
INTRODUCTION - Vanderbilt Universityetd.library.vanderbilt.edu/available/etd-03282006-160241/... ·...
177
CHAPTER I INTRODUCTION Renal transplantation is the surgical placement and vascular integration of a human kidney from a living or cadaveric donor into a patient who has end stage renal disease (ESRD). It is considered the only treatment that restores reasonably normal kidney function and health (Wallace, 1998). Although renal transplantation brings many benefits to patients, it is potentially associated with a number of drawbacks, which include constant risk of rejection, the need to comply with a complex medication regimen capable of producing pronounced side effects, and the need for ongoing medical supervision. These drawbacks are also stressors for patients (Fallon, Gould, & Wainwright, 1997), with some of the most important being fear of kidney transplant rejection, worries about the risk of infection, compliance with the medication regimen, repeated hospitalizations, and changes in body appearance (Fallon et al., 1997; Kong & Molassiotis, 1999). Thus, renal transplant patients experience stress and uncertainty, which influence their health-related quality of life (HRQOL). Coping, defined as cognitive and behavioral efforts to manage stressors (Lazarus and Folkman, 1984), is considered an important predictor of HRQOL of renal transplant patients (White et al., 1990). Problem-focused coping and religious coping were positively correlated to HRQOL in renal transplant patients (Christensen et al., 2000, 2002; Frazier, Davis-Ali, & Dahl, 1995; Tix & Frazier, 1998), while emotion-focused coping (evasive, emotive, and fatalistic coping) was less effective in adjustment of renal transplant patients (Lindqvist,
Transcript of INTRODUCTION - Vanderbilt Universityetd.library.vanderbilt.edu/available/etd-03282006-160241/... ·...

CHAPTER I
INTRODUCTION
Renal transplantation is the surgical placement and vascular integration of a
human kidney from a living or cadaveric donor into a patient who has end stage renal
disease (ESRD). It is considered the only treatment that restores reasonably normal
kidney function and health (Wallace, 1998). Although renal transplantation brings many
benefits to patients, it is potentially associated with a number of drawbacks, which
include constant risk of rejection, the need to comply with a complex medication regimen
capable of producing pronounced side effects, and the need for ongoing medical
supervision. These drawbacks are also stressors for patients (Fallon, Gould, &
Wainwright, 1997), with some of the most important being fear of kidney transplant
rejection, worries about the risk of infection, compliance with the medication regimen,
repeated hospitalizations, and changes in body appearance (Fallon et al., 1997; Kong &
Molassiotis, 1999). Thus, renal transplant patients experience stress and uncertainty,
which influence their health-related quality of life (HRQOL). Coping, defined as
cognitive and behavioral efforts to manage stressors (Lazarus and Folkman, 1984), is
considered an important predictor of HRQOL of renal transplant patients (White et al.,
1990). Problem-focused coping and religious coping were positively correlated to
HRQOL in renal transplant patients (Christensen et al., 2000, 2002; Frazier, Davis-Ali, &
Dahl, 1995; Tix & Frazier, 1998), while emotion-focused coping (evasive, emotive, and
fatalistic coping) was less effective in adjustment of renal transplant patients (Lindqvist,

2
Carlsson, & Sjödén, 2004). However, factors affecting coping were not well documented
in the literature on renal transplant studies. According to Lazarus and Folkman�s (1984)
model of stress and coping, appraisal is a cognitive mediator affecting coping. Self-
efficacy and social support were found to influence patients� appraisals of their situations
and then their coping behaviors in various chronic illnesses (Hagger & Orbell, 2003;
Manne & Zautra, 1989; Merluzzi & Martinez-Sanchez, 1997; Ptacek et al., 2002; Shaw,
1999). It is necessary for nurses to understand the coping strategies patients use and
factors influence coping, then develop interventions to help patients use effective coping
strategies to reduce stress related to renal transplantation. It is expected that these
strategies would help renal transplant patients improve their HRQOL. Thus, the
proposed study is designed to investigate the relationships among cognitive appraisal of
health, perceived self-efficacy, perceived social support, coping, and HRQOL in renal
transplant patients.
Renal transplantation is considered the first-choice method of renal replacement
therapy for ESRD patients who have no physical or psychological contraindications
(Jacobs & Luciani, 1992). When successful, a transplant helps restore the recipient to a
healthier daily life. If a transplant is unsuccessful, the patient can return to dialysis or
have a second transplant (Wallace, 1998). There are more than 500,000 renal transplant
patients in the world (Ji, 2002). In 2002, the incidence of renal transplant in the US was
51.22 per 1 million population, with a 3:2 ratio between men and women (Annual Report,
2003). Each year since 1993 in the United States, more than 10,000 kidney transplants
have been performed on patients with ESRD (Wallace, 1998).

3
With advanced medical techniques and immunosuppressive medications, patient
survival rates also have improved. According to the Annual Report of the Organ
Procurement and Transplantation Network (2003), the one year patient/graft survival rate
in the US was 94.0%/88.4%, the three year patient/graft survival rate was 88.4%/78.5%,
and the five year patient/graft survival rate was 79.9%/63.3%. However, renal
transplantation is not risk-free. The risks of transplantation include rejection, infection,
cardiovascular problems, increased incidence of malignancies such as lymphomas and
skin cancers, hypertension, and steroid-induced complications (Harasyko, 1989). Among
them, rejection is the main complication that causes graft failure. The majority of
irreversible rejection episodes occur within the first three to six months after
transplantation (McCarley & Lewis, 1996). To prevent and control graft rejection,
immunosuppressive therapy is used after transplantation. Immunosuppressive
medications have many side effects, with infection being the most common complication.
Leukopenia, high blood pressure, facial and body changes, increased appetite, hair
growth, bone pain, muscular weakness, depression, anxiety, irritability, sexual
dysfunction, and personality changes are common side effects (Duborsky & Penn, 1980;
Matas, 2002). These side effects not only impact patients� health and functioning but
also their psychological response.
The high cost of the operation and the life-long immunosuppressive medications
present a significant economic challenge for renal transplant patients and their families as
well as for society. The intensive follow-up regimen influences renal transplant patients�
daily and social activities and employment and, in turn, increases their economic burden
(Molzahn, Northcott, & Dossetor, 1997). Hauser and colleagues (1991) also suggested

4
that repeated hospitalizations of transplant patients and intensive follow-up in the first
year post-transplant severely disturb normal family life and usually cause their children
anxiety and loneliness.
In summary, renal transplantation may negatively impact a patient�s physical,
psychological, socioeconomic, and family status. Renal transplant patients live with
chronic illness even after transplantation has been performed successfully (Fallon et al.,
1997). They worry about rejection and have distress related to side effects of
medications, economic burden, family relationships, and social functioning; all of these
problems influence their HRQOL.
Renal transplantation is a chronic condition that involves the total human
environment for supportive care and self-care. It not only affects the patients but also the
family and society. The long-term nature of post-transplant healthcare often creates the
need for ongoing family support and thus presents an additional potential burden (Lewis
et al. 1990). Additionally, the relatively high cost of the surgery and life-long
immunosuppressive medications bring economic consequences for patients� families as
well as society. The intensive follow-up regimen may impact daily and social activities
and employment, which in turn may exacerbate the economic burden (Molzahn,
Northcott, & Dossetor, 1997). Thus, helping renal transplant patients effectively cope
with the negative impact of transplantation and increasing opportunities for employment
are important issues for both healthcare professionals and society.
Increasing quality and years of healthy life is one of the two major goals of
Healthy People 2010 (U.S. Department of Health and Human Services, 2000).
Additionally, chronic illness is one of the 28 focus areas identified by Healthy People

5
2010. Clearly, renal transplantation is a problem of significant interest to U.S. society.
Improvement of the HRQOL of renal transplant patients is consistent with the goals of
Healthy People 2010.
Because advanced technology and therapies have produced longer survival after
renal transplantation, HRQOL of renal transplant patients has become an increasingly
important healthcare issue. Health-related quality of life is considered a primary end-
point in healthcare (Pais-Ribeiro, 2004). Survival, HRQOL, and cost-effectiveness are
the main parameters to evaluate ESRD treatment (Gritsch, 1996). Studies have shown
that renal transplant patients face many new challenges after transplantation (Fallon et al.,
1997; Frey, 1990; White et al., 1990). They experience some physical, psychological,
socioeconomic, and family problems, which influence their HRQOL. To achieve the
goal of Healthy People 2010 and enhance clinical outcomes, it is important for healthcare
professionals to help these patients cope with the impact of renal transplantation.
Healthcare professionals need to develop interventions to educate renal transplant
patients to use effective coping strategies to better manage the side effects of
immunosuppressive medications and increase their socialization and their ability to
maintain employment. Thus, their general state of health and well-being will be
improved.
Nursing, as a discipline, encompasses �the diagnosis and the treatment of human
responses to actual or potential health problems� (American Nurses� Association [ANA],
1995, p. 6). �Attention to the full range of human experiences and responses to health
and illness without restriction to a problem-focused orientation� (ANA, 1995, p. 6) is
included as one of the four essential features of contemporary nursing practice. The

6
holistic perspective of nursing addresses both physiological and psychological concerns
of patients. From this standpoint, understanding the experience of renal transplant
patients, identifying their response to transplantation, and helping them effectively cope
with its impacts are within the realm of nursing. McHaffie (1992) stated that helping
patients develop successful coping strategies is an essential element of nursing, and how
well a person copes is central in determining his or her well-being. Nurses have a unique
role and must take professional responsibility for assisting patients and their families
learn to cope with events effectively and to achieve an optimum HRQOL.
Thousands of patients with ESRD have received renal transplantation. Renal
transplant recipients experience a variety of factors that negatively impact their HRQOL
in comparison to the healthy population and other clinical populations. One important
focus of nursing is to promote well-being of both healthy and ill people (ANA, 1995).
Thus, how to improve these patients� HRQOL is a phenomenon of specific interest for
nephrology nurses. In doing so, nephrology nurses must be able to educate renal
transplant patients about self-care skills, including recognizing the signs and symptoms
associated with impending rejection and preventing infection. They must also be able to
develop evidence-based protocols for follow-up care. Most importantly, they must be
able to help patients develop the skills to cope with the stresses experienced after renal
transplantation. It is important to understand coping and HRQOL in renal transplant
patients. With increased understanding of these phenomena, nephrology nurses may
develop effective interventions to help renal transplant patients use adaptive coping
strategies to improve their HRQOL. Additionally, the body of nursing knowledge on
coping and HRQOL in renal transplant patients will be enhanced.

7
Renal transplant patients live with a chronic illness once transplantation has been
performed successfully. They face many new challenges and experience stress, which
require them to cope with ongoing stressors. Cognitive appraisal, personal (e.g., self-
efficacy), and situational (e.g., social support) variables are identified in the literature as
predictors of coping and HRQOL in individuals with chronic illness, such as cancer,
multiple sclerosis, and rheumatoid arthritis. However, these variables were not
examined in renal transplant patients. The purpose of this study was to investigate the
relationships among cognitive appraisal of health, perceived self-efficacy, perceived
social support, coping, and HRQOL in renal transplant patients. Because there is a lack
of conceptual model in renal transplant studies, a modified model derived from Lazarus
and Folkman�s (1984) Model of Stress and Coping was proposed and tested in patients
following renal transplantation. In addition, the effects of clinical factors (e.g., duration
of dialysis, history of hospitalizations, time post-transplantation, side effects of
immunosuppressive medications, and donor type) that are ignored in most psychosocial
renal studies were considered in this study. Information from this study may help
nurses develop nursing interventions that facilitate effective coping strategies and
improve HRQOL of renal transplant patients.

8
CHAPTER II
REVIEW OF LITERATURE
The purpose of this review was to examine the conceptual and empirical literature
relevant to the study of coping and HRQOL in renal transplant patients. This review of
literature was organized into four major sections: a review of the conceptual and
methodological approaches to HRQOL in renal transplant patients; a review of the
conceptual and methodological approaches to coping in renal transplant patients; a
synthesis of the conceptual and methodological knowledge of coping and HRQOL in
renal transplant patients; and a proposed conceptual framework.
Health-related Quality of Life in Renal Transplant Patients
History of the Concept of Health-related Quality of Life
The term quality of life (QOL) was first mentioned in 1920 (Pigou, 1920) and was
widely acknowledged in the 1960s. Since the World Health Organization (WHO)
defined health as being not only the absence of disease and infirmity but also the
presence of physical, mental, and social well-being (WHO, 1948), QOL issues have
become more prevalent in healthcare research and practice. Although it has become an
important health outcome, there is no standard definition of QOL.
In the 1960s and the 1970s, QOL was usually defined globally and incorporated
ideas of satisfaction/dissatisfaction and happiness/unhappiness (Farquhar, 1995). Quality
9
of life was defined by Abrams (1973) as the degree of satisfaction or dissatisfaction felt
by people with various aspects of their lives and by Andrew (1974) as the extent to which
pleasure and satisfaction characterized human existence. These are all examples of
global definitions. Because of the generality of this kind of definition, it tells us little
about the components of QOL or how the concept should be operationalized.
In the 1980s and the 1990s, definitions of QOL often were broken down into a
series of dimensions and this trend continues today. George and Bearon (1980) defined
QOL in terms of four underlying dimensions. Two objective dimensions are general
health and functional status, and socioeconomic status; two subjective dimensions that
reflect the personal judgment of the individual are life satisfaction and related measures,
and self-esteem and related measures. Another example is Clark and Bowling�s (1989)
definition which stated that QOL was not only functional ability, level of activity, mental
state, and longevity but also included the concepts of privacy, freedom, and respect for
the individual, freedom of choice, emotional well-being, and maintenance of dignity.
Dimensional definitions are useful for empirical work and easier to operationalize. Some
researchers have combined the global and dimensional definitions of QOL. For example,
Ferrans and Power (1985) defined QOL as a person�s perception or sense of well-being
that stems from satisfaction or dissatisfaction with the areas of life that are important to
him or her. This model includes four domains: health and functioning, psychological /
spiritual, socioeconomic, and family.
The terms �quality of life� and �health-related quality of life� are often used
interchangeably in healthcare research, although QOL is a much broader concept,
including many more domains of life than HRQOL. Health-related quality of life
10
concerns the impact of disease and treatment on the lives of patients and is the subjective
assessment of the impact of disease and treatment across the physical, psychological,
social, and somatic domains of functioning and well-being (Revicki et al., 2000).
Similarly, Cella (1995) defined HRQOL as the extent to which one�s usual or expected
physical, emotional, and social well-being are affected by a medical condition or its
treatment. Testa and Simonson (1996) stated that HRQOL refers to the physical,
psychological, and social domains of health, seen as distinct areas that are influenced by a
person�s experiences, beliefs, expectations, and perceptions, and can be measured in two
dimensions, which are objective assessments of functioning and health status and more
subjective perceptions of health. There seems to be agreement among researchers that
HRQOL takes into account levels of physical, mental, social, and role functioning, and
includes abilities, relationships, perceptions, values, satisfaction, and well being (Bergner,
1989; Patrick & Erickson, 1993; Testa & Simonson, 1996; Ware & Sherbourne, 1992).
There are several major differences between QOL and HRQOL. Quality of life
represents a broad range of human experiences including many domains, such as
community, education, family life, friendships, health, housing, marriage, nation,
neighborhood, self, standard of living, and work (Campbell, Converse, & Rodgers, 1976).
Quality of life is used in sociology, economy, political science, and psychology. HRQOL
focuses on health and is often used in the healthcare field. In healthcare research,
HRQOL describes what the person has experienced as the result of medical care. It
assesses the differences between what the person expected from the treatment and what
the reality was.

11
Conceptual Approaches to Health-related Quality of Life of Renal Transplant Patients
HRQOL was not clearly defined in renal transplantation studies during the 1980s.
The researchers implied that QOL was life satisfaction and well-being (Bremer et al.,
1989; Bremer & McCauley, 1986; Evans, Hart, & Manninen, 1984). Bremer and
colleagues (1989) described objective QOL as life condition and resources (e.g., income,
education, activities, employment), and subjective QOL as the cognitive evaluation of
objective conditions and emotional responses to those conditions. From the 1990s,
HRQOL was well recognized as a multidimensional concept including physical,
psychological, and social domains in most renal transplantation studies. For example,
QOL was defined as patients� subjective appraisal of their physical, psychological, and
social functioning (Moons et al., 2002). Each of the domains comprises diverse
components. The physical domain includes functional capacity and work capacity; the
psychological domain includes life satisfaction, well-being, self-esteem, anxiety, and
depression; and the social domain concerns labor rehabilitation, pastimes, and familial
and social interaction. Hathaway and colleagues (1998) defined QOL as a
multidimensional construct including physical, psychosocial, functional, and self esteem
dimensions.
Conceptual frameworks for HRQOL were not well documented. Only a few
researchers mentioned QOL frameworks in their studies. Herrman�s (1997) definition of
QOL, which refers to quality of life as a person�s perception of his/her position in life
within the culture and value systems and in relation to individual goals, expectations,
values, and concerns, was used as a framework in some studies (Franke et al., 2000;
Kong & Molassiotis, 1999). Ortuzar (2001) proposed that evaluation of QOL of the

12
transplant patient should include �his or her self-determination, control, and
responsibility over his or her own life� (p. 1915) along with the level of functional
capabilities of the person. Ortuzar also mentioned that the psychosocial dimension is
fundamental in understanding QOL of renal transplant patients. Geest and Moons (2000)
indicated that a transplant patient�s subjective appraisal of side-effects of
immunosuppressive regimens should be included in the QOL framework. Hathaway and
colleagues (2003) provide the QOL framework for the Patient Outcomes Registry for
Transplant Effects on Life (PORTEL). The framework is composed of five interrelated
domains, which are health factors, social factors, major health events, major life events,
and quality of life and related factors. The first four domains interact with one another
and together influence quality of life in terms of its physical and psychological
components.
Definition of HRQOL in renal transplant patients evolved from a global concept
as life satisfaction and well-being to a multidimensional, subjective construct including
physical, psychological, and social domains. HRQOL is considered to relate to
individual goals, expectations, values, and concerns. For renal transplant patients,
subjective appraisal of side effects of immunosuppressive regimens and functional
capacities should be included in the evaluation of HRQOL. The psychosocial dimension
is fundamental in renal transplant patients� HRQOL due to fears of transplant rejection,
emotional stress caused by the chronic character of the illness, difficulties of employment,
and the loss of social opportunities.

13
Methodological Approaches to Health-related Quality of Life of Renal Transplant Patients
With advanced immunosuppressive therapy, patients� survival rates have
increased and HRQOL has become an increasingly important parameter for evaluating
the outcome of renal transplantation. HRQOL of renal transplant patients has been
extensively studied in recent decades. Fifty-four studies on HRQOL in renal transplant
patients were reviewed for this paper. These studies were conducted in 14 countries, with
the majority of the studies conducted in the US (41%). One study included US, European,
and Australian sites. Study designs, samples, measurements of HRQOL, factors
influencing HRQOL, and strengths and limitations of these studies are discussed in this
section.
Designs and samples for the studies. A majority of the 54 studies (55.6%) used
cross-sectional designs in which respondents were assessed once after transplant. Some
researchers included comparison or control groups within the study design. Among the
comparison studies, most researchers compared the transplant patients with dialysis
patients, and some researchers examined the effects of immunosuppressive medications.
A growing number of recent studies have used a stronger prospective design and
longitudinal investigations (5 prospective, 9 longitudinal studies) in which respondents
were assessed both before and after transplantation. In the longitudinal studies,
respondents were assessed periodically, usually for the first 1-2 years after transplant, but
sometimes for much longer periods. There were two test-retest design studies to assess
an instrument and two qualitative studies to explore the experiences of renal transplant
patients. Sample sizes varied widely across these studies, from small samples of 10 to
very large samples of more than 700 renal transplant patients.
14
Measurements of health-related quality of life used in the studies. Quality of life
is a very complex concept that has not been well defined. As a result, a great number of
measurement instruments have been developed. It is well recognized in the literature that
evaluation of QOL of renal transplant patients should include multiple dimensions that
are both objective and subjective. Generic and specific instruments were used to measure
QOL of renal transplant patients. Generic instruments assess health concepts that
represent basic human values and are relevant to everyone�s health status and well-being.
Generic instruments permit comparison across different populations and different
treatments. In contrast, specific instruments focus on problems associated with specific
diseases, groups of patients, or areas of function. Specific instruments may be more
sensitive to changes in disease or treatment-related factors. There is a trend to use both
generic and specific instruments in recent studies. In the 1980s, generic instruments such
as the Structure of Psychological Well-being including Positive and Negative Affect
Scales and the Affect Balance Scale (Bradburn, 1969); the Quality of American Life
consisting of Life Satisfaction, the Index of General Affect and the Index of Well-being
(Campbell, Converse, & Rodgers, 1976); and objective measurements such as the
Karnofsky Index and the Comorbid Index were used most often (Bremer et al., 1989;
Bremer & McCauley, 1986; Evans, Hart, & Manninen, 1984; Johnson, McCauley, &
Copley, 1982). These measurements were consistent with the global definition of QOL.
In the early 1990s, as QOL was accepted as a multidimensional construct, some
researchers developed questionnaires to measure physical, emotional, and social well-
being, vocational rehabilitation, leisure time activities, family relations, and sexual
adjustment (Gorlen et al., 1993; Koch & Muthny, 1990; Simmons & Abress, 1990).
15
Hathaway and colleagues (1990) developed a transplant interview guide to evaluate post-
transplant QOL expectations. In the late 1990s, generic instruments, such as the Sickness
Impact Profile (SIP), the Medical Outcomes Study 36-item short form (SF-36®), and
Brief Symptom Inventory (BSI), were most frequently used in the studies. Some disease-
specific instruments also were developed such as Ferrans and Powers� (1985) Quality of
Life Index (QLI)-Transplant Version, Kidney Transplant Questionnaire (Laupacis et al.,
1993), and End-Stage Renal Disease Symptom Checklist-Transplantation Module
(Franke et al., 1999). The SF-36 was widely used across the world after it was developed
by Ware and Sherbourne (1992). Findings have shown that the SF-36 is a proper method
to evaluate HRQOL in renal transplant patients (Feurer et al., 2004; Manu et al., 2001),
and it has been used in many studies with the renal transplant population. Jacobs and
colleagues (1998) conducted a study to determine whether the self-administered Kidney
Transplant Questionnaire (KTQ) performs similarly to the interview and demonstrated
that the self-administered KTQ exhibited high internal consistency and validity, and the
intra-scale correlations between interview and self-administration also were high.
Health-related quality of life of renal transplant patients and factors influencing it.
The terms QOL and HRQOL were used interchangeably in these studies. There is
consensus in the literature that renal transplant patients with functional grafts had a better
QOL than patients treated with various dialysis techniques (Bremer et al., 1989; Cameron
et al., 2000; Franke et al., 2000; Fujisawa et al., 2000; Jofre et al., 1998; Koch & Muthny,
1990; Laupacis et al., 1996; Mingardi et al., 1998; Muthny & Koch, 1991; Rebollo et al.,
2000; Russell et al., 1992; Simmons & Abress, 1990). Patients� QOL improved after
transplantation (Fisher et al., 1998; Jofre et al., 1998; Luk,, 2004; Ponton et al., 2001),
16
comparable to the general population in some dimensions (i.e., physical, psychological,
daily activities, and the global index of QOL) (Bremer et al., 1989; Franke et al., 2000).
However, in France and Japan, renal transplant patients reported lower physical and
general health than the general population (Karam et al., 2003; Tsuji-Hayashi et al.,
1999).
QOL of renal transplant patients with different immunosuppressive regimens also
has been examined (Moons et al., 2002; Oberbauer et al., 2003; Reimer et al., 2002;
Shield et al., 1997; Simmons & Abress, 1990). Patients treated with sirolimus alone
demonstrated better QOL in fatigue, appearance, and vitality dimensions than patients
with the treatment combination of sirolimus and cyclosporine A (Oberbauer et al., 2003).
Reimer and colleagues (2002) reported patients with tacrolimus-based therapy had
significantly better SF-36 physical component summary scores and better scores on the
subscales regarding physical functioning and general health as well as overall disease-
specific QOL than patients with cyclosporine-microemulsion based therapy. However,
some researchers reported that the increases in HRQOL scores were similar for the two
groups (tacrolimus-based vs cyclosporine-microemulsion based), favoring tacrolimus-
based therapy in only Physical Appearance scale (Sheld et al., 1997). Patients with
steroid-free regimens demonstrated better social, role-emotional functioning, mental
health, and lower symptom occurrence and distress levels compared with patients taking
steroids (Moons et al., 2002).
The source of the transplanted organ also influences the QOL of renal transplant
patients. The incidence of physical HRQOL impairment was greater in recipients of
transplants from cadaveric donors than in recipients of transplants from living donors

17
(Griva et al., 2002). The recipients of cadaveric organs demonstrated less overall
improvement at year one than recipients of organs from living donors (Kizilisik et al.,
2003). Patients receiving a kidney transplant from a living donor with a highly
supportive family environment exhibited a reduction in depression, increased mobility,
and increased social functioning (Christensen et al., 2002). Evans and colleagues (1984)
reported no significant differences in either objective or subjective QOL assessment
between recipients of cadaveric organs and living-related organs in their study with
randomly selected renal transplant patients.
Demographic variables and medical conditions that influence the QOL of renal
transplant patients have been investigated. Female renal transplant patients had a poorer
QOL and demonstrated less improvement after transplantation (Franke, 2003; Jofre et al.,
1998; Johnson et al., 1998; Mingardi et al., 1998; Muthny & Koch, 1991; Rebollo et al.,
2000). Matas and colleagues (2002) reported that male renal transplant patients had
lower QOL on the Life Satisfaction Index and the Transplant Care Index than female
renal transplant patients. This inconsistency with other studies may be related to the
focus of these instruments on self-care and personal relationships.
The effect of age on QOL is controversial. In some studies, younger renal
transplant patients had better QOL than elderly patients (Franke et al., 2000; Jofre et al.,
1998; Muthny & Koch, 1991). However, Humar and colleagues (2003) reported that the
overall benefit on QOL was similar for both a younger and older group, and the older
group scored higher with regard to social functioning and mental health. Rebollo et al.
(2001) indicated that elderly renal transplant patients had higher scores than younger
patients in the physical function, bodily pain, general health, social function, role
18
emotional, and mental health subscales of the SF-36. However, the sample size of
elderly renal transplant patients was smaller than younger patients (28 vs 213) in this
study. Another reason for these controversial findings may be related to the studies being
conducted in different countries (Spain, Germany, and US).
Indo-Asian renal transplant patients had a significantly lower QOL than
Caucasian European patients in physical health, mental health, kidney disease-targeted
issues, patient satisfaction, and social deprivation (Bakewell, Higgins, & Edmunds, 2001).
Johnson et al. (1998) reported African-American renal transplant patients achieved less
improvement than Caucasian-Americans in affective dimensions, such as self-image and
emotional behavior, as well as functional measures. Some studies indicated education
was positively related to the QOL of renal transplant patients (Matas et al., 2002; Pinson
et al., 2000; Rebollo et al., 2000).
Comorbidity was inversely related to QOL (Bremer et al., 1989; Hricik et al.,
2001; Jofre et al., 1998; Rebollo et al., 2000). Diabetes had negative effects on QOL
(Baiardi et al., 2002; Kizilisik et al., 2003; Matas et al., 2002; Pinson et al., 2000). Serum
creatinine concentration was associated with scores on the general health, vitality, and
social function subscales of the SF-36 (Ichikawa et al., 2000; Tsuji-Hayashi et al., 1999).
Rejection and the number of hospitalizations also negatively affected the QOL of renal
transplant patients (Hathaway et al., 1998; Shield et al., 1997; Simmons & Abress, 1990).
Adverse effects of immunosuppression were common in renal transplant patients. The
main adverse effects were unusual hair growth, gingival hyperplasia, easy bruising, slow
healing, weight gain, hypertension, sexual dysfunction, bone pain, muscular weakness,
and headaches, and these side effects had negative effects on QOL (Hricik et al., 2001;

19
Ichikawa et al., 2000; Matas et al., 2002; Witzke et al., 1997). It seems that
immunosuppressive therapy has adverse effects and these adverse effects, along with
comorbidities, and rejection have negative impacts on QOL of renal transplant patients.
Time after transplantation also may influence QOL of renal transplant patients.
Two cross-sectional design studies compared QOL of patients at different stages post-
transplant. A study conducted in Italy demonstrated there was a significant improvement
in the QOL between the pre-transplant and the immediate post-transplant (first 6 months)
patients, but the QOL progressively worsened during the third year post-transplant period,
and then settled back to levels similar to those recorded immediately after transplant
(Ponton et al., 2001). Another study conducted in Japan compared QOL among short-
term (<5 year), middle-term (5-10 years), and long-term (>10 years) post-transplant
patients and indicated that the middle-term group had the highest SF-36 scores and the
long-term group had the lowest scores (Ichikawa et al., 2000). Studies on QOL of long-
term (>10 years) post-transplant patients showed that the majority of these patients
reported a good QOL and were almost fully rehabilitated in the second and third decade
after their transplant (Gorlen et al., 1993; Pisani et al., 1997).
There are several longitudinal studies on the evolution of QOL of renal transplant
patients over time, and some findings are inconsistent. Some studies indicated patients�
overall functional performance improved after transplantation at 3 months, 6 months, and
1 year, after which it stabilized at year 2 (Kizilisik et al., 2003; Pinson et al., 2000).
Matas et al. (2002) assessed 598 renal transplant patients every three months and
observed no significant improvement in Life Satisfaction Index scores and a small
significant improvement in Transplant Care Index scores over time. Laupacis et al. (1996)

20
reported renal transplant globally improved patients� QOL compared to pre-transplant,
with these improvements stabilizing throughout the two years of follow-up. In general,
renal transplant patients seem to have stable QOL after one year post-transplant.
There is one study on stress and QOL (Fallon, Gould, & Wainwright, 1997), and
there are two studies on stress, coping, and QOL (Kong & Molassiotis, 1999; White et al.,
1990) in the reviewed articles. The major stressors identified in these studies were fear of
rejection, compliance with a complex medication regimen, side-effects of medications,
uncertainty about the future, fear of infection, repeated hospitalizations, social adjustment,
and the cost factor. Findings also indicated patients between one and five years post-
transplant experienced the most stress and less changes in QOL scores than the patients
within six weeks and five or more than five years post-transplant (Fallon, Gould, &
Wainwright, 1997). White et al. (1990) investigated stress, coping, and QOL in 55 adult
kidney transplant recipients within the first 6 months and found that total stress was
negatively related to QOL, and total coping was positively related to QOL after transplant.
Some studies also reported that psychological problems had a negative impact on the
QOL of renal transplant patients (Franke et al., 2003; Hricik et al., 2001).
Summary. The QOL of renal transplant patients was a well documented benefit
related to transplantation. Different factors have been associated with the HRQOL
perceived by patients, such as patient factors (i.e., age, gender, education, psychological
distress) and clinical factors (i.e., comorbidities, adverse medication effects, time since
transplant, treatment type, donor type). However, there are some limitations in the
literature. There is a lack of homogeneity of the groups of patients compared and poor
conceptualization of QOL in most studies. In many studies, the case-mix adjustment has
21
not been considered to correct such variables as age, comorbidities, and socioeconomic
factors. The majority of the studies were cross-sectional designs and some studies had
small sample sizes. A quality of life framework was not mentioned in the majority of the
studies. Many studies were conducted with wide differences in cultural patterns,
durations of follow up, and instruments, all of which made it difficult to compare studies.
Self-administered questionnaire bias was not mentioned. Most studies were done in
transplant centers where the researchers worked; therefore, the patients� loyalty to the
medical team may have made patients answer the questions in positive ways. There were
no intervention studies and the usefulness of the findings in actual practice was not
addressed. Personal and psychosocial factors influencing QOL also were not well
documented. Some studies showed that there were differences in QOL expectations
between patients and health care professionals (Hathaway, Strong, & Ganza, 1990;
Hauser et al., 1991). Patients� perceptions of transplantation and coping strategies used
to cope with the situation need further investigation. In future studies, psychological
factors such as stress, appraisal, and coping in renal transplant patients and their
associations with HRQOL need to be explored.
Coping in Renal Transplant Patients
History of Coping
In the 1960s, the concept of coping began to be formally used along with the
interest in stress. Some researchers labeled certain �adaptive� defense mechanisms
�coping� activities, and their work was within the tradition of defense mechanism

22
research (Parker & Endler, 1996). This traditional approach to coping emerged from two
different literatures: animal experimentation and psychoanalytic ego psychology. Within
the animal model, coping is frequently defined as acts that control aversive
environmental conditions, thereby lowering psychophysiological disturbance. The
emphasis is largely on avoidance and escape behavior. In the psychoanalytic ego
psychology model, coping is defined as realistic, flexible thoughts and acts that solve
problems and thereby reduce stress (Lazarus & Folkman, 1984). While carefully
addressing the limitations and defects of the traditional approach that emphasized coping
as a style or trait, Lazarus and Folkman (1984) defined coping as �constantly changing
cognitive and behavioral efforts to manage specific external and/or internal demands that
are appraised as taxing or exceeding the resources of the person� (p. 141). This approach
views coping as an ongoing dynamic process and is concerned with what the person
actually thinks or does in a specific context, as well as changes in these thoughts and
actions across encounters. Lazarus (1993) further conceptualized coping as a purposeful
response that attempts to change the person-environment realities behind negative
emotions and attempts to change either what is attended to or how it is appraised. This
definition was derived from a cognitive-motivational-relational theory of emotion, which
emphasizes the process of appraisal and relational meaning. Coping is considered to be a
goal-directed process in which the individual orients thoughts and behaviors toward the
goals of resolving the source of stress and managing emotional reactions to stress
(Lazarus, 1993).

