Is it MG Crisis? Dr Chan Yan Fat Alfred Caritas Medical Center 20/01/2009.
77
Is it MG Crisis? Dr Chan Yan Fat Alfred Caritas Medical Center 20/01/2009
-
Upload
ayla-pretty -
Category
Documents
-
view
216 -
download
2
Transcript of Is it MG Crisis? Dr Chan Yan Fat Alfred Caritas Medical Center 20/01/2009.

Is it MG Crisis?
Dr Chan Yan Fat Alfred
Caritas Medical Center
20/01/2009

Background history
• 82-year-old woman, ex-smoker
• Mother of 6 children
• Resident in Canada and being FU at there
• Post-radioactive-iodine hypothyroidism
• Asthma with nil attack for years
• Essential hypertension
• Ocular myasthenia gravis (MG) since 2002

Long term medication
• L-thyroxine 75 microgram daily
• Candesartan 8mg daily
• Ventolin 2 puffs Qid PRN
• Becotide 2 puffs BD
• Pyridostigmine (Mestinon) 60mg BD

History of present illness
• Visit Hong Kong since one week ago• Upper respiratory infection since arrival• Fever and sputum for 3 days, and put on oral Levo
floxacin 100mg BD + Romilar• Subjective double vision for one day, with bilatera
l upper limb weakness + numbness, but still able to walk
• While at Precious blood Hospital, developed choking and SOB

To CMC AED 9/3/08 at 1900
• BP 202/89, pulse 72, SaO2 88% room air
• GCS 15/15, Fever 38.0 degree
• Speak full sentence, SaO2 96% at 2L O2
• “muscle weakness” at 4/5
• Chest clear; PFR 170 170 150
• Impression: mild MG
• Decision: consult ICU


Direct ICU admission
• Failed bedside swallowing test
• Impaired abduction of eyes at both side
• No facial weakness or fatigability
• Power: bilateral upper limb 4-/5
bilateral LL 4/5 proximal; 5/5 distal
• Bilateral down-going plantar
• Normal deep tendon reflex

Differential diagnosis
• Generalized myasthenia gravis (MG) with ocular and bulbar involvement
• Thyroid ophthalmopathy + myopathy
• Brainstem pathology
• Motor cranial nerve pathology
• Pharyngeal-cervical-brachial variant of Gullain-Barre Syndrome

Impression at ICU
Generalized MG with bulbar involvement
Precipitated by……

Famous MG precipitating causes
• Antibiotics: aminoglycosides; macrolides; fluoroquinolone; tetracyclines
• Anesthetic: lidocaine; procaine; NMB• Cardiac: betablocker; CCB; procainamide• Steroids• Anticonvulsant: phenytoin; gabapentin• Others: Opiods; thyroxine; diuretics; anti-ch
olinergics; iodinated contrasts; URI

Management by on-call MO
• Keep NPO for possible intubation later
• Increase Mestinon 60mg tds
• Insert RT for medication
• Check CBP/RFT/LFT/INR/ABG/ESR
• Blood, sputum and urine for culture
• Serum viral titre
• Urgent plain CT brain

Blood test
• WCC 15.4 (Neutrophil 85.4%)
• Hemoglobin 13.5 with MCV 89.9
• ESR 87
• CK 145; albumin 37, globulin 42
• RFT and LFT normal
• TSH 1.79 (0.50-4.70)
• pH 7.41, CO2 42.6, O2 176, HCO3 26


Progress on 10/3/08 at ICU D2
• Subjective deterioration and require frequent suction of oral secretion/ sputum
• Examination in AM around:Hoarseness and weak coughDrooling of salivaPoor AE over both chest
• Impression: MG crisis

Bronchoscopy
• Very poor cough effort
• Continuous aspiration of saliva and upper airway secretion into lower tract
• BAL done at right lower lobe for virus study and bacterial culture

Management at ICU day 2
• Endotracheal intubation
• Start IV Augmentin for chest infection
• Start iv Intragram (IVIG) 21g (BW 53kg), plan daily dose for 5 days
• Trace old record from Canada family doctor about the diagnosis and previous workup of myasthenia gravis

Progress at ICU day 4
• All ocular movement is full, no ptosis• Hand-grip 3/5; right wrist flexion 2/5; rest o
f upper limb power 0/5 !• Both thigh 3/5, both ankle 4/5• Absent deep tendon reflex of lower limb, m
arkedly decreased at upper limb• Paraesthesia over 4 limb, nil sensory level• BP 100/55, fever down

Atypical presentation of MG!
Deterioration with iv Ig
Other pathology?

Can it be due to MG crisis
Pros• Symmetrical proximal
muscle weakness
• Previous ocular MG
• Bulbar symptom
• Precipitating factors of crisis seen
Cons• Different symptom a
nd sign from past
• Severity of physical sign not fluctuating
• Global areflexia
• Sensory symptoms

Management at ICU day 4
• Stop Intragram
• Off Mestinon plan to have more MG workup first e.g. electrophysiology
• Urgent MRI cervical spine to upper thoracic spine to look for cord lesion
• Trace again past medical record from Canada doctor by relative



Urgent MRI report
• Serpentine intradural extramedullary flow-related signals and flow voids are demonstrated from C5 to T9 level, but no definite intramedullary involvement.
• No hemorrhage or abnormal signal in cord• No mass effect on cervical/ thoracic cord• Impression: spinal vascular malformation, li
kely spinal dural AV fistula

Can it be spinal cord insult?!
Pros• Tetraparesis
• Areflexia
• Hypotension
• Normal cognitive function all along
• MRI showed vascular lesion around cord
Cons• Proximal affected pref
erentially
• No sensory level
• Bulbar symptoms
• Ophthalmoplegia, though improved
• Normal cord signal

Progress at ICU day 5
• Orthopedics intramedullary lesion better be managed by neurosurgery
• Neurosurgery no evidence of acute element for intervention, suggest to transfer patient when nil airway problem
• ICU noted good respiratory effort with spontaneous tidal volume >400ml. Failed extubation because of aspiration problem

Progress at ICU day 6 (1)
Medical summary from Canada• Patient presents as ptosis and diplopia in Ju
ne 2002. Nil peripheral/ bulbar or respiratory involvement
• Nil Tensilon test, nil anti-acetylcholine receptor antibody checked
• Prompt effect with Mestinon• CT thorax showed no thymoma

Progress at ICU day 6 (2)
• Proximal muscle power 2/5, distal 4/5
• Double-blinded Tensilon test
no significant change in limb power
• Bedside EMG: no typical decrement of amplitude with repetitive stimulation
• Acetylcholine receptor binding antibody
10.57 (<0.45, ELIZA method)

Every sign must have
explanation

Neurologist (ICU Day 7)
• All along no cognitive impairment
• No objective sensory deficit
• Diplopia on presentation, though remitted
• Bulbar symptom: choking/ hoarseness
• Both shoulder and hip power 2/5
• Both ankle/wrist and hand power 4/5
• Global areflexia + withdrawal plantar
• Impression: Miller Fisher syndrome

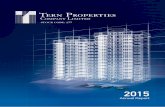
Retrospectively, look at the graph of vital signs…….

BP/P
240
220
200
180
160
140
120
100
80
60
Temp
40
39
38
37
SBP
Temp
Pulse
8P 9/3 8A 10/3 8P 10/3 8A 11/3 8P 11/3
ICU intubation
Off sedation
On sedation
Off sedation

Management at ICU day 7 (1)
• Contrast CT brain nil significant lesion• Lumbar puncture
Protein 1.85, glucose 4.0 (serum 9.0) unfit for cell count PCR for HSV/ VZV not detected
• Check ANF/ANCA/Anti-cardiolipin/ lupus anticoagulant/ cold agglutinin/ atypical pneumonia titer/ CMV and EBV serology

Management at ICU day 7 (2)
• Check Anti-Ganglioside Q1b antibody by private lab
• Give 3 more days of Intragram 21g daily
• Plan perform nerve conduction test on working day to detect any features of polyneuropathy, and to differentiate demyelinating/ axonal degeneration if any

Progress at ICU day 9
• Shoulder/ elbow power 4-/5; hand 5/5
• Hip/ knee power 3/5; ankle 4/5
• Nerve conduction test bedsideAbsent F wave response in 5 nervesProlonged distal latencyAmplitude and velocity within normalNo conduction block; sural nerve sparedAxonal degeneration; motor dominant

Progress at ICU day 10
• Proximal power 4/5, distal power 5/5
• Right brachioradialis reflex intact, right knee jerk has minimal response
• Complained of severe headache and low back pain. ?neck stiffness on exam
• ?Mechanical injury of AVM during LP

CT brain + C-spine + L-spine
• Brain showed nil significant abnormality
• No abnormal vasculature in cervical cord
• Small enhancing vessels along surface of thecal sac at level down to L2
• No evidence of bleeding from vessel

Our decision

Further progress
• Off RT and oral diet tolerated since day 11
• Discharge to general ward on day 15
• Anti-Ganglioside Q1b 105 (<20)
• ANF 1: 80; Anti-ds DNA 13 (<35)
• C-ANCA weak +ve; PR3-ANCA 6 (<20)
• Cold agglutinin 8 (<32)
• Lupus anticoagulant not detected
• Anti-cardiolipin IgG 9.5 (weak +ve)

At rehabilitation
• Repeated NCT on day 19 showed improving polyneuropathy. Yet EMG showed equivocal MG features
• Repeated Tensilon test on day 25 Still NEGATIVE result
• Neurology opinion not to resume Mestinon since MG not the dominant illness
• Home on day 48

Neurology FU
• No ocular/ bulbar or peripheral symptom• Private MRI brain and brain stem
bilateral frontal lobe atrophy only• Imp: assay for AChR binding antibody in H
A is ELIZA, may not be specific enough• Decision: check AChR binding antibody (R
IA) + AChR modulating antibody + AChR blocking antibody


Myasthenia Gravis overview
• Autoimmune disease
• Antibodies against post-synaptic acetylcholine receptor (AChR), or receptor associated protein (muscle-specific TK)
• Fluctuating weakness of muscles in various combination of ocular; bulbar; limb; resp
• Two clinical form: Ocular vs. Generalized

Presenting symptoms
• Ocular: >50%. Among ocular presentation, >50% progress to generalized in 2 years
• Bulbar: 15%. Dysarthria/ dysphagia and fatigable chewing
• Proximal limb: <5% as presenting symptom
• Rare: isolated neck; isolated resp; isolated distal limb weakness

Bedside diagnostic test of MG
• Tensilon test:Sensitivity is 0.92 for ocular; Sensitivity is 0.88 for generalizedFalse +ve: MND; brainstem tumor
• Ice-pad test:Best use for ocular MGSensitivity: 0.94 for ocular; Sensitivity: 0.82 for generalized
Neuromuscular disorders 2006; 16: 459-67

Ice test
2 min ice
Ophthalmology 1999: 106:1282

Electrophysiological studies
Repetitive nerve stimulation (RNS)
• Motor nerve is stimulated 6-10 times under low frequencies (2-3 Hz)
• Positive result if decrement in compound muscle action potential >10% within 4-5 stimuli
• Post-activation exhaustion
• Post-tetanus potentiation
• Sensitivity: 50% if ocular
• Sensitivity: 75% if generalized

30 seconds post-ex Post-activation exhaustion
Normal MG

Acetylcholine receptor antibodies 1. Binding antibody
Most sensitive: 0.93 in severe generalized MG False +ve in Eaton-Lambert; MND; myositis Positive in SLE; PBC; thymoma; relative of MG
2. Blocking Found in 50% of generalized disease May be seen in 1% of MG with negative binding a
ntibody
3. Modulating Increases sensitivity only ~5% to binding antibody
Neurology 1997; 48 (5): S23-27

Other antibodies
1. Striational antibody (anti-striated muscle) Present in 30% of MG only, but 80% in those thy
moma-assocated MG Useful marker of thymoma at age 20-50
2. Muscle-specific receptor TK (MuSK) Present in 50% of Ach-R Ab negative case ?Different pathogenesis with seropositive Oculobulbar rather than pure ocular Nil thymoma or even ?thymic atrophy Respond less to cholinesterase inhibitor
Semin Neurol 2004; 24:31


Our patients had all three AchR antibodies positive, with titre hig
h or very high at OPD

Evaluation of 550 patients with MGSaunders 2001

History of Guillain Barre Syndrome
Landry’s ascending paralysis 1859• Landry described 10 cases of weakness which asce
nded from lower limb to become generalized, and one of died of asphyxia
• “usually a motor disorder characterized by a gradual diminution of muscular strength with flaccid limbs and without contractures, convulsions or reflex movements”
• “weakness spreads rapidly from the lower to the upper parts of the body with a universal tendency to become generalised”
• Landry offered no explanation of disease

• Guillain and Barre spotted two soldiers in WWI becoming partially paralyzed, but then recovered spontaneously
• With Strohl, a paper was published in 1916, reporting educed reflexes and CSF finding of raised protein without high WCC
• In 1927, Guillain Barre syndrome was introduced, but Strohl…...

Guillain BarreStrohl

Essential features of GBS
• Progressive symmetrical muscle weakness associated with depressed deep tendon reflexes, usually begins at proximal legs
• Severity varies a lot from mild difficulty in walking to complete paralysis and respiratory failure
• Extremities, facial, bulbar and respiratory muscles are affected in combination

Other features of GBS
• Facial weakness >50%• Oropharyngeal weakness 50%• Oculomotor weakness 15%• Respiratory failure ventilation 30%• Begins from face and UL 10%• Paresthesias in hand/feet 80% (Yet nil sign)• Prominent severe back pain • Dysautonomia 70% (e.g. HT alt with shock)
NEJM 1992; 326: 1130

BP/P
240
220
200
180
160
140
120
100
80
60
Temp
40
39
38
37
SBP
Temp
Pulse
8P 9/3 8A 10/3 8P 10/3 8A 11/3 8P 11/3
ICU intubation
Off sedation
On sedation
Off sedation

Atypical GBS features
• Meningism• Papilloedema• Vocal cord palsy• Hearing loss• Mental state change e.g. hallucination, delu
sion and vivid dream has been reported in a cohort of 139 patients of GBS in ICU
Brain 2005; 128: 2535

GBS Pathogenesis
• Heterogenous syndrome caused by immune-mediated peripheral nerve damage after being evoked by antecedent infection
• Acute inflammatory demyelinating polyradiculoneuropathy (AIDP): epitopes in Schwann cell surface membrane
• Acute motor axonal neuropathy (AMAN): epitopes in axonal membrane

Possible antecedent infections
• Campylobacter jejuniGenerate antibody to specific ganglioside GM160% of AMAN/ AMSANAxonal degeneration worse prognosis
• CMV/ Epstein-Barr virus/ Mycoplasma
• HIV
• ?VZV/ HSV/ H influenzae

Diagnostic criteria (NINDS)
• Required featuresProgressive weakness >1 limb, rangin
g from minimal LL to complete tetraparesis, bulbar/facial muscles and ophthalmoplegia
Areflexia. Typiclly global areflexia, but distal areflexia + hyporeflexia at knee/ biceps will suffice

Diagnostic criteria (NINDS)
• Supportive featuresProgression of symptoms over days to 4/52Symmetrical involvementBilateral facial nerve weaknessAutonomic dysfunctionMild sensory symptoms/ signsRaised CSF protein with normal white cell
Ann Neurol 1978; 3: 565

Nerve conduction test
• Early change (~1 week)Signify nerve root demyelinationAbsent or prolonged F wavesAbsent H reflexes
• Intermediate change (~1-2 weeks)Increased distal latencyTemporal dispersion of motor response
• Late change (> 3-4 weeks)Slowing of conduction velocity


GBS variant
• Acute motor axonal neuropathy (AMAN)
• Acute motor and sensory axonal (AMSAN)
• Pharyngeal-cervical-brachial
• Paraparesis only
• Acute pandysautonomia
• Miller-Fisher syndrome
• Bickerstaff encephalitis

Differential diagnosis for GBS
• Acute polyneuropathies
• Vasculitis
• Spinal cord: compression; myelitis
• Neuromuscular junction: MG; Eaton-Lambert; botulism
• Muscle: polymyositis; CIM

Miller Fisher syndrome
• Triad: ophthalmoplegia, ataxia and areflexia• 20% patient may have extremities weakness• Anti-Ganglioside q1b antibody present in 8
5-90% of cases• NCT shows absent or diminished sensory re
sponse, and may show similar change of AIDP for cases with weakness
• CSF has similar change with GBS


Differential diagnosis for MFS
• Brainstem stroke
• Myasthenia gravis
• Wernicke encephalopathy
• Other neuromusclar junction disease e.g. Eaton-Lambert, botulism
• Bickerstaff encephalitis: ophthalmoplegia + ataxia + hyper-reflexia + anti-G Q1b +ve

Treatment of MFS
• Supportive care including ventilatory support, DVT prophylaxis, pain control
• Cardiovascualar monitoring and control
• Cholinesterase inhibitor not useful
• Immunomodulating therapy: IVIG; plasmapheresis
• Steroid has not been shown beneficial

Plasma exchange
• Maximal benefit when given within 7 days
• ?Optimal number of exchange. Possibly lying between 4-6 exchanges
• Dose of volume: 200-250ml/kg weight
• Shorten median time to recover walking by 40-50% compared to supportive treatment
• May be a problem in hemodynamics

IV IG
• Five days of IVIG of 0.4g/kg body weight
• No inferiority compared to plasmapheresis
• Common minor side-effect: headache
• Other effects: aseptic meningitis; allergy; skin rash; acute renal failure
• Life-threatening anaphylaxis reportedBrain 2007; 130: 2245-2257


Prognosis
• Median time to walk unaided 53-85 days• 5-10% patients with prolonged ventilator de
pendency, and incomplete recovery• Overall mortality 5%; 20% ventilator cases• Poor prognosis indicator: old age; rapid ons
et; diarrhoea preceded; ventilator need; reduced distal motor response amplitude <20% of normal; axonal degeneration

In summary, our patient
• Past history of ocular MG
• Symptom and sign suggest MFS
• MRI shows bystander vascular malformation around spinal cord
• NCT showed axonal degeneration
• Improved rapidly
• Presence of anti-gangliose Q1b antibody
• Anti-AchR antibodies signify underlying MG

Wish you happy lunar new year