Iron Metabolism: Interactions with Normal and Disordered ...
14
2012; doi: 10.1101/cshperspect.a011668 Cold Spring Harb Perspect Med Tomas Ganz and Elizabeta Nemeth Erythropoiesis Iron Metabolism: Interactions with Normal and Disordered Subject Collection Hemoglobin and Its Diseases Clinical Correlates Hemoglobin Variants: Biochemical Properties and Gell, et al. Christopher S. Thom, Claire F. Dickson, David A. The Prevention of Thalassemia Antonio Cao and Yuet Wai Kan Classification of the Disorders of Hemoglobin Bernard G. Forget and H. Franklin Bunn The Switch from Fetal to Adult Hemoglobin Vijay G. Sankaran and Stuart H. Orkin -Thalassemia α The Molecular Basis of Douglas R. Higgs -Thalassemias β the Pathophysiology and Clinical Manifestations of Arthur W. Nienhuis and David G. Nathan Evolution of Hemoglobin and Its Genes Ross C. Hardison Development of Gene Therapy for Thalassemia Arthur W. Nienhuis and Derek A. Persons -Hemoglobinopathies β Severity in the The Search for Genetic Modifiers of Disease Guillaume Lettre Myelodysplastic Syndrome -Thalassemia, Mental Retardation, and α Richard J. Gibbons Health Burden of the Hemoglobinopathies World Distribution, Population Genetics, and Thomas N. Williams and David J. Weatherall -Thalassemia Intermedia: A Clinical Perspective β Rachmilewitz Khaled M. Musallam, Ali T. Taher and Eliezer A. Disordered Erythropoiesis Iron Metabolism: Interactions with Normal and Tomas Ganz and Elizabeta Nemeth Thalassemia and Sickle Cell Anemia Hematopoietic Stem Cell Transplantation in al. Guido Lucarelli, Antonella Isgrò, Pietro Sodani, et of Hemoglobinopathies Pluripotent Stem Cells in Research and Treatment Natasha Arora and George Q. Daley http://perspectivesinmedicine.cshlp.org/cgi/collection/ For additional articles in this collection, see Copyright © 2012 Cold Spring Harbor Laboratory Press; all rights reserved Press on February 15, 2013 - Published by Cold Spring Harbor Laboratory http://perspectivesinmedicine.cshlp.org/ Downloaded from
Transcript of Iron Metabolism: Interactions with Normal and Disordered ...

2012; doi: 10.1101/cshperspect.a011668Cold Spring Harb Perspect Med Tomas Ganz and Elizabeta Nemeth ErythropoiesisIron Metabolism: Interactions with Normal and Disordered
Subject Collection Hemoglobin and Its Diseases
Clinical CorrelatesHemoglobin Variants: Biochemical Properties and
Gell, et al.Christopher S. Thom, Claire F. Dickson, David A.
The Prevention of ThalassemiaAntonio Cao and Yuet Wai Kan
Classification of the Disorders of HemoglobinBernard G. Forget and H. Franklin Bunn
The Switch from Fetal to Adult HemoglobinVijay G. Sankaran and Stuart H. Orkin
-ThalassemiaαThe Molecular Basis of Douglas R. Higgs -Thalassemiasβthe
Pathophysiology and Clinical Manifestations of
Arthur W. Nienhuis and David G. NathanEvolution of Hemoglobin and Its Genes
Ross C. HardisonDevelopment of Gene Therapy for Thalassemia
Arthur W. Nienhuis and Derek A. Persons
-HemoglobinopathiesβSeverity in the The Search for Genetic Modifiers of Disease
Guillaume LettreMyelodysplastic Syndrome
-Thalassemia, Mental Retardation, andα
Richard J. Gibbons
Health Burden of the HemoglobinopathiesWorld Distribution, Population Genetics, and
Thomas N. Williams and David J. Weatherall
-Thalassemia Intermedia: A Clinical Perspectiveβ
RachmilewitzKhaled M. Musallam, Ali T. Taher and Eliezer A.
Disordered ErythropoiesisIron Metabolism: Interactions with Normal and
Tomas Ganz and Elizabeta NemethThalassemia and Sickle Cell AnemiaHematopoietic Stem Cell Transplantation in
al.Guido Lucarelli, Antonella Isgrò, Pietro Sodani, et
of HemoglobinopathiesPluripotent Stem Cells in Research and Treatment
Natasha Arora and George Q. Daley
http://perspectivesinmedicine.cshlp.org/cgi/collection/ For additional articles in this collection, see
Copyright © 2012 Cold Spring Harbor Laboratory Press; all rights reserved
Press on February 15, 2013 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from

Iron Metabolism: Interactions with Normal andDisordered Erythropoiesis
Tomas Ganz and Elizabeta Nemeth
Department of Medicine and Department of Pathology and Laboratory Medicine, David Geffen School ofMedicine, University of California, Los Angeles, California 90095
Correspondence: [email protected]
Hemoglobinopathies and other disorders of erythroid cells are often associated with abnor-mal iron homeostasis. We review the molecular physiology of intracellular and systemic ironregulation, and the interactions between erythropoiesis and iron homeostasis. Finally, wediscuss iron disorders that affect erythropoiesis as well as erythroid disorders that cause irondysregulation.
Iron overload is a common complication ofhemoglobinopathies treated by erythrocyte
transfusions (1 mL of packed erythrocytes con-tains about 1 mg of iron) and those associatedwith ineffective erythropoiesis, which stimulatesthe hyperabsorption of dietary iron. With theincreasing use of transfusion therapy, iron over-load has become a major cause of morbidity andpremature mortality. More recently, the effectivetreatment of iron overload by iron chelation hasdramatically improved survival (Cunningham2008; Telfer 2009). This work reviews recent ad-vances in our understanding of the molecularbasis of iron homeostasis and its disorders.
IRON BIOLOGY AND HOMEOSTASIS
Iron Intake
Iron is the most abundant element on Earth bymass and the fourth most abundant in theEarth’s crust but it readily oxidizes into insolu-ble compounds with poor bioavailability. In
this environment, biological organisms evolvedto conserve iron. Quantitative analysis of tissueiron distribution and fluxes in humans illus-trates how this is accomplished (Finch 1994).The typical adult human male contains about4 g of iron of which about 2.5 g is in hemoglo-bin, 1 g is stored predominantly in hepatocytesand hepatic and splenic macrophages, and mostof the rest is distributed in myoglobin, cyto-chromes, and other ferroproteins. Only about1–2 mg/d, or ,0.05%/d, is lost from the bodypredominantly through desquamation and mi-nor blood loss. In the steady state, this amountis replaced through intestinal iron absorption.Although the loss of iron may increase slightlywith increasing iron stores, these changes do notsignificantly contribute to homeostasis; intesti-nal iron absorption is by far the predominantdeterminant of the iron content of the body. Atypical Western diet provides about 15 mg ofiron per day and only �10% is absorbed. Re-covery from blood loss causes an increase in ironabsorption up to 20-fold, indicating that the
Editors: David Weatherall, Alan N. Schechter, and David G. Nathan
Additional Perspectives on Hemoglobin and Its Diseases available at www.perspectivesinmedicine.org
Copyright # 2012 Cold Spring Harbor Laboratory Press; all rights reserved; doi: 10.1101/cshperspect.a011668
Cite this article as Cold Spring Harb Perspect Med 2012;2:a011668
1
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
Press on February 15, 2013 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from

duodenum where iron absorption takes placehas a large reserve capacity for iron absorption.Pathological increase of intestinal iron absorp-tion is a common cause of iron overload, ac-counting for the excess iron in hereditary hemo-chromatosis and untransfused b-thalassemia.Blood transfusions and parenteral administra-tion of iron compounds bypass the regulatorybottleneck of iron absorption and constitutethe other major cause of iron overload.
