International Mediterranean Universitymhcag.com/wp-content/uploads/2016/03/Dissertation_EN.pdf ·...
69
Thesis International Mediterranean University Martin Keymer Private Institute for Dermatology Dipl. hol. med. M. Keymer Thesis written under the supervision of private lecturer Dipl. hol. med. M. Keymer Atopic Dermatitis (Neurodermatitis) and Bioresonance Therapy. presented by Daniel Jakob from Trub BE (Switzerland) Approved at the request of Dr. László Villányi, Szent István University, Gödöllő, Hungary 2008 Thesis for the acquisition of a doctoral degree in Medicine from a higher medical faculty at the Szent István University
Transcript of International Mediterranean Universitymhcag.com/wp-content/uploads/2016/03/Dissertation_EN.pdf ·...
Thesis
International Mediterranean University
Martin Keymer Private Institute for Dermatology
Dipl. hol. med. M. Keymer
Thesis written under the supervision of private lecturer Dipl. hol. med. M. Keymer
Atopic Dermatitis (Neurodermatitis) and Bioresonance Therapy.
presented by Daniel Jakob
from Trub BE
(Switzerland)
Approved at the request of Dr. László Villányi, Szent István University, Gödöllő, Hungary 2008
Thesis
for the acquisition of a doctoral degree in
Medicine from a higher medical faculty
at the Szent István University

International Mediterranean University
College, Faculty of Bioenergetic Medicine, Malta
Thesis written under the supervision of private lecturer Dipl. hol. med. M. Keymer
Atopic Dermatitis (Neurodermatitis) and Bioresonance Therapy.
Thesis presented on 23 April 2004.
Read and approved by private lecturer Dipl. hol. med. M. Keymer Dozent of the I.M.U.
Authorised for publication on 25 April 2004
Table of Contents Page I
Table of Contents I Table of Contents ........................................................................................................................................................ I
II Table of Contents ...................................................................................................................................................... II
1 Introduction ............................................................................................................................3
2 Fundamentals ........................................................................................................................4
2.1 Diet ...................................................................................................................................................................... 4 2.2 Weakened Skin Defence Mechanisms ................................................................................................................ 5 2.3 Higher Tendency to Allergies .............................................................................................................................. 5 2.4 Worsening in connection with Psychological Stress ........................................................................................... 5 2.5 What Stages Does Atopic Eczema Go Through? ................................................................................................. 5 2.6 Symptoms ........................................................................................................................................................... 6 2.7 Changes of the Skin ............................................................................................................................................. 6 2.8 Unusual forms of atopic eczema: ....................................................................................................................... 7
3 Diagnostic Criteria Used in the Treatment Sessions .........................................................8
3.1 First-Order Diagnosis Criteria ............................................................................................................................. 8 3.2 Second-Order Diagnostic Criteria ....................................................................................................................... 8 3.3 Relevant Observations ........................................................................................................................................ 8
4 The Treatment of Atopic Eczema (Neurodermatitis) ........................................................ 10
4.1 External Treatment ........................................................................................................................................... 10 4.2 Internal Treatment ............................................................................................................................................ 10
5 Bioresonance Therapy ........................................................................................................ 11
5.1 Electromagnetic Oscillations ............................................................................................................................ 11 5.2 The Separator ................................................................................................................................................... 12 5.3 The Cybernetic Regulating Cycle Between Patient and Bicom Device .............................................................. 13 5.4 Pischinger's Ground Regulation System ........................................................................................................... 14 5.5 Endogenous and Exogenous Noxious Agents ................................................................................................... 15
6 The Application of the Cybernetic Regulating Cycle ....................................................... 16
6.1 Representation of the Cybernetic Regulating Cycle .......................................................................................... 17
7 Applied Test Procedure ...................................................................................................... 18
7.1 The Biotensor .................................................................................................................................................... 18 7.2 Test Materials Used .......................................................................................................................................... 18 7.3 Biophysical Resonance Testing Put to the Test ................................................................................................. 19 7.4 The Method of the Comparitive Study .............................................................................................................. 19
8 Therapy Methodology in the Study .................................................................................... 20
8.1 8.1 Therapeutic Procedure ................................................................................................................................ 20
9 Assessment of Laboratory Findings ................................................................................. 21
9.1. First Pathogen Detection in the First Patient Group from Blood and Stool ...................................................... 21 9.2. Second Pathogen Detection in the Second Patient Group from Blood and Stool ............................................. 21 9.3. Survey of Allergies in All 20 Patients ................................................................................................................. 22 9.4. Analysis of the 20 Stool Samples for Intestine Mycoses and Fermentative Dyspepsia .................................... 22 9.5. Testing of Chewing Gum or Blood Drops for Heavy Metals.............................................................................. 23

10 How Does Perinatal Transmission of Yeast Fungi Spores Occur? ................................. 24
10.1 Pathogens ......................................................................................................................................................... 24 10.2 Transmission of Yeasts ...................................................................................................................................... 25 10.3 Yeast Infection in Post-Partum Newborns ........................................................................................................ 25 10.4 Different Sites of Infection with Yeast Fungus .................................................................................................. 26
11 Discussion of Study Results .............................................................................................. 27
12 First Case Study .................................................................................................................. 28
12.1 Course of Treatment for Patient S. B. ............................................................................................................... 29 12.2.1 Scatology (Stool Culture) - Stool Laboratory Biochemical Screening ............................................................ 30 12.2.2 Frequency Specific Microcurrent Therapy for Intestinal Mycoses and Parasite Treatment ......................... 31 12.2.3 Fundamental Medical History (5 Elements) - Blood Laboratory Biochemical Screening .............................. 32 12.2.4 Follow-Up Medical History (Vaccines/Metals) - Blood Laboratory Biochemical Screening .......................... 33 12.2.5 Orthomolecular (Vitamins, Etc.) - Blood Laboratory Biochemical Screening................................................ 34 12.2.6 Repertorisation of Homoeopathic Medicines as Concomitant Therapy ....................................................... 35 12.2.7 Repertorisation of Homoeopathic Medicines as Concomitant Therapy ....................................................... 36 12.2.8 Repertorisation of Homoeopathic Medicines as Concomitant Therapy ....................................................... 37
13 Second Case Study ............................................................................................................. 38
13.1 Course of Treatment for Patient I. M. ............................................................................................................... 39 13.1 The Diagnosis of Coeliac Disease ...................................................................................................................... 40 13.2.1 Blood/Serum Analysis by the External Laboratory Viollier ........................................................................... 41 13.2.2 Scatology (Stool Culture) - Stool Laboratory Biochemical Screening ............................................................ 42 13.2.3 Foods/Luxury Foods - Blood Laboratory Biochemical Screening .................................................................. 43 13.2.4 Food Additives/Preservatives - Blood Laboratory Biochemical Screening .................................................... 44 13.2.5 Orthomolecular (Vitamins, Etc.) - Blood Laboratory Biochemical Screening................................................ 45 13.2.6 Investigation into Primary Causes - Blood Laboratory Biochemical Screening ............................................ 46 13.2.7 Viruses/Bacteria/Fungi/Animal Skin Cells - Blood Laboratory Biochemical Skin .......................................... 47 13.2.8 Fundamental Medical History (5 Elements) - Blood Laboratory Biochemical Screening .............................. 48 13.2.9 Follow-Up Medical History (Vaccines/Metals etc-) - Blood Laboratory Biochemical Screening ................... 49 13.2.10 Special Medical History (Degenerated Cells) - Blood Laboratory Biochemical Screening ........................ 50 13.2.11 Blood Laboratory Biochemical Screening ................................................................................................. 51 13.2.12 Blood Laboratory Biochemical Screening Follow-Up Medical History (1st Follow-Up) ............................ 52 13.2.13 Blood Laboratory Biochemical Screening Special Medical History (1st Follow-Up) ................................. 53 13.2.14 Blood Laboratory Biochemical Screening Fundamental Medical History (1st Follow-Up) ....................... 54 13.2.15 Blood Laboratory Biochemical Screening Follow-Up Medical History (2nd Follow-Up) ........................... 55 13.2.16 Blood Laboratory Biochemical Screening ................................................................................................. 56 13.2.17 Blood Laboratory Biochemical Screening ................................................................................................. 57 13.2.18 Blood Laboratory Screening with Biotensor ............................................................................................. 58 13.2.19 Blood Laboratory Biochemical Screening ................................................................................................. 59 13.2.20 Blood Laboratory Screening with Biotensor ............................................................................................. 60 13.3.21 Blood Laboratory Screening with Biotensor ............................................................................................. 61
14 Summary of Results ............................................................................................................ 62
14.1 The following treatment regimen has resulted from the study ........................................................................ 62 14.2 Treatment Results for All 20 Study Patients ..................................................................................................... 63
15 References ........................................................................................................................... 64
16 List of Tables ....................................................................................................................... 65
17 List of Figures ...................................................................................................................... 65
18 CURRICULUM VITAE ........................................................................................................... 66

Introduction Page 3
1 Introduction
The term "Neurodermatitis" comes from the words Neuron (neuron = nerve) and Dermatitis (inflammations of the skin; dermis = skin; -itis = inflammation). This term was coined at the end of the 19th century, when a connection between changes of the skin and an inflammation of the nerves was erroneously inferred. In modern dermatology, the expressions atopic dermatitis or atopic eczema are preferable.
Atopic eczema or neurodermatitis (atopic dermatitis, endogenous eczema) is a chronic skin condition which results mainly in dry skin, as well as a tendency to develop eczemas (inflammation of the epidermis) and itching.
The terms dermatitis and eczema refer generally to an inflammation of the skin, regardless of the underlying cause. The word "eczema" additionally emphasizes the long duration (chronicity) of the inflammatory changes of the skin. Since atopic eczema is largely attributable to a genetic predisposition, eczema flare-ups may occur without a recognizable external cause, e.g. a contact allergy. For this reason, the expressions endogenous eczema and atopic eczema are also used. Endogenous means originating from within (endo- = within; -gen = originating). "Atopic" actually means "out of place" (a- = un-, not; topos = place, region).
In order to obtain a clearer picture of this type of skin disease, of its progression, and of BICOM-Therapy treatment perspectives, a study was conducted with 20 patients aged between 6 months and 15 years of age, focusing on the "Therapeutic House" of the Private Institute for Dermatology run by private lecturer Dipl. hol. med. M. Keymer. Two patient categories were differentiated. Patients in the first category had been previously treated with a steroid (orally or applied as a cream); patients in the second category had had no contact with steroids. Some of the patients in the second category received an anti-allergy allopathic drug (Zyrtec).
As well as Bioresonance Therapy (BRT), a second type of instrumental therapy was conducted
in this study: Frequency Therapy (FT) as developed by Dr. Clark. It was adapted with the help of Mr. B. Schärer (electronics technician). The application of
frequencies occurred using a frequency generator constructed by the Hameg company.

Fundamentals
Page 4
Fundamentals: www. lifeline.de
2 Fundamentals
The disposition to develop atopic eczema is inherited and is often accompanied by increased susceptibility to hay fever and bronchial asthma. Atopic eczema, hay fever and bronchial asthma are thus also referred to as atopic disease. Despite heredity of an atopic disease, it is not actually a genetic disease. Only the disposition is inherited. Environmental factors such as diet, stress and psychological and emotional stresses influence the progression of the disease. There is a higher disposition to develop allergies and a weakened immune system reaction on the surface of the skin against bacteria and viruses.
2.1 Diet As mentioned above, diet can strongly influence the progression of atopy. For example, the skin may become irritated as a result of consumption of citrus fruits (oranges, lemons, kiwis, pineapple and others) or fruit juices. There is no underlying allergic reaction with release of histamine, a messenger substance, but rather a non-specific irritation of the skin due to unspecified substances contained in these foods. Spicy food, coffee, tea or alcohol may increase itching associated to atopic eczema due to increased blood circulation in the skin. There is no specific diet to follow, as long as there are no known allergies. In this case, it is not possible to avoid abstinence from the food in question (foods which cause allergy may not be eaten for a pre-defined period of time). In particular, if there are atopies and allergies, pork meat must be strictly avoided, because there is a strong affinity to human cells and the meat is highly toxic for a variety of reasons:
a) Excessive fat content also in the cell (normal only in the tissue) b) Very high cholesterol content (arteriosclerosis) c) Bad protein structure of the meat, therefore very high recovery rate. It rots very quickly and
thus strains the intestine, leading to a serious worsening of the intestine immune system, which accounts for about 70% of the overall immune system. Decomposition frees poisons, which are primarily found in the excretory organs, to which also the skin belongs. All this considering that the state of the skin is already very complex.
d) Meat also has strongly negative effects on the structure of connective tissue. It is strongly sulphurous, which brings increased water retention in the connective tissue with it. It swells like a sponge, which puts severe strain on collagen and elastic fibres and leads to faster skin ageing. It strongly dries out and fine cracks form. It can also lead to increased scaling and consequent strong itching. These are exactly the symptoms which are observed also in atopic eczema and neurodermatitis.
e) Pork meat contains a high histamine concentration, the highest occurring in slaughter animals. Histamine, as is well known, is a highly effective tissue hormone and is involved especially in the aggressive reactions of allergy sufferers. Consequently, pork meat promotes allergic processes, from hay fever and asthma to skin allergies and neurodermatitis. Histamine also participates in inflammatory processes, such as abscesses, boils, carbuncles, intestinal inflammations and vein inflammations. With each exposure to stress, histamine is released, exceeding a healthy level of stress and fosters the adverse occurrences linked to stress loads, such as neuroses, psychoses and depressions.

Fundamentals
Page 5
Fundamentals: www. lifeline.de
2.2 Weakened Skin Defence Mechanisms
There are some peculiarities to the way that the immune system functions in persons with atopic disposition. The reactions of the immune system which protect the skin from infections caused by pathogens develop in a weakened manner in persons with atopic disposition.
Furthermore, inflammatory changes of the skin, especially if they accompanied by oozing and followed by crusts forming, are an excellent breeding ground for bacteria. An increased density of bacteria on the skin surface brings with it a new inflammatory reaction with the consequence of increased itchiness. The risk of a second infection is present also for dry, scaly eczema patches due to the disruption of the stratum corneum. Scratching of the itchy eczema patch leads to skin injuries, which may be very small or even clearly visible as partly bloody "scratch marks". Such injuries further favour the penetration of bacteria in the skin and thus the inflammatory reaction of the eczema. Once this vicious circle has begun, it can under certain circumstances lead to an acute aggravation of the eczema.
2.3 Higher Tendency to Allergies
The increased readiness to react with an allergy upon contact with an actually harmful substance is in contrast to the immune deficiency on the skin surface (towards bacteria and viruses).
The term allergy - in contrast to a protective defensive reaction to pathogens - refers to a reaction of the immune system which causes sickness to a substance which is in itself harmless, such as cat hair, grass pollen or the metabolic products of dust mites. About 75% of all patients with atopic eczema show a positive reaction to different allergens in the skin test.
Even though people with atopic eczema have a higher tendency to certain allergies and allergic disorders such as hay fever or bronchial asthma, atopic eczema in itself is not an allergic disorder. Rather, it is contact with a substance to which a subject is allergic (e.g. grass pollen) that may under certain circumstances trigger an eczema flare-up.
2.4 Worsening in connection with Psychological Stress
Frequent observations of affected subjects show visible worsening of their skin condition in connection with family disputes and with stress at school or at work. It is not yet known exactly how the psyche is able to influence the appearance of visible skin changes. However, the proven causality between acute flare-ups and psycho-energetic changes is significant.
2.5 What Stages Does Atopic Eczema Go Through?
An eczema patch goes through three stages. Among infants, cradle cap, perianal dermatitis or diaper dermatitis may be the first initial manifestation of atopic eczema. Eczema patches may also appear on the hairy scalp and cheeks; this was confirmed for the 20 infants which were tested and treated. In older children and also in adults, the areas of skin usually involved are around the joints and on the limbs. However, the atopic eczema developed a-typically in two of the study cases.

