (H.A., J.J.) and Second University Clinic of Internal Medicine (P.L.P., C.E.M.), Aarhus University Hospital, Aarhus, Denmark. Address correspondence and reprint requests to Dr. H. Andersen, Neurologisk afd. F, Aarhus Kommunehospital, Nerrebrogade 44, 8000 Aarhus C, Denmark. Received for publication 28 June 1995 and accepted in revised form 16 November 1995. CV, coefficient of variation; MMT, manual muscle testing; MNCV, motor nerve conduction velocity; NCV, nerve conduction velocity; NDS, neurological disability score; NSS, neuropathy symptom score; PT, peak torque; ROM, range of motion; SNCV, sensory nerve conduction velocity; VPT, vibratory perception threshold. and autonomic dysfunctions have been well studied and during recent years a battery of cutaneous perception thresh- old tests and autonomic function tests have been developed and validated to characterize and monitor the neuropathy (4-10). In contrast, very little is known about motor function in diabetic patients, which may be explained by the predom- inance of sensory symptoms and signs in diabetic neuropa- thy. However, a recent population-based epidemiological study of diabetic neuropathy indicated that clinically appar- ent muscle weakness is a severe disturbance in IDDM patients with more advanced neuropathy (11). Clinically apparent muscle weakness is most frequently a foot drop with the inability to walk on heels. Testing of this muscle function has been used to distinguish between mild and more severe neuropathy (12). Until now the muscular per- formance has been evaluated according to graded clinical scales or daily-day-function tests (1,11,13). Clearly, there is a need for a new quantitative approach to study muscular performance in diabetic patients. In previous studies, muscle weakness was evaluated with the neurological disability score (NDS), which reflects the clinical severity of the neuropathy including manual muscle testing (MMT) of the strength of all major muscle groups (13,14). The NDS allows muscle weakness to be quantitated with a score of 1 to 4 reflecting a 25, 50, 75, and 100% weakness of the evaluated muscle group. Nonetheless, it has previously been reported that MMT is unable to detect a 25% change in strength of knee extension and of plantar flexion (15). In contrast with sensory and autonomic disturbances, no validated quantitative method has been established for the quantification of motor disturbances. The aim of the present study was to evaluate muscular performance at the ankle with quantitative and standardized techniques to test the hypothesis that muscular weakness is a hitherto less recognized but important clinical manifesta- tion of diabetic neuropathy in long-term IDDM patients. To correlate the findings to the prevalence and degree of neuropathy, nephropathy, and angiopathy, the patients were studied by means of clinical, electrophysiological, and per- ception threshold tests and classified according to their albumin excretion and degree of retinopathy. RESEARCH DESIGN AND METHODS Patients and control subjects. All IDDM patients at the diabetes outpatient clinic aged <65 years and with a diabetes duration >20 years were invited to participate in the study. Fifty-eight patients, 19 women and 39 men, agreed to participate. Patients were not included if they had severe cardiac or lung disease, acute or chronic musculoskeletal dis- ease, acute metabolic dysregulation, any other neurological or endo- crine disease, symptomatic macroangiopathy, or any previous or present lower limb asymmetric proximal weakness. The patient histories were searched for other explanations of polyneuropathy, and in every case it ! 440 DIABETES, VOL. 45, APRIL 1996 Downloaded from http://diabetesjournals.org/diabetes/article-pdf/45/4/440/361900/45-4-440.pdf by guest on 19 January 2022
Transcript of Isokinetic Muscle Strength in Long-Term IDDM Patients in - Diabetes

Isokinetic Muscle Strength in Long-Term IDDMPatients in Relation to Diabetic ComplicationsHenning Andersen, Per L. Poulsen, Carl E. Mogensen, and Johannes Jakobsen
The isokinetic muscle strength in 56 IDDM patients with>20 years of diabetes duration and in their individuallysex-, age-, weight-, and height-matched control subjectswas assessed. Peak torque of foot dorsal and plantarflexion and knee and wrist extension and flexion wasmeasured. The neuropathic condition was assessed by aneurological disability score, a neuropathy symptomscore, nerve conduction studies, and quantitative sensoryexamination. All results were summed to obtain a neu-ropathy rank-sum score for each patient. According totheir renal albumin excretion, the patients were classi-fied to have normo-, micro-, or macroalbuminuria. Inaddition, according to their retinal status, patients wereclassified as having no, simple, or proliferative retinopa-thy. The IDDM patients had a 21% reduction of musclestrength of both ankle dorsal ( P < l x 10~4) and plantarflexors (P < 0.01), compared with control subjects. A16% reduction of knee extensors (P < 0.005) and a 17%reduction of knee flexors (P < 0.01) was found. Incontrast, muscle strength in wrist flexors and extensorswas not significantly reduced (10 and 11%, respectively[NS]). In patients with the most severe weakness, musclestrength of the calf muscles was only 50% of the expectedperformance. Correlations were found between the neu-ropathy rank-sum score and the muscle strength of ankledorsal (r = -0.66, P < 1 x 10~7) and plantar flexors (r =-0.51, P < 0.0005), knee extensors (r = -0.51, P <0.0005) and flexors (r = -0.44, P < 0.005), and wristflexors (r = —0.41, P < 0.005). No correlation was foundfor wrist extensors (r = 0). Neither were there anyrelationships between muscle strength at the ankle andknee and the degree of albuminuria or retinopathy. Inconclusion, motor performance is substantially impairedin long-term EDDM patients, and the weakness is relatedto the presence of neuropathy but not to albuminuria orretinopathy per se. Diabetes 45:440-445, 1996
Polyneuropathy is a common complication of diabe-tes and may result in sensory, autonomic, andmotor disturbances (1). The manifestations rangefrom subclinical alterations in nerve function to
disabling dysfunctions such as pain, foot ulcers, walkinginstability, and frequent injuries from falling (2,3). Sensory
From the Department of Neurology (H.A., J.J.) and Second University Clinic ofInternal Medicine (P.L.P., C.E.M.), Aarhus University Hospital, Aarhus, Denmark.
