
Intranasal drug delivery Intranasal drug delivery is now recognized to be a useful and reliable...
28
Intranasal drug delivery Intranasal drug delivery is now recognized to be a useful and reliable alternative to oral and parenteral routes. Undoubtedly, the intranasal administration of medicines for the symptomatic relief and prevention or treatment of topical nasal conditions has been widely used for a long period of time. However, recently, the nasal mucosa has seriously emerged as a therapeutically viable route for the systemic drug delivery. In general, among the primary targets for intranasal administration are pharmacologically active compounds with poor stability in gastrointestinal fluids, poor intestinal absorption and/or extensive hepatic first-pass elimination, such as peptides, proteins and polar drugs.
-
Upload
michael-knight -
Category
Documents
-
view
249 -
download
4
Transcript of Intranasal drug delivery Intranasal drug delivery is now recognized to be a useful and reliable...

Intranasal drug delivery
Intranasal drug delivery is now recognized to be a useful and reliable alternative to oral and parenteral routes. Undoubtedly, the intranasal administration of medicines for the symptomatic relief and prevention or treatment of topical nasal conditions has been widely used for a long period of time. However, recently, the nasal mucosa has seriously emerged as a therapeutically viable route for the systemic drug delivery. In general, among the primary targets for intranasal administration are pharmacologically active compounds with poor stability in gastrointestinal fluids, poor intestinal absorption and/or extensive hepatic first-pass elimination, such as peptides, proteins and polar drugs.

Nasal Cavity: Anatomy
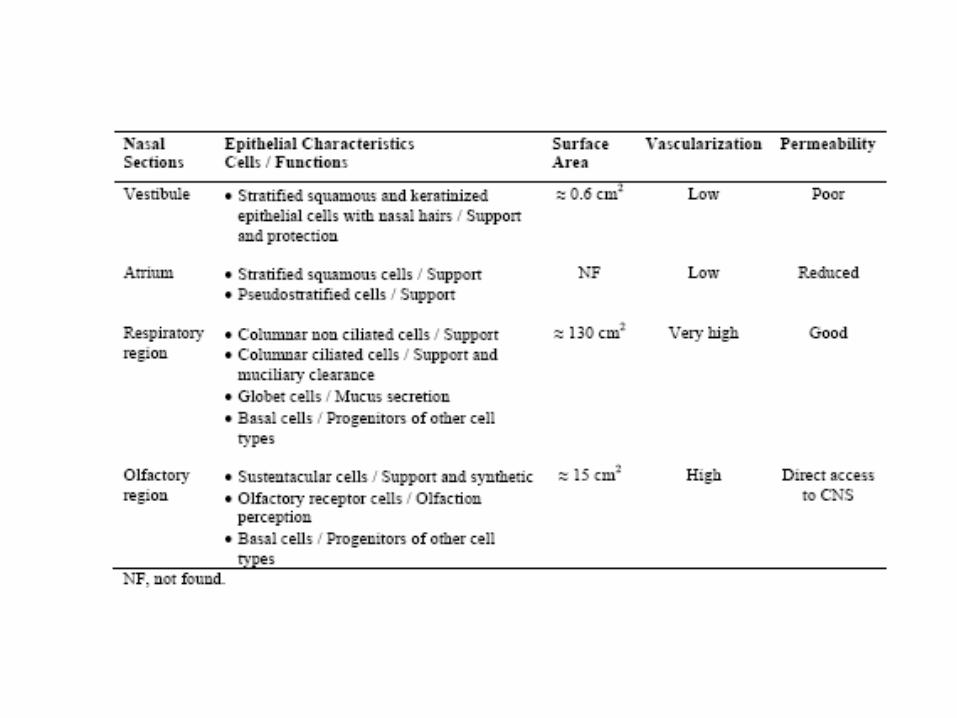
It is divided by middle (ornasal) septum into twosymmetrical halves, eachone opening at the facethrough nostrils andextending posterior to thenasopharynx. Bothsymmetrical halves consistof four areas (nasalvestibule, atrium, respiratoryregion and olfactory region)that are distinguished accordingto their anatomic and histologicalcharacteristics

Nasal vestibule:Nasal vestibule is the most anterior part of the nasal cavity,just inside the nostrils, and presents an area about 0.6cm2. Here, there are nasal hairs, which filter the inhaledparticles. Histologically, this nasal portion is covered by astratified squamous and keratinized epithelium withsebaceous glands. These nasal vestibular characteristicsare desirable to afford high resistance against toxicenvironmental substances but, at the same time, theabsorption of substances including drugs becomes verydifficult in this region
Atrium: is the intermediate area between nasal vestibule and respiratory region. Its anterior section is constituted by a stratified squamous epithelium and the posterior area by pseudostratified columnar cells presenting microvilli