23
Theory of Coping
Lazarus and Folkman�s (1984) Stress and Coping Model is the best known and
most widely used model in coping research. The basic assumption of the model is that
individuals who are confronted with a stressor evaluate this stressor and that this
evaluation determines their emotional or behavioral reactions. This evaluation is called
cognitive appraisal, which is defined as �the process of categorizing an encounter, and its
various facets, with respect to its significance for well-being� (Lazarus & Folkman, 1984,
p. 31). Cognitive appraisal can be classified as primary appraisal and secondary appraisal.
Primary appraisal refers to a set of cognitions regarding the impact or significance of the
stressful encounter (e.g., it is a threat, challenge, or harm/loss to his or her well-being),
whereas secondary appraisal refers to a set of cognitions concerning one�s resources or
options for dealing with the encounter. Coping is defined as any effort to manage
external or internal demands that are appraised as negative or challenging. External
demands refer to the encounter itself, while internal demands refer to the emotional
reactions to the encounter. Problem-focused and emotion-focused coping are the two
major functions of coping. Problem-focused coping involves activities that aim to
change the elements of the stressful situation. In contrast, emotion-focused coping
involves activities that modify one�s emotional reactions resulting from the stressful
situation and make life bearable by avoiding situations that can be overwhelming if
confronted directly (Lazarus & Folkman, 1984).
The consequences of coping may be effective or ineffective for managing
psychological, social, and physiological stressors. Most people use various forms of
coping in a stressful situation; however, problem-focused coping predominates when

24
people feel that something constructive can be done, and emotion-focused coping
predominates when people believe the stressful situation cannot be changed (Lazarus,
1990). Problem-focused coping is viewed as a more effective strategy in Western
societies (Lazarus, 1993). Unsuccessful coping appears to be more associated with
emotion-focused coping, such as avoidant strategies, wishful thinking, and self-blame
(Folkman et al., 1986). Some findings indicate that emotion-focused coping strategies
seem to be more adaptive in the short run, whereas problem-focused coping may be more
adaptive in the long run (Suls & Fletcher, 1985).
In Lazarus and Folkman�s (1984) model of stress and coping, appraisal and
coping were considered as processes, and relationships among stress, appraisal, and
coping were stated clearly. The model particularly emphasized appraisal as the cognitive
mediator affecting coping. This model is suitable to study chronic illness conditions.
However, there are some limitations to this original stress and coping model. Although
Lazarus and Folkman (1984) emphasized the person-situation transactions, the situation
dimension is poorly represented in this model. The model also neglected interactions
with the context, such as the importance of social support on coping, and also overlooked
the effects of the individual as a whole person who has a particular goal or motivation,
situational intentions, belief systems and a life pattern of plans, and social connections on
the meaning of an event. A few researchers have addressed some of the limitations
through incorporating other models into this stress and coping model (Schwarzer, 1998;
Shaw, 1999).
25
Self-efficacy
Schwarzer (1998) gave an overview of personal and social coping resources from
a social-cognitive perspective. Schwarzer highlighted perceived self-efficacy as a
personal coping resource for managing a stressful situation. Bandura (1995) defined self-
efficacy as �the belief in one�s capabilities to organize and execute the course of action
required to manage prospective situations� (p. 2). Self-efficacy gives one a sense of
control over the environment. Efficacy expectancy is the belief that a person can and has
the intention to complete a specific behavior required to produce a desired outcome, and
outcome expectancy is the estimate that a given behavior will lead to the outcome
(Bandura, 1977). Efficacy expectancies reflect the belief of being able to master
challenging demands by means of adaptive action and an optimistic view of one�s
capacity to deal with stress. Self-efficacy makes a difference in how people feel, think,
and act. This resource plays an important role in determining how a person copes. Self-
efficacy also can affect a person�s motivation to act. High self-efficacy individuals
probably choose to perform more challenging tasks, set higher goals, and stick to them.
They tend to select a challenging setting, explore their environment, or create new
situations. Macdonald et al. (1998) also suggested that greater perceived self-efficacy
predicted increased frequency of the use of problem-focused coping, and high self-
efficacy individuals appeared to be more likely to cope with day-to-day stressors. Self-
efficacy as a personal coping resource affects appraisal, which affects motivation and
then coping behaviors.
There are three levels of measurement of self-efficacy in the literature. According
to Bandura (1977), self-efficacy is specific to behaviors and the situations, and is most

26
appropriately measured at a very specific level. A number of scales were developed to
assess self-efficacy for specific health behaviors (e.g., healthy eating behavior,
Schwarzer, 1993) and showed considerable power in predicting the specific behaviors
within a particular context. Some researchers argued that more general measures are
better suited for predicting more general patterns of behaviors and a lot of highly
general measures of self-efficacy were developed (Smith et al., 1991; Wallston, 1989).
These general measures have demonstrated strong relationships to broad adaptive
outcomes (Smith, Wallston, & Smith, 1995). After considering few measures assessing
efficacy/competence beliefs at a more intermediate, domain-specific level, Smith and
colleagues (1995) designed the Perceived Health Competence Scale (PHCS) to assess
efficacy/competence beliefs concerning one�s health at this intermediate level of
domain-specificity. This scale would be appropriate in this study for investigating renal
transplant patients� beliefs of capability to perform healthy behaviors to cope with their
health conditions, especially for the early period renal transplant patients who have little
experience and have not yet developed more specific expectancies.
Social Support
Social support generally is viewed as a generic construct including social
networks and social interactions (Schreurs & Ridder, 1997). Cohen and Syme (1985)
defined social support as the processes by which interpersonal relationships protect
individuals against the deleterious effects of stress and promote psychological well-being.
Weiss (1974) described social support as a composite concept including (1) a sense of
belonging; (2) a provision for intimacy or attachment; (3) an opportunity for nurturing
27
behavior; (4) the availability of assistance in the form of informational, emotional, and
instrumental help; and (5) a reassurance of individual worth and role accomplishments.
The mechanisms through which social support influences coping and psychological well-
being were explored by researchers. There are two theoretical models of social support.
The direct effects model proposes that social support has beneficial effects irrespective of
whether the persons are under stress or not; there is a direct link between social support
and health outcomes. This model derives from a statistical main effect of social support
(Cohen & Wills, 1985). The stress-buffering model suggests that social support protects
persons against the deleterious effects of stress at times of crisis. It derives from a
statistical interaction effect, that is, there should be a positive correlation between social
support and health outcomes for persons facing high stress, but no correlation between
them for persons with little or no stress (Cohen & Wills, 1985). The key to stress-
buffering is the perception that others will provide resources when they are needed and
the beliefs about its availability are more important for health and adjustment than
whether or not one actually receives support (Cohen, Gottlieb, & Underwood, 2001). In
the buffering model, social support is connected with coping. Schreurs and Ridder (1997)
suggested four ways to link coping and social support in the context of chronic disease:
(1) seeking social support as a form of coping, (2) social support as a coping resource, (3)
social support as dependent on coping, and (4) coping by a social system.
In this study, social support may be perceived as a coping resource. Integrated
into the Lazarus and Folkman�s (1984) Stress and Coping Model, social support is a
resource that affects appraisals of stressors. With more resources available, perceptions
of the amount of control one has or the level of one�s self-efficacy with regard to coping
28
may increase. In turn, these beliefs may influence whether a given event is appraised as
stressful and what course of coping is pursued (Ptacek et al., 2002). In addition to
influencing coping by altering appraisals, social support resources may also directly
affect specific coping efforts. Higher levels of perceived support may facilitate the use of
generally more adaptive coping strategies and inhibit the use of generally less adaptive
strategies.
Conceptual Approaches to Coping in Renal Transplant Patients
Coping has not been clearly defined in renal transplant studies. Lazarus and
Folkman�s (1980, 1984) definition of coping was used in two studies (Kong &
Molassiotis, 1999; White et al., 1990). Coping referred to the person�s constantly
changing cognitive and behavioral efforts made to manage specific external and internal
demands that were appraised as taxing or exceeding the resources of the person. It
involves on-going appraisal and reappraisal of the dynamic person-environment
relationship.
Appraisals related to spiritual beliefs also can be incorporated into Lazarus and
Folkman�s (1984) Stress and Coping Model. Religious coping was defined by Tix and
Frazier (1998) as the use of cognitive or behavioral techniques, in the face of stressful life
events, that arise out of one�s religion or spirituality. Spirituality is considered as a
resource that affects secondary appraisals and would foster improved coping with health-
related post-transplant adverse events (Martin & Sachse, 2002). Spirituality was defined
by Reed (1987) as an awareness of one�s inner self and a sense of connection to a higher
being, nature, others, or to some purpose greater than oneself. It is multidimensional,

29
existential in meaning and composition, and fundamental to the well-being of chronically
ill individuals (O�Neill & Kenny, 1998).
Most renal transplant studies did not present/utilize a conceptual framework of
coping. Some researchers mentioned Lazarus and Folkman�s (1984) Stress and Coping
Model, but they did not apply the model to their studies. Some researchers focused on
only one aspect of coping. Coping as a style or process was not clearly stated. Factors
influencing coping were not mentioned.
Methodological Approaches to Coping in Renal Transplant Patients
Eleven articles that focused on stress, coping, and adjustment were reviewed.
Across the 11 studies, eight were conducted in the US, and the other three were done in
China, UK, and Sweden. Designs, samples, stressors, measurements of coping, coping
strategies, and associations among stress, coping, and HRQOL in renal transplant
patients are discussed in this section.
Designs and samples. Most studies (82%) utilized a cross-sectional design. Only
two studies used a prospective design in which participants were assessed twice. Some
researchers included comparison groups to compare the transplant patients at different
stages after transplantation. All the studies applied convenience sampling methods to
recruit participants. The sample size varied from 28 to 297 participants, with the majority
of studies including less than 100 renal transplant patients.
Stressors experienced by renal transplant patients. According to Lazarus and
Folkman�s (1984) Stress and Coping Model, stressors precipitate appraisals which then
trigger coping behaviors. Stressors experienced by renal transplant patients were

30
investigated in some of the reviewed studies. Frey (1990) explored stressors in renal
transplant recipients at six weeks after transplant. The Kidney Transplant Recipient
Stress Scale (KTRSS) (Hayward et al., 1989) was used to determine stressors. Findings
demonstrated that the most salient stressor was the possibility of repeated hospitalizations.
The next four in order were possibility of rejection, cost of medications, uncertainty
about the future, and side effects of medications. The least stressful stressor was changes
in friends. The next four least-stressful items included admission process, loss of contact
with dialysis patients, changes in spiritual activities, and unfamiliar surroundings. The
stressors of most concern were similar to those in other studies. Sutton and Murphy
(1989) reported the stressors of renal transplant patients less than four years post-
transplant. The five highest stressors were cost, fear of rejection, weight gain,
uncertainty concerning the future, and limitation of physical activities. Fear of not being
accepted by friends and family, feeling that the kidney transplant is not part of one�s body,
and reversal in family roles with the children were the lowest. White et al. (1990) found
that health-related items (concern about the success of transplant, risk of infections, side
effects) were the most stressful for patients in the first six months after renal transplant;
work-related items were least stressful. Fisher et al. (1998) interviewed 5 patients who
had undergone their first transplant within the previous four months and found that risk of
rejection and possibility of repeated hospitalization were of greatest concern to their
patients.
In London, Fallon, Gould, and Wainwright (1997) conducted a study on stress of
renal transplant patients using the modified KTRSS. The most important stressors were
identified as fear of rejection, worries about risk of infection, worries prior to clinic visits,

31
repeated hospitalizations, and changes in body appearance. Cost was not considered an
important stressor in this sample, which may be related to the health insurance policy in
England. Another study was conducted in China by Kong and Molassiotis (1999). These
researchers used an open-ended question inquiring about stressors or concerns
experienced by renal transplant patients. The main stressors/concerns were fear of
rejection, compliance with a complex regimen, side-effects of medications, uncertainty
about the future, fear of infection, social adjustment, and the cost factor.
Frazier, Davis-Ali, and Dahl (1995) compared the stress experienced by kidney
transplant patients and their spouses. Patients experienced significantly more overall
stress than spouses. Patients reported significantly more stress than spouses on side
effects and interpersonal relationships; spouses reported significantly more stress on
patients� future health. The stressors� rank for patients was (1) financial issues; (2) fears
regarding future health and medication side effects; (3) interpersonal relationships and
medical regimen; and (4) complying with the medical regimen. For spouses, the rank was
(1) financial issues and concerns regarding the patient�s future health; (2) medication side
effects; (3) interpersonal relationships; and (4) following the medical regimen.
The most salient stressors identified in these studies were similar, which are cost,
fear of rejection, side effects of medications, uncertainty about the future, compliance
with a complex regimen, and repeated hospitalizations. Most of the studies examined
newly transplanted patients; thus it is not surprising to get consistent findings. Only two
studies explored stress at different stages following transplant and indicated that patients
1 to 5 years post-transplant experienced the most stress (Fallon et al., 1997; Sutton &
Murphy, 1989). The limitations of these studies were small sample sizes and cross-

32
sectional designs. Larger sample sizes including different stages of post-transplant
patients are needed to compare the stressors experienced by renal transplant patients.
Longitudinal design studies also are needed, so that the changes in stressors over time
will be captured.
Coping strategies used by renal transplant patients. Coping consists of the
cognitive and behavioral efforts to manage specific demands appraised as stressful
(Lazarus & Folkman, 1984). Some researchers investigated coping strategies used by
renal transplant patients to cope with transplantation. Lindqvist, Carlsson,and Sjödén
(2004) conducted a study to compare use and perceived effectiveness of different coping
strategies in people with kidney transplants (n=30) and an individually matched sample
of the general Swedish population(n=30). The Jalowiec Coping Scale (Jalowiec, 1991)
was used to measure coping strategies. Results showed that renal transplant patients used
significantly more optimistic, supportive, self-reliant and less emotive coping than the
general population. Renal transplant patients regarded self-reliant and confrontive coping
as more effective and emotive coping as less effective than the general population.
Evasive, emotive, and fatalistic coping were associated with low perceived efficiency in
handling various aspects of conditions. Strong positive correlations in renal transplant
patients were found between use and effectiveness ratings for most coping strategies.
Similarly, Sutton and Murphy (1989) identified that patients used more problem-oriented
coping (e.g., try to look at the problem objectively, maintain some control over the
situation) than affective-oriented coping (e.g., take drugs, drink alcohol, blame someone
else). Prayer also was found as one of the most used coping methods. Sutton and
Murphy further compared the coping methods between patients 0-23 months post-

33
transplant and patients 24-48 months post-transplant. There were no significant
differences on the mean total coping scores, but the two groups differed on affective-
oriented coping scores with the 24-48 months group scoring higher. Kong and
Molassiotis conducted a study on 101 Chinese renal transplant patients (with 23 within
one year and 78 more than one year post-transplant) in Hong Kong using the Chinese
Coping Scale to assess coping. Findings suggested Chinese renal transplant patients used
more internal locus of coping than external locus of coping, and there were no significant
differences between patients within one year and patients more than one year post-
transplant for overall coping score and all coping subscale scores. White, Ketefian, Starr,
and Voepel-Lewis (1990) assessed coping strategies used by adult kidney transplant
recipients in the first six months after transplant. The coping section of the Kidney
Transplant Questionnaire (Ketefian & Starr, 1987) was used to measure coping and found
that the highest scoring coping strategies were on the distancing/ detachment and self-
control/ accepting responsibility subscale (positive attitudes), while the escape/wishful
thinking subscale scores were the lowest. Religious coping also was identified as a
popular coping strategy in dealing with transplant-related stress (Tix & Frazier, 1998).
Martin and Sachse (2002) indicated that female renal transplant patients reported high
levels of spiritual perspective.
Renal transplant patients seem to use more optimistic, supportive, self-reliant and
less emotive coping than the general population. Generally, renal transplant patients used
more problem-oriented coping than affective-oriented coping; however, renal transplant
patients within two to four years post-transplant used more affective-oriented coping than
patients within two years post-transplant. Distancing/detachment and self-

34
control/accepting were used most, while escape/wishful thinking were used least in
patients within the first six months after renal transplant. Religious coping was also
frequently used in dealing with transplant-related stress. Cultural differences in coping
were found, which indicated that Chinese renal transplant patients used less emotional
discharge. They used more internal locus of coping than external locus of coping.
Different labels of coping strategies and different instruments measuring coping
presumably with varying levels of psychometric validation were used in these studies,
making it difficult to compare and reach conclusions across studies. Some researchers
did not mention the conceptual framework for their studies; thus, we cannot evaluate if
they measured what they wanted to measure well.
Associations of stress, coping, and health-related quality of life. The relationships
among stress, coping, and HRQOL also were explored in some of the studies. White et al.
(1990) examined stress, coping, and QOL in adult kidney transplant recipients within the
first six months and found that total stress was positively correlated with total coping.
Both total stress and total coping were important predictors of QOL after transplant.
Stress was negatively related to QOL; in contrast, coping was positively related to QOL.
However, Sutton and Murphy (1989) found that total stressor scores were not
significantly correlated with total coping scores or total problem-oriented coping scores;
total stressor scores were only significantly correlated with total affective-oriented coping
scores. This inconsistent finding may be related to the different instruments used to
measure stress and coping and patients� time post-transplant differing in the two studies.
Christensen et al. (2000) conducted a prospective study to examine the effect of
patient coping preferences on change in depression following renal transplantation. Sixty
35
patients were assessed using the Krantz Health Opinion Survey (KHOS) (Krantz, Baum,
& Wideman, 1980) and the Beck Depression Inventory (BDI) (Beck et al., 1961) while
on the waiting list and reassessed approximately 12 months later. Among the 33 patients
receiving transplant during the follow-up period, those with a high preference for health-
related information showed a substantial reduction in depression, and patients with a low
preference for information exhibited a slight increase in depression. Among the 27
patients not receiving transplant, preference for information had no effect on depression.
Patient differences in preference for behavioral involvement had no significant effect on
depression.
The effects of religious coping on adjustment were investigated in renal transplant
patients and significant others by Tix and Frazier (1998). Results suggested that there
was an overall positive relationship between religious coping and psychological
adjustment. Religious coping at three months was related to greater life satisfaction at
three and 12 months for patients and significant others and to less distress at three months
for significant others. Religious coping was associated with less distress and more life
satisfaction for Protestant significant others than for Catholic significant others. For all
samples, cognitive restructuring, social support, and perceived control, whether
considered independently or together, did not account for the significant effects of
religious coping. It seemed that religious coping was positively correlated to life
satisfaction for both renal transplant patients and significant others. Religious coping
benefited Protestant significant others more than Catholic significant others in relation to
psychological adjustment. Martin and Sachse (2002) also discussed that female
36
transplant patients with higher levels of spiritual perspective had higher levels of spiritual
religious well-being and existential well-being.
Frazier, Davis-Ali, and Dahl (1995) investigated stressors, social support, and
adjustment in kidney transplant patients and their spouses. Patient and spouse adjustment
was assessed using standardized measures � the Dyadic Adjustment Scale (DAS)
(Spanier, 1976) and the Beck Depression Inventory (BDI) (Beck et al., 1961). Patients
reported receiving significantly more helpful behaviors, which involved concern and
support, than unhelpful behaviors, which involved criticism, over-concern, and advice
giving, from their spouses. Patients who received more helpful support were more
satisfied with their marriages and were less depressed; those who received more
unhelpful support were more depressed than patients who received less unhelpful support.
The strongest predictor of patients� marital satisfaction was the amount of helpful support
they received from their spouses and the second was stress level, while the strongest
predictor of patients� depression was their total amount of stress. Patients who were
experiencing higher stress benefited more from the support they received from their
spouses. For spouses, total stress was negatively correlated with marital satisfaction and
positively correlated with depression. Spouses who were more stressed offered less
helpful and more unhelpful support than spouses who were less stressed. Helpful support
from a spouse has a positive correlation with adjustment, and family support may have
the same function.
Christensen et al. (2002) examined the effect of family environment and donor
source on patient HRQOL following renal transplantation. The Family Relationships
Index from the Family Environment Scale (FES) (Moos & Moos, 1986) was used as a

37
measure of family support. The Beck Depression Inventory (BDI) (Beck et al., 1961)
and the Sickness Impact Profile (SIP) (Bergner et al., 1981) were used to assess patient
emotional distress and HRQOL respectively. FES scores were initially lower in the
cadaveric-donor group, but increased significantly after transplant, while FES scores
were initially higher in the living-donor group and remained unchanged after transplant.
BDI scores and Scores on the SIP Recreational Functioning Scale decreased significantly
from pre-transplant to post-transplant in both groups. Post-transplant depression levels
were nearly identical for both groups. The interaction of donor source and family
environment was a significant predictor of change in depression and HRQOL. Patients
who received a kidney from a living donor and who also reported a more supportive
family environment exhibited a reduction in depression, improved mobility, and
improved social functioning from pre-transplantation to post-transplantation. In contrast,
those living-donor recipients with less family support exhibited slightly increased
depression and diminished mobility and social functioning after transplantation. Among
patients receiving a cadaveric renal graft, those with high versus low levels of family
support showed similar reductions in depression and modest improvements in HRQOL.
In summary, total stress was negatively related to HRQOL in renal transplant
patients. Total stressor scores were positively correlated to total affective-oriented
coping scores. High preference for health-related information was related to reduction in
depression among renal transplant patients. Overall, religious coping was related to
greater life satisfaction for patients and less distress for significant others. Patients with
more helpful support were more satisfied with their marriages and were less depressed.
38
A more supportive family environment predicted improved mobility and improved social
functioning post-transplantation among living-donor recipients.
Summary of these coping studies. Findings showed that renal transplant patients
experience stress after transplantation. Fear of rejection, side effects of medications,
uncertainty about the future, cost, and the possibility of repeated hospitalizations are the
main stressors. Renal transplant patients tend to use optimistic, self-reliant, self-control,
supportive seeking, problem-solving, and religious coping strategies to deal with
transplant-related stress, whereas escape/wishful thinking, evasive, emotive, fatalistic
coping and affective-oriented coping were used less frequently. It also is suggested that
renal transplant patients regard problem-oriented coping as more effective than emotive
coping. Some studies found that stress was negatively related to HRQOL in renal
transplant patients. Total stressor scores were positively correlated to total affective-
oriented coping scores. Religious coping, information seeking, helpful support, and
family support were positively correlated with HRQOL in renal transplant patients, while
evasive, emotive, and fatalistic coping were associated with low perceived efficiency in
handling various aspects of illness.
The relationships among stress, coping, and HRQOL in renal transplant patients
are not well documented. Some studies described the stress, coping and QOL of renal
transplant patients, but they did not link them together. Most studies focused on only one
aspect of coping and correlated it only to psychological adjustment. In some prospective
studies, coping strategies were measured at one time point; thus, the changes in coping
cannot be identified. Different labels of coping strategies and different instruments
measuring coping were used, and patients at different stages post-transplant were

39
assessed in these studies, thus making it difficult to compare and reach conclusions across
studies. Appraisals of transplantation in renal transplant patients were not mentioned in
these studies. Factors influencing coping in renal transplant patients were not addressed
either. Instruments used to measure QOL/ well-being were not satisfactory. Quality of
life is a multidimensional concept, but some researchers measured it using one question.
Inadequate sample size in some studies and cross-sectional design are other limitations.
Most studies investigated only renal transplant patients less than one year after
transplantation.
Synthesis of Conceptual and Methodological Knowledge of Coping and Health-related Quality of Life in Renal Transplant Patients
Strengths and Weaknesses of Conceptual Approaches
Several researchers presented definitions of HRQOL in renal transplant patients.
There was agreement that HRQOL is a multidimensional, subjective construct including
physical, psychological, and social domains. HRQOL also was related to individual
goals, expectations, values, and concerns by some researchers. The psychosocial
dimension was considered fundamental to renal transplant patients� HRQOL. Some
researchers pointed out that renal transplant patients� subjective appraisals of side effects
of immunosuppressive regimens and functional capacities should be included in
evaluating HRQOL. However, there was no elaborated conceptual framework of
HRQOL in renal transplant patients. Only one framework on HRQOL in transplant
patients was provided by Hathaway and colleagues (2003). This framework needs
further evaluation with renal transplant patients. Based on the literature, HRQOL in renal

40
transplant patients may be the perceptions of the impacts of renal transplantation on their
functioning and wellbeing, which includes physical, psychological, and social domains.
A few researchers used Lazarus and Folkman�s (1984) definition of coping and
mentioned Lazarus and Folkman�s (1984) Stress and Coping Model in their studies.
However, this model was not well applied in these coping studies. Appraisal as a key
component in Lazarus and Folkman�s model was not addressed in these coping studies.
Factors influencing appraisal and coping were not mentioned either. Some researchers
defined religious coping and spirituality, but they did not incorporate them into a
framework. Coping in renal transplant patients was not well defined and there is no
framework to link coping and HRQOL in renal transplant patients in these studies.
A framework, which incorporated Lazarus and Folkman�s Stress and Coping
Model and Social Cognitive Theory on self-efficacy, and social support, may be useful to
renal transplant studies. Applying this framework, the cognitive appraisal of renal
transplantation would influence patients� coping behaviors, and then affect their HRQOL.
Self-efficacy as a personal coping resource may affect renal transplant patients� appraisal
of their conditions, and then their coping behaviors. As coping resources, social support
may precede the coping process through influencing appraisals and coping efforts. Social
support may enable renal transplant patients to use effective coping strategies by helping
them understand the situation faced and reducing emotional stress, helping them have a
positive appraisal of their health condition, and increasing their motivation to perform
positive health behaviors; thus improving their HRQOL.

41
Strengths and Weaknesses of Methodological Approaches
The HRQOL of renal transplant patients was well documented and demonstrated
that renal transplant patients had better HRQOL than before transplantation. Clinical
factors such as comorbidities, adverse effects, time since transplant, treatment type, and
donor type have been investigated and shown to be correlated to patients� HRQOL.
However, there is a lack of homogeneity of the groups of patients compared in most QOL
studies. A variety of questionnaires were used, and studies were conducted with major
differences in cultural patterns and durations of follow up. It was not mentioned if the
researchers used power analyses to determine the sample sizes in the reviewed studies.
Personal and psychosocial factors influencing QOL also were not well documented in
these QOL studies.
It is well recognized that renal transplant patients experience stress after
transplantation. The stressors of most concern have been identified, which are cost, fear
of rejection, side effects of medications, uncertainty about the future, compliance with a
complex regimen, and repeated hospitalizations. Renal transplant patients tend to use
optimistic, supportive, self-reliant coping, religious coping, and problem-oriented coping
to cope with the stressors. Affective-oriented coping, escape/wishful thinking, and
emotive coping are used less frequently. It also is suggested that renal transplant patients
regard problem-oriented coping as more effective than emotive coping. Some studies
indicated that stress was negatively related and coping was positively related to HRQOL
after transplantation. Overall, religious coping, information seeking, helpful support, and
family support were positively correlated with psychological adjustment in renal
transplant patients.

42
Most coping studies used small sample sizes, assessed renal transplant patients at
different stages post-transplant, used different instruments to measure coping and
HRQOL, and focused on only one aspect of coping (e.g., religious coping). All of these
differences/factors made it difficult to compare and integrate the results across studies.
Obviously, studies on coping and HRQOL of renal transplant patients focus more on the
effects of coping on psychological well-being. There is a need for systematic
examination of the relationships among stress, coping, and HRQOL in a study with a
larger sample size. Factors influencing coping in renal transplant patients were not
addressed in these studies. There also is no well-developed instrument designed to
measure coping in this specific population.
Gaps in the Literature
Research on coping in renal transplant patients is in its initial stage, although
HRQOL of renal transplant patients has been maturing. A theoretical framework for
studying coping and HRQOL in renal transplant patients has not been well developed.
Some coping studies mentioned Lazarus and Folkman�s (1984) Stress and Coping Model.
However, they did not apply or strictly follow this model. Appraisal and coping
processes are the central concepts in this model. No researchers assessed appraisals of
renal transplant patients in their studies. Personal and situational factors that influence
the appraisal processes were not addressed in these studies. Appraisal is the cognitive
mediator that affects coping in stressful situations. If we do not know how patients
appraise their situation, it is difficult for us to interpret why patients use different coping
strategies. Coping as a process is also context specific. Reviewed studies used different
43
instruments to measure coping, and they did not mention if the instruments were
modified to be specific to renal transplantation. Specific measurement of coping in renal
transplant patients needs to be developed. Additionally, coping is multidimensional and
multifunctional, and people use different coping strategies to deal with a stressful
encounter. In the overall coping process, coping strategies are interdependent and work
together; thus, studies focused only on one aspect of coping were incomplete.
Most studies only linked coping to psychological adjustment, such as depression.
Effects of coping on behavioral, physiological, or objective health-related outcomes were
not well addressed. Some studies examined the relationship between coping and QOL;
however, QOL was not defined and the instrument used to measure QOL did not capture
the multidimensional characteristics of QOL. Intervention studies related to helping renal
transplant patients cope effectively with stressful situations were not found in the
reviewed literature.
Most studies used convenience sampling methods with small sample sizes. Some
studies included renal transplant patients at only one stage post-transplant (e.g., six
weeks, six months); thus, these studies cannot compare coping strategies and HRQOL at
different stages post-transplant.
Proposed Conceptual Framework
Theoretical and methodological limitations in the studies of coping and HRQOL
in renal transplant patients were identified in the reviewed literature. Efforts are made to
address some of these limitations in this study. Considering the lack of a specific
theoretical framework for studying coping and HRQOL in renal transplant patients, a

44
particular conceptual model was proposed. Based on the findings of the literature,
Lazarus and Folkman�s (1984) Stress and Coping Model integrated with Social Cognitive
Theory on self-efficacy, and literature on social support and HRQOL served as the
theoretical basis for this proposed model (Figure 1).
Figure 1: Proposed Model of Coping and HRQOL in Renal Transplant Patients (Modified from Lazarus and Folkman�s (1984) Stress and Coping Model)
Cognitive Appraisal of Health Primary-Secondary-
Coping Strategy Problem-focused Emotion-focused
Perceived Self-efficacy
Perceived Social Support
Health-related Quality of Life Perception of functioning and well-being: Physical, Psychological, Social domains
Renal Transplantation History of transplant-related hospitalizations Side effects of immunosuppressive medications Donor type Duration of dialysis Time post-transplant

45
In this proposed model, coping is defined as a process and the way in which
individuals apply their coping options depends on the cognitive appraisal of renal
transplantation. Personal variables, also called �personal coping resources� (e.g.,
perceived self-efficacy), and situational variables (e.g., perceived social support) affect
patients� cognitive appraisal, and their coping behaviors. An individual�s coping is
constantly changing in response to external demands and subjective appraisals.
Effectiveness of coping depends on the fit between coping strategies and the situation.
Choices of coping strategies are related to HRQOL of renal transplant patients. Health-
related quality of life is defined as the subjective assessment of the impact of renal
transplant across the physical, psychological, and social domains of functioning and well-
being.
According to the literature, renal transplant patients live with chronic conditions,
face many new challenges, and experience continuing stresses. They have the risk of
kidney rejection, must take immunosuppressive medications with side effects and high
cost, need ongoing follow-up and repeated hospitalization, and are uncertain about the
future. Patients� cognitive appraisal of these conditions would affect their coping
behaviors. Renal transplant patients� perceived self-efficacy gives them a sense of
control over their conditions, thus influencing their appraisals. Patients who have or
perceive a high level of self-efficacy may believe they can control the situation and may
not appraise transplantation as extremely stressful. In addition, a sense of one�s own
ability motivates one to act and to choose and perform more challenging tasks; therefore,
perceived self-efficacy also affects the coping strategies patients use. Patients who have
a high level of self-efficacy may use more problem-focused coping strategies.

46
Renal transplant patients do not live in a vacuum, and environmental variables
have effects on their coping. Social support is one of the most significant factors.
Studies in cancer patients suggested that perceived social support not only enhances
specific coping efforts directly but also influences the appraisal processes (Komproe et al.,
1997; Ptacek et al., 2002). In the early post-transplant period, renal transplant patients
need to obtain information on self-care, medications, and follow-up regimens, and need
to attend hospital clinics. They cannot go to work and/or shoulder the responsibility for a
family. They need support from medical professionals, family, and friends. Social
support offers resources, referrals to professional services, encouragement to seek
assistance, provision of information and problem-solving techniques. Patients who
perceive high levels of social support may tend to use adaptive coping strategies and may
have better HRQOL.
Research Questions
The purposes of this study were to examine relationships among measures of
coping and HRQOL in renal transplant patients, and to identify factors influencing the
coping process. Based on the knowledge derived from the reviewed literature on coping
and HRQOL, a conceptual model was proposed and the following research questions
were addressed in this study.
Research Questions
1. Does the hypothesized model fit the data following renal transplantation?

47
2. What are the effects of clinical factors (donor type, history of transplantation
related hospitalizations, side effects of immunosuppressive medications, duration of
dialysis, and time post-transplantation) on perceived self-efficacy, perceived social
support, cognitive appraisal of health, coping, and HRQOL following renal
transplantation?
Hypotheses
1. Perceived self-efficacy has both direct and indirect effects on coping, and
exerts a direct effect on cognitive appraisal of health.
2. Perceived social support exerts both direct and indirect effects on coping, and a
direct effect on cognitive appraisal of health.
3. Cognitive appraisal of health has a direct effect on coping strategies.
4. Coping strategies have a direct effect on HRQOL.
5. Clinical factors related to renal transplantation have direct effects on cognitive
appraisal of health.
Definition of Terms
Cognitive appraisal of health. Cognitive appraisal of health was defined as the
process by which an individual evaluates or judges a potential health problem for
meaning and significance to their well-being, and is composed of both primary and
secondary dimensions (Lazarus & Folkman, 1984).

48
Coping. Coping was defined as constantly changing cognitive and behavioral
efforts to manage specific external and/or internal demands that are appraised as taxing or
exceeding personal resources (Lazarus & Folkman, 1984).
Perceived Self-efficacy. Perceived self-efficacy was defined as the belief that one
is capable to organize and execute a course of action to attain what is desired (Wallston,
2001).
Perceived Social Support. Perceived social support was defined as the belief in
the availability of support including attachment/intimacy, social integration, nurturance,
reassurance of worth, and assistance (Weiss, 1974).
Health-related Quality of Life (HRQOL). Health-related quality of life was
defined as the subjective assessment of the impact of disease and treatment across the
physical, psychological, social domains of functioning and well-being (Revicki et al.,
2000).

49
CHAPTER III
METHODOLOGY
The purpose of this chapter is to describe the methodology used in this study of
coping and HRQOL of renal transplant patients. Study design, description of research
setting, sample and sampling plan, data collection methods, and data analysis procedures
are presented.
Study Design
A descriptive, correlational, cross-sectional design with a sample that includes
patients at two distinct periods post-transplant (early [less than 1year] and later [1 to 3
years post transplant]) was used in this study to examine coping and HRQOL in renal
transplant patients and to test the proposed model. In this study, cognitive appraisal of
health, perceived self-efficacy, perceived social support, coping strategies, and HRQOL
were measured using self-report instruments. Demographic and clinical factors also were
included.
Research Setting
This study was conducted at a major transplant center located in the Southeastern
Unites Sates. The center draws patients from Middle Tennessee, Southern Kentucky, and
Northern Alabama.

50
Sample and Sampling Plan
Sample Characteristics
The target population of this study was adult renal transplant recipients. The
accessible population was renal transplant recipients who are managed at the Vanderbilt
Transplant Center. Participants who met the following inclusion criteria were invited to
participate in the study: (1) at least 18 years of age; (2) had received a renal transplant on
only one occasion; (3) with a functioning kidney graft (defined as not needing dialysis
support) at the time of enrollment; (4) had a clinic appointment that is at one of the
following periods: less than 1 year post-transplant, and 1 to 3 years post-transplant at the
time of enrollment; (5) able to read and understand English.
Potential participants were excluded if they had received more than one renal
transplant; if they had received another organ or tissue transplant (e.g., liver, pancreas,
and stem cell); if they presented with a failed graft (requiring dialysis support) at the time
of enrollment; if they were unable to read English; or if they declined to participate.
Previous transplant experience may influence how patients perceive their illness, appraise
their conditions, and then the selection of their coping strategies. Patients with a failed
kidney graft may return to dialysis, and they have different situations and experience
different stresses. Participants with these conditions were excluded to avoid potential
confounds. Participants who did not read English could not be included because of the
study�s reliance on English language-based survey instruments and the unavailability and
expense of translation services.

51
Sample Size
Convenience sampling was used to recruit participants. A multiple regression-
based approach model was used to conduct the power analysis in order to determine the
number of observations required to achieve either an incremental or cumulative squared
multiple correlation coefficient (R2) within a target range assuming a given number of
predictor variables. On the basis of previous studies conducted in this transplant center, a
moderate effect (cumulative R2 = 0.14-0.17) would be expected, and the target sample
size was identified accordingly. One hundred and sixty participants were included in this
study with 141 participants who had complete data being included in the multivariate
models. With a maximum of 10 variables in any regression model, cumulative R2 = 0.15
(moderate effect), alpha set at 0.05 (two tailed), and sample size of 140, the power of this
study was 0.94 (Borenstein et al., 1997).
Recruitment
The principal investigator and data manager queried the Patient Analysis and
Tracking System (PATS) database weekly to identify eligible patients, and provided
appropriate survey packets to the renal transplant clinic staff. Eligible patients were
given a survey packet at the time of check-in to the clinic and were asked to return it
before leaving. As described in the IRB-approved cover letter, patients were not
obligated to complete survey packets. A knowledgeable clinic staff member (e.g.,
transplant nurse coordinator) was available to answer questions that patients may have
had about the surveys or the research program.

52
Data Collection Methods
Instruments
Each of the key constructs in the proposed model was measured using self-report
instruments. In the following section, a description of each of the instruments used to
measure cognitive appraisal of health, perceived social support, perceived self-efficacy,
coping strategies, and HRQOL is provided. Instruments were selected on the basis of
their applicability for self-report, published reliability and validity, and limited response
burden. Demographic characteristics and clinical factors related to renal transplant are
also described.
The Cognitive Appraisal of Health Scale (CAHS) (Appendix A). The CAHS
(Kessler, 1998) is a self-report instrument developed to measure primary and secondary
appraisals associated with potentially stressful health-related events. It is derived from
Lazarus and Folkman�s Stress and Coping Model. The CAHS contains 28 items with
four separate scales measuring the primary appraisal dimensions of threat (5 items),
challenge (6 items), harm/loss (8 items), benign/irrelevant (4 items), and 5 items
measuring the secondary appraisal dimensions of coping options and resources. Four out
of the five items measuring secondary appraisal were developed by Folkman et al. (1986);
one was added by Kessler (1998). All items are scored on a 5-point Likert scale ranging
from 1 (strongly disagree) to 5 (strongly agree). Higher scores indicate more agreement
with the appraisal item or scale. The CAHS was tested with a breast cancer sample and
demonstrated sound reliability and validity. The internal consistency of each of the
primary appraisal scales was greater than 0.70 (threat 0.85, challenge 0.72,
53
benign/irrelevant 0.78, and harm/loss 0.88) (Kessler, 1998). The psychometric
evaluation also was investigated with prostate cancer patients (Ahmad, 2005). The 13-
item three-factor model of CAHS was supported. The Cronbach�s alphas for the three-
factor were 0.79 for harm/loss appraisal, 0.74 for threat appraisal, 0.70 for challenge, and
0.70 for the total scale (Ahmad, 2005).
The CAHS with 28 items (Kessler, 1998) was used in this study. Preliminary
factor analysis was conducted and a weighted single composite scale score was used as a
predictor in the path analyses and as a criterion measure in analysis of variance-based
models.
Personal Resource Questionnaire (PRQ 2000) (Appendix B). The PRQ2000
(Weinert, 2000) has been revised from the PRQ85 (Weinert, 1987) and the Personal
Resource Questionnaire (Brandt & Weinert, 1981) to measure perceived level of social
support. It is a self-administered instrument composed of 15 items on a 7-point Likert
scale. The conceptual framework is based on Weiss�s (1969, 1974) model of relational
functions. The item responses range from 1 (strongly disagree) to 7 (strongly agree).
Scores of the 15 items are summed to calculate the total score, which ranges from 15 to
105, with higher scores indicating higher levels of perceived social support. The internal
consistency reliability ranged from 0.87 to 0.93 in various samples with chronic illness,
such as multiple sclerosis, cancer, and cardiac disease (Weinert, 2003). Preliminary
construct validity estimates are similar to those found for the PRQ82 and PRQ85
(Weinert, 2003).
Perceived Health Competence Scale (PHCS) (Appendix C). The PHCS (Smith et
al., 1995) is a valid and reliable measure of perceived self-efficacy relevant to one�s

54
health in general. It measures the degree to which one feels competent to effectively
manage one�s health outcomes. The PHCS is an eight-item scale that asks the subjects
about their level of agreement with phrases such as, �I handle myself well with respect to
my health,� and �Typically, my plans for my health don�t work out well.� Level of
agreement is measured with a Likert response scale with possible responses ranging from
�Strongly disagree� (1) to �Strongly agree� (5). Negatively-valenced items are reverse
scored before summing across all eight items. The psychometric properties of the
instrument are supported by data from five studies of both healthy and chronically ill
adult subjects (Smith et al., 1995). The internal consistency of the scale ranged from 0.82
to 0.90. Stability estimates varied from 0.82 over a one-week interval for healthy
undergraduates, to 0.60 over approximately 2.5 years among persons with arthritis (Smith
et al., 1995). The PHCS also demonstrated sound predictive validity and convergent
validity within these samples (Smith et al., 1995).
Brief COPE (Appendix D). The Brief COPE (Carver, 1997) is the abbreviated
version of the COPE inventory (Carver, Scheier, & Weintraub, 1989). The Brief COPE
consists of 14 scales with 2 items each, assessing different coping dimensions: 1) active
coping, 2) planning, 3) using instrumental support, 4) using emotional support, 5) venting,
6) behavioral disengagement, 7) self-distraction, 8) self-blame, 9) positive reframing, 10)
humor, 11) denial, 12) acceptance, 13) religion, and 14) substance use. Ratings are made
on a four-point Likert scale: 1=I did not do this at all, to 4=I did this a lot. This inventory
is built from acknowledged theoretical models (Lazarus & Folkman� Stress and Coping
Model, 1984; Behavioral Self-regulation Model, Carver & Scheier, 1981, 1990). It can
be used to assess trait coping (the usual way people cope with stress in everyday life) and
55
state coping (the particular way people cope with a specific stressful situation). As the
COPE inventory, the Brief COPE is a measure used for many health-relevant studies:
drugs addiction, aging, breast cancer, depression, AIDS. The internal consistency alpha
ranged from 0.50 to 0.90 for the 14 scales. All exceeded 0.60 except for Venting, Denial,
and Acceptance (Carver, 1997). The state version of this inventory will be used. The
directions for this inventory will be modified to fit the renal transplant condition. The
substance use subscale will not be used in this study because it does not fit the clinical
situation of this population. Renal transplant patients take many medications and the
questions in the substance use subscale may be very confusing. Preliminary factor
analysis was performed to determine the composition of the second-order factors of this
inventory. Two distinct second-order factors (engagement coping and disengagement
coping strategies) were identified and individuals� weighted scores on these second-order
factors were used in the path analyses and as criterion measures in analysis of variance-
based models.
Medical Outcomes Study 36-item Short Form Health Survey (SF-36®) (Appendix
E). The SF-36® is one of the most widely used and validated instruments for the
measurement of generic, self-reported HRQOL. Eight subscales, physical functioning
(PF), role physical (RP), bodily pain (BP), general health (GH), vitality (VT), social
functioning (SF), role emotional (RE), and mental health (MH), are generated as unit-
weighted sums of specific item scores. After standardizing these scales to z-scores based
on means and standard deviations for the general US population, aggregate physical and
mental component summary scales (the PCS and MCS, respectively) are computed by
summing across the eight differentially weighted scales. In the final step, each

56
component score is transformed to a normalized T-score having a mean of 50 and
standard deviation of 10. Higher scores represent better quality of life. Cronbach's alpha
coefficient of this measurement ranged from .65 to .94, and the test-retest correlation
coefficients was .65 to .97 in other populations (Ware, 1997). The SF-36® has been
frequently used in kidney transplant population studies. Cronbach's alpha coefficients
were 0.76 for PCS and 0.80 for MCS in a previous study at the Vanderbilt Transplant
Center (Feurer et al., 2004).
Demographic and Clinical Data (Appendix G). Demographic characteristics and
related clinical information were collected through the Patient Analysis and Tracking
System (PATS) and clinical databases. It included gender, age, race, level of education,
marital status, original cause of ESRD, type of dialysis, duration of dialysis before
transplant, donor type, relationship of living donor, time post-transplant, current
immunosuppressive medications, history of rejection episodes (grade and date of
diagnosis), and number of transplant-related hospitalizations. Additionally, data specific
to the side effects experienced related to the immunosuppressive medications were
assessed using a symptom checklist developed by the investigator, clinical experts, and
the committee (Appendix F). It includes a list of 12 symptoms of side effects of
immunosuppressive medications. Participants were asked to indicate if they were
currently experiencing the symptoms, and if yes, how bothersome each symptom was (0=
No symptoms, 1 = Yes, but bothers me not at all, 2 = bothers me slightly, 3 = bothers me
moderately, 4 = bothers me quite a bit, to 5 = bothers me extremely). Preliminary factor
analysis was performed and a one-component solution was derived. A single composite
score was used in subsequent analyses.

57
Procedures
After the study was approved by the IRB, subject recruitment began. The
principal investigator prepared survey instruments. Only packet identification codes
appeared on the surveys, which contained no personally identifying information. The
clinic setting used for the study regularly collects information from patients at specific
monitoring points (e.g., 3 months, 6 months, and annually post transplant). The
questionnaires for this study were embedded in the survey packets distributed to patients
willing to complete the forms. All pages comprising a packet of surveys were pre-
printed so that a large volume of packets was able to be prepared in advance. Survey
packets and a cover letter with description of the project, response confidentiality, the
consent procedure, and contact information were packaged in unsealed envelopes.
The principal investigator and Transplant Center QOL data manager queried the
PATS database weekly and prepared appropriate survey packets and delivered them to
the clinical staff for distribution. Packets were distributed at the time of check in and
patients were invited to participate, as explained in a cover letter. As explained in the
cover letter, patients are not required to participate and may consent to participate by
completing and returning the surveys. Knowledgeable clinic staff (e.g., transplant nurse
coordinator) was present at the clinic to answer patients� questions.
Completed survey packets were stored in secured cabinets. The principal
investigator double-entered the survey data into a password protected, Excel-based data
set that was backed up on the secure Transplant Center data storage �drive�.
Information linking the packet and patient identifiers, and dates of distribution and
58
return, was maintained in a log that was kept in a secure location by the principal
investigator and electronically by the data managers as a separate PATS data set.
Human Subjects� Protection
Study participation was open to both women and men of all ethnic or racial
groups. No one was excluded based upon gender, race, or ethnicity. There were no
anticipated potential risks to participants involved in this study. Participants may have
been inconvenienced by the time required for questionnaire completion, and the impact
of response burden was assessed during the initial phase of data collection. The nature of
the research was explained in an IRB-approved cover letter to potential participants,
along with the fact that data are confidential, participation is voluntary, and that choosing
not to participate would not influence clinical care. Protection against possible breaches
of confidentiality derived from several factors: 1) survey data did not contain any
personally identifying information; 2) surveys packets had pre-printed packet
identification codes; 3) surveys were returned in sealed envelopes; 4) a separate data set
linking patient identifiers to survey packet identifiers was maintained; 5) all data
managers and persons who analyzed the data have approved access to necessary records
and routinely work with and protect the confidentiality of sensitive medical records; 6) all
computers and confidential data bases were password protected. Individual participants
may not have benefited from participation. However, an improved understanding of
coping and HRQOL following renal transplantation has the potential to benefit renal
transplant patients and their families through its impact on post-transplant clinical care.
59
Adherence to study protocol was verified by the PI and any deviations or reasons
for drop out were documented and discussed with the dissertation chair. The PI and the
biostatistician met, at a minimum, every other week to discuss the progress of recruitment
and any issues regarding safety to the participants. The PI also periodically checked the
documentation to assess for any unanticipated problems. There were no unanticipated
and/or serious events that needed to be reported to the IRB per IRB requirements.
Data Analysis Procedures
Statistical analyses were performed using the SPSS-PC (v14.0) and AMOS (v6.0)
statistical packages. Prior to data analysis, each variable was examined using frequency
distributions and visual representations, such as histograms or boxplots, to identify any
outliers, missing values, coding errors. Distribution characteristics including tests of
Normality also were examined. If any unusual or missing values were identified, the raw
data were reexamined to rectify any data collection or entry errors. After cleaning and
verifying the raw data, complete data were available on 141 participants for the path
analyses and 143 participants for the ANOVA models. Because there were few missing
values (≤ 12%), the path analyses and analysis of variance-based models were conducted
using observations having complete data. Other analyses were performed using data
from participants who had complete data on the particular variable of interest.
Distribution of the data was explored. Some subscales of Brief COPE were identified as not
being normally distributed, and the weighted second-order factor scores were used for
analyses. Following data cleaning, descriptive statistics (e.g., percentages, means, standard
deviations) were used to describe the sample. An indexed table was used to display the
demographic characteristics of the sample. Descriptive statistics were also used to
60
summarize the study variables. Internal consistency reliability of the major instruments such
as CAHS, Brief COPE, PRQ2000, PHCS, and HRQOL were examined. Second-order factor
analysis was conducted on the four CAHS subscales and the 13 Brief COPE scales for the
purpose of discerning the factor structure of these instruments and deriving weighted
composite scores (for each of these instruments) for application in the subsequent path
analyses and analysis of variance-based models. Multiple regression-based path analysis,
multivariate analysis of covariance (MANCOVA), and multivariate analysis of variance
(MANOVA) were used to analyze the data to answer research questions.
Research question 1. Does the hypothesized model fit the data following renal
transplantation?
For this question, a series of nested path analyses were used to test the initial,
alternative, and hypothesized models. Procedures for performing path analysis are
described in the following section.
Preparation for the Path Analysis
The zero-order correlations among model variables were examined. Dichotomous
variables such as donor type (living vs cadaveric) were dummy coded before analysis.
History of transplant-related hospitalizations was categorized as no hospitalization and
having hospitalizations following transplantation. Duration of dialysis before
transplantation also was categorized as less and equal 6 months and more than 6 months.
Variables in the correlation matrix are listed below.
Renal transplantation related variables: History of transplant-related hospitalizations,
side effects of immunosuppressive medications, donor type, duration of dialysis, and time
post-transplant.

61
Perceived self-efficacy
Perceived social support
Cognitive appraisal of health: One second-order factor-CAHS composite.
Coping strategies: Two second-order factors-engagement coping strategies and
disengagement coping strategies.
HRQOL: Physical component summary and mental component summary.
Initial model. An initial model which posits the largest number of direct and
indirect effects was developed (Figure 2). In this model, there are five exogenous, renal
transplantation-related variables (history of transplant-related hospitalizations, side
effects of immunosuppressive medications, donor type, duration of dialysis, and time
post-transplant) and six endogenous variables: HRQOL (PCS or MCS), which is
completely endogenous and is therefore affected by all exogenous (transplant-related)
variables and all other endogenous variables (perceived self-efficacy, perceived social
support, cognitive appraisal of health, and engagement and disengagement coping
strategies); engagement and disengagement coping strategies, which are affected by the
exogenous variables and by perceived self-efficacy, perceived social support, and
cognitive appraisal of health; cognitive appraisal of health, which is affected by the
exogenous variables and by perceived self-efficacy, and perceived social support;
perceived social support, which is affected by the exogenous variables; and perceived
self-efficacy, which is affected by the exogenous, renal transplantation-related variables.
In this model, perceived self-efficacy, perceived social support, cognitive appraisal of
health, and coping strategies exert direct and indirect effects on all subsequent
endogenous variables. The only two effects that are not posited in this model are any

62
direct relationship between perceived self-efficacy and perceived social support, and
between engagement and disengagement coping strategies. The set of multiple
regression equations that collectively represent the initial model are listed below.
(1a) DPCS=a + b1X1 + b2X2 + b3X3 + b4X4 + b5X5 + b6X6 + b7X7 + b8X8 + b9X9 + b10X10
(1b) DMCS=a + b1X1 + b2X2 + b3X3 + b4X4 + b5X5 + b6X6 + b7X7 + b8X8 + b9X9 +b10X10
(2) DCSE=a + b1X1 + b2X2 + b3X3 + b4X4 + b5X5 + b6X6 + b7X7 + b8X8
(3) DCSD=a + b1X1 + b2X2 + b3X3 + b4X4 + b5X5 + b6X6 + b7X7 + b8X8
(4) DCAHC=a + b1X1 + b2X2 + b3X3 + b4X4 + b5X5 + b6X6 + b7X7
(5) DPSE=a + b1X1 + b2X2 + b3X3 + b4X4 + b5X5
(6) DPSS=a + b1X1 + b2X2 + b3X3 + b4X4 + b5X5

63
Figure 2: Initial Model
Alternative model. An alternative model was posited to test whether perceived
self-efficacy and perceived social support are exogenous or mediating variables (Figure
3).
8. Cognitive Appraisal of Health Composite-X8
9,10. Coping Strategies Engagement-X9 Disengagement-X10
6. Perceived Self-efficacy-X6
7. Perceived Social Support-X7
Health-related Quality of Life Physical Component Summary (PCS) or Mental Component Summary (MCS)
Renal Transplantation-related correlated Exogenous Variables 1. History of transplant-related hospitalizations-X1 2. Side effects of immunosuppressive medications-X2 3. Donor type-X3 4. Duration of dialysis-X4 5. Time post-transplant-X5

64
Figure 3: Alternative Model
In this model, renal transplantation-related variables, perceived self-efficacy, and
perceived social support are modeled as correlated exogenous variables. Four
endogenous variables, cognitive appraisal of health, engagement and disengagement
coping strategies, and HRQOL (PCS or MCS) remain. The following set of multiple
regression equations are needed to represent the alternative model. The goodness of fit of
8. Cognitive Appraisal of Health Composite-X8
9, 10. Coping Strategies Engagement-X9 Disengagement-X10
6. Perceived Self-efficacy-X6
7. Perceived Social Support-X7
Health-related Quality of Life Physical Component Summary (PCS) or Mental Component Summary (MCS)
Renal Transplantation-related correlated Exogenous Variables 1. History of transplant-related hospitalizations-X1 2. Side effects of immunosuppressive medications-X2 3. Donor type-X3 4. Duration of dialysis-X4 5. Time post-transplant-X5

65
the alternative model (in relation to its fully saturated counterpart) was tested using the
chi-square statistic and the goodness-of-fit index.
(1a) DPCS=a + b1X1 + b2X2 + b3X3 + b4X4 + b5X5 + b6X6 + b7X7 + b8X8 + b9X9 + b10X10
(1b) DMCS=a + b1X1 + b2X2 + b3X3 + b4X4 + b5X5 + b6X6 + b7X7 + b8X8 + b9X9 +b10X10
(2) DCSE=a + b1X1 + b2X2 + b3X3 + b4X4 + b5X5 + b6X6 + b7X7 + b8X8
(3) DCSD=a + b1X1 + b2X2 + b3X3 + b4X4 + b5X5 + b6X6 + b7X7 + b8X8
(4) DCAHC=a + b1X1 + b2X2 + b3X3 + b4X4 + b5X5 + b6X6 + b7X7
Hypothesized model. A hypothesized model was constructed. It was
hypothesized that perceived self-efficacy has both direct and indirect effects on coping
strategies and direct effects on cognitive appraisal of health; perceived social support has
both direct and indirect effects on coping strategies and direct effects on cognitive
appraisal of health; cognitive appraisal of health has direct effects on coping strategies;
coping strategies have direct effects on HRQOL; and renal transplantation-related
variables have direct effects on cognitive appraisal of health. Figure 4 shows the
hypothesized model. There are four endogenous variables: the fully endogenous variable,
HRQOL (PCS or MCS); engagement and disengagement coping strategies, which are
modeled as mediating the effects of the transplantation-related variables, cognitive
appraisal of health, perceived self-efficacy, and perceived social support on HRQOL; and
cognitive appraisal of health, which is modeled as mediating the effects of all the
exogenous variables on subsequent endogenous variables. Thus, the set of multiple
regression equations needed to represent the hypothesized model are:
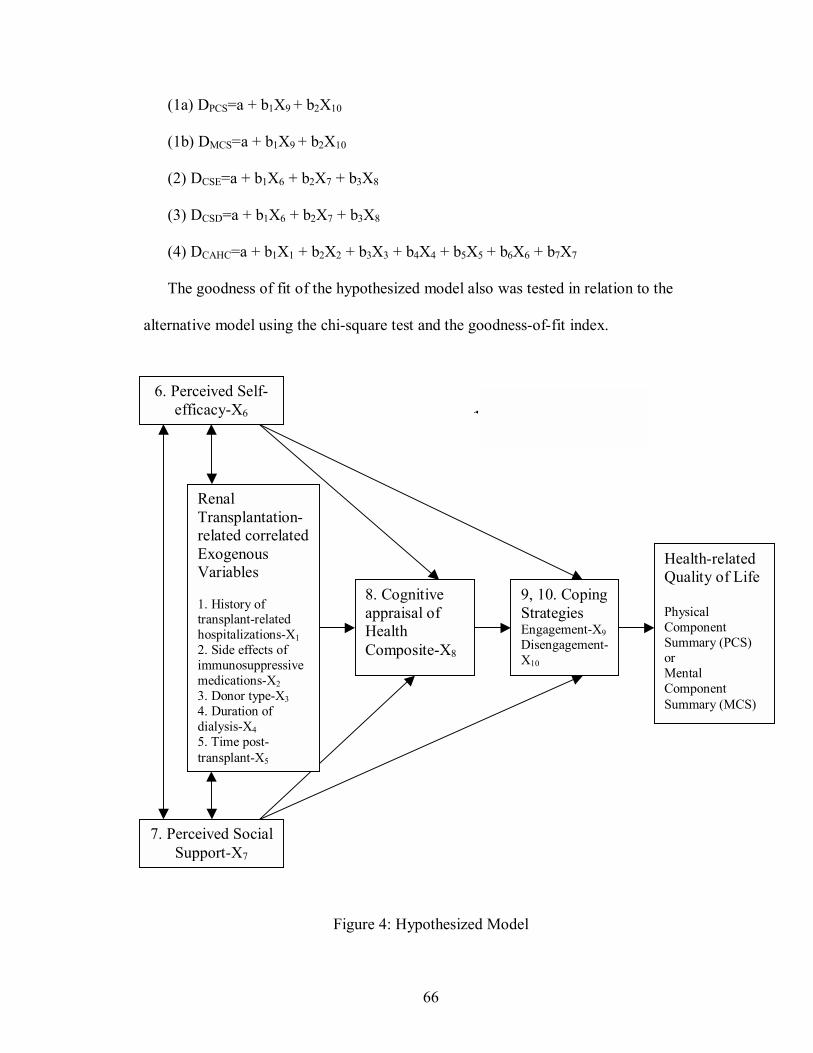
66
(1a) DPCS=a + b1X9 + b2X10
(1b) DMCS=a + b1X9 + b2X10
(2) DCSE=a + b1X6 + b2X7 + b3X8
(3) DCSD=a + b1X6 + b2X7 + b3X8
(4) DCAHC=a + b1X1 + b2X2 + b3X3 + b4X4 + b5X5 + b6X6 + b7X7
The goodness of fit of the hypothesized model also was tested in relation to the
alternative model using the chi-square test and the goodness-of-fit index.
Figure 4: Hypothesized Model
8. Cognitive appraisal of Health Composite-X8
9, 10. Coping Strategies Engagement-X9 Disengagement-X10
6. Perceived Self-efficacy-X6
7. Perceived Social Support-X7
Health-related Quality of Life Physical Component Summary (PCS) or Mental Component Summary (MCS)
Renal Transplantation-related correlated Exogenous Variables 1. History of transplant-related hospitalizations-X1 2. Side effects of immunosuppressive medications-X2 3. Donor type-X3 4. Duration of dialysis-X4 5. Time post-transplant-X5
67
Analysis
A series of nested path analyses were performed to test the initial, alternative, and
hypothesized models. Path coefficients were derived as linear regression coefficients.
Standardized coefficients (β) were reported because they allow comparison of the
absolute (either positive or negative valence) relative magnitude of one path with that of
other paths in the model. Total effects including the direct effects (simple paths) and
indirect effects (compound paths) were calculated.
Research question 2. What are the effects of clinical factors (donor type, history
of transplantation-related hospitalizations, duration of dialysis, side effects of
immunosuppressive medications, and time post-transplant) on the psychosocial variables
and HRQOL?
Multivariate Analysis of Covariance (MANCOVA) was used to address the
effects of donor type (living vs cadaveric), history of transplantation related
hospitalizations (yes vs none), duration of dialysis (≤ 6 months and >6 months), side
effects of immunosuppressive medications (score ≤ 17 and score >17) on cognitive
appraisal of health, perceived self-efficacy, perceived social support, coping strategies,
and HRQOL with the time post-transplant as a covariate. A separate Multivariate
Analysis of Variance (MANOVA) was used to test the effect of time post-transplant (less
than 1 year and 1 to 3 years post-transplant) on these psychosocial variables.

68
CHAPTER IV
RESULTS
This chapter presents the results of the data analyses used to examine the research
questions posed in this dissertation research study. Six principal sections are provided.
In section one, a description of the sample is given including frequencies, percentages,
means, standard deviations, and minimum and maximum scores. Section two presents
the descriptive statistics for each instrument including the instrument�s internal
consistency reliability, means, standard deviation, minimum and maximum scores,
skewness and kurtosis. In section three, the bivariate relationships between observed
variables in the proposed model are presented. Section four addresses the findings for the
path analysis for the test of the hypothesized relationships in the model for coping and
HRQOL. Section five presents the results of data analyses for the second research
question asked in the study. Section six briefly summarizes the chapter.
Description of the Sample
A total of 160 renal transplant patients with 55 in the early post-transplant period
(less than 1 year) and 105 in the later period (1 to 3 years) participated in this study.
Demographic data including age, gender, marital status, race, and level of education
were collected (see Table 1, 2). The convenience sample (N=160) in this study ranged
in age from 18 to 75 years (M=47.7, SD=13.2). The sample consisted of 86 males
(53.8%) and 74 females (46.3%). Approximately 70.6% (n=113) of participants were

69
married, while the remaining participants were single (n=31, 19.4%), widowed (n=4,
2.5%), separated (n=3, 1.9%), or divorced (n=9, 5.6%). The majority of participants
were Caucasian (n=124, 77.5%), with the remaining participants identified as African
American (n=33, 20.6%) or Asian (n=3, 1.9%). Regarding the level of education, the
majority of participants had high school education (n=93, 58.1%), 21.3% (n=34) of
participants attended college, 15% (n=24) of participants had an associate/bachelor�s
degree, and 3.1% (n=5) of participants had a graduate degree.
Table 1. Summary of Participant Demographic Data Variable
Early Group (n=55)
Frequency (%)
Later Group (n=105)
Frequency (%)
Total Sample (N=160)
Frequency (%)
p** Gender Male Female
32 (58.2) 23 (41.8)
54 (51.4) 51 (48.6)
86 (53.8) 74 (46.3)
.416
Age (years) *
46.4 (14.3)
48.4 (12.6)
47.7 (13.1)
.357
Marital Status Married Single Widowed Separated/ Divorced
37 (67.3) 11 (20.0) 1 (1.8) 6 (10.9)
76 (72.4) 20 (19.0)
3 (2.9) 6 (5.7)
113 (70.6) 31 (19.4)
4 (2.5) 12 (7.5)
.718
Race African-American Asian Caucasian
10 (18.2) 1 (1.8)
44 (80.0)
23 (21.9) 2 (1.9)
80 (76.2)
33 (20.6) 3 (1.9)
124 (77.5)
.856
Education Level Less than high school High school Attended college Associated/bachelor
degree Graduate degree
2 (3.6) 28 (50.9) 13 (23.6) 9 (16.4)
3 (5.5)
2 (1.9) 65 (61.9) 21 (20.0) 15 (14.3)
2 (1.9)
4 (2.5) 93 (58.1) 34 (21.3) 24 (15.0)
5 (3.1)
.514
* Data reported are the Mean (SD) ** Type I error probability level for the chi-square or t-test of differences between groups

70
Using chi-squared tests of proportions, with alpha of <.05, no differences were
found between the early period post-transplant and later period post-transplant groups
on gender, marital status, race, and education level. An independent sample t test
demonstrated that there was no difference in age between the two groups.
Clinical data including original cause of ESRD, type of dialysis, duration of
dialysis before transplant, donor type, relationship of living donor, time post-transplant,
current immunosuppressive medications, history of rejection episodes, and number of
transplant-related hospitalizations, were recorded because they are important variables
for the renal transplant population (see Table 2). The major causes of ESRD in this
sample were hypertension (n=41, 25.6%) and diabetes (n=27, 16.9%), followed by adult
polycystic kidney disease (n=16, 10.0%), and IgA nephropathy (n=14, 8.7%). In terms
of type of dialysis, 61.3% (n=98) of participants had hemodialysis and 24.3% (n=39)
had peritoneal dialysis. Approximately 14% of participants received no dialysis before
transplantation. The duration of dialysis before transplantation ranged from 0 to 275
months (M=23.7, SD=32.0), with 70% (n=112) of participants having dialysis more than
six months. More than half of the participants received a living donor graft (n=95,
59.4%) with 37.5% of them biologically-related and 21.9% not biologically-related such
as spouse or friends, while the remaining participants received cadaveric donor graft
(n=65, 40.6%). Regarding current immunosuppressive medications, the majority of
participants (n=103, 64.4%) were taking steroids (prednisone), mycophenolate mofetil
(Cellcept), and tacrolimus (Prograf); 19.4% (n=31) were prescribed prednisone, Cellcept,
and sirolimus (Rapamune); 6.8% (n=11) reported taking prednisone, Cellcept, and
Neoral; and 4.4% (n=7) received the prednisone avoidance protocol (taking Cellcept and

71
Prograf, or Cellcept and Rapamune). Approximately 90% (n=144) of the study
participants had no graft rejection episodes, while 8.8% (n=14) of participants had one
rejection episode and only two (1.2%) participants had two rejection episodes. Because
few participants had rejection episodes in this study, history of rejection was not
included in the regression models and MANOVA analyses. The majority of the study
participants had no transplant-related hospitalizations (n=95, 59.4%), with the remaining
participants hospitalized once (n=41, 25.6%) or more than once (n=24, 15.0%). The
length of time since transplantation was also recorded and ranged from 3 to 43 months
(M=18.8, SD=12.8).
The differences in the clinical data between the early and later period post-
transplant groups also were tested. Results from chi-squared tests indicated that there
were no significant differences in original cause of ESRD, type of dialysis before
transplantation, duration of dialysis (≤ 6 months/ > 6 months), donor type (living/
cadaveric), immunosuppressive medications, rejection episodes, and grade of rejection
between the two groups. However, there was a statistically significant difference in
history of transplant-related hospitalizations (yes/no) between the two groups (p = .013).
The result indicated that more participants in the early group had no history of transplant-
related hospitalizations than participants in the later group. The difference between the
two groups on months of dialysis therapy before transplantation was examined using
independent t test and no difference was found between the early and later period post-
transplant groups.
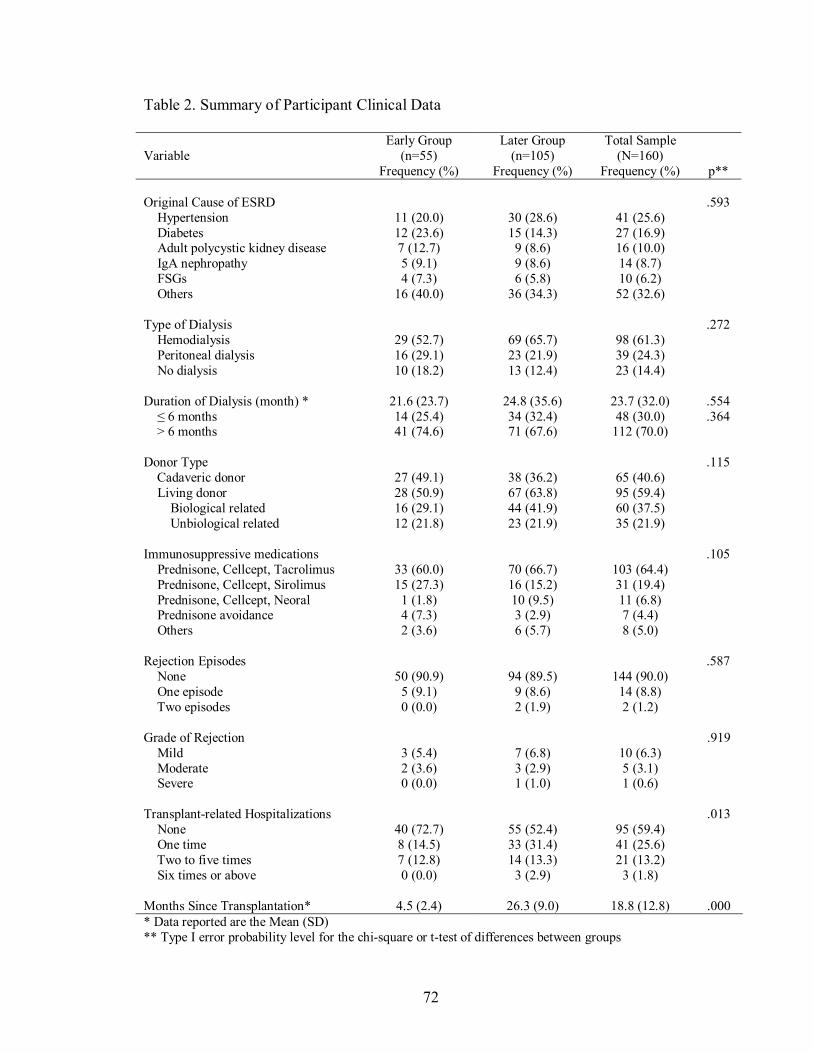
72
Table 2. Summary of Participant Clinical Data Variable
Early Group (n=55)
Frequency (%)
Later Group (n=105)
Frequency (%)
Total Sample (N=160)
Frequency (%)
p** Original Cause of ESRD Hypertension Diabetes Adult polycystic kidney disease IgA nephropathy FSGs Others
11 (20.0) 12 (23.6) 7 (12.7) 5 (9.1) 4 (7.3)
16 (40.0)
30 (28.6) 15 (14.3)
9 (8.6) 9 (8.6) 6 (5.8)
36 (34.3)
41 (25.6) 27 (16.9) 16 (10.0) 14 (8.7) 10 (6.2) 52 (32.6)
.593
Type of Dialysis Hemodialysis Peritoneal dialysis No dialysis
29 (52.7) 16 (29.1) 10 (18.2)
69 (65.7) 23 (21.9) 13 (12.4)
98 (61.3) 39 (24.3) 23 (14.4)
.272
Duration of Dialysis (month) * ≤ 6 months > 6 months
21.6 (23.7) 14 (25.4) 41 (74.6)
24.8 (35.6) 34 (32.4) 71 (67.6)
23.7 (32.0) 48 (30.0)
112 (70.0)
.554 .364
Donor Type Cadaveric donor Living donor Biological related Unbiological related
27 (49.1) 28 (50.9) 16 (29.1) 12 (21.8)
38 (36.2) 67 (63.8) 44 (41.9) 23 (21.9)
65 (40.6) 95 (59.4) 60 (37.5) 35 (21.9)
.115
Immunosuppressive medications Prednisone, Cellcept, Tacrolimus Prednisone, Cellcept, Sirolimus Prednisone, Cellcept, Neoral Prednisone avoidance Others
33 (60.0) 15 (27.3)
1 (1.8) 4 (7.3) 2 (3.6)
70 (66.7) 16 (15.2) 10 (9.5) 3 (2.9) 6 (5.7)
103 (64.4) 31 (19.4) 11 (6.8) 7 (4.4) 8 (5.0)
.105
Rejection Episodes None One episode Two episodes
50 (90.9) 5 (9.1) 0 (0.0)
94 (89.5) 9 (8.6) 2 (1.9)
144 (90.0) 14 (8.8) 2 (1.2)
.587
Grade of Rejection Mild Moderate Severe
3 (5.4) 2 (3.6) 0 (0.0)
7 (6.8) 3 (2.9) 1 (1.0)
10 (6.3) 5 (3.1) 1 (0.6)
.919
Transplant-related Hospitalizations None One time Two to five times Six times or above
40 (72.7) 8 (14.5) 7 (12.8) 0 (0.0)
55 (52.4) 33 (31.4) 14 (13.3)
3 (2.9)
95 (59.4) 41 (25.6) 21 (13.2)
3 (1.8)
.013
Months Since Transplantation*
4.5 (2.4)
26.3 (9.0)
18.8 (12.8)
.000
* Data reported are the Mean (SD) ** Type I error probability level for the chi-square or t-test of differences between groups

73
Description of Instruments
Instrument Reliability
All the main instruments for the research study were tested for internal consistency
reliability using Cronbach�s alpha (see Table 3). Reliability coefficients for most scales
approached or exceeded 0.70 except the benign/irrelevant (α=.53) subscale of CAHS, and
some of the subscales of Brief COPE such as self-distraction (.45), active coping (.50),
behavioral disengagement (.59), positive reframing (.63), and self-blame (.66). It is
important to note that each of the subscales of Brief COPE has only two items.
Descriptive Statistics of the Instruments
Descriptive statistics from the Cognitive Appraisal of Health Scale (CAHS), Brief
COPE, Perceived Health Competence Scale (PHCS), Personal Resource Questionnaire
(PRQ), Medical Outcomes Study 36-item Short Form Health Survey (SF-36®), and the
Symptom Checklist are summarized in Table 4.
CAHS. Cognitive appraisal of health was measured using CAHS. Only the primary
appraisal subscales which include threat, challenge, harm/loss, and benign/irrelevant were
analyzed in this study. Higher scores indicate more agreement with the subscales. Scores
on the four subscales can range from 5 to 25 for the Threat scale, 6 to 30 for the Challenge
scale, 8 to 40 for the Harm/Loss scale, and 4 to 20 for the Benign/Irrelevant scale. In this
study, participant scores ranged from 5 to 23 (M=12.02, SD=3.83) for the Threat scale, 6 to
30 (M=22.84, SD=4.13) for the Challenge scale, 8 to 38 (M=19.75, SD=7.09) for the
Harm/Loss scale, and 4 to 18 (M=10.58, SD=2.95) for the Benign/Irrelevant scale.

74
Table 3. Internal Consistency Reliability of Instruments
Instrument
Cronbach�s Alpha
SF-36 PCS MCS
.78
.81 Brief COPE Self-distraction Active coping Denial Use of emotional support Use of instrumental support Behavioral disengagement Venting Positive reframing Planning Humor Acceptance Religion Self-blame
.45
.50
.72
.72
.71
.59
.72
.63
.68
.88
.70
.86
.66 PHCS (Perceived Health Competence Scale)
.82
PRQ (Personal Resource Questionnaire)
.93
CAHS (Cognitive Appraisal of Health Scale) Threat Challenge Harm/loss Benign/irrelevant
.73
.76
.89
.53 Symptom Survey
.79
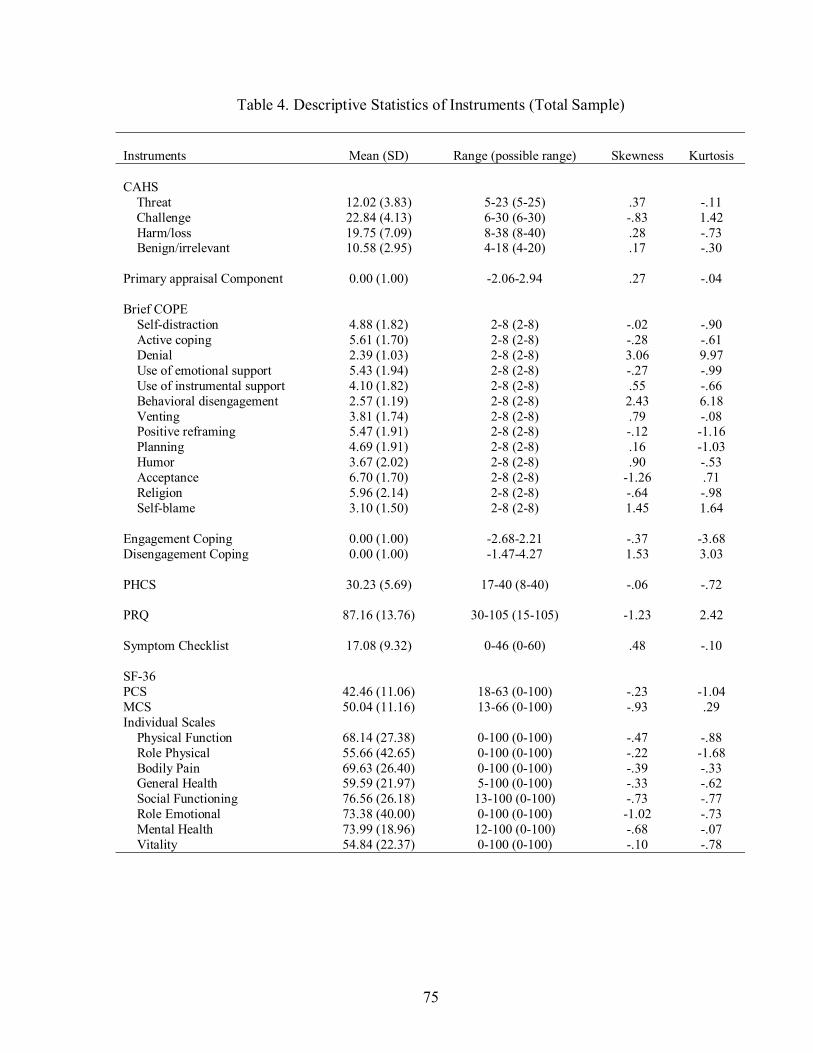
75
Table 4. Descriptive Statistics of Instruments (Total Sample)
Instruments
Mean (SD)
Range (possible range)
Skewness
Kurtosis
CAHS Threat Challenge Harm/loss Benign/irrelevant Primary appraisal Component
12.02 (3.83) 22.84 (4.13) 19.75 (7.09) 10.58 (2.95)
0.00 (1.00)
5-23 (5-25) 6-30 (6-30) 8-38 (8-40) 4-18 (4-20)
-2.06-2.94
.37 -.83 .28 .17
.27
-.11 1.42 -.73 -.30
-.04
Brief COPE Self-distraction Active coping Denial Use of emotional support Use of instrumental support Behavioral disengagement Venting Positive reframing Planning Humor Acceptance Religion Self-blame Engagement Coping Disengagement Coping
4.88 (1.82) 5.61 (1.70) 2.39 (1.03) 5.43 (1.94) 4.10 (1.82) 2.57 (1.19) 3.81 (1.74) 5.47 (1.91) 4.69 (1.91) 3.67 (2.02) 6.70 (1.70) 5.96 (2.14) 3.10 (1.50)
0.00 (1.00) 0.00 (1.00)
2-8 (2-8) 2-8 (2-8) 2-8 (2-8) 2-8 (2-8) 2-8 (2-8) 2-8 (2-8) 2-8 (2-8) 2-8 (2-8) 2-8 (2-8) 2-8 (2-8) 2-8 (2-8) 2-8 (2-8) 2-8 (2-8)
-2.68-2.21 -1.47-4.27
-.02 -.28 3.06 -.27 .55 2.43 .79 -.12 .16 .90
-1.26 -.64 1.45
-.37 1.53
-.90 -.61 9.97 -.99 -.66 6.18 -.08 -1.16 -1.03 -.53 .71 -.98 1.64
-3.68 3.03
PHCS
30.23 (5.69)
17-40 (8-40)
-.06
-.72
PRQ
87.16 (13.76)
30-105 (15-105)
-1.23
2.42
Symptom Checklist
17.08 (9.32)
0-46 (0-60)
.48
-.10
SF-36 PCS MCS Individual Scales Physical Function Role Physical Bodily Pain General Health Social Functioning Role Emotional Mental Health Vitality
42.46 (11.06) 50.04 (11.16)
68.14 (27.38) 55.66 (42.65) 69.63 (26.40) 59.59 (21.97) 76.56 (26.18) 73.38 (40.00) 73.99 (18.96) 54.84 (22.37)
18-63 (0-100) 13-66 (0-100)
0-100 (0-100) 0-100 (0-100) 0-100 (0-100) 5-100 (0-100) 13-100 (0-100) 0-100 (0-100) 12-100 (0-100) 0-100 (0-100)
-.23 -.93
-.47 -.22 -.39 -.33 -.73 -1.02 -.68 -.10
-1.04 .29
-.88 -1.68 -.33 -.62 -.77 -.73 -.07 -.78

76
Table 5. Descriptive Statistics of Instruments (Early Group)
Instruments
Mean (SD)
Range (possible range)
Skewness
Kurtosis
CAHS Threat Challenge Harm/loss Benign/irrelevant Primary appraisal Component
11.54 (3.97) 24.02 (4.31) 19.34 (6.54) 10.74 (2.77)
-0.15 (0.94)
5-22 (5-25) 6-30 (6-30) 8-33 (8-40) 6-18 (4-20)
-2.06-2.08
.50 -1.81 .16 .78
.25
.07 5.46 -.96 .26
.01
Brief COPE Self-distraction Active coping Denial Use of emotional support Use of instrumental support Behavioral disengagement Venting Positive reframing Planning Humor Acceptance Religion Self-blame Engagement Coping Disengagement Coping
5.19 (1.80) 6.21 (1.57) 2.25 (0.83) 5.94 (1.83) 4.38 (1.92) 2.43 (0.91) 3.85 (1.88) 5.81 (1.86) 5.12 (2.06) 3.73 (2.06) 6.85 (1.67) 5.98 (2.06) 3.00 (1.23)
0.29 (1.00) -0.09 (0.79)
2-8 (2-8) 2-8 (2-8) 2-6 (2-8) 2-8 (2-8) 2-8 (2-8) 2-5 (2-8) 2-8 (2-8) 2-8 (2-8) 2-8 (2-8) 2-8 (2-8) 2-8 (2-8) 2-8 (2-8) 2-6 (2-8)
-2.56-2.21 -1.32-2.18
-.32 -.63 3.49 -.52 .37 1.88 .73 -.24 -.12 .92
-1.68 -.67 .89
-.53 .87
-.79 -.32
11.56 -.75 -.80 2.11 -.53 -1.22 -1.15 -.43 2.37 -.87 -.66
.17 .71
PHCS
32.02 (5.13)
19-40 (8-40)
-.48
-.42
PRQ
90.33 (10.63)
67-105 (15-105)
-.33
-.75
Symptom Checklist
17.06 (9.07)
2-42 (0-60)
.30
-.03
SF-36 PCS MCS Individual Scales Physical Function Role Physical Bodily Pain General Health Social Functioning Role Emotional Mental Health Vitality
43.29 (10.53) 50.94 (10.21)
71.94 (25.36) 55.00 (43.41) 71.04 (24.66) 63.04 (20.41) 76.36 (25.87) 77.58 (37.44) 75.96 (18.28) 57.78 (21.03)
20-63 (0-100) 21-63 (0-100)
11-100 (0-100) 0-100 (0-100) 22-100 (0-100) 20-100 (0-100) 25-100 (0-100) 0-100 (0-100) 32-100 (0-100) 10-100 (0-100)
-.38 -1.01
-.69 -.19 -.23 -.38 -.58 -1.34 -.53 -.22
-.80 .60
-.44 -1.76 -1.26 -.67 -1.03 .14 -.59 -.56

77
Table 6. Descriptive Statistics of Instruments (Later Group)
Instruments
Mean (SD)
Range (possible range)
Skewness
Kurtosis
CAHS Threat Challenge Harm/loss Benign/irrelevant Primary appraisal Component
12.26 (3.75) 22.24 (3.92) 19.94 (7.39) 10.49 (3.06)
0.08 (1.02)
5-23 (5-25) 11-30 (6-30) 8-38 (8-40) 4-17 (4-20)
-2.02-2.94
.33 -.38 .31 -.04
.25
-.11 .13 -.70 -.56
-.06
Brief COPE Self-distraction Active coping Denial Use of emotional support Use of instrumental support Behavioral disengagement Venting Positive reframing Planning Humor Acceptance Religion Self-blame Engagement Coping Disengagement Coping
4.73 (1.81) 5.30 (1.68) 2.47 (1.11) 5.17 (1.96) 3.95 (1.77) 2.65 (1.31) 3.78 (1.67) 5.29 (1.93) 4.48 (1.81) 3.64 (2.01) 6.63 (1.72) 5.95 (2.18) 3.16 (1.60)
-0.15 (0.97) 0.04 (1.09)
2-8 (2-8) 2-8 (2-8) 2-8 (2-8) 2-8 (2-8) 2-8 (2-8) 2-8 (2-8) 2-8 (2-8) 2-8 (2-8) 2-8 (2-8) 2-8 (2-8) 2-8 (2-8) 2-8 (2-8) 2-8 (2-8)
-2.68-1.75 -1.47-4.27
.13 -.12 2.88 -.14 .64 2.38 .84 -.05 .26 .90
-1.09 -.63 1.56
-.38 1.57
-.81 -.50 8.94 -1.03 -.54 5.64 .27
-1.14 -.90 -.55 .16
-1.02 1.86
-.56 3.06
PHCS
29.31 (5.77)
17-40 (8-40)
.17
-.57
PRQ
85.58 (14.87)
30-105 (15-105)
-1.25
2.12
Symptom Checklist
17.10 (9.49)
0-46 (0-60)
.56
-.10
SF-36 PCS MCS Individual Scales Physical Function Role Physical Bodily Pain General Health Social Functioning Role Emotional Mental Health Vitality
42.46 (11.06) 50.04 (11.16)
66.13 (28.30) 56.01 (42.45) 68.87 (27.36) 57.73 (22.64) 76.67 (26.46) 71.15 (41.30) 72.93 (19.32) 53.30 (22.99)
18-63 (0-100) 13-66 (0-100)
0-100 (0-100) 0-100 (0-100) 0-100 (0-100) 5-100 (0-100) 13-100 (0-100) 0-100 (0-100) 12-100 (0-100) 0-100 (0-100)
-.16 -.88
-.36 -.24 -.44 -.27 -.81 -.89 -.74 -.03
-1.12 .16
-1.03 -1.66 -.82 -.63 -.63 -1.02 .11 -.84

78
These results indicated that participants in this study had a high degree of agreement with
the challenge appraisal of their health and a moderate degree of agreement with the threat,
harm/loss, and benign/irrelevant appraisal of their health.
In order to enhance the power of the statistical analyses by reducing the covariate
set, factor analysis on the four primary appraisal subscales of CAHS was performed to
identify the second-order factors to be used in the analyses for this study. A one-
component solution (63.49% of total variance) was derived and interpreted as the primary
appraisal of health. The component matrix was as follows: Threat (0.85), Challenge (-
0.72), Harm/Loss (0.85), and Benign/Irrelevant (-0.76). A weighted single component
score (M=0, SD=1) was used with a higher score indicating negative primary appraisal of
health (e.g., threat, harm, or loss).
Brief COPE. Coping strategies used by participants were assessed by Brief
COPE. There are 13 subscales with 2 items in each scale. Scores on each of the
subscales can range from 2 to 8. Higher scores on the subscale indicate more use of the
coping strategies represented by the subscale. In this study, actual scores on the 13
subscales ranged from 2 to 8. Results show that participants in this study used active
coping, emotional support, positive reframing, acceptance, and religion coping
moderately or a lot. Denial, behavioral disengagement, and self blame are used a little or
not at all by the participants.
Second-order factor analysis also was conducted on the 13 subscales of Brief
COPE to improve the power of the statistical analyses by reducing the covariate set.
Some of the subscales had lower reliabilities, some subscales had higher skewness, and
there were too many variables in the path models. A two-component solution (46.83%)

79
was derived based on the scree plot, the percentage of variance extracted, and item
loadings. Component 1 (31.94% variance) includes acceptance, active coping, use of
emotional support, use of instrumental support, planning, positive reframing, religion,
and self-distraction. Component 2 (14.89%) includes behavioral disengagement, denial,
humor, self-blame, and venting. The two-component solution was interpreted as
engagement coping (component 1) and disengagement coping (component 2). The
weighted component scores (M=0, SD=1) were used in this study. Higher scores in the
first weighted component indicated more use of engagement coping strategies, while
higher scores in the second weighted component indicated more use of disengagement
coping strategies.
PHCS. The Perceived Health Competence Scale (PHCS) was used to assess
perceived self-efficacy on health of participants in this study. After reverse scoring the
negatively valenced items, all scores on eight items are summed. Total scores on PHCS
can range from 8 to 40. Higher scores indicate a higher degree of perceived self-efficacy.
Participant scores in this study ranged from 17 to 40 (M=30.23, SD=5.69). These data
suggest that study participants had a high degree of perceived self-efficacy with respect
to their health.
PRQ. Perceived social support was measured using the Personal Resource
Questionnaire (PRQ). Scores on the PRQ can range from 15 to 105. High scores
indicate a high level of perceived social support. Actual scores in this study ranged from
30 to 105 (M=87.16, SD=13.76). These results indicate participants in this study
perceived high levels of social support.
80
SF-36. Self-reported HRQOL was measured by SF-36 in this study. SF-36 has
eight scales with scores ranging from 0 to 100 for each of them. The physical component
summary scale (PCS) and the mental component summary scale (MCS) are derived from
transforming and summing across the eight standardized weighted subscales. Scores on
the PCS and the MCS can range from 0 to 100 and are normed to the general US
population with a mean of 50 and standard deviation of 10. Higher scores represent
better HRQOL. In this study, participant scores on the PCS ranged from 18 to 63
(M=42.46, SD=11.06), while scores on the MCS ranges from 13 to 66 (M=50.04,
SD=11.16). These data suggest that participants in this study had a lower physical
HRQOL and a normal mental HRQOL in comparison to the general US population.
Symptom Checklist. The Symptom Checklist was developed by the researcher
and her dissertation committee to measure the side-effects of immunosuppressive
medications. Principal component analysis with varimax rotation was used to evaluate
the latent dimensionality of the 12 item symptom checklist. A one-component solution
(31.43%) was derived on the basis of the scree plot, percentage of variance extracted,
salient item loading, and solution clarity. Total scores are obtained by summing the 12
item scores and can range from 0 to 60. High scores indicate that the individuals were
experiencing more bothersome symptoms. The Cronbach�s alpha of this symptom
checklist was .79 in this study. Participant scores in this study ranged from 0 to 46
(M=17.08, SD=9.32). Based on these results, participants experienced mildly bothersome
side-effects of immunosuppressive medications. The median score on the symptom
checklist was 17. The median split was used to create the subgroups rather than the mean
score because two equal size groups could be obtained. Using the scores on the symptom

81
checklist, participants in this study were categorized into two groups, scores ≤ 17 group
(n=71) and scores >17 group (n=70). This classification was used to test the effect of
medication side-effects on the psychosocial variables in this study.
Table 5 and Table 6 show the descriptive statistics for each of the instruments by
group (the early group and the later group). The differences between the psychosocial
variables were examined using MANOVA in the research question 2. The results are
described later in this chapter.
Correlational Analysis Between Observed Variables
The zero-order correlations for observed variables in the models for the total
group of subjects are presented in Table 7. There was a significant positive relationship
between negative primary appraisal of health and disengagement coping (r=.42, p<.01).
The more the participants appraised their health condition as a threat, harm/loss, the more
they used disengagement coping. There were significant negative correlations between
negative primary appraisal and PCS (r=-.45, p<.01) and between negative primary
appraisal and MCS (r=-.54, p<.01). These results indicated that the more the participants
appraised their health condition negatively (higher scores), the worse their physical and
mental HRQOL (lower scores).
There was a significant negative relationship between perceived self-efficacy and
negative primary appraisal (r=-.62, p<.01). The lower the degree of perceived self-
efficacy of the participants, the more negatively they appraised their health condition.
Perceived self-efficacy also was negatively related to disengagement coping (r=-.39,
p<.01). The higher the degree of perceived self-efficacy, the less disengagement coping

82
was used. Perceived self-efficacy also had significant correlations with PCS (r=.41,
p<.01) and MCS (r=.44, p<.01). These data suggested that participants with a higher
degree of perceived self-efficacy had better physical and mental HRQOL.
The correlation analysis showed that perceived social support had a significant
negative relationship with negative primary appraisal (r=-.35, p<.01). The higher the
level of perceived social support, the less the participants appraised their health condition
as a threat or harm/loss. There was a statistically significant positive relationship
between perceived social support and engagement coping (r=.21, p<.05) and a significant
negative relationship between perceived social support and disengagement coping (r=-.18,
p<.05). These results indicated that participants in this study who reported higher levels
of perceived social support tended to use more engagement coping and less
disengagement coping. Perceived social support was also moderately correlated to
perceived self-efficacy (r=.34, p<.01). This result suggested that participants with a
higher level of perceived social support reported a higher degree of perceived self-
efficacy. Perceived social support had a significant negative relationship with time post-
transplant (r=-.14, p<.05). This result indicated that the longer the time post-transplant,
the lower the degree of perceived social support participants reported. This correlation
analysis also demonstrated that perceived social support was significantly related to PCS
(r=.21, p<.05) and MCS (r=.27, p<.01). The higher the level of social support perceived
by participants, the better HRQOL they reported.
There was a significant negative relationship between disengagement coping and
MCS (r=-.45, p<.05); a significant negative relationship between disengagement coping
and PCS (r=-.18, p<.05). These results indicated that participants who used more

83
disengagement coping reported worse physical and mental HRQOL. Correlation analysis
demonstrated that engagement coping had no statistically significant relationships with
either PCS or MCS (all p>.05).
Side-effect symptoms related to immunosuppressive medications had a significant
positive relationship with negative primary appraisal (r=.44, p<.01). The more
bothersome the symptoms reported by participants, the more they appraised their health
condition negatively. There was also a significant positive correlation between the
degree of bothersome medication side-effects and disengagement coping (r=.40, p<.01).
This result indicated that participants who reported more bothersome symptoms used
more disengagement coping. Correlation analysis demonstrated that the level of
bothersome symptoms was inversely related to perceived self-efficacy (r=-.47, p<.01),
PCS (r=-.32, p<.05), and MCS (r=-.46, p<.01). These results suggested that participants
with more bothersome symptoms reported a lower degree of perceived self-efficacy,
worse physical and worse mental HRQOL.
History of transplant-related hospitalizations had a significant positive
relationship with negative primary appraisal (r=.17, p<.05). This result indicated that
participants who reported having transplant-related hospitalizations appraised their health
condition negatively. History of transplant-related hospitalizations was also negatively
related to perceived social support (r=-.18, p<.05) and physical HRQOL (r=-.18, p<.05).
These results suggested that participants with a history of transplant-related
hospitalizations reported a lower degree of perceived social support and lower physical
HRQOL.
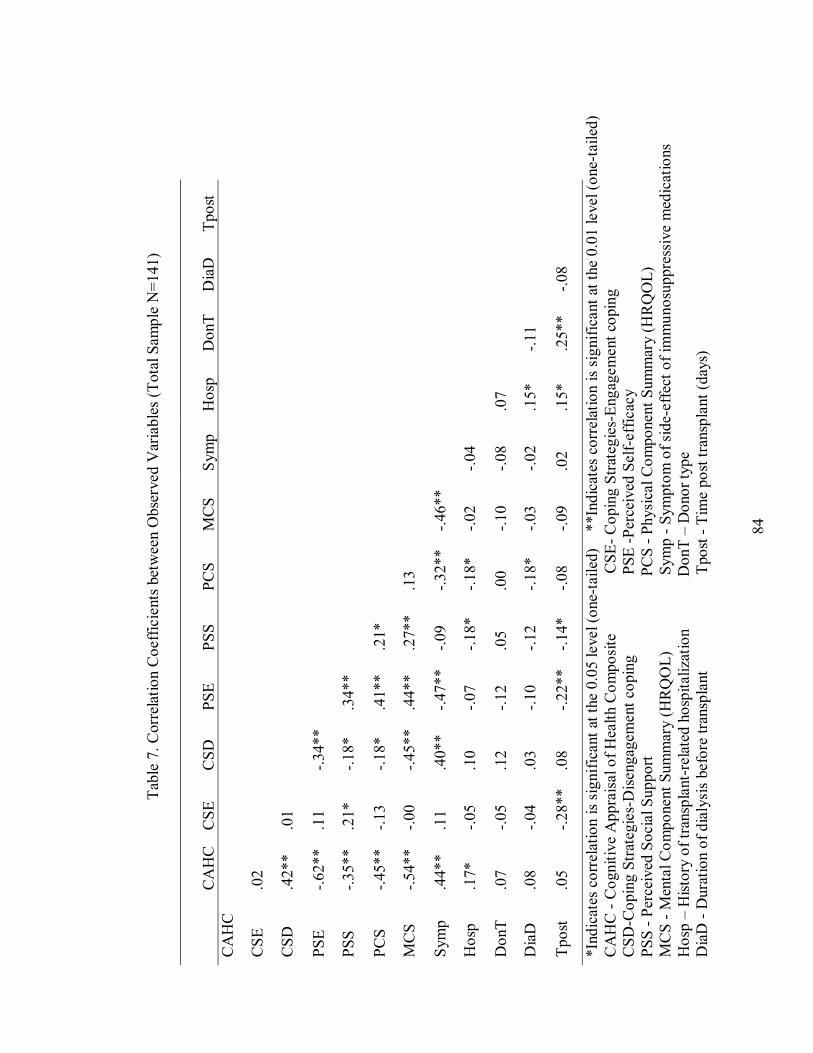
84
Tabl
e 7.
Cor
rela
tion
Coe
ffici
ents
bet
wee
n O
bser
ved
Var
iabl
es (T
otal
Sam
ple
N=1
41)
C
AH
C
CSE
C
SD
PSE
PSS
PCS
MC
S Sy
mp
Hos
p D
onT
Dia
D
Tpos
t C
AH
C
CSE
.0
2
CSD
.4
2**
.01
PSE
-.62*
* .1
1 -.3
4**
PSS
-.35*
* .2
1*
-.18*
.3
4**
PCS
-.45*
* -.1
3 -.1
8*
.41*
* .2
1*
MC
S -.5
4**
-.00
-.45*
* .4
4**
.27*
* .1
3
Sym
p .4
4**
.11
.40*
* -.4
7**
-.09
-.32*
* -.4
6**
Hos
p .1
7*
-.05
.10
-.07
-.18*
-.1
8*
-.02
-.04
Don
T .0
7 -.0
5 .1
2 -.1
2 .0
5 .0
0 -.1
0 -.0
8 .0
7
Dia
D
.08
-.04
.03
-.10
-.12
-.18*
-.0
3 -.0
2 .1
5*
-.11
Tpos
t .0
5 -.2
8**
.08
-.22*
* -.1
4*
-.08
-.09
.02
.15*
.2
5**
-.08
*Ind
icat
es c
orre
latio
n is
sign
ifica
nt a
t the
0.0
5 le
vel (
one-
taile
d)
**I
ndic
ates
cor
rela
tion
is si
gnifi
cant
at t
he 0
.01
leve
l (on
e-ta
iled)
C
AH
C -
Cog
nitiv
e A
ppra
isal
of H
ealth
Com
posit
e
C
SE- C
opin
g St
rate
gies
-Eng
agem
ent c
opin
g C
SD-C
opin
g St
rate
gies
-Dise
ngag
emen
t cop
ing
PSE
-Per
ceiv
ed S
elf-
effic
acy
PSS
- Per
ceiv
ed S
ocia
l Sup
port
PC
S - P
hysi
cal C
ompo
nent
Sum
mar
y (H
RQ
OL)
M
CS
- Men
tal C
ompo
nent
Sum
mar
y (H
RQ
OL)
Sym
p - S
ympt
om o
f sid
e-ef
fect
of i
mm
unos
uppr
essi
ve m
edic
atio
ns
Hos
p �
Hist
ory
of tr
ansp
lant
-rel
ated
hos
pita
lizat
ion
Don
T �
Don
or ty
pe
Dia
D -
Dur
atio
n of
dia
lysi
s be
fore
tran
spla
nt
Tp
ost -
Tim
e po
st tr
ansp
lant
(day
s)

85
Tabl
e 8.
Cor
rela
tion
Coe
ffici
ents
bet
wee
n O
bser
ved
Var
iabl
es (E
arly
Gro
up N
=46)
CA
HC
C
SE
CSD
PS
E PS
S PC
S M
CS
Sym
p H
osp
Don
T D
iaD
Tp
ost
CA
HC
C
SE
-.00
C
SD
.28*
-.0
6
PS
E -.6
3**
.15
-.27*
PSS
-.34*
* .1
5 -.1
4 .4
3**
PCS
-.41*
* -.1
8 -.0
5 .4
7**
.54*
*
MC
S -.5
1**
.22
-.42*
* .4
6**
.25*
.1
1
Sy
mp
.51*
* .0
1 .3
2*
-.63*
* -.3
5**
-.52*
* -.4
6**
H
osp
.15
-.22
.20
-.02
-.30*
-.0
7 -.0
4 -.0
1
D
onT
.12
-.01
.14
-.17
-.07
.17
-.25*
.1
2 .2
4
Dia
D
-.16
-.19
.00
-.04
.17
-.03
-.06
-.07
.21
-.09
Tpos
t -.1
6 -.2
4 -.1
0 .0
0 -.0
3 .2
3 .0
6 .0
2 .0
8 .0
3 .1
8
*Ind
icat
es c
orre
latio
n is
sign
ifica
nt a
t the
0.0
5 le
vel (
one-
taile
d)
**I
ndic
ates
cor
rela
tion
is si
gnifi
cant
at t
he 0
.01
leve
l (on
e-ta
iled)
C
AH
C -
Cog
nitiv
e A
ppra
isal
of H
ealth
Com
posit
e
C
SE- C
opin
g St
rate
gies
-Eng
agem
ent c
opin
g C
SD-C
opin
g St
rate
gies
-Dise
ngag
emen
t cop
ing
PSE
-Per
ceiv
ed S
elf-
effic
acy
PSS
- Per
ceiv
ed S
ocia
l Sup
port
PC
S - P
hysi
cal C
ompo
nent
Sum
mar
y (H
RQ
OL)
M
CS
- Men
tal C
ompo
nent
Sum
mar
y (H
RQ
OL)
Sym
p - S
ympt
om o
f sid
e-ef
fect
of i
mm
unos
uppr
essi
ve m
edic
atio
ns
Hos
p �
Hist
ory
of tr
ansp
lant
-rel
ated
hos
pita
lizat
ions
Don
T �
Don
or ty
pe
Dia
D -
Dur
atio
n of
dia
lysi
s be
fore
tran
spla
nt
Tp
ost -
Tim
e po
st tr
ansp
lant
(day
s)
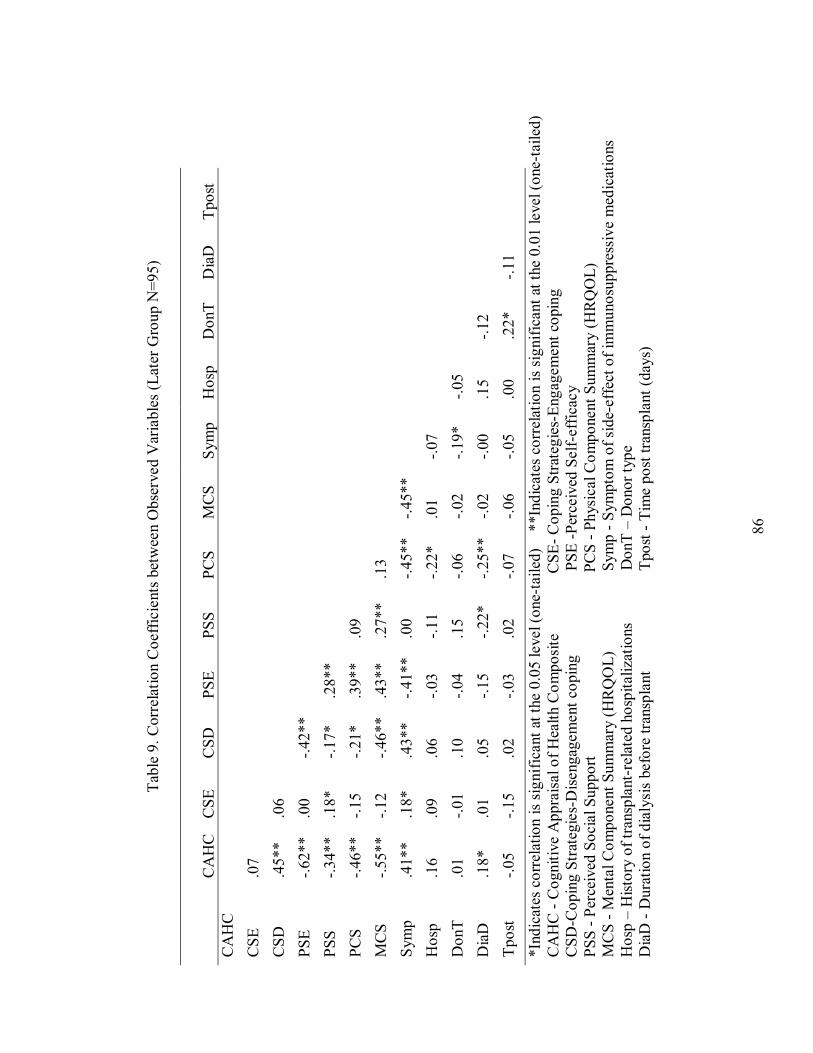
86
Tabl
e 9.
Cor
rela
tion
Coe
ffici
ents
bet
wee
n O
bser
ved
Var
iabl
es (L
ater
Gro
up N
=95)
CA
HC
C
SE
CSD
PS
E PS
S PC
S M
CS
Sym
p H
osp
Don
T D
iaD
Tp
ost
CA
HC
C
SE
.07
C
SD
.45*
* .0
6
PS
E -.6
2**
.00
-.42*
*
PSS
-.34*
* .1
8*
-.17*
.2
8**
PCS
-.46*
* -.1
5 -.2
1*
.39*
* .0
9
MC
S -.5
5**
-.12
-.46*
* .4
3**
.27*
* .1
3
Sy
mp
.41*
* .1
8*
.43*
* -.4
1**
.00
-.45*
* -.4
5**
H
osp
.16
.09
.06
-.03
-.11
-.22*
.0
1 -.0
7
D
onT
.01
-.01
.10
-.04
.15
-.06
-.02
-.19*
-.0
5
Dia
D
.18*
.0
1 .0
5 -.1
5 -.2
2*
-.25*
* -.0
2 -.0
0 .1
5 -.1
2
Tp
ost
-.05
-.15
.02
-.03
.02
-.07
-.06
-.05
.00
.22*
-.1
1
*Ind
icat
es c
orre
latio
n is
sign
ifica
nt a
t the
0.0
5 le
vel (
one-
taile
d)
**I
ndic
ates
cor
rela
tion
is si
gnifi
cant
at t
he 0
.01
leve
l (on
e-ta
iled)
C
AH
C -
Cog
nitiv
e A
ppra
isal
of H
ealth
Com
posit
e
C
SE- C
opin
g St
rate
gies
-Eng
agem
ent c
opin
g C
SD-C
opin
g St
rate
gies
-Dise
ngag
emen
t cop
ing
PSE
-Per
ceiv
ed S
elf-
effic
acy
PSS
- Per
ceiv
ed S
ocia
l Sup
port
PC
S - P
hysi
cal C
ompo
nent
Sum
mar
y (H
RQ
OL)
M
CS
- Men
tal C
ompo
nent
Sum
mar
y (H
RQ
OL)
Sym
p - S
ympt
om o
f sid
e-ef
fect
of i
mm
unos
uppr
essi
ve m
edic
atio
ns
Hos
p �
Hist
ory
of tr
ansp
lant
-rel
ated
hos
pita
lizat
ions
Don
T �
Don
or ty
pe
Dia
D -
Dur
atio
n of
dia
lysi
s be
fore
tran
spla
nt
T
post
- Ti
me
post
tran
spla
nt (d
ays)

87
There was a significant negative correlation between duration of dialysis before
transplantation and physical HRQOL (r=-.18, p<.05). This result suggested that
participants who received dialysis more than 6 months reported a lower physical HRQOL.
Relationships between time post-transplantation and other variables also were
assessed. Correlation analysis demonstrated that time post-transplantation had significant
negative associations with engagement coping (r=-.28, p<.01) and perceived self-efficacy
(r=-.22, p<.01). These results indicated that the longer the time post-transplantation, the
less engagement coping was used by the participants and they reported a lower degree of
perceived self-efficacy.
Correlational analyses between the observed variables in the model also were
performed for the early period post-transplant group (Table 8) and later group (Table 9).
Results indicated that perceived self-efficacy was significantly related to perceived social
support, physical and mental HRQOL, while perceived self-efficacy had a significant
inverse relationship with negative primary appraisal of health and side effects of
immunosuppressive medications in both groups. There were significant positive
relationships between perceived social support and physical and mental HRQOL, and
significant negative relationships between perceived social support and negative primary
appraisal of health, side effects of immunosuppressive medications, and history of
transplant-related hospitalizations in the early group. However, perceived social support
was not significantly related to physical HRQOL, side effects of immunosuppressive
medications, and history of transplant-related hospitalizations in the later group.
Perceived social support had a significant negative relationship with duration of dialysis
before transplantation in the later group. Negative primary appraisal of health was

88
significantly related to disengagement coping and side effects of immunosuppressive
medications, and negatively related to physical and mental HRQOL in both groups.
There was a significant negative relationship between disengagement coping and mental
HRQOL in both groups. Disengagement coping was not significantly related to physical
HRQOL in the early group, but there was a significant negative relationship to physical
HRQOL in the later group. Side effects of immunosuppressive medications had a
significant positive relationship with disengagement coping and negative relationships
with physical and mental HRQOL in both groups, while side effects of
immunosuppressive medications was also positively related to engagement coping in the
later group. History of transplant-related hospitalizations was negatively related to
physical HRQOL in the later group and no significant relationship was found in the early
group. Donor type had a negative relationship with mental HRQOL in the early group
and a negative relationship with side effects of immunosuppressive medications in the
later group. There were no significant relationships found between duration of dialysis,
time post-transplant and other variables in the early group. However, duration of dialysis
had a significant negative correlation to perceived social support and physical HRQOL;
time post-transplant was positively related to donor type in the later group.
Path Analysis of Proposed Models
A series of nested path analyses were used to test the initial, alternative, and
hypothesized models using the AMOS program. Participants with complete data on all
measures were included (N=141) to perform all the multiple regression analyses. To test
the model fit, the following indices were used in the analysis: the chi-square fit statistic (χ2),
89
relative chi-square (ratio of chi-square to degree of freedom, χ2/df), the goodness of fit
index (GFI), and the comparative fit index (CFI). These indices were chosen because they
are commonly reported in the literature and Bollen (1989) suggested that assessing model
fit should be based on multiple goodness-of-fit indices. The chi-square fit statistic (χ2)
assesses the discrepancy between the observed data and a restricted structure resulting from
the model under consideration. A high chi-square value leads to the rejection of the null
hypothesis of model fit. A limitation of the chi-square fit statistic is that it is greatly
influenced by sample size and violations of multivariate normality (Jöreskog & Sörbom,
1988). The relative chi-square is calculated by dividing the chi-square value by the
degrees of freedom. The relative chi-square should be less than three if the fit between the
data and model is to be considered good (Bollen, 1989). This index is an indication of how
well the model under scrutiny matches an alternative model (Jöreskog & Sörbom, 1988).
The GFI directly assesses the extent to which the model reproduces the data, and it
indicates the relative amount of the observed variances and covariance that are associated
with the model. The CFI assesses the extent to which the model reproduces the data as
compared to a baseline model in which all variables are uncorrelated. Values of 0.9 or
above for the GFI and CFI usually suggest good model fit (Bollen, 1989).
Initial Model
Analyses of the initial models predicting PCS and MCS were performed first.
Results showed the initial model predicting PCS did not fit the data well in relation to its
fully saturated counterpart. The χ2 statistic was significant (13.20, p= 0.001) with 2
degrees of freedom (df). The χ2 /df was 6.60. The goodness of fit index (GFI) was 0.98.

90
The comparative fit index (CFI) was 0.83. Similarly, the saturated model predicting MCS
also did not fit the data with χ2 (13.20, df =2, p= 0.001), χ2 /df (6.60), GFI (0.98), and CFI
(0.83).
Alternative Model
In the alternative models predicting PCS and MCS, paths from transplantation-
related variables to perceived self-efficacy and perceived social support were removed and
perceived self-efficacy and perceived social support were added to the correlated
exogenous variable set. Model fit analyses demonstrated that the alternative model
predicting PCS fit the data well. The χ2 statistic was not significant (0.00, p=0.995) with 1
degree of freedom. The χ2 /df was 0.00. Both the GFI and the CFI were 1.00. Results of
the alternative model predicting MCS mirrored the results for PCS, and fit the data well.
Path coefficients are summarized in Table 10. Path coefficients are bolded if the p-value
was ≤ 0.1.
Nested path analyses were performed for the alternative model predicting PCS. A
series of nested models were set up by constraining some paths by setting the selected path
coefficients to equal zero. Alternative model 1 had no constrained paths; alternative model
2 constrained the paths with p-values greater than 0.1; alternative model 3 constrained the
paths with p-values greater than 0.05; and alternative model 4 constrained the paths with p-
values greater than or equal to 0.05 (see Table 10).