Address correspondence and reprint requests to Dr. H. Andersen, Neurologiskafd. F, Aarhus Kommunehospital, Nerrebrogade 44, 8000 Aarhus C, Denmark.
Received for publication 28 June 1995 and accepted in revised form 16November 1995.
CV, coefficient of variation; MMT, manual muscle testing; MNCV, motor nerveconduction velocity; NCV, nerve conduction velocity; NDS, neurological disabilityscore; NSS, neuropathy symptom score; PT, peak torque; ROM, range of motion;SNCV, sensory nerve conduction velocity; VPT, vibratory perception threshold.
and autonomic dysfunctions have been well studied andduring recent years a battery of cutaneous perception thresh-old tests and autonomic function tests have been developedand validated to characterize and monitor the neuropathy(4-10). In contrast, very little is known about motor functionin diabetic patients, which may be explained by the predom-inance of sensory symptoms and signs in diabetic neuropa-thy. However, a recent population-based epidemiologicalstudy of diabetic neuropathy indicated that clinically appar-ent muscle weakness is a severe disturbance in IDDMpatients with more advanced neuropathy (11). Clinicallyapparent muscle weakness is most frequently a foot dropwith the inability to walk on heels. Testing of this musclefunction has been used to distinguish between mild andmore severe neuropathy (12). Until now the muscular per-formance has been evaluated according to graded clinicalscales or daily-day-function tests (1,11,13). Clearly, there is aneed for a new quantitative approach to study muscularperformance in diabetic patients.
In previous studies, muscle weakness was evaluated withthe neurological disability score (NDS), which reflects theclinical severity of the neuropathy including manual muscletesting (MMT) of the strength of all major muscle groups(13,14). The NDS allows muscle weakness to be quantitatedwith a score of 1 to 4 reflecting a 25, 50, 75, and 100%weakness of the evaluated muscle group. Nonetheless, it haspreviously been reported that MMT is unable to detect a 25%change in strength of knee extension and of plantar flexion(15). In contrast with sensory and autonomic disturbances,no validated quantitative method has been established forthe quantification of motor disturbances.
The aim of the present study was to evaluate muscularperformance at the ankle with quantitative and standardizedtechniques to test the hypothesis that muscular weakness isa hitherto less recognized but important clinical manifesta-tion of diabetic neuropathy in long-term IDDM patients. Tocorrelate the findings to the prevalence and degree ofneuropathy, nephropathy, and angiopathy, the patients werestudied by means of clinical, electrophysiological, and per-ception threshold tests and classified according to theiralbumin excretion and degree of retinopathy.
RESEARCH DESIGN AND METHODSPatients and control subjects. All IDDM patients at the diabetesoutpatient clinic aged <65 years and with a diabetes duration >20 yearswere invited to participate in the study. Fifty-eight patients, 19 womenand 39 men, agreed to participate. Patients were not included if they hadsevere cardiac or lung disease, acute or chronic musculoskeletal dis-ease, acute metabolic dysregulation, any other neurological or endo-crine disease, symptomatic macroangiopathy, or any previous or presentlower limb asymmetric proximal weakness. The patient histories weresearched for other explanations of polyneuropathy, and in every case it
!
440 DIABETES, VOL. 45, APRIL 1996
Dow
nloaded from http://diabetesjournals.org/diabetes/article-pdf/45/4/440/361900/45-4-440.pdf by guest on 19 January 2022

H. ANDERSEN AND ASSOCIATES
was judged whether the findings were typical of diabetic neuropathy.Patients were classified according to their urinary albumin excretion:<20 jjLg/min (normoalbuminuria), between 20 and —200 jjug/min (incip-ient nephropathy), and >200 |xg/min (overt nephropathy). Furthermore,the retinal status of the patients was classified as no, simplex, orproliferative retinopathy by an ophthalmologist. For comparison of themotor performance with healthy subjects, 56 healthy age-, sex-, height-and weight-matched control subjects were recruited among hospitalemployees, blood donors, and friends and relatives. To calculate apredicted value for the muscle strength of the diabetic patients, addi-tionally 65 control subjects were tested. Based on an interview aboutweekly physical activities, the control subjects were chosen to have acomparable amount of physical exertion in the patient and the controlgroups. All patients and control subjects gave informed consent to thestudy, which was approved by the local ethics committee.Clinical evaluation. All patients were examined by a trained neurolo-gist (J.J.) and evaluated according to a neuropathy symptom score(NSS) (13) and a NDS (16). The NSS is the number of symptoms ofmotor, sensory, and autonomic disturbances. The NDS is a combinedscore obtained from the neurological examination of muscle weakness,activity of tendon reflexes, and assessment of sensation on the great toeand index finger. HbAlc, blood glucose, and serum creatinine weredetermined with standard laboratory methods. The urinary albuminexcretion was determined with a radioimmunoassay (17).Electrophysiological studies. Nerve conduction studies were per-formed with standard surface stimulation and recording techniquesusing an electromyograph (DANTEC Counterpoint, Skovlunde, Den-mark) with standard filter settings (18). Motor nerve conduction velocity(MNCV) was measured in the dominant forearm segment of the median(elbow to wrist) nerve and in the nondominant leg segment of theperoneal (below capitulum fibulae to ankle) nerve. Sensory nerveconduction velocity (SNCV) was measured in the nondominant suralnerve with orthodromic activation and with antidromic activation of thedominant median nerve (wrist to finger II and III). For MNCV, Z-scoreswere calculated from values of healthy volunteers obtained with similartechniques (18). For SNCV, normal values previously determined inage-matched normal control subjects were adopted.Vibratory perception threshold (VPT) studies. VPT was evaluatedat dominant index finger pulp and nondominant dorsum of the great toeusing forced choice techniques (CASE IV, WR Medical Electronics,Stillwater, MN). Before the examination, patients were given writteninstructions and a demonstration of the technique. The threshold wasdetermined with the 4, 2, and 1 stepping algorithm (9). The VPTs foreach patient were compared with a normative database, and thecorresponding percentiles for the dominant finger pulp and the non-dominant great toe were determined.