Iron Recycling
Under normal circumstances, the reutilizationof iron recycled from senescent cells accountsfor most of the iron flux in humans. With theerythrocyte lifespan of 120 d, 20–25 mg of ironis required to replace the 20–25 mL of erythro-cytes that must be produced every day to main-tain a steady state. Other cell types also turn overbut their much lower iron content contributesrelatively little to the iron flux. Macrophages inthe liver, spleen, and marrow (formerly calledthe reticuloendothelial system) phagocytose se-nescent or damaged erythrocytes, degrade theirhemoglobin to release heme, extract iron fromheme using heme oxygenase (Poss and Tonega-wa 1997), and recycle the iron to the extracellu-lar fluid and plasma. Steady-state iron flux fromrecycling can increase up to 150 mg/d in con-ditions with ineffective erythropoiesis in whichthe number of erythroid precursors is increasedand accompanied by the apoptosis of hemoglo-binized erythrocyte precursors in the marrowand shortened erythrocyte survival (Beguinet al. 1988).
Iron Distribution and Storage
Free iron is highly reactive and causes cell andtissue injury through its ability to catalyze theproduction of reactive oxygen species. In livingorganisms, iron is complexed with proteins orsmall organic molecules (citrate, acetate), whichmitigate its reactivity. Transferrin is the physio-logical carrier of iron in plasma. Normally, only20%–40% of the available binding sites ontransferrin molecules are occupied by ferriciron. The iron content of plasma is only 2–3 mg
so this compartment must turn over every fewhours. Erythrocyte precursors take up iron al-most exclusively through transferrin receptors(TfR1) so the iron supply to erythrocyte precur-sors is completely dependent on plasma trans-ferrin. In contrast, hepatocytes and other non-erythroid cells can also take up iron that is notbound to transferrin (nontransferrin-boundiron or NTBI), a process that becomes impor-tant during iron overload when plasma trans-ferrin saturation reaches 100% (Breuer et al.2000). The predominant cellular storage formof iron is the hollow spherical protein ferritinwhose cavity contains iron in ferric form com-plexed with hydroxide and phosphate anions.
Regulation of Plasma Iron Concentrations
Despite varying dietary iron intake and changesin erythropoietic activity owing to occasionalor periodic blood loss, iron concentrations inplasma normally remain in the 10–30 mM range.Chronically low concentrations decrease ironsupply to erythropoiesis and other processesleading to anemia and dysfunction of othercell types sensitive to iron deprivation. Chroni-cally high iron concentrations lead to intermit-tent or steady-state saturation of transferrin withiron and the generation of NTBI with conse-quent deposition of excess iron in the liver, en-docrine glands, cardiac myocytes, and other tis-sues. Excess cellular iron may cause tissue injuryby catalyzing the generation of reactive oxygenspecies, which can cause DNA damage, lipidperoxidation, and oxidation of proteins.
Systemic Iron Homeostasis
Phenomenological description of systemic ironhomeostasis was developed starting in the 1930s(Finch 1994). Homeostatic mechanisms regu-late dietary iron absorption and iron depositioninto or withdrawal from stores depending on theamount of stored iron (“stores regulator”) andthe requirements of erythropoiesis (“erythro-poietic regulator”). The description of the mo-lecular processes that underlie iron homeostasishas progressed rapidly in the last two decadesbut is still not complete.
T. Ganz and E. Nemeth
2 Cite this article as Cold Spring Harb Perspect Med 2012;2:a011668
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
Press on February 15, 2013 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from

CELLULAR IRON REGULATION
Cellular Iron
Cells require iron predominantly for incorpora-tion into various ferroproteins, where iron existsin iron–sulfur clusters, in heme or hemelikeprosthetic moieties, or in other more looselyassociated forms. It now appears that most celltypes in the body autonomously regulate theiriron uptake solely to meet their individual re-quirements for iron. These cells do not exportappreciable amounts of iron and are presumedto give up their iron only when they undergo celldeath and are recycled by macrophages. In con-trast, several specialized cell types supply or storeiron to meet the needs of the entire organism,and are therefore equipped to export iron intoextracellular fluid and plasma. Iron-exportingcells include duodenal enterocytes that absorbdietary iron, macrophages that recycle ironfrom senescent or dead cells, and macrophagesand hepatocytes that store iron and release it tomeet systemic demand. During pregnancy, theplacental syncytiotrophoblast must transportmaternal iron into the fetal circulation to meetthe iron requirements of fetal growth and devel-opment. The endothelial cells that form theblood–brain barrier must also selectively trans-port iron as it now appears that the iron con-centrations in the brain are not appreciably in-creased in systemic iron overload disorders.Finally, erythroid precursors need much moreiron than any other cell type as each cell synthe-sizes more than a billion heme molecules, there-fore facing greater iron-homeostatic challenges.
Cellular Iron Uptake
Transferrin-mediated iron uptake is the best un-derstood mechanism of cellular iron import.Although the transferrin receptor (TfR1) is ex-pressed in many cell types, erythrocyte precur-sors contain most of the TfR1 molecules andtake up the great majority of iron-transferrinin the organism. Iron-transferrin is endocytosedvia the cell membrane TfR1 and internalizedinto endosomal recycling vesicles. As the vesicleacidifies, the low pH releases the transferrin-bound ferric iron and the iron-free (apo)trans-
ferrin-TfR1 complex returns to the cell mem-brane (Fig. 1). The neutral pH at the membranecauses the apotransferrin to dissociate fromTfR1, whereupon apotransferrin diffuses awayto be loaded with iron again, repeating the cycle.From the vesicle, iron is delivered to mitochon-dria where it is incorporated into protoporphy-rin IX to form heme, or incorporated into na-scent iron–sulfur clusters. Alternatively, ironcan be exported from the vesicle into the cyto-plasm where it is incorporated into cytoplasmicferroproteins or stored in cytoplasmic ferritin.
Nontransferrin-bound iron (NTBI) (Breueret al. 2000) usually accumulates when the iron-binding capacity of transferrin is exceeded andthen circulates complexed mostly with citrate oracetate. Hemoglobinopathies such as b-thalas-semia major and intermedia are associated withparticularly high levels of NTBI. Some cells, in-cluding hepatocytes, cardiomyocytes, and cellsof endocrine glands can take up NTBI, althoughthe precise mechanism is not well understood.Candidate NTBI transporters include L-typevoltage-gated calcium channels, DMT-1 andZip14.
Intracellular Iron Transport
To undergo transport to the cytoplasm or mi-tochondria, ferric iron must be reduced to itsferrous form through the action of ferrireduc-tases. Recent studies indicate that Steap (six-transmembrane epithelial antigen of the pros-tate) proteins 1–4 are among the relevant fer-rireductases, with Steap3 having a particularimportance in erythroid precursors (Fig. 1), as-sisted perhaps by Steap2 and Steap4 (Ohgamiet al. 2006). To reach the cytoplasm, ferrous ironmust cross the membrane of the vesicle. In manycells, the proton-dependent ferrous iron trans-porter divalent metal transporter-1 (DMT1)appears essential for iron transport from thevacuole into the cytoplasm but in macrophagesits homolog natural resistance-associated mac-rophage protein (Nramp1) may also contribute(Soe-Lin et al. 2009). Because of its chemicalreactivity, iron is chaperoned in the cytoplasm,at least in part by multifunctional poly(RC)-binding proteins (PCBPs) (Shi et al. 2008). In
Iron Metabolism
Cite this article as Cold Spring Harb Perspect Med 2012;2:a011668 3
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
Press on February 15, 2013 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from

particular, PCBP1 mediates the delivery of ironto cytoplasmic ferritin and both PCBP1 and 2are involved in the delivery of iron to cytoplas-mic iron-dependent prolyl and asparaginyl hy-droxylases that mediate oxygen sensing (Nandalet al. 2011). It is not known how iron is trans-ported to mitochondria. In erythroid cells, thereis evidence for a “kiss-and-run” mechanism(Fig. 1) whereby iron could be transferredfrom endosomal vesicles directly to mitochon-dria (Sheftel et al. 2007) but it is not clear howmuch this mechanism contributes to the ironflux into mitochondria and whether it alsofunctions in nonerythroid cell types.