Fundamentals
Page 6
Fundamentals: www. lifeline.de
The subjects presented the eczema also in the armpit and on the side of the torso. Further varieties of eczema are the so-called minimal eczema and dyshidrotic hand eczema.
2.6 Symptoms
The symptoms of atopic eczema are diverse and, among other things, age-dependent. In general, three stages can be observed as an eczema develops: the acute stage, as the eczema forms, the chronic stage and the final stage with the thickening of the stratum corneum and a coarsening of the skin surface.
a) During the acute initial stage of eczema, inflammatory changes appear, such as: reddening, swelling of the skin, oozing and crust formation, in particular due to secretions drying out. If this early inflammatory reaction is treated promptly, correctly and fully, there is legitimate hope that the eczema may be treated successfully and that a manifestation or a further chain of allergic sequelae may be avoided.
b) If children in this stage are treated with a steroid, the eczema is usually stopped, as occurred also in ten of the patients tested for this study, but the eczema progresses to the chronic stage. This shows with the formation of red papules which itch intensely, whereas other predictable attendant symptoms and other additional manifestation (family diathesis) do not develop.
c) If the eczema progresses to the manifest stage, that is, if the eczema continues for a prolonged period of time, the epidermis may thicken due to a higher rate of cell division in the basal cell layer. The stratum corneum, in particular, becomes thickened and becomes noticeable in the form of white scaling. In a chronic manifestation of eczema, sections of the skin feel rougher, exhibiting lichenification.
d) In particularly severe cases among affected children, there is a danger of psychological harm, not least because of the scabbed scratch marks which often present at this stage and are visible to others, as well as the strongly altered appearance of the skin. The constant pain of the affected skin patches (hollow of the knee, elbows, neck, chest and torso) leads to a diminished quality of life. In families with many children, only one of which is affected, the manifest forms often lead to jealousy and quarrelling. The reason is the increase in care and concern for the sick child.
2.7 Changes of the Skin
The affected skin areas of the children treated in the study included first of all the expected areas: elbows, hollows of the knee, chest, side of the neck and torso. They also included more unusual areas: wrists, back of the hands and thighs. The same skin areas may of course also be affected in adults.
1. Lips: In subjects with a predisposition to eczema, the lips have a strong tendency to dry out. The lips dry out especially during the colder months of the year; licking (wetting) the lips may even lead to so-called lip lick dermatitis (cheilitis). This may further lead to angular cheilitis (perlèche) and, over time, to cracks in the skin (rhagades).
2. Eyelids: Reddening and eczema on the eyelids were also observe when, in spring or in summer, the skin of the face came into contact with pollen. In these cases, it is not infrequent for the eyelids to swell significantly.

Fundamentals
Page 7
Fundamentals: www. lifeline.de
3. Pityriasis alba: Pityriasis alba refers to light, fine-scaled patches of skin about the size of a coin (pityron = small; alba = white). They occur mainly in children, on the face or arms and do not, in themselves, constitute a disease.
4. Rhagades: These painful cracks in the skin (rhagades) appear at the base of the earlobe, at the corners of the mouth or in the space between the fingers of affected subjects.
2.8 Unusual forms of atopic eczema:
A particular form of atopic eczema is dyshidrotic hand eczema. Contrary to previous assumptions, there is no link between the changes of the skin and the functioning of the sweat glands (dys = bad; hidrosis = sweating).
It is characterised by many small (often no bigger than the head of a needle) and very itchy blisters filled with clear fluid on the sides of the fingers and/or toes and on the palms of the hands and/or the soles of the feet. This unusual form often occurs due to underlying allergy to nickel or perfumes (cosmetic and personal care products), or dermatomycosis. Chronic skin damage due to clogging of the skin pores (the skin is the largest excretory organ), for example because of alkaline soaps or cleaning products, paraffin derivatives and paraffin-based cosmetic products, may facilitate the onset of dyshidrotic eczema, especially if the subject is also a smoker (more toxic excretory products than non-smokers).

Diagnostic Criteria Page 8
Fundamentals: www. lifeline.de
3 Diagnostic Criteria Used in the Treatment Sessions
3.1 First-Order Diagnosis Criteria
a) Eczema in areas which are typical for atopic eczema (elbow, hollow of the knees, nape
of the neck, neck and face)
b) Strong itching, chronic course (longer than six months) and repeated relapses of the disease
c) One or more family members falling ill with atopic eczema, hay fever or bronchial
asthma.
d) Familial allergic predisposition such as allergies to foods or food components.
Testing of all 20 patients aged between 6 months and 15 years for allergies to foods or food components using biochemical screening of blood drops using a biotensor.
20 P Wheat Gluten Lactose Egg white
Citrus fruits Meat Food additives Nuts
18P 4P 5P 5P 6P 4P 18P 6P
Table 1: Various types of food or food additive allergy were ascertained in all tested patients.
Further diagnostic indications for initial classification: – Vitamin B deficiency – Subject exposed to heavy metals, also prenatally – Excessive exposure to vaccines through multiple vaccinations – Excessively low pH-values in urine
3.2 Second-Order Diagnostic Criteria
So-called stigmata of atopy are certain physical features that are statistically more frequent in patients with atopic disposition than in the general population. These features are not determined by atopic eczema itself and may also occur in subjects with healthy skin. The occurrence or lack of one or more atopic stigmata can neither demonstrate nor exclude an atopic disposition.
3.3 Relevant Observations
In subjects with atopic disposition, itching occurs more frequently than in others if they wear wool directly on the skin. Itching may occur also during heavy perspiration. The face of subjects with atopic disposition frequently appears pale; the eyes may also be circled by dark rings (parasites and/or helminths).
In the younger patients of the treatment set especially (usually starting from 4 years of age), a double lower eyelid was observed. This double eyelid occurs in about 60% of all subjects with atopic disposition, but only in about 20% of the general population. Furthermore, it was also established that the eyebrows appear to thin out laterally.

Diagnostic Criteria Page 9
Fundamentals: www. lifeline.de
In the presence of atopic disposition, the skin appears wrinkly due to dryness.
Also, the hand lines on the palms were observed to be more pronounced.
A tendency to constriction of blood vessels in the skin, known as "white dermographism", was also identified.
All of the 20 patients with atopic eczema or disposition who were treated in the study had a positive stool culture. Intestinal candidosis with Candida albicans and Candida parapsilosis as the peri-natal form was found in all patients; one parasitosis was also identified. Considering that, as already mentioned, the intestine accounts for about 70% of the immune system, a progression of atopy is certain with this additional and significant weakening of the immune system. Consequently, it is not possible to stop the progression of atopy over the long term without an effective therapy for the intestine and subsequent symbiotic development of the intestinal environment.
Dermographism (derma = skin, graphein = to draw) literally means "drawing on the skin". Firm stroking of the skin with the tip of an object normally leads to dilation of the blood vessels and to streak-shaped reddening of the skin. This red line can be observed in most subjects with atopic disposition (and also in some people with healthy skin); due to vasocostriction, after about 15 to 60 seconds it transforms into a white stripe.

The Treatment of Atopic Dermatitis Page 10
The Treatment of Atopic Dermatitis www. lifeline.de
4 The Treatment of Atopic Eczema (Neurodermatitis)
The treatment of atopic eczema/neurodermatitis in the 20 study patients was composed by internal and external treatments. The therapy began with regular and universally paraffin-free skin care.
4.1 External Treatment
All patients were immediately administered gamma-Linolenic acid (evening primrose oil 600 units), which has a lipoid effect. Fats may be built into the stratum corneum of the skin; they may bind to and carry away toxins and inflammatory substances. Furthermore, a rose cream by the brand Wala was used to refatten the skin, which significantly improved skin topography. For preponderantly dry skin with scabbing and scaling, a cream with viola tricolor (heartsease) was also used, with almond oil as an addition. With these combinations, a substantial improvement of itching and an improvement of skin protection (reinfection) was reached.
The external treatment was continued until complete healing. In some cases, bath milk (Wala brand) was also used, added to bathwater. A spontaneous improvement of the skin occurred in all patients within 14 days of gamma-Linolenic acid administration. A mercurius solubilis ointment (Wala brand) was also used with good results on weeping or open wounds.
Laser application was not carried out in this study. In other cases of atopic eczema, it was used to obtain very good results in healing open and weeping wounds.
4.2 Internal Treatment In this study, treatment occurred by means of bioresonance therapy (abbr. BRT), using a Bicom 2000 device manufactured by Bicom. This bioresonance device works with a modulation mat (integrated magnetic field).
The treatment of all pathogenic germs (fungi/parasites) found was carried out by means of current frequencies (system by Dr. Clark, although with our own modified frequencies), know as Frequency Specific Microcurrent Therapy (abbr. FSMT) with a frequency generator produced by Hameg.
Additionally, all subjects received a concomitant homoeopathic treatment in support of the therapy. To complete the entire therapy, treatment of the miasmatic load (miasma = genetic information) was carried out in all study patients. This avoided possible earlier links (disease information) breaking out again in this genetic material.

Bioresonance Therapy Page 11
BICOM Resonance Therapy: Martin Keymer HAUG Verlag 4th edition, improved
5 Bioresonance Therapy
The expression "Bioresonance therapy" ("BRT" in short) was coined in 1987 by the Brügemann-Institut to refer to "therapy with the patient's own oscillation". This form of therapy can be traced back to Dr. F. Morell [a], who originally presented his idea in 1977.
Truly great, historic inventions are often surprisingly simple. Morell's postulate that the pathological energies of the body itself can be taken in order to implement a highly individual and effective therapy from them has introduced a new age in medicine.
5.1 Electromagnetic Oscillations
A quick outline of the idea: All diseases and their pre-conditions are accompanied or caused by electromagnetic oscillations. There are no pathological manifestations without the presence of pathological oscillations (oscillations which originate from an existing disease or which lead to a disease) in or around the body. In the body of any one patient, pathological electromagnetic (that is, originating in the cell, which has its magnetic field) oscillations are active alongside healthy ones. The spectrum of the waves ranges from very short (MHz) to extremely long (Hz). Pathological oscillations in the body disturb the physiological states of balance and the cybernetic regulating cycle. They adapt to the human biorhythm, which alters accordingly (imbalance of the oscillation ratio). The body becomes ill when the dynamic equilibrium cannot be maintained through counter-regulation. In addition, there are also numerous underlying conditions that the patient is not aware, which may further stress the body. Conventional diagnostics do not take them into consideration or cover them. The electromagnetic oscillations of a patient include literally all information which is necessary for the therapy, even though in a not yet decoded form.
Because the patient's own oscillations are electromagnetic in nature, they can be obtained from the patient's body by means of electrodes. The electrodes are made up of multiple layers. The middle layer contains a magnetic coated film with a magnetic field force which is equivalent to the maximum strength of the magnetic field of the Earth. Since the magnetic field fully permeates body tissue, oscillation are registered and entered into the therapy device not only from the skin surface, but also from inside the tissue and the organs (Fig. 1).
Figure 1: The Bicom electrodes feature a magnetic field which is equivalent in strength to that of the Earth's magnetic field. Therefore, they not only capture the bioenergetic oscillation of the skin, but instead they penetrate the tissue and are thus able to collect information from inside the body.

Bioresonance Therapy
Page 12
BICOM Resonance Therapy: Martin Keymer HAUG Verlag 4th edition, improved
How the Separator Functions
5.2 The Separator
Using a device known as a separator (molecular absorption circuit), the physiological oscillations, which are qualitatively equal in all human beings, are filtered out using a filter, following an idea of L. Mersmann [b]. For this purpose, substances are used which enter into resonance only with the physiological oscillations, and not with the different pathological frequencies that vary from patient to patient depending on exposure and illness. Likewise, electromagnetic and geopathic interference frequencies are not picked up by this filter. Thus, the separator only enters into resonance only with harmonic frequencies, and not disharmonious ones. Only the disharmonious frequencies are transferred from the exit of the separator. In this way, it is possible to separate the harmonic and disharmonious frequencies (Fig. 2).
Figure 2: A separator in the BICOM device divides the ultrafine electromagnetic oscillations collected from the patients body into physiological and pathological oscillations.
Bicom device with integrated separator
Entry A = All Frequencies
H = physiological part
Di = pathological part
Exit

Bioresonance Therapy
Page 13
BICOM Resonance Therapy: Martin Keymer HAUG Verlag 4th edition, improved
5.3 The Cybernetic Regulating Cycle between Patient and Bicom Device
From the exit of the device, the therapeutic oscillations are given back to the patient through a second electrode, which returns the physiological frequencies positively (positive feedback), whereas the pathological oscillations are returned negatively, that is to say inverted (negative feedback). The patient's electromagnetic field of the patient immediately reacts to the therapy signals and, in turn, returns a consequently altered oscillation oscillation pattern to the bioresonance device. This process is constantly repeated in fractions of seconds. In this way, pathological oscillations in the body are reduced and, in the ideal situation, ultimately eliminated. The body is thereby again able to regulate itself with its biological processes. The physiological balance can thus be reinstated (Fig. 3).
Figure 3: Using an electrode, the patient's body signals are guided from one of the hands into the device entry. The pathological frequencies are filtered out in the device and inverted. These oscillations are made available at the device exit as therapeutic oscillations and are guided through the other hand into the patient's body again by means of a second electrode.
This is the principle of bioresonance therapy. Morell called this type of treatment "Moratherapy", in which the word "Mora" is made up by the first letter of the names Morell and Rasche. Rasche, Morell's son-in-law, built the first therapy device of this kind; it was calld "Mora" device. In the course of ten years, the Institut für Regulative Medizin in Gräfelfingen made this process known worldwide among therapists. To be able to carry out successful therapy with bioresonance, each patient must be tested for his or her excretion capacity; in the event of a dysregulation of the excretory organs, these must be made able to excrete and regulate before proceeding. Otherwise, the patient will be led to a further health crisis.
The patient and the BICOM device together form
a closed cycle ENTRY
incoming oscillations
ENTRY
pathological oscillations
EXIT
incoming
oscillations pathological oscillations
outgoing oscillations
Therapy Oscillations
pathological oscillations eliminated
Outcome:

Bioresonance Therapy
Page 14
BICOM Resonance Therapy: Martin Keymer HAUG Verlag 4th edition, improved
5.4 Pischinger's Ground Regulation System
The system in which this regulation occurs is known as "Pischinger's Ground Regulation System",
and it is named after Prof. Pischinger [c] (Vienna).
Figure 4: The ground regulation system in soft tissue, according to M. Keymer. Removal of exogenous or endogenous noxious agents through the blood and lymph, as well as the organs. Study materials of the IMU College PD Martin Keymer.
Cell supply channel Capillary cell
Cell detoxification
through the blood
Cell detoxification through the lymph
Transport
of
nutrients
and
oxygen
through
the blood
Artery
Lymph vessel with blind ending in tissue
Re
mo
va
l o
f w
aste
p
rod
ucts
Organ cells
Capillaries
Organ cells
Accumulation of Toxin Excesses from the Cell and Storage of External Toxins
Removal of waste products
Neural supply of the
cell through the
termination of the
autonomic nervous
system

Bioresonance Therapy
Page 15
BICOM Resonance Therapy: Martin Keymer HAUG Verlag 4th edition, improved
5.5 Endogenous and Exogenous Noxious Agents
All endogenous and exogenous noxious agents (noci = harmfulness, pathogenic cause) must be evacuated from the body through the excretory systems for toxins (out of the cell) and the detoxifying organs (stomach/intestine, liver/gall bladder, kidneys/bladder and the skin). If there is an acute strain, then the typical symptoms of a detoxification reaction appear, such as diarrhoea, vomiting, sweating, etc. In the event of chronic intoxications, no choice remains for the body except to store these toxin excesses in the body. The toxin storage then occurs in "Pischinger's Ground Regulation System".
Therefore, this system is almost an internal landfill, in which the body stores these huge amounts of poisonous substances. This "toxic waste" can be stored here for years and continue to accumulate. It is only through an improvement of the body's excretory capacity or by stopping a chronic intoxication, e.g. by removing eczema patches or by decontamination from toxins in living spaces, that a reduction of the stored poisons can be brought about. If this does not occur, then the summation of the toxic substances and the cumulation of toxic effects which reciprocally exacerbate one another lead to the function of Pischinger's system (storage of toxins in order not to excrete them) finally impairing the supply and disposal of substances in the cells. This subsequently leads to a reduction of parenchyma functions of the parenchyma cells in the organsm, until ultimately irritation of the cellular metabolism presents, usually overlapping into the stages of the anaerobic metabolic processes.
However, the anaerobic metabolism produces large amounts of lactic acid, which are handed over to the mesenchyme and push the body's pH values into the acid range. This is damaging especially because the inadequate disposal of toxins and waste products creates a vicious cycle; as this situation builds up, the body finds itself constantly in the acid range. As a rule, this is the start of chronic symptoms, the origin of which should be searched for in the years or even decades of summation and cumulation of different toxic exposures with an inadequate excretory capacity.