Isokinetic muscle testing. The maximal isokinetic muscle strength(peak torque [PT]) of the ankle dorsal and plantar flexion, kneeextension and flexion, and wrist extension and flexion was evaluatedwith an isokinetic dynamometer (Lido Active Multyoint II, Loredan,West Sacramento, CA). The dynamometer was calibrated in accordancewith recommendations from Loredan. The computer software packageLIDOACT 5.3D was used for data collection.
The nondominant leg and the dominant arm were tested. Handdominance was determined by the preferred hand for hammering, andleg dominance was determined by the preferred leg for kicking a ball.Before the tests, subjects received instructions about the proceduresand were asked to perform a warmup of at least five submaximalrepetitions with increasing strength to become familiarized with theinstrumentation. Before each test, a passive movement sequence pro-vided by the LIDOACT software was used to weigh the limb throughoutthe defined range of motion (ROM), and force measurements wereautomatically corrected for the limb weight. The subjects were in-structed to push and pull "as hard and fast as possible" through the fullavailable ROM at every trial. To secure standardized instructions(volume of command and degree of encouragement), the verbal instruc-tions of one of the examiners were tape recorded and used in allexaminations. Every test included eight reciprocal trials with maximaleffort. A 10-s rest period was interposed between every trial. Data wereaccepted if the coefficient of variation (CV) for torque values throughoutthe movement of the eight repetitions did not exceed 10%. This was doneto discard results obtained front subjects who did not show maximaleffort. If the CV was >10%, the person was retested once. If at thesecond test the CV was > 10%, data were discarded if no outlayer torquecurve could be identified.
At the ankle test, subjects were in a sitting position with 70° and 80°
flexion at the knee and hip joint, respectively, as measured with ahand-held goniometer. The anatomical axis, defined as a line perpendic-ular to a point just distal to the midpoint of the lateral malleolus, wasaligned with the axis of the dynamometer. The foot was placed on thefoot plate and secured by two straps placed over the dorsum of the foot.In addition, straps were placed around the pelvis and trunk and a thighcuff was placed just above the knee for further stabilization. The fullROM was 48° ranging 24° from the neutral position in both plantar anddorsal direction, and the velocity was 607s. This ROM was smaller thanthe mobility of the ankle joint in all but one diabetic patient. All testsstarted with dorsal flexion followed by plantar flexion.
At the knee test, subjects were in a sitting position, straps wereplaced around the pelvis and trunk, and a thigh bolster was positionedfirmly on the thigh to avoid dislocation of the anatomical axis of rotationduring the test. A line perpendicular to a point through the mostprominent part of the lateral femoral condyle was aligned with the axisof the dynamometer. The full ROM was 70° (from 80° to 10° flexion ofthe knee), and all tests started with extension followed by flexion. Thevelocity was 907s. At the wrist test, the subjects were positioned sittingwith the forearm pronated on an arm rest. The line perpendicular to thewrist 1.5 cm distal to the distal end of the ulna was aligned to the axisof the machine. The full ROM was 55° starting from a 20° extendedposition moving to a 35° of flexion followed by a reciprocal extension.The velocity was 907s.
One patient had symptoms and electrophysiological signs of a carpaltunnel syndrome, and the strength measurements of wrist flexion andextension were discarded. Three other patients were not tested at thewrist because of complaints of pain or previous surgical intervention inthe hand.Definitions, calculations, and statistical analysis. The minimalcriteria for diabetic neuropathy were adopted (8,11). Patients weredefined as having neuropathy if at least two of the following fourcategories were abnormal, one being an abnormality of nerve conduc-tion or sensory examination: i ) NSS > 1; 2) NDS & 2; 3) abnormalnerve conduction velocity (NCV) in at least two of four nerves; and 4)abnormal VPT at index finger and great toe (^98th percentile).
For each patient, a predicted strength value for all six muscle groupswas calculated by using a multiple regression analysis including thevariables age, height, and weight for each sex. Hereby the actual musclestrength of each patient could be expressed as a percentage of thepredicted strength. Finally, the muscle strength at the three joints wascalculated as the average of the relative strength of the extensors andflexors.