Mitochondria and Iron
Consistent with their autonomous evolutionaryorigin, mitochondria are equipped with distinctiron transporters. Iron uptake into mitochon-dria depends on the inner mitochondrial mem-brane proteins mitoferrin 1 and 2, with the for-mer predominantly expressed in erythroid cellsand the latter ubiquitously (Paradkar et al. 2009;Troadec et al. 2011). In erythroid cells, mitofer-rin 1 interacts with the ATP-binding transporterAbcb10 and with ferrochelatase to form a plau-sible pathway for the delivery of iron for hemeformation (Chen et al. 2010). How heme is
Tf reloaded with Fe3+
by macrophages and duodenal enterocytes
Decreased pH
TfFe
3+
Tf
TfR1
TfR1
DM
T1
Tf
Steap3
TfR1
Fe3+
Fe2+
Fe2+Ch K & R
Hemoglobin
Hemeexport
Mfrn1
Mfrn1
Fpn
FLVCR
1
Mitochondria
Fe3+
Tf
TfR1
Figure 1. Iron traffic in erythrocyte precursors synthesizing hemoglobin. Iron is taken up as diferric transferrinby the transferrin receptor (TfR1). Acidification of the endocytic vesicle releases ferric iron from transferrin, andthe membrane ferrireductase Steap3 reduces it to ferrous iron, which is then exported to the cytoplasm byDMT1. The complex of iron-free apotransferrin (Tf ) and TfR1 is returned to the plasma membrane where theneutral pH causes Tf to dissociate from its receptor. The transferrin cycle is completed when Tf is reloaded withferric iron by duodenal enterocytes or iron-recycling macrophages. Ferrous iron exported by DMT1 may bedelivered to mitochondrial mitoferrin-1 (Mfrn1) by direct contact (the kiss-and-run mechanism, K&R) orthrough intermediate transport by as-yet uncharacterized cytoplasmic chaperones (Fe2þCh). Mitoferrin-1imports iron into mitochondria where iron is incorporated into newly synthesized heme. Heme is exportedvia an unknown exporter (Heme export) and incorporated into globin chains to generate hemoglobin. Undersome circumstances, iron is exported as ferrous iron via ferroportin (Fpn) or as heme via feline leukemia virus Creceptor (FLVCR1).
T. Ganz and E. Nemeth
4 Cite this article as Cold Spring Harb Perspect Med 2012;2:a011668
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
Press on February 15, 2013 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from

exported from mitochondria for incorporationinto hemoglobin and other hemoproteins is notknown. Mitochondria also contain a distinctferritin, mitochondrial ferritin, for local ironstorage.
Cellular Iron Homeostasis
Cellular, as opposed to systemic, iron homeosta-sis assures that sufficient but not excessiveamounts of iron are taken up by each cell tomeet its individual requirement for ferroproteinsynthesis. The system that has evolved relieson posttranscriptional regulation through theinteraction of iron-regulatory proteins (IRP1and IRP2) with iron-regulatory elements (IREs)in messenger RNAs (mRNAs) that encode keyiron transporters, ferroproteins, and enzymesinvolved in iron-utilizing pathways. The IRE/IRP system effectively regulates iron uptake, pro-vides for the storage of excess iron in ferritin, andcoordinates the synthesis of heme, iron–sulfurclusters, and ferroproteins with the availabilityof iron. The system in effect acts to decreasewasted expenditure of synthetic energy and sub-strates, and to prevent accumulation of toxicforms of iron. Target mRNAs contain IREs thatform characteristic stem-loop structures eitherin the 50 region, where IRP binding repressestranslation and decreases protein synthesis, orin the 30 region where IRP binding prevents en-donucleases from cleaving sensitive regions ofthe mRNA, thus stabilizing mRNA and increas-ing protein synthesis (Casey et al. 1988). IRP1and IRP2 are structurally related but interactwith iron in distinct ways. Both proteins bindto IREs when cellular iron levels are low. In thepresence of iron, IRP1 incorporates an iron–sulfur cluster, does not bind IREs, and acts asan aconitase enzyme converting citrate to isoci-trate in the Krebs cycle. In contrast, IRP2 is ubiq-uitinated by a complex iron-dependent processand then degraded in proteasomes (Salahudeenet al. 2009; Vashisht et al. 2009). The dual spe-cificity of IRP1/aconitase may have a functionalrole in the regulation of erythropoiesis by ironavailability, as the provision of the aconitaseproduct isocitrate reverses some of the suppres-sive effect of iron deprivation on erythropoiesis
and the enzymatic inhibition of aconitase hasthe opposite effect (Bullock et al. 2010; Talbotet al. 2011). Many mRNAs are regulated by theIRP/IRE system (Sanchez et al. 2011) and fallinto three classes: (1) iron acquisition, generallywith IREs in the 30 region resulting in increasedprotein synthesis during cellular iron depriva-tion; (2) iron utilization and storage, with IREsin the 50 region, resulting in repressed proteinsynthesis during iron deprivation; and (3) ironexport, with IREs also in the 50 region and pro-tein synthesis repressed during iron deprivation.Proteins subject to IRE/IRP regulation includeTfR1 and DMT1 involved in cellular iron uptake,aminolevulinic acid synthase 2, which catalyzesthe first step of the heme synthesis pathway inerythroid cells, the heavy and light subunits offerritin involved in iron storage, and ferroportin,the iron exporter expressed in tissues and cellsinvolved in iron export to plasma. The net effectof the IRE/IRP response during cellular irondeficiency is to increase cellular iron uptake,mobilize iron from cellular storage, decreaseiron utilization, and, when iron becomes suffi-cient or excessive to reverse these responses anddirect more iron into cellular storage and ex-port. Further fine-tuning of iron import andexport is achieved by differential splicing of tar-get mRNAs in different tissues to either includeor exclude IREs. As an example, systemic adap-tation to iron deficiency may be facilitated bya ferroportin mRNA isoform that lacks IRE,which may allow iron-transporting duodenalenterocytes to deliver iron to plasma for system-ic needs even if the enterocyte is sensing irondeficiency, and may transfer iron from ery-throid cells to other tissues more critically de-pendent on iron (Zhang et al. 2009).
Generalized Regulation of Protein Synthesisby Iron in Erythroid Cells
In addition to the regulation of the synthesis ofindividual proteins by iron, erythroid cells alsocontain a mechanism for a generalized adaptiveresponse to iron deficiency. This response is af-fected by the heme-regulated inhibitor kinase(HRI) belonging to a class of kinases activatedbycellular stress, including nutrient deprivation,
Iron Metabolism
Cite this article as Cold Spring Harb Perspect Med 2012;2:a011668 5
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
Press on February 15, 2013 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from

viral infection, and endoplasmic reticulumstress(Chen 2007). During iron deficiency as hemeconcentrations drop, heme dissociates fromHRI, causing it to undergo specific autophos-phorylation to become a catalytically active ki-nase targeting thea subunit of eukaryotic trans-lational initiation factor 2 (eIF2a). ActivatedHRI inhibits translational initiation by phoshor-ylating eIF2a. Not all protein synthesis is inhib-ited however, as activated HRI may promote thesynthesis of transcription factors that are protec-tive during iron-deficient erythropoiesis (Liuet al. 2008). A priori, it is not obvious how irondeficiency results in the production of smaller,less-hemoglobinized erythrocytes rather thanfewer normally sized and hemoglobinized cells.Studies with HRI-deficient mice showed thatHRI protects erythroid precursors from apopto-sis induced by excessive production of globinchains and contributes to the microcytosis andhypochromia seen in iron deficiency, erythro-poietic protoporphyria, and b-thalassemia.