The Cybernetic Loop Page 16
BICOM Resonance Therapy: Martin Keymer HAUG Verlag 4th edition, improved
6 The Application of the Cybernetic Regulating Cycle
The term "Cybernetics" was coined by Wiener [d]. Cybernetics comes from the Greek and is the "art of steering". Cybernetics comprises the principle of actio/reactio. For each deviation from a set course (action), the captain must enact a reaction, a correction by means of steering.
Cybernetics has introduced an interdisciplinary cooperation, the relevance of which should not be underestimated in relation to advancements in very diverse scientific fields. The core of cybernetics is the so-called cybernetic regulating cycle. It is widely employed in technology. However, the body also features a number of such regulating cycles.
Before a regulating cycle can begin functioning, an "objective" or "setpoint" must be defined. When flying, it would be the destination airport; when setting the central heating, it would be 21°C. The objective in the body's own regulating cycles would, for example, be to reach a body temperature of 36°C or blood sugar levels of 85-110 mg.
The next part of the regulating cycle is an activity in the direction of the objective. On the way to the objective, how far the activity carried out to that point has led to reaching the objective is constantly being tested. Any deviations are reported to the regulation headquarters. The "regulation headquarters" make a correction in the direction of reaching the objective on the basis of the information received. This "feedback" and the corrections are applied repeatedly, until the objective is reached. Thus, the components of the cybernetic regulating cycle are the following:
a) a Setpoint b) an Activity, in order to reach the objective c) a Measurement and a Feedback regarding what has been achieved so far d) a Correction, if the feedback and the value require it
e) further actions, feedback and corrections until the objective is reached (Fig. 5)
Figure 5: The function of the system remains within a tolerance range. If this function is derailed, feedback is sent to the system, which consequently enacts a correction.
Diagram Showing How the Cybernetic Regulating Cycle
Functions
Representation of the Cybernetic Regulating Cycle
Setpoint⇒ C⇒A⇒M
⇑⇐ F⇐⇓ Correction mechanism Activity
curve
Tolerance - range
NORM
Tolerance - range
Correction mechanism
D = Deviation CF = Control / Feedback
Sy
stem

The Cybernetic Loop Page 17
BICOM Resonance Therapy: Martin Keymer HAUG Verlag 4th edition, improved
6.1 Representation of the Cybernetic Regulating Cycle
The image below intends to illustrate how the cybernetic regulating cycle is used in bioresonance therapy. For didactic purposes, a single pathological oscillation is represented as an example; the body's own oscillations actually comprise multiple signals over a large frequency range (Fig. 6).
Figure 6: At the beginning of the therapy, the patient passes oscillation 1a to the BICOM device (F). The oscillation is inverted in the device and then returned to the patient as oscillation 2a (C). The patient has a reaction (A) and s/he then passes an altered oscillation, which we indicate as 1b (M), to the BICOM device. The device then returns a consequently corrected therapy oscillation (2b) to the patient. The patient reacts to oscillation 2b and "reports" this to the device by entering an oscillation which is again altered. This process continues over the entire treatment.
The device does not store the oscillations obtained from the patient at the start of the therapy; rather, patient and BRT device form a cybernetic regulating cycle. Thereby, the highest degree of therapy effectiveness is reached.
The setpoint of BRT is the reduction and ultimately elimination of pathological oscillations in the body, in order to allow the body's own regulation mechanisms to become active without hindrances. With this objective, BRT fully shares the aims of classical natural medicine. No doctor can reach a greater result than that of fully restoring the body's own regulation mechanisms. Chronic illnesses begin where the body's own regulation mechanisms are no longer capable of unfolding their power due to pathological signals which have become overpowering. With BRT, nature itself is given the chance to regain "rule" of the body and re-establish health. For infants and toddlers, this sometimes occurs with a few seconds of treatment time. For older, chronically ill patients, the process requires 3 to 5 or more therapy sessions each with 5-15 minutes treatment time.
The patient and the BICOM device together form a cybernetic regulating cycle.
F
C M
A
ENTRY EXIT
incoming pathological oscillations
outgoing inverted oscillations
Inverting results in
= Zero signal in the body

Test Procedure Page 18
BICOM Resonance Therapy: Martin Keymer HAUG Verlag 4th edition, improved
7 Applied Test Procedure
The test procedure which was used in this study is the biotensor. It was applied in the patient's absence to a drop of blood drawn from him or her. The biotensor was chosen because of the following reasons:
a) Quick detection of pathological oscillations b) Convenient operations on blood drops, independently from the patient's presence c) Objective and precise diagnosis d) Possibility to carry out also mental testing e) Possibility to immediately test therapy success f) Possibility to test therapy steps g) Safe testing of pathological or allergic substances, medications etc.
7.1 The Biotensor
The biotensor is a device which measures values of biochemical/biophysical process and then converts them into electric signals. The signals are obtained using an electrode. The biotensor comprises an antenna, which looks a bit like a key (although different shapes are available) and to which a flexible metal rod is attached at one end, and a metal grip at the other end. The grip is connected to the test part of the bioresonance device by a cable. The antenna, which captures oscillations and is located at one end, is placed between the blood drop and the substance to be tested or the test ampoule from the test tray in use, which can be measured through an electrode.
A separating (vertical) swing indicates that there is no resonance between the substance and the blood drop. A connecting (horizontal) swing indicates that there is a resonance between the substance and the blood drop which should be adequately classified. This means that there is a resonance (connection) between the information of the test material (test ampoule or native preparation) and an already existing, equivalent piece of information in the patient's blood drop In many cases, the biotensor is the most advantageous and fastest test procedure in bioresonance therapy.
Figure 7: Biotensor
However, a precise anamnesis of the patient is required as an indication for the selection of the test ampoules or the test materials in order to test successfully.
7.2 Test Materials Used
The test ampoules are prepared by the Regumed company and the Martin Keymer Private Institute for Dermatology. The former are known as "combined testing technique" CTT, the latter as "interconnected testing technique" ITT. Each drop of blood was tested with these ampoules (biochemical screening)
The patient's capillary blood for the tests was taken from a finger or heel and placed on a cellulose swab. We also tested skin swabs, which were taken directly from the skin with cotton swabs soaked in alcohol. We also requested a stool sample from each patient in order to obtain a stool culture.

Test Procedure Page 19
BICOM Resonance Therapy: Martin Keymer HAUG Verlag 4th edition, improved
7.3 Biophysical Resonance Testing Put to the Test
Allergen testing in comparison: IgE/IgG was compared to biotensor testing in an instructive and interesting study carried out by Dr. P. G. Valeske [e], in which he contrasts the results of an energetic test procedure with the generally known IgE/IgG. The study was conducted with 18 subjects who presented different allergies. It is being recounted here merely as an example; it has no connection to the study on "atopic eczema".
The link between this biophysical testing of an allergy and the biochemical examinations of conventional medicine may lie in the determination of the allergy specific IgG antibodies. With this comparative study between tensor testing and the determination of IgG antibodies, the reliability of test results obtained with the biotensor can be substantiated, as this study shows.
7.4 The Method of the Comparitive Study
18 patients with asthma, neurodermatitis, hay fever, enteropathy, itching, etc. blood was taken at the same time for testing with the biotensor (blood drop on cellulose swab) and for IgE and IgG determination. The allergens found with the biotensor were checked using IgE and IgG grids (external laboratory). In some cases, further allergens were identified in the laboratory. For reasons of cost, this investigation was limited to 18 patients and 5 determinations each.
In the comparison of the allergy tests with the biotensor and the results of the allergy-specific immunoglobulins, the results practically always coincided. The biotensor showed a negative result which differed from the IgG determination in 9 of the 65 total single tests available. On the contrary, each positive value obtained with the biotensor could be confirmed at least by the IgG value, but often (16 times) also by the IgE value.
Allergens
Allergen total Biotensor IgE IgG
Milk 12 11 0 12
Wheat 14 11 6 12
Egg white 9 7 2 6
Soy 3 3 1 3
Yeast 2 2 1 2
Apple 2 2 1 2
Rye 6 5 3 5
Oat 1 1 1 1
Barley 2 2 1 2
Gluten 4 2 0 4
Tomato 1 1 0 1
Candida 2 2 0 2
Egg yolk 2 2 0 2
Hazelnut 2 2 0 2
Pork 1 1 1 1
Sole 1 1 1 1
Orange 1 1 1 1
Sum 65 56 19 59
Table 2: Test Results in Comparison Biotensor-IgG

Therapy System Page 20
IMU International Mediterranean University: Study materials for bioenergetic medicine
8 Therapy Methodology in the Study
The treatment process followed the criteria of the "Therapeutic House" which was founded by M. Keymer. It was applied without variations to all 20 patients. We implemented therapy intervals in 14-day cycles and verified the previous treatment with laboratory follow-ups.
8.1 8.1 Therapeutic Procedure
1.) Laboratory analysis with biotensor technology and discussion of the therapeutic procedure
2.) Application of gamma-linolenic acids
3.) Repertorisation of an appropriate concomitant homoeopathic medicine
4.) Testing of excretion and therapeutic capacity
5.) Start of BRT therapy and specific medication, depending on the existing condition: Intestine therapy for mycoses with Para-Rizol, Candida Cleanse capsules, intestine cleansing capsules and Trenev Trio capsules. For children, Mycostatin instead of Para-Rizol. Frequency Specific Microcurrent Therapy (FSMT) to treat pathogens, parasites and mycoses.
6.) Excretions of heavy metal toxins and other toxins:
Chlorella algae tablets and coriander drops.
7.) Therapy to build-up the immune system: BRT, echinacea drops, vitamin C and B complex.
8.) Repertorisation of miasms
9.) Treatment with miasms: homoeopathic medicines
10.) Final review of the therapy

Laboratory Findings
Page 21
9 Assessment of Laboratory Findings
Assessment of the laboratory findings obtained for the 20 patients treated in this study, aged between 6 months and 15 years. 12 of the chosen patients had been previously treated with and exposed to steroids (cortisone). Administration occurred both orally and using cortisone creams produced by several brands. The other 8 patients had already taken at least one allergy medication once and had been exposed. The laboratory tests which were carried out with biotensor technology were checked with fresh blood after each completed treatment.
9.1. First Pathogen Detection in the First Patient Group from Blood and Stool
Assessment of the 12 patients who had been previously treated with a steroid. These patients were aged between 6 months and 15 years.
Number of P:
Bacteria Viruses Parasites Laboratory evidence
chron. acute
chron. acute chron. acute
12 P 12 P 4P 6 P 2 P 12 P 10 P prior to treatment
12 P 0 P 10 P 6 P 3 P 0 P 0 P during treatment
12 P 0 P 5 P 0 P 0 P 0 P 0 P after treatment
Table 3: 1. Patient group (12 P) with previous exposure to steroids
The treatment of pathogens and parasites was carried out with BRT and FSMT. Relatively high reinfection through skin wounds (scratches) and suppressed skin responses, as well as counter reactions to cortisone treatment, were clearly recognisable during treatment. End of treatment occurred after 8 weeks for all patients. In this patient group, the state of the skin appeared still quite rough in the previously treated areas. These areas required further treatment with fatty ointment for quite some time. Despite good end results, the relapse rate, 5:12, remained
very high (
9.2. Second Pathogen Detection in the Second Patient Group from Blood and Stool
Assessment of the remaining 8 out of 20 study patients; these patients had been previously treated with allergy medication. These patients were aged between 6 and 24 months.
Number of P:
Bacteria Viruses Parasites Laboratory evidence
chron. acute
chron. acute chron. acute
8 P 8 P 2 P 1 P 2 P 8 P 0 P prior to treatment
8 P 8 P 3 P 3 P 0 P 0 P 0 P during treatment
8 P 0 P 2 P 0 P 0 P 0 P 0 P after treatment
Table 4: 2. Patient group (8 P) with previous exposure to allergy medication
The treatment of pathogens and parasites was carried out with BRT and FSMT also in this group. Skin wounds through scratching were also found in this patient group. However, in proportion to the scratch marks, reinfection was relatively lower than in the first group, which is probably linked to a more stable immune situation. End of treatment occurred after 8 weeks for all patients. The state of the skin in the patients who had been previously exposed to an allergy medication already appeared to be relatively good in the previously treated areas. The skin was further treated with fatty ointment also in this case. The recurrence rate amounted to 2 out of 8 patients (= 25%) here.
Laboratory Findings
Page 22
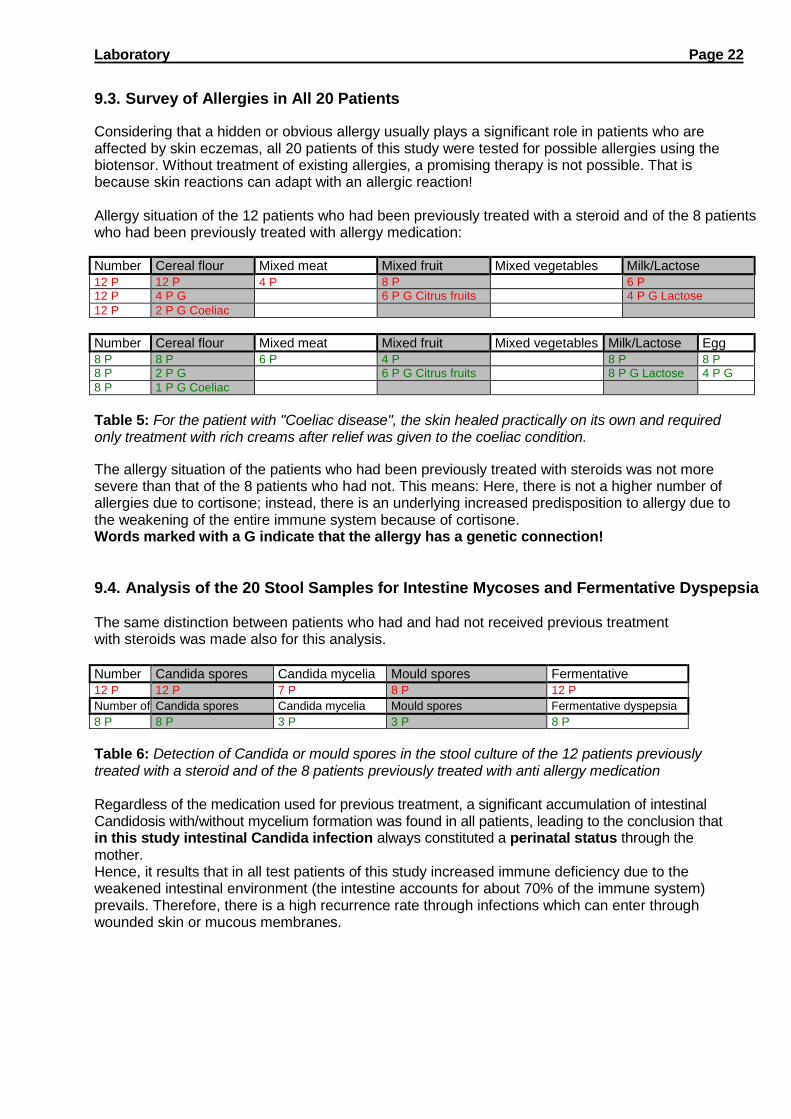
9.3. Survey of Allergies in All 20 Patients
Considering that a hidden or obvious allergy usually plays a significant role in patients who are affected by skin eczemas, all 20 patients of this study were tested for possible allergies using the biotensor. Without treatment of existing allergies, a promising therapy is not possible. That is because skin reactions can adapt with an allergic reaction!
Allergy situation of the 12 patients who had been previously treated with a steroid and of the 8 patients who had been previously treated with allergy medication:
Number of P
Cereal flour Mixed meat Mixed fruit Mixed vegetables Milk/Lactose
12 P 12 P 4 P 8 P 6 P 12 P 4 P G 6 P G Citrus fruits 4 P G Lactose
12 P 2 P G Coeliac disease
Number of P
Cereal flour Mixed meat Mixed fruit Mixed vegetables Milk/Lactose Egg white 8 P 8 P 6 P 4 P 8 P 8 P
8 P 2 P G 6 P G Citrus fruits 8 P G Lactose 4 P G
8 P 1 P G Coeliac disease
Table 5: For the patient with "Coeliac disease", the skin healed practically on its own and required only treatment with rich creams after relief was given to the coeliac condition.
The allergy situation of the patients who had been previously treated with steroids was not more severe than that of the 8 patients who had not. This means: Here, there is not a higher number of allergies due to cortisone; instead, there is an underlying increased predisposition to allergy due to the weakening of the entire immune system because of cortisone. Words marked with a G indicate that the allergy has a genetic connection!
9.4. Analysis of the 20 Stool Samples for Intestine Mycoses and Fermentative Dyspepsia
The same distinction between patients who had and had not received previous treatment with steroids was made also for this analysis.
Number of P
Candida spores Candida mycelia Mould spores Fermentative dyspepsia 12 P 12 P 7 P 8 P 12 P
Number of P
Candida spores Candida mycelia Mould spores Fermentative dyspepsia
8 P 8 P 3 P 3 P 8 P
Table 6: Detection of Candida or mould spores in the stool culture of the 12 patients previously treated with a steroid and of the 8 patients previously treated with anti allergy medication
Regardless of the medication used for previous treatment, a significant accumulation of intestinal Candidosis with/without mycelium formation was found in all patients, leading to the conclusion that in this study intestinal Candida infection always constituted a perinatal status through the mother. Hence, it results that in all test patients of this study increased immune deficiency due to the weakened intestinal environment (the intestine accounts for about 70% of the immune system) prevails. Therefore, there is a high recurrence rate through infections which can enter through wounded skin or mucous membranes.

