Iposodiemia: diagnosi e trattamento -...
51
Iposodiemia: diagnosi e trattamento Enrico Fiaccadori Unita’ di Fisiopatologia dell’Insufficienza Renale Acuta e Cronica Dipartimento di Medicina Clinica e Sperimentale Universita’ degli Studi di Parma
Transcript of Iposodiemia: diagnosi e trattamento -...

Iposodiemia: diagnosi e trattamento
Enrico Fiaccadori Unita’ di Fisiopatologia dell’Insufficienza Renale Acuta e Cronica
Dipartimento di Medicina Clinica e Sperimentale
Universita’ degli Studi di Parma

Hyponatremia
• Epidemiology and outcome
• Pathophysiology as the basis for diagnosis and treatment
• The role of pharmacologic and non pharmacologic treatment

Hyponatremia: a disturbing
clinical problem

Hyponatremia: the most frequent
electrolyte disorder

2014

Making prompt diagnosis, relieving acute CNS-related symptoms (cerebral edema), avoiding the possible harmful effects of the treatment
itself (overcorrection)

The best path to patient’ safety in
when approaching
hyponatremia
Know the pathophysiology

Hyponatremia is mainly a problem of water (relative or absolute excess of water on sodium)

Mechanisms of hyponatremia
a) Loss of sodium (more Na than H2O) b) Gain of water • Excess drinking hypotonic fluids, or
excess parenteral hypotonic fluids and/or • Reduced/inappropriate water excretion

The body response to water load: what is to be expected from physiology
• Urinary output rapidly increases: > 80% of a 20 ml/Kg
water load (15’) should be eliminated in 4 hours
• Urine should be maximally diluted (urinary osmolality low, 50-100 mOsm/L) Uosm/Posm < 1
• No clinically relevant changes in serum sodium levels (venous blood)
• AVP (Antidiuretic hormone) should be totally suppressed water reabsorption in the kidney is reduced

• Is it possible to have hyponatremia only by increasing water (or hypotonic fluid) intake?
• If free water excretion cannot be adequately increased, what are the possible mechanisms?
Pathophysiological questions

Yes, if one is able to drink water at a rate faster than the maximum water excretion capacity of the normal kidney (at least 750 mls/hour or 16 liters/day)
Is it possible to have hyponatremia only by water gain?

Large input of water in patients with hyponatremia
Halperin ML 2010
Psycogenic polydipsia

Yes, if one is able to drink water at a rate faster than the maximum water excretion capacity of the normal kidney (at least 750 mls/hour)
Yes, if there are interfering factors on the kidney
ability to normally excrete a water load • Reduced distal delivery of fluid (limited amount of water
available for excretion): renal failure, volume depletion • AVP activity is not totally suppressed (inappropriate
secretion and/or activity of AVP)
Is it possible to have hyponatremia only by water gain?


There are 4 major mechanisms of
inappropriate secretion of/or activity of AVP
Volume depletion/hypotension,
nausea, pain inflammation, drugs
neoplasia
drugs
Genetic alterations of the ADH receptor

Syndrome of inappropriate secretion of ADH (SIADH): inappropriate for the presence of hypotonicity

Algorhytm for the differential diagnosis of hyponatremia (1)
ERBP Guidelines 2014

Algorhytm for the differential diagnosis of hyponatremia (2)
ERBP Guidelines 2014



What is the best rate for correction of hyponatremia?
No «best» rate can be defined a priori: it depends from the severity of symptoms, the type of
hyponatremia (acute vs chronic), the underlying comorbidities, the accompanying electrolyte disorders

The main problem with therapy in hyponatremia The difficult equilibrium in brain cells between how much
correction is enough and how much is too much
CNS complications of acute
hyponatremia (brain edema)
CNS complications of chronic
hyponatremia therapy (ODS)

Acute hyponatremia is always associated with cell swelling (brain edema)

Chronic hyponatremia
Rapid correction of chronic hyponatremia risk of brain cell dehydration ODS
48 hours

Osmotic Demielynation Syndrome
• Delayed, gradual neurologic deterioration (up to vegetative state, coma and death) appearing one to several days after a rapid correction of chronic hyponatremia
• Clinically defined, since imaging not always positive in the early phases
• Definite diagnosis by CT scan or MR

