Intravenous thrombolysis for acute ischemic stroke
2
Case Report Intravenous Thrombolysis for Acute Ischemic Stroke in a Patient Receiving Rivaroxaban Anne Landais, MD,* and Caroline Ginoux, MD† Background: Rivaroxaban is an oral direct factor Xa inhibitor increasingly used in stroke prevention in nonvascular atrial fibrillation, primary prevention and treat- ment of venous thromboembolism, and secondary prevention in acute coronary syndromes. Methods: Thrombolytic treatment has established efficacy in acute ischemic stroke. Results: We report the case of a 76-year-old female under rivaroxa- ban for paroxysmal nonvalvular atrial fibrillation who presented an acute ischemic stroke. The brain magnetic resonance imaging diffusion-weighted sequences showed increased signal in the territory of the left middle cerebral artery. Platelet count was normal. PT was 55% (normal, 70-120); the international normalized ratio was 1.51 (normal, .90-1.40). She underwent intravenous thrombolysis 210 minutes after stroke onset without bleeding complication and with complete clinical recov- ery. Conclusions: This case underlines the need for further studies on the safety of thrombolysis in stroke patients taking rivaroxaban. Our case emphasizes the urgent need for sensitive coagulation bed-side tests during stroke emergencies. Key Words: Acute stroke—thrombolysis—rivaroxaban—new direct oral anticoagulant. Ó 2015 by National Stroke Association Rivaroxaban is an oral direct factor Xa inhibitor increas- ingly used in stroke prevention in nonvascular atrial fibrillation, primary prevention and treatment of venous thromboembolism, and secondary prevention in acute coronary syndromes. Thrombolytic treatment (rt-PA) has established efficacy in acute ischemic stroke. 1 We report the case of a 76-year-old female with past medical history of paroxysmal nonvalvular atrial fibrilla- tion, heart failure (New York Heart Association class I), pulmonary embolism, and hypertension, who presented to the emergency department for brutal-onset aphasia at 8.15 am. Five days previously, she had come to the emergency department for cardiac decompensation; a paroxysmal atrial fibrillation was diagnosed and treatment by rivar- oxaban 15 mg once daily (although the creatinine clear- ance according to the Cockroft–Gault formula was 57 mL/minute, thus needing no dosage adjustment) was introduced by the cardiologist before she returned home where she took her treatment regularly. The last intake was at 6.00 am. On arrival, she presented with isolated aphasia without any motor deficit, the National Institute of Health Stroke Score score on admission was 4. The brain magnetic resonance imaging diffusion-weighted se- quences showed increased signal in the territory of the left middle cerebral artery (Fig 1) with left M2 branches less visible than right ones on time of flight sequence. Blood pressure was 132/85 mm Hg. Platelet count was From the *Neurology Department, University Hospital of Pointe- a-Pitre, Route de Chauvel, Abymes Guadeloupe; and †Emergency Unit, University Hospital of Pointe- a-Pitre, Route de Chauvel, Abymes Guadeloupe, France. Received July 2, 2014; accepted October 27, 2014. A.L. has received compensation for travel expenses from Bayer Healthcare and Boehringer Ingelheim. C.G. has nothing to disclose. Address correspondence to Anne Landais, MD, Neurology Depart- ment, University Hospital of Pointe- a-Pitre, Route de Chauvel, 97139 Abymes Guadeloupe, France. E-mail: [email protected] . 1052-3057/$ - see front matter Ó 2015 by National Stroke Association http://dx.doi.org/10.1016/j.jstrokecerebrovasdis.2014.10.014 Journal of Stroke and Cerebrovascular Diseases, Vol. -, No. - (---), 2015: pp e1-e2 e1
-
Upload
javier-pacheco-paternina -
Category
Health & Medicine
-
view
72 -
download
0
Transcript of Intravenous thrombolysis for acute ischemic stroke

Case
ReportIntravenous Thrombolysis for Acute Ischemic Stroke in a PatientReceiving Rivaroxaban
Anne Landais, MD,* and Caroline Ginoux, MD†
From the *Neurology
�a-Pitre, Route de Chauv
Unit, University Hospi
Abymes Guadeloupe, Fr
Received July 2, 2014;
A.L. has received com
Healthcare and Boehring
Address corresponden
ment, University Hospita
Abymes Guadeloupe, Fr
1052-3057/$ - see front
� 2015 by National Str
http://dx.doi.org/10.1
Journal of Stroke and C
Background: Rivaroxaban is an oral direct factor Xa inhibitor increasingly used in
stroke prevention in nonvascular atrial fibrillation, primary prevention and treat-
ment of venous thromboembolism, and secondary prevention in acute coronary
syndromes. Methods: Thrombolytic treatment has established efficacy in acute
ischemic stroke. Results: We report the case of a 76-year-old female under rivaroxa-
ban for paroxysmal nonvalvular atrial fibrillation who presented an acute ischemic
stroke. The brain magnetic resonance imaging diffusion-weighted sequences
showed increased signal in the territory of the left middle cerebral artery. Platelet
count was normal. PTwas 55% (normal, 70-120); the international normalized ratio
was 1.51 (normal, .90-1.40). She underwent intravenous thrombolysis 210 minutes
after stroke onset without bleeding complication and with complete clinical recov-
ery. Conclusions: This case underlines the need for further studies on the safety of
thrombolysis in stroke patients taking rivaroxaban. Our case emphasizes the urgent
need for sensitive coagulation bed-side tests during stroke emergencies. Key Words:
Acute stroke—thrombolysis—rivaroxaban—new direct oral anticoagulant.
� 2015 by National Stroke Association
Rivaroxaban is an oral direct factor Xa inhibitor increas-
ingly used in stroke prevention in nonvascular atrial
fibrillation, primary prevention and treatment of venous
thromboembolism, and secondary prevention in acute
coronary syndromes. Thrombolytic treatment (rt-PA)
has established efficacy in acute ischemic stroke.1
We report the case of a 76-year-old female with past
medical history of paroxysmal nonvalvular atrial fibrilla-
Department, University Hospital of Pointe-
el, Abymes Guadeloupe; and †Emergency
tal of Pointe-�a-Pitre, Route de Chauvel,
ance.
accepted October 27, 2014.
pensation for travel expenses from Bayer
er Ingelheim. C.G. has nothing to disclose.
ce to Anne Landais, MD, Neurology Depart-
l of Pointe-�a-Pitre, Route de Chauvel, 97139
ance. E-mail: [email protected].
matter
oke Association
016/j.jstrokecerebrovasdis.2014.10.014
erebrovascular Diseases, Vol. -, No. - (---
tion, heart failure (New York Heart Association class I),
pulmonary embolism, and hypertension, who presented
to the emergency department for brutal-onset aphasia at
8.15 am.
Five days previously, she had come to the emergency
department for cardiac decompensation; a paroxysmal
atrial fibrillation was diagnosed and treatment by rivar-
oxaban 15 mg once daily (although the creatinine clear-
ance according to the Cockroft–Gault formula was
57 mL/minute, thus needing no dosage adjustment)
was introduced by the cardiologist before she returned
home where she took her treatment regularly. The last
intake was at 6.00 am.
On arrival, she presented with isolated aphasia
without any motor deficit, the National Institute of
Health Stroke Score score on admission was 4. The brain
magnetic resonance imaging diffusion-weighted se-
quences showed increased signal in the territory of the
left middle cerebral artery (Fig 1) with left M2 branches
less visible than right ones on time of flight sequence.
Blood pressure was 132/85 mm Hg. Platelet count was
), 2015: pp e1-e2 e1

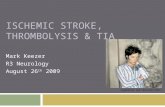
Figure 1. Brain magnetic resonance imaging Diffusion-weighted sequence
showing increased signal in the territory of the left middle cerebral artery.
A. LANDAIS AND C. GINOUXe2
normal (265,000 [150,000-400,000]). Prothrombin time
was 55% (normal, 70-120); the international normalized
ratio (INR) was 1.51 (normal, .90-1.40), fibrinogen was
5.44 g/L (1.7-4). No other coagulation test was available
in emergency in our hospital. Particularly, we did not
have specific rivaroxaban plasma concentration dosage
and specific anti–factor Xa activity.
After discussion with the family concerning the risk of
major and eventually fatal bleeding during thrombolysis
under NOAC, and after they decided to take the risk and
gave their consent, the patient received 63 mg rt-PA
3 hours and 30 minutes (210 minutes) after onset of symp-
toms and 5 hours and 45 minutes (345 minutes) after the
last intake of rivaroxaban. She rapidly improved to an
NIHSS of 0 and completely recovered from her aphasia.
The control computed tomography scan performed the
day after showed no hemorrhagic transformation.
Discussion
There are few reports about strokes under rivaroxaban,
their treatment, and outcome.2,3 It is possible that the
favorable clinical outcome and the absence of bleeding
complications in our case are related to the reduced
dose of rivaroxaban. Assays measuring specific
anticoagulation effects are not always available but
should be performed before rt-PA is given, as PT/INR in
patients under vitamin K antagonist.4 Our case empha-
sizes the need for sensitive bed-site tests during emergen-
cies. Recent guidelines recommend that intravenous
thrombolysis in rivaroxaban-treated patients may be
considered if the plasma concentration of rivaroxaban is
less than 100ng/L5 or if anti–factor Xa activity is normal.1,5
Further studies on thrombolysis in patients taking
rivaroxaban are necessary, attempting to establish precise
thresholds of anti–factor Xa activity under which it
would be safe, as with patients anticoagulated by
vitamin K antagonist, its use is contraindicated for those
with an INR of 1.7 or more. Antagonists for new oral
anticoagulant drugs are under development, and it is
possible that these antagonists may not induce a
procoagulant response. Thrombolysis would therefore be
possible.
References
1. Jaunch EC, Saver JL, Adams HP, et al. Guidelines for theearly management of patients with acute ischemic stroke:a guideline for health professionals from the AmericanHeart Association/American Stroke Association. Stroke2013;44:870-947.
2. Fluri F, Heinen F, Kleinschnitz C. Intravenous thromboly-sis in a stroke patient receiving rivaroxaban. CerebrovasDis Extra 2013;3:153-155.
3. Van Hooff R-J, Nieboer K, De Smedt A, et al. Intravenousthrombolysis with recombinant tissue plasminogen acti-vator for acute ischemic stroke in a patient treated with ri-varoxaban. Clin Neurol Neurosurg 2014;122:131-132.
4. Samama MM, Constant G, Spiro TE, et al. Laboratoryassessment of rivaroxaban: a review. Thromb J 2013;11:11.
5. Steiner T, B€ohm M, Dichgans M, et al. Recommendationsfor the emergency management of complications associ-ated with the new direct oral anticoagulants (DOACs),apixaban, dabigatran and rivaroxaban. Clin Res Cardiol2013;102:399-412.