To quantify the degree of neuropathy, a neuropathy rank-sum scorewas calculated for each patient. The neuropathy rank-sum score was asummation of the rank scores from the NSS, NDS, VPTs, and NCVs.Thereby the patients were ranked according to the severity ofneuropathy based upon clinical, quantitative sensory, and electrophysi-ological examinations. To avoid the correlation of clinical and quantita-tive measures of motor dysfunction, scores due to symptoms or signs ofmuscular weakness were excluded from the total NSSs and NDSs. TheVPTs were ranked according to the sum of the two percentiles obtainedfrom the index finger and great toe. The NCVs were ranked for each ofthe four nerves investigated, and finally the mean sum score for the fourconduction studies was used for the total rank sum. The MNCVs wereranked according to the calculated Z-score. If no action potential couldbe obtained because of atrophy of the muscle, the highest rank-sumscore was given. For SNCVs a score of 0 was given if the NCV was withinnormal limits, and a score of 2 was given if either an SNCV was belownormal limits or no action potential could be obtained.
The primary study parameters were PT of dorsal and plantar flexionat the ankle and PT of the extension and flexion of the knee and wrist.To test the statistical significance of muscular strength differencesbetween diabetic patients and control subjects, an unpaired Student's ttest with a 1% Bonferroni corrected limit of significance was applied. Forall other tests, a 5% limit of significance was applied. The comparisionsamong the nonneuropathic, the asymptomatic, and the symptomaticneuropathic groups were performed with an unpaired Student's t test.To estimate the correlations between the muscle strength and theneuropathy rank-sum score as well as the various laboratory findings,Pearson product-moment correlation analysis was used. The influenceof neuropathy, nephropathy, and retinopathy on the strength wasevaluated with multiple regression analyses. Normoalbuminuria, incipi-ent nephropathy, and overt nephropathy were scored as 1, 2, and 3,respectively, and normal funduscopy, simplex, and proliferative retinop-athy as 1, 2, and 3, respectively.
DIABETES, VOL. 45, APRIL 1996 441
Dow
nloaded from http://diabetesjournals.org/diabetes/article-pdf/45/4/440/361900/45-4-440.pdf by guest on 19 January 2022

MUSCLE STRENGTH IN DIABETES
TABLE 1Clinical data for IDDM patients
Nonneuropathic patientsAsymptomatic neuropathic patientsSymptomatic neuropathic patients
n
131924
Sex (M/F)
7/611/820/4
Age (years)
44 (34-62)41 (31-61)49 (31-64)
Weight (kg)
66(51-120)75 (55-92)76(61-110)
Duration ofdiabetes(years)
28 (20-39)28 (20-47)29 (21-35)
Nephropathy(none, incipient, overt)
9,2,210, 2, 711, 6, 7
Retinopathy(none, simplex,proliferative)
4,8, 13,10, 61,10,13
Data are medians (range).
RESULTSThe diabetic patients were aged 46.1 ±9.1 years (average ±SD) with a body weight of 75.2 ± 13.1 kg and a height of 175± 7.8 cm. The median duration of diabetes was 29 years(range 20-47). Two patients were excluded after the testbecause of poor cooperation during the isokinetic muscletesting. The control subjects were aged 45.8 ± 10.4 yearswith a body weight of 75.0 ± 10.6 kg and a height of 175 ±8.6 cm. The amount of physical exercise per week was 0.7 ±1.2 h for the patients and 0.8 ± 1.6 h for the control subjects.Clinical and demographic details for the patients are pre-sented in Table 1. The laboratory findings for all diabeticpatients showed a median HbAlc of 9.0% (range 6.8-12.1).The serum creatinine level was 86 mmol/1 (range 61-153),and the blood glucose level was 8.3 mmol/1 (range 2.1-20.1).These data are shown in relation to the neuropathic status inTable 2. The NSS resulted in a median score of 0. Fourteenpatients had a NSS of 1, and 10 patients had 2 or moresymptoms. The majority of symptomatic patients com-plained of numbness or prickling of the feet. Only threepatients complained of muscle weakness. Nine male patientscomplained of loss of penile erection, among whom one hadloss of urinary control. The median NDS including MMT forall patients was 13 (range 0-46), while the 25th and 75thpercentiles of the NDS were 6 and 23, respectively. Thirteenpatients had scores for muscle weakness, and the total NDSfor these patients was 31 (range 13-46). The neuropathicpatients with a NDS <15 had predominantly absent tendonreflexes and decreased sensation for touch, prick, and vibra-tion at the great toe.
The electrophysiological examination of the median nervefor all diabetic patients showed a MNCV of 51.7 m/s (range41.0-60.2) with a Z-score at 1.44 (range -0.85-4.39). TheMNCV and the Z-score of the peroneal nerve were 39.6 m/s(range 23.0-49.4) and 2.19 (range -0.35-6.49), respectively.In eight patients, the MNCV of the peroneal nerve could notbe determined because of atrophy of the extensor digitorumbrevis muscle. SNCVs of the median and sural nerve were47.8 m/s (range 36.2-60.0) and 44.7 m/s (range 33.4-55.8),respectively. In 27 patients, no action potential could beobtained from the sural nerve, and in 11 patients, no actionpotential could be obtained from the median sensory nerve.Four patients refused nerve conduction studies. Abnormal
VPTs both at the great toe and at the index finger were foundin 24 patients. According to the minimal criteria for diabeticneuropathy, 13 patients were defined as nonneuropathic and43 patients were defined as neuropathic, among whom 24had symptomatic neuropathy.
