Investing ahead of the curve
16
Paying it forward to improve access in Vietnam Safeguarding the next generation’s health in Malaysia The challenges of diabetes care in Indonesia TBL Quarterly Q1 2013 Investing ahead of the curve Today’s actions for tomorrow’s health
-
Upload
novo-nordisk-as -
Category
Documents
-
view
230 -
download
3
description
Novo Nordisk TBL Quarterly Q1 2013. The theme of this first issue is ‘Investing ahead of the curve’. We chose this theme to show why and how we - and all partners in diabetes care - must act now if we want to ensure a healthier future, one in which our ability to treat diabetes fits the needs of patients. In it you will find stories from Indonesia, Malaysia and Vietnam that we believe demonstrate the value of long-term business decisions. We hope to inspire and start a conversation about the challenges and the actions we must make now, together, to solve them.
Transcript of Investing ahead of the curve
Paying it forward to improve access in Vietnam
Safeguarding the next generation’s health in Malaysia
The challenges of diabetes care in Indonesia
TBL Quarterly Q1 2013
Investing ahead of the curveToday’s actions for tomorrow’s health
TBL QUARTERLY 2
In those 90 years we have seen a dramatic increase in the number of people with type 2 diabetes. Today, four out of five are living in low- and middle-income countries, many having no or limited access to treatment and care. Year after year, new projections outstrip previous ones, always predicting a future with more and more people living with diabetes. Many of these countries simply cannot keep up to adequately provide the healthcare needed.
Faced with a future in which health outcomes look likely to deteriorate, one in which those living with diabetes and their families will carry the heaviest burden, our TBL principle guides our response. We know that the sustainability of our business is best secured by strengthening access to proper healthcare for those who need it, regardless of where they live or what their circumstances are.
The theme of this first issue is ‘Investing ahead of the curve’. We chose this theme to show why and how we - and all partners in diabetes care - must act now if we want to ensure a healthier future, one in which our ability to treat diabetes fits the needs of patients.
In it you will find stories from Indonesia, Malaysia and Vietnam that we believe demonstrate the value of long-term business decisions. We hope to inspire and start a conversation about the challenges and the actions we must make now, together, to solve them.
Lise KingoExecutive Vice President and Chief of StaffsNovo Nordisk
I am pleased to introduce to you the first issue of Novo Nordisk’s quarterly sustainability publication – the TBL Quarterly.
It is a publication about who we are as a company and how we do business.
Who we are is the outcome of thousands of decisions made by colleagues across our global organisation. But it is how these decisions are made that determine whether we will be successful. And more importantly, successful for the long term.
At Novo Nordisk, we believe that long-term business success is supported by decisions that take into account three considerations: will the actions taken be financially, socially and environmentally responsible? It’s what we call the Triple Bottom Line business principle, or TBL, as the 34,700 Novo Nordisk employees have come to call it. Novo Nordisk has had a long history of working systematically and proactively to balance the needs of patients with our responsibility as a business. So, although this quarterly publication is new, our TBL business principle is not.
For 90 years, Novo Nordisk has been in the business of treating diabetes. It started with Danish Nobel laureate August Krogh and his wife, Marie’s visit to the United States in 1922. Marie was a doctor and had diabetes. She learnt of the discovery of insulin made by a team of scientists in Canada, led by Frederick Banting and Charles Best and convinced August to travel to Canada and seek permission to produce insulin in Denmark. This decision led to the first patients being treated with insulin produced in Denmark in 1923. The rest, you can say, is history.