Iron and Hypoxia Sensing
The hypoxia-sensing pathway may also contrib-ute to cellular iron homeostasis. Prolyl and as-paraginyl hydroxylases, which inactivate the HIFtranscription factors, are not only sensitive tooxygen tension but also to iron concentrationsbecause they use iron as a catalytic cofactor. Insupport of the potential role of HIF in iron reg-ulation, tissue-specific deletion of HIF2a inmouse enterocytes decreased intestinal iron ab-sorption as well as the expression of DMT1 inenterocytes (Mastrogiannaki et al. 2009). HIF2abound to the DMT1 promoter and transacti-vated it. The broader physiologic function ofHIF in cellular iron homeostasis still remains tobe established and may vary in different tissuesdepending on oxygen tension and other factors.
SYSTEMIC IRON HOMEOSTASIS
The Central Role of Hepcidin
Systemic iron homeostasis encompasses the reg-ulatory circuitry that controls the absorption ofdietary iron, the concentration of iron in extra-
cellular fluid and blood plasma, and the releaseof iron from macrophages involved in iron re-cycling and from iron-storing hepatocytes. Itnow appears that there is a single systemic reg-ulator of iron, the hepatic peptide hormonehepcidin. The hormone inhibits iron deliveryto plasma and extracellular fluid thereby con-trolling the concentration of iron in plasma.Hepcidin inhibits the transfer of dietary ironfrom duodenal enterocytes to plasma, the re-lease of recycled iron from macrophages to plas-ma, and the release of stored iron from hepato-cytes (Fig. 2). Fetal hepcidin inhibits the transferof maternal iron across the placenta to the fetalcirculation. At the molecular level, hepcidin actsby binding to its receptor, ferroportin, and caus-ing its endocytosis and proteolysis, which re-sults in decreased iron release from cells to plas-ma and extracellular fluid. Ferroportin is foundat very low concentrations in most cell types butmuch higher amounts in professional iron-transporting tissues, including the duodenal en-terocytes and splenic macrophages. Intermedi-ate concentrations of ferroportin are detectablein hepatocytes.
Regulation of Hepcidin Synthesis
Hepatocytes are the main source of hepcidin,with much lower amounts produced by macro-phages, adipocytes, and perhaps other cells.Hepcidin synthesis is controlled predominantlyat the transcriptional level and is increased byplasma iron-transferrin as well as by iron storedin hepatocytes (the “stores” regulator), is sup-pressed in response to increased iron require-ments of erythroid precursors (the “erythroid”regulator), and is potently stimulated by in-flammation (Fig. 2).
Regulation of Hepcidin Synthesis by Iron
Iron regulation of hepcidin is mediated by thecanonical bone morphogenetic protein path-way adapted for hepcidin regulation by iron-specific molecular components (Fig. 3). Nor-mal iron regulation in the murine modelrequires the iron-specific ligand bone morpho-genetic protein 6 (BMP6), interacting with the
T. Ganz and E. Nemeth
6 Cite this article as Cold Spring Harb Perspect Med 2012;2:a011668
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
Press on February 15, 2013 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from

BMP receptor. Another iron-specific compo-nent required for normal hepcidin regulationby iron is the membrane protein hemojuvelin,which interacts with BMPs as well as with theBMP receptor. The BMP receptor is a ligand-activated serine/threonine kinase, which phos-phorylates the cytoplasmic proteins Smad1,5, and 8. Together with the common Smad4,the phosphorylated Smads form heterodimers,which reach the nucleus and enhance the tran-scription of hepcidin. The synthesis of the BMP6ligand appears to be responsive predominantlyto iron stores rather than transferrin saturation,and compared to the large changes in hepcidinexpression, BMP6 changes in a relatively narrowrange. In contrast, changes in extracellular iron-transferrin concentration affect signal transduc-tion by the BMP receptor even in the absence ofchanges in BMP6 mRNA concentration, indi-
cating that iron-transferrin modulates the sensi-tivity of the receptor to its ligands. It is notknown with certainty how the concentration ofiron-transferrin is sensed but ablation of HFE orTfR2, and especially the combined loss of bothmolecules, decreases hepcidin expression andinterferes with the sensing of transient changesin iron-transferrin while preserving the increasein BMP6 and the chronic hepcidin response toiron loading (Wallace et al. 2009; Ramos et al.2011; Corradini et al. 2011). A plausible currentmodel postulates that iron-transferrin is sensedby TfR1 and TfR2, with HFE shuttling betweenthe two molecules depending on iron-transfer-rin concentrations. At higher iron-transferrinconcentrations, the association of TfR2 andHFE somehow potentiates BMP receptor com-plex signaling. Two other proteins, GPI-linkedhemojuvelin (Papanikolaou et al. 2004) and the
Liver Spleen
Inflammation
Hepcidin
Hepcidin
Hepcidin
Fpn
Fpn
Duodenum
Erythropoietic signal
Bone marrow
Iron signals
Fpn
PlasmaFe-Tf
Erythrocytes
LiverFe
Figure 2. Iron homeostasis. Through membrane ferroportin (Fpn), iron flows into plasma (pale blue arrows)from duodenal enterocytes, iron-storing hepatocytes, and iron-recycling macrophages predominantly in thespleen. Iron-transferrin (Fe-Tf ) is mostly delivered to the marrow (pale blue arrow) where iron is incorporatedinto erythrocyte hemoglobin (red). When the erythrocytes live out their lifespan (normally 120 d in humans),their hemoglobin and heme are degraded in the macrophages, mostly in the spleen, and iron is returned into theplasma iron pool. Hepatocytes secrete hepcidin under the control of stimulatory signals that reflect liver ironstores and plasma iron concentrations (blue), inhibitory signals reflecting erythropoietic activity (red), andinflammatory cytokines (green). Hepcidin causes the degradation of Fpn and thereby inhibits iron delivery toplasma and the erythropoietic bone marrow.