Laboratory Findings
Page 23
9.5. Testing of Chewing Gum or Blood Drops for Heavy Metals
A heavy metal intoxication was found in all 20 patients. In this case, the division of patients is based on the statements of their mothers, depending on whether or not they had dental work during pregnancy. In 9 cases, the mother of the patient had dental work during pregnancy, not for the other 11 patients. The intoxication occurs via the mother's milk and placenta.
Number of P
Amalgam Mercury Cadmium Silver
9 P 9 P 7 P 5 P 8 P
Number of P
Amalgam Mercury Cadmium Silver
11 P 6 P 5 P 3 P 1 P
Table 7: Again, the analysis is significantly higher in cases with previous dental work than in those which had no previous dental work. Concomitantly, a higher aluminium concentration was established in the first 9 patients than in the other 11 patients, whose mothers' had no dental work carried out during pregnancy. With these analyses, it remains unclear to what extent the exposure to fungal spores or mycelia through the mother is favoured by intake of heavy metals.

Perinatal Fungal Infections
Page24
Vaginalmykose und perinatale Pilzinfektion. Karger Verlags AG 1982
10 How Does Perinatal Transmission of Yeast Fungi Spores Occur?
The answer to this question was pursued by Professor Dr. med. Johannes D. Schnell [g] in a number of studies at the gynecological clinic of the University of Düsseldorf. The objective and the substance of the studies were the identification of the sources of possible perinatal fungi contamination. Examinations were carried out on intrauterine material (upper and lower pole of the egg), vaginal material, nipples of nursing mothers, furnishings and newborn care staff.
10.1 Pathogens
The fungi which could be detected in the vagina and in newborns fell exclusively into the category of imperfect yeasts. Propagation through growth occurs by means of cell budding (Fig. 8a and 8b)The most frequently occurring species was Candida albicans, although by now over 80 types of Candida are known. The following are clinically relevant: Candida albicans, Candida parapsilosis, Candida krusei, Candida stellatoidea, Candida tropicalis, Candida pseudotropicalis, Candida guilliermondii and Candida pelliculosa. The species of Candida mentioned above can form pseudomycelia as well as sprout cells. Geotrichum candidum was previously understood to be a yeast fungus but later classified as a deuteromycetes.
8a
8b
Figure 8: 2. Germination. Ring-shaped bulge and beginning cytoplasm bulge (small arrow) as well as advanced sprout cell formation (large arrow) of Candida albicans. a) Scanning electron microscope picture of a young Candida albicans culture, with c. 8400 x enlargement. b) Transmission electron microscope picture of Candida albicans cells in a vaginal epithelial cell, with c. 8400 x enlargement.

Perinatal Fungal Infections
Page25
Vaginalmykose und perinatale Pilzinfektion. Karger Verlags AG 1982
10.2 Transmission of Yeasts
There are isolated descriptions in literature of infections of the chorion and amnion due to Candida albicans, as well as of foetus infections with retained amniotic sacs, first by Benirschke and later by Raphael [h]. Cultural studies on 50 pregnant women ante partum showed that one out 8 infections in material obtained from the placenta was due to Candida albicans. In the other 42 cases, this could not be completely ruled out.
The main infection occurred through the vagina when the waters had already broken. At the end of pregnancy, fungal yeast infections are about 2.5 times higher than in healthy women who are not pregnant. The highest infection rate occurs in the first 12 hours after waters breaking. After that, the infection rate continues to decrease. This form of transmission of yeast from the mother's vagina to the child's body during birth (Tab. 8) could be established in 67.9% of cases. The dependence of fungal yeast infections in children directly post partum (after birth) from the mother's affliction is highly significant (X2 =360.9; p< 0,001).
Mother, antepartum Child, postpartum
Vaginal findings n (= 100%) negative
positive
n % n %
Negative 444 (447-3)' 435 98.0 9 2.0
Positive 159 (160-1)' 51 32.1 108 67.9
Total 607
Table 8: Yeast infection in the child directly post partum in relation to the mother's vaginal findings
10.3 Yeast Infection in Post-Partum Newborns
The different types of disease in the newborns can be classified based on frequency: 1. Mycoses of the oral cavity (thrush, also without known plaque) 2. Mycoses of the genital and anal area and of the skin (nappy rash) 3. Mycoses of the gastro-intestinal tract (oesophagus, small intestine) 4. Mycoses of the organs and fungal sepsis
Based on the research carried out and on available literature it can be assumed that during neonatal period about 1 out 4 newborns comes into contact with yeast. But not all of these children become sick. For this reason, already in 1880 Epstein [i] coined the expression "latent microbism of thrush fungi" when he discovered the germs also in the mouths of healthy infants. The diagnosis "thrush" is still today all too often understood as a purely descriptive term. Thrush is equated to mycosis; the fungal infection is thus present even if the typically associated coatings cannot be ascertained. The contaminations of the genital and anal areas (nappy rashes) can be seen as early as 5 days of age, also in other skin areas, and they reach their peak by 6 months of age.

Perinatal Fungal Infections
Page26
Vaginalmykose und perinatale Pilzinfektion. Karger Verlags AG 1982
10.4 Different Sites of Infection with Yeast Fungus
Figure 9: Oral Thrush at 4 Days of Age Figure 10: Inguinal and Genital Area Thrush at 5 Days of Age
Figure 11: Extensive Nappy Rash at 4 Weeks of Age (starting at 10 days of age inadequately treated)
Figure 12: Candida Bronchopneumonia
Fungal elements in the terminal bronchioles and alveoli
Gastro-intestinal mycoses constitute the most serious type of fungal infection. In this situation, the entry of yeast in the bloodstream can cause fungal growth in the organs; and very often a lethal fungal sepsis may arise. De Gavallèr [j], with 288 autopsies of infants who had died after 3 days of age, established in 25% of cases the presence of candidosis, which constituted the main cause of death in 3.4% of the autopsies. Bronchopulmonary candidosis was identified in 1.05% out of 1000 autopsies of newborns.
Illnesses contracted by nursing were not confirmed during the studies; however, a contamination of the nipples through yeas can occur in the mother. This often leads to one of the unpleasant mastitis conditions. Further sources of transmission were found in the newborn care staff and in medical equipment. The reasons for this lie above all in inadequate hygiene.

Discussion Page 27
11 Discussion of Study Results Atopic eczema (neurodermatitis) is seen as being only partially curable in conventional medicine. If the outbreak occurs during childhood, there is even talk of "growing out of eczema". The expression refers to the state of the skin recovering through treatment with steroids, the metabolism gradually being built up and the immune system supposedly stabilising. Any connected allergies change or shift to a different level (e.g. respiratory) over time. The classical course of treatment in conventional medicine is still today taking place with cortisone, light therapy and fatty ointments. In part also with abstinence from particular foods, in those cases in which an allergy screening is carried out. According to the present state of our knowledge, intestinal mycoses or parasite infections are not discussed in relation to atopic eczema anywhere in conventional medical literature. The same is true of prenatal heavy metal intoxication. In each case, the energetic information of the stages of the disease undergone are preserved with this form of therapy, which may always lead to new connections. At this stage, it cannot be foreseen to what incidence of disease this might lead.
In human medicine or anthroposophic hospitals, bioresonance therapy is not used or recommended. No intestine therapy or treatments against parasites are carried out here, either. However, heavy metal intoxication is treated in some cases.
Based on this study, we can state that with a therapy based on our model and our criteria, atopic eczema (neurodermatitis) is curable with a relatively low recurrence rate. Furthermore, if previous treatment does not include steroids, the danger of further "allergic conditions" is lower, at 25%, that that for cases previously treated with steroids, for which the risk amounts to 42%. (see p. 19) This study also confirms the very high relief from allergies (over 85%) by means of BICOM therapy, which is highly significant in the therapy of atopic eczema (neurodermatitis). The therapeutic successes in this study are also based on the fact that we were able to treat only patients in childhood. The longer the disease and the connected symptoms persist, the more difficult it becomes for the therapy to be successful.
If conservative (conventional medical) therapies are compared to alternative therapies in comparable stages of atopic eczema (neurodermatitis), the conclusion can be derived that alternative therapy is preferable to conventional treatment, also for the benefit of the patient.
The conclusion of this study is thus that the pre- and peri-natal contamination by germs, mycoses, parasites and heavy metals should be viewed as the basic stress; actually, the claim arises that in most cases this must be the prerequisite for the appearance of an atopy or endogenous eczematous condition. An allergic predisposition is indeed causal, but not necessarily present as a concomitant symptom.
If all women were examined prior to pregnancy and treated in advance in the event of positive stool and vaginal findings or of existing dental implants, there would be fewer post-natal illnesses and allergies among infants. Which we strongly recommend, based on this study!
For clarification, two case studies are presented.

1. Case Study - Patient S. B. Page 28
12 First Case Study Naturopath D. Jakob Patient: S. B., 1 year old, female
Date of birth: 18. 04. 2002 Treatment period: from 16 April '03 to 12 June '03
Diagnostic Findings From Blood Work, Clinical Anamnesis and Stool Culture: Atopic dermatitis Pre-natal heavy metal intoxication Peri-natal intestinal Candidosis with Candida albicans +++ (=threefold increase of admissible sprout cell formation)
Medical History: About 6 months after birth, appearance of skin eczema in the hollows of the knee concomitantly with hip correction on one side. After further 3 months, unclear disease with large pus-filled blisters. Cause unknown! Treatment with antibiotics. In December, ill again with lung inflammation (bacterial), again treated with antibiotics. Since about 3 - 4 weeks, propagation of the eczema on the whole body. Visible scratch marks on the whole body and face. Furthermore, the patient has had an obstinate cold already for one month, which has been unsuccessfully treated with allopathic medicine. Medication until now: antibiotics, antihistamines; cough mixture and fatty creams Stool: daily, mushy Drinking: Baby bottle (water)
Familial Predisposition: bland
Laboratory Findings/Samples: Biochemical screening with blood drops on cellulose swabs and stool culture (ITT, CTT).
Therapy: Start of therapy with gamma-Linolenic acids (evening primrose Epogam 1000 units) daily 2x1 capsules. Concomitant introduction of single BICOM treatment with the programs: - Basic program with conductance value 125 - Heavy metal excretion 997 - Follow-up programme: Detoxification of mucous membranes 999 Frequency specific microcurrent therapy for the treatment of bacterial status Sugar and yeast restriction
Medication: Homoeopathic agents, rose cream, viola tricolor cream, Mycostatin 24 ml and Epogam 1000
Treatment: At 14-day intervals
Outcome:
After three completed treatment sessions in the medical practice and three consultations for the addition of medicines, the patient was completely symptom-free and has remained so until now.
Overleaf: Pictures of the state of the skin before, during and after treatment. Copies of blood and stool laboratory examinations and corresponding follow-ups.

1. Case Study - Patient: S. B. Page 29
12.1 Course of Treatment for Patient S. B.
Figure 13:
Figure 14:
Figure 15:
Patient aged 1 year, with about 5 months
without indications of incipient atopy with the following situation:
About 6 months after birth, appearance of skin eczema in the hollows of the knee concomitantly with hip correction on one side. After further 3 months, unclear disease with large pus-filled blisters. Cause unknown! Treatment with antibiotics.
In December, ill again with lung inflammation (bacterial), again treated with antibiotics.
Aged 13 months, the patient has full-blown atopic eczema, which has spread over the face and trunk. Substantial scratch marks on the face and thoracic region.
The mother came with the child with this state of the skin during consultation hours for an alternative therapy.
The patient now has a normal state of the skin, after 8 weeks of therapy with 14-day intervals, and is discharged as cured. The existing candidosis was also successfully treated.
Treatment occurred three times in the medical practice, with three consultation for the addition of medicines.
Follow-up in July 2003: the patient is still free of symptoms.

Laboratory Findings of Patient S. B.
Page 30
12.2.1 Scatology (Stool Culture) - Stool Laboratory Biochemical Screening
Laboratory E-Screening
Stool culture: Bacteria/Parasites/Fungi
Date: 1. 24. APR. 2003 4.
2. 19. MAY 2003 5.
3. Conductance value:
Patient Name: S B
Anal swab Stool sample
Initials:
Moulds: 1170 1171
1 2 3 4 5 Protozoa: 1170
1171 1 2 3 4 5
Mould Mix 1: Entamoeba histolytica
Mould Mix 2: Lamblia intestinalis
Mould Mix 3: trichomonads
Cladosporium cladosporioides Bacteria 1170 1171
Smut Mix Campylobacter coli
Geotrichum candida Campylobacter pylori
Parasites: 1171 1171 Dyspesia coli
1 Ancylostoma canimim 386/400 +3 Enterobacter
2 Ascaris lumbricoides 408 Enterococcus
3 Ascaris lumbricoides larvae 408 . Escherichia coli
4 Borrelia burgdorferi 380 Proteus
5 Clonorchis sinensis adult 414 Salmonella TP
6 Clonorchis sinensis eggs 427 Salmonella D
7 Dirofilaria 409 +3 Serratia
8 Echinococcus granulosus hydatid 461.50 Candida: 1170 1171
9 Echinococcus granulosus eggs 446.50 Albicans +3
10 Echinococcus multilocularis 458.35 Parapsil
11 Entamoeba coli histolytica Tropoz 385 crusei
12 Eurytrema pancreaticum 421 Mites: 1170 1171
13 Fasciola hepatica adult 427 Flour Mites
14 Fasciola hepatica eggs 425 +3 Food Mites 1
15 Fasciola hepatica cercaria 427 +3 Food Mites 2
16 Fasciola buski adult 434 Worms: 1170 1171
17 Fasciola buskii eggs 434 +3 Ascaris lumbricoides
18 Gardia cysticercus 364.80 Oxyuris vermicularis
19 Gardia trio 424 Taenia saginata
20 Haemoproteus 393 Coeliac
disease:
192 191
21 Naegleria fowleri 362 Cereal flour
22 Onchocerca volvulus 440 Gluten
23 Proteus vulgaris 374.80 +3 Gliadin
24 Pneumocysticus carinii 407 +3 Miscellaneo
us:
25 Schistosoma japonicum 473 +3
26 Schistosoma mansoni 353
27 Schistosoma japonicum in copula 473
28 Strongyloides stercoralis 400 +3
29 Taenia pisiformis cysticercus 480
30 Taenia pisiformis eggs 468
31 Taenia pisiformis cysticercus 475 +3
32 Taenia solium solex 448
33 Toxoplasma gondii 389.60 +3
34 Toxoplasma humanpath. Strain 395
35 Trichinella spiralis 404.50 +3
36 Trichomonas vaginalis 381
37 Trypanosoma cruzi 463

Laboratory Findings of Patient S. B.
Page 31
12.2.2 Frequency Specific Microcurrent Therapy for Intestinal Mycoses and Parasite Treatment Practice for alternative medicine FNH/NVS Naturopath D. Jakob Tel 01/970 30 55
Patient report
Client number: 917
Surname: B. First name: S. Street / Number: Post code: Tel.:
Report limited to 19 May 2003
Monday, 19 May 2003 09:03 Profile: Duration: Signal form: Frequency: Amplitude: Offset:
Candida albicans.txt 5.00000000 Sinus 264.799988 4.800000 5.000000
Monday, 19 May 2003 09:03 Profile: Duration: Signal form: Frequency: Amplitude: Offset:
Antibody Frequenz allg 5000.txt 10.000000 Sinus 500.000000 4.800000 5.000000

Laboratory Findings of Patient S. B.
Page 32
12.2.3 Fundamental Medical History (5 Elements) - Blood Laboratory Biochemical Screening
FUNDAMENTAL MEDICAL HISTORY
Patient Name: B. S. Date: 20 May 2003 Initials: Conductance value:
Disorders of the Meridians
Yin 3 bacterial 2 dist. excretion 5 acute 8
Yang 6 heavy metal 9 Interstitial cell tissue 7 chron. 10
Viral 1 chemical 4 Degen. cells 11Cave: additional SA
Disorders of the Meridians
F E M WA WO
FIRE EARTH METAL WATER WOOD
WA hormones Stomach Large intestine Urinary system Large joints
M hormones Spleen Lung Kidney Small joints
Small intestine Pancreas Bronchi Female genital Liver
Circulation Metabolism Skin Male genital Bile tracts
Heart Brain Connective tissue Lymph Fatty tissue
threefold increase CNS Ligaments Teeth Muscles
Sensory organs Tendons Paranasal sinuses Spine
Organdegen. Allerg. reaction
Steam. Fire Steam. Earth Steam. Metal Steam. Water Steam. Wood
Parasites and Environmental Exposure
Amoebas Parasites 3 Worms 1 Ticks Earth radiation PCB (skin) (general)
Tapeworms Parasites 4 Worms 2 Formaldehyde PCP (liver) (bladder/kidneys)
Leeches Parasites 5 Worms 3 Anti-parasites A Radio waves Radar waves (lungs) (blood)
Fleas Parasites 6 Worms 4 acute exposure B Fungicide Radioactivity (muscle) (intestine)
Helminths Parasites 7 Worms 5 chron. exposure C Hexachloroben. X-rays (CNS) (tissues)
Lice Protozoa Worms Insecticides UV-light
(skin)
Leishmania Schistosoma Worms 7 Excretion gen. 8 Cortisone Smog (lungs)
Mites Biting houseflies/gadflies Worms 8 Barbiturates Mineral fibres General anaesthetic (lymph)
Parasites 1 Taeniidae Worms Local anaesthesia Nitrate Water veins (sensory organs)
Parasites 2 Trichomonads Worms 10
(CNS)
Electrosmof Ozone Against external factors