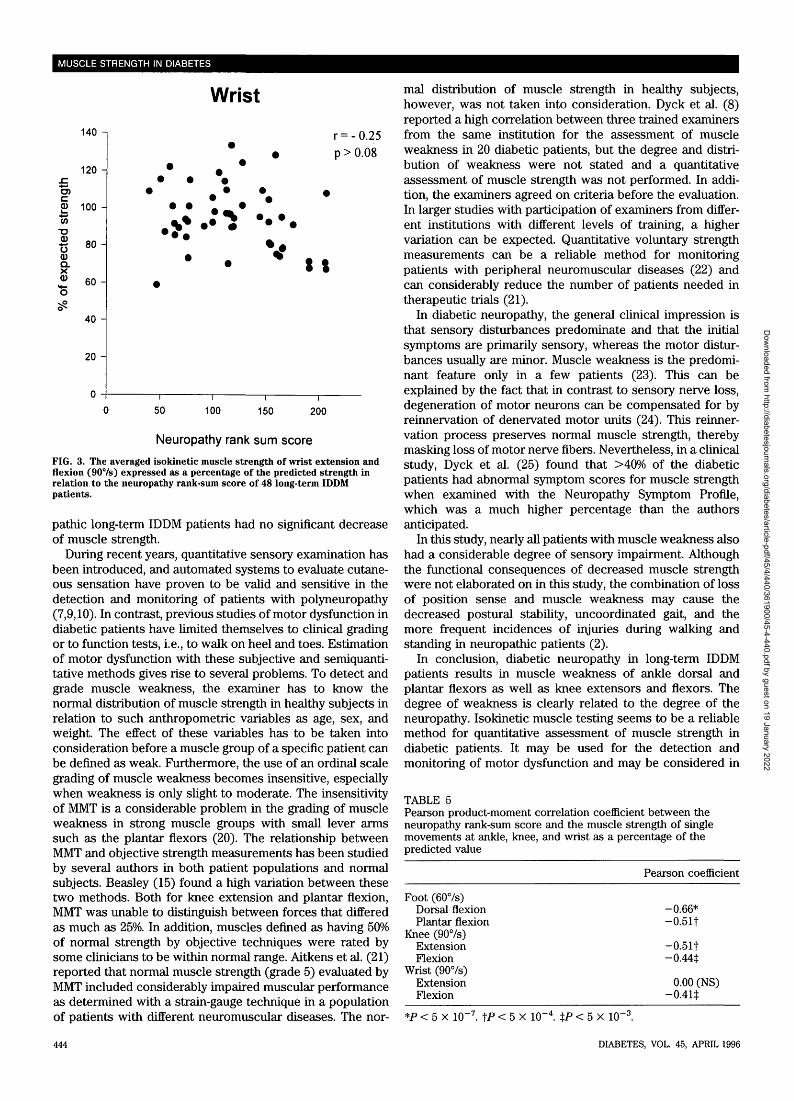
The isokinetic muscle strength for all patients was signif-icantly reduced for both calf and thigh muscles when com-pared with matched control subjects (Table 3). The musclestrength was lower for the neuropathic patients, especiallyfor the patients with symptomatic neuropathy (Table 4). Inthe nonneuropathic group, only 1 of 13 patients had <75% ofthe predicted isokinetic muscle strength at the ankle (P <0.005 vs. symptomatic and P < 0.05 vs. asymptomatic) andwrist (NS vs. the symptomatic and asymptomatic neuro-pathic groups). No patient had <75% of the expectedstrength at the knee (P < 0.005 vs. the symptomatic groupand P < 0.05 vs. the asymptomatic group). In the asymptom-atic neuropathic group, 5 of 19 patients had <75% of theexpected strength at the ankle (NS vs. the symptomaticgroup), 4 patients had <75% at the knee (NS vs. the symp-tomatic group), and no patients had <75% at the wrist (P <0.03 vs. the symptomatic group). In the symptomatic neuro-pathic group, 10 of 24 patients had <75% of the expectedstrength at the ankle, and an additional 2 patients had <50%of the expected strength. At the knee, 11 of 24 symptomaticpatients had <75% of the expected strength. The isokineticmuscle strength was lowest among patients with overtnephropathy and proliferative retinopathy. However, whenmultiple regression analyses were used to disentangle thethree intercorrelated variables neuropathy, retinopathy, andnephropathy, neither nephropathy nor retinopathy per seinfluenced the muscle strength at the ankle (retinopathy P >0.27; nephropathy P > 0.63) or knee (retinopathy P > 0.84;nephropathy P < 0.22). Furthermore, there were no relation-ships between muscle strength at the ankle and creatinine (r= -0.01), HbAlc (r = -0.13), or blood glucose (r = -0.03).A highly significant correlation between muscle strength andthe severity of neuropathy was found for both the ankle andknee (Figs. 1 and 2). In contrast, there was no significantcorrelation between the strength at the wrist and the neu-ropathy rank-sum score (Fig. 3). In addition, a significantcorrelation was found between ankle dorsal and plantarstrength (r = 0.49, P < 0.0002) and between knee extension
TABLE 2Laboratory findings for IDDM patients
Nonneuropathic patientsAsymptomatic neuropathic patientsSymptomatic neuropathic patients
n
131924
Serum creatinine ((xmol/1)
80 (66-96)91 (61-142)88 (70-153)
Blood glucose (mmol/1)
9.9(2.1-19.9)8.0(2.4-20.1)6.5 (3.0-20.0)
HbAlc (%)
8.5 (7.2-10.0)9.3 (6.8-12.1)9.3(6.9-11.1)
Data are medians (range).
442 DIABETES, VOL. 45, APRIL 1996
Dow
nloaded from http://diabetesjournals.org/diabetes/article-pdf/45/4/440/361900/45-4-440.pdf by guest on 19 January 2022

H. ANDERSEN AND ASSOCIATES
Ankle
stre
ngth
expe
cted
s%
of
120 -
100 -
80 -
60 -
40 -
20 -
0 -
• •
i i i i
•V *
*
r = -0.66
p < l * 1 0 - 7
i
i i i i
0 20 40 60 80 100 120 140 160 180 200 220 240
Neuropathy rank sum score
FIG. 1. The averaged isokinetic muscle strength of ankle dorsal andplantar flexion (607s) expressed as a percentage of the predictedstrength in relation to the neuropathy rank-sum score of 53 long-termIDDM patients.
and flexion (r = 0.70, P < IX 10 8). There was no correla-tion between wrist extension and flexion (r = 0.25, P > 0.07).Finally, there was a negative relationship between the isoki-netic muscle strength of all muscle groups except for wristextension and the neuropathy rank-sum score (Table 5).
DISCUSSIONIt is well known that mild distal muscle weakness canaccompany predominant distal symmetrical sensory neurop-athy in diabetic patients (1). There are numerous quantitativestudies on sensory and autonomic disturbances. In contrast,no quantitative and objective studies of muscle strength havepreviously been performed. Muscle weakness in diabetesmost frequently becomes apparent as a footdrop (11,12).Whether this reflects a primary involvement of the dorsalflexors of the foot has never been investigated. The present
TABLE 3Maximal isokinetic muscle strength (PT) at the ankle (607s), knee(907s), and wrist (907s) in diabetic patients and in controlsubjects
Movement
AnkleDorsalPlantar
KneeExtensionFlexion
WristExtensionFlexion
n
5353
5252
5051
Diabetic patients(Nm)
24.3 ± 6.8*87.8 ± 23.2t
150.8 ± 38.5*82.4 ± 20.2|
8.5 ± 2.4 (NS)15.1 ±3.6(NS)
Control subjects(Nm)
30.7 ± 7.5111.0 ± 28.7
178.6 ± 52.899.6 ± 31.0
9.5 ± 3.216.8 ± 5.4
TABLE 4Isokinetic muscle strength as a percentage of the expectedstrength in relation to neuropathy
Ankle Knee Wrist
All patientsNonneuropathic patientsAsymptomatic neuropathic
patientsSymptomatic neuropathic
patients
80 ± 16.8 84 ± 19.8 94 ± 17.192 ± 16.6 99 ± 15.8 99 ± 17.0
81 ± 13.6 85 ± 13.6 100 ± 14.0
73 ± 17.0 77 ± 23.2 ± 16.7
Data are means ± SD. The ankle strength is the average strength ofdorsal and plantar flexion, and the knee and wrist strength are theaverages of the strength of flexion and extension.
study was primarily designed to quantify the strength ofankle dorsal and plantar flexors because of the clinicalimpression in earlier studies. More proximal thigh and un-derarm muscle groups were also studied to describe thedistribution of the muscular involvement.
The main findings of this study are that muscle weaknessis substantial in long-term IDDM patients with neuropathy,and muscle weakness of ankle dorsal and plantar flexors,knee extensors and flexors, and wrist flexors was signifi-cantly related to the degree of neuropathy. Second, theplantar flexors were involved to the same degree as thedorsal flexors. This is in contrast with the general clinicalimpression, which is probably due to the fact that weaknessof the dorsal flexors is easier to detect clinically (20). Third,the distribution of muscle weakness is not limited to theankle but includes knee extensors and flexors almost to thesame degree as the ankle dorsi and plantar flexors. This is asurprising observation because motor involvement of themore proximal leg muscles was not anticipated except inpatients with very severe neuropathy (1). Finally, nonneuro-
Knee
140 -i
120 -
O)
"S 80
CDQ.
3 60 -
40 -
20 -
r = -0.51
p< 0,0002
50 100 150 200
Data are means ± SD. *P < 1 X 10~4. tP < 0.01.
Neuropathy rank sum score
FIG. 2. The averaged isokinetic muscle strength of knee extension andflexion (907s) expressed as a percentage of the predicted strength inrelation to the neuropathy rank-sum score of 51 long-term IDDMpatients.
DIABETES, VOL. 45, APRIL 1996 443
Dow
nloaded from http://diabetesjournals.org/diabetes/article-pdf/45/4/440/361900/45-4-440.pdf by guest on 19 January 2022
MUSCLE STRENGTH IN DIABETES
Wrist
140 -i
120 -
60 H
40 -
20 -
r = -0.25
p > 0.08
0) 100 -
dsti
% 8 0 -
d)Q .X
*
• 11
50 100 150 200
Neuropathy rank sum score
FIG. 3. The averaged isokinetic muscle strength of wrist extension andflexion (907s) expressed as a percentage of the predicted strength inrelation to the neuropathy rank-sum score of 48 long-term IDDMpatients.
pathic long-term IDDM patients had no significant decreaseof muscle strength.
During recent years, quantitative sensory examination hasbeen introduced, and automated systems to evaluate cutane-ous sensation have proven to be valid and sensitive in thedetection and monitoring of patients with polyneuropathy(7,9,10). In contrast, previous studies of motor dysfunction indiabetic patients have touted themselves to clinical gradingor to function tests, i.e., to walk on heel and toes. Estimationof motor dysfunction with these subjective and semiquanti-tative methods gives rise to several problems. To detect andgrade muscle weakness, the examiner has to know thenormal distribution of muscle strength in healthy subjects inrelation to such anthropometric variables as age, sex, andweight. The effect of these variables has to be taken intoconsideration before a muscle group of a specific patient canbe defined as weak. Furthermore, the use of an ordinal scalegrading of muscle weakness becomes insensitive, especiallywhen weakness is only slight to moderate. The insensitivityof MMT is a considerable problem in the grading of muscleweakness in strong muscle groups with small lever armssuch as the plantar flexors (20). The relationship betweenMMT and objective strength measurements has been studiedby several authors in both patient populations and normalsubjects. Beasley (15) found a high variation between thesetwo methods. Both for knee extension and plantar flexion,MMT was unable to distinguish between forces that differedas much as 25%. In addition, muscles defined as having 50%of normal strength by objective techniques were rated bysome clinicians to be within normal range. Aitkens et al. (21)reported that normal muscle strength (grade 5) evaluated byMMT included considerably impaired muscular performanceas determined with a strain-gauge technique in a populationof patients with different neuromuscular diseases. The nor-
mal distribution of muscle strength in healthy subjects,however, was not taken into consideration. Dyck et al. (8)reported a high correlation between three trained examinersfrom the same institution for the assessment of muscleweakness in 20 diabetic patients, but the degree and distri-bution of weakness were not stated and a quantitativeassessment of muscle strength was not performed. In addi-tion, the examiners agreed on criteria before the evaluation.In larger studies with participation of examiners from differ-ent institutions with different levels of training, a highervariation can be expected. Quantitative voluntary strengthmeasurements can be a reliable method for monitoringpatients with peripheral neuromuscular diseases (22) andcan considerably reduce the number of patients needed intherapeutic trials (21).
In diabetic neuropathy, the general clinical impression isthat sensory disturbances predominate and that the initialsymptoms are primarily sensory, whereas the motor distur-bances usually are minor. Muscle weakness is the predomi-nant feature only in a few patients (23). This can beexplained by the fact that in contrast to sensory nerve loss,degeneration of motor neurons can be compensated for byreinnervation of denervated motor units (24). This reinner-vation process preserves normal muscle strength, therebymasking loss of motor nerve fibers. Nevertheless, in a clinicalstudy, Dyck et al. (25) found that >40% of the diabeticpatients had abnormal symptom scores for muscle strengthwhen examined with the Neuropathy Symptom Profile,which was a much higher percentage than the authorsanticipated.
In this study, nearly all patients with muscle weakness alsohad a considerable degree of sensory impairment. Althoughthe functional consequences of decreased muscle strengthwere not elaborated on in this study, the combination of lossof position sense and muscle weakness may cause thedecreased postural stability, uncoordinated gait, and themore frequent incidences of injuries during walking andstanding in neuropathic patients (2).
In conclusion, diabetic neuropathy in long-term IDDMpatients results in muscle weakness of ankle dorsal andplantar flexors as well as knee extensors and flexors. Thedegree of weakness is clearly related to the degree of theneuropathy. Isokinetic muscle testing seems to be a reliablemethod for quantitative assessment of muscle strength indiabetic patients. It may be used for the detection andmonitoring of motor dysfunction and may be considered in
TABLE 5Pearson product-moment correlation coefficient between theneuropathy rank-sum score and the muscle strength of singlemovements at ankle, knee, and wrist as a percentage of thepredicted value
Foot (607s)Dorsal flexionPlantar flexion
Knee (907s)ExtensionFlexion
Wrist (907s)ExtensionFlexion
Pearson coefficient
-0.66*-0.51t
-0.51t-0.44$
0.00 (NS)-0.4U
*P < 5 X 10 5 X 10"4. %P < 5 x 10"
444 DIABETES, VOL. 45, APRIL 1996
Dow
nloaded from http://diabetesjournals.org/diabetes/article-pdf/45/4/440/361900/45-4-440.pdf by guest on 19 January 2022

H. ANDERSEN AND ASSOCIATES
treatment trials and prevention studies in diabetic neuropa-thy in long-term IDDM patients.
ACKNOWLEDGMENTSThis work was supported by the Karen Elise Jensen Foun-dation, the Novo Nordisk Foundation, and the Danish Dia-betes Association.
Professor M. Vaeth is acknowledged for valuable sugges-tions for the statistical analyses. B. Holmboe, P. Kousgaard,B. Lousdal, T. Beikes, and M. M0rkholt are acknowledged fortheir excellent technical assistance.