The nasal respiratory region: is the largest part of theNasal cavity and it is divided in superior, middle and inferiorturbinates which are projected from the lateral wall.Turbinate bone refers to any of the scrolled spongy bonesof the nasal passages. These specialized structures areresponsible For humidification and temperature regulationof inhaled air. Between them there are spaces, calledmeatus, which are passageways where airflow is created toassure a close contact of the inhaled air with the respiratorymucosal surface. The nasal respiratory mucosa,considered the most important section for delivering drugssystemically, is constituted by the epithelium, basementmembrane and lamina propria (mucosa). The basementmembrane is a thin sheet of fibers that underlies theepithelium

Many of the epithelial cells are covered on their apical surface with microvilli and the major part of them also has fine projections, called cilia. Actually, microvilli are important to enhance the respiratory surface area, while cilia are essential to transport the mucus toward the nasopharynx. Under physiological conditions, nasal epithelium is covered with a thin mucus layer produced by secretory glands (globet cells). These ones secrete granules filled with mucin, a glycoprotein that determines the viscosity of the mucus. The nasal mucus layer is only 5 μm thick and it is organized in two distinct layers: an external, viscous and dense, and aninternal, fluid and serous. Overall, nasal mucus layer consists of 95% of water, 2.5-3% of mucin, and 2% of electrolytes, proteins, lipids, enzymes, antibodies, sloughed epithelial cells and bacterial products. Nasal mucus is indispensablefor several physiological functions, such as humidification and warming of the inhaled air, and also offers physical and enzymatic protection. The presence of mucin in the nasal mucus layer is crucial because it may trap large molecular weight drugs, such as peptide and proteins

The olfactory region is located in the roof of the nasal cavity and extends a short way down the septum and lateral wall. Its neuroepitheliumis the only part of the CNS that is directly exposed to the external environment. Similarly to the respiratory epithelium, the olfactory one is also pseudostratified but contains specialized olfactory
receptor cells important for smell perception .
The olfactory mucosa (smelling area in nose) is in direct contact with the brain and CSF. Medications absorbed across the olfactory mucosa directly enter the CSF.
This area is termed the nose brain pathway and offers a rapid, direct route for drug delivery to the brain.

ADVANTAGES OF NASAL DRUG DELIVERY SYSTEMS
1) Easy accessibility and needle free drug application without the necessity of trained personnel facilitates self medication, thus improving patient compliances compared to parenteral routes.
2) Good penetration of, especially lipophilic, low molecular weight drugs through the nasal mucosa. For instance the absolute nasal bioavailability of fentanyl is about 80%
3) Rapid absorption and fast onset of action due to relatively large absorption surface and high vascularization. Thus the Tmax of fentanyl after nasal administration was less than or equal to 7 minute comparable to intravenous. Nasal
administration of suitable drug would therefore be effective in emergency therapy as an alternative to parenteral administration routes.

4) Potential for direct delivery of drug to the central nervous system via the olfactory region, thus by-passing the blood brain barrier.
5) Avoidance of the harsh environmental conditions in the gastrointestinal tract (chemical and enzymatic degradation of drugs).
6) Avoidance of hepatic first pass metabolism and thus potential for dose reduction compared to oral delivery.

BARRIERS FOR NASAL DRUG DELIVERY
(i) Low bioavailability-Bioavailability of polar drugs is generally low, about 10% for low molecular weight drugs and not above 1% for peptides such as calcitonin and insulin The most important factor limiting the nasal absorption of polar drugs and especially large molecular weight polar drugs such as peptides and proteins is the low membrane permeability.
(ii) Mucociliary clearance- The general fast clearance of
the administered formulation from the nasal cavity due to the mucociliary clearance mechanism is another factor of importance for low membrane transport. This is especially the case when the drug is not absorbed rapidly enough across the nasal mucosa.

iii) Enzymatic Degradation-Another contributing, butoften less considered factor to the low bioavailability of peptides and proteins across the nasal mucosa is the possibility of an enzymatic degradation of the molecule in the lumen of the nasal cavity or during passage through the epithelial barrier. These sites both contain exopeptidases such as mono and diaminopeptidases that can cleave peptides at their N and C termini and endopeptidases, which can attack internal peptide bonds.
IV) P glycoprotein efflux: Drug absorption may be hindered by efflux transporters such as P-glycoproteins (Pgps). Basically, Pgps are a group of glycosylated membrane proteins found in the epithelial cells of small intestine and other body tissues. A large variety of hydrophilic and amphiphilic compounds are detoxified through active Pgp mediated efflux transport in nasal mucosa.