Iron Metabolism
Cite this article as Cold Spring Harb Perspect Med 2012;2:a011668 7
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
Press on February 15, 2013 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from
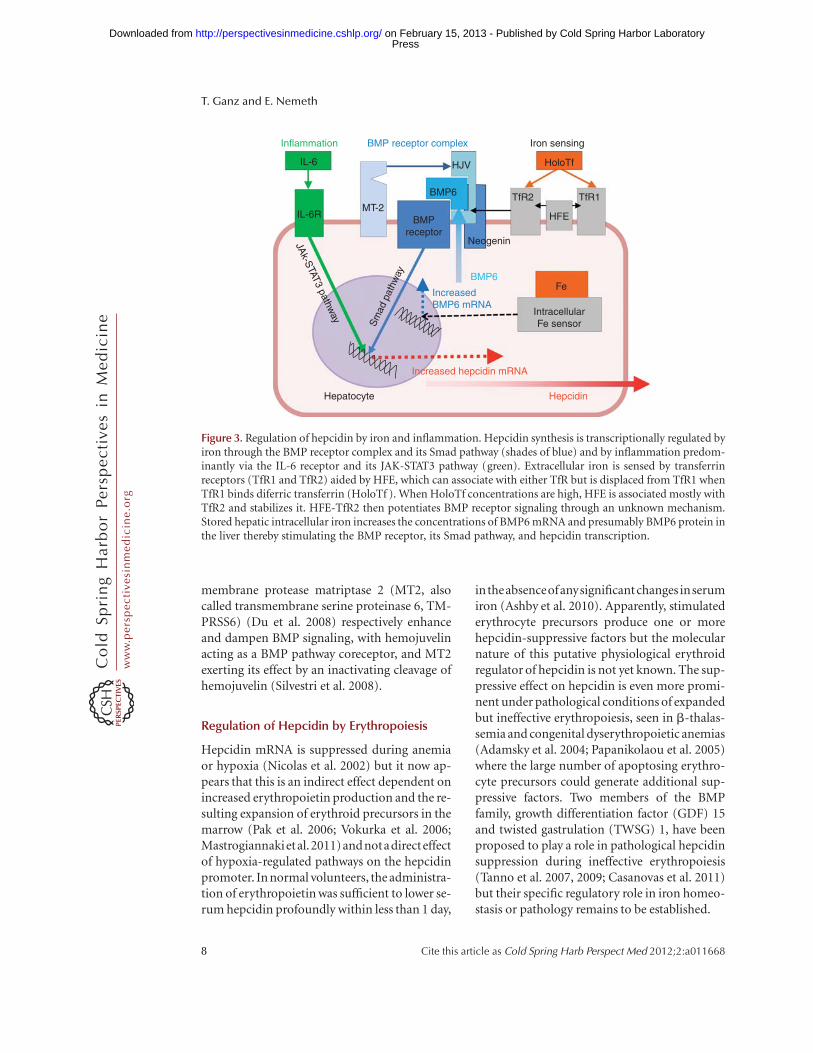
membrane protease matriptase 2 (MT2, alsocalled transmembrane serine proteinase 6, TM-PRSS6) (Du et al. 2008) respectively enhanceand dampen BMP signaling, with hemojuvelinacting as a BMP pathway coreceptor, and MT2exerting its effect by an inactivating cleavage ofhemojuvelin (Silvestri et al. 2008).
Regulation of Hepcidin by Erythropoiesis
Hepcidin mRNA is suppressed during anemiaor hypoxia (Nicolas et al. 2002) but it now ap-pears that this is an indirect effect dependent onincreased erythropoietin production and the re-sulting expansion of erythroid precursors in themarrow (Pak et al. 2006; Vokurka et al. 2006;Mastrogiannakietal.2011)andnotadirecteffectof hypoxia-regulated pathways on the hepcidinpromoter. In normal volunteers, the administra-tion of erythropoietin was sufficient to lower se-rum hepcidin profoundly within less than 1 day,
intheabsenceofanysignificantchanges inserumiron (Ashby et al. 2010). Apparently, stimulatederythrocyte precursors produce one or morehepcidin-suppressive factors but the molecularnature of this putative physiological erythroidregulator of hepcidin is not yet known. The sup-pressive effect on hepcidin is even more promi-nent under pathological conditions of expandedbut ineffective erythropoiesis, seen in b-thalas-semia and congenital dyserythropoietic anemias(Adamsky et al. 2004; Papanikolaou et al. 2005)where the large number of apoptosing erythro-cyte precursors could generate additional sup-pressive factors. Two members of the BMPfamily, growth differentiation factor (GDF) 15and twisted gastrulation (TWSG) 1, have beenproposed to play a role in pathological hepcidinsuppression during ineffective erythropoiesis(Tanno et al. 2007, 2009; Casanovas et al. 2011)but their specific regulatory role in iron homeo-stasis or pathology remains to be established.
Inflammation
IL-6
IL-6RMT-2
BMP6
HJV HoloTf
Iron sensing
TfR1TfR2
Neogenin
Sm
ad p
athw
ay
JAk-S
TAT3 pathway
Fe
Increased hepcidin mRNA
HepcidinHepatocyte
IntracellularFe sensor
BMP6
IncreasedBMP6 mRNA
BMP receptor complex
HFEBMPreceptor
Figure 3. Regulation of hepcidin by iron and inflammation. Hepcidin synthesis is transcriptionally regulated byiron through the BMP receptor complex and its Smad pathway (shades of blue) and by inflammation predom-inantly via the IL-6 receptor and its JAK-STAT3 pathway (green). Extracellular iron is sensed by transferrinreceptors (TfR1 and TfR2) aided by HFE, which can associate with either TfR but is displaced from TfR1 whenTfR1 binds diferric transferrin (HoloTf ). When HoloTf concentrations are high, HFE is associated mostly withTfR2 and stabilizes it. HFE-TfR2 then potentiates BMP receptor signaling through an unknown mechanism.Stored hepatic intracellular iron increases the concentrations of BMP6 mRNA and presumably BMP6 protein inthe liver thereby stimulating the BMP receptor, its Smad pathway, and hepcidin transcription.
T. Ganz and E. Nemeth
8 Cite this article as Cold Spring Harb Perspect Med 2012;2:a011668
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
Press on February 15, 2013 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from

Regulation of Hepcidin by Inflammation
During infections and inflammation, the syn-thesis and serum concentrations of hepcidinare greatly increased (Pigeon et al. 2001; Nicolaset al. 2002; Nemeth et al. 2003, 2004; Ganz et al.2008). This regulatory circuitry is thought to berelated to the possible role of hepcidin in hostdefense whereby hepcidin-mediated iron re-striction may limit microbial growth. Multi-ple cytokines stimulate hepcidin transcriptionduring inflammation, chief among them IL-6(Nemeth et al. 2003, 2004) and the membersof the BMP family (Maes et al. 2010). Interleu-kin-6 activates the JAK-STAT3 pathway (Fig. 3),with STAT3 binding to canonical binding sites inthe hepcidin promoter, leading to transcription-al stimulation of hepcidin synthesis (Wrightingand Andrews 2006; Pietrangelo et al. 2007; VergaFalzacappa et al. 2007). The BMP and IL-6 path-ways are synergistic through a mechanism that isnot yet fully defined (Verga Falzacappa et al.2008; Maes et al. 2010). Inflammation may con-tribute to elevated serum hepcidin levels seen inmany adult patients with sickle cell anemia(Kroot et al. 2009; Porter 2009).
DISORDERS OF IRON HOMEOSTASIS
Iron Deficiency
Worldwide, iron deficiency is the most commoniron disorder (see Miller 2012). Although it isthought of as a predominantly acquired prob-lem caused by blood loss and inadequate ironintake, genetic predisposition may modulatethe susceptibility to this condition as illustratedby genome-wide association studies (Benyaminet al. 2009a,b; Chambers et al. 2009; Tanakaet al. 2010). Not surprisingly, associations havebeen reported between serum iron concentra-tions and polymorphisms and mutations intransferrin, HFE, and MT2 (TMPRSS6).
Anemia of Inflammation (Anemia ofChronic Disease)
Infections and inflammatory disorders are acommon cause of iron maldistribution, mediat-ed by increased plasma hepcidin concentrations
that restrict the release of recycled iron frommacrophages and hepatocyte stores, and inter-fere with the absorption of dietary iron. Ironrestriction limits hemoglobin synthesis andcontributes to anemia although other factors(inadequate erythropoietin production, cyto-kine effects on the marrow, decreased erythro-cyte lifespan) may also participate, dependingon the underlying disease. Clinically, this disor-der is manifested most often as a normocyticnormochromic anemia with hypoferremia, butthe anemia can be microcytic, especially in chil-dren or very chronic inflammatory disorders.