Sustainabilityis about looking ahead
TBL QUARTERLY 3
The challenges of diabetes care in Indonesia
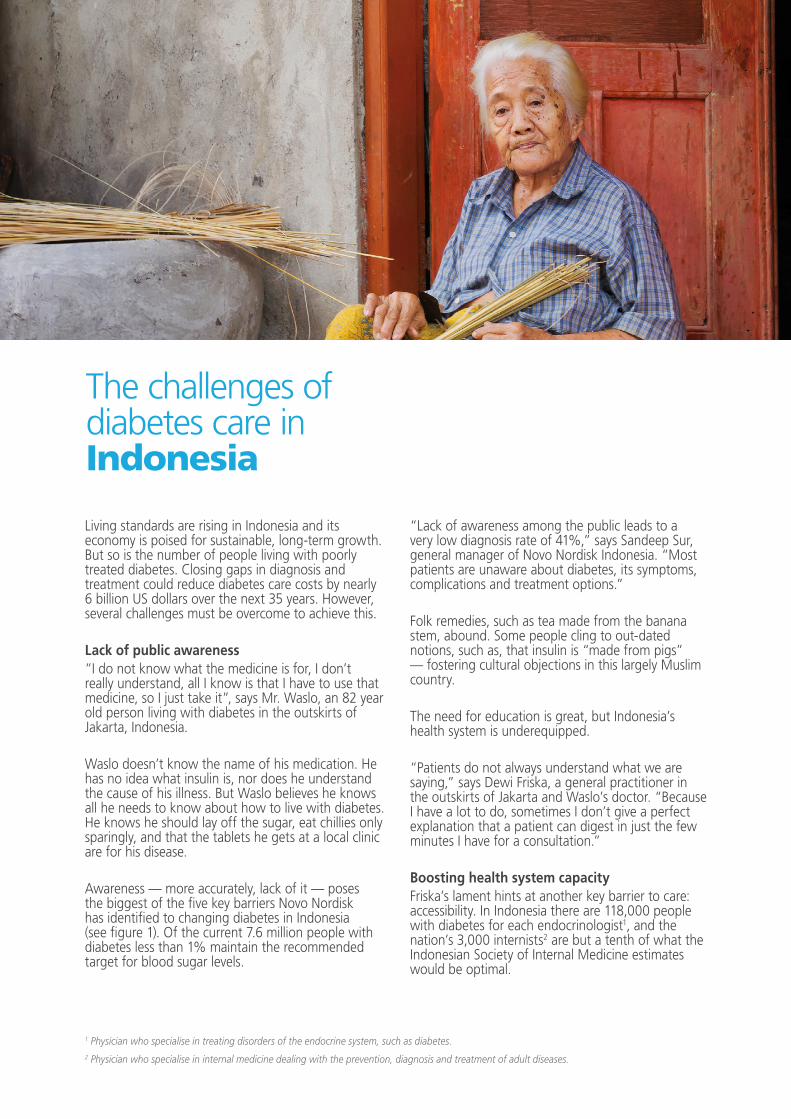
Living standards are rising in Indonesia and its economy is poised for sustainable, long-term growth. But so is the number of people living with poorly treated diabetes. Closing gaps in diagnosis and treatment could reduce diabetes care costs by nearly 6 billion US dollars over the next 35 years. However, several challenges must be overcome to achieve this.
Lack of public awareness “I do not know what the medicine is for, I don’t really understand, all I know is that I have to use that medicine, so I just take it”, says Mr. Waslo, an 82 year old person living with diabetes in the outskirts of Jakarta, Indonesia.
Waslo doesn’t know the name of his medication. He has no idea what insulin is, nor does he understand the cause of his illness. But Waslo believes he knows all he needs to know about how to live with diabetes. He knows he should lay off the sugar, eat chillies only sparingly, and that the tablets he gets at a local clinic are for his disease.
Awareness — more accurately, lack of it — poses the biggest of the five key barriers Novo Nordisk has identified to changing diabetes in Indonesia (see figure 1). Of the current 7.6 million people with diabetes less than 1% maintain the recommended target for blood sugar levels.
“Lack of awareness among the public leads to a very low diagnosis rate of 41%,” says Sandeep Sur, general manager of Novo Nordisk Indonesia. “Most patients are unaware about diabetes, its symptoms, complications and treatment options.”
Folk remedies, such as tea made from the banana stem, abound. Some people cling to out-dated notions, such as, that insulin is “made from pigs” — fostering cultural objections in this largely Muslim country.
The need for education is great, but Indonesia’s health system is underequipped.
“Patients do not always understand what we are saying,” says Dewi Friska, a general practitioner in the outskirts of Jakarta and Waslo’s doctor. “Because I have a lot to do, sometimes I don’t give a perfect explanation that a patient can digest in just the few minutes I have for a consultation.”