Laboratory Findings of Patient S. B.
Page 33
12.2.4 Follow-Up Medical History (Vaccines/Metals) - Blood Laboratory Biochemical Screening
FOLLOW-UP MEDICAL HISTORY
Patient Name Date: 24 April 2003 Initials: Conductance value:
Orthopaedic Condition
CSD TSD LSD Muscle stabilisation 1
C1 TH1 TH7 L1 Muscles Ligament stabilisation 2
C2 TH2 TH8 L2 Ligaments Tendon stabilisation 3
C3 TH3 TH9 L3 Tendons Joint stabilisation 4
C4 TH4 TH10 L4 Small joints
C5 TH5 TH11 L5 Large joints
C6 TH6 TH12 Bones
C7 Bone stabilisation 5
Spine gen.
stabilisation Iliosacral/hip Bone fractures 6
CSD st. TSD st. LSD stabilisation
Vaccines/Metals
Diphtheria vacc. Pertussis vacc. Rubella vacc. Vaccine excretion 1 Aluminium Silver
Diphtheria
pathogen Pertussis pathogen Rubella pathogen Vaccination damage
collection 2 Amalgam Teflon
TBE vaccine Measles vacc. Tetanus vacc. Vaccination complications
3 Lead Preservatives]
TBE pathogen Measles pathogen Tetanus pathogen Tolerance impr. 4 Cadmium Formaldehyde
Yellow fever
vacc. Mumps vacc. Rabies vacc. Complications incr. 5 Gold
Yellow fever
pathogen Mumps pathogen Rabies pathogen Cobalt
Influenza vacc. Smallpox vacc. Tuberculosis vacc. Copper Antibiotics
Influenza
pathogen Smallpox pathogen Tuberculosis
pathogen Nickel The pill
Hepatitis vacc. Polio vacc. Chickenpox vacc. Palladium Ecbolic substances
Hepatitis
pathogen Polio pathogen Chickenpox pathogen Mercury Tocolytic substances
Allergic Exposure
Food chemistry 1 Barley Lectin Horses Fish Nut mix
Bacterial influence 2 Oat Phasin Beef Poultry Sweeteners
Toxins in living spaces Carbohydrates Bee/wasp Sheep Veal Colourings
Viral influence 4 Sweet corn Animal hair gen. Pollen gen. Lamb Wood preserver
Heavy metal exposure 5 Rice Goose feathers House dust Beef Food flavourings
Fungal infection 6 Rye Dogs Hay dust Pork meat Metals
Stress 7 Wheat Insects Milk Pip fruit Detergents
Genetic cause 8 Grain flour Rabbits Lactose int. Stone fruit penicillin
Major allergen 9 Gliadin Cats Egg white Citrus fruits Cold urticaria
Basic foods 10 Gluten Guinea Pigs Chicken eggs Fructose Sun allergy

Laboratory Findings of Patient S. B.
Page 34
12.2.5 Orthomolecular (Vitamins, Etc.) - Blood Laboratory Biochemical Screening
Laboratory E-Screening
Orthomolecular testing
Date:I. 20 MAY 2003 4
2 5
3 Conductance value:
Patient Name: B. S.
Blood Sputum Initials:
Vitamins: 1170 1171 1 2 3 4
Enzymes: 1170 1171 1 2 3 4
Beta-carotene Betaine
Vitamin A Bromelain
Vitamin Bl Coenzyme Q10
Vitamin B2 Lipase
Vitamin B3 Papain
Vitamin B4 Superoxide dismutase (SOD)
Vitamin B5 Nucleic
acids: 1170 1171
Vitamin B6 RNA + DNA
Vitamin B12 Amino acids: 1170 1171
Vitamin Bl5 L-Carnitine
Biotin L-Arginine
Cholin and inositol L-Cysteine
Folic acid L-Glutamine + B6
Vitamin C1 L-Lysine
Vitamin E L-Histidine
Vitamin D DL-Methionine
Vitamin F L-Phenylalanine
Minerals: 1170 1171
Other: 1170 1171
Calcium orotate
Calcium citrate
Chromium GTC
Chromium orotate
Iron chelate
Potassium gluconate
Manganese orotate
Copper
Magnesium citrate
Magnesium orotate
Zinc orotate
Zinc citrate
Silicic acid
Selenium
There are no orthomolecular deficiencies despite the Candidosis, which is very unusual! This indicates very small to no mycelium formation and thus that the mucous membranes of the intestine are intact. The healing of the skin was consequently quick, with relatively simple treatment measures.

Repertorisation - Patient S. B. Page 35
12.2.6 Repertorisation of Homoeopathic Medicines as Concomitant Therapy
Naturopath D. Jakob (25349)
S.B. Neurodermatitis with ongoing respiratory infection
Sum of symptoms (class. by degrees) This analysis includes 388 medications and 7 Symptoms.
Intensity was taken into account
1. Skin - Dry 1 181
2. Skin - Inflammation 1 76 3. Skin - Itching 1 283 4. Skin - Rashes - Redness 1 67 5 Skin - Rashes - Eczema 1 167 6 Skin - Rashes - Children; in - newborns; in 1 2
7. Skin - Rashes - Scratches, after 1 63
1
dulc.
2
sulph.
3
rhus-t.
4
ars.
5
merc.
6
calc.
7
lyc.
8
sil.
9
graph.
10
phos.
11
petr.
12
sep.
13
staph.
14
mez.
15
nit-ac.
16
arn.
17
bry.
18
kali-
s.
19
bell.
20
con.
21
lach.
22
ph-ac.
23
ant-c.
7/15 6/18 6/17 6/15 6/15 6/14 6/14 6/14 6/13 6/13 6/12 6/12 6/12 6/11 6/10 6/9 6/9 6/9 6/8 6/8 6/8 6/8 6/7
1. 3 3 2 3 2 3 3 3 2 3 3 2 2 1 2 2 3 1 3 1 2 2 1
2. 2 2 3 2 3 2 1 3 1 1 1 1 2 1 2 2 1 2 1 1 1 1 1
3. 2 3 3 3 3 2 3 3 3 2 2 3 3 3 2 1 2 2 1 2 2 2 2
4. 2 3 2 2 3 2 1 1 2 3 1 1 1 2 2 2 1 1 1 1 1 1 1
5. 3 4 4 3 2 3 3 2 4 3 3 3 2 3 1 1 1 2 1 2 1 1 1
6. 1 - - - - - - - - - - - - - - - - - - - - - -
7. 2 3 3 2 2 2 3 2 1 1 2 2 2 1 1 1 1 1 1 1 1 1
16 April 2003

Repertorisation - Patient S. B. Page 36
12.2.7 Repertorisation of Homoeopathic Medicines as Concomitant Therapy Naturopath D. Jakob (25349) B S Neurodermatitis Sum of symptoms (class. by degrees) This analysis includes 35 medications and 5 Symptoms. Intensity was taken into account
1. Skin - Rashes - Eczema - itching 1 4
2. Skin - Rashes - Eczema - dry - Children; in 3 1
3. Skin - Rashes - copper coloured 1 24
4. Skin - Rashes - rough 1 5
5. Skin - Rashes - grainy 3 7
1
phos.
2 hep.
3 rhus-t.
4 am-c.
5 calc-s.
6 graph.
7 nat-m.
8 zinc.
9 falco-pe.
10 ars.
11 mez.
12 alum.
13 carb-an.
14 ars-i.
15 calc.
16 kali-i.
17 kreos.
18 lyc.
19 merc.
20 nit-ac.
4/4 3/6 3/4 3/3 3/3 3/3 3/3 3/3 3/3 2/3 2/3 2/2 1/3 1/2 1/2 1/2 1/2 1/2 1/2 1/2
1. - - 1 - - - - - - 1 1 - - - _ - - - -
2. - - - - 1 - - - - - - - - - - - - - - -
3. 1 - 2 _ _ - - - - 2 2 1 3 2 2 2 2 2 2 2
4. - - 1 - - - - - - - - 1 - - - - - - - -
5. 1 2 - 1 - 1 1 1 1 - - - - - - - - - - -
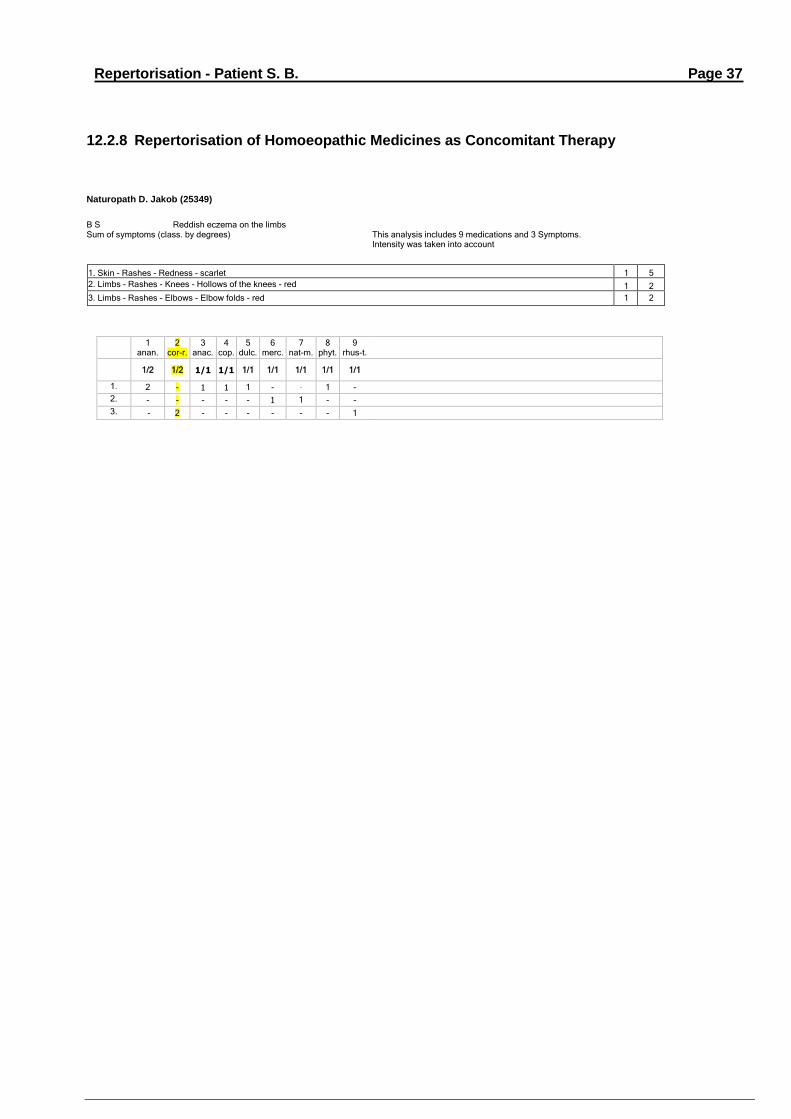
Repertorisation - Patient S. B. Page 37
12.2.8 Repertorisation of Homoeopathic Medicines as Concomitant Therapy Naturopath D. Jakob (25349)
B S Reddish eczema on the limbs Sum of symptoms (class. by degrees) This analysis includes 9 medications and 3 Symptoms. Intensity was taken into account
1. Skin - Rashes - Redness - scarlet 1 5
2. Limbs - Rashes - Knees - Hollows of the knees - red 1 2
3. Limbs - Rashes - Elbows - Elbow folds - red 1 2
1 anan.
2 cor-r.
3 anac.
4 cop.
5 dulc.
6 merc.
7 nat-m.
8 phyt.
9 rhus-t.
1/2 1/2 1/1 1/1 1/1 1/1 1/1 1/1 1/1
1. 2 - 1 1 1 - - 1 -
2. - - - - - 1 1 - -
3. - 2 - - - - - - 1
2. Case Study - Patient I. M.
Page 38
13 Second Case Study
Naturopath D. Jakob Patient: I. M., 1 year old, male Date
of birth: 27 November 2001 Treatment period: from 20 August '02 to 04 April '03
Diagnostic Findings From Blood Work, Clinical Anamnesis and Stool Culture: Full-blown atopic eczema (neurodermatitis) Pre-natal heavy metal intoxication Peri-natal intestinal Candidosis with Candida albicans +++ Pre-existing coeliac disease
Medical History: About 3 months after birth, appearance of a nappy rash and cradle cap. A weeping eczema also formed on the face and spread to the thoracic region and limbs. Severe redness, scabbed, oozing and covered with pustules. Visible scratch marks on all affected body areas. The boy is currently still being nursed. Appears lymphatic and bloated, the remaining skin looks reddish-blue and shimmery. Medication until now: cortisone cream. Stool: daily, very mushy, greenish-yellow, appearance similar to scrambled eggs.
Drinking: still nursed.
Familial Predisposition: Child's mother, existing pollinosis dating back years and food allergy. Child's father, existing pollinosis
Laboratory Findings/Samples: Stool culture, Biochemical screening with blood drops on cellulose swabs (ITT, CTT).
Therapy: Start of therapy with gamma-Linolenic acids (evening primrose Epogam 1000 units) daily 2x1 capsules. Test excretory capacity. Concomitant introduction of BICOM treatment with the programs: - Basic programme with conductance value 125 (tested again at each session) - Follow-up programmes 198/997/998/997 - Additional programmes 565/960/561/447/910/143/999 Introduction of Candida treatment with sugar and yeast restriction Treatment of bacteria, parasites and mycoses with frequency specific microcurrent therapy
Medication: Homoeopathic agents, rose cream, bath milk, mercurialis ointment, Mycostatin 24 ml and Epogam 1000
Treatment Rhythm At 14-day intervals
Outcome: After eight treatments completed at the medical practice with BRT, FSMT and medication, the patient was extensively symptom-free. After relief was given to the coeliac condition, a spontaneous healing reaction occurred on the skin. Occasionally, the consumption of certain foods still leads to small areas of skin reddening.
Overleaf: Pictures of the state of the skin before, during and after treatment. Copies of blood and stool laboratory examinations and corresponding follow-ups. Copies from extern. Laboratory Viollier for coeliac disease follow-up

2. Case Study - Patient I. M.
Page 39
13.1 Course of Treatment for Patient I. M.
Figure 16:
Figure 17:
Figure 18:
Patient aged 3 months with visible severe cradle cap and incipient inflammatory atopic eczema (neurodermatitis).
Existing Clinical Status: Nappy rash, peri-natal intestinal candidosis and parasite infection. Severe mercury intoxication Lymphatic constitution (edema) DD: Coeliac disease. Since the patient is still being breastfed, already existing food reactions occurred (family diathesis through the mother).
The patient is now suffering from an acutely inflamed, weeping atopic eczema at the described and visible affected areas over the whole body, as an "atypical" form. The skin on the face and chest is at this stage covered in purulent pustules (bact. infection through intense scratching).
Due to the already significant weakening of the intestine (candida and coelica disease), an increasing weakness of the immune system followed. In this case, gamma-Linolenic acids did not give immediate relief. This occurred only after the coeliac disease was treated with BRT and homoeopathic medicines.
Patient is now 2 years of age; the state of the skin is very good.
Despite the intense therapy over 8 months, the patient still occasionally displays reactions to certain foods, which cause reddening in the hollow of the knees or, with consumption of sausage products, pustules. Milk products sometimes still cause vomiting. A possible explanation resides in the severe intestinal stress due to candidosis and concomitant coeliac disease. The patient was treated again for these reactions with BRT.