Hoorn EJ et al., Q J Med 2005; 98:529-540

Sterns RH et al., Am J Kidney Dis 2010; 56:774-779
Simple goals for the treatment of severe chronic hyponatremia

Treatment of acute/symptomatic hyponatremia: practical aspects
• First of all define the target and the rate of correction in mEq/hour for how many hours, then calculate how much of the saline solution available should be infused
• With 3% NaCl: to induce a correction rate of 1 meq/L/h using 3% saline, one should infuse the body weight as millilitres/hour a man with a BW of 70 Kg will increase serum Na by approximately 1 meq/hour when infused with 3% NaCl at a rate of 70 ml/hour
• With NaCl vials (20 mEq/10 ml): to induce a correction rate of 1 meq/L/h using NaCl vials, one should infuse 20 ml/hour (i.e. 40 mEq) in a subject with a BW of 70 Kg and a total body water of 42 L, serum Na will increase by approximately 1 meq/hour
• Potassium: if K is needed (hypokalemia and K depletion), take it into account : if K is co-administered calculate it as sodium
• Avoid fixed algorythms, be careful with formulas

Adrogue HJ, Madias N Engl J Med 2000; 342:1581-89
Are formulas useful for the correction of hyponatremia?

Problems with formulas for hyponatremia correction
• Underestimation of correction in case of volume depletion or if the kidney regains spontaneously its water excretion ability
• Ongoing urinary losses of water, Na and K not considered
• K intake not always considered
Formulas may be useful to set the start of therapy,
but they do not completely avoid
the risk of overcorrection

Hyponatremia correction and the risk for overcorrection
• Is there any risk that spontaneous correction of hyponatremia may increase the planned rate of correction, leading to unanticipated overcorrection?
• How to avoid too rapid spontaneous correction of hyponatremia?

Correcting acute/symptomatic hyponatremia
Na+E + K+
E
Total body water
Add osmoles to the numerator
Serum Na+ =
Subtract water from the denominator
The excretion of 1 L/hour of maximally
diluted urine will increase serum Na by
2-3 mEq/L/hour

«Apart from doctors, the main cause of
overcorrection in hyponatremia
is the kidney itself, if it regains rapidly the ability to excrete water»
The wiseman should reflect carefully, anticipating the possibility that the kidney
may become an overcorrection factor, especially when temporary
causes of hyponatremia are acting
ConfuCius

The critical issue in acute/symptomatic hyponatremia is to anticipate the
possible causes of rapid correction
Causes of temporary
hyponatremia risk for
rapid, unanticipated
correction

Desmopressin and free water administration to slow
an excessively rapid correction of hyponatremia

Hoorn EJ et al., Q J Med 2005; 98:529-540
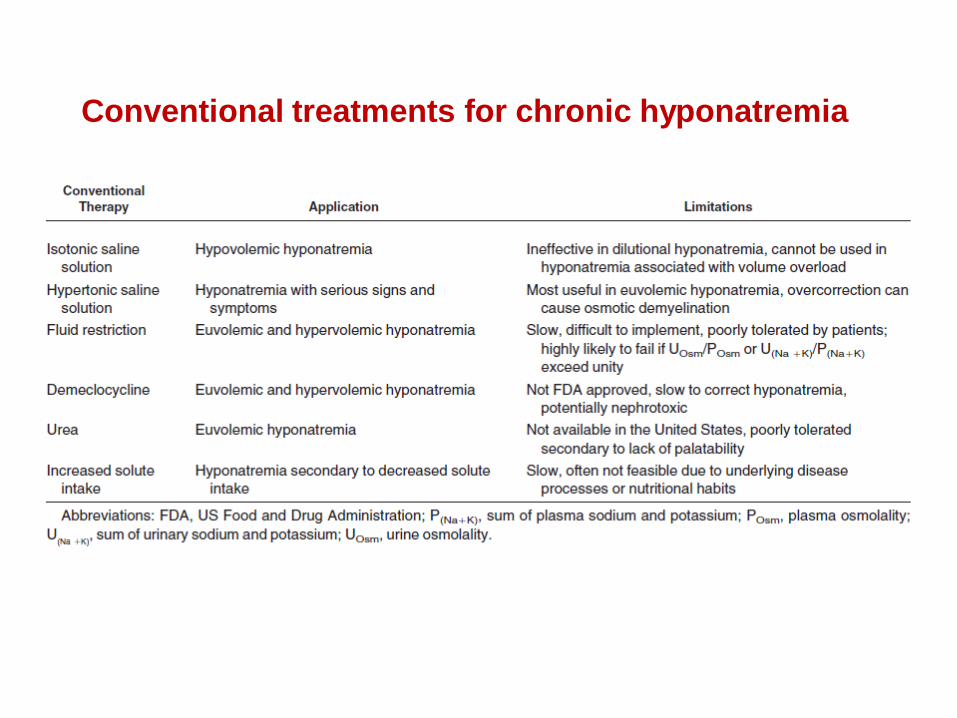
Conventional treatments for chronic hyponatremia

Vaptans are the antagonists of vasopressin receptors
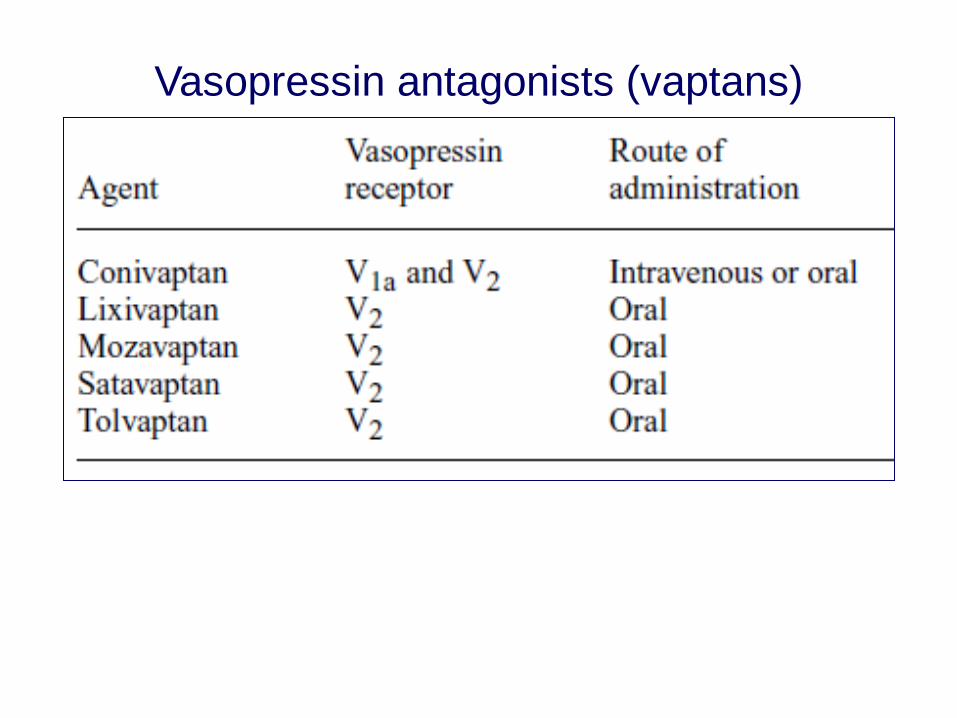
Vasopressin antagonists (vaptans)


Serum sodium (SNa) values during treatment with vaptans
and urea. Each point is the mean value of serum sodium for the 12
patients (mean + SD)
- SNa increased more than 12 mmol/L the first day in 12/35 patients (37%) and in 13 patients the increase in SNa was higher than 18 mol/L/48 hr
- In two of these patients the intensivist lowered the SNa again by
giving desmopressin (DDAVP) and water
- No cases of clinical osmotic demyelination syndrome (ODS) developed




Maximum dose 120 mg/day

Berl T et al., J Am Soc Nephrol 2010; 21:705-712
In hyponatremic patients tolvaptan is highly effective without significantly increasing liver enzymes

Take home messages • In acute symptomatic hyponatremia rapid, partial
increase in serum Na levels to limit cerebral edema
• In chronic symptomatic hyponatremia slow correction to avoid iatrogenic neurologic injury (ODS)
• Take into account the kidney as a cause of unanticipated hypercorrection (look at temporary causes of hyponatremia)
• In-depth knowledge of pathophysiology the base for a safe approach