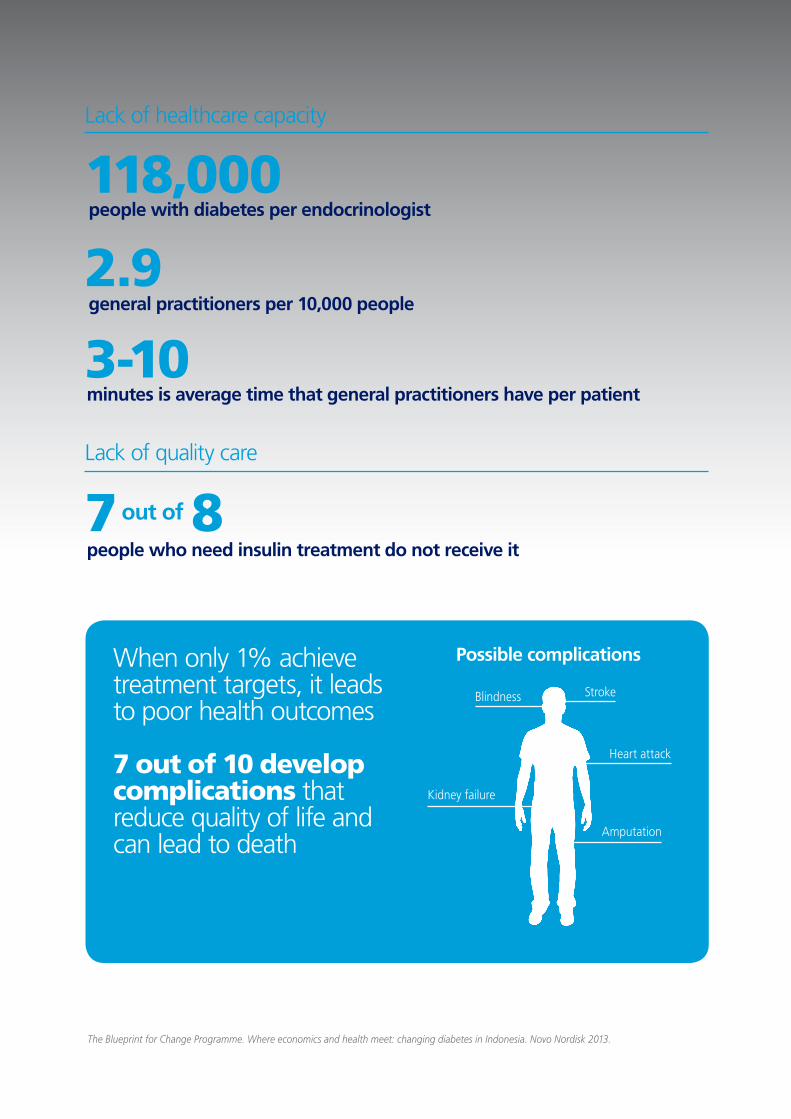
Boosting health system capacityFriska’s lament hints at another key barrier to care: accessibility. In Indonesia there are 118,000 people with diabetes for each endocrinologist1, and the nation’s 3,000 internists2 are but a tenth of what the Indonesian Society of Internal Medicine estimates would be optimal.
1 Physician who specialise in treating disorders of the endocrine system, such as diabetes.2 Physician who specialise in internal medicine dealing with the prevention, diagnosis and treatment of adult diseases.

TBL QUARTERLY 4
General practitioners like Friska could be a resource for relieving this burden. But with just 2.9 for every 10,000 people in Indonesia, overwhelmed general practitioners typically spend only 3 to 10 minutes with a patient. Moreover, the average general practitioner receives two hours of diabetes education during medical training. Relatively few are comfortable prescribing insulin and instructing patients to use it.
A training programme with a holistic focus on medication, nutrition and exercise, has been closing this gap in supply and demand. Since 2010, the INSPIRE programme (an educational programme developed by Steno Diabetes Center and the Indonesian Society of Endocrinology) has provided more than 1,200 internists with know-how to manage diabetes more effectively. Now, the Indonesian Society of Endocrinology, the Steno Diabetes Center and Novo Nordisk have already strengthened INSPIRE and expanded its reach to general practitioners.
By increasing the scope of INSPIRE, general practitioners will be added to the skill base of medical professionals able to diagnose and treat diabetes complications.
Cultivating relationshipsINSPIRE is an example of how eliminating barriers to care requires strong relationships among partners with complementary strengths. “No one player can lift this major and growing burden of diabetes in Indonesia alone,” says Sandeep Sur.
Take the barrier of availability, which is scarce in rural areas. In Ternate, a World Diabetes Foundation project has established a diabetes care centre with a physician, provided education and training, and purchased supplies. In its first two years, the clinic served 371 people.
Figure 1. Five barriers to improve diabetes care in Indonesia
Such cross-sector involvement is at the core of the Ministry of Health’s National Diabetes Plan. Since 2012, Novo Nordisk, together with industry peers, has worked with the Ministry of Health to support and make actionable the Ministry’s diabetes plan. Keeping the National Diabetes Plan’s goals a national priority is also an important element to mitigate the affordability barrier as Indonesia implements universal health coverage in 2014.
There’s a long way to go, but continued investments and partnerships can minimise quality-of-care barriers for millions of people living with diabetes like Waslo. It all starts with creating awareness.
“Education is the most important thing in my country,” says Roy Sibarani, an endocrinologist at RS Pantai Indah Kapuk hospital. “It is cheap compared to the money we spend on curing.”
Want to know more?Read how Novo Nordisk addresses the challenges of diabetes care in Indonesia in the Blueprint for Change Programme’s most recent publication

TBL QUARTERLY 5
7.6 million people in Indonesia have diabetes but only 1% achieve treatment targets. Here are some of the reasons why:
Lack of awareness
Diabetes can be cured by drinking banana stem tea
Misbeliefs about diabetes
Eating live insects will help your diabetes
Insulin is made from pigs
The barriers to carein Indonesia
are unaware that they have diabetes
59%
In rural areas, undiagnosed diabetets may be as high as 70%
TBL QUARTERLY 6
Lack of healthcare capacity
people with diabetes per endocrinologist
general practitioners per 10,000 people
minutes is average time that general practitioners have per patient
Lack of quality care
When only 1% achieve treatment targets, it leads to poor health outcomes
7 out of 10 develop complications that reduce quality of life and can lead to death
Possible complications
Stroke
Kidney failure
Blindness
Heart attack
Amputation
The Blueprint for Change Programme. Where economics and health meet: changing diabetes in Indonesia. Novo Nordisk 2013.
118,000
2.9
3-10
7 8people who need insulin treatment do not receive it
out of

TBL QUARTERLY 7
Safeguarding the next generation’s health
Imagine preventing diabetes in the next generation. It might look something like this:
At a local health clinic in a bustling Kuala Lumpur suburb, a young Malaysian couple is waiting for their appointment. The walls of the clinic are adorned with posters that show how disease prevention takes place in the growing embryo. Nutrition guides are stacked neatly on the tables.
The couple is waiting to begin a new programme that will reduce their child’s risk of diabetes, heart disease and some forms of cancer. A nurse calls out the couple’s name and they follow her into one of the clinics rooms.
Though the woman is not pregnant, in fact the couple doesn’t plan on starting a family until the following year, they are taking the first step to preventing diabetes in their future son or daughter.
With the global rise of type 2 diabetes, and Malaysia is no exception, a new approach to diabetes prevention is about to turn imagination into reality.
And it couldn’t come at a more needed time.
The flipside of developmentOver the past 50 years, Malaysia has had one of the best economic records in Asia. Gross domestic
product, an indicator of a country’s standard of living, has been growing on average at 6.5%. Poverty rates have decreased and both infant and maternal mortality rates have fallen dramatically. But with Malaysia’s success has come a steady rise in type 2 diabetes.
In a 2012 survey conducted by the Malaysian Ministry of Health, an estimated 2.6 million people over 18 have been diagnosed with diabetes in Malaysia. That’s 15.2% of the adult population. With approximately 30% of the population being overweight, current projections predict a future that does not look very bright. By 2020, the number of people living with diabetes will reach 4.3 million. By 2030, the costs associated with diabetes will increase by 60%.
If Malaysia is to stay on its current economic growth, the foundation for a very different future must be built.
A team of researchers, the Malaysian Ministry of Health and Novo Nordisk believe that the corner stone for this foundation is found in an emerging field of science – the Developmental Origins of Health and Disease.
Getting a head start on diabetesIn very simple terms, the Developmental Origins of Health and Disease argues that the risk of developing
TBL QUARTERLY 7
TBL QUARTERLY 8
diabetes and other chronic diseases is set-up early in life, primarily during pregnancy. More than two decades of research support the argument.
Two studies from researchers at Harvard Medical School have shown that there is a strong correlation between a mother’s weight gain during pregnancy and the increased risk that her child would be overweight or obese.
But according to University of Southampton Professor Mark Hanson, the influence goes even further back.
“A women’s health status prior to pregnancy is a major contributing factor to diabetes risk transfer from generation to generation,” Hanson says. “If we want to make a real difference in preventing diabetes, pre-conception health is when we have the biggest opportunity.”
Evidence for this is not easy to gather without waiting decades for the child to enter adulthood. But researchers have found a solution. They have compared children born to obese mothers with their siblings born after the mother underwent a successful antiobesity surgery. Both children have the same genes and the same family dietary habits, but the second child experienced a very different environment in the womb. In a 2006 study published in the journal Pediatrics, researchers found that the children born to mothers postsurgery were 52% less likely to be obese than siblings born to the same mother when she was still heavy.
Healthy lifestyle change also proves to be effective. A 2012 study from the American Journal of Clinical Nutrition showed that women who had healthy dietary patterns prior to pregnancy had less risk of developing gestational diabetes1.
“But even with solid evidence, making lifestyle changes that lead to improved physical health is no easy task,” says Hanson.
In a December 2012 paper published in the open access, peer-reviewed journal, BMC Public Health, Hanson and co-authors write that interventions aimed at weight loss in adults to prevent excessive weight gain during pregnancy have had limited success. This holds true in developed countries and even more so in developing societies like Malaysia.
“Many activities have been done to increase the health literacy and awareness about diabetes. In spite of this, the number of people living with diabetes in Malaysia is increasing rapidly. What we need is a new hope to reduce the prevalence of diabetes in the long term,” says Henrik Bendix Dahl, general manager, Novo Nordisk Malaysia.
Dahl is hopeful that a new programme in Malaysia offers a unique and innovative approach to preventing diabetes. The programme has been given the name - Jom Mama – which translates directly from Malay as ‘Come on Mama!’.
What is driving health?Since June 2012, a private-public partnership between Novo Nordisk, the Malaysian Ministry of Health, Steno Diabetes Center, the University of Southampton UK and the University of Witwatersrand Johannesburg has been working to achieve consensus on the key issues facing young couples in Malaysia.
Priya Matzen, director of social innovation projects at Novo Nordisk, remembers being daunted by the task that lay before her and her team during the consensus workshops.
“If Malaysia is to stay on its current economic growth, the foundation for a very different future must be built.”
1 A condition in which women exhibit glucose intolerance of variable degree with onset or first recognition during pregnancy.
TBL QUARTERLY 9
“We knew that translating the developmental origins science into a concrete programme was the best route to prevention. But encouraging young couples to make healthier choices is an enormous challenge. We all favour today’s efforts over tomorrow’s rewards – i.e. we tend to underrate future benefits relative to current comfort,” says Matzen.
According to Matzen, community involvement and listening to young couples was the key to shrinking the challenge. Since the start of 2013, Matzen and her team have been convening both community leaders and healthcare professionals in a series of workshops to build consensus on life and health priorities of young couples in Malaysia. The team has employed a unique approach to stakeholder engagement - the Delphi technique. The technique is a systematic and interactive research method to derive consensus amongst a group of individuals.
By the end of the fourth workshop, the 33 member group achieved consensus on four main challenges young couples face in their daily lives. These challenges were an important identifier of the influential drivers of health.
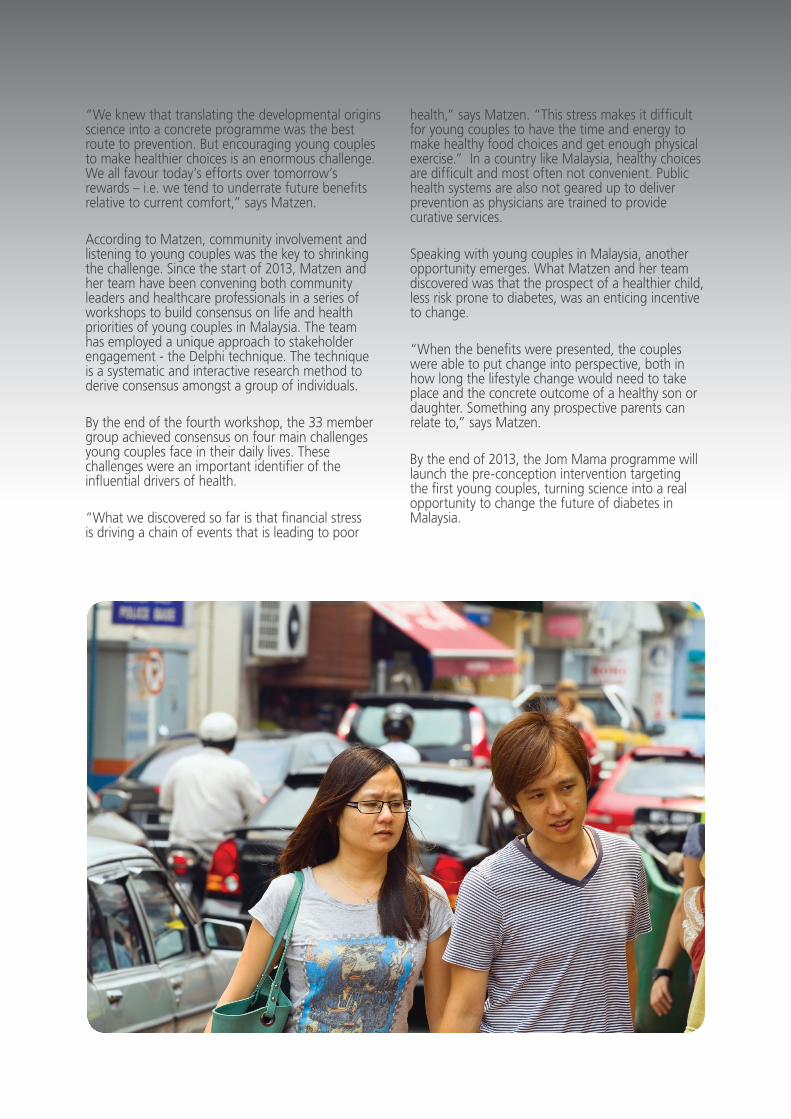
“What we discovered so far is that financial stress is driving a chain of events that is leading to poor
health,” says Matzen. “This stress makes it difficult for young couples to have the time and energy to make healthy food choices and get enough physical exercise.” In a country like Malaysia, healthy choices are difficult and most often not convenient. Public health systems are also not geared up to deliver prevention as physicians are trained to provide curative services.