2. Case Study - Patient I. M.
Page 40
13.1 The Diagnosis of Coeliac Disease The differential diagnosis of coeliac disease was confirmed, in accordance with the examinations carried out on blood and stool. At the same time, in this patient there is a very high familial predisposition to food allergies due to the mother; only general causes were recorded for the father. The treatment of coeliac disease, on its own, required several tests in order to cover all foods, food additives and other causes, since allergic components often have an underlying reaction which can only be recognized with different analyses. After the treatment was completed, there are still occasional allergic reactions to foods, which could not be identified in the therapy.
The complex clinical and anamnestic picture due to candidosis, atopic eczema and coeliac disease is in itself sufficient to explain the complex laboratory analyses. There was also a severe mercury intoxication.
The two case studies very clearly show the difference between a localized atopic eczema in the hollow of the knees and elbow folds without allergic predisposition and an eczema affecting the entire body with oozing and scaling, along with allergic predisposition. As practically the entire body of the patient in the second case study was affected, the treatment took on a very complex form. Gamma-Linolenic acids, which were applied as basic treatment for all patients, did not help at all in this case. Only after the second BRT session was the patient ready for the concomitant therapy with medication.
Subsequently, a different progression of the severity of the clinical picture showed itself also between the two patients with the same condition. The problem of reactions, which we experienced also in other cases which had undergone previous treatment with a steroid, emerged very clearly in this case due to the additional presence of coeliac disease. In the second case, with known atopy and eczema and candidosis in the intestine, the more distinct form appeared, with involvement of the sub-dermal structure due to high reinfection of the wounded skin and to the severely weakened defences with the additional sickness in the intestine (the intestine accounts for about 70% of the immune system). The recognition of the role of the intestine for the immune system clearly illustrates, with the examinations of the stool carried out in the study, that the peri-natal weakening of the intestinal mucosa, significantly impairs the immune system, which anyhow is not yet fully developed, and how important it is for the mucosa to be and remain intact and functioning.
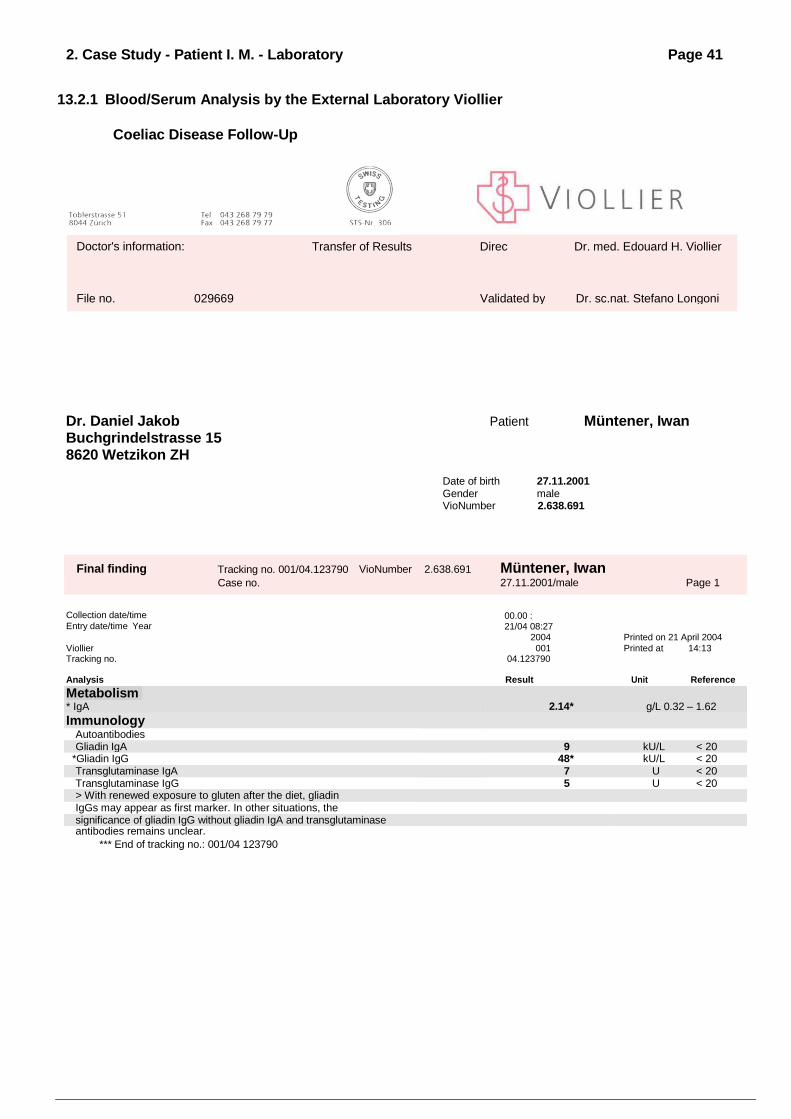
2. Case Study - Patient I. M. - Laboratory Findings
Page 41
13.2.1 Blood/Serum Analysis by the External Laboratory Viollier
Coeliac Disease Follow-Up
Dr. Daniel Jakob Patient Müntener, Iwan
Buchgrindelstrasse 15 8620 Wetzikon ZH
Date of birth 27.11.2001 Gender male VioNumber 2.638.691
Final finding Tracking no. 001/04.123790
Case no.
VioNumber 2.638.691 Müntener, Iwan 27.11.2001/male Page 1
Collection date/time
Entry date/time Year
00.00 :21/04 08:27
2004
Printed on 21 April 2004
Viollier 001 Printed at 14:13 Tracking no. 04.123790 Analysis Result Unit Reference
Metabolism * IgA
2.14*
g/L 0.32 – 1.62
Immunology Autoantibodies Gliadin IgA 9 kU/L < 20
*Gliadin IgG 48* kU/L < 20 Transglutaminase IgA 7 U < 20 Transglutaminase IgG 5 U < 20 > With renewed exposure to gluten after the diet, gliadin IgGs may appear as first marker. In other situations, the significance of gliadin IgG without gliadin IgA and transglutaminase antibodies remains unclear.
*** End of tracking no.: 001/04 123790
Doctor's information: Transfer of Results Director
Dr. med. Edouard H. Viollier
File no. 029669 Validated by Dr. sc.nat. Stefano Longoni

2. Case Study - Patient I. M. - Laboratory Findings
Page 42
13.2.2 Scatology (Stool Culture) - Stool Laboratory Biochemical Screening
Laboratory E-Screening
Scatology/Stool Culture: Bacteria/Parasites/Fungi
Date: 1 20 AUG. 2002 4 Initials:
2 16 SEP 2002 Initials: 5 Initials:
3 Initials: Conductance value:
Patient Name: I.M.
Anal swab Stool sample
Initials:
Moulds: 1170 1171
1 2 3 4 5 Protozoa: 1170
1171 1 2 3 4 5
Mould Mix 1: Entamoeba histolytica
Mould Mix 2: Lamblia intestinalis
Mould Mix 3: +3 trichomonads
Cladosporium cladosporioides Bacteria 1170 1171
Smut Mix Campylobacter coli
Geotrichum candida Campylobacter pylori
Parasites: 1171 1171 Dyspesia coli +2
1 Ancylostoma canimim 386/400 +3 Enterobacter
2 Ascaris lumbricoides 408 Enterococcus
3 Ascaris lumbricoides larvae 408 Escherichia coli
4 Borrelia burgdorferi 380 Proteus
5 Clonorchis sinensis adult 414 Salmonella TP
6 Clonorchis sinensis eggs 427 Salmonella D
7 Dirofilaria 409 Serratia
8 Echinococcus granulosus hydatid 461.50 Candida: 1170 1171
9 Echinococcus granulosus eggs 446.50 Albicans +3
10 Echinococcus multilocularis 458.35 Parapsil +3
11 Entamoeba coli histolytica Tropoz 385 crusei +3
12 Eurytrema pancreaticum 421 Mites: 1170 1171
13 Fasciola hepatica adult 427 Flour Mites
14 Fasciola hepatica eggs 425 Food Mites 1
15 Fasciola hepatica cercaria 427 +3 Food Mites 2
16 Fasciola buski adult 434 Worms: 1170 1171
17 Fasciola buskii eggs 434 +3 Ascaris lumbricoides
18 Gardia cysticercus 364.80 Oxyuris vermicularis
19 Gardia trio 424 Taenia saginata
20 Haemoproteus 393 +3 Coeliac
disease: 192 191
21 Naegleria fowleri 362 +3 Cereal flour
22 Onchocerca volvulus 440 Gluten
23 Proteus vulgaris 374.80 +2 Gliadin +3
24 Pneumocysticus carinii 407 Miscellaneous
:
25 Schistosoma japonicum 473
26 Schistosoma mansoni 353
27 Schistosoma japonicum in copula 473
28 Strongyloides stercoralis 400
29 Taenia pisiformis cysticercus 480
30 Taenia pisiformis eggs 468 +3
31 Taenia pisiformis cysticercus 475 +2
32 Taenia solium solex 448
33 Toxoplasma gondii 389.60
34 Toxoplasma humanpath. Strain 395
35 Trichinella spiralis 404.50
36 Trichomonas vaginalis 381
37 Trypanosoma cruzi 463

2. Case Study - Patient I. M. - Laboratory Findings
Page 43
13.2.3 Foods/Luxury Foods - Blood Laboratory Biochemical Screening
Laboratory E-Screening
Basic test: Foods/Luxury Foods
Date: 1 23 AUG. 2002 4 04 APR 2003 Initials:
2 12 SEP 2002 Initials: 5. Initials:
3. 20. NOV 2002 Initials: Conductance value:
Patient Name: I.M. Swab Blood Stool Initials:
Seasoning: 1191 192 Fish: 191 192
Mustard Fish Mix 1: +2
Pepper Fish Mix 2:
Cloves Herring
Salt Cod
Paprika Salmon
Cayenne Mackerel
Plaice +3
Vegetables: 191 1192 Cereals: 191 192
Vegetable mix +3 Buckwheat
Beans Spelt +3
Carrots Barley
Spinach Oat
Tomatoes Millet
Onion +2 Sweet corn
Paprika Rice
Chives Rye
Luxury Foods 191 192 Sesame
Honey Wheat +3
Coffee Gliadin +3
Cocoa Yeast +3
Alcohol Soy
Tea Fruit 191 192
Sugar Apple +3
Chocolate Apricot
Nuts 191 192 Banana +3
Peanut Pear
Hazelnut Strawberry
Almonds Grapefruit
Walnut +3 Raspberry
Sunflower seeds Currant
Cashew nuts Cherry
Pumpkin seeds Orange +3
Linseed Peach
Milk 191 1192 Gooseberry
Cow's milk Grape
Milk sugar +3 Lemon
Cream +3 Nectarine
Butter +3 Pineapple
Egg 191 192 Meat 191 192
Egg yolk Pork +3
Egg white +3 Veal +3
Special
Foods 191 192 Mutton/Lamb +3
Chicken
Beef

2. Case Study - Patient I. M. - Laboratory Findings
Page 44
13.2.4 Food Additives/Preservatives - Blood Laboratory Biochemical Screening
Laboratory E-Screening
Food Additives/Preservatives
Date: 1 23 AUG. 2002 4 Initials:
2 12 SEP 2002 Initials: 5 Initials:
3 Initials: Conductance value:
Patient Name: I.M. Blood Serum Initials:
Colourings: 1170 11171 1 2 3 4 5 Antioxidants:17
1
1170 11171 1 2 3 4 5 E102 Tartrazine +3 E 310 Propyl gallate
E104 Quinoline yellow E 312 Dodecyl gallate
E 1 10 Orange yellow S E 320 Butylated hydroxyanisole (BHA) +2
E 120 Carmine +3 E32I Butylated hydroxytoluene (BHT)
E 122 Azorubine Ethoxyquin
E 123 Amaranth +3 Flavourings: 1170 11171
E 124 Cochineal Red A Apple aroma
E 127 Erythrosine Apricot aroma
E132 Indigotine +3 Banana aroma
E 133 Brilliant Blue FCF +3 Pear aroma
E 151 Brilliant Black BN Coca-Cola aroma
Yellow mix (E104/EI10/E124) +3 Strawberry aroma
Red mix (E124/E132) Eugenol
Brown mix (E104/E124/E127/E132) Raspberry aroma
Preservatives: 1170 11171 Cherry aroma
E 200 Sorbic acid Herbal aroma +3
E 202 Potassium sorbate +3 Orange aroma
E 210 Benzoic acid Rhum aroma
E 211 Sodium benzoate +3 Vanilla aroma
E 212 Potassium benzoate Vanillin
E 214 Ethylparaben Cinnamaldehyde
E 216 Propylparaben +3 Lemon aroma
E 218 Methylparaben Sweeteners: 1170 11171
Kathon - CG (=Euxyl) Aspartame
E 220 Sulfur dioxide Cyclamate
E 221 Sodium sulfite Saccharin-N
E 223 Sodium metabisulfite Fructose - +2
E 224 Potassium metabisulfite Lactose
E 230 Biphenyl Mannitol
E 233 Thiabendazole Sorbitol
E 249 Potassium nitrite +2 Other: 1170 11171
E 250 Sodium nitrite Acetylsalicylic acid
E 251 Sodium nitrate +2 Quinine
E 252 Potassium nitrate Arabic gum
Emulsifiers 1170 11171 Sodium fluoride
E 322 Lecithin S (soya) Phenol
E322 Lecithin D (egg yolk) Procain
E 338 Phosphoric acid Salicylic acid
E 339 b Disodium phosphate Sulfadiazine
E 340 a Monopotassium phosphate Sulfaguanidine
E 340 b Dipotassium phosphate Tartaric acid
E 340 c Tripotassium phosphate Citric acid +2
E341 c Tripotassium phosphate
E 412 Guar
E 450 Monosodium phosphate
E 450 a Trisodium diphosphate
E 450 c Sodium polyphosphate
E62I Monosodium glutamate +1
E 622 Monopotassium glutamate +2
E 623 Calcium glutamate +3

2. Case Study - Patient I. M. - Laboratory Findings
Page 45
13.2.5 Orthomolecular (Vitamins, Etc.) - Blood Laboratory Biochemical Screening
Laboratory E-Screening
Orthomolecular testing
Date: 1 23 AUG. 2002 4
2 12 SEP 2002 5
3 Conductance value:
Patient Name: I.M. Blood Sputum Initials:
Vitamins: 1170 1171 1 2 3 4 Enzymes: 1170 1171 1 2 3 4
Beta-carotene Betaine
Vitamin A Bromelain
Vitamin Bl +2 Coenzyme Q10
Vitamin B2 Lipase
Vitamin B3 Papain
Vitamin B4 Superoxide dismutase (SOD)
Vitamin B5 Nucleic acids: 1170 1171
Vitamin B6 +2 RNA + DNA
Vitamin B12 Amino acids: 1170 1171
Vitamin B15 +3 L-Carnitine
Biotin L-Arginine
Cholin and inositol L-Cysteine
Folic acid L-Glutamine + B6
Vitamin C1 L-Lysine
Vitamin E +3 L-Histidine
Vitamin D DL-Methionine
Vitamin F L-Phenylalanine
Minerals: 1170 1171 Other: 1170 1171
Calcium orotate +2
Calcium citrate
Chromium GTC
Chromium orotate
Iron chelate +3
Potassium gluconate
Manganese orotate
Copper
Magnesium citrate
Magnesium orotate
Zinc orotate +2
Zinc citrate
Silicic acid +3
Selenium

2. Case Study - Patient I. M. - Laboratory Findings
Page 46
13.2.6 Investigation into Primary Causes - Blood Laboratory Biochemical Screening
Laboratory E-
Screening
Investigation into Primary Causes
1 Date: 20 AUG. 2002 4 Initials:
2 04 APR 2003 Initials: Date prior to
treatment: Date prior to
treatment:
3 Initials: 20 AUG. 2002 04 APR 2003
Patient Name: I.M. Swab Stool Chewing Gum Test Blood Sputum Initials:
A01 Arsenicum album D200 Virus Virus infection* chron +2
A02 Natrium sulfuricum D60 Bacterial infection*
A03 Monilia albicans D30 Fungi infection
A04 Indican D30 Idolum Small intestine dysbiosis
A05 Scotalum D30 Scatolum Large intestine dysbiosis +3
A06 Fungus 1 Allergen D30 Fungi infection*
A07 Fungus 2 Allergen D30 Fungi infection* chron. +3
A08 Mycosis Oris D30 Fungal infection of the mouth*
A09 Silicea D60 Geopathic exposure
A1O Phosphorus D60 Electromagnetic exposure
All Dioxine Sdf. D30 Dioxin exposure
A12 PCB D30 PCP exposure
A13 Histaminum dihydrochl. D60 Allergic exposure (non-food) +3
A14 Causticum H. D30 Food intolerance, pseudo-allergy +3
A15 Serotonin-creatinine-sulfate (If Causticum D30 is positive, sometimes also individually)
A16 Mercurius solub. H. D30 Gen. mercury exposure +3
BO1 Silver amalgam D30 Exposure to Gamma-2-Amalgam +2
B02 Non-Gamma-2-Amalgam D30 Exposure to Non-Gamma-2-Amalgam
B03 Palladium metallicum D30 Palladium exposure
B04 Conium D30 Benign tumours of all kinds*
B05 Rhus toxicodendron D60 Cysts*
B06 Psorinum Nos. D30 Premalignant*
B07 Carcinominum deg.-Nos D60 Precancerous*
B08 Carcinominum deg.-Nos D30 Cancerous*
B09 Erythrocytes Gl D6 Erythrocytes anomaly
B1O Lymphocytes Gl D6 Lymphocytes anomaly
B11 Granulocytes Gl D6 Granulocytes anomaly
B12 Thrombocytes Gl D6 Thrombocytes anomaly
B13 Cholesterinum D60 Individually elevated cholesterol levels
B14 Acidum uricum D60 Individually elevated uric acid levels
B15 Chromium met. D2000 Filter ampoules
B16 Zinkuni metallicum D60 Filter ampoules
Ampoules marked with a cross must be placed in the cubicle with the filter ampoule. If the measured value lies below 50 (+2= yellow mark),
the situation is primarily chronic
If the measured value is significantly higher, then there is an acute situation.