MECHANISM OF DRUG ABSORPTION
• The first step in the absorption of drug from the nasalcavity is passage through the mucus. Small, unchargedparticles easily pass through this layer. However, large orcharged particles may find it more difficult to cross. Mucin,the principle protein in the mucus, has the potential to bindto solutes, hindering diffusion.
• Subsequent to a drug’s passage through the mucus, there are several mechanisms for absorption through the mucosa
-The first mechanism involves an aqueous route of transport, which is also known as the paracellular route. This route is slow and passive. There is an inverse log-log correlation between intranasal absorption and the molecular weight of water-soluble compounds. Poor bioavailability was observed for drugs with a molecular weight greater than 1000 Daltons

- The second mechanism involves transport through a lipoidal route that is also known as the transcellular process and is responsible for the transport of lipophilic drugs that show a rate dependency on their lipophilicity.
-Drugs also cross cell membranes by an active transport route via carrier-mediated means or transport through the opening of tight junctions. Larger peptides and proteins are able to pass the nasal membrane using an endocytotic transport process but only in low amounts
Although tight junctions are dynamic structures and can open and close to a certain degree when needed, the mean size of these channels is of the order of less than 10 Å and the transport of larger molecules is considerably more limited

FACTORS INFLUENCING NASAL DRUG ABSORPTION
A) Factors Related to Drug
a) Lipophilicity: On
Increasing lipophilicity, the
permeation of the compound
normally increases through
nasal mucosa. Although the nasal
mucosa was found to have some
hydrophilic character, it appears that
these mucosae are primarily
lipophilic in nature and the
lipid domain plays an important
role in the barrier function of these
membranes
•.
Blood stream
Lipophilic molecules

Lipophilic compounds tend to readily cross biological membranes via the transcellular route since they are able to partition into the lipid (bilayer) of the cell membrane and diffuse into and traverse the cell in the cell cytoplasm.
b) Chemical Form: The chemical form of a drug can be important in determining absorption. For example, conversion of the drug into a salt or ester form can alter its absorption. It was also observed that in-situ nasal absorption of carboxylic acid esters of L-Tyrosine was significantly greater than that of L-Tyrosine.
C) Drug solubility and dissolution rate: Solubility of the drug or dosage form is the first prerequisite for absorption and bioavailability of powder dosage form. Superior stability of solid powder dosage forms, controlled release mode and its ease of manufacturing may provide number of solid nasal dosage forms to the market in near future.
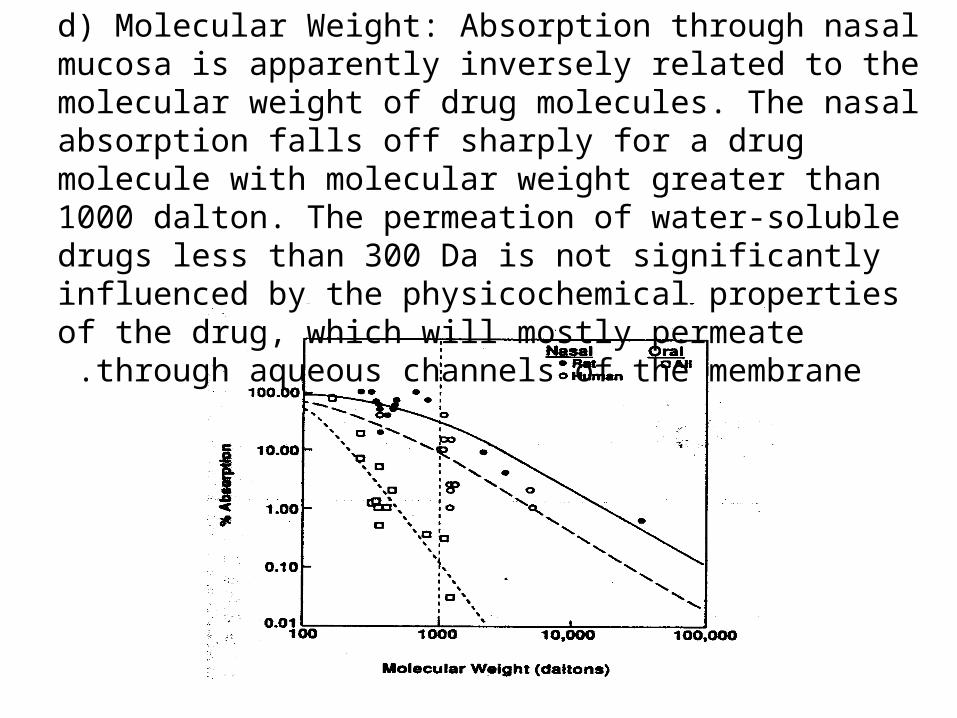
d) Molecular Weight: Absorption through nasal mucosa is apparently inversely related to the molecular weight of drug molecules. The nasal absorption falls off sharply for a drug molecule with molecular weight greater than 1000 dalton. The permeation of water-soluble drugs less than 300 Da is not significantly influenced by the physicochemical properties of the drug, which will mostly permeate through aqueous
channels of the membrane .