Speaking with young couples in Malaysia, another opportunity emerges. What Matzen and her team discovered was that the prospect of a healthier child, less risk prone to diabetes, was an enticing incentive to change.
“When the benefits were presented, the couples were able to put change into perspective, both in how long the lifestyle change would need to take place and the concrete outcome of a healthy son or daughter. Something any prospective parents can relate to,” says Matzen.
By the end of 2013, the Jom Mama programme will launch the pre-conception intervention targeting the first young couples, turning science into a real opportunity to change the future of diabetes in Malaysia.
TBL QUARTERLY 10
Paying it forward to improve access in Vietnam
In November 2012, Novo Nordisk opened a new office in Ho Chi Minh City. In partnership with the Vietnamese Ministry of Health, the company launched the Vietnam Diabetes Care Program to tackle some of the main challenges of diabetes in Vietnam such as the limited number of physicians trained in diabetes care, the large number of undiagnosed patients and the limited diabetes care infrastructure. One of the key actions is taking place in collaboration with Steno Diabetes Center to run diabetes education programmes over the next three years.
Jane Rohde Voigt, Education Development at Steno Diabetes Center, recently returned from a trip to Vietnam.
“I was particularly surprised to see the high number of patients with foot ulcers – a diabetes-related complication which is often treated at a late stage in Vietnam. It is within timely management of diabetes and complication screening and treatment that we can make a difference to patients with our education programme,” says Voigt.
Together with Ulla Bjerre-Christensen, Head of Steno Education Center, Voigt has been engaging
with local partners in Vietnam to develop a Train-the-Trainer education programme. The programme’s goal is to provide better care for diabetes patients by training more healthcare professionals. The trip to Vietnam was an important step in getting a clearer picture of the local challenges and needs.
The need for better and earlier treatmentVietnam is experiencing a rapid rise in the prevalence of diabetes. It is estimated that there are close to 5 million people with diabetes in Vietnam1. In many cases, diagnosed patients are treated sub-optimally and the majority of patients fail to achieve recommended treatment targets. But most troubling is the more than 60% that remain undiagnosed, a contributing factor to why close to 6 out of 10 people with diabetes in Vietnam have some form of complications2. One such complication is foot ulcers which ultimately can lead to amputations.
These estimates suggest critical challenges ahead. Delays in diagnosis and treatment deficiencies ultimately make diabetes-related complications more likely and will inevitably increase healthcare costs. But it is the individual and their family that are the hardest hit. Untreated diabetes can reduce a
1 Diabetes Attacking the Very Young in Vietnam. Available from: http://news.newamericamedia.org/news/view_article.html?article_id=ac20ba715ac9eaa42fec5045e45937a8 (accessed 24 April 2013). 2 Yokokawa et al. International Electronic Journal of Health Education, 2010; 13:1-13.3 International Diabetes Federation. A Call to Action on Diabetes. 2010. Available from: http://www.idf.org/webdata/Call-to-Action-on-Diabetes.pdf (accessed 24 April 2013).
TBL QUARTERLY 11
household’s income, contribute to poor educational performance and worsen quality of life3. A crucial first step in addressing the diabetes burden in Vietnam is to increase the number of general practitioners trained in diabetes care. This is where the Train-the-Trainer concept enters the scene.
“Novo Nordisk’s insulins have been helping thousands of patients across Vietnam since 1992. Being the world leader in diabetes care, we need to further support the Ministry of Health in Vietnam and doctors in the fight against the diabetes pandemic in Vietnam,” says Jayagovindan Thyagarajan, general manager, Novo Nordisk Vietnam.
Spreading knowledge like ripples in the waterThe Train-the-Trainer concept aims to increase the knowledge about diabetes among internists4 and general practitioners. It forms part of the public-private partnership known as the Vietnam Diabetes Care Program. Launched in 2012 with a three year action plan, the programme brings together Steno Diabetes Center, Novo Nordisk, the Vietnamese Ministry of Health, the Vietnam Association of Diabetes and Endocrinology and leading hospitals across the country.
The plan is focused on five objectives: increase awareness about diabetes, improve screening for
people at risk, train more physicians on diabetes management, achieve better control among treated patients and improve access to diabetes care including vulnerable populations like pregnant women and children.
To fulfil one of the objectives, Steno Diabetes Center aims to train Vietnamese endocrinologists, specialists in diabetes, and give them the skills to train internists and general practitioners in diabetes care. By building a network of general practitioners educated in diabetes management, Steno aims to improve treatment by giving the skills to the healthcare professionals who are most often the first point of contact for diabetes patients.
“With a large diabetes patient population, but a small number of trained endocrinologists, general practitioner training is considered the cornerstone for future success in reaching out to more people in Vietnam,” says Thyagarajan.
In August 2013, Steno will begin the training of 60 endocrinologists in both Ho Chi Minh City and Hanoi. They will do the same in 2014 and 2015. The endocrinologists will then pass on their newly acquired knowledge to general practitioners in their community. Over three years, the network should grow to 2000 diabetes educated healthcare
4 Physician who specialise in internal medicine dealing with the prevention, diagnosis and treatment of adult diseases.

TBL QUARTERLY 12
professionals. The paying-it-forward approach will create a reach that goes much further than what is possible today. But it does not come without challenges.
“Steno has more than 20 years of experience with diabetes education. However, what is relatively new is how we work with local partners to develop materials intended for training that will be conducted by other professionals than us,” Bjerre-Christensen points out. Making sure that it fits local needs puts special demands on the development process of the education material.
Diabetes education – Vietnam styleIn the first half of 2013, Steno Diabetes Center will develop the material for the training of the endocrinologists. The programme material will be co-created with the Vietnam Association of Diabetes & Endocrinology and will focus on current concepts in diabetes management as well as teaching methods.
“We are passing on knowledge about diabetes care, but to get there we need to focus on communication methods and pedagogics,” says Voigt. When the materials have been co-created to ensure proper understanding and use, they will have education material to be used by the endocrinologists when training general practitioners on screening, diagnostics and treatment of diabetes and its complications.
According to Bjerre-Christensen, local adaptation is fundamental to a successful process. “It is crucial that the education material fits to the Vietnamese context. The healthcare professionals have to be able to apply it in reality – or else it will not benefit the patients.”
So far, cultural differences and language have been the biggest challenges, however, the Vietnamese health community has shown a great interest and a tremendous willingness to work towards finding suitable solutions.
Towards a brighter futureReaching out to 2000 healthcare professionals, both endocrinologists and general practitioners, is expected to have a positive impact on diabetes management in Vietnam. In fact, preliminary results from the evaluation of a similar programme in Indonesia show that knowledge about diabetes was significantly improved among healthcare professionals who participated in the training.
With improved knowledge, healthcare professionals are able to detect complications earlier and provide better treatment. As the network grows, the Vietnam Diabetes Care Program will spread much needed diabetes treatment knowledge. Knowledge that should reduce healthcare costs and improve quality of life for people with diabetes. For the individual patient this could mean living a healthy life with properly treated diabetes and feet that are free from diabetes-related ulcers.
TBL QUARTERLY 13
The people driving sustainability – around the globe
What does your work with responsible sourcing entail?
Lene: If you take a helicopter perspective, basically what we are aiming to do with the responsible sourcing programme is to extend the Triple Bottom Line business principle to our supply chain so that our suppliers work according to good standards.
Victoria: We work with sourcing and finance professionals across the organisation to identify potential responsible sourcing risks within our supply base and to ensure that we have actions in place to mitigate those risks in order to protect the Novo Nordisk brand.
What are the most challenging issues when carrying out your work?
Victoria: From my perspective it would be the diverse types and number of suppliers that we work with. For indirect spend1, we have around 40,000 suppliers and being able to identify a pragmatic risk based approach to handling those suppliers is quite a challenge but something we are making good progress with.
Lene: Promoting responsible sourcing improvements with suppliers in countries where law enforcement
in this area is weak is a challenge because of the differences in culture, local standards and business practices.
What does it take to be good at your job?
Victoria: Communication, communication, communication! I rely heavily on the people who work with me here in headquarters but also at our regional offices around the world. My colleagues need to understand, from me, what they and their suppliers need to do in relation to responsible sourcing and then communicate that on to their suppliers.
Lene: Being based in Denmark, we quite often sit a long way from our colleagues at the local sites, so it is about being able to support those who locally engage with the suppliers to implement responsible sourcing, as to some of them it is new.
If we take this to a personal level, what would have been the biggest personal success?
Lene: Recently, I have been involved in a project in Russia where we are building a new factory. My role has been to support the project, ensuring that responsible sourcing and business ethics are
1 Indirect spend refers to products or services purchased that are not directly linked to Novo Nordisk products.
Novo Nordisk’s responsible sourcing programme has shaped the company’s approach to business conduct throughout its supply chain. With more than 40,000 suppliers, Novo Nordisk sources from countries around the globe, some of these countries are characterised by weak enforcement of international law. For Victoria Stone and Lene Fergusson, this means understanding the risks and impacts associated with the social, ethical and environmental performance of Novo Nordisk’s suppliers and continually working with them to support their journey towards responsible business practices.