2. Case Study - Patient I. M. - Laboratory Findings
Page 47
13.2.7 Viruses/Bacteria/Fungi/Animal Skin Cells - Blood Laboratory Biochemical Skin
Laboratory E-
Screening
Viruses/Bacteria/Fungi/Animal Skin
Cell
1 Date: 20 AUG. 2002 4 Initials:
2 16 SEP 2002 Initials: 5 Initials:
3 Initials: Conductance value:
Patient Name: I.M. Urine Biopsy Swab Sputum Blood Stool Initials:
Bacteria: 1170 1171 1 2 3 4 5 Viruses: 1170 1171 1 2 3 4 5
Actinobactcr actinomycclicans Nos. Verruca vulgaris Nos.
Actinomyccs israelii Nos. Condylomata acuminata Nos.
Aerobacter aerogenes Nos. Adeno 12 Virus Type Nos.
Aerovbactcr cum coli Nos. Adenoviren Nos.
Bacillus cereus Nos. Herpes simplex Nos.
Bacillus thuringensis Nos. Herpes virus Type 6 Nos.
Bacillus acidophilus Nos. Varicella Zoster +2
Bacterium coli Nos. Herpes zoster
Bacterium dysentcriae Nos. C'ytomegalie Nos.
Bacterium faecalis alkaligencs Nos. Epstein-Barr Nos.
Bacterium Gacrtncr Nos. Infectious mononucleosis Nos.
Bacterium Morgan Nos. Variola Nos.
Bacterium proteus Nos. Hepatitis Nos.
Bacterium pyocyaneus Nos. Hepatitis A Nos.
Bacterium subtilis Nos. Hepatitis B Nos.
Baeteroides Nos Hepatitis B with EB-Virus Nos.
Bang Nos. Hepatitis C Nos.
BCG. Nos. Hepatitis Non A non B
Borrelia burgdorferi Nos. Coxsackie A2
Branhamella catarrhalis Nos. Coxsackie A3
Brucella meliense Nos Coxsackie A4
Clostridium botulinum Nos. Coxsackie A7
Campylobacter Nos. Coxsackie Bl
Campylobacter pylori Nos. Coxsackie B2
Chlamydia trachomatis Nos. Coxsackie B3
Cholera Virbro Nos. Coxsackie B4
Clostridium difflcile Nos Coxsackie B5
Corynebacterium diphtheria Nos. Coxsackie B6
Enterococcinum Nos. Poliomy elitis Nos.
Erysipelas suum Nos. Sterp faecalis Rhinotracheitis bovinum Nos.
Escherichia verotoxinbildend Nos. Rotaviruses
Ciardncrella vaginalis Nos. üistempermum Nos. Paramyxoviruses
Haemophilus influenzae Nos. Morbillium Nos. Paramyxoviruses
Haemophilus influenzae Serotype B Parotitis Nos. Paramyxoviruses
Catarrhal mixed flora nos. Newcastle disease Virus Nos. Myxoviruses
klebsilla pneumoniae Nos. RSV-Virus Parainfluenza Viruses
Leeionella pneumoniae Nos. Lyssinum Nos.
Leptospirosis p.c.gt. W. Nos. Rubeolae Nos. Togaviridae
Leptospirosis Dengue fever Nos.
Listeriose Nos. TBE Tick-borne encephalitis
Meningococcinum Nos. Erythema infecta acuta Nos Parvoviruses
Mycoplasma pneumoniae Nos.
Nocardia astcroides Nos. Moulds: 1170 1171
Ornithose Nos. Chlamydia psittaci Mould Mix 1:
Pasteurelia multocida Mould Mix 2:
Petostreptococcus anaerobius Mould Mix 3:
Pertussinum Nos.
Pneumococcinum Nos.
Q fever rickettsia burnetii
Rickettsia prowazeki Nos. Dermatophytes 1170 1171
Salmonella TP typhi et paratyphi Trichophytum rubum
Salmonella typhimurium Enteritis infectosa Trichophy tum montagor
Salmonella virchow Nos. Microsporiuni canis
Sarcina ventriculi Nos. Malassezia lurcher
Scarlatinum Nos. Scarlet streptococci Other path. Substances: 1170 1171
Staphylococcinum Nos.
Staphy lococcus aureus Nos.
Staphylostreptococcinum Nos.
Streptococcus viridens
Streptococcus py rogenes
Streptococcinum Nos.
Streptococcus haemolyticus Nos.
Strong Nos. Shigella flexneri
Tetanus Nos. Clostridium tetani
Tuberculinum Mycobacterium tuberculosis Nos.
Tuberculinum avis Nos.
Tuberculinum bovinum Nos.
Ureaplasma urealytica Nos.
Yersinia enterocolitica Nos.
Rickettsia sp. Tick bite fever

2. Case Study - Patient I. M. - Laboratory Findings Page 48
13.2.8 Fundamental Medical History (5 Elements) - Blood Laboratory Biochemical Screening
FUNDAMENTAL MEDICAL HISTORY
Patient Name: Date: 17 SEP 2002: Pat.No. 694:
Basic Physical Contaminations
Geopathy Electrosmog Radioactivity
Focal Toxicosis
Organ nosodes Illness nosodes Scars
Immunology
Bacteria Fungi Viruses
Protozoa Parasites Vaccines
Toxicology
Home Industrial Medication
Environment Poisons Dental materials
Allergies
Foods Contact allergies Allergens
Food additives Metals Medication
Elements
Fire Water Viral Chemical Interstitial cell tissue
Earth Wood Bacterial excretion 5 Acute
Metal Yin/Yang Heavy metal Degen. Cells chron.
Disorders of the Meridians
FIRE EARTH METAL WATER WOOD
WA hormones Stomach Large intestine Urinary system Large joints
M hormones Spleen Lung Kidney Small joints
Small intestine Pancreas Bronchi Female genital Liver
Circulation Metabolism Skin Male genital Bile tracts
Heart Brain Connective tissue Lymph Fatty tissue
threefold increase CNS Ligaments Teeth Muscles
Degenerated cells Sensory organs Tendons Paranasal sinuses Spine
Organdegen. Allerg. reaction
Steam. Fire Steam. Earth Steam. Metal Steam. Water Steam. Wood

2. Case Study - Patient I. M. - Laboratory Findings Page 49
13.2.9 Follow-Up Medical History (Vaccines/Metals etc-) - Blood Laboratory Biochemical Screening
FOLLOW-UP MEDICAL HISTORY
Patient Name: I.M. 27.11.01 Date: 17 SEP 2002 Pat.No. 694
Orthopaedic Condition
CSD TSD LSD Muscle stabilisation
C1 TH1 TH7 L1 Muscles Ligament stabilisation
C2 TH2 TH8 L2 Ligaments Tendon stabilisation
C3 TH3 TH9 L3 Tendons Joint stabilisation
C4 TH4 TH10 L4 Small joints
C5 TH5 TH11 L5 Large joints
C6 TH6 TH12 Bones
C7 Bone stabilisation
Spine gen.
stabilisation Iliosacral/hip Bone fractures
CSD st. CSD st. LSD stabilisation
Vaccines/Metals
Diphtheria vacc. Pertussis vacc. Rubella vacc. Vaccine excretion Aluminium o + Silver o
Diphtheria pathogen Pertussis pathogen Rubella pathogen Vaccination damage collection 2 Amalgam Teflon
TBE vaccine Measles vacc. Tetanus vacc. Vaccination complications Lead Preservatives
TBE pathogen Measles pathogen Tetanus pathogen Tolerance impr. Cadmium Formaldehyde
Yellow fever vacc. Mumps vacc. Rabies vacc. Complications incr. o+ Gold
Yellow fever pathogen Mumps pathogen Rabies pathogen Cobalt
Influenza vacc. Smallpox vacc. Tuberculosis vacc. Copper Antibiotics +
Influenza pathogen Smallpox pathogen Tuberculosis
pathogen Nickel The pill
Hepatitis vacc. Polio vacc. Chickenpox vacc. Palladium Ecbolic substances
Hepatitis pathogen Polio pathogen Chickenpox pathogen Mercury Tocolytic substances
Allergic Exposure
Food chemistry Barley Lectin Horses Fish Nut mix
Bacterial influence Oat Phasin Beef Poultry Sweeteners
Toxins in living spaces Carbohydrates Bee/wasp Sheep Veal Colourings
Viral influence Sweet corn Animal hair gen. Pollen gen. Lamb Wood preserver
Heavy metal exposure Rice Goose feathers House dust Beef Food flavourings
Fungal infection Rye Dogs Hay dust Pork meat Metals
Stress Wheat Insects Milk Pip fruit Detergents
Genetic Cause + Grain Flour o Rabbits Lactose int. Stone fruit penicillin
Major allergen Gliadin + Cats Egg white Citrus fruits Cold urticaria
Basic foods Gluten Guinea Pigs Chicken eggs Fructose Sun allergy

2 Case Study - Patient I. M. - Laboratory Findings Page 50
13.2.10 Special Medical History (Degenerated Cells) - Blood Laboratory Biochemical Screening
Special Medical History
Patient Name: I.M. Date: 17 SEP 2002 Pat.No. 694
Degenerated cells
Preliminary stage Healthy tissue preliminary
stage Prevent ascites Immune system stabilisation Adenomata
Degeneration Healthy tissue Degeneration Immune Deficiency Killer cells Atheromata
Diversification Healthy tissue Diversification Channel chemother. Prevent neoplasia Fibromata
Degeneration 1 (blood) Degeneration 8
(gonadoblastoma)
Degeneration 15
(kidneys) Intestine improvement Psyche stabilisation Lipomata
Degeneration 2 (breast) Degeneration 9 (skin) Degeneration 16 (rectum) DNA stabilisation RNA stabilisation Lymphogra.
Degeneration 3 (large intestine)|
Degeneration 10 (bladder) Degeneration 17 (stomach)
Free radicals bind. Radiother. Excr. Melanomata
Degeneration 4 (small intestine) o
Degeneration 11 (liver) Degeneration 18 (pancreas)
Genetic Defect o Thrombosis prep. Myomata
Degeneration 5 (glands) Degeneration 12 (leukaemia) Degeneration 19
(prostate) Promote healing o Cell stabilisation Polyps
Degeneration 6 (Ganglion) Degeneration 13 (lungs) Degeneration 20 (uterus) Hormone balance Cysts
Degeneration 7 (brain) Degeneration 14 (lymph) Degeneration 21 (spleen) Channel hormonal ther.

2. Case Study - Patient I. M. - Laboratory Findings
Page 51
13.2.11 Blood Laboratory Biochemical Screening
Fundamental Medical History (5 Elements 1st Follow-Up)
FUNDAMENTAL MEDICAL HISTORY
Patient Name: I.M. Date: 1 OCT 2002: Pat.No. 694:
Basic Physical Exposure
Geopathy Electrosmog Radioactivity
Focal Toxicosis
Organ nosodes Illness nosodes Scars
Immunology
Bacteria Fungi Viruses
Protozoa Parasites Vaccines
Toxicology
Home Industrial Medication
Environment Poisons Dental materials
Allergies
Foods Contact allergies Allergens
Food additives Metals Medication
Elements
Viral 1 Chemical 4 Interstitial cell tissue 7
Bacterial 2 excretion 5 acute 8 chron 10
Yin 3 Yang 6 heavy metal 9 Degen. Cells 11 .
Disorders of the Meridians
F E M WA WO
FIRE EARTH METAL WATER H WOOD
WA hormones Stomach Large intestine Urinary system Large joints
M hormones Spleen Lung Kidney Small joints
Small intestine Pancreas Bronchi Female genital Liver
Circulation Metabolism Skin Male genital Bile tracts
Heart Brain Connective tissue Lymph Fatty tissue
threefold increase CNS Ligaments Teeth Muscles
Sensory organs Tendons Paranasal sinuses Spine
Organdegen. Allerg. reaction 2.9.7
4.10.11
Steam. Fire Steam. Earth Steam. Metal Steam. Water Steam. Wood

2. Case Study - Patient I. M. - Laboratory Findings
Page 52
13.2.12 Blood Laboratory Biochemical Screening Follow-Up Medical History (1st Follow-Up)
FOLLOW-UP MEDICAL HISTORY
Patient Name: I.M. Date: 01 OCT 2002 Pat.No. 694
Orthopaedic Condition
CSD TSD LSD Muscle stabilisation
C1 TH1 TH7 L1 Muscles Ligament stabilisation
C2 TH2 TH8 L2 Ligaments Tendon stabilisation
C3 TH3 TH9 L3 Tendons Joint stabilisation
C4 TH4 TH10 L4 Small joints
C5 TH5 TH11 L5 Large joints
C6 TH6 TH12 Bones
C7 Bone stabilisation
Spine gen.
stabilisation Iliosacral/hip Bone fractures
CSD st. CSD st. LSD stabilisation
Vaccines/Metals
Diphtheria vacc. Pertussis vacc. Rubella vacc. Vaccine excretion 1 Aluminium Silver
Diphtheria pathogen Pertussis pathogen Rubella pathogen Vaccination damage collection 2 Amalgam Teflon
TBE vaccine Measles vacc. Tetanus vacc. Vaccination complications 3 Lead Preservatives
TBE pathogen Measles pathogen Tetanus pathogen Tolerance impr. 4 Cadmium Formaldehyde
Yellow fever vacc. Mumps vacc. Rabies vacc. Complications incr. 5 Gold
Yellow fever pathogen Mumps pathogen Rabies pathogen Cobalt 4
Influenza vacc. Smallpox vacc. Tuberculosis vacc. Copper Antibiotics
Influenza pathogen Smallpox pathogen Tuberculosis pathogen Nickel The pill
Hepatitis vacc. Polio vacc. Chickenpox vacc. Palladium Ecbolic substances
Hepatitis pathogen Polio pathogen Chickenpox pathogen Mercury Tocolytic substances
Allergic Exposure
Food chemistry 1 Barley Lectin Horses Fish Nut mix
Bacterial influence 2 Oat 8 Phasin Beef Poultry Sweeteners
Toxins in living spaces Carbohydrates Bee/wasp Sheep Veal Colourings
Viral influence 4 Sweet corn Animal hair gen. Pollen gen. Lamb Wood preserver
Heavy metal exposure 5 Rice Goose feathers House dust Beef Food flavourings
Fungal infection 6 Rye Dogs Hay dust Pork meat Metals
Stress 7 Wheat Insects Milk Pip fruit Detergents
Genetic cause 8 Grain flour Rabbits Lactose int. Stone fruit Penicillin
Major allergen 9 Gliadin 8.9 Cats Egg white Citrus fruits Cold urticaria
Basic foods 10 Gluten Guinea Pigs Chicken eggs Fructose Sun allergy

2. Case Study - Patient I. M. - Laboratory Findings
Page 53
13.2.13 Blood Laboratory Biochemical Screening Special Medical History (1st Follow-Up)
Special Medical History
Patient Name: I.M. Date: 01 OCT 2002 Pat.No. 694
Degenerated cells
Preliminary stage 1 Healthy tissue preliminary
stage 4 7 Prevent ascites
18 Immune system
stabilisation Adenomata A
Degeneration 2 Healthy tissue Degeneration 5 8 Immune Deficiency 19 Killer cells Atheromata B
Diversification 3 Healthy tissue Diversification
6 9 Channel chemother. 20 Prevent neoplasia Fibromata C
Degeneration 1 (blood) Degeneration 8
(gonadoblastoma)
Degeneration 15
(kidneys) 10 Intestine improvement 21 Psyche stabilisation Lipomata D
Degeneration 2 (breast) Degeneration 9 (skin) Degeneration 16 (rectum) 12 DNA stabilisation 22 DNA stabilisation Lymphogra. E
Degeneration 3 (large
intestine)| Degeneration 10 (bladder)
Degeneration 17
(stomach) 13 Free radicals bind. 23 Radiother. Excr. Melanomata F
Degeneration 4 (small intestine) o
3,5
10,12 Degeneration 11 (liver)
Degeneration 18 (pancreas)
14 Genetic Defect o 24 Thrombosis prep. Myomata G
Degeneration 5 (glands) Degeneration 12 (leukaemia) Degeneration 19
(prostate) 15 Promote healingf o 25 Cell stabilisation Polyps H
Degeneration 6 (Ganglion) Degeneration 13 (lungs) Degeneration 20 (uterus) 16 Hormone balance Cysts I
Degeneration 7 (brain) Degeneration 14 (lymph) Degeneration 21 (spleen) 17 Channel hormonal ther.