e) Partition Coefficient, pH and pKa: As per the pH partition theory, unionized species are absorbed better compared with ionized species and the same holds true in the case of nasal absorption. Nasal pH (4.5-6.5) is essential for physiological defense mechanism against microbial organisms. Lysozyme is present in nasal secretion, which is responsible for destroying certain microorganism at acidic pH. Lysozyme inactivation at alkaline condition leads to nasal infection and hence it affects the nasal mucociliary clearance and bioavailability of nasal formulations. The amount of drug that exists in unionized form in nasal cavity is a function of pka of the drug molecule and pH of nasal secretion. As nasal secretion pH is a fairly constant in healthy human subjects, pKa of drug molecule determines the degree of ionization and hence bioavailability of nasally administered drugs. Manipulation of micro environmental pH of nasal mucosa is not advisable, because acidic pH causes nasal irritation followed by increase in the nasal mucociliary clearance rate, whereas alkaline pH leads to the microbial susceptibility and infection.

B) Factors Related to Formulation
B1) Drug concentration, dose, and dose volume: No clear effect for drug concentration on nasal absorptionwas found. Nasal absorption of l-tyrosyl-L-tyrosine was found toincrease with increasing concentration of the drug. Theabsorption of aminopyrine from rat nasal mucosa wasconstant as a function of its concentration. Interestingly, nasalabsorption of salicylic acid was decreased with increasingconcentration of administered drug. Low absorption of highconcentration of salicylic acid was lined with its nasalepithelial toxicity and nasal membrane resistance. if the drug undergoespassive diffusion, it should obey linear relationship between drugconcentration and absorption. But this is not true because variousfactors such as quantity and nature of mucus, mucociliary clearance,and membrane resistance.

Nasal cavity has capacity to retain limited volume of the administered dose, beyond which formulation will drain out of the nasal cavity. The ideal dosage form for better absorption should possess dose volume around 25 µl - 150 µl. The maximum dose is soluble in minimum quantity of liquid dosage form (less than 200 µl) .
B2) Osmolarity of dosage form: profound influence of osmolarity on nasal drug absorption was found. High concentration of sodium chloride not only leads to higher bioavailability but also toxicity to nasal epithelial cells, because shrinkage of the nasal epithelial mucosa was observed at high salt concentration. The maintenance of isotonicity of the formulation will reduce the nasal epithelial cell damage and hence it will reduce the toxicity of the nasal formulation.

B3) Deposition site of dosage form: Nasal drops, traditionally used in formulations suffer from short nasal residential time. A higher viscosity of the formulation increases contact time between the drug and the nasal mucosa thereby increasing the time for permeation. At the same time, highly viscous formulations interfere with the normal functions like mucociliary clearance and thus alter the permeability of drugs. Nasal gel has poor spreading abilities due to its high viscosity and hence it shows narrow distribution area in nasal cavity. Low clearance rate of nasal powder dosage form has shown better patient compliance, especially in children if the taste and smell of dosage form is unacceptable. Furthermore, powder properties such as particle size and shape, density and flow characteristics and dosage form delivery devices have an influence on the distribution of drug in nose and hence it affects the absorption and bioavailability
Strategies to Improve Nasal Bioavailability
Nasal permeation enhancers: Permeation enhancers have
been employed for improving the absorption of poorly
absorbed and large molecular weight compounds. Complete
mechanism of drug absorption enhancement through nasal
mucosa is not known. However, various mechanisms such as
increase in the membrane fluidity, creating transient
hydrophilic pores, decreasing the viscosity of mucous layer
and opening up of tight junctions are the proposed
mechanisms of permeation enhancers, which improve the
bioavailability of nasal dosage forms.

The ideal characteristics of nasal permeation enhancers are as follows:
1. It should be pharmacologically inert.
2. It should be non-allergic, non-toxic, and non-irritating.
3. It should be highly potent.
4. It should be compatible with a wide variety of drugs and excipients.
5. It should be odorless, tasteless, and colorless.
6. It should be inexpensive and readily available in highest purity.
7. It should be accepted by many regulatory agencies all around the world.

Surfactants are the most effective permeation enhancers, but the issues like nasal irritation, epithelial toxicity, and ciliostatic activity are the barriers for usage of surfactant as a nasal permeation enhancer. The extent of nasal absorption of insulin from nebulizer spray was observed to be pH dependent indicating maximum absorption at acidic pH. However, nasal absorption of insulin with surfactants like saponins, and glycolate was significantly increased even at acidic pH, which correlated with hypoglycemic effect. Comparative pharmacokinetics of intranasal delivery of salmon calcitonin was studied with various surfactants. A 10-fold increase in serum calcitonin levels over the control group (calcitonin without surfactant) was observed in formulations incorporated with surfactants.
Surfactants

Enzyme inhibitors:
A number of studies have described the role of enzyme inhibitors on bioavailability of nasal formulations. Mostly peptidase and protease inhibitors, such as bestatin, amastatin, boroleucin, borovaline, aprotinin, and trypsin inhibitors. are widely used to improve the bioavailability of protein and peptide molecules. The absorption enhancers such as bile salts exert enzyme inhibition and hence enhance the absorption and bioavailability.
Cyclodextrins :
Cyclodextrins are cyclic oligossacharidescomposed of glucose units joined trough α-1,4-glycosidic bonds resulted from bacterial digestion of cellulose. Structurally, they have a hydrophilic outer surface and a lipophilic central cavity where apolar drugs can be included. Cyclodextrins are used as complexing agents to improve nasal drug absorption by increasing drug solubility and stability. They can also work as absorption enhancers, since they interact with the lipophilic components of biological membranes changing their permeability.

Phospholipids (Liposomes): are surface active compounds, which are found in both animal cells as well as plant cells. Lysophosphatidylcholine is the most extensively studied phospholipid as a nasal permeation enhancer. Liposomes are phospholipids vesicles composed by lipid bilayers enclosing one or more aqueous compartments and wherein drugs and other substances can be included. Liposomal drug delivery systems present various advantages such as the effective encapsulation of small and large molecules with a wide range of hydrophilicity and pKa values. In fact, they have been found to enhance nasal absorption of peptides such as insulin and calcitonin by increasing their membrane penetration. This has been attributed to the increasing nasal retention of peptides, protection of the entrapped peptides from enzymatic degradation, and mucosal membrane disruption .
Although widely used in intranasal medicinal preparations, cyclodextrins present some local and systemic toxicity. Alterations of nasal morphology, ciliary beat frequency, erythrocyte haemolysis and citotoxic effects have also been reported. Amongst cyclodextrins, beta cyclodextrin is being considered to have a Generally Recognized As Safe (GRAS) status.

Bioadghesive polymers:
Chitosan is a linear polysaccharide consisting of b (1-4) linked D-glucosamine with randomly located N-acetylglucosamine groups depending upon the degree of deacetylation of the polymer. Chitosan is derived from chitin which is a fully acetylated polymer. Due to its biodegradability, biocompatibility and bioadhesive properties associated to a low toxicity, chitosan is widely used in intranasal formulations.
Strong cationic nature of chitosan promotes interaction with sialic acid present in mucosa and hence it opens the tight junction of nasal epithelial cells.
Chitosan is used in several intranasal pharmaceutical forms, including powders, liquids, gels, microparticles and microspheres.

Nanoparticles: are solid colloidal particles with diameters raging from 1-1000 nm. They consist of macromolecular materials and can be therapeutically used as adjuvant in vaccines or as drug carriers, in which the active substance is dissolved, entrapped, encapsulated, adsorbed or chemically attached. Nanoparticles may offer several advantages due to their small size, but only the smallest nanoparticles penetrate the mucosal membrane by paracellular route and in a limited quantity because of the tight junctions. Controversial results are found when using nanoparticles in intranasal drug delivery. In fact, there are few publications where in nanoparticle formulations did not significantly enhance the drug transport across the nasal cavity. The low bioavailability obtained can be due to the fact that particles are probably taken up by M-cells in the nasal associated lymphoid tissue and, therefore, transported into the lymphatic system.
Microspheres: Microsphere technology has been widely applied in designing formulations for nasal drug delivery. Microspheres are usually based on mucoadhesive polymers (chitosan, alginate), which present advantages for intranasal drug delivery. Furthermore, microspheres may also protect the drug from enzymatic metabolism and sustain drug
release, prolonging its effect .



