Responsible sourcing - it’s like planting little seeds with the supplier

TBL QUARTERLY 14
an integrated part of the project execution. We have here recognised that we are working in a country with different norms and practise and that responsible sourcing requirements in general are new to our suppliers –therefore we have provided training to the suppliers to explain about our requirements, the audit process etc. Now it is rewarding to see incremental improvements, greater awareness and not least willingness and commitment from suppliers, even though not everything can be solved in a day.
Victoria: Last year, one of my personal successes was to identify all suppliers with highest responsible sourcing risks and to engage with them, via their day to day Novo Nordisk contact, to implement action plans to mitigate that risk. Again, this is something that couldn’t have been done without the support from Novo Nordisk colleagues around the world interacting with suppliers.
In what situation did you feel like you made a difference?
Lene: In relation to audits and the follow-up process where you actually see suppliers taking on-board some of the improvements. It could be minor things but it could mean a huge deal to some of the people working in the factory and to the environment surrounding it. Once we did a pre-screening of a potential supplier who was releasing too much nickel into the sewer. Even though we hadn’t placed any orders yet, the supplier valued the feedback and put a new neutralisation system in place. The interesting thing was that the authorities had actually visited the supplier a few months before, but they had ignored the problem.
Victoria: In our area when we started doing responsible sourcing audits with some indirect spend suppliers there was one supplier we approached who was initially very reluctant when we requested the audit and it took quite some negotiating on different levels to get them to agree, but in the end they did and we conducted the audit and identified areas for improvement. The success in this story comes from their recent confirmation that all the resulting actions have now been closed which in turn means, for this supplier at least, conditions for their employees have improved.
During audits with a supplier, how do you ensure an open and honest exchange?
Victoria: In the audit I was just referring to, and as is usual practice, in addition to our experienced responsible sourcing auditors, we used one of our employees from our local office who spoke the local language to talk to the supplier’s employees. This worked really well because she could build a rapport
with them, in their language, and got a good idea of whether they were being honest in their answers to her questions.
Lene: Honesty and openness in the audit process is important, therefore our auditors also emphasise upfront that the audit process is not about de-selecting suppliers, but about establishing a basis for a solid business relationship and continuous improvement.
What is the step by step approach with a non-compliant supplier?
Lene: Usually we find out if a supplier is non-compliant when we conduct an audit. We do approximately 30 to 50 responsible sourcing audits every year, so it is not all our suppliers that go through this process. At the audit, a number of non-conformities will be identified and we grade the non-conformities into different levels –critical, major or minor. The supplier will be informed about the non-conformities and asked to make a corrective action plan. The sourcing responsible, the auditor and I will then be involved in approving the action plan and agree on timelines. The supplier will usually send us documentation to demonstrate they have actually implemented the actions we agreed on.
Do you find any gaps between the Novo Nordisk responsible sourcing standards and the suppliers’ local practice?
Lene: Absolutely, our suppliers will basically be operating from what is the norm in their country. I also think we have to keep in mind that although we strive to have suppliers adhere to our standards, it is about continuous improvement, and we realise
Victoria Stone works as a project manager for responsible sourcing in the Corporate Procurement department at Novo Nordisk.

TBL QUARTERLY 15
that we cannot change the world from one day to another and neither can our suppliers. You need to take it to another level, it’s like planting little seeds with the supplier, because for some of them it is the first time they hear of responsible sourcing.
Victoria: Ensuring responsible sourcing is a two way street where focus is not only required on our continuous improvement but also that of our suppliers who should work to uphold the Novo Nordisk responsible sourcing standards in a way that is consistent with their own company programmes.
Lene Fergusson works as a sourcing project manager in the Global Engineering Sourcing department at Novo Nordisk.
Learn more about Novo Nordisk’s approach to responsible sourcing

About sustainability at Novo Nordisk
Headquartered in Denmark, Novo Nordisk is a global healthcare company with 90 years of innovation and leadership in diabetes care. The company also has leading positions within haemophilia care, growth hormone therapy and hormone replacement therapy. Novo Nordisk strives to conduct its activities in a financially, environmentally and socially responsible way. The strategic commitment to corporate sustainability has brought the company onto centre stage as a leading player in today’s business environment, recognised for its integrated reporting, stakeholder engagement and consistently high sustainability performance. In 2013, Novo Nordisk received the Pharmaceuticals and Biotechnology industry group top ranking on Corporate Knight’s list of Global 100 Most Sustainable Corporations.
We want to hear from you!Novo Nordisk believes that reaching out to stakeholders helps us to reconcile dilemmas and find common ground for more sustainable solutions. If you have any questions, comments or suggestions regarding this issue of the TBL Quarterly, please send us a mail at [email protected] or send us a tweet to @novonordisktbl
For a deeper look at how Novo Nordisk works with sustainability, visit our website at novonordisk.com/sustainability