2. Case Study - Patient I. M. - Laboratory Findings
Page 54
13.2.14 Blood Laboratory Biochemical Screening Fundamental Medical History (1st Follow-Up)
FUNDAMENTAL MEDICAL HISTORY
Patient Name: I.M. Date: 17 OCT 2002: Pat.No. 694:
Basic Physical Exposure
Geopathy Electrosmog Radioactivity
Focal Toxicosis
Organ nosodes Illness nosodes Scars
Immunology
Bacteria Fungi Viruses
Protozoa Parasites Vaccines
Toxicology
Home Industrial Medication
Environment Poisons Dental materials
Allergies
Foods Contact allergies Allergens
Food additives Metals Medication
Elements
Viral 1 Chemical 4 Interstitial cell tissue 7
Bacterial 2 excretion 5 acute 8 chron 10
Yin 3 Yang 6 heavy metal 9 Degen. Cells 11 .
Disorders of the Meridians
F E M WA WO
FIRE EARTH METAL H WATER WOOD
WA hormones Stomach Large intestine Urinary system Large joints
M hormones Spleen Lung Kidney Small joints
Small intestine Pancreas Bronchi Female genital Liver
Circulation Metabolism Skin Male genital Bile tracts
Heart Brain Connective tissue Lymph Fatty tissue
threefold increase CNS Ligaments Teeth Muscles 18.10.
Sensory organs Tendons 10, 3, 6 Paranasal sinuses Spine
Organdegen. Allerg. reaction
Steam. Fire Steam. Earth Steam. Metal Steam. Water Steam. Wood

2. Case Study - Patient I. M. - Laboratory Findings
Page 55
13.2.15 Blood Laboratory Biochemical Screening Follow-Up Medical History (2nd Follow-Up)
FOLLOW-UP MEDICAL HISTORY
Patient Name: I.M. Date: 17 OCT 2002 Pat.No. 694
Orthopaedic Condition
CSD TSD LSD Muscle stabilisation
C1 TH1 TH7 L1 Muscles Ligament stabilisation
C2 TH2 TH8 L2 Ligaments Tendon stabilisation
C3 TH3 TH9 L3 Tendons Joint stabilisation
C4 TH4 TH10 L4 Small joints
C5 TH5 TH11 L5 Large joints
C6 TH6 TH12 Bones
C7 Bone stabilisation
Spine gen.
stabilisation Iliosacral/hip Bone fractures
CSD st. TSD st. LSD stabilisation
Vaccines/Metals
Diphtheria vacc. Pertussis vacc. Rubella vacc. Vaccine excretion 1 Aluminium Silver
Diphtheria pathogen Pertussis pathogen Rubella pathogen Vaccination damage collection 2 Amalgam Teflon
TBE vaccine Measles vacc. Tetanus vacc. Vaccination complications 3 Lead Preservatives
TBE pathogen Measles pathogen Tetanus pathogen Tolerance impr. 4 Cadmium Formaldehyde
Yellow fever vacc. Mumps vacc. Rabies vacc. Complications incr. 5 Gold ok
Yellow fever pathogen Mumps pathogen Rabies pathogen Cobalt
Influenza vacc. Smallpox vacc. Tuberculosis vacc. Copper Antibiotics
Influenza pathogen Smallpox pathogen Tuberculosis
pathogen Nickel The pill
Hepatitis vacc. Polio vacc. Chickenpox vacc. Palladium Ecbolic substances
Hepatitis pathogen Polio pathogen Chickenpox pathogen Mercury Tocolytic substances
Allergic Exposure
Food chemistry 1 Barley Lectin Horses Fish Nut mix
Bacterial influence 2 Oat Phasin Beef Poultry Sweeteners ok
Toxins in living spaces Carbohydrates Bee/wasp Sheep Veal Colourings
Viral influence 4 Sweet corn Animal hair gen. Pollen gen. Lamb Wood preserver
Heavy metal exposure 5 Rice Goose feathers House dust Beef Food flavourings
Fungal infection 6 Rye Dogs Hay dust Pork meat Metals
Stress 7 Wheat Insects Milk Pip fruit Detergents
Genetic cause 8 Grain flour Rabbits Lactose int. Stone fruit Penicillin
Major allergen 9 Gliadin Cats Egg white Citrus fruits Cold urticaria
Basic foods 10 Gluten Guinea Pigs Chicken eggs Fructose Sun allergy

2. Case Study - Patient I. M. - Laboratory Findings
Page 56
13.2.16 Blood Laboratory Biochemical Screening
Special Medical History (2nd Follow-Up)
Special Medical History
Patient Name: I.M. Date: 17 OCT 2002 Pat.No. 694
Degenerated cells
Preliminary stage 1 Healthy tissue preliminary
stage 4 7 Prevent ascites
18 Immune system
stabilisation Adenomata A
Degeneration
2 ok
Healthy tissue Degeneration 5 8 Immune Deficiency 19 Killer cells Atheromata B
Diversification
3
Healthy tissue Diversification
6 9 Channel chemother. 20 Prevent neoplasia Fibromata C
Degeneration 1 (blood) Degeneration 8 (gonadoblastoma)
Degeneration 15 (kidneys)
10 Intestine improvement 21 Psyche stabilisation Lipomata D
Degeneration 2 (breast) Degeneration 9 (skin) Degeneration 16 (rectum) 12 DNA stabilisation 22 DNA stabilisation Lymphogra. E
Degeneration 3 (large
intestine)| Degeneration 10 (bladder)
Degeneration 17
(stomach) 13 Free radicals bind. 23 Radiother. Excr. Melanomata F
Degeneration 4 (small intestine) o
Degeneration 11 (liver) Degeneration 18 (pancreas)
14 Genetic Defect 24 Thrombosis prep. Myomata G
Degeneration 5 (glands) Degeneration 12 (leukaemia) Degeneration 19
(prostate) 15 Promote healing 25 Cell stabilisation Polyps H
Degeneration 6 (Ganglion) Degeneration 13 (lungs) Degeneration 20 (uterus) 16 Hormone balance Cysts I
Degeneration 7 (brain) Degeneration 14 (lymph) Degeneration 21 (spleen) 17 Channel hormonal ther.

2. Case Study - Patient I. M. - Laboratory Findings
Page 57
13.2.17 Blood Laboratory Biochemical Screening
Fundamental Medical History (3rd Follow-Up)
FUNDAMENTAL MEDICAL HISTORY
Patient Name: I.M. Date: 31 OCT 2002: Pat.No. 694:
Basic Physical Exposure
Geopathy Electrosmog Radioactivity
Focal Toxicosis
Organ nosodes Illness nosodes Scars
Immunology
Bacteria Fungi Viruses
Protozoa Parasites Vaccines
Toxicology
Home Industrial Medication
Environment Poisons Dental materials
Allergies
Foods Contact allergies Allergens
Food additives Metals Medication
Elements
Yin 3 Bacterial 2 excretion 5 acute 8
Yang 6 heavy metal 9 Interstitial cell tissue 7 chron 10
Viral 1 Chemical 4 Degen. Cells 11 .
Disorders of the Meridians
F E M WA WO
FIRE EARTH METAL WATER WOOD
WA hormones Stomach Large intestine Urinary system Large joints
M hormones Spleen Lung Kidney Small joints
Small intestine Pancreas Bronchi Female genital Liver
Circulation Metabolism Skin Male genital Bile tracts 7,8,4,2
Heart Brain Connective tissue Lymph Fatty tissue
threefold increase CNS Ligaments Teeth Muscles.
Sensory organs Tendons Paranasal sinuses Spine
Organdegen. Allerg. reaction 04 NOV 2002
Steam. Fire Steam. Earth Steam. Metal Steam. Water Steam. Wood

2. Case Study - Patient I. M. - Laboratory Findings
Page 58
13.2.18 Blood Laboratory Screening with Biotensor Fundamental Medical History (4th Follow-Up)
FUNDAMENTAL MEDICAL HISTORY
Patient Name: I.M. Date: 29 NOV 2002: Pat.No. 694:
Basic Physical Exposure
Geopathy Electrosmog Radioactivity
Focal Toxicosis
Organ nosodes Illness nosodes Scars
Immunology
Bacteria Fungi Viruses
Protozoa Parasites Vaccines
Toxicology
Home Industrial Medication
Environment Poisons Dental materials
Allergies
Foods Contact allergies Allergens
Food additives Metals Medication
Elements
Yin 3 Bacterial 2 excretion 5 acute 8
Yang 6 heavy metal 9 Interstitial cell tissue 7 chron 10
Viral 1 Chemical 4 Degen. Cells 11 .
Disorders of the Meridians
F E M WA WO
FIRE EARTH METAL WATER WOOD
WA hormones Stomach Large intestine Urinary system Large joints
M hormones Spleen Lung Kidney Small joints
Small intestine Pancreas Bronchi Female genital Liver
Circulation Metabolism Skin Male genital Bile tracts
Heart Brain Connective tissue Lymph Fatty tissue ok
threefold increase CNS Ligaments Teeth Muscles.
Sensory organs Tendons Paranasal sinuses Spine
Organdegen. Allerg. reaction
Steam. Fire Steam. Earth Steam. Metal Steam. Water Steam. Wood

2. Case Study - Patient I. M. - Laboratory Findings
Page 59
13.2.19 Blood Laboratory Biochemical Screening
Follow-Up Medical History (New Analysis of Allergic Exposure)
FOLLOW-UP MEDICAL HISTORY
Patient Name: I.M. Date: 15 JAN 2003 Pat.No. 694
Orthopaedic Condition
CSD TSD LSD Muscle stabilisation 1
C1 TH1 TH7 L1 Muscles Ligament stabilisation 2
C2 TH2 TH8 L2 Ligaments Tendon stabilisation 3
C3 TH3 TH9 L3 Tendons Joint stabilisation 4
C4 TH4 TH10 L4 Small joints
C5 TH5 TH11 L5 Large joints
C6 TH6 TH12 Bones
C7 Bone stabilisation 5
Spine gen. stabilisation
Iliosacral/hip Bone fractures 6
CSD st. TSD st. LSD stabilisation
Vaccines/Metals
Diphtheria vacc. Pertussis vacc. Rubella vacc. Vaccine excretion 1 Aluminium Silver
Diphtheria pathogen Pertussis pathogen Rubella pathogen Vaccination damage collection 2 Amalgam Teflon
TBE vaccine Measles vacc. Tetanus vacc. Vaccination complications 3 Lead Preservatives
TBE pathogen Measles pathogen Tetanus pathogen Tolerance impr. 4 Cadmium Formaldehyde
Yellow fever vacc. Mumps vacc. Rabies vacc. Complications incr. 5 Gold
Yellow fever pathogen Mumps pathogen Rabies pathogen Cobalt
Influenza vacc. Smallpox vacc. Tuberculosis vacc. Copper Antibiotics
Influenza pathogen Smallpox pathogen Tuberculosis pathogen Nickel The pill
Hepatitis vacc. Polio vacc. Chickenpox vacc. Palladium Ecbolic substances
Hepatitis pathogen Polio pathogen Chickenpox pathogen Mercury Tocolytic substances
Allergic Exposure
Food chemistry 1 Barley Lectin Horses Fish Nut mix
Bacterial influence 2 Oat Phasin Beef Poultry Sweeteners
Toxins in living spaces Carbohydrates Bee/wasp Sheep Veal Colourings
Viral influence 4 Sweet corn Animal hair gen. Pollen gen. Lamb Wood preserver
Heavy metal exposure 5 Rice Goose feathers House dust Beef Food flavourings
Fungal infection 6 Rye Dogs Hay dust Pork meat Metals
Stress 7 Wheat Insects Milk Pip fruit Detergents
Genetic cause 8 Grain flour Rabbits Lactose intol. 7/8
Stone fruit Penicillin
Major allergen 9 Gliadin Cats Egg white Citrus fruits Cold urticaria
Basic foods 10 Gluten Guinea Pigs Chicken eggs Fructose Sun allergy

2. Case Study - Patient I. M. - Laboratory Findings
Page 60
13.2.20 Blood Laboratory Screening with Biotensor Follow-Up Medical History (New Analysis 1st Follow-Up)
FOLLOW-UP MEDICAL HISTORY
Patient Name: I.M. Date: 10 April 2003 Pat.No. 694
Orthopaedic Condition
CSD TSD LSD Muscle stabilisation 1
C1 TH1 TH7 L1 Muscles Ligament stabilisation 2
C2 TH2 TH8 L2 Ligaments Tendon stabilisation 3
C3 TH3 TH9 L3 Tendons Joint stabilisation 4
C4 TH4 TH10 L4 Small joints
C5 TH5 TH11 L5 Large joints
C6 TH6 TH12 Bones
C7 Bone stabilisation 5
Spine gen.
stabilisation Iliosacral/hip Bone fractures 6
CSD st. TSD st. LSD stabilisation
Vaccines/Metals
Diphtheria vacc. Pertussis vacc. Rubella vacc. Vaccine excretion 1 Aluminium Silver
Diphtheria
pathogen Pertussis pathogen Rubella pathogen Vaccination damage
collection 2 Amalgam Teflon
TBE vaccine Measles vacc. Tetanus vacc. Vaccination complications
3 Lead Preservatives
TBE pathogen Measles pathogen Tetanus pathogen Tolerance impr. 4 Cadmium Formaldehyde
Yellow fever
vacc. Mumps vacc. Rabies vacc. Complications incr. 5 Gold
Yellow fever
pathogen Mumps pathogen Rabies pathogen Cobalt
Influenza vacc. Smallpox vacc. Tuberculosis vacc. Copper Antibiotics
Influenza
pathogen Smallpox pathogen Tuberculosis
pathogen Nickel The pill
Hepatitis vacc. Polio vacc. Chickenpox vacc. Palladium Ecbolic substances
Hepatitis
pathogen Polio pathogen Chickenpox pathogen Mercury Tocolytic substances
Allergic Exposure
Food chemistry 1 Barley Lectin Horses Fish Nut mix
Bacterial influence 2 Oat Phasin Beef Poultry Sweeteners ok
Toxins in living spaces Carbohydrates Bee/wasp Sheep Veal Colourings
Viral influence 4 Sweet corn Animal hair gen. Pollen gen. Lamb Wood preserver
Heavy metal Exposure 5 Rice Goose feathers House dust Beef Food flavourings
Fungal infection 6 Rye Dogs Hay dust Pork meat Metals
Stress 7 Wheat Insects Milk Pip fruit Detergents
Genetic cause 8 Grain flour Rabbits Lactose int. Stone fruit Penicillin
Major allergen 9 Gliadin Cats Egg white Citrus fruits Cold urticaria
Basic foods 10 Gluten Guinea Pigs Chicken eggs Fructose Sun allergy

2. Case Study - Patient I. M. - Laboratory Findings
Page 61
13.3.21 Blood Laboratory Screening with Biotensor
Follow-Up Medical History (New Analysis 2nd Follow-Up)
FOLLOW-UP MEDICAL HISTORY
Patient Name: I.M. Date: 10 April 2003 Pat.No. 694
Orthopaedic Condition
CSD TSD LSD Muscle stabilisation 1
C1 TH1 TH7 L1 Muscles Ligament stabilisation 2
C2 TH2 TH8 L2 Ligaments Tendon stabilisation 3
C3 TH3 TH9 L3 Tendons Joint stabilisation 4
C4 TH4 TH10 L4 Small joints
C5 TH5 TH11 L5 Large joints
C6 TH6 TH12 Bones
C7 Bone stabilisation 5
Spine gen. stabilisation
Iliosacral/hip Bone fractures 6
CSD st. TSD st. LSD stabilisation
Vaccines/Metals
Diphtheria vacc. Pertussis vacc. Rubella vacc. Vaccine excretion 1 Aluminium Silver
Diphtheria pathogen Pertussis pathogen Rubella pathogen Vaccination damage collection 2 Amalgam Teflon
TBE vaccine Measles vacc. Tetanus vacc. Vaccination complications 3 Lead Preservatives
TBE pathogen Measles pathogen Tetanus pathogen Tolerance impr. 4 Cadmium Formaldehyde
Yellow fever vacc. Mumps vacc. Rabies vacc. Complications prev. 5 Gold
Yellow fever pathogen Mumps pathogen Rabies pathogen Cobalt
Influenza vacc. Smallpox vacc. Tuberculosis vacc. Copper Antibiotics
Influenza pathogen Smallpox pathogen Tuberculosis pathogen Nickