Detection Algorithms in Implantable Cardioverter Defibrillators
Upload
curtis-mathewsCategory
view
219download
1
INTRODUCTION: INTRODUCTION: implantable cardioverter-defibrillators (ICDs) have clearly demonstrated to terminate an elevated percentage of sustained ventricular tachycardia (SVTs), both with shock therapy and, painlessly, with antitachycardia pacing (ATP). The purpose of this study was to investigate the efficacy and safety of ATP as 1st line therapy for terminating SVTs, occurring in patients (pts) with coronary artery disease (CAD) and severely depressed left ventricular ejection fraction (LVEF), due to not reversible causes, comparing this approach with shock.
CONCLUSIONS: CONCLUSIONS: our data suggest that ATP is a safe and effective therapeutic approach for SVTs termination, also in pts with DCM and very depressed LVEF; then, this therapeutic approach should be programmed “on” in all patients regardless LVEF.
SHOCK REDUCTION USING ATP AS 1ST LINE THERAPY FOR SHOCK REDUCTION USING ATP AS 1ST LINE THERAPY FOR SPONTANEOUS SUSTAINED VENTIRCULAR TACHYCARDIA IN PATIENTS SPONTANEOUS SUSTAINED VENTIRCULAR TACHYCARDIA IN PATIENTS
WITH ISCHEMIC DILATED CARDIOMYOPATHY AND SEVERLY DEPRESSED WITH ISCHEMIC DILATED CARDIOMYOPATHY AND SEVERLY DEPRESSED VENTRICULAR FUNCTION VENTRICULAR FUNCTION
Authors: Stefano Nardi MD, PhD, Luigi Argenziano MD, PhDAuthors: Stefano Nardi MD, PhD, Luigi Argenziano MD, PhD
Arrhythmia, Electrophysiologic Center and Cardiac Pacing Unit, Heart Department, PO Pineta Grande, Castel Volturno (CE), Italy (I)
METHODS:METHODS: from March 2004 through June 2013, 408 consecutive patients (pts) were considered eligible for this study, according with MADIT and/or SCD-HeFT criteria, and 387 of them (94,8%) accepted and underwent ICD implant. Pts were randomly assigned to ATP group (190/387) or shock group (197/387) and three zone of detection were assigned in all pts: a slow VTs window (320-400 msec), a fast VTs window (240-320 msec), and a ventricular fibrillation (VF) window (<320 msec). In ATP group, 3 burst sequence were programmed in slow VT zone and 1 burst sequence was programmed in fast VTs zone (burst sequences of 8-10 pulses at 88% CL) before shock, respectively, whereas in shock group (197/169) shock was adopted as 1st line therapy for all SVTs. No statistically differences, in term of age (72,2 vs 73,4, p=NS), sex (man 73,1% vs 69,3%, p=NS), NYHA functional class (2,8 vs 2,6, p=NS), LVEF (24,5% vs 26,9%) and drugs therapy were observed between two groups. Based on the evaluation of stored electrograms (EGMs), we aimed to prospectively follow pts and to analyze these two different therapeutic approach.
RESULTS:RESULTS: A total of 3.288 spontaneous VTs episodes occurred in 171 pts (41,9%) during a mean follow-up of 54,4±23,1 months (90 pts in ATP group and 81 pts in shock group). Among these, 2.235/3.288 (67,9%) were SVTs and 612 of them (27,4%) were detected in VF zone, and then treated with primary shock delivery, whereas in the remaining 1,623 of them (72,6%), 936 episodes occurred in ATP group (57,6%) and 687 episodes occurred in shock group (42,4%). In ATP group, ATP was able to terminate successfully 80,7% of SVTs, failed in 9,3% of SVTs, finally reverted by shocks, and in 10% of SVTs ATP was able to converted arrhythmias in a slower VT, outside the VT zone. 61% of these slower SVTs were self-terminating whereas 39% were redetected and treated. Finally, in primary intention-to-treat basis, ATP was successful in 834/936 SVTs (89%) and unsuccessful in 102/936 SVTs (11%). In contrast, 657/687 (95,6%) of all SVTs episode detected in VT zone and that occur in shock group were shock terminated, whereas 30/657 (4,4%) were accelerated into VF zone. The individual termination rate and acceleration rate per pt were comparable in both groups, as well as mean time of SVT termination (ATP=12.6 sec vs Shock=10.9 sec, p=NS).
SCARS
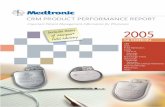
Figure 1: Rationale for ATP Rx is that a “WAVE-FRONT” critically temporized with VTCL and applied proximal to the “Slow Conduction
Zone” is able to capture the CIRCUIT, then interrupt the reentry
Does PAcINg Fast VT REducE Shock Rx? (PAIN FREE study *)
• All pts presents Ischemic - DCM (220 pts)• 93% of ep in traditional VF window (CL<320ms) are detect as FVT• ATP very efficacy for treatment FVT (77%)• 1 st ATP sequence in FVT zone was efficacy in 90% cases
LOW risk of Acceleration
Acceleration in 4-7% comparable with studies with ATP in traditional VT zone LOW risk of Syncope Syncope in 2% of cases, comparable with other studies with ICD
* Wathen M, Sweeney M, DeGroot P. Circulation. ‘01
BCL - adaptative
X % average tachycardia interval rilevato
Figure 2: ATP programmability with adaptative cycle length
RESULTS total RESULTS total episodes 3,288episodes 3,288
Pts with VTs Pts with VTs SVTs episodes SVTs episodes in VT zonein VT zone
Global Global 171 (44,1%)171 (44,1%) 16231623
ATP GroupATP Group 9090 936 (57,6%)936 (57,6%)
SHOCK GroupSHOCK Group 8181 687 (42,4%)687 (42,4%)
Delivered Therapy
ATP GROUPATP GROUP Successfull Successfull
Therapy (89%) Therapy (89%)
SHOCK GROUPSHOCK GROUP Successfull Successfull
Therapy (95,6%)Therapy (95,6%)
Figure 4: Results of a registry comparing ATP vs shock therapy as primary choice of VT treatment for a total of 387 pts enrolled