Intravascular Ultrasound to Assess Extracranial Vertebral Artery Restenosis: Case Report
4
Intravascular Ultrasound to Assess Extracranial Vertebral Artery Restenosis: Case Report Rishi Gupta, MD, Archit Bhatt, MD, Mounzer Kassab, MD, Arshad Majid, MD From the Department of Neurology, Michigan State University, East Lansing, MI Keywords: Vertebral artery stenosis, stent, angioplasty, intravascular ultra- sound. Acceptance: Received August 23, 2007, and in revised form August 23, 2007. Accepted for publication October 22, 2007. Correspondence: Address correspon- dence to Rishi Gupta, MD, Department of Neurology, Michigan State University, 138 Service Road, A-217, East Lansing, MI 48824. E-mail: [email protected] J Neuroimaging 2008;18:336-339. DOI: 10.1111/j.1552-6569.2007.00220.x ABSTRACT We present a case report of a patient who developed restenosis 5 months after initial stent placement. computed tomography (CT) angiography revealed a 70% stenosis, while conventional angiography revealed a 40% stenosis. An intravascular ultrasound (IVUS) was used to assess the degree of narrowing along with the mechanism causing the stenosis. IVUS can be utilized to resolve discrepancies between imaging modalities for degree of stenosis and also aid in determining the mechanism of restenosis after stent placement in the extracranial vertebral arteries. Intravascular ultrasound (IVUS) has become an accepted tech- nique in assessing adequacy of stent placement and mecha- nism of stent restenosis in the coronary arteries. 1 IVUS has allowed clinicians to determine the plaque morphology and also to better understand the effect of arterial remodeling. 2 Post- stent placement restenosis has been thought to be due to intimal hyperplasia (IH) particularly at the distal stent margins. 3 Un- derstanding the mechanism is important in order to decide the treatment modality. We describe a patient who underwent stenting and angio- plasty of a symptomatic extracranial left vertebral artery os- tium stenosis who returned with a restenosis at the distal stent margin. IVUS was utilized to determine the mechanism of restenosis and the patient was treated successfully with a second stent. Case Presentation An 81-year-old woman with a history of hypertension and hy- perlipidemia presented with complaints of ataxia, dysarthria, and diplopia. She underwent an MRI study of the brain that re- vealed the presence of acute embolic infarcts in the cerebellum. A CT angiogram (CTA) revealed a right vertebral artery that was atretic, a high-grade stenosis of the extracranial left verte- bral artery and an absence of posterior communicating arteries. The patient was on aspirin therapy prior to this event and thus was counseled on stenting and angioplasty of the left vertebral artery lesion. Procedure The patient was given a load of clopidogrel 300 mg 24 hours prior to the procedure and maintained on aspirin 325 mg a day. A 5 French catheter was utilized to perform angiography of the left subclavian artery, which confirmed the presence of a calcified plaque at the ostium of the left vertebral artery (Fig 1A). Intravenous heparin was given as a bolus to maintain an activated clotting time (ACT) of greater than 250 seconds. After placement of a 6 French guide catheter in the left subclavian artery, a .014-inch microwire was used to traverse the lesion. A 4.5 × 20 mm Libert ´ e stent (Boston Scientific Corp. Natick, MA, USA) was navigated across the lesion and deployed at nominal pressure. Poststent placement angiographic imaging (Fig 1B) revealed patency of the stent and the patient was discharged home on aspirin and clopidogrel therapy for 6 months. The patient returned at 5 months with one short episode of diplopia that resolved after 1 hour. A repeat 64-channel CTA was performed that revealed a 66% stenosis distal to the stent (Fig 2). The patient was then brought to angiography for con- sideration of revascularization. A 6 French guide catheter was placed in the left subclavian artery and angiography was performed revealing a 40% stenosis distal to the stent with mild in stent restenosis (Fig 3). A 0.014- inch microwire was used to traverse the narrowing distal to the stent after a bolus of intravenous heparin was given to maintain an ACT of greater than 250 seconds. A 3 French Atlantis SR 40 MHz IVUS catheter (Boston Scientific Corp.) was placed over the microwire just distal to the stenosis. A pullback was performed at .5 mm/second over the narrowed segment and through the portion covered with the stent. The cross-sectional area (CSA) of the lumen just distal to the stent was 5.7 mm 2 and the CSA of the vessel was 19.1 mm 2 (Fig 4A). This corresponded to a 70% narrowing due to plaque formation. Through the stent there was minimal stenosis noted consistent with IH (Fig 4B). Thus a 5.0 × 12 mm Libert ´ e stent (Boston Scientific Corp. ) was successfully deployed at nominal pressure across the stenotic segment (Fig 5). The IVUS catheter was placed again across the newly stented segment and this confirmed that the lesion had been reduced with a minimal residual narrowing. The patient 336 Copyright ◦ C 2008 by the American Society of Neuroimaging
-
Upload
rishi-gupta -
Category
Documents
-
view
214 -
download
2
Transcript of Intravascular Ultrasound to Assess Extracranial Vertebral Artery Restenosis: Case Report

Intravascular Ultrasound to Assess Extracranial Vertebral ArteryRestenosis: Case Report
Rishi Gupta, MD, Archit Bhatt, MD, Mounzer Kassab, MD, Arshad Majid, MDFrom the Department of Neurology, Michigan State University, East Lansing, MI
Keywords: Vertebral artery stenosis,stent, angioplasty, intravascular ultra-sound.
Acceptance: Received August 23,2007, and in revised form August 23,2007. Accepted for publication October22, 2007.
Correspondence: Address correspon-dence to Rishi Gupta, MD, Department ofNeurology, Michigan State University, 138Service Road, A-217, East Lansing, MI48824. E-mail: [email protected]
J Neuroimaging 2008;18:336-339.DOI: 10.1111/j.1552-6569.2007.00220.x
A B S T R A C TWe present a case report of a patient who developed restenosis 5 months after initialstent placement. computed tomography (CT) angiography revealed a 70% stenosis, whileconventional angiography revealed a 40% stenosis. An intravascular ultrasound (IVUS)was used to assess the degree of narrowing along with the mechanism causing the stenosis.IVUS can be utilized to resolve discrepancies between imaging modalities for degree ofstenosis and also aid in determining the mechanism of restenosis after stent placementin the extracranial vertebral arteries.
Intravascular ultrasound (IVUS) has become an accepted tech-nique in assessing adequacy of stent placement and mecha-nism of stent restenosis in the coronary arteries.1 IVUS hasallowed clinicians to determine the plaque morphology andalso to better understand the effect of arterial remodeling.2 Post-stent placement restenosis has been thought to be due to intimalhyperplasia (IH) particularly at the distal stent margins.3 Un-derstanding the mechanism is important in order to decide thetreatment modality.
We describe a patient who underwent stenting and angio-plasty of a symptomatic extracranial left vertebral artery os-tium stenosis who returned with a restenosis at the distal stentmargin. IVUS was utilized to determine the mechanism ofrestenosis and the patient was treated successfully with a secondstent.
Case PresentationAn 81-year-old woman with a history of hypertension and hy-perlipidemia presented with complaints of ataxia, dysarthria,and diplopia. She underwent an MRI study of the brain that re-vealed the presence of acute embolic infarcts in the cerebellum.A CT angiogram (CTA) revealed a right vertebral artery thatwas atretic, a high-grade stenosis of the extracranial left verte-bral artery and an absence of posterior communicating arteries.The patient was on aspirin therapy prior to this event and thuswas counseled on stenting and angioplasty of the left vertebralartery lesion.
ProcedureThe patient was given a load of clopidogrel 300 mg 24 hoursprior to the procedure and maintained on aspirin 325 mg aday. A 5 French catheter was utilized to perform angiographyof the left subclavian artery, which confirmed the presence of
a calcified plaque at the ostium of the left vertebral artery (Fig1A). Intravenous heparin was given as a bolus to maintain anactivated clotting time (ACT) of greater than 250 seconds. Afterplacement of a 6 French guide catheter in the left subclavianartery, a .014-inch microwire was used to traverse the lesion. A4.5 × 20 mm Liberte stent (Boston Scientific Corp. Natick, MA,USA) was navigated across the lesion and deployed at nominalpressure. Poststent placement angiographic imaging (Fig 1B)revealed patency of the stent and the patient was dischargedhome on aspirin and clopidogrel therapy for 6 months.
The patient returned at 5 months with one short episode ofdiplopia that resolved after 1 hour. A repeat 64-channel CTAwas performed that revealed a 66% stenosis distal to the stent(Fig 2). The patient was then brought to angiography for con-sideration of revascularization.
A 6 French guide catheter was placed in the left subclavianartery and angiography was performed revealing a 40% stenosisdistal to the stent with mild in stent restenosis (Fig 3). A 0.014-inch microwire was used to traverse the narrowing distal to thestent after a bolus of intravenous heparin was given to maintainan ACT of greater than 250 seconds. A 3 French Atlantis SR40 MHz IVUS catheter (Boston Scientific Corp.) was placedover the microwire just distal to the stenosis. A pullback wasperformed at .5 mm/second over the narrowed segment andthrough the portion covered with the stent. The cross-sectionalarea (CSA) of the lumen just distal to the stent was 5.7 mm2 andthe CSA of the vessel was 19.1 mm2 (Fig 4A). This correspondedto a 70% narrowing due to plaque formation. Through the stentthere was minimal stenosis noted consistent with IH (Fig 4B).Thus a 5.0 × 12 mm Liberte stent (Boston Scientific Corp. ) wassuccessfully deployed at nominal pressure across the stenoticsegment (Fig 5). The IVUS catheter was placed again across thenewly stented segment and this confirmed that the lesion hadbeen reduced with a minimal residual narrowing. The patient
336 Copyright ◦C 2008 by the American Society of Neuroimaging
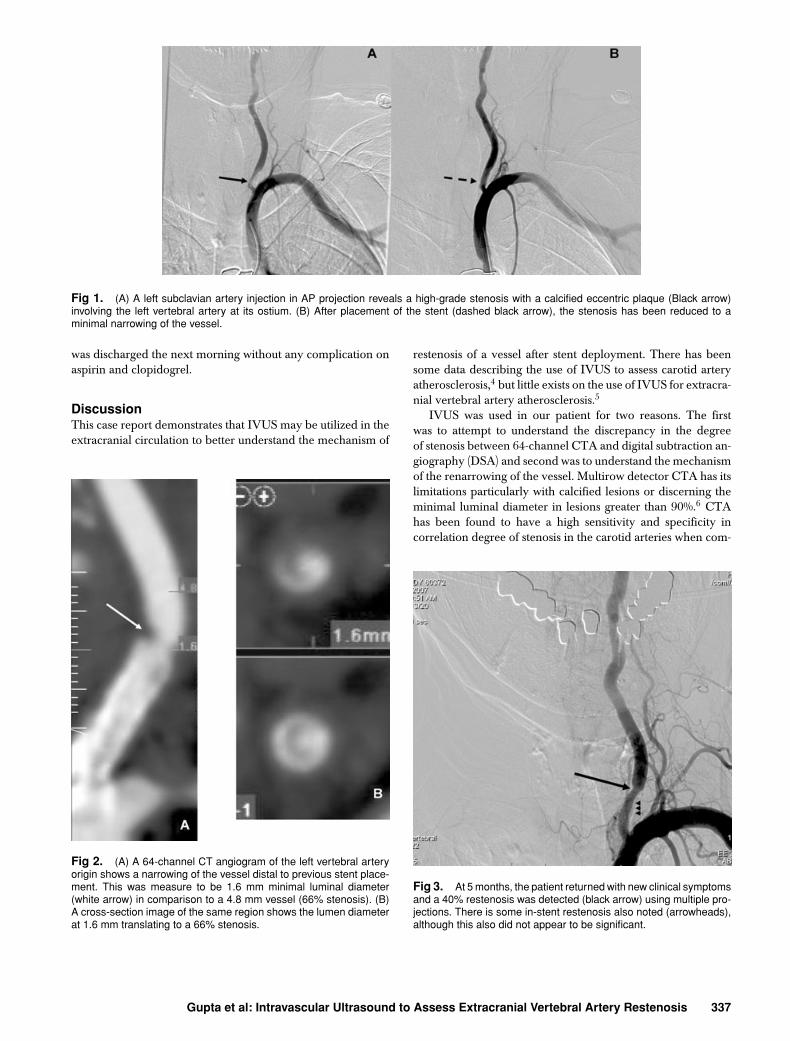
Fig 1. (A) A left subclavian artery injection in AP projection reveals a high-grade stenosis with a calcified eccentric plaque (Black arrow)involving the left vertebral artery at its ostium. (B) After placement of the stent (dashed black arrow), the stenosis has been reduced to aminimal narrowing of the vessel.
was discharged the next morning without any complication onaspirin and clopidogrel.
DiscussionThis case report demonstrates that IVUS may be utilized in theextracranial circulation to better understand the mechanism of
Fig 2. (A) A 64-channel CT angiogram of the left vertebral arteryorigin shows a narrowing of the vessel distal to previous stent place-ment. This was measure to be 1.6 mm minimal luminal diameter(white arrow) in comparison to a 4.8 mm vessel (66% stenosis). (B)A cross-section image of the same region shows the lumen diameterat 1.6 mm translating to a 66% stenosis.
restenosis of a vessel after stent deployment. There has beensome data describing the use of IVUS to assess carotid arteryatherosclerosis,4 but little exists on the use of IVUS for extracra-nial vertebral artery atherosclerosis.5
IVUS was used in our patient for two reasons. The firstwas to attempt to understand the discrepancy in the degreeof stenosis between 64-channel CTA and digital subtraction an-giography (DSA) and second was to understand the mechanismof the renarrowing of the vessel. Multirow detector CTA has itslimitations particularly with calcified lesions or discerning theminimal luminal diameter in lesions greater than 90%.6 CTAhas been found to have a high sensitivity and specificity incorrelation degree of stenosis in the carotid arteries when com-
Fig 3. At 5 months, the patient returned with new clinical symptomsand a 40% restenosis was detected (black arrow) using multiple pro-jections. There is some in-stent restenosis also noted (arrowheads),although this also did not appear to be significant.
Gupta et al: Intravascular Ultrasound to Assess Extracranial Vertebral Artery Restenosis 337

Fig 4. An IVUS catheter was placed across the stenosis. (A) At the distal stent margin was a 70% stenosis consistent with an atheroscleroticplaque (heterogenous echoic signals). The dotted white region is the cross-sectional area of the vessel (19.1 mm2) while the solid whitearrow is the cross-sectional area of the lumen (5.7 mm2). (B) IVUS through the stent (solid white arrows) confirmed there was minimal intimalhyperplasia (dashed white arrow) surrounding the stent. This was not a significant stenosis.
pared with DSA.6 When discrepancy occurs between the twoimaging modalities, IVUS may help to resolve the difference.IVUS is more sensitive in detecting atherosclerosis in coronaryvessels when compared with angiography.7
IVUS has distinct advantages over angiography in detectingthe circumferential appearance of the vessel wall allowing forplaque characterization. Hypoechoic signals are typically seenwith soft plaque, while hyperechoic signals are noted with calci-fied lesions. IH tends to have a mixed signal characteristic dueto fibrous scar tissue.8 On angiography, the sizing of the ves-sel may be inaccurate due to magnification and calibration ofequipment utilized, thus IVUS may be a more accurate methodof delineating the luminal diameter of a vessel. The last advan-
Fig 5. After placement of a stent across the stenosis, there isresolution of the narrowed segment.
tage of IVUS is that it may aid in assessing the wall apposition ofthe stent. Poor apposition of the stent may be linked with higherrates of restenosis and acute thrombosis in the coronary liter-ature9 and may be of a particular concern in the extra-cranialvertebral artery where restenosis rates are high.
Recent evidence through IVUS suggests that there may beseveral factors leading to lumen loss after a stent placement ina coronary vessel including: IH, "negative remodeling" (con-traction of the external elastic membrane) or redistribution ofplaque material after stent placement.1,2,3 Identifying the mech-anism of restenosis is important as the treatment for IH is bal-loon angioplasty while recurrence of plaque can be treated withstent deployment. Additionally, the distal edges of the stent arefelt to be regions where IH commonly occurs.3 In our patient,the distal margin of the stent accrued new plaque as opposedto IH.
Restenosis can occur as high as 42% of the time in theextracranial vertebral artery after stent placement,10 althoughsome authors have reported rates as low as 7% with the useof drug eluting stents.11 Small reference vessel diameter andlonger lesions12 have been linked to restenosis, but the mech-anism has not been rigorously studied and been presumed tobe linked to IH. IVUS may help in future study of restenosis ofthese vessels.
Although IVUS may help in certain instances in ascertainingthe degree of stenosis, it is limited in that passing the catheterthrough a high-grade stenosis may be technically difficult andcause vessel injury or dissection. The catheter in its currentform cannot be navigated easily into the intracranial circula-tion and thus it precludes safe assessment of all cerebral lesions.Artifacts are noted particularly if the device is not in the per-pendicular plane to the lesion and thus experience is requiredto assess lesions. Despite these limitations, in extracranial verte-bral artery lesions that are relatively straight segments it may beof added value to assess stent wall apposition and better delin-eate the degree of stenosis if there is a discrepancy in diagnostictesting.
In conclusion, we describe a patient who underwent suc-cessful placement of a stent in the extracranial vertebral artery
338 Journal of Neuroimaging Vol 18 No 3 July 2008

for a restenosis after confirming this was plaque reaccumula-tion through the use of IVUS. Future studies are required todetermine the safety of IVUS for assessing extracranial stenoticlesions.
References1. Bose D, von Birgelen C, Erbel R. Intravascular ultrasound for the
evaluation of therapies targeting coronary atherosclerosis. J Am CollCardiol 2007;49:925-932.
2. Mintz GS, Popma JJ, Pichard AD, Kent KM, Satler LF, Wong C,Hong MK, Kovach JA, Leon MB. Arterial remodeling after coro-nary angioplasty. A serial intravascular ultrasound study. Circulation1996;94:35-43.
3. Weissman NJ, Wilensky RL, Tanguay JF, Bartorelli AL, Moses J,Wllliams DO, Bailey S, Martin JL, Canos MR, Rudra H, PopmaJL, Leon MB, Kaplan AV, Mintz GS. Extent and distribution ofin-stent intimal hyperplasia and edge effect in non-radiation stentpopulation. Am J Cardiol 2001;88:248-252.
4. Clark DJ, Lessio S, O’Donoghue M, Tsalamandris C, SchainfeldR, Rosenfield K. Mechanisms and predictors of carotid artery stentrestenosis: a serial intravascular ultrasound study. J Am Coll Cardiol2006;47:2390-2396.
5. Hayashi K, Kitagawa N, Morikawa M, Kaminogo M. A caseof intimal hyperplasia induced by stenting for vertebral arteryorigin stenosis: assessed on intravascular ultrasound. Neurol Res2003;25:357-360.
6. Berg M, Zhang Z, Ikonen A, Sipola P, Kalviainen R, Manninen H,Vanninen R. Multidetector row CT angiography in the assessment
of carotid artery disease in symptomatic patients: comparison withrotational angiography and digital subtraction angiography. AJNRAm J Neuroradiol 2005;26:1022-1034.
7. Tobis JM, Mallery J, Mahon D, Lehmann K, Zalesky P, GriffithJ, Gessert J, Moriuchi M, McRae M, Dwyer ML. Intravascularultrasound imaging of human coronary arteries in vivo. Analysisof tissue characterizations with comparison to in vitro histologicalspecimens. Circulation 1991;83:913-926.
8. Potkin BN, Bartorelli AL, Gessert JM, Neville RF, Almagor Y,Roberts WC, Leon MB. Coronary artery imaging with intravascularhigh-frequency ultrasound. Circulation 1990;81:1575-1585.
9. Fitzgerald PJ, Oshima A, Hayase M, Metz JA, Bailey SR, BaimDS, Cleman MW, Deutsch E, Diver DJ, Leon MB, Moses JW,Oesterle SN, Overlie PA, Pepine CJ, Safian RD, Shani J, SimontonCA, Smalling RW, Teirstein PS, Zidar JP, Yeung AC, Kuntz RE,Yock PG. Final results of the can routine ultrasound influence stentexpansion (CRUISE) study. Circulation 2000;102:523-530.
10. SSYLVIA Study Investigators. Stenting of symptomatic atheroscle-rotic lesions in the vertebral or intracranial arteries (SSYLVIA):study results. Stroke 2004;35:1388-1392.
11. Gupta R, Al-Ali F, Thomas AJ, Horowitz MB, Barrow T, VoraNA, Uchino K, Hammer MD, Wechsler LR, Jovin TG. Safety,feasibility and short-term follow up of drug eluting stent placementin the intracranial and extracranial circulation. Stroke 2006;37:2562-2566.
12. Lin YH, Liu YC, Tseng WY, Juang JM, Hung CS, Lin JW, JengJS, Yip PK, Kao HL. The impact of lesion length on angiographicrestenosis after vertebral artery origin stenting. Eur J Vasc EndovascSurg 2006;32:379-385.
Gupta et al: Intravascular Ultrasound to Assess Extracranial Vertebral Artery Restenosis 339