Iron-Refractory Iron Deficiency Anemia
This relatively rare condition is detected in chil-dren who present with an unexplained hypo-ferremia and microcytic anemia resistant tooral iron administration, and partially resistanteven to intravenous iron supplementation. Thepatients have elevated or high normal hepcidinlevels (Finberg et al. 2008) in stark contrast tocommon iron deficiency in which serum hepci-din is very lowor undetectable (Ganz et al. 2008).
Iron Overload from Transfusions
Blood transfusions deliver �1 mg of iron foreach mL of packed erythrocytes or more than200 mg per each unit transfused, effectively by-passing the regulatory mechanisms that controliron intake. Excess iron may eventually causetoxicity and organ damage, and can only be re-moved by phlebotomy (contraindicated if pa-tient is still anemic) or by treatment with che-lating agents. Extrapolating from clinical datafor iron-related toxicity in hereditary hemo-chromatosis, chelation therapy is recommendedafter 10–20 transfusions for those patients whoneed chronic erythrocyte transfusions (Britten-ham 2011).
Hereditary Hemochromatosis andRelated Disorders
Hereditary hemochromatosis is a group of ge-netic disorders that impede either hepcidin pro-duction or its regulation by iron (Nicolas et al.
Iron Metabolism
Cite this article as Cold Spring Harb Perspect Med 2012;2:a011668 9
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
Press on February 15, 2013 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from

2001; Papanikolaou et al. 2005) or, very rarely,cause the resistance of ferroportin to internali-zation by hepcidin (Fernandes et al. 2009; Shamet al. 2009). In the order of increasing severity ofhepcidin deficiency and iron overload, autoso-mal recessive forms can result from mutationsin genes encoding HFE, TfR2, hemojuvelin, andhepcidin. Ferroportin resistance to hepcidin isattributable to autosomal-dominant mutationsin ferroportin that either interfere with hepci-din binding or with ferroportin internalization.Additional genes that caused iron overload intransgenic mouse models but have not yet beenimplicated in humans include BMP6 (Andrio-poulos Jr. et al. 2009; Meynard et al. 2009) andneogenin (Lee et al. 2010). Hepatic iron over-load can also develop as a part of more complexgenetic diseases, including deficiencies of trans-ferrin and ceruloplasmin and loss-of-functionmutations in DMT1 (Pietrangelo et al. 2011). Inthese disorders, iron-restrictive anemia devel-ops because of diminished iron release frommacrophages (ceruloplasmin deficiency), irondelivery to erythrocytes (transferrin deficiency),or iron utilization by erythrocyte precursors(DMT1 loss of function). In contrast, simplehereditary hemochromatosis in humans hasonly modest effects on erythropoiesis, limitedto a slight increase in mean corpuscular volume(McLaren et al. 2007).
Iron Overload Associated with IneffectiveErythropoiesis
Ineffective erythropoiesis is acondition inwhichlarge numbers of marrowerythrocyte precursorsundergo apoptosis and so fail to complete mat-uration into erythrocytes. Genetic lesions thatcause ineffective erythropoiesis prominentlyinclude thalassemias and congenital dysery-thropoietic anemias. In these disorders, hepci-din is suppressed (Adamsky et al. 2004; Papani-kolaou et al. 2005; Kearneyet al. 2007; Casanovaset al. 2011) causing hyperabsorption of dietaryiron and iron overload even in the absenceof erythrocyte transfusions (Origa et al. 2007).Transfusions partially relieve the erythropoie-tin-driven expansion of ineffective erythropoie-sis and raise hepcidin concentrations (Kearney
et al. 2007) but cause iron overload owing to theiron content of transfused blood.
Modulation of Ineffective Erythropoiesis byIron Availability
Recent studies in mouse models of thalassemiasuggest that increased concentrations of plasmairon in this condition may further unbalanceheme and globin synthesis and worsen ineffec-tive erythropoeisis, and conversely, that re-stricting the iron supply through the administra-tion of apotransferrin or hepcidin may improveerythropoiesis (Gardenghi et al. 2010a,b; Liet al. 2010). It remains to be seen whether similarinterventions will be helpful in human disease.
CONCLUDING REMARKS
Iron homeostasis is intimately intertwined witherythropoiesis, the main destination of iron inhumans and other vertebrates. Iron overload isa clinically important aspect of various hemo-globinopathies because of transfusion-inducediron overload and because of pathological sup-pression of hepcidin synthesis with resultinghyperabsorption of dietary iron. Advances inthe understanding of iron homeostasis and itsinteractions with erythropoiesis should trans-late into improved outcomes for patients withhemoglobinopathies.
REFERENCES�Reference is also in this collection.
Adamsky K, Weizer O, Amariglio N, Breda L, Harmelin A,Rivella S, Rachmilewitz E, Rechavi G. 2004. Decreasedhepcidin mRNA expression in thalassemic mice. Br JHaematol 124: 123–124.
Andriopoulos B Jr, Corradini E, Xia Y, Faasse SA, Chen S,Grgurevic L, Knutson MD, Pietrangelo A, Vukicevic S,Lin HY, et al. 2009. BMP6 is a key endogenous regulatorof hepcidin expression and iron metabolism. Nat Genet41: 482–487.
Ashby DR, Gale DP, Busbridge M, Murphy KG, Duncan ND,Cairns TD, Taube DH, Bloom SR, Tam FW, Chapman R,et al. 2010. Erythropoietin administration in humanscauses a marked and prolonged reduction in circulatinghepcidin. Haematologica 95: 505–508.
Beguin Y, Stray SM, Cazzola M, Huebers HA, Finch CA.1988. Ferrokinetic measurement of erythropoiesis. ActaHaematol 79: 121–126.
T. Ganz and E. Nemeth
10 Cite this article as Cold Spring Harb Perspect Med 2012;2:a011668
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
Press on February 15, 2013 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from

Benyamin B, Ferreira MA, Willemsen G, Gordon S, Mid-delberg RP, McEvoy BP, Hottenga JJ, Henders AK, Camp-bell MJ, Wallace L, et al. 2009a. Common variantsin TMPRSS6 are associated with iron status and erythro-cyte volume. Nat Genet 41: 1173–1175.
Benyamin B, McRae AF, Zhu G, Gordon S, Henders AK,Palotie A, Peltonen L, Martin NG, Montgomery GW,Whitfield JB, et al. 2009b. Variants in TF and HFE explainapproximately 40% of genetic variation in serum-trans-ferrin levels. Am J Hum Genet 84: 60–65.
Breuer W, Ronson A, Slotki IN, Abramov A, Hershko C,Cabantchik ZI. 2000. The assessment of serum nontrans-ferrin-bound iron in chelation therapy and iron supple-mentation. Blood 95: 2975–2982.
Brittenham GM. 2011. Iron-chelating therapy for transfu-sional iron overload. N Engl J Med 364: 146–156.
Bullock GC, Delehanty LL, Talbot AL, Gonias SL, Tong WH,Rouault TA, Dewar B, Macdonald JM, Chruma JJ, Gold-farb AN. 2010. Iron control of erythroid development bya novel aconitase-associated regulatory pathway. Blood116: 97–108.
Casanovas G, Swinkels DW, Altamura S, Schwarz K, Laa-rakkers CM, Gross HJ, Wiesneth M, Heimpel H, Muck-enthaler MU. 2011. Growth differentiation factor 15in patients with congenital dyserythropoietic anaemia(CDA) type II. J Mol Med 89: 811–816.
Casey JL, Hentze MW, Koeller DM, Caughman SW, RouaultTA, Klausner RD, Harford JB. 1988. Iron-responsive ele-ments: Regulatory RNA sequences that control mRNAlevels and translation. Science 240: 924–928.
Chambers JC, Zhang W, Li Y, Sehmi J, Wass MN, Zabaneh D,Hoggart C, Bayele H, McCarthy MI, Peltonen L, et al.2009. Genome-wide association study identifies variantsin TMPRSS6 associated with hemoglobin levels. Nat Ge-net 41: 1170–1172.
Chen JJ. 2007. Regulation of protein synthesis by the heme-regulated eIF2a kinase: Relevance to anemias. Blood 109:2693–2699.
Chen W, Dailey HA, Paw BH. 2010. Ferrochelatase forms anoligomeric complex with mitoferrin-1 and Abcb10 forerythroid heme biosynthesis. Blood 116: 628–630.
Corradini E, Meynard D, Wu Q, Chen S, Ventura P, Pietran-gelo A, Babitt JK. 2011. Serum and liver iron differentlyregulate the bone morphogenetic protein 6 (BMP6)-SMAD signaling pathway in mice. Hepatology 54: 273–284.
Cunningham MJ. 2008. Update on thalassemia: Clinicalcare and complications. Pediatr Clin North Am 55: 447–460.
Du X, She E, Gelbart T, Truksa J, Lee P, Xia Y, Khovananth K,Mudd S, Mann N, Moresco EM, et al. 2008. The serineprotease TMPRSS6 is required to sense iron deficiency.Science 320: 1088–1092.
Fernandes A, Preza GC, Phung Y, De Domenico I, Kaplan J,Ganz T, Nemeth E. 2009. The molecular basis of hepci-din-resistant hereditary hemochromatosis. Blood 114:437–443.
Finberg KE, Heeney MM, Campagna DR, Aydinok Y, Pear-son HA, Hartman KR, Mayo MM, Samuel SM, Strouse JJ,Markianos K, et al. 2008. Mutations in TMPRSS6 causeiron-refractory iron deficiency anemia (IRIDA). Nat Ge-net 40: 569–571.
Finch C. 1994. Regulators of iron balance in humans. Blood84: 1697–1702.
Ganz T, Olbina G, Girelli D, Nemeth E, Westerman M. 2008.Immunoassay for human serum hepcidin. Blood 112:4292–4297.
Gardenghi S, Grady RW, Rivella S. 2010a. Anemia, ineffec-tive erythropoiesis, and hepcidin: Interacting factors inabnormal iron metabolism leading to iron overload inbeta-thalassemia. Hematol Oncol Clin North Am 24:1089–1107.
Gardenghi S, Ramos P, Marongiu MF, Melchiori L, Breda L,Guy E, Muirhead K, Rao N, Roy CN, Andrews NC, et al.2010b. Hepcidin as a therapeutic tool to limit iron over-load and improve anemia in b-thalassemic mice. J ClinInvest 120: 4466–4477.
Kearney SL, Nemeth E, Neufeld EJ, Thapa D, Ganz T, Wein-stein DA, Cunningham MJ. 2007. Urinary hepcidin incongenital chronic anemias. Pediatr Blood Cancer 48:57–63.
Kroot JJ, Laarakkers CM, Kemna EH, Biemond BJ, SwinkelsDW. 2009. Regulation of serum hepcidin levels in sicklecell disease. Haematologica 94: 885–887.
Lee DH, Zhou LJ, Zhou Z, Xie JX, Jung JU, Liu Y, Xi CX,Mei L, Xiong WC. 2010. Neogenin inhibits HJV secre-tion and regulates BMP-induced hepcidin expressionand iron homeostasis. Blood 115: 3136–3145.
Li H, Rybicki AC, Suzuka SM, von BL, Breuer W, Hall CB,Cabantchik ZI, Bouhassira EE, Fabry ME, Ginzburg YZ.2010. Transferrin therapy ameliorates disease in b-thal-assemic mice. Nat Med 16: 177–182.
Liu S, Bhattacharya S, Han A, Suragani RN, Zhao W, Fry RC,Chen JJ. 2008. Haem-regulated eIF2a kinase is necessaryfor adaptive gene expression in erythroid precursors un-der the stress of iron deficiency. Br J Haematol 143:129–137.
Maes K, Nemeth E, Roodman GD, Huston A, Esteve F,Freytes C, Callander N, Katodritou E, Tussing-Hum-phreys L, Rivera S, et al. 2010. In anemia of multiplemyeloma, hepcidin is induced by increased bone mor-phogenetic protein 2. Blood 116: 3635–3644.
Mastrogiannaki M, Matak P, Keith B, Simon MC, Vaulont S,Peyssonnaux C. 2009. HIF-2a, but not HIF-1a, promotesiron absorption in mice. J Clin Invest 119: 1159–1166.
Mastrogiannaki M, Matak P, Mathieu JR, Delga S, Mayeux P,Vaulont S, Peyssonnaux C. 2011. Hepatic HIF-2 down-regulates hepcidin expression in mice through epo-me-diated increase in erythropoiesis. Haematologica doi:10.3324/haematol.2011.056119.
McLaren CE, Barton JC, Gordeuk VR, Wu L, Adams PC,Reboussin DM, Speechley M, Chang H, Acton RT, HarrisEL, et al. 2007. Determinants and characteristics of meancorpuscular volume and hemoglobin concentration inwhite HFE C282Y homozygotes in the hemochromatosisand iron overload screening study. Am J Hematol 82:898–905.
Meynard D, Kautz L, Darnaud V, Canonne-Hergaux F, Cop-pin H, Roth MP. 2009. Lack of the bone morphogeneticprotein BMP6 induces massive iron overload. Nat Genet41: 478–481.
� Miller JL. 2012. Iron deficiency anemia: A common andcurable disease. Cold Spring Harb Perspect Med doi:10.1101/cshperspect.a011866.
Iron Metabolism
Cite this article as Cold Spring Harb Perspect Med 2012;2:a011668 11
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
Press on February 15, 2013 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from

Nandal A, Ruiz JC, Subramanian P, Ghimire-Rijal S, Sinna-mon RA, Stemmler TL, Bruick RK, Philpott CC. 2011.Activation of the HIF prolyl hydroxylase by the ironchaperones PCBP1 and PCBP2. Cell Metab 14: 647–657.
Nemeth E, Valore EV, Territo M, Schiller G, Lichtenstein A,Ganz T. 2003. Hepcidin, a putative mediator of anemia ofinflammation, is a type II acute-phase protein. Blood 101:2461–2463.
Nemeth E, Rivera S, Gabayan V, Keller C, Taudorf S, Peder-sen BK, Ganz T. 2004. IL-6 mediates hypoferremia ofinflammation by inducing the synthesis of the iron reg-ulatory hormone hepcidin. J Clin Invest 113: 1271–1276.
Nicolas G, Bennoun M, Devaux I, Beaumont C, Grand-champ B, Kahn A, Vaulont S. 2001. Lack of hepcidingene expression and severe tissue iron overload in up-stream stimulatory factor 2 (USF2) knockout mice.Proc Natl Acad Sci 98: 8780–8785.
Nicolas G, Chauvet C, Viatte L, Danan JL, Bigard X, DevauxI, Beaumont C, Kahn A, Vaulont S. 2002. The gene en-coding the iron regulatory peptide hepcidin is regulatedby anemia, hypoxia, and inflammation. J Clin Invest 110:1037–1044.
Ohgami RS, Campagna DR, McDonald A, Fleming MD.2006. The Steap proteins are metalloreductases. Blood108: 1388–1394.
Origa R, Galanello R, Ganz T, Giagu N, Maccioni L, Faa G,Nemeth E. 2007. Liver iron concentrations and urinaryhepcidin in b-thalassemia. Haematologica 92: 583–588.
Pak M, Lopez MA, Gabayan V, Ganz T, Rivera S. 2006. Sup-pression of hepcidin during anemia requires erythropoi-etic activity. Blood 108: 3730–3735.