91
Table 10. Path Coefficients in the Alternative Model Predicting PCS and MCS
Unstandardized S.E. Standardized P Self-efficacy on CAHS -.083 .014 -.477 .000 Hospitalization on CAHSc .263 .131 .128 .046 Social support on CAHS -.012 .005 -.162 .017 Symptom on CAHS .024 .008 .214 .003 Duration of dialysis on CAHSa,b,c -.018 .136 -.009 .892 Time post-transplant on CAHSb,c .000 .000 -.117 .078 Donor type on CAHSa,b,c .124 .136 .060 .364 Self-efficacy on Engagement Copinga,b,c .023 .020 .127 .253 Self-efficacy on Disengagement copinga,b,c -.018 .018 -.103 .316 Hospitalization on Engagement Copinga,b,c .036 .173 .017 .837 Hospitalization on Disengagement Copinga,b,c .112 .154 .055 .469 Social support on Disengagement Copinga,b,c -.003 .006 -.045 .580 Symptom on Engagement Copinga,b,c .016 .011 .137 .144 Symptom on Disengagement Coping .030 .009 .273 .002 Donor type on Engagement Copinga,b,c .018 .178 .009 .918 Donor type on Disengagement Copinga,b.c .230 .158 .113 .145 Duration of dialysis on Engagement Copinga,b,c -.073 .177 -.034 .680 Time post-transplant on Engagement Coping -.001 .000 -.239 .005 Time post-transplant on Disengagement Copinga,b,c .000 .000 -.005 .948 Social support on Engagement Coping .013 .006 .182 .038 CAHS on Engagement Copinga,b,c .119 .110 .117 .278 CAHS on Disengagement Coping .200 .098 .203 .041 Duration dialysis on Disengagement Copinga,b,c .025 .158 .012 .875 Self-efficacy on PCSb,c .371 .194 .192 .056 CAHS on PCS -2.854 1.083 -.259 .008 Hospitalization on PCSa,b.c -2.515 1.680 -.111 .134 Symptom on PCSa,b,c -.172 .107 -.141 .109 Donor type on PCSa,b,c .474 1.729 .021 .784 Duration of dialysis on PCSb,c -3.058 1.717 -.130 .075 Time post-transplant on PCSa,b,c -.002 .002 -.067 .391 Social support on PCSa,b,c .037 .063 .047 .559 Disengagement Coping on PCSa,b,c 1.052 .917 .094 .252 Engagement Coping on PCS -1.853 .817 -.172 .023 Self-efficacy on MCSa,b,c .014 .180 .007 .939 CAHS on MCS -3.519 1.004 -.318 .000 Hospitalization on MCSa,b,c 1.846 1.556 .081 .236 Symptom on MCS -.277 .099 -.225 .005 Donor type on MCSa,b.c -1.642 1.602 -.072 .305 Duration of dialysis on MCSa,b,c -.304 1.591 -.013 .848 Time post-transplant on MCSa,b,c -.001 .002 -.030 .679 Social support on MCSa,b,c .094 .058 .119 .106 Disengagement Coping on MCS -2.260 .850 -.201 .008 Engagement Coping on MCSa,b,c -.052 .757 -.005 .945
a: path constrained in alternative model 2 b: path constrained in alternative model 3 c: path constrained in alternative model 4

92
Model fit analyses demonstrated that alternative model 1 and the other three
alternative models fit the data. Fit indices for models 1 to 4 were as follows: 1) χ2 =0.00, χ2
/df =0.00, p=0.995; 2) χ2 =16.42, χ2 /df =0.78, p=0.746; 3) χ2 =27.40, χ2 /df =1.14, p=0.286;
and 4) χ2 =32.58, χ2 /df =1.30, p=0.142. Results of model comparisons indicated
alternative models 2, 3, and 4 were not significantly different from alternative model 1 if it
was assumed that alternative model 1 was correct (all p>.1). However, alternative models
3 and 4 were significantly different from alternative model 2 if it was assumed that
alternative model 2 was correct (all p<.05). Alternative model 2 was derived as an
empirical model predicting PCS based on the nested path analyses (see Figure 5). Path
coefficients in the empirical model predicting PCS are summarized in Table 11.
For the alternative model predicting MCS, the same analytic steps were performed.
Model fit analyses showed all four models predicting MCS fit the data well. There were
no significant differences between model 2 (χ2 =15.12, χ2 /df =0.69, p=0.857), model 3 (χ2
=17.26, χ2 /df =0.75, p=0.797), and model 4 (χ2 =19.93, χ2 /df =0.83, p=0.701). Results of
model comparisons demonstrated that alternative models 2, 3, and 4 predicting MCS were
not significantly different from alternative model 1 for MCS if it was assumed that
alternative model 1 for MCS was correct (all p >.6). Alternative models 3 and 4 for MCS
were not significantly different from alternative model 2 for MCS if it was assumed that
alternative model 2 for MCS was correct (all p>.05). Alternative model 4 for MCS was not
significantly different from alternative model 3 for MCS if it was assumed that alternative
model 3 for MCS was correct (p=.102). Alternative model 2 was derived as an empirical
model predicting MCS based on the nested path analyses (see Figure 6). Path coefficients
in the empirical model predicting MCS are summarized in Table 12.
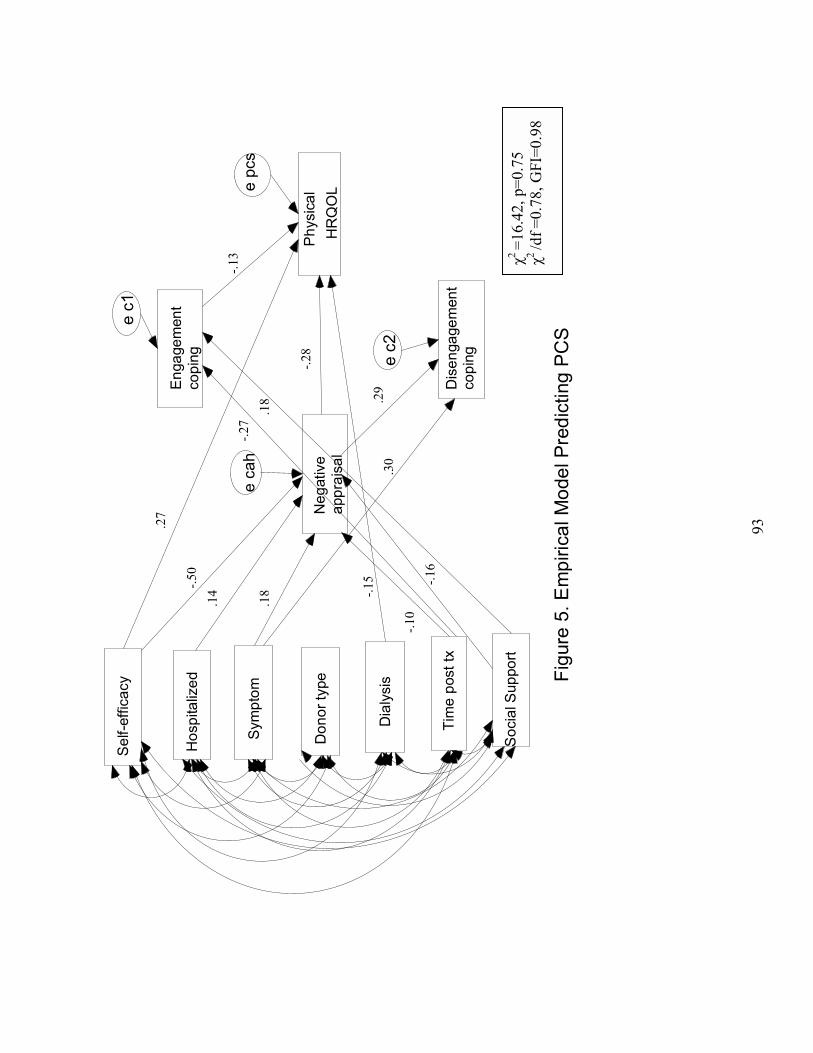
93
Sel
f-effi
cacy
Soc
ial S
uppo
rt
Sym
ptom
Phy
sica
l H
RQ
OL
Tim
e po
sttx
Neg
ativ
e
appr
aisa
l
Eng
agem
ent
copi
ng
Dis
enga
gem
ent
copi
ng
Hos
pita
lized
Don
or ty
pe
Dia
lysi
s Figu
re 5
. Em
piric
al M
odel
Pre
dict
ing
PC
S
e c1
e pc
s
e c2
e ca
h
.27
-.13
-.50
.14
-.16
.18
-.10
-.27
.18
.30
.29
-.15
-.28
χ2=1
6.42
, p=0
.75
χ2 /d
f =0.
78, G
FI=0
.98

94
Sel
f-effi
cacy
Soc
ial S
uppo
rt
Sym
ptom
Men
tal
HR
QO
L
Tim
e po
st tx
Neg
ativ
e ap
prai
sal
Eng
agem
ent
copi
ng
Dis
enga
gem
ent
copi
ng
Hos
pita
lized
Don
or ty
pe
Dia
lysi
s
Figu
re 6
. Em
piric
al M
odel
Pre
dict
ing
MC
S
e c1
e m
cs
e c2
e ca
h
-.51
.13
-.16
.18
-.10
-.26
.17
.28
.29
-.23
-.36
-.19
χ2=1
5.12
, p=0
.86
χ2 /d
f =0.
69, G
FI=0
.98
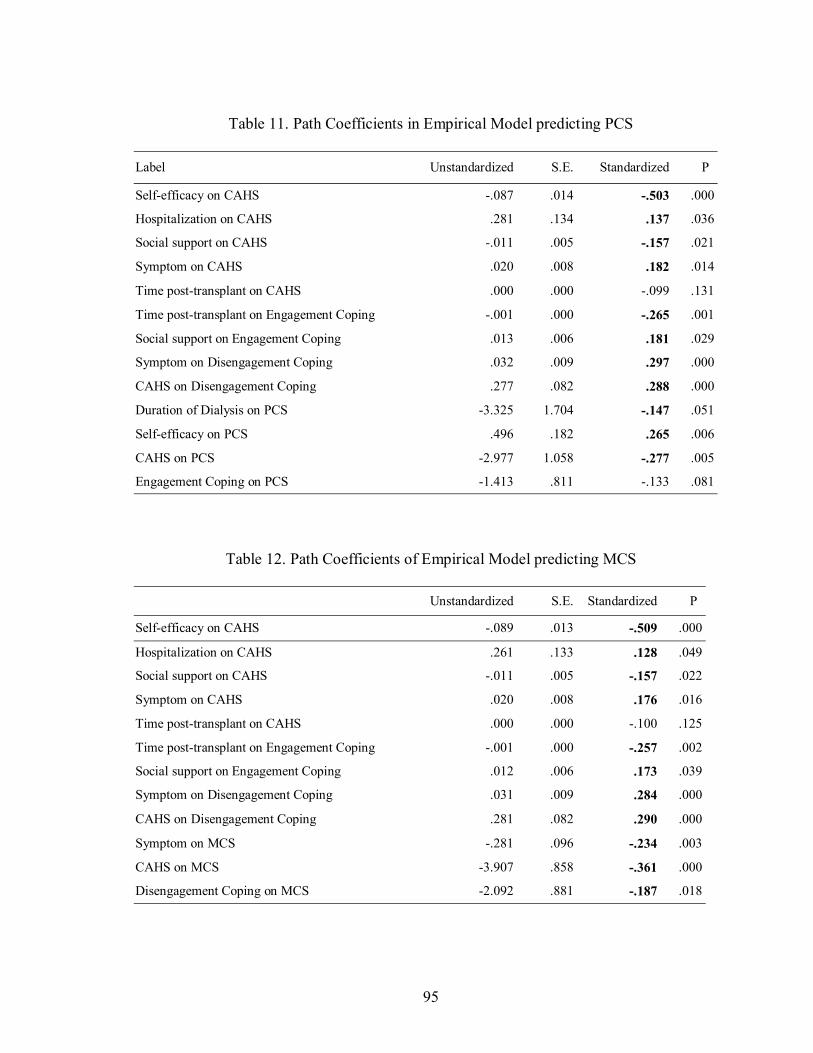
95
Table 11. Path Coefficients in Empirical Model predicting PCS
Label Unstandardized S.E. Standardized P
Self-efficacy on CAHS -.087 .014 -.503 .000
Hospitalization on CAHS .281 .134 .137 .036
Social support on CAHS -.011 .005 -.157 .021
Symptom on CAHS .020 .008 .182 .014
Time post-transplant on CAHS .000 .000 -.099 .131
Time post-transplant on Engagement Coping -.001 .000 -.265 .001
Social support on Engagement Coping .013 .006 .181 .029
Symptom on Disengagement Coping .032 .009 .297 .000
CAHS on Disengagement Coping .277 .082 .288 .000
Duration of Dialysis on PCS -3.325 1.704 -.147 .051
Self-efficacy on PCS .496 .182 .265 .006
CAHS on PCS -2.977 1.058 -.277 .005
Engagement Coping on PCS -1.413 .811 -.133 .081
Table 12. Path Coefficients of Empirical Model predicting MCS
Unstandardized S.E. Standardized P
Self-efficacy on CAHS -.089 .013 -.509 .000
Hospitalization on CAHS .261 .133 .128 .049
Social support on CAHS -.011 .005 -.157 .022
Symptom on CAHS .020 .008 .176 .016
Time post-transplant on CAHS .000 .000 -.100 .125
Time post-transplant on Engagement Coping -.001 .000 -.257 .002
Social support on Engagement Coping .012 .006 .173 .039
Symptom on Disengagement Coping .031 .009 .284 .000
CAHS on Disengagement Coping .281 .082 .290 .000
Symptom on MCS -.281 .096 -.234 .003
CAHS on MCS -3.907 .858 -.361 .000
Disengagement Coping on MCS -2.092 .881 -.187 .018

96
Hypothesized Model
Model fit analyses demonstrated that the hypothesized model predicting PCS did
not suitably fit the data. The χ2 statistic was significant (51.59, p=0.000) with 19 degrees
of freedom. The χ2 /df ratio was 2.72. The GFI was 0.93 and the CFI was 0.50. Path
analyses for the alternative model for PCS indicated the path from CAHS to PCS (β=-.26,
p=.008) and the path from perceived self-efficacy to PCS (β=.19, p=.056) represented
significant effects. A modified hypothesized model predicting PCS was derived by adding
paths from CAHS to PCS and from perceived self-efficacy to PCS (see Figure 7).
Model fit analyses demonstrated that the modified hypothesized model for PCS fit
the data well. The χ2 statistic was not significant (27.02, p=0.058) with 17 degrees of
freedom. The χ2 /df ratio was 1.59. The GFI was 0.97 and the CFI was 0.85. The model
comparisons were performed on the alternative model for PCS, the modified hypothesized
model for PCS, and the hypothesized model for PCS. Results indicated that the modified
hypothesized model and the hypothesized model for PCS were significantly different from
the alternative model for PCS (all p<.05) if it was assumed that the alternative model was
correct. The hypothesized model for PCS was significantly different from the modified
model for PCS if it was assumed that the modified model for PCS was correct (p <.05).
For the hypothesized model predicting MCS, results of model fit analyses indicated
that it did not suitably fit the data. The χ2 statistic was significant (50.24, p=0.000) with 19
degrees of freedom. The χ2 /df ratio was 2.64. The GFI was 0.94 and the CFI was 0.52. A
modified hypothesized model predicting MCS was developed (see Figure 8). Paths from
CAHS to MCS and from symptom to MCS, which were significant in the path analyses for
the alternative model for MCS (β=-.32, p=.000, and β=-.23, p=.005, respectively) were

97
added in the modified hypothesized model predicting MCS. Results of model fit analyses
indicated that the modified hypothesized model for MCS fit the data well. The χ2 statistic
was not significant (23.51, p=0.133) with 17 degrees of freedom. The χ2 /df ratio was 1.38.
The GFI was 0.97 and the CFI was 0.90. Model comparisons also were performed on the
alternative model for MCS, the modified hypothesized model for MCS, and the
hypothesized model for MCS. Results suggested that the modified hypothesized model for
MCS was not significantly different (p=.101) and the hypothesized model for MCS were
significantly different (p <.05) from the alternative model for MCS if it was assumed that
the alternative model for MCS was correct. The hypothesized model for MCS was
significantly different from the modified hypothesized model for MCS if it was assumed
that the modified model for MCS was correct (p <.05).
Path coefficients in the modified hypothesized models for PCS and MCS are
summarized in Table 13 and Table 14. Standardized total effects including direct and
indirect effects for the endogenous variables were also calculated (see Table 15, Table 16).
Results indicated that perceived self-efficacy had the largest total effects on negative
primary appraisal of health (-.45), disengagement coping (-.36), and physical HRQOL (.39),
while negative primary appraisal of health had the largest total effects on engagement
coping (.21) in the modified hypothesized model predicting PCS. In the modified
hypothesized model predicting MCS, perceived self-efficacy had the largest total effects on
negative primary appraisal of health (-.46) and disengagement coping (-.36), while
negative primary appraisal of health had the largest total effects on engagement coping (.21)
and mental HRQOL (-.43).
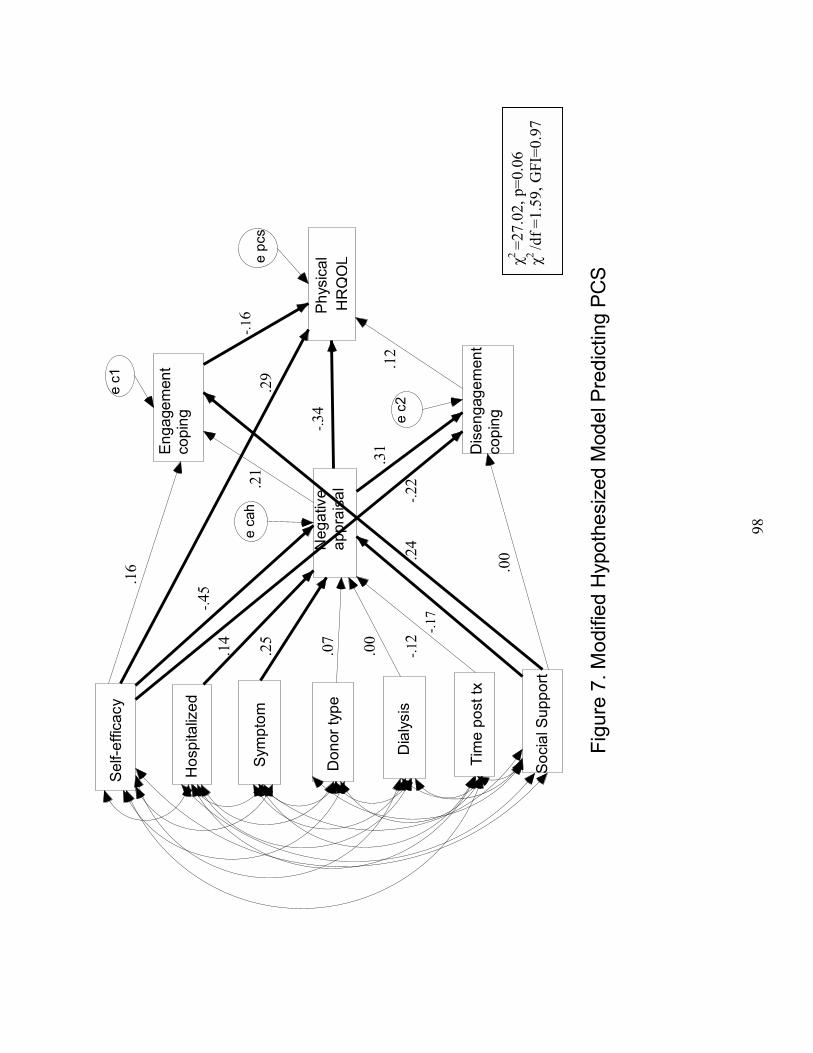
98
Sel
f-effi
cacy
Soc
ial S
uppo
rt
Sym
ptom
Phy
sica
lH
RQ
OL
Tim
e po
st tx
Neg
ativ
e ap
prai
sal
Eng
agem
ent
copi
ng
Dis
enga
gem
ent
copi
ng
Hos
pita
lized
Don
or ty
pe
Dia
lysi
s
Figu
re 7
. Mod
ified
Hyp
othe
size
d M
odel
Pre
dict
ing
PC
S
e c1
e pc
s
e c2
e ca
h
.14
-.17
.25
.00
-.12
.07
-.45
.00.2
4
.21
.31
.16
-.22
-.34
-.16
.12
.29
χ2=2
7.02
, p=0
.06
χ2 /d
f =1.
59, G
FI=0
.97
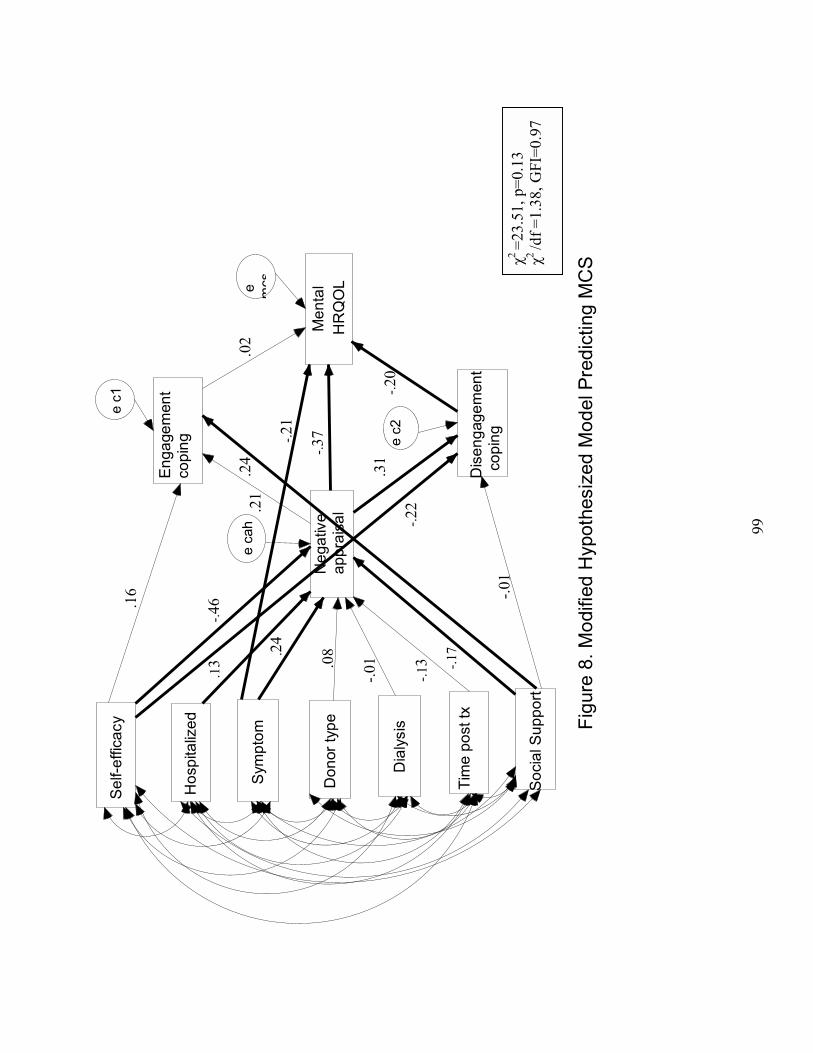
99
Sel
f-effi
cacy
Soc
ial S
uppo
rt
Sym
ptom
Men
tal
HR
QO
L
Tim
e po
st tx
Neg
ativ
e ap
prai
sal
Eng
agem
ent
copi
ng
Dis
enga
gem
ent
copi
ng
Hos
pita
lized
Don
or ty
pe
Dia
lysi
s Figu
re 8
. Mod
ified
Hyp
othe
size
d M
odel
Pre
dict
ing
MC
S
e c1
e mcs
e c2
e ca
h
.13
.24
-.17
-.01
-.13.0
8
-.46 -.0
1
.24
.21
.31
.16
-.22
-.37
.02
-.20
-.21
χ2=2
3.51
, p=0
.13
χ2 /d
f =1.
38, G
FI=0
.97

100
Table 13. Path Coefficients in the Modified Hypothesized Model Predicting PCS
Label Unstandardized S.E. Standardized P Hospitalization on CAHS .294 .135 .140 .029Social support on CAHS -.012 .005 -.172 .012Symptom on CAHS .030 .009 .254 .001Duration of dialysis on CAHS .003 .142 .001 .983Time post-transplant on CAHS .000 .000 -.124 .074Donor type on CAHS .148 .139 .070 .288Self-efficacy on CAHS -.078 .014 -.448 .000Social support on Disengagement Coping .000 .006 .004 .966Social support on Engagement Coping .016 .006 .239 .012CAHS on Engagement Coping .200 .108 .210 .064CAHS on Disengagement Coping .287 .097 .308 .003Self-efficacy on Engagement Coping .027 .019 .163 .150Self-efficacy on Disengagement coping -.036 .017 -.222 .032CAHS on PCS -3.632 1.074 -.344 .000Engagement Coping on PCS -1.763 .857 -.160 .040Disengagement Coping on PCS 1.402 .987 .124 .156Self-efficacy on PCS .530 .186 .287 .004
Table 14. Path Coefficients in the Modified Hypothesized Model Predicting MCS
Unstandardized S.E. Standardized P Self-efficacy on CAHS -.080 .014 -.456 .000Hospitalization on CAHS .263 .134 .127 .050Social support on CAHS -.013 .005 -.173 .012Symptom on CAHS .029 .009 .244 .002Duration of dialysis on CAHS -.020 .136 -.009 .883Time post-transplant on CAHS .000 .000 -.129 .062Donor type on CAHS .162 .141 .077 .251Social support on Disengagement Coping .000 .006 -.007 .933Social support on Engagement Coping .017 .007 .240 .012CAHS on Engagement Coping .202 .109 .212 .064CAHS on Disengagement Coping .285 .097 .307 .003Self-efficacy on Engagement Coping .028 .019 .164 .147Self-efficacy on Disengagement Coping -.036 .017 -.219 .035Disengagement Coping on MCS -2.314 .913 -.201 .011Engagement Coping on MCS .186 .794 .017 .815symptom on MCS -.265 .101 -.212 .009CAHS on MCS -3.992 .943 -.373 .000
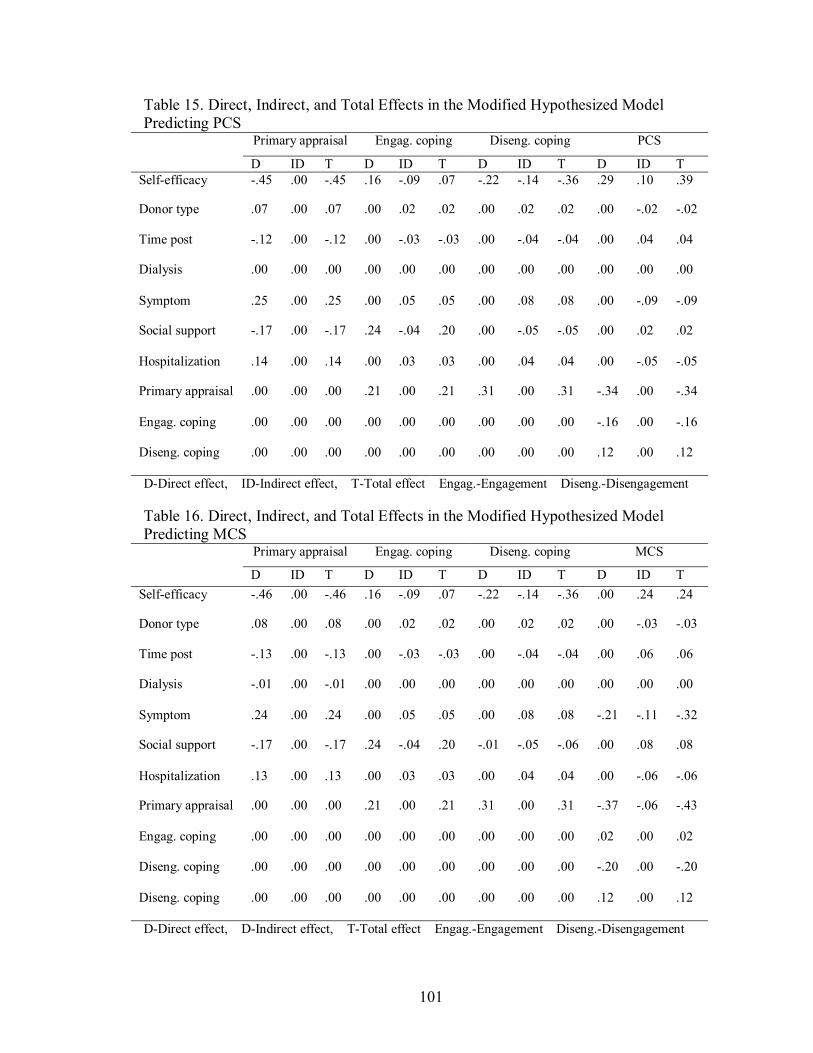
101
Table 15. Direct, Indirect, and Total Effects in the Modified Hypothesized Model Predicting PCS
Primary appraisal Engag. coping Diseng. coping PCS
D ID T D ID T D ID T D ID T Self-efficacy -.45 .00 -.45 .16 -.09 .07 -.22 -.14 -.36 .29 .10 .39
Donor type .07 .00 .07 .00 .02 .02 .00 .02 .02 .00 -.02 -.02
Time post -.12 .00 -.12 .00 -.03 -.03 .00 -.04 -.04 .00 .04 .04
Dialysis .00 .00 .00 .00 .00 .00 .00 .00 .00 .00 .00 .00
Symptom .25 .00 .25 .00 .05 .05 .00 .08 .08 .00 -.09 -.09
Social support -.17 .00 -.17 .24 -.04 .20 .00 -.05 -.05 .00 .02 .02
Hospitalization .14 .00 .14 .00 .03 .03 .00 .04 .04 .00 -.05 -.05
Primary appraisal .00 .00 .00 .21 .00 .21 .31 .00 .31 -.34 .00 -.34
Engag. coping .00 .00 .00 .00 .00 .00 .00 .00 .00 -.16 .00 -.16
Diseng. coping .00 .00 .00 .00 .00 .00 .00 .00 .00 .12 .00 .12
D-Direct effect, ID-Indirect effect, T-Total effect Engag.-Engagement Diseng.-Disengagement
Table 16. Direct, Indirect, and Total Effects in the Modified Hypothesized Model Predicting MCS
Primary appraisal Engag. coping Diseng. coping MCS
D ID T D ID T D ID T D ID T Self-efficacy -.46 .00 -.46 .16 -.09 .07 -.22 -.14 -.36 .00 .24 .24
Donor type .08 .00 .08 .00 .02 .02 .00 .02 .02 .00 -.03 -.03
Time post -.13 .00 -.13 .00 -.03 -.03 .00 -.04 -.04 .00 .06 .06
Dialysis -.01 .00 -.01 .00 .00 .00 .00 .00 .00 .00 .00 .00
Symptom .24 .00 .24 .00 .05 .05 .00 .08 .08 -.21 -.11 -.32
Social support -.17 .00 -.17 .24 -.04 .20 -.01 -.05 -.06 .00 .08 .08
Hospitalization .13 .00 .13 .00 .03 .03 .00 .04 .04 .00 -.06 -.06
Primary appraisal .00 .00 .00 .21 .00 .21 .31 .00 .31 -.37 -.06 -.43
Engag. coping .00 .00 .00 .00 .00 .00 .00 .00 .00 .02 .00 .02
Diseng. coping .00 .00 .00 .00 .00 .00 .00 .00 .00 -.20 .00 -.20
Diseng. coping .00 .00 .00 .00 .00 .00 .00 .00 .00 .12 .00 .12
D-Direct effect, D-Indirect effect, T-Total effect Engag.-Engagement Diseng.-Disengagement

102
Hypothesis 1. Perceived self-efficacy has both direct and indirect effects on
coping, and exerts a direct effect on cognitive appraisal of health. This hypothesis was
partially supported. Perceived self-efficacy was a significant predictor of negative
primary appraisal of health in both modified hypothesized models for PCS and MCS (β=
-.45, p=.000, and β= -.46, p=.000, respectively). Individuals with low degrees of
perceived self-efficacy were predicted to appraise their health conditions negatively (as
threat or harm/loss). Perceived self-efficacy had both a direct effect (β= -.22, p<.05 in
both modified models) and an indirect effect (both β= -.14) through primary appraisal of
health on disengagement coping. Participants who reported low degrees of perceived
self-efficacy were predicted to use more disengagement coping. Perceived self-efficacy
was not a significant predictor of engagement coping in both modified hypothesized
models for PCS and MCS (both p>.1).
Hypothesis 2. Perceived social support exerts both direct and indirect effects on
coping, and a direct effect on cognitive appraisal of health. This hypothesis was partially
supported. Perceived social support had a direct effect on negative primary appraisal of
health (both β= -.17, p<.05) in the modified hypothesized models for PCS and MCS.
Participants with low degrees of perceived social support were predicted to appraise their
health as a threat or harm/loss. Perceived social support had a significant direct effect on
engagement coping (both β= .24, p=.012) and no significant indirect effects on
engagement coping (both p>.05) in both modified hypothesized models. Perceived social
support had no significant direct effect (both p>.90), but had an indirect effect on
disengagement coping through negative primary appraisal of health (both β = -.05) in
both modified hypothesized models. Thus, participants with a high degree of perceived

103
social support were predicted to use more engagement coping and less disengagement
coping by appraising their health positively (as a challenge or benign/irrelevant).
Hypothesis 3. Cognitive appraisal of health has a direct effect on coping strategies.
This hypothesis was partially supported. Negative primary appraisal of health had a
direct effect on disengagement coping (both β= .31, p= .003) in the two modified
hypothesized models. Participants who appraised their health negatively (as a threat or
harm/loss) were predicted to use more disengagement coping strategies. Negative
primary appraisal of health was not a significant predictor of engagement coping in either
modified hypothesized models (both p> .05).
Hypothesis 4. Coping strategies have a direct effect on HRQOL. This hypothesis
was partially supported. In the modified hypothesized model predicting PCS,
engagement coping was a significant predictor of physical HRQOL (β= -.16, p= .040),
while disengagement coping was not a significant predictor of physical HRQOL
(p= .156). The results indicated that participants who used more engagement coping
were predicted to report a lower physical HRQOL. In the modified hypothesized model
predicting MCS, disengagement coping was a significant predictor of mental HRQOL
(β= -.20, p= .011), while engagement coping was not a significant predictor of mental
HRQOL (p= .815). The results suggested that the more the disengagement coping used,
the lower the mental HRQOL of the participants.
Hypothesis 5. Clinical factors related to renal transplantation have direct effects on
the cognitive appraisal of health. This hypothesis was partially supported. History of
transplant related hospitalizations (β= .14, p=.029 and β= .13, p=.050, respectively) and
side-effects of immunosuppressive medications (β= .25, p= .001 and β= .24, p=.002,

104
respectively) had direct effects on primary cognitive appraisal of health, while donor type,
duration of dialysis before transplantation, and time post-transplant were not significant
predictors for the primary appraisal of health (all p>.05) in both modified hypothesized
models. Participants who had history of transplant-related hospitalizations and
experiencing more bothersome symptoms of medication side effects were predicted to
appraise their health negatively (as a threat or harm/loss).
Multivariate Analysis of Variance on Research Question Two
Research question 2. What are the effects of clinical factors (donor type, history
of transplant-related hospitalizations, side effects of immunosuppressive medications,
duration of dialysis, and time post-transplantation) on perceived self-efficacy, perceived
social support, cognitive appraisal of health, coping, and HRQOL following renal
transplantation?
The effects of clinical factors such as donor type (living vs cadaveric), duration of
dialysis before transplantation (≤6 months, >6 months), history of transplant related
hospitalizations (yes vs no), and symptom of side-effects of immunosuppressive
medications (scores≤17, vs scores>17) on the psychosocial variables (e.g., perceived self-
efficacy, perceived social support, cognitive appraisal of health [negative primary appraisal
component], coping strategies [engagement coping, disengagement coping], and HRQOL
[PCS, MCS]) were evaluated using Multivariate Analysis of Covariance (MANCOVA)
with the time post-transplant as the covariate. The effect of time post-transplant on the
criterion measures needed to be controlled because, as expected, correlational analysis
showed that time post-transplant had significant relationships with some of the

105
psychosocial variables such as engagement coping and perceived self-efficacy. Levene�s
test of equality of error variances was performed first and was supported for all of the
dependent variables (all p>.05). Initial multivariate analyses demonstrated statistically
significant omnibus main effects for medication side effects on the psychosocial variables
(p<.01). There were no omnibus main effects for donor type, duration of dialysis before
transplantation, and history of hospitalizations on these psychosocial variables (all p>.05).
Table 6 summarizes the tests of the main effects for clinical factors on all the psychosocial
variables. Participants with high scores (>17) on symptom checklist reported high scores
on CAHC, which indicated they appraised their health condition negatively (p=.00).
Participants with high scores (>17) on the symptom checklist used more disengagement
coping (p=.00) and they had a lower degree of perceived self-efficacy, physical and mental
HRQOL (all p=.00).
Table 17. MANCOVA of Clinical Factors on Psychosocial Variables Controlling for Time Post-transplant (N=143)
Univariate Tests (p) Multivariate Test (p) CAHC CSE CSD PSE PSS PCS MCS
Intercept
.000
Symptom (≤ 17, >17)
.000
.000
.069
.000
.000
.714
.000
.000
Donor type (living, cadaver)
.329
.212
.736
.087
.089
.322
.765
.156
Duration of dialysis (≤ 6M, >6M)
.324
.273
.564
.438
.036
.264
.025
.377
History of hospitalizations (Y/N)
.211
.072
.984
.325
.895
.074
.078
.918
Covariate (time post)
.012
CAHC - Cognitive Appraisal of Health Composite CSE- Coping Strategies-Engagement coping CSD-Coping Strategies-Disengagement coping PSE -Perceived Self-efficacy PSS - Perceived Social Support PCS - Physical Component Summary (HRQOL) MCS-Mental Component Summary (HRQOL)

106
The main effects of time post-transplant on the psychosocial variables were also
assessed using multivariate analysis of variance (MANOVA) (see Table 7). The length of
time post-transplant was categorized as the early period (less than 1 year) and later period
(1 to 3 years). Results indicated that there were statistically significant main effects of time
post-transplant on the psychosocial variables (p=.027). Results demonstrated that
participants in the early period post-transplant used more engagement coping strategies
than participants in the later period (p=.005). Participants in the later period post-
transplant also reported a lower degree of perceived self-efficacy and perceived social
support than those in the early period (p=.004, p=.040, respectively). There were no main
effects of time post-transplant on primary appraisal, disengagement coping, PCS, and MCS
(all p>.05).
Table 18. Effects of Time Post-transplant Group on Psychosocial Variables (N=143)
Early Group M (SD)
Later Group M (SD)
F ratio (df=1)
p
Primary appraisal
-.14 (.89)
.07 (1.05)
1.45
.231
Engagement coping
.32 (1.04)
-.19 (.98)
8.23
.005
Disengagement coping
-.11 (.79)
.02 (1.10)
.49
.484
Perceived self-efficacy
32.32 (5.10)
29.39 (5.84)
8.65
.004
Perceived social support
90.32 (10.90)
85.19 (15.19)
4.28
.040
Physical component summary
43.73 (10.71)
42.33 (11.34)
.49
.485
Mental component summary
51.07 (9.72)
49.69 (11.81)
.48
.489
107
Summary of Results
One hundred and sixty adult renal transplant patients participated in this study.
Most of them were married and Caucasian. Hypertension and diabetes were the major
causes of ESRD for the participants. The majority of the participants in this study had
hemodialysis before transplantation, with an average duration of two years. More than half
of the participants received a living donor graft and took prednisone, Cellcept, and Prograf
for immunosuppressive therapy. Few participants experienced an episode (or episodes) of
rejection following transplantation. The majority of the participants had no transplant-
related hospitalizations. The average length of time post-transplant was one and a half
years.
Participants in this study indicated that they appraised their health as a challenge
rather than a threat. They reported greater use of active coping, emotional support, positive
reframing, acceptance, and religion coping strategies and less use of denial, behavioral
disengagement, and self-blame coping strategies. Participants viewed themselves as
capable of managing their health and perceived that social support was available to them.
They experienced few symptoms of side-effects of immunosuppressive medications and if
experienced, these symptoms bothered them only slightly. Participants had a lower
physical HRQOL than the U.S. general population and a mental HRQOL that was
equivalent to the general U.S. population as assessed by SF-36 scores.
Bivariate correlational analyses showed that negative primary appraisal had a
moderate positive relationship with disengagement coping. Participants who endorsed
health primary appraisals as threat or harm/loss reported more use of disengagement
coping and they also reported lower physical and mental HRQOL. Participants with a high

108
degree perceived self-efficacy and perceived social support appraised their health as a
challenge or benign/irrelevant. Participants with a high degree of perceived self-efficacy
reported a high degree of perceived social support, used less disengagement coping, and
reported higher physical and mental HRQOL. Participants with a high degree of perceived
social support also used less disengagement coping, and reported high physical and mental
HRQOL. Participants who reported numerous bothersome symptoms on the checklist
appraised their health as a threat or harm/loss, used more disengagement coping, had lower
degrees of perceived self-efficacy, and reported lower physical and mental HRQOL.
Participants with longer time post-transplant used less engagement coping and reported
lower degrees of perceived self-efficacy.
Model fit analyses indicated that the alternative models predicting PCS and MCS fit
the data well, while the initial and hypothesized models for PCS and MCS did not fit the
data well. The modified hypothesized models predicting PCS and MCS were derived by
adding in the paths from perceived self-efficacy to PCS and from primary appraisal of
health to PCS in the hypothesized model for PCS and by adding in the paths from
medication side effects to MCS and from primary appraisal of health to MCS in the
hypothesized model for MCS. Both modified hypothesized models fit the data well. Path
analyses demonstrated that perceived self-efficacy had a significant direct effect on
negative primary appraisal of health and physical HRQOL, and had both a direct effect and
an indirect effect through primary appraisal on disengagement coping. Perceived social
support had significant direct effects on negative primary appraisal of health and
engagement coping, while perceived social support had an indirect effect on
disengagement coping through negative primary appraisal of health. History of transplant-

109
related hospitalizations and side effects of immunosuppressive medications were found to
have direct effects on primary cognitive appraisal of health. Side effects of
immunosuppressive medications had a direct effect on mental HRQOL. Results also
indicated that negative primary appraisal of health had a significant direct effect on
disengagement coping, physical and mental HRQOL. Regarding the effects of coping
strategies on HRQOL, the findings suggest that engagement coping had a significant direct
effect on physical HRQOL, while disengagement coping had a significant direct effect on
mental HRQOL
The effects of clinical factors on psychosocial variables were evaluated. There
were no significant effects of donor type, duration of dialysis before transplantation, or
history of transplant-related hospitalizations on the psychosocial variables after controlling
for time post-transplant. There were significant effects of symptoms and time post-
transplant on these psychosocial variables. Participants with high scores (>17) on
symptom checklist appraised their health as threat or harm/loss, used more disengagement
coping, had lower perceived self-efficacy, physical and mental HRQOL than participants
with low scores (<17) on the symptom checklist. Participants less than one year post-
transplant used more engagement coping, reported higher degrees of perceived self-
efficacy and perceived social support than participants in the later period post-transplant.

110
CHAPTER V
DISCUSSION
The relationships among clinical factors, perceived self-efficacy, perceived social
support, cognitive appraisal of health, coping, and HRQOL following renal transplantation
were tested in this study with 160 renal transplant patients. This chapter presents a
discussion of the study results in five principal sections: (a) sample characteristics, (b)
interpretation of instruments, (c) interpretation of bivariate correlation analysis, (d)
interpretation of the findings related to research questions, (e) study strengths and
limitations, (f) recommendations for future research, and (g) conclusions and implications
for nursing practice.
Sample Characteristics
The characteristics of the sample in this dissertation research study were similar to
those of previous studies reported in the literature and, for the most part, reflected the
characteristics of renal transplant patients in the U.S. reported by the Organ Procurement
and Transplantation Network (OPTN; Annual report 2004). Of the 160 participants, 77.5%
were Caucasian and 20.6% were African-American. This percentage is consistent with the
annual report (2004), which documented 79.4% of recipients of living donor kidneys were
Caucasian and 15.0% were African-American, while 63.0% of recipients of cadaveric
donor kidneys were Caucasian and 29.6% were African-American. Sehgal (2000) also
reported African-American patients were less likely to have access to transplantation
111
compared with Caucasian patients. The majority of the participants (70.6%) were married,
compared to 66.3% in Franke et al�s (2003) study. Participants were well-educated, and
39.3% had a college or postgraduate degree. The mean age of this sample was 47.7 years
old, which mirrored the 47.7 years mean age in Rowenberger et al.�s (2005) study. The
mean age also is similar to previous studies in this transplant center (Kizilisik et al., 2003;
Pinson et al., 2000). Approximately 54% of the participants were male and 46% were
female. This gender distribution was slightly different from the 3:2 ratio between male and
female renal transplant patients reported by OPTN (Annual Report, 2004). The percentage
of females was higher compared to previous studies (Hathaway et al., 1998; Kizilsik et al.,
2003; Rosenberger et al., 2005). The first two leading causes of ESRD for the participants
were hypertension (25.6%) and diabetes (16.9%), which also reflected the common causes
of ESRD as reported by OPTN (Annual Report, 2004). The majority (61.3%) of the
participants in this study received hemodialysis therapy before transplantation and the
mean dialysis time was 2 years. These findings are similar with Rosenberger et al.�s (2005)
and Hathaway et al.�s (1998) studies. More than half of the participants received a living
donor graft (59.4%). This percentage is consistent with the trend reported by OPTN
(Annual report, 2004). The medications used for immunosuppressive therapy in this study
were similar to those reported in the annual report (2004), which were prednisone (91.4%),
tacrolimus (69.1%), Cellcept (82.3%), and sirolimus (21.2%). To enhance the
homogeneity of this study, only participants who were short-term post-transplant were
included. The mean time post-transplant was 18.8 months. Only 10% of participants had
one or two rejection episodes following transplantation, and the majority (59.4%) of the
participants had no transplant-related hospitalizations. Few studies in the literature

112
documented the data on rejection and hospitalizations. Thus, it is difficult to compare
these data with data from other studies.
There were no statistical significant differences on most of the demographic and
clinical data except the history of transplant-related hospitalizations between the early and
later period post-transplant groups. In the later period post-transplant groups, there were
more participants who had a history of transplant-related hospitalizations. One possible
explanation may be that the longer the time post-transplant, the greater the risk of having
rejection, infection, and side effects of medications, with a greater incidence of
hospitalization.
Interpretation of Instruments
The Cognitive Appraisal of Health
The Cognitive Appraisal of Health (CAHS) (Kessler, 1998) was used to measure
the participants� appraisal of health in this study. Internal consistency reliabilities of the
subscales of threat, challenge, and harm/loss were appropriate and similar with Kessler�s
(1998) study. However, the internal consistency reliability of the benign/irrelevant
subscale was not acceptable (0.53) and lower than the reliability reported in Kessler�s
(1998) study on breast cancer patients (0.78). The items in the benign/irrelevant subscale,
such as �I have nothing to lose because of this health condition;� �I don�t think much about
this health condition;� and �This health condition doesn�t affect my life;� seemed
unsuitable to renal transplant patients� health condition and seemed to measure different

113
interpretations of the health condition (e.g., no loss, not thinking, not affecting life). The
subscale needs to be refined and examined in other studies of renal transplant patients.
Participants scored relatively higher on the challenge subscale compared to other
subscales, so they indicated greater agreement with the challenge appraisal. There were no
previous studies assessing the cognitive appraisal of health in renal transplant patients, so
we cannot compare this finding with other studies. One possible explanation for this
finding may be that renal transplantation is considered the first-choice method of renal
replacement therapy for ESRD patients that helps restore the patients to a healthier daily
life (Jacobs & Luciani, 1992; Wallace, 1998). In addition, patients perceive transplantation
as a gift of life; therefore, participants appraise their health positively.
A one-component solution which explained 63.49% of total variance was derived
from the second-order factor analysis on the four subscales. This solution was consistent
with the theoretical bases of the CAHS that designated the four subscales measuring the
primary appraisal dimensions of cognitive appraisal (Kessler, 1998). Because the
challenge and benign/irrelevant subscales were negatively related to the component, while
threat and harm/loss subscales were positively related to the component, a higher weighted
score on the component suggested a negative primary appraisal of health.
Brief COPE
The Brief COPE (Carver, 1997) was used to measure coping strategies used by the
participants. The internal consistency reliabilities of some subscales, such as self-
distraction, active coping, behavioral disengagement, were low (Cronbach�s alpha less than
0.6) and the reliabilities of other subscale were appropriate. This alpha was different from

114
Carver�s reliability data in studies on breast cancer, depression, and AIDS. It was reported
the Cronbach�s alpha of the subscales of denial, venting, and acceptance were less than 0.6,
while the Cronbach�s alpha of other subscales exceeded 0.6 (Carver, 1997). The
inconsistency may be related to the different population studied. The lower internal
consistency reliabilities also may be explained by only two items in each subscale. This is
the first study using the Brief COPE to measure coping in renal transplant patients. The
reliability of this scale needs to be further examined in this population.
Participants in this study reported they used more active coping, emotional support,
positive reframing, acceptance, and religious coping, with relatively less use of denial,
behavioral disengagement, and self-blame coping. This finding was consistent with data
from previous studies on coping in renal transplant patients (Lindqvist, Carlsson, & Sjödén,
2004; Sutton & Murphy, 1989; Tix & Frazier, 1998). Lindqvist, Carlsson,and Sjödén
(2004) reported renal transplant patients used significantly more optimistic, supportive, and
self-reliant coping strategies, and less emotive coping in their study. Sutton and Murphy
(1989) also suggested that patients used more problem-oriented coping (e.g., try to look at
the problem objectively, maintain some control over the situation) than affective-oriented
coping (e.g., take drugs, drink alcohol, blame someone else). Religious coping also was
identified as a popular coping strategy in dealing with transplant-related stress (Sutton &
Murphy, 1989; Tix & Frazier, 1998). The names of coping strategies in these studies were
different because different coping measurements were used. However, the patterns of
coping strategies used more often and used less were similar because renal transplant
patients used more positive, active coping strategies and used less passive coping strategies.

115
Second-order factor analysis suggested there were two components for the 13
subscales of Brief COPE, which were interpreted as engagement coping and
disengagement coping. The two-component solution was different from Lazarus and
Folkman�s (1984) problem-focused and emotion-focused coping dimensions. Engagement
coping for this study included some problem-focused coping (e.g., planning, active coping,
and use of instrumental support) and some positive emotion-focused coping (e.g.,
acceptance, use of emotional support), while disengagement coping included behavioral
disengagement and some negative emotion-focused coping (e.g., denial, self-blame). This
two-component solution was consistent with Compas et al.�s (2001) conceptualization of
coping, which indicated that engagement coping includes responses that are oriented either
toward the source of stress or toward one�s emotions or thoughts; disengagement coping
refers to responses that are oriented away from the stressor or one�s emotions or thoughts.
This study was the first study using second order factors of Brief COPE in renal transplant
patients. The reliability and validity need to be further evaluated.
Perceived Health Competence Scale (PHCS)
Perceived self-efficacy related to health was measured using the PHCS. The
internal consistency reliability of this scale was adequate and similar with reliabilities
reported in other studies on healthy and chronic illness subjects (Smith et al., 1995). The
PHCS was not used in previous renal transplant studies. The findings of this study
suggested that participants had a high degree of perceived self-efficacy related to health.
Participants in this study all had a functional kidney graft. The literature indicated that
transplant patients reported better health compared to pre-transplant patients. All of these

116
factors may influence their perceived self-efficacy, and they reported high self-efficacy
scores on this scale.
Personal Resource Questionnaire (PRQ 2000)
The Personal Resource Questionnaire (PRQ 2000) was used to assess the perceived
social support of the participants. This questionnaire was used widely with patients with
other chronic illnesses, but had not been used in renal transplant patients before. The
internal consistency reliability of this questionnaire was high and within the range of the
Chronbach�s alpha values reported by Weinert (2003). Participants reported high levels of
perceived social support in this study. This finding was consistent with Frazier, Davis-Ali,
and Dahl�s (1995) study which indicated renal transplant patients received more helpful
social support and Christensen et al.�s (2002) study which suggested both cadaveric-donor
and living-donor renal transplant patients reported higher family support after
transplantation. This finding was also consistent with the fact that patients with high social
support have a greater chance of being selected for transplantation therapy.
Medical Outcomes Study 36-item Short Form Health Survey (SF-36®)
Self-reported HRQOL was measured using the SF-36®. This scale has
been used extensively in renal transplant patients. The internal consistency reliability for
the PCS and MCS were adequate and similar with reliabilities in a previous study (Feurer
et al., 2004). Participants in this study reported lower physical HRQOL compared with
the general U.S. population, especially role physical and general health subscales. This
was consistent with the studies conducted by Karam et al. (2003) and Tsuji-Hayashi et al.

117
(1999) which indicated renal transplant patients reported lower physical and general
health than the general population. The findings were inconsistent with Baiardi et al.�s
(2002) study which suggested renal transplant patients reported a slightly higher physical
HRQOL. The inconsistency may be related to the fact that Baiardi et al.�s study was
conducted in Italy with a small sample size of 34 renal transplant patients. Participants in
this study reported similar mental HRQOL to the general U.S. population. This finding
was consistent with previous studies (Karam et al., 2003; Rebollo et al., 2000). However,
Humar et al. (2003) reported older renal transplant recipients had better mental HRQOL
than national norms.
Symptom Checklist
The symptom checklist was developed for this dissertation research to measure the
side effects of immunosuppressive medications. The internal consistency reliability of the
symptom checklist was adequate. Factor analysis suggested a one-component solution
which indicated it measures one construct. As a group, participants scored low on the
checklist, which indicated that they experienced mildly bothersome side effects of
immunosuppressive medications. This finding was consistent with Rosenberger et al.�s
(2005) study which suggested renal transplant patients reported low stress from adverse
effects of immunosuppressive medication. The symptom checklist was newly developed
and the symptoms were related to the currently used immunosuppressive protocol
(prednisone, Cellcept, tacrolimus/sirolimus). The reliability and validity needs further
examination.

118
Interpretation of Bivariate Correlation Analysis
Bivariate correlation analysis was performed between observed variables in the
models. Relationships between transplant-related factors, personal and social resources,
appraisal of health, coping, and HRQOL were identified and explained below.
Transplant-related Variables and Psychosocial Variables
Side effects of immunosuppressive medications were positively related to negative
primary appraisal of health. This finding was expected. Participants experiencing more
bothersome symptoms of medication side effects would be more likely to appraise their
health as harm/loss. Experiencing more bothersome symptoms was associated with lower
degrees of perceived self-efficacy and greater use of disengagement coping strategies.
Participants with more bothersome side effects of medication may believe they cannot
control their health, reported lower degrees of perceived self-efficacy and used more
behavioral disengagement coping, denial, or self-blame coping strategies. More
bothersome symptoms of side effects of medications were related to worse physical and
mental HRQOL. This finding was consistent with the findings of previous studies which
indicated that higher levels of symptom distress are associated with lower perceived overall
quality of life (Geest & Moons, 2000; Hricik et al., 2001; Matas et al., 2002).
A history of transplant-related hospitalizations was positively correlated to negative
primary appraisal of health. Participants having hospitalizations appraised their health as
threat or harm/loss. This finding was expected. Results also suggested participants with a
history of hospitalizations reported lower degrees of perceived social support. Hospitalized
patients need more social support, and the available social support may not meet their

119
needs. Thus, they reported lower degrees of perceived social support. History of
transplant-related hospitalizations was negatively related to physical HRQOL. This
finding was reasonable. Hospitalized participants were patients who had transplant-related
complications such as rejection, infection, and these complications affect patients� physical
health. Therefore, they reported lower physical HRQOL.
Duration of dialysis before transplantation was identified as having a negative
relationship with physical HRQOL. This finding was consistent with Kizilisik et al.�s
(2003) study which indicated renal transplant patients who received dialysis therapy for six
months or more before transplant demonstrated lower physical HRQOL. Participants
receiving more than six months of dialysis before transplant were positively correlated with
episodes of transplant-related hospitalization. Participants with longer term dialysis had
more complications and worse health and were more likely to be hospitalized.
Time post-transplant was correlated to perceived self-efficacy. Participants with a
longer time post-transplant reported lower degrees of perceived self-efficacy. Although
transplant patients had better health outcomes than before, they still live with a chronic
health condition and need ongoing supervision and life-long immunosuppressive therapy.
These factors may influence their perceived self-efficacy. Results also suggested that the
longer the time post-transplant, the less the participants used engagement coping. This
finding was inconsistent with previous studies which suggested there were no differences
in frequency of problem-oriented coping between early and later period post-transplant
patients (Kong & Molassiotis, 1999; Sutton & Murphy, 1989). The time post-transplant
also was related to a history of transplant-related hospitalizations. The longer the time of
post-transplant, the more chances to have rejection, infection, and side effects of

120
medication, with greater chances of hospitalization. Living donor transplantation was also
related to longer time post-transplant. This finding was consistent with the findings of
Evans et al. (1984), who suggested renal transplant patients with living donor grafts had
higher survival rates and higher graft retention rates. The type of donor transplantation
(living or cadaveric) was not correlated to other variables in this study. This finding was
unexpected and needs further examination.
Correlations between Psychosocial Variables
Negative primary appraisal of health was positively correlated to disengagement
coping and negatively correlated to both physical and mental HRQOL. This was consistent
with previous theoretical works that suggested negative appraisals trigger emotional coping
and disengagement behavior (Lazarus & Folkman, 1984; Schwarzer, 1998). Participants
who appraised their health negatively used more disengagement coping. The relationship
between primary appraisal and HRQOL was not examined in previous renal transplant
studies. Participants who appraised their health as threat or harm/loss may have worse
health status and reported lower HRQOL.
Perceived self-efficacy was highly negatively correlated to negative primary
appraisal of health. Participants with high degrees of perceived self-efficacy appraised
their health less negatively. This finding supports previous theoretical works (Lazarus &
Folkman, 1984; Schwarzer, 1998; Shaw, 1999), which suggested perceived self-efficacy as
personal coping resource influences the primary appraisal in the coping process. Perceived
self-efficacy also was negatively related to disengagement coping. Participants with high
degrees of perceived self-efficacy believed they could control their health, so they would

121
not choose the disengagement coping strategies (e.g. denial, self-blame). Perceived self-
efficacy positively related to both physical and mental HRQOL. This finding was
consistent with previous theoretical and empirical studies that indicated that perceived self-
efficacy had a positive correlation with quality of life (Bandura, 2002; Cunningham,
Lockwood, & Cunningham, 1991; Han et al., 2005).
Perceived social support was negatively related to negative primary appraisal,
positively correlated to engagement coping, and negatively correlated to disengagement
coping. Perceived social support as a coping resource influences an individual�s primary
appraisal and coping strategies (Lazarus & Folkman, 1984; Schreurs & Ridder, 1997).
Participants with the perception or belief that others are available to provide emotional,
informational, and material resources in times of need may appraise their health less
negatively and tend to use more engagement coping strategies (e.g., active coping,
planning, use of emotional and instrumental support). Perceived social support had a
positive relationship with both physical and mental HRQOL. This finding was consistent
with findings from previous studies which suggested high degrees of perceived social
support were associated with better health outcomes (Cohen & Wills, 1985; Frazier, Davis-
Ali, & Dahl, 1995). Results also indicated that perceived social support was positively
correlated to perceived self-efficacy. This finding was reasonable. Participants with high
levels of perceived social support may perceive that they have a greater ability to control
their situation and reported higher degrees of perceived self-efficacy.
Disengagement coping was negatively related to both physical and mental HRQOL.
This finding was consistent with findings from previous studies which suggested that
disengagement forms of coping, such as denial, self-blame, behavioral disengagement were
122
related to poorer health outcomes (Folkman & Moskowitz, 2004). There were no
significant correlations between engagement coping and physical/mental HRQOL in this
study. This finding was unexpected and inconsistent with previous studies which indicated
that engagement coping (e.g., planning, use of informational support, active coping) was
related to better health outcomes (Christensen et al., 2000; Lindqvist, Carlsson, & Sjödén,
2004; Tix & Frazier, 1998). The specific relationship between coping and health outcomes
are probably affected by diverse personal and situational factors and need to be further
examined in complex model analysis.
Interpretation of Research Questions
Research Question 1. Does the hypothesized model fit the data following renal
transplantation?
Model fit analyses demonstrated that the initial models for PCS and MCS did not
fit the data well. Both the chi-squares were significant, which suggests that the models
should be rejected. The relative chi-squares were more than three and the CFI were less
than 0.90, which also suggested they were not a good fit with the data. For the initial
models, the important direct relationship between perceived self-efficacy and perceived
social support was missing, so it is reasonable that the initial models for PCS and MCS
were not a good fit for the data.
Perceived self-efficacy and perceived social support were considered as personal
and social resources for coping in this study. They were considered contextual factors as
the transplant-related variables were (e.g., history of hospitalizations, side-effect of
immunosuppressive medications, and donor type), which influence the coping process.

123
The paths from transplant-related variables to perceived self-efficacy and perceived
social support were removed in the alternative models for PCS and MCS. Perceived self-
efficacy and perceived social support were examined as exogenous variables. Results
indicated that the alternative models for PCS and MCS fit the data well. However, there
were a lot of non-significant paths in the alternative models. An empirical model
predicting PCS excluding paths with a p value more than 0.1 was derived and nested path
analyses suggested it fit the data well, and not statistically significant different from the
alternative model predicting PCS. Based on the nested path analyses, an empirical model
predicting MCS excluding paths with a p value more than 0.1 was derived. Analyses
indicated that the model fit the data well and was not significantly different from the
alternative model predicting MCS. The empirical models predicting PCS and MCS were
developed using only statistical criteria as indicators that may maximize a statistical fit to
the data, while ignoring the theoretical implications. An acceptable model should
consider both the theoretical and statistical soundness.
The researcher developed the hypothesized models for PCS and MCS based on
Lazarus and Folkman�s (1984) Stress and Coping Model. Unfortunately, the
hypothesized models did not fit the data well. Compared to the alternative model for
PCS, the significant paths from perceived self-efficacy to PCS and from primary
appraisal of health to PCS were absent in the hypothesized model predicting PCS. A
modified hypothesized model predicting PCS was derived by adding the paths from
perceived self-efficacy to PCS and from the primary appraisal of health to PCS in the
hypothesized model predicting PCS. The model analyses indicated that the modified
hypothesized model predicting PCS fit the data better than the hypothesized model

124
predicting PCS. Similarly, by adding the significant paths from the primary appraisal of
health to MCS and from medication side effects symptoms to MCS in the hypothesized
model predicting MCS, a modified hypothesized model predicting MCS was derived.
Analyses also suggested the model fit the data better than the hypothesized model
predicting MCS.
The modified hypothesized models predicting PCS and MCS were acceptable
because the models were developed by considering both the theoretical and statistical
meanings, and the models demonstrated good solutions and an adequate fit for the data.
The models suggested that HRQOL of renal transplant patients is the outcome of a
complex interplay between the transplant-related factors, personal and social resources
(perceived self-efficacy and perceived social support), cognitive appraisal of health, and
coping strategies. In the modified hypothesized models predicting PCS and MCS, history
of transplant-related hospitalization and medication side effects symptoms had a
significant direct positive effect on negative primary appraisal of health. Cognitive
appraisal refers to the evaluative process that reflects the person�s subjective
interpretation of an event (Lazarus & Folkman, 1984). Experiencing hospitalizations and
bothersome medication side effects symptoms would actually promote negative
appraisals of health. Perceived self-efficacy and perceived social support demonstrated
significant direct negative effects on negative primary appraisal of health. This finding
was consistent with previous theoretical works (Lazarus & Folkman, 1984; Schwarzer,
1998; Shaw, 1999), which suggested perceived self-efficacy and perceived social support
as resources that influence the primary appraisal in the coping process. Participants with

125
high degrees of perceived self-efficacy and perceived social support appraised their
health less negatively.
For the coping variables in the modified hypothesized models, results indicated
that negative primary appraisal of health had a significant positive direct effect on
disengagement coping; perceived self-efficacy had a significant negative direct effect on
disengagement coping; while perceived social support had a significant positive effect on
engagement coping. The findings were consistent with previous theoretical and empirical
works and are discussed in the following section on hypotheses.
Negative primary appraisal of health was found to have significant negative direct
effects on both physical and mental HRQOL. Cognitive appraisal was studied extensively
as an integrative part of the coping process and was not directly linked to health outcomes
in previous theoretical and empirical works. However, some studies on other chronic
illness suggested that lower threat and higher controllability appraisals were associated
with better psychosocial adjustment and health status (Pakenham & Rinaldis, 2001). It is
reasonable that participants who appraised their health negatively (as threat, harm/loss)
reported lower HRQOL. Perceived self-efficacy demonstrated a significant positive direct
effect on physical HRQOL. This finding was consistent with the literature. The theory on
self-efficacy suggests that it can have main effects on quality of life, as well as a moderate
effect on distress in the relationship to health (Bandura, 2002). Some empirical literature
on chronic illness also indicated that perceived self-efficacy had a positive correlation with
quality of life (Cunningham, Lockwood, & Cunningham, 1991; Han et al., 2005).
Participants with high degrees of perceived self-efficacy may think they have control over
their health and abilities to do daily activities, so they reported higher physical HRQOL.

126
Results also suggested that engagement coping had a significant negative effect on physical
HRQOL and disengagement coping had a significant negative effect on mental HRQOL.
The negative relationship between engagement coping and physical HRQOL was
unexpected and the effects of coping on HRQOL were discussed in the section on
hypothesis 5. Another interesting finding was that medication side effects symptoms had a
significant negative direct effect on mental HRQOL. This finding was consistent with
previous studies that suggested that adverse effects of immunosuppressive medication had
negative effects on life satisfaction and perceived overall quality of life (Geest & Moons,
2000; Hricik et al., 2001; Matas et al., 2002). Participants experiencing more bothersome
medication side effects symptoms may feel distress, lack of ability to perform work or
other activities, and disturbed relationships with family and friends, and therefore they
reported lower mental HRQOL.
Side effects of immunosuppressive medications, primary appraisal of health,
perceived self-efficacy, and perceived social support were significant predictors for coping
or HRQOL of the studied participants. Perceived self-efficacy had the largest total effect
on primary appraisal of health, followed by side effects of medication. Perceived social
support and primary appraisal had a nearly equivalent total effect on engagement coping.
Perceived self-efficacy had the largest total effects on disengagement coping and physical
HRQOL, followed by primary appraisal of health. For mental HRQOL, primary appraisal
of health had the largest total effects, followed by side effects of medication and perceived
self-efficacy. Few studies on renal transplant patients have examined the relationships
among these variables. However, as previously discussed, perceived self-efficacy,
perceived social support, and cognitive appraisal were significant predictors for health

127
outcomes in patients with other chronic illnesses. These findings suggest that increasing
the degrees of perceived self-efficacy, perceived social support, altering the negative
appraisal of health, and decreasing the effects of the side effects of immunosuppressive
medication are important nursing interventions that can improve the HRQOL of renal
transplant patients.
Five hypotheses were derived from the hypothesized models. The following
section focuses on the discussion of these hypotheses.
Hypothesis 1. As predicted, perceived self-efficacy had a significant direct effect
on negative primary appraisal of health. Participants with low degrees of perceived self-
efficacy were predicted to appraise their health conditions negatively (as threat or
harm/loss). According to Bandura (1995), perceived self-efficacy is the belief of what
one can do and this cognition mirrors a sense of control over the environment. Self-
efficacy makes a difference in how people feel and think. A low degree of perceived
self-efficacy is associated with depression, anxiety, helplessness, and pessimistic
thoughts (Schwarzer, 1998). Thus, individuals with low degrees of perceived self-
efficacy tend to appraise their health negatively. Perceived self-efficacy had both direct
effects and indirect effects through primary appraisal of health on disengagement coping.
This finding was consistent with theoretical literature (Schwarzer, 1998; Shaw, 1999).
Perceived self-efficacy as a personal coping resource affects primary appraisal and the
coping strategies selected by individuals. Participants with low degrees of perceived self-
efficacy might lack the motivation to act and invest less effort into changing the situation.
They used more disengagement coping such as behavioral disengagement or denial.

128
Hypothesis 2. Perceived social support had a direct negative effect on negative
primary appraisal of health. Participants with less perceived social support were
predicted to appraise their health as threat or harm/loss. This finding was consistent with
Lazarus and Folkman�s (1984) Stress and Coping Theory. According to Lazarus and
Folkman (1984), social support influences and informs primary and secondary appraisals
through a proactive response that minimizes stressful events before they become major
stressors. The perceptions of social support could potentially buffer the negative
emotional impact of stress appraisals through positive appraisals of the situation, or by
buffering against high levels of stress through the provision of material coping resources.
Thus, individuals with high levels of perceived social support appraised their health less
negatively.
Perceived social support had a significant positive direct effect on engagement
coping. This finding was consistent with theoretical works that suggested social support
plays a buffering role in stressful situations. Perceived social support has been studied
extensively as a coping resource and identified as having linkages with problem-focused
coping (Lazarus & Folkman, 1984; Schreurs & Ridder, 1997). The perception or belief
that others are available to provide emotional, informational, and material resources in
times of need influences what course of coping is pursued (Ptacek et al., 2002).
Individuals with high levels of perceived social support tended to use more engagement
coping strategies (e.g., active coping, planning, use of emotional and instrumental
support). Findings from this study suggested perceived social support had no significant
direct effect on disengagement coping. This finding was unexpected and inconsistent
with previous theoretical works that suggested a negative association between perceived

129
social support and emotion-focused coping (e.g., denial and self-blame). However,
perceived social support had an indirect effect on disengagement coping through negative
primary appraisal of health. This finding indicated participants with high degrees of
perceived social support used less disengagement coping by appraising their health
positively. This finding was consistent with Lazarus and Folkman�s (1984) Stress and
Coping Theory, which suggested that perceptions of social support affect coping through
their impact on appraisals of stressful situations.
Few empirical studies on renal transplant patients investigated the relationships
among perceived social support, appraisal, and coping. Some studies examined the
relationship between social support and psychological outcomes, which demonstrated
that social support or family support was negatively related to depression in renal
transplant patients (Christensen et al., 2002; Frazier, Davis-Ali, & Dahl, 1995). In this
study, perceived social support was not found to be a significant predictor for both
physical and mental HRQOL. This inconsistency may be due to differences in the
outcome constructs measured. The relationship between perceived social support and
HRQOL needs further exploration.
Hypothesis 3. Negative primary appraisals of health had a direct effect on
disengagement coping and no direct effect on engagement coping. Participants who
appraised their health negatively (as threat or harm/loss) were predicted to use more
disengagement coping strategies. This finding was consistent with Lazarus and
Folkman�s (1984) Stress and Coping Theory. According to Lazarus and Folkman (1984),
primary appraisal refers to a set of cognitions regarding the impact or significance of the
stressful encounter. In primary appraisals, a situation is perceived as being a challenge,

130
threat, harm/loss, or benign/irrelevant (Kessler, 1998; Schwarzer, 1998). With negative
appraisals, such as harm/loss, the person surrenders, overwhelmed by feelings of
helplessness and uncontrollability, which triggers disengagement coping strategies (e.g.,
behavioral disengagement, denial, self-blame, and venting). In addition, with negative
appraisals, the person is less likely to try engagement coping such as planning, active
coping, and use of instrumental support to change the stressful situation.
Hypothesis 4. Engagement coping had a significant negative direct effect on
physical HRQOL. The result indicated that participants who used more engagement
coping were predicted to report a lower physical HRQOL. This finding was interesting
and inconsistent with some research studies. Engagement coping (e.g., planning, active
coping, use of instrumental support, religion coping) was correlated with better health
outcomes in previous studies (Christensen et al., 2000; Lindqvist, Carlsson, & Sjödén,
2004; Tix & Frazier, 1998). However, Folkman and Moskowitz (2004) suggested that
some kinds of coping (e.g., seeking of instrumental support, problem-focused forms of
coping) are sometimes associated with negative outcomes, sometimes with positive ones,
and sometimes with neither, depending on characteristics of the appraised stressful
encounter. Theoretically, people who choose coping strategies that fit the appraised
controllability of a task will have better outcomes than people who do not (Folkman &
Moskowitz, 2004). For the participants, they may appraise the transplant-related
stressors such as side effects of medication and risk of rejection as uncontrollable, so
engagement coping strategies may not fit the context, resulting in negative outcomes.
Another explanation may be that this study was a cross-sectional design and cannot
determine any causal relationship. Participants reporting lower physical HRQOL had
131
limited daily activities and poor energy and needed more support, so they used more
engagement coping strategies such as use of instrumental support. Results also indicated
that disengagement coping had a negative direct effect on mental HRQOL. The more
disengagement coping was used, the lower the mental HRQOL of the participants. This
finding was consistent with previous theoretical and empirical studies which indicated
that certain kinds of coping strategies such as denial and behavioral disengagement are
consistently associated with poor mental health outcomes (Folkman & Moskowitz, 2004).
Hypothesis 5. History of transplant-related hospitalizations and side effects of
immunosuppressive medications had direct effects on primary cognitive appraisal of
health, while donor type, duration of dialysis before transplantation, and time post-
transplant were not significant predictors for primary appraisal of health. Participants
who had a history of transplant-related hospitalizations and reported more bothersome
medication side effects symptoms were predicted to appraise their health negatively (as
threat or harm/loss). No previous studies investigated the relationship between
transplant-related variables and cognitive appraisal of health. One plausible explanation
for this finding may be that hospitalizations and side effects of medications were the most
stressful events after transplantation for the participants. These events disrupt their
normal daily lives and bring distress to them. Thus, participants appraised their health
negatively. The finding that donor type, duration of dialysis before transplantation, and
time post-transplant had no significant direct effects on primary appraisal of health was
unexpected. It was reported that donor source, length of dialysis therapy prior to
transplantation, and time post-transplant affected the physical HRQOL of renal transplant
patients (Griva et al., 2002; Kizilisik et al., 2003). The participants in this study were
132
short-term post-transplant. They all (living or cadaveric donor transplantation) had a
functional kidney graft and they did not need dialysis. Therefore donor type and history
of dialysis before transplantation may not influence their appraisals of health. The
relationship between donor type, duration of dialysis before transplantation, time post-
transplant, and cognitive appraisals needs to be further examined in long-term post-
transplant patients.
Research Question 2. What are the effects of clinical factors (donor type, history of
transplant-related hospitalizations, side effects of immunosuppressive medications,
duration of dialysis, and time post-transplantation) on perceived self-efficacy, perceived
social support, cognitive appraisal of health, coping, and HRQOL following renal
transplantation?
Donor type (living vs. cadaveric) had no main effects on perceived self-efficacy,
perceived social support, cognitive appraisal of health, coping, and HRQOL following
renal transplantation. There were few studies in the literature addressing the effects of
donor type on perceived self-efficacy, perceived social support, cognitive appraisal of
health and coping in renal transplant patients. Some previous studies examined the effects
of donor type on the HRQOL of renal transplant patients. The finding of this study was
consistent with AasebØ et al. (2005) and Evans et al. (1984) who reported there were no
significant differences in HRQOL of recipients based on living vs. cadaveric donor kidney
transplantation. However, Griva et al. (2002) reported that the incidence of physical
HRQOL impairment was greater in cadaveric donor transplant recipients than living donor
transplant recipients. One possible explanation for this conflicting finding in Griva et al�s
study may be the large difference in the sample sizes of the living donor and cadaveric

133
donor transplantation groups (76 vs. 271) in Griva�s study. It was unexpected that donor
type had no main effects on perceived social support. It was expected that living donor
recipients might feel they had closer social network ties and perceived a higher level of
social support than cadaveric donor recipients. Griva et al. (2002) revealed that living
donor kidney recipients expressed stronger feelings of guilt in relation to the donor, which
may counteract the positive effect of closer social network ties. Another possible
explanation for the lack of significant main effects may be that participants in this study
reported high levels of perceived social support with a mean of 87 (range 15 to 105)
regardless of the donor type.
There were no differences in perceived self-efficacy, perceived social support,
cognitive appraisal of health, coping, and HRQOL following renal transplantation between
patients who had a history of transplant-related hospitalizations and those who had no
history of transplant-related hospitalizations. There were few studies with which we can
compare this finding. One possible explanation may be that the majority of the participants
had no transplant-related hospitalizations and most of the participants who had a history of
hospitalization were only hospitalized once. The finding of the effect of hospitalization on
HRQOL was consistent with Fujisawa et al. (2000) who reported there was no significant
difference in HRQOL when comparing renal transplant patients who had a period of
hospitalization with those with no history of hospitalization. However, results from the
study of Hathaway et al. (1998) indicated the number of hospital days in the first 6 months
predicted the quality of life of kidney transplant patients at 12 months. This finding
suggested that perhaps the duration of hospitalization was more important than whether or
134
not there were any transplant-related hospitalizations. The effect of the duration of
transplant-related hospitalizations on the psychosocial variables merits further exploration.
Results of the MANCOVA demonstrated that side effects of immunosuppressive
medications had significant main effects on the psychosocial variables. Univarate tests
revealed that participants with high scores (>17) on the symptom checklist appraised their
health condition more negatively; used more disengagement coping; had lower perceived
self-efficacy; and had lower physical and mental HRQOL than participants with low scores
(≤ 17). There were no significant differences in perceived social support and engagement
coping between the high and low scoring groups. Side effects of immunosuppressive
medications were considered the main stressor by renal transplant patients in many studies
(Fallon, Gould, & Wainwright, 1997; Frazier, Davis-Ali, & Dahl, 1995; Frey, 1990; Kong
& Molassiotis, 1999; Sutton & Murphy, 1989; White et al., 1990). Participants with
bothersome symptoms of medication side effects may feel more stressed and then may
appraise their health negatively. High stress and threat appraisal were positively correlated
to disengagement coping (Folkman, 1984; Sutton & Murphy, 1989). Thus participants with
high scores on the symptom checklist used more disengagement coping. With more
bothersome symptoms, participants may believe that they cannot manage their situation,
and these beliefs may cause lower perceived self-efficacy. Some previous studies
demonstrated that adverse effects of immunosuppressive medication were quite common
and headaches had the strongest negative effect on life satisfaction (Hricik et al., 2001;
Matas et al., 2002). Geest and Moons (2000) also indicated that higher levels of symptom
distress were associated with lower perceived overall quality of life. The findings from

135
these earlier studies supported the findings of the current study that indicated participants
with more bothersome symptoms of side effects reported lower HRQOL.
There were no significant main effects of duration of dialysis before transplantation
(≤ 6 months vs. > 6 months) on perceived self-efficacy, perceived social support, cognitive
appraisal of health, coping, or HRQOL following renal transplantation. The effects of
duration of dialysis on perceived self-efficacy, perceived social support, cognitive appraisal
of health, and coping of renal transplant patients were not documented in the literature.
Participants in this study with a functional graft were able to quit dialysis following
transplantation. They felt better than before and the experiences of dialysis before
transplantation may not influence the current subjective assessment of psychosocial
variables. However, patients with a longer history of dialysis had more complications
compared to those with less dialysis, which may influence their HRQOL. Kizilisik et al.
(2003) found that patients receiving dialysis therapy for six months or more demonstrated
lower post-transplant physical component scores on the SF-36 than patients who were
transplanted preemptively. In this study, although multivariate analysis indicated there
were no significant main effects, the univariate test noted that participants who had more
than six months of dialysis before transplantation reported lower physical HRQOL than
those who had equal to or less than six months of dialysis.
Time post-transplant had significant main effects on engagement coping, perceived
self-efficacy, and perceived social support, while it had no statistically significant main
effects on primary cognitive appraisal, disengagement coping, physical or mental HRQOL.
Participants in the early period post-transplant (less than 1 year) used more engagement
coping strategies than participants in the later period (1 to 3 years) and there were no
136
differences in using disengagement coping strategies between the two groups. These
findings differed from those reported by Kong and Molassiotis (1999), who found no
statistically significant differences in overall coping and all coping subscale scores between
patients within one year post-transplant and patients more than one year post-transplant.
This inconsistency may be due to the small sample size (23 in the early period vs. 78 in the
later period) in Kong and Molassiotis�s study. Another possible explanation may be that
Kong and Molassiotis examined the coping strategies in Chinese renal transplant patients
and used a different coping scale. Participants in the early period post-transplant face
many new challenges such as learning new self-care skills, intensive follow-up
appointments, and a need for informational and instrumental support. Thus, they use more
engagement coping (e.g., use of instrumental support, planning). Participants in the later
period post-transplant reported lower degrees of perceived self-efficacy and perceived
social support. Few previous studies examined the effects of time post-transplant on these
two variables in renal transplant patients. Participants in the later period post-transplant
still live with a chronic illness condition, face the high risk of chronic rejection, and need
ongoing supervision. All of these factors may influence their perceived self-efficacy.
Participants in the later period post-transplant had less need for social support compared to
immediate post-transplant patients. Their relatives and friends may think they have
adapted to this situation and not continue to provide support. Thus, they reported lower
degrees of perceived social support.
Cognitive primary appraisal of renal transplant patients has not been documented in
the literature. Effects of time on HRQOL were examined in some previous studies and
different patterns of changes in HRQOL were found. A study conducted by Ponton et al.

137
(2001) demonstrated there was a significant improvement in HRQOL between pre-
transplant and immediate post-transplant (first 6 months) patients, but the HRQOL
progressively worsened during the period of 7 to 36 months, and then settled back to levels
similar to those recorded immediately after transplant. Pinson et al. (2000) reported renal
transplant patients made small gains in physical performance and no changes in HRQOL
after transplantation, and then remained stable within the two years post-transplant.
Findings from the current study were consistent with Pinson et al.�s study which suggested
there were no statistically significant differences in HRQOL between the early period (less
than 1 year) and later period (1 to 3 years) groups.
Strengths and Limitations of the Study
Study Strengths
The major distinction of the study is that it is the first research study to test a
theoretical model of coping and HRQOL in renal transplant patients with a large sample size.
By incorporating personal and situational factors into the model, this study attempted to
identify how contextual factors influence the coping process and HRQOL in renal transplant
patients. This dissertation study attempted to synthesize a more expansive and functional
portrait of a person�s experience in coping with transplantation. Another distinction of this
study is that data were collected during the early post-transplant period (less than 1 year) and
at a later period (1 to 3 years following transplantation), which captured the different
relationships among the variables at two stages post-transplant and provided opportunities for
comparison between the two groups.
138
In this study, both objective and subjective, self-reported data were collected from all
subjects, which enhances the study�s validity. The effects of clinical factors such as duration
of dialysis, donor type, history of transplantation related hospitalizations, and side effects of
immunosuppressive medications on coping and HRQOL were assessed, which provide the
objective data for the study. Psychosocial variables were measured using instruments with
established validity and reliability that had been validated in patients with chronic illnesses,
which enhances the construct validity of this study. A relatively large sample size was
obtained providing adequate power for the statistical analyses. Path analysis and multivariate
statistical methods were used to analyze the data.
Study Limitations
There were several limitations in this study, including factors that potentially impact
external validity, construct validity, and internal validity. External validity is concerned with
the generalizability of the findings to other samples. Study participants were recruited from a
single transplant center that was affiliated with an academic health science center. The
geographic location of the transplant center may introduce potential bias that could limit the
generalizability of the findings to other populations of renal transplantation. Another factor
potentially influencing the external validity of this study is the convenience sampling method
used in this study. The convenience sample potentially limited representation of the broader
characteristics of the general renal transplant population. Participants in this study were more
educated than the general population; had a higher percentage of females compared to the
gender distribution of general renal transplant population; and were short term post-transplant.
Therefore, the findings from this study would only potentially apply to a renal transplant
population with similar characteristics.

139
Construct validity refers to the extent to which instruments used in the study actually
measure the constructs of interest. The symptom checklist was developed for this
dissertation study and was untested in other samples. Using an untested symptom checklist
may potentially impact the construct validity of the study, although it showed adequate
internal consistency reliability in this study. The reliability and validity of the checklist need
to be further evaluated.
Use of the composite cognitive appraisal of health (CAHS) and Brief COPE scores in
data analysis may be another limitation in terms of exploring the influences of these
constructs in depth. By using the composite scores, we cannot identify the potential key roles
of the subscales represented in the CAHS and Brief COPE. Thus, it is difficult to determine
whether a given outcome can be attributed to certain kinds of appraisals (e.g. threat,
harm/loss, challenge, and benigh/irrelevant) or particular coping strategies (e.g. active coping,
positive reframing, use of instrumental support). In addition, most measures are self-
administered questionnaires that may be influenced by fluctuations in respondent attention,
motivation, comprehension, and response biases such as social desirability (Lispsey, 1990),
which can potentially cause measurement error.
Finally, use of a descriptive, correlational, cross-sectional design limits the ability to
make causal conclusions about the variables studied. This cross-sectional, one-time data
collection method also was unable to verify the temporal sequence of variables. This factor
is particularly salient in relation to the findings regarding cognitive appraisal of health,
coping, and HRQOL. Because participants were not studied prospectively over time, it is not
clear if the negative appraisal of health predicted worse HRQOL or worse HRQOL led to a
negative appraisal of health. Similarly, for the relationship between engagement coping and
physical HRQOL, it is difficult to interpret whether greater use of engagement coping

140
predicted worse physical HRQOL or worse physical HRQOL promoted greater use of
engagement coping.
Recommendations for Future Research
With respect to study strengths, limitations, and findings, the following strategies
are recommended for future research. First, research samples need to be recruited from
other geographic regions and minority populations in an attempt to study these
relationships in more diverse samples.
Second, longitudinal and experimental designs are needed to address the issue of
causality. In addition, the longitudinal study could start at the evaluation of transplantation
stage, enabling changes in the coping process from pre-transplant to post-transplant to be
captured. For the study design, another recommendation would be to blend quantitative
and qualitative methodologies. Qualitative research may help identify, clarify, or confirm
key constructs and themes that portray perceptions and experiences about coping with renal
transplantation.
Third, the model tested in this study can be modified by including gender, race, and
education level and removing some non-significant clinical data (e.g., donor type, duration
of dialysis) in future studies. Literature suggested gender, race, and education level are
important factors that influence HRQOL.
Fourth, the symptom checklist needs further examination in other organ transplant
patients (e.g., liver, heart, lung transplant). Since symptoms of immunosuppressive
medication side effects are important predictors for coping and HRQOL, the checklist can
be used to examine whether similar effects occurs in other organ transplant patients, and its
reliability and validity can be tested in these populations.

141
Finally, replication studies are recommended. The process of theory validation
requires systematic replication and cross-validation to increase confidence in the
generalizability of findings. The theory validation process involves considering whether
the model varies across groups. The model of coping and HRQOL was tested in a sample
consisting of both kidney transplant patients at an early period (less than 1 year) and later
period (1 to 3 years) post-transplant. Further studies could examine whether the model fits
the data in a sample including only patients at immediate post-transplant (less than 6
months) or at long-term post-transplant (more than 3 years). The model also could be
tested with different organ transplant patients (e.g., liver, heart, and lung transplant
patients). Analysis of data across groups and model comparison over time would provide a
more in-depth understanding of the model of coping and HRQOL.
Conclusions and Implications for Nursing Practice
There has been relatively little empirical research on testing models of coping and
HRQOL in renal transplant patients. This study examined the relationships between
transplant-related clinical variables (history of transplant-related hospitalizations, side-
effect of immunosuppressive medications, donor type, duration of dialysis before
transplant, and time post-transplant), perceived self-efficacy, perceived social support,
cognitive appraisal of health, coping, and HRQOL in a model of coping and HRQOL. This
model was developed based upon the theoretical model of Lazarus and Folkman�s (1984)
stress and coping, and statistical fit. Findings suggested the modified hypothesis models
predicting PCS and MCS fit the data well. Findings demonstrated that history of transplant-
related hospitalizations, side effects of immunosuppressive medications, perceived self-
142
efficacy, and perceived social support are significant predictors for negative primary
appraisal of health. Perceived self-efficacy and negative primary appraisal are significant
predictors for disengagement coping, while perceived social support is a significant
predictor for engagement coping. Perceived self-efficacy, negative primary appraisal of
health, and engagement coping are significant predictors for physical HRQOL. Side
effects of immunosuppressive medications, negative primary appraisal of health, and
disengagement coping are significant predictors for mental HRQOL. Findings also
indicated that there were no significant effects of donor type, duration of dialysis before
transplantation, or history of transplant-related hospitalizations on the psychosocial
variables after controlling for time post-transplant. Participants with high scores (>17) on
the symptom checklist appraised their health negatively, used more disengagement coping,
had lower degrees of perceived self-efficacy, and reported lower physical and mental
HRQOL than participants with low scores (<17) on the symptom checklist. Participants
less than one year post-transplant used more engagement coping, and reported higher
degrees of perceived self-efficacy and perceived social support than participants in the later
period post-transplant. These findings have important theoretical and practical
implications for nursing.
This study provides preliminary evidence to support the modified hypothesis model
on coping and HRQOL in renal transplant patients. The testing of the model of coping and
HRQOL advances theoretical knowledge of the concepts of coping and HRQOL. This
model also can provide a conceptual framework for future studies in the area of coping and
HRQOL. Findings from this study not only provide empirical support for important
established relationships related to coping and HRQOL, but also provide some new

143
findings, such as primary appraisal of health having direct effects on both physical and
mental HRQOL. This model can guide nursing practice by providing a framework that
incorporates various individual and situational variables relevant to nurses working with
transplant patients. The model may contribute to the development of effective intervention
strategies to help patients cope with their transplantation and improve their HRQOL.
Findings suggested that perceived self-efficacy had the largest effects on negative
primary appraisal of health, disengagement coping, and physical HRQOL. This finding
indicated that perceived self-efficacy plays an important role in the model. Renal
transplant nurses need to consider developing interventions to enhance perceived self-
efficacy in patients. If self-efficacy can be enhanced, patients may appraise their health
less negatively, use less disengagement coping, and report higher physical HRQOL.
Symptoms of immunosuppressive medications were also identified as significant predictors
for negative primary appraisal of health and mental HRQOL. This finding provides
empirical support recommending the development of new medication with fewer side
effects, using a protocol with optimal benefit for patients, and actively treating with the
symptoms of medication side effects. Renal transplant nurses also need to develop
interventions to alleviate bothersome symptoms and educate patients about coping with the
side effects of medications. Primary appraisal of health served as a mediator and plays a
key role in the model of coping and HRQOL. In addition to physical impairment
influencing HRQOL, the model suggested that the subjective appraisal of health probably
affects how people cope and assess their HRQOL. Therefore, renal transplant nurses need
to understand the perceptions of their patients and help them alter their negative appraisals
of their health.

144
Health-related quality of life of renal transplant patients is the outcome of a
complex interplay between clinical factors, personal and social resources, cognitive
appraisal of health, and coping strategies. Holistic and dynamic interventions including
physical and psychosocial components are needed to help renal transplant patients cope
with transplantation and improve their HRQOL.

145
APPENDIX A
COGNITIVE APPRAISAL OF HEALTH SCALE (CAHS)
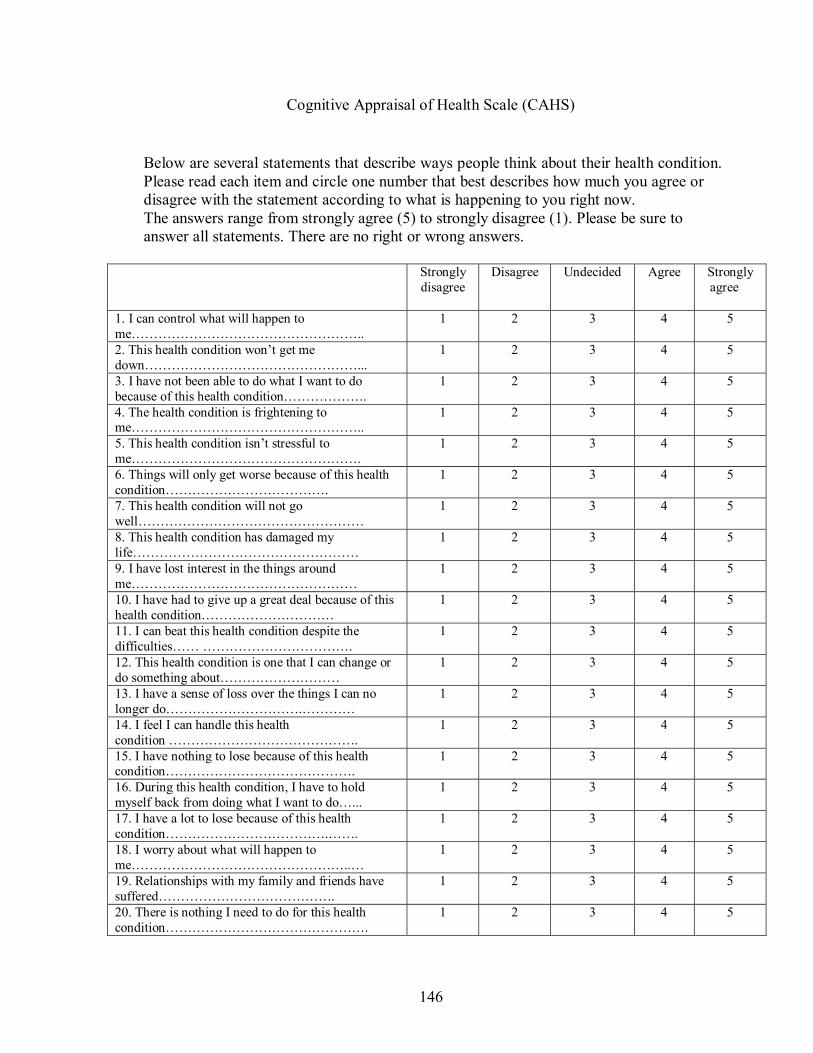
146
Cognitive Appraisal of Health Scale (CAHS)
Below are several statements that describe ways people think about their health condition. Please read each item and circle one number that best describes how much you agree or disagree with the statement according to what is happening to you right now. The answers range from strongly agree (5) to strongly disagree (1). Please be sure to answer all statements. There are no right or wrong answers.
Strongly disagree
Disagree Undecided Agree Strongly agree
1. I can control what will happen to me�����������������..
1 2 3 4 5
2. This health condition won�t get me down����������������...
1 2 3 4 5
3. I have not been able to do what I want to do because of this health condition������.
1 2 3 4 5
4. The health condition is frightening to me�����������������..
1 2 3 4 5
5. This health condition isn�t stressful to me�����������������.
1 2 3 4 5
6. Things will only get worse because of this health condition������������.
1 2 3 4 5
7. This health condition will not go well�����������������
1 2 3 4 5
8. This health condition has damaged my life�����������������
1 2 3 4 5
9. I have lost interest in the things around me�����������������
1 2 3 4 5
10. I have had to give up a great deal because of this health condition����������
1 2 3 4 5
11. I can beat this health condition despite the difficulties�� �����������.
1 2 3 4 5
12. This health condition is one that I can change or do something about���������
1 2 3 4 5
13. I have a sense of loss over the things I can no longer do����������.����
1 2 3 4 5
14. I feel I can handle this health condition ��������������.
1 2 3 4 5
15. I have nothing to lose because of this health condition��������������.
1 2 3 4 5
16. During this health condition, I have to hold myself back from doing what I want to do�...
1 2 3 4 5
17. I have a lot to lose because of this health condition������������.��.
1 2 3 4 5
18. I worry about what will happen to me����������������..�
1 2 3 4 5
19. Relationships with my family and friends have suffered�������������.
1 2 3 4 5
20. There is nothing I need to do for this health condition���������������.
1 2 3 4 5

147
Strongly disagree
Disagree Undecided Agree Strongly agree
21. I have been harmed in some way by this health condition�������..�����
1 2 3 4 5
22. I need to know more before I can do anything about this health condition��������.
1 2 3 4 5
23. I don�t think much about this health condition���������������.
1 2 3 4 5
24. This health condition has caused me to learn more about myself�����������.
1 2 3 4 5
25. I have been hurt by this health condition�����������..���..
1 2 3 4 5
26. There is a lot I can do to overcome this health condition���������������.
1 2 3 4 5
27. I have to accept this health condition���������������.
1 2 3 4 5
28. This health condition doesn�t affect my life������������������
1 2 3 4 5

148
APPENDIX B
PERSONAL RESOURCE QUESTIONNAIRE (PRQ2000)

149
PERSONAL RESOURCE QUESTIONNAIRE (PRQ2000)
Below are some statements with which some people agree and others disagree. Please read each statement and CIRCLE the response most appropriate for you. There is no right or wrong answer.
1 STRONGLY DISAGREE 2 DISAGREE 3 SOMEWHAT DISAGREE 4 NEUTRAL 5 SOMEWHAT AGREE 6 AGREE
7 STRONGLY AGREE
Q-1. There is someone I feel close to who makes me feel secure����������������..
1 2 3 4 5 6 7
Q-2. I belong to a group in which I feel important�����������������.
1 2 3 4 5 6 7
Q-3. People let me know that I do well at my work (job, homemaking)�������������..
1 2 3 4 5 6 7
Q-4. I have enough contact with the person who makes me feel special������������.
1 2 3 4 5 6 7
Q-5. I spend time with others who have the same interests that I do��������������.
1 2 3 4 5 6 7
Q-6. Others let me know that they enjoy working with me (job, committees, projects)�������
1 2 3 4 5 6 7
Q-7. There are people who are available if I need help over an extended period of time������..
1 2 3 4 5 6 7
Q-8. Among my group of friends we do favors for each other�����������������
1 2 3 4 5 6 7
Q-9. I have the opportunity to encourage other to develop their interests and skills��������.
1 2 3 4 5 6 7
Q-10. I have relatives or friends that will help me out even if I can�t pay them back���������..
1 2 3 4 5 6 7
Q-11. When I am upset, there is someone I can be with who lets me be myself����������.
1 2 3 4 5 6 7
Q-12. I know that others appreciate me as a person������������������..
1 2 3 4 5 6 7
Q-13. There is someone who loves and cares about me�������������������...
1 2 3 4 5 6 7
Q-14. I have people to share social events and fun activities with���������������..
1 2 3 4 5 6 7
Q-15. I have a sense of being needed by another person
1 2 3 4 5 6 7

150
APPENDIX C
PERCEIVED HEALTH COMPETENCE SCALE (PHCS)

151
Perceived Health Competence Scale (PHCS)
This is a questionnaire designed to determine the way in which different people view certain important issues related to their health. Each item is a belief statement, with which you may agree or disagree. Next to each statement is a scale that ranges from strongly disagree (1) to strongly agree (5). Respond to each of the following items by putting a mark through one box next to each statement, using the response choices listed below. Please try to respond to each item separately without thinking about the other items. Choose your answers thoughtfully and make your answers as true FOR YOU as you can. Please answer every item. There are no �right� or �wrong� answers, so choose the most accurate answer for YOU-not what you think most people would say or do. Strongly Strongly
Disagree Agree 1 2 3 4 5
1. It is difficult for me to find effective solutions for health problems that come my way������������...
2. I find efforts to change things that I don�t like about my health are ineffective�����������..
3. I handle myself well with respect to my health������������
4. I am able to do things for my health as well as most other people����..
5. I succeed in the projects I undertake to improve my health�������.
6. Typically, my plans for my health don�t work out well��������
7. No matter how hard I try, my health doesn�t turn out the way I would like�
8. I�m generally able to accomplish my goals with respect to my health���.
1 2 3 4 5
1 2 3 4 5
1 2 3 4 5
1 2 3 4 5
1 2 3 4 5
1 2 3 4 5
1 2 3 4 5
1 2 3 4 5

152
APPENDIX D
BRIEF COPE
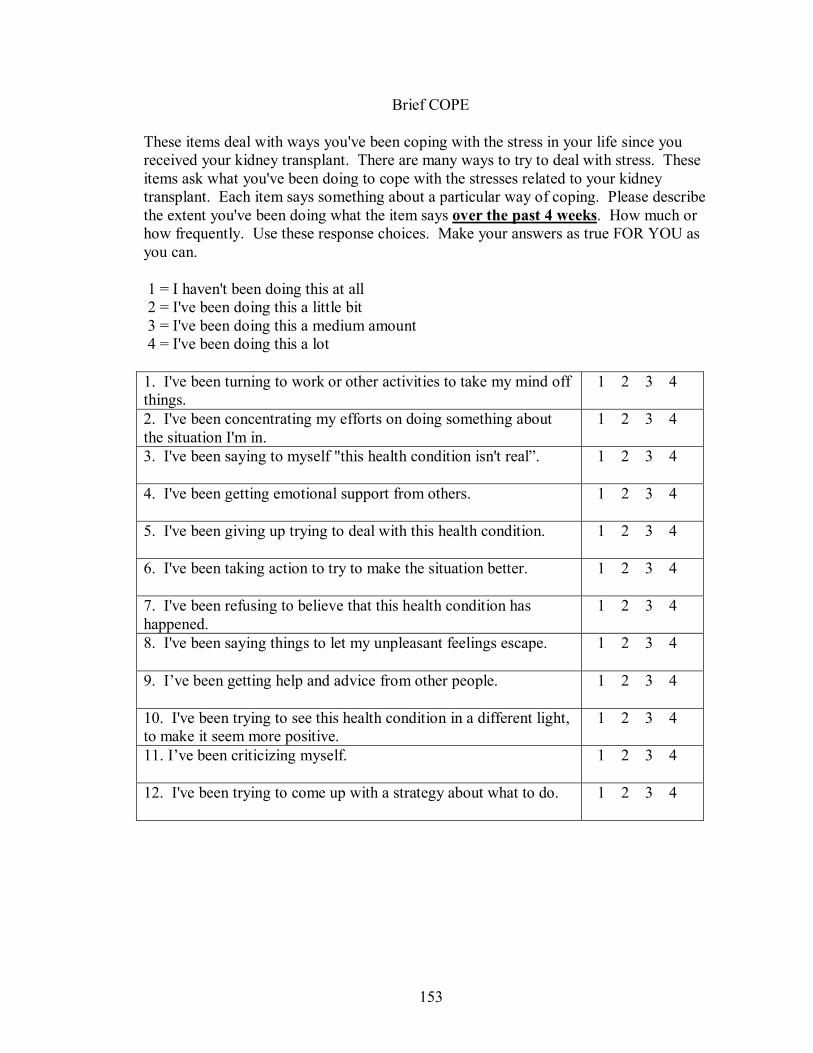
153
Brief COPE
These items deal with ways you've been coping with the stress in your life since you received your kidney transplant. There are many ways to try to deal with stress. These items ask what you've been doing to cope with the stresses related to your kidney transplant. Each item says something about a particular way of coping. Please describe the extent you've been doing what the item says over the past 4 weeks. How much or how frequently. Use these response choices. Make your answers as true FOR YOU as you can.
1 = I haven't been doing this at all 2 = I've been doing this a little bit 3 = I've been doing this a medium amount 4 = I've been doing this a lot
1. I've been turning to work or other activities to take my mind off things.
1 2 3 4
2. I've been concentrating my efforts on doing something about the situation I'm in.
1 2 3 4
3. I've been saying to myself "this health condition isn't real�.
1 2 3 4
4. I've been getting emotional support from others.
1 2 3 4
5. I've been giving up trying to deal with this health condition.
1 2 3 4
6. I've been taking action to try to make the situation better.
1 2 3 4
7. I've been refusing to believe that this health condition has happened.
1 2 3 4
8. I've been saying things to let my unpleasant feelings escape.
1 2 3 4
9. I�ve been getting help and advice from other people.
1 2 3 4
10. I've been trying to see this health condition in a different light, to make it seem more positive.
1 2 3 4
11. I�ve been criticizing myself.
1 2 3 4
12. I've been trying to come up with a strategy about what to do.
1 2 3 4
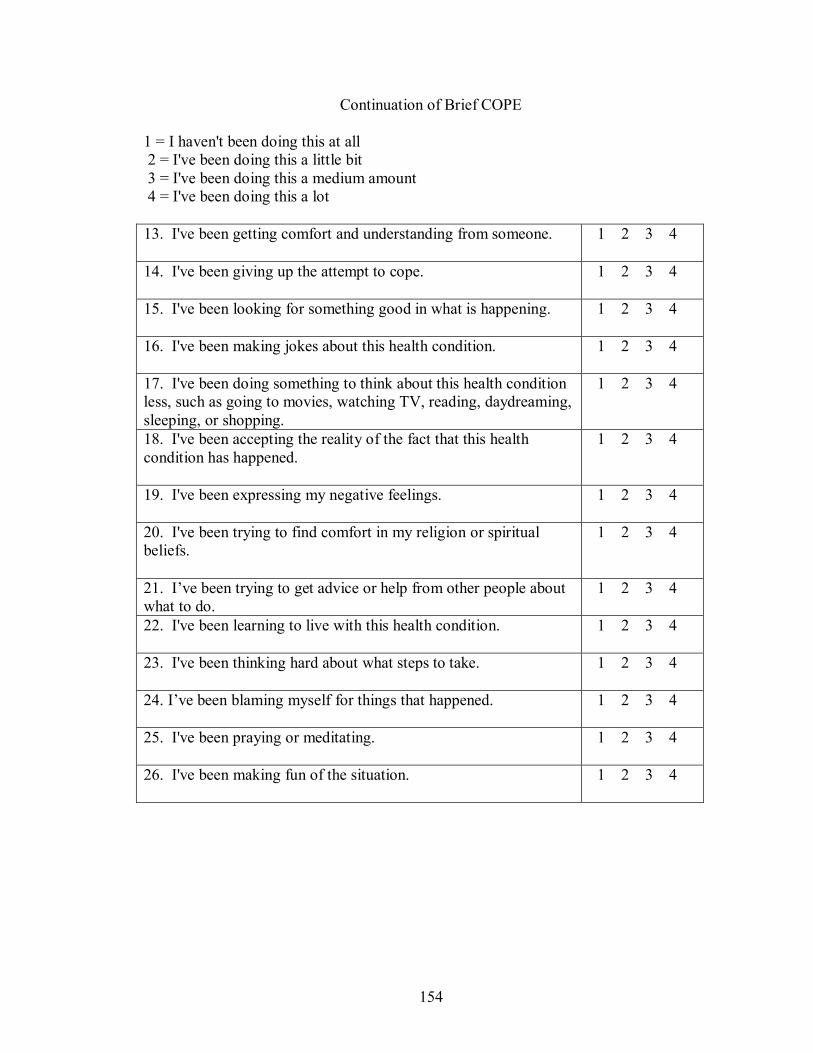
154
Continuation of Brief COPE
1 = I haven't been doing this at all 2 = I've been doing this a little bit 3 = I've been doing this a medium amount 4 = I've been doing this a lot 13. I've been getting comfort and understanding from someone.
1 2 3 4
14. I've been giving up the attempt to cope.
1 2 3 4
15. I've been looking for something good in what is happening.
1 2 3 4
16. I've been making jokes about this health condition.
1 2 3 4
17. I've been doing something to think about this health condition less, such as going to movies, watching TV, reading, daydreaming, sleeping, or shopping.
1 2 3 4
18. I've been accepting the reality of the fact that this health condition has happened.
1 2 3 4
19. I've been expressing my negative feelings.
1 2 3 4
20. I've been trying to find comfort in my religion or spiritual beliefs.
1 2 3 4
21. I�ve been trying to get advice or help from other people about what to do.
1 2 3 4
22. I've been learning to live with this health condition.
1 2 3 4
23. I've been thinking hard about what steps to take.
1 2 3 4
24. I�ve been blaming myself for things that happened.
1 2 3 4
25. I've been praying or meditating.
1 2 3 4
26. I've been making fun of the situation.
1 2 3 4

155
APPENDIX E
HEALTH STATUS SURVEY (SF-36®)

156
Health Status Survey (SF-36®)
This survey asks for your views about your health. Answer each question by marking a circle with the best answer you can give. Thank you.
1. In general, would you say your health is:
Excellent Very good Good Fair Poor
(Mark only one circle).
The following items are about activities you might do during a typical day. Does your health now limit you in these activities? If so, How much?
Yes, Limited
a lot
Yes, Limited a little
No, Not
Limited at all
2. Vigorous activities, such as running, lifting heavy objects, participating in strenuous sports�����.
3. Moderate activities, such as moving a table, pushing a vacuum cleaner, bowling or shopping��.
4. Lifting or carrying groceries���������
5. Climbing several flights of stairs�������.
6. Climbing one flight of stairs���������
7. Bending, kneeling, or stooping��������
8. Walking more than a mile����������
9. Walking several blocks�����������
10. Walking one block������������.
11. Bathing or dressing yourself��������..
During the past 4 weeks, have you had any of the following problems with your work or other regular daily activities as a result of your physical health?
Yes No
12. Cut down on the amount of time you spent on other work activities�
13. Accomplished less than you would like������������
14. Were limited in the kind of work or other activities�������.
15. Had difficulty performing work or other activities (for example, it took extra effort)
During the past 4 weeks, have you had any of the following Yes No

157
problems with your work or other regular daily activities as a result of any emotional problems (such as feeling depressed or anxious)? 16. Cut down the amount of time you spent on work or other activities��..
17. Accomplished less than you would like�������������..
18. Didn�t do work or other activities as carefully as usual�������..
19 During the past 4 weeks, to what extent has your physical health or emotional problems interfered with your normal social
Not at all
Slightly
Moderately
Quite a bit
Extremely
activities with family, friends, neighbors or groups?...........................................................
20. How much bodily pain have you had during the past 4 weeks?..
None Very Mild
Mild Moderate
Severe Very Sever
e 21. During the past 4 weeks, how much did pain interfere with your normal work
Not at all
A little bit
Moderately
Quite a bit
Extremely
(including both outside the home and housework)?....................................................
The following questions are about how you feel and how things have been with you during the past 4 weeks. For each question, please give the one answer that comes closest to the way you have been feeling. How much time during the past 4 weeks:
All of the
time
Most of the time
A good bit of the
time
Some of the time
A little of the time
None of the time
22. Did you feel full of pep?......
23. Have you been a very nervous person?.........................
24. Have you felt so down in the dumps that nothing could cheer you up?.......................................
25. Have you felt calm and peaceful?....................................

158
26. Did you have a lot of energy?.......................................
27. Have you felt downhearted and blue?....................................
28. Did you feel worn out?........
29. Have you been a happy person?......................................
30. Did you feel tired?...............
31. During the past 4 weeks, how much of the time has your physical health or emotional problems interfered with your social activities (like visiting with friends, relatives, etc.)?.........................................
All of the
time
Most of the time
Some of the time
A little of the time
None of the time
How TRUE or FALSE is each of the following statements for you?
Definitely true
Mostlytrue
Don�t know
Mostly false
Definitely false
32. I seem to get sick a little easier than other people������������
33. I am as healthy as anybody I know�..
34. I expect my health to get worse���
35. My health is excellent������..
36. Compared to one year ago, how would you rate your health in general now?
Much better
Somewhat better
About the same
Somewhat worse
Much worse
159
APPENDIX F
SYMPTOM CHECKLIST

160
Symptom Checklist
We are interested in learning about symptoms that you currently have that may be related to your kidney transplant. If you are currently experiencing any of the following symptoms, please check the appropriate box for that symptom.
Yes I have this and it bothers me
No
I don�t have this Not at all
Slightly Moderately Quiet a bit
Extremely
1. excess hair growth
2. hair loss
3. headache
4. hand tremors
5. overgrowth of gum tissue
6. diarrhea/GI distress
7. acne
8. difficulty sleeping
9. high blood sugar
10. high blood pressure
11. weight gain
12. tiredness

161
APPENDIX G
DEMOGRAPHIC AND CLINICAL DATA FORM
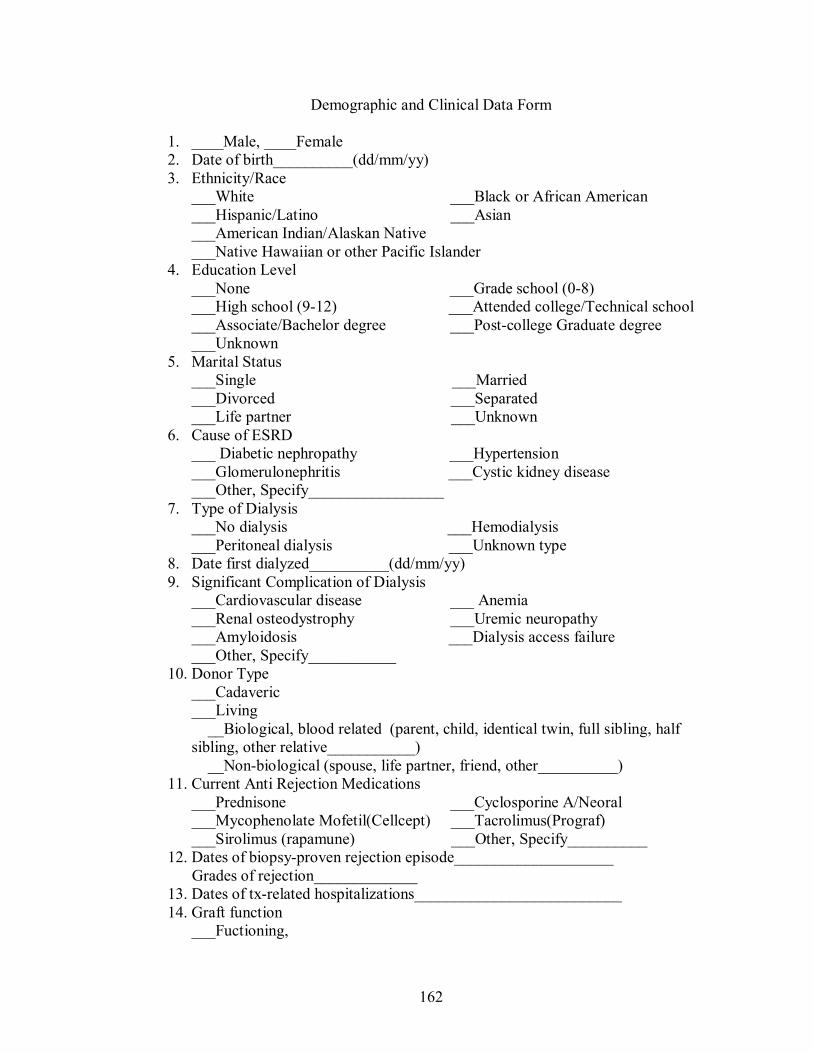
162
Demographic and Clinical Data Form
1. ____Male, ____Female 2. Date of birth__________(dd/mm/yy) 3. Ethnicity/Race
___White ___Black or African American ___Hispanic/Latino ___Asian ___American Indian/Alaskan Native ___Native Hawaiian or other Pacific Islander
4. Education Level ___None ___Grade school (0-8) ___High school (9-12) ___Attended college/Technical school ___Associate/Bachelor degree ___Post-college Graduate degree ___Unknown
5. Marital Status ___Single ___Married ___Divorced ___Separated ___Life partner ___Unknown
6. Cause of ESRD ___ Diabetic nephropathy ___Hypertension ___Glomerulonephritis ___Cystic kidney disease ___Other, Specify_________________
7. Type of Dialysis ___No dialysis ___Hemodialysis ___Peritoneal dialysis ___Unknown type
8. Date first dialyzed__________(dd/mm/yy) 9. Significant Complication of Dialysis
___Cardiovascular disease ___ Anemia ___Renal osteodystrophy ___Uremic neuropathy ___Amyloidosis ___Dialysis access failure ___Other, Specify___________
10. Donor Type ___Cadaveric ___Living __Biological, blood related (parent, child, identical twin, full sibling, half sibling, other relative___________) __Non-biological (spouse, life partner, friend, other__________)
11. Current Anti Rejection Medications ___Prednisone ___Cyclosporine A/Neoral ___Mycophenolate Mofetil(Cellcept) ___Tacrolimus(Prograf) ___Sirolimus (rapamune) ___Other, Specify__________
12. Dates of biopsy-proven rejection episode____________________ Grades of rejection_____________ 13. Dates of tx-related hospitalizations__________________________ 14. Graft function
___Fuctioning,

163
Serum Creatinine_______mg/dl Creatinine clearance_______ml ___Failed
15. Date of transplanted_____________(dd/mm/yy)

164
REFERENCES
Aasebϕ, W., Midtvedt, K., Hartmann, A. and Stavem, K. (2005) Predictors of health-related quality of life in hypertensive recipients following renal transplantation. Clinical Transplantation, 19, 756-762.
Abrams, M.A. (1973) Subjective social indications. Social Trends, 4, 35-36.
Ahmad, M.M. (2005) Psychometric evaluation of the Cognitive Appraisal of Health Scale with patients with prostate cancer. Journal of Advanced Nursing, 49 (1), 78-86.
Aldwin, C.M. (1994) Stress, coping, and development: An integrative perspective. New
York: Guilford.
American Nurses� Association (1995) Nursing�s social policy statement. Washington, DC: American Nurses� Publications.
Andrews, F.M. (1974) Social indicators and perceived life quality. Social Indicators
Research, 1, 279-299. Annual Report (2003) of the Organ Procurement and Transplantation Network and the
Scientific Registry of Transplant Recipients: Transplant Data, 2003, March 16. http://www.optn.org/data/annualReport.asp.
Aranda, M.P., & Knight, B.G. (1997) The influence of ethnicity and culture on the
caregiver stress and coping process: A sociocultural review and analysis. The Gerontologist, 37(3), 342-354.
Baiardi, F., Esposti, E.D., Cocchi, R., Fabbri, A., Sturani, A., Valpiani, G., & Fusaroli, M.
(2002) Effects of clinical and individual variables on quality of life in chronic renal failure patients. Journal of Nephrology, 15(1), 61-67.
Bakewell, A.B., Higgins, R.M., & Edmunds, M.E. (2001) Does ethnicity influence
perceived quality of life of patients on dialysis and following renal transplant? Nephrology Dialysis Transplantation, 16, 1395-1401.
Bandura, A. (2002) Self-efficacy: The exercise of control. New York: W.H. Freeman. Bandura, A. (1977) Self efficacy: Toward a unifying theory of behavioral change.
Psychological Review, 84(2), 191-215. Bandura, A. (Ed.). (1995) Self efficacy in changing societies. New York: Cambridge University Press.

165
Bergner, M. (1989) Quality of life, health status, and clinical research. Med Care, 27 (Suppl), 148-156.
Bollen, K.A. (1989) Structural equations with latent variables. New York: John Wiley &
Sons. Borenstein, M., Rothstein, H., & Cohen, J. (1997) Power and precision: A computer
program for statistical power analysis and confidence intervals. Teaneck: Biostat. Bradburn, N.M. (1969) The structure of psychological well-being. Chicago: Aldine. Brandt, P., & Weinert, C. (1981) PRQ: A social support measure. Nursing Research, 30,
277-280. Bremer, B.A., & McCauley, C.R. (1986) Quality-of-life measures: Hospital interview
versus home questionnaire. Health Psychology, 5(2), 171-177. Bremer, B.A., McCauley, C.R., Wrona, R.M., & Johnson, J.P. (1989) Quality of life in
end-stage renal disease: A reexamination. American Journal of Kidney Diseases, 13(3), 200-209.
Cameron, J.I., Whiteside, C., Katz, J., & Devins, G.M. (2000) Differences in quality of life
across renal replacement therapies: A meta-analytic comparison. American Journal of Kidney Disease, 35(4), 629-637.
Campbell, A., Converse, P., & Rodgers, W. (Eds.). (1976) The quality of American life.
New York: Russell Sage Foundation. Compas, B.E., Connor-Smith, J.K., Saltzman, H., Thomsen, A.H., & Wadsworth, M.E.
(2001) Coping with stress during childhood and adolescence: problems, progress, and potential in theory and research. Psychological Bulletin, 127(1), 87-127.
Carone, D.A., Jr., & Barone, D.F. (2001) A social cognitive perspective on religious
beliefs: Their functions and impact on coping and psychotherapy. Clinical Psychology Review, 21(7), 989-1003.
Carver, C.S. (1997) You want to measure coping but your protocol�s too long: Consider
the Brief COPE. International Journal of Behavioral Medicine, 4, 92-100. Carver, C.S., Scheier, M.F., & Weintraub, J.K. (1989) Assessing coping strategies: A
theoretically based approach. Journal of Personality and Social Psychology, 56, 267-283.
Cella, D.F. (1995) Measuring quality of life in palliative care. Sem Oncol, 22(Suppl 3), 73-
81.

166
Chang, E.C. (1998) Dispositional optimism and primary and secondary appraisal of a stressor: Controlling for confounding influences and relations to coping and psychological and physical adjustment. Journal of Personality and Social Psychology, 74(4), 1109-1120.
Christensen, A.J., Ehlers, S.L., Raichle, K.A., Bertolatus, J.A., & Lawton, W.J. (2000)
Predicting change in depression following renal transplantation: effect of patient coping preferences. Health Psychology, 19(4), 348-353.
Christensen, A.J., Raichle, K., Ehlers, S.L., & Bertolatus, J.A. (2002) Effect of family
environment and donor source on patient quality of life following renal transplantation. Health Psychology, 21(5), 468-476.
Clark, P., & Bowling, A. (1989) Observational study of quality of life in nursing homes
and a long-stay ward for the elderly. Ageing and Society, 9, 123-148. Cohen, S., & Syme, S.L. (Eds.). (1985) Social support and health. New York: Academic
Press. Cohen, S., & Will, T.A. (1985) Stress, social support, and the buffering hypothesis.
Psychological Bulletin, 98, 310-357. Cohen, S., Gottlieb, B.H., & Underwood, L.G. (2001) Social relationships and health:
Challenges for measurement and intervention. Advances in Mind-Body Medicine, 17, 129-141.
Covic, A., Seica, A., Gusbeth-Tatomir, P., Gavrilovici, O., & Goldsmith, D.J.A. (2004)
Illness representations and quality of life scores in haemodialysis patients. Nephrol Dial Transplant, 19(8), 2078-2083.
Cunningham, A.J., Lockwood, G.A., & Cunningham, J.A. (1991) A relationship between
perceived self-efficacy and quality of life in cancer patients. Patient Education and Counseling, 17(1), 71-78.
Duborsky, S.L., & Penn, I. (1980) Psychiatric consideration in renal transplant surgery.
Psychosomatics, 21, 481-491. Evans, R.W., Hart, L.G., & Manninen, D.L. (1984) A comparative assessment of the
quality of life of successful kidney transplant patients according to source of graft. Transplantation Proceedings, 16(5), 1353-1358.
Fallon, M., Gould, D., & Wainwright, S.P. (1997) Stress and quality of life in the renal
transplantation patient: A preliminary investigation. Journal of Advanced Nursing, 25(3), 562-570.

167
Farquhar, M. (1995) Definitions of quality of life: A taxonomy. Journal of Advanced Nursing, 22, 502-508.
Ferrans, C.E., & Powers, M.J. (1985) Quality of Life Index: Development and
psychometric properties. Advances in Nursing Science, 8(1), 15-24. Feurer, I.D, Moore, D.E, Speroff, T., Liu, H., Payne, J., Harrison, C., & Pinson, C.W.
(2004) Refining a health-related quality of life assessment strategy for solid organ transplant patients. Clinical Transplantation, 18(Suppl. 12), 1-8.
Fisher, R., Gould, D., Wainwright, S., & Fallon, M. (1998) Quality of life after renal
transplantation. Journal of Clinical Nursing, 7, 553-563. Fitzpatrick, R., Newman, S., Lamb, R., & Shipley, M. (1988) Social relationships and
psychological well-being in rheumatoid arthritis. Social Science and Medicine, 27, 399-403.
Folkman, S. (1992) Making a case for coping. In B. Carpenter (Ed.), Personal coping:
Theory, research, and application (pp. 38-39). Westport, Connecticut: Praeger. Folkman, S., Lazarus, R.S., & Dunkel-Schetter, C. (1986) The dynamics of a stressful
encounter: Cognitive appraisal, coping, and encounter outcomes. Journal of Personality and Social Psychology, 50, 992-1003.
Folkman, S., & Moskowitz, J.T. (2004) Coping: Pitfalls and promise. Annual Review of
Psychology, 55, 745-774. Franke, G.H., Heemann, U., Kohnle, M., Luetkes, P., Maehner, N., & Reimer, J. (2000)
Quality of life in patients before and after kidney transplantation. Psychology and Health, 14, 1037-1049.
Franke, G.H., Reimer, J., Kohnle, M., Luetkes, P., Maehner, N., & Heemann, U. (1999)
Quality of life in end-stage renal disease patients after successful kidney transplantation: Development of the ESRD symptom checklist-transplantation module. Nephron, 83, 31-39.
Franke, G.H., Reimer, J., Philipp, T., & Heemann, U. (2003) Aspects of quality of life
through end-stage renal disease. Quality of Life Research, 12, 103-115. Frazier, P.A., Davis-Ali, S.H., & Dahl, K.E. (1995) Stressors, social support, and
adjustment in kidney transplant patients and their spouses. Social Work in Health Care, 21(2), 93-108.
Frey, G.M. (1990) Stressors in renal transplant recipients at six weeks after transplant.
ANNA Journal, 17(6), 443-446,450.

168
Fujisawa, M., Ichikawa, Y., Yoshiya, K., Isotani, S., Higuchi, A., Nagano, S., et al. (2000) Assessment of health-related quality of life in renal transplant and hemodialysis patients using the SF-36 health survey. Urology, 56, 201-206.
Fusilier, M.R, Ganster, D.C., & Mayes, B.T. (1987) Effects of social support, role stress,
and locus of control on health. Journal of Management, 13, 517-528. Geest, S.D., & Moons, P. (2000) The patient�s appraisal of side-effects: The blind spot in
quality-of-life assessments in transplant recipients. Nephrol Dial Transplant, 15, 457-459.
George, L.K., & Bearon, L.B. (Ed.). (1980) Quality of life in older persons: Meaning and
measurement. New York: Human Sciences Press. Gorlen, T., Ekeberg, Q., Abdelnoor, M., Enger, E., & Aarseth, H.P. (1993) Quality of life
after kidney transplantation: A 10-22 years follow-up. Scandinavian Journal of Urology and Nephrology, 27, 89-92.
Gritsch, H.A. (1996) Renal transplantation-improving the quality of life (editorial).
Journal of Urology, 56, 889. Griva, K., Ziegelmann, J.P., Thompson, D., Jayasena, D., Davenport, A., Harrison, M., &
Newman, S.P. (2002) Quality of life and emotional responses in cadaver and living related renal transplant recipients. Nephrology Dialysis Transplantation, 17, 2204-2211.
Hagger, M., & Orbell, S. (2003) A meta-analytic review of the common-sense model of
illness representations. Psychology and Health, 18(2), 141-184. Han, K.S., Lee, S.J., Park, E.S., Park, Y.J., & Cheol, K.H. (2005) Structural model for
quality of life of patients with chronic cardiovascular disease in Korea. Nursing Research, 54(2), 85-96.
Harasyko, C. (1989) Kidney transplantation. Nursing Clinics of North America, 24(4),
851-862. Harrell, F.E., Jr. (2001) Progression modeling strategies with applications to linear
models, logistic regression, and survival analysis. New York: Springer. Hathaway, D.K., Barr, M.L., Ghobrial, R.M., Rodrigue, J., Bogner, S., Prendergast, M.M.,
& Subaiya, I. (2003). The PORTEL registry: Overview and selected findings. Progress in Transplantation, (Suppl June), 3-13.
Hathaway, D., Strong, M., & Ganza, M. (1990) Post transplant quality of life
expectations. ANNA Journal, 17, 433-439, 450.
169
Hathaway, D.K., Winsett, R.P., Johnson, C., Tolley, E.A., Hartwig, M.. Milstead, J., Wicks, M.N., & Gaber, A.O. (1998) Post kidney transplant quality of life prediction models. Clinical Transplantation, 12, 168-174.
Hathaway, D., Winsett, R., & Peters, T. (1987) Psychosocial assessment of renal
transplant recipients. Dialysis & Transplantation, 16(8), 442. Hathaway, D., Winsett, R., Prendergast, M., & Subaiya, I. (2003). The first report from
the patient outcomes registry for transplant effects on life (PORTEL): differences in side-effects and quality of life by organ type, time since transplant and immunosuppressive regimens. Clinical Transplantation, 17, 183-194.
Hauser, L.M., Williams, J., Strong, M., & Hathaway D. (1991) Predicted and actual
quality of life changes following renal transplantation. Journal of the American Nephrology Nurses Association, 18(3), 295-303.
Hayward, M.B., Kish, J.P., Frey, G.M., Kircher, J.M., Carr, L.S., & Wolfe, C.M. (1989)
An instrument to identify stressors in transplant recipients. American Nephrology Nurses� Association Journal, 16, 81-84.
Helman, C.G. (1990) Culture, health and illness (2nd ed.). Toronto: Wright. Herrman, H. (1997) Universal construct of quality of life. Findings of the Global field
Test of the World Health Organization Quality of Life Assessment Instrument (WHOQOL). Paper presentation in the Quality of Life Symposium, Hong Kong.
Hertel, B.R. (1976) Minimizing error variance introduced by missing data routines in
survey analysis. Sociological Methods and Research, 4, 41-49. Holahan, C.J., & Moos, R.H. (1994) Life stressors and mental health: Advances in
conceptualizing stress resistance. In W.R. Avison & I.H. Gotlib (Eds.), Stress and mental health: Contemporary issues and prospects for the future (pp. 213-238). New York: Plenum.
Holahan, C.J., Moos, R.H., Holahan, C.K., & Brennen, P.L. (1997) Social context,
coping strategies, and depressive symptoms: An expanded model with cardiac patients. Journal of Personality and Social Psychology, 72, 918-928.
Hricik, D.E., Halbert, R.J., Barr, M.L., Helderman, J.H., Matas, A.J., Pirsch, J.D., et al.
(2001) Life Satisfaction in renal transplant recipients: Preliminary results from the transplant learning center. American Journal of Kidney Disease, 38(3), 580-587.
Humar, A., Denny, R., Matas, A.J., & Najarian, J.S. (2003) Graft and quality of life
outcomes in older recipients of a kidney transplant. Experimental and Clinical Transplantation, 2, 69-72.

170
Ichikawa, Y., Fujisawa, M., Hirose, E., Kageyama, T., Miyamoto, Y., Sakai, Y., et al. (2000) Quality of life in kidney transplant patients. Transplantation Proceedings, 32, 1815-1816.
Jacobs, C., & Luciani, J. (1992) Reappraisal of longterm renal replacement therapy.
Renal transplantation: Medical versus statistical approach. Blood Purification, 10(1), 5-12.
Jacobs, R.J., Pescovitz, M.D., Brook, B., Birnbaum, J., Dean, J., & Pus, N. (1998) A self-
administered quality of life questionnaire for renal transplant recipients. Nephron, 79, 123-124.
Ji, S.M. (2002) Basis and new development of clinical research on renal transplantation.
New Medicine, 33, 370-371. Jofre, R., Lopez-Gomez, J.M., Moreno, F., Sanz-Guajardo, D., & Valerrabano, F. (1998)
Changes in quality of life after renal transplantation. American Journal of Kidney Disease, 32(1), 93-100.
Johnson, J.P., McCauley, C.R., & Copley, J.B. (1982) The quality of life of hemodialysis
and transplant patients. Kidney International, 22, 286-291. Jöreskog, K.G., & Sörbom, D. (1988) LISREL 7: A guide to the program and applications. Chicago: SPSS, Inc. Joseph, J.T., Baines, L.S., Morris, M.C., & Jindal, R.M. (2003) Quality of life after
kidney and pancreas transplantation: A review. American Journal of Kidney Diseases, 42(3), 431-445.
Karam, V.H., Gasquet, I., Delvart, V., Hiesse, C., Dorent, R., Danet, C., et al. (2003)
Quality of life in adult survivors beyond 10 years after liver, kidney, and heart transplantation. Transplantation, 76(12), 1699-1704.
Keesing, R.M. (1981) Cultural anthropology: A contemporary perspective. New York:
Holt, Rinehart, and Winston. Kessler, T.A. (1998) The Cognitive Appraisal of Health Scale: Development and
psychometric evaluation. Research in Nursing & Health, 21, 73-82. Kizilisik, A.T., Feurer, I.D., VanBuren, D.H., Wise, P., Buren, D.V., Hopkins, J., et al.
(2003) Effects of diabetes and cadaveric organs on functional performance and health-related quality of life after kidney transplantation. The American Journal of Surgery, 186, 535-539.
Koch, U., & Muthny, F.A. (1990) Quality of life in patients with end-stage renal disease
in relation to the method of treatment. Psychotherapy psychosomatic, 54, 161-171.

171
Komproe, I.H., Rijken, M., Ros, W.J.G., & Winnubst, J.A.M. (1997) Available support
and received support: Different effects under stressful circumstances. Journal of Social and Personal Relationships, 14, 59-77.
Kong, I. L., & Molassiotis, A. (1999) Quality of life, coping and concerns in Chinese
patients after renal transplantation. International Journal of Nursing Study, 36(4), 313-22.
Laupacis, A., Keown, P., Pus, N., Krueger, H., Ferguson, B., Wong, C., & Muirhead, N.
(1996) A study of the quality of life and cost-utility of renal transplantation. Kidney International, 50, 235-242.
Laupacis, A., Pus, N., Muirhead, N., Wong, C., Ferguson, B., & Keown, P. (1993)
Disease-specific questionnaire for patients with a renal transplant. Nephron, 64, 226-231.
Lazarus, R.S. (1990) Theory-based stress measurement. Psychology Inquiry, 1, 3-51. Lazarus, R.S. (1993) Coping theory and research: Past, present, and future.
Psychosomatic Medicine, 55, 234-247.Co. Lazarus, R.S. (2000) Toward better research on stress and coping. American Psychologist,
55(6), 665-673. Lazarus, R.S., & Folkman, S. (1984) Stress, appraisal and coping. New York: Springer
Publishing. Lepore, S.J., Evans, G.W., & Schneider, M.L. (1991) Dynamic role of social support in
the link between chronic stress and psychological distress. Journal of Personality and Social Psychology, 61, 899-909.
Leventhal, H., Leventhal, E.A., & Contrada, R.J. (1998) Self-regulation, health, and
behavior: A perceptual-cognitive approach. Psychology and Health, 13, 717-733. Leventhal, H., & Nerenz, D. (1985) The assessment of illness cognition. In P. Karoly
(Ed), Measurement strategies in health psychology, (pp.517-555). New York: Wiley. Lewis, V.T., Starr, A., Ketefian, S., & White, J.M. (1990) Stress, coping, and quality of
life in family members of kidney transplant recipients. Journal of the American Nephrology Nurses Association, 17(6), 427-431.
Linqvist, R., Carlsson, M., & Sjödén, P.-O. (2004) Coping strategies of people with
kidney transplants. Journal of Advanced Nursing, 45(1), 47-52.

172
Lipsey, M.W. (1990) Design sensitivity: Statistical power for experimental research. Newbury Park: Sage Publications.
Luk, W.S.-C. (2004) The HRQoL of renal transplant patients. Journal of Clinical
Nursing, 13, 201-209. Macdonald, E.M., Pica, S. Mcdonald, S., Hayes, R.L., & Baglioni, A.J., Jr. (1998) Stress
and coping in early psychosis: Role of symptoms, self-efficacy, and social support in coping with stress. British Journal of Psychiatry-Supplementum, 172(33), 122-127.
Manne, S.L., & Zautra, A.J. (1989) Spouse criticism and support: Their association with
coping and psychological adjustment among women with rheumatoid arthritis. Journal of Personality and Social Psychology, 56, 608-617.
Manu, M.A., Radulescu, S., Harza, M., Manu, R., Capsa, D., & Sinescu, I. (2001) Quality
of life assessed by SF-36 health survey in renal transplant patients. Transplantation Proceedings, 33, 1927-1928.
Martin, J.C., & Sachse, D.S. (2002) Spirituality characteristics of women following renal
transplantation. Nephrology Nursing Journal, 29(6), 577-581. Matas, A.J., Halbert, R.J., Barr, M.L., Helderman, J.H., Hrick, D.E., Pirsch, J.D., et al.
(2002) Life satisfaction and adverse effects in renal transplant recipients: A longitudinal analysis. Clinical Transplantation, 16, 113-121.
McCarley, T., & Lewis, S.L. (1996) Acute and chronic renal failure. In S. M. Lewis, I. C.
Collier, & M. M. Heitkemper (Eds.), Medical-surgical nursing: Assessment and management of clinical problem (4th ed.) (pp. 1371-1412). St. Louis: Mosby.
McColl, M.A. Lei, H., & Skinner, H. (1995) Structural relationships between social
support and coping. Social Science & Medicine, 41(3), 395-407. McCrae, R.R., & Costa, P.T., Jr. (1986) Personality, coping, and coping effectiveness in
an adult sample. Journal of Personality, 54, 384-405. McHaffie, H.E. (1992) Coping: an essential element of nursing. Journal of Advanced
Nursing, 17, 933-940. Merluzzi, T.V., & Martinez-Sanchez, M.A. (1997) Assessment of self-efficacy and
coping with cancer: Development and validation of the cancer behavior inventory. Health Psychology, 16, 1-8.
Mingardi, G. and the DIA-QOL Group (1998) Quality of life and end stage renal disease
therapeutic programs. The International Journal of Artificial Organs, 21(11), 741-747.

173
Molzahn, E., Northcott, C., & Dossetor, B. (1997) Quality of life of individuals with end stage renal disease: Perceptions of patients, nurses, and physicians. Journal of the American Nephrology Nurses Association, 24(3), 325-333.
Moons, P., Vanrenterghem, Y., Hooff, J.P. van, Squifflet, J.P., Margodt, D., Mullens, M.,
et al. (2002) Steroids may compromise quality of life of renal transplant recipients on a tacrolimus-based regimen. Transplantation Proceedings, 34, 1691-1692.
Moss-Morris, R., Petrie, K. J., & Weinman, J. (1996) Functioning in chronic fatigue
syndrome: Do illness perceptions play a regulatory role? British Journal of Health Psychology, 1, 15-25.
Moss-Morris, R., Weinman, J., Petrie, K. J., Horne, R., Cameron, L. D., & Buick, D.
(2002) The revised illness perception questionnaire (IPQ-R). Psychology and Health, 17, 1-16.
Muthny, F.A., & Koch, U. (1991) Quality of life of patients with end-stage renal failure:
A comparison of hemodialysis, CAPD, and transplantation. Contrib Nephrpl, 89, 265-273.
Newton, R.R., & Rudestam, K.E. (1999) Your statistical consultant: Answers to your
data analysis questions. Thousand Oaks, CA: Sage Publication. Oberbauer, R., Hutchison, B., Eris, J., Arias, M., Claesson, K., Mota, A., et al. (2003)
Health-related quality-of-life outcomes of sirolimus-treated kidney transplant patients after elimination of cyclosporine A: results of a 2-year randomized clinical trial. Transplantation, 75(8), 1277-1285.
O�Neill, D.P., & Kenny, E.K. (1998) Spirituality and chronic illness. Image: Journal of
Nursing Scholarship, 30(3), 275-281. Ortuzar, M.G. (2001) Ethics and quality of life of kidney transplant patient.
Transplantation Proceedings, 33, 1913-1916. Pais-Riberiro, J.L. (2004) Quality of life is a primary end-point in clinical settings.
Clinical Nutrition, 23, 121-130.
Pakenham, K.I., & Rinaldis, M. (2001) The role of illness, resources, appraisal, and
coping strategies in adjustment to HIV/AIDS: the direct and buffering effects. Journal of Behavioral Medicine, 24(3), 259-279.
Parker, J.D.A. and Endler, N.S. (1996) Coping and defense: A historical overview. In M.
Zeidner & N.S. Endler (Eds.), Handbook of coping: Theory, research, applications. New York: Wiley.
174
Patrick, D.L., & Erickson, P. (Ed.). (1993) Health status and health policy: Quality of life in health care evaluation and resource allocation. New York: Oxford University Press.
Pigou, A.C. (Ed.). (1920) The economics of welfare. London: MacMillan. Pinson, C.W., Feurer, I.D., Payne, J. L., Wise, P.E., Shockley, S., & Speroff, T. (2000)
Health-related quality of life after different types of solid organ transplantation. Annals of Surgery, 232(4), 597-607.
Pisani, F., Vennarecci, G., Tisone, G., Buonomo, O., Iaria, G., Rossi, S., et al. (1997)
Quality of life and long-term follow-up after kidney transplantation: A 30-year clinical study. Transplantation Proceedings, 29, 2812-2813.
Ponton, P., Rupolo, G.P., Marchini, F., Feltrin, A., Perin, N., Mazzoldi, M.A., et al.
(2001) Quality-of-life change after kidney transplantation. Transplantation Proceedings, 33, 1887-1889.
Ptacek, J.T., Pierce, G.R., & Ptacek, J.J. (2002) The social context of coping with
prostate cancer. Journal of Psychosocial Oncology, 20(1), 61-80. Reed, P.G. (1987) Spirituality and well-being in terminally ill hospitalized adults.
Research in Nursing and Health, 10, 335-344. Rebollo, P., Ortega, F., Baltar, J.M., Alvarez-Ude, F., Navascues, R.A., Urena, A., &
Avarez-Grande, J. (2001) Is the loss of health-related quality of life during renal replacement therapy lower in elderly patients than in younger patients? Nephrology Dialysis Transplantation, 16, 1675-1680.
Rebollo, P., Ortega, F., Baltar, J.M., Badia, X., Alvarez-Ude, F., Diaz-Corte, C., et al.
(2000) Health related quality of life (HRQOL) of kidney transplanted patients: variables that influence it. Clinical Transplant, 14, 199-207.
Reimer, J., Franke, G.H., Philipp, T., & Heemann, U. (2002) Quality of life in kidney
recipients: Comparison of tacrolimus and cyclosporine-microemulsion. Clinical Transplantation, 16, 48-54.
Revicki, D.A., & Leidy, N.K. (1998) Questionnaire scaling: models and issues. In
Staquet M., Hays R., & Fayers P. (Eds) Quality of life assessment in clinical trials: Methods and practice (pp. 157-182). Oxford: Oxford University Press.
Revicki, D.A., Osoba, D., Faiclough, D., Barofsky, I., Berzon, R., Leidy, N.K., &
Rothman, M. (2000) Recommendations on health-related quality of life research to support labeling and promotional claims in United States. Quality of Life Research, 9, 887-900.

175
Rosenberger, J., Geckova, A.M., van Dijk, J.P., Roland, R., van den Heuvel, W.J.A., &
Groothoff, J.W. (2005) Factors modifying stress from adverse effects of immunosuppressive medication in kidney transplant recipients. Clinical Transplantation, 19, 70-76.
Rotter, J.B. (1975) Some problems and misconceptions related to the construct of internal
versus external control of reinforcement. Journal of Consulting and Clinical Psychology, 43, 56-67.
Russell, J.D., Beecroft, M.L., Ludwin, D., & Churchill, D.N. (1992) The quality of life in
renal transplantation- A prospective study. Transplantation, 54(4), 656-660. Scheier, M.F., & Carver, C.S. (1985) Optimism, coping, and health: Assessment and
implications of generalized outcome expectancies. Health Psychology, 4, 219-247. Schreurs, K.M.G., & Ridder D.T.D. (1997) Integration of coping and social support
perspectives: Implications for the study of adaptation to chronic disease. Clinical Psychology Review, 17(1), 89-112.
Schwarzer, R. (1993) Optimism, vulnerability, and self-beliefs as health-related
cognitions: A systematic overview. Psychology and Health, 9, 161-180. Schwarzer, R. (1998) Stress and coping from a social-cognitive perspective. Annals of the
New York Academy of Sciences, 851, 531-537. Sehgal, A.R. (2000) Outcomes of renal replacement therapy among blacks and women.
American Journal of Kidney Diseases, 35(4 suppl 1), 148-152. Shaw, C. (1999) A framework for the study of coping, illness behavior and outcomes.
Journal of Advanced Nursing, 29(5), 1246-1255. Shield, C.F., McGrath, M.M., & Goss, T.F. et al. (1997) Assessment of health-related
quality of life in kidney transplant patients receiving tacrolimus (FK506)-based versus cyclosporine-based immunosuppression. Transplantation, 64(12), 1738-1743.
Simmons, R.G., & Abress, L. (1990) Quality-of-life issues for end-stage renal disease
patients. American Journal of Kidney Disease, 15(3), 201-208. Simmons, R.G., Abress, L., & Anderson, C.R. (1988) Quality of life after kidney
transplantation. Transplantation, 45(2), 415-421. Smith, C.A., Dobbins, C.J., & Wallston, K.A. (1991) The mediational role of perceived
competence in psychological adjustment to rheumatoid arthritis. Journal of Applied Social Psychology, 21, 1218-1247.

176
Smith, M.S., Wallston, K.A., & Smith, C.A. (1995) The development and validation of the Perceived Health Competence Scale. Health Education Research: Theory and Practice, 10, 51-64.
Suls, J., & Fletcher, B. (1985) The relative efficacy of avoidant and nonavoidant coping
strategies: A meta-analysis. Health Psychology, 4, 249-288. Sutton, T.D., & Murphy, S.P. (1989) Stressors and patterns of coping in renal transplant
patients. Nursing Research, 38(1), 46-49. Taylor, S.E., & Aspinwall, L.G. (1996) Mediating and moderating processes in
psychosocial stress. In H.B. Kaplan (Ed.), Psychosocial stress: Perspectives on structure, theory, life-course, and methods (pp. 71-110). San Diego: Academic Press.
Testa, M.A., & Simonson, D.C. (1996) Assessment of quality-of-life outcomes. The New
England Journal of Medicine, 334(13), 835-840. Tix, A.P., & Frazier, P.A. (1998) The use of religious coping during stressful life events:
Main effects, moderation, and mediation. Journal of Consulting and Clinical Psychology, 66(2), 411-422.
Tsuji-Hayashi, Y., Fukuhara, S., Green, J., Takai, I., Shinzato, T., Uchida, K., et al. (1999)
Health-related quality of life among renal-transplant recipients in Japan. Transplantation, 68(9), 1331-1335.
U.S. Department of Health and Human Services. (2000, November) Healthy People 2010:
Understanding and improving health. (2nd ed.). Available at: www,health.gov/healthypeople/
Wallace, A.M. (1998) Renal transplantation. Association of Operating Room Nurses
(AORN) Journal, 68(6), 964-993. Wallston, K.A. (2001) Conceptualization and operationalization of perceived control. In
A. Baum & T.A. Revenson & J.L. Singer (Eds.), Handbook of health psychology. Mahwah, NJ: Lawrence Erlbaum Associates.
Wallston, K.A., Brown, G.K., Stein, M.J., & Dobbins, C.J. (1989) Comparing long and
short versions of the arthritis impact measurement scales. Journal of Rheumatology, 16, 1105-1109.
Ware, J.E. (1997) SF-36 health survey: Manual and interpretation guide. Health Institute,
New England Medical Center: Boston. Ware, J.E., & Sherbourne, C.D. (1992) The MOS 36-item Short Form Health Survey
(SF-36): I. Conceptual framework and item selection. Med Care, 30, 473-483.
177
Weinert, C. (1987) A social support measure: PRQ85. Nursing Research, 36, 273-277. Weinert, C. (2000) Social support in cyberspace. Rehabilitation Nursing, 25, 129-135. Weinert, C. (2003) Measuring social support: PRQ2000. In O. Strickland & C. DiIorio
(Eds.), Measurement of nursing outcomes: Vol. 3. Self care and coping (pp. 161-172). New York: Springer.
Weiss, R. (1974) The provision of social relationships. In D. Rubin (Ed.), Doing unto
others (pp.17-26). Englewood Cliffs, NJ: Prentice-Hall. White, M.J., Ketefian, S., Starr, A.J., & Voepel-Lewis, T. (1990) Stress, coping, and
quality of life in adult kidney transplant recipients. ANNA Journal, 17(6), 421-424. WHO (1948) Preamble to the Constitution of the World Health Organization as adopted
by the International Health Conference, New York, 19-22 June, 1946; signed on 22 July 1946 by the representatives of 61 States (Official Records of the World Health Organization, no. 2, p. 100) and entered into force on 7 April 1948.
Witzke, O., Becker, G., Franke, G., Binek, M., Philipp, T., & Heemann, U. (1997)
Kidney transplantation improves quality of life. Transplantation Proceedings, 29, 1569-1570.


