REFERENCES1. Thomas PK, Tomlinson DR: Diabetic and hypoglycemic neuropathy. In
Peripheral Neuropathy. Dyck PJ, Thomas PK, Griffin JW, Low PA,Poduslo JF, Eds. Philadelphia, Saunders, 1993, p. 1219
2. Cavanagh PR, Derr JA, Ulbrecht JS, Maser RE, Orchard TJ: Problemswith gait and posture in neuropathic patients with insulin-dependentdiabetes mellitus. Diabetic Med 9:469-474, 1992
3. Cavanagh PR, Young MJ, Adams JE, Vickers KL, Boulton AJ: Radio-graphic abnormalities in the feet of patients with diabetic neuropathy.Diabetes Care 17:201-209, 1994
4. Fisher BM, Frier BM: Usefulness of cardiovascular tests of autonomicfunction in asymptomatic diabetic patients. Diabetes Res Clin Pract6:157-160, 1989
5. Yamasaki Y, Ueda N, Kishimoto M, Tani A, Ishida Y, Kawamori R,Kamada T: Assessment of early stage autonomic nerve dysfunction indiabetic subjects-application of power spectral analysis of heart ratevariability. Diabetes Res 17:73-80, 1991
6. Maselli RA, Jaspan JB, Soliven BC, Green AJ, Spire JP, Arnason BG:Comparison of sympathetic skin response with quantitative sudomotoraxon reflex test in diabetic neuropathy. Muscle Nerve 12:420-423, 1989
7. Dyck PJ, Bushek W, Spring EM, Karnes JL, Litchy WJ, O'Brien PC,Service FJ: Vibratory and cooling detection thresholds compared withother tests in diagnosing and staging diabetic neuropathy. Diabetes Care10:432-440, 1987
8. Dyck PJ, Kratz KM, Lehman KA, Karnes JL, Melton LJ III, O'Brien PC,Litchy WJ, Windebank AJ, Smith BE, Low PA, Service FJ, Rizza RA,Zimmerman BR: The Rochester Diabetic Neuropathy Study: design,criteria for types of neuropathy, selection bias, and reproducibility ofneuropathic tests. Neurology 41:799-807, 1991
9. Dyck PJ, O'Brien PC, Kosanke JL, Gillen DA, Karnes JL: A 4, 2, and 1stepping algorithm for quick and accurate estimation of cutaneoussensation threshold. Neurology 43:1508-1512, 1993
10. Dyck PJ, Zimmerman IR, O'Brien PC, Ness A, Caskey PE, Karnes J,Bushek W: Introduction of automated systems to evaluate touch-pres-sure, vibration, and thermal cutaneous sensation in man. Ann Neuivl4:502-510, 1978
11. Dyck PJ, Kratz KM, Karnes JL, Litchy WJ, Klein R, Pach JM, Wilson DM,O'Brien PC, Melton LJ: The prevalence by staged severity of various typesof diabetic neuropathy, retinopathy, and nephropathy in a population-based cohort: the Rochester Diabetic Neuropathy Study. Neuivlogy43:817-824, 1993
12. Dyck PJ, Karnes JL, O'Brien PC, Litchy WJ, Low PA, Melton LJ III: TheRochester Diabetic Neuropathy Study: reassessment of tests and criteriafor diagnosis and staged severity. Neurology 42:1164-1170, 1992
13. Dyck PJ, Sherman WR, Hallcher LM, Service FJ, O'Brien PC, Grina LA,Palumbo PJ, Swanson CJ: Human diabetic endoneurial sorbitol, fructose,and myo-inositol related to sural nerve morphometry. Ann Neuivl8:590-596, 1980
14. Keen H, Payan J, Allawi J, Walker J, Jamal GA, Weir AI, Henderson LM,Bissessar EA, Watkins PJ, Sampson M, Gale EAM, Scarpello J, BoddieHG, Hardy KJ, Thomas PK, Misra P, Halonen JP: Treatment of diabeticneuropathy with T-linolenic acid: the T-Linolenic Acid Multicenter TrialGroup. Diabetes Care 16:8-15, 1993
15. Beasley WC: Quantitative muscle testing: principles and applications toresearch and clinical services. Arch Phys Med Rehabil 42:398- 425, 1961
16. Dyck PJ: Quantitating severity of neuropathy. In Peripheral Neuivpathy.Dyck PJ, Thomas PK, Griffin JW, Low PA, Poduslo JF, Eds. Philadelphia,Saunders, 1993, p. 686
17. Miles DW, Mogensen CE, Gundersen HJG: Radioimmunoassay for uri-nary albumin using a single antibody. Scand J Clin Lab Invest 26:5-11,1970
18. Stalberg E, Falck B: Clinical motor nerve conduction studies. MethodsClin Neurophysiol 4:61-80, 1993
20. Bourque PR, Dyck PJ: Selective calf weakness suggests intraspinalpathology, not peripheral neuropathy. Arch Neurol 47:79-80, 1990
21. Aitkens S, Lord J, Bernauer E, Fowler WM Jr, Lieberman JS, Berck P:Relationship of manual muscle testing to objective strength measure-ments. Muscle Nerve 12:173-177, 1989
22. Wiles CM, Kami Y: The measurement of muscle strength in patients withperipheral neuromuscular disorders. J Neurol Neuwsurg Psychiatry46:1006-1013, 1983
23. Said G, Goulon Goeau C, Slama G, Tchobroutsky G: Severe early-onsetpolyneuropathy in insulin-dependent diabetes mellitus: a clinical andpathological study [see comments]. N EnglJ Med 326:1257-1263, 1992
24. Saito T, Sato T, Miura Y: Postural hypotension and plasma cat-echolamines in diabetics. In Diabetic Neuivpathy. Goto Y, Horiuchi A,Kogure K, Eds. Amsterdam, Excerpta Medica, 1982, p. 247
25. Dyck PJ, Karnes J, O'Brien PC, Swanson CJ: Neuropathy SymptomProfile in health, motor neuron disease, diabetic neuropathy, and amy-loidosis. Neurology 36:1300-1308, 1986
DIABETES, VOL. 45, APRIL 1996 445
Dow
nloaded from http://diabetesjournals.org/diabetes/article-pdf/45/4/440/361900/45-4-440.pdf by guest on 19 January 2022


