Papanikolaou G, Samuels ME, Ludwig EH, MacDonald ML,Franchini PL, Dube MP, Andres L, MacFarlane J, Sakel-laropoulos N, Politou M, et al. 2004. Mutations in HFE2cause iron overload in chromosome 1q-linked juvenilehemochromatosis. Nat Genet 36: 77–82.
Papanikolaou G, Tzilianos M, Christakis JI, Bogdanos D,Tsimirika K, MacFarlane J, Goldberg YP, SakellaropoulosN, Ganz T, Nemeth E. 2005. Hepcidin in iron overloaddisorders. Blood 105: 4103–4105.
Paradkar PN, Zumbrennen KB, Paw BH, Ward DM, KaplanJ. 2009. Regulation of mitochondrial iron importthrough differential turnover of mitoferrin 1 and mito-ferrin 2. Mol Cell Biol 29: 1007–1016.
Pietrangelo A, Dierssen U, Valli L, Garuti C, Rump A, Cor-radini E, Ernst M, Klein C, Trautwein C. 2007. STAT3 isrequired for IL-6-gp130-dependent activation of hepci-din in vivo. Gastroenterology 132: 294–300.
Pietrangelo A, Caleffi A, Corradini E. 2011. Non-HFE he-patic iron overload. Semin Liver Dis 31: 302–318.
Pigeon C, Ilyin G, Courselaud B, Leroyer P, Turlin B, BrissotP, Loreal O. 2001. A new mouse liver-specific gene, en-coding a protein homologous to human antimicrobialpeptide hepcidin, is overexpressed during iron overload.J Biol Chem 276: 7811–7819.
Porter JB. 2009. Pathophysiology of transfusional iron over-load: Contrasting patterns in thalassemia major andsickle cell disease. Hemoglobin 33: S37–S45.
Poss KD, Tonegawa S. 1997. Heme oxygenase 1 is requiredfor mammalian iron reutilization. Proc Natl Acad Sci 94:10919–10924.
Ramos E, Kautz L, Rodriguez R, Hansen M, Gabayan V,Ginzburg Y, Roth MP, Nemeth E, Ganz T. 2011. Evidencefor distinct pathways of hepcidin regulation by acute andchronic iron loading in mice. Hepatology 53: 1333–1341.
Salahudeen AA, Thompson JW, Ruiz JC, Ma HW, Kinch LN,Li Q, Grishin NV, Bruick NK. 2009. An E3 ligase possess-ing an iron-responsive hemerythrin domain is a regulatorof iron homeostasis. Science 326: 722–726.
Sanchez M, Galy B, Schwanhaeusser B, Blake J, Bahr-Iva-cevic T, Benes V, Selbach M, Muckenthaler MU, HentzeMW. 2011. Iron regulatory protein-1 and -2: Transcrip-tome-wide definition of binding mRNAs and shaping ofthe cellular proteome by iron regulatory proteins. Blood118: e168–e179.
Sham RL, Phatak PD, Nemeth E, Ganz T. 2009. Hereditaryhemochromatosis due to resistance to hepcidin: Highhepcidin concentrations in a family with C326S ferropor-tin mutation. Blood 114: 493–494.
Sheftel AD, Zhang AS, Brown C, Shirihai OS, Ponka P. 2007.Direct interorganellar transfer of iron from endosome tomitochondrion. Blood 110: 125–132.
Shi H, Bencze KZ, Stemmler TL, Philpott CC. 2008. A cy-tosolic iron chaperone that delivers iron to ferritin. Sci-ence 320: 1207–1210.
Silvestri L, Pagani A, Nai A, De Domenico I, Kaplan J, Ca-maschella C. 2008. The serine protease matriptase-2(TMPRSS6) inhibits hepcidin activation by cleavingmembrane hemojuvelin. Cell Metab 8: 502511.
Soe-Lin S, Apte SS, Andriopoulos B Jr, Andrews MC,Schranzhofer M, Kahawita T, Garcia-Santos D, Ponka P.2009. Nramp1 promotes efficient macrophage recyclingof iron following erythrophagocytosis in vivo. Proc NatlAcad Sci 106: 5960–5965.
Talbot AL, Bullock GC, Delehanty LL, Sattler M, Zhao ZJ,Goldfarb AN. 2011. Aconitase regulation of erythropoi-esis correlates with a novel licensing function in erythro-poietin-induced ERK signaling. PLoS ONE 6: e23850.
Tanaka T, Roy CN, Yao W, Matteini A, Semba RD, Arking D,Walston JD, Fried LP, Singleton A, Guralnik J, et al. 2010.A genome-wide association analysis of serum iron con-centrations. Blood 115: 94–96.
Tanno T, Bhanu NV, Oneal PA, Goh SH, Staker P, Lee YT,Moroney JW, Reed CH, Luban NL, Wang RH, et al. 2007.High levels of GDF15 in thalassemia suppress expressionof the iron regulatory protein hepcidin. Nat Med 13:1096–1101.
Tanno T, Porayette P, Sripichai O, Noh SJ, Byrnes C, Bhupa-tiraju A, Lee YT, Goodnough JB, Harandi O, Ganz T, et al.2009. Identification of TWSG1 as a second novel ery-throid regulator of hepcidin expression in murine andhuman cells. Blood 114: 181–186.
Telfer P. 2009. Update on survival in thalassemia major.Hemoglobin 33: S76–S80.
Troadec MB, Warner D, Wallace J, Thomas K, Spangrude GJ,Phillips J, Khalimonchuk O, Paw BH, Ward DM, KaplanJ. 2011. Targeted deletion of the mouse Mitoferrin1 gene:From anemia to protoporphyria. Blood 117: 5494–5502.
Vashisht AA, Zumbrennen KB, Huang X, Powers DN, Du-razo A, Sun D, Bhaskaran N, Persson A, Uhlen M, Sang-felt O, et al. 2009. Control of iron homeostasis by an iron-regulated ubiquitin ligase. Science 326: 718–721.
T. Ganz and E. Nemeth
12 Cite this article as Cold Spring Harb Perspect Med 2012;2:a011668
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
Press on February 15, 2013 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from

Verga Falzacappa MV, Vujic SM, Kessler R, Stolte J, HentzeMW, Muckenthaler MU. 2007. STAT3 mediates hepatichepcidin expression and its inflammatory stimulation.Blood 109: 353–358.
Verga Falzacappa MV, Casanovas G, Hentze MW, Muck-enthaler MU. 2008. A bone morphogenetic protein(BMP)-responsive element in the hepcidin promotercontrols HFE2-mediated hepatic hepcidin expressionand its response to IL-6 in cultured cells. J Mol Med 86:531–540.
Vokurka M, Krijt J, Sulc K, Necas E. 2006. Hepcidin mRNAlevels in mouse liver respond to inhibition of erythropoi-esis. Physiol Res 55: 667–674.
Wallace DF, Summerville L, Crampton EM, Frazer DM, An-derson GJ, Subramaniam VN. 2009. Combined deletionof Hfe and transferrin receptor 2 in mice leads to markeddysregulation of hepcidin and iron overload. Hepatology50: 1992–2000.
Wrighting DM, Andrews NC. 2006. Interleukin-6 induceshepcidin expression through STAT3. Blood 108: 3204–3209.
Zhang DL, Hughes RM, Ollivierre-Wilson H, Ghosh MC,Rouault TA. 2009. A ferroportin transcript that lacks aniron-responsive element enables duodenal and erythroidprecursor cells to evade translational repression. CellMetab 9: 461–473.
Iron Metabolism
Cite this article as Cold Spring Harb Perspect Med 2012;2:a011668 13
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
Press on February 15, 2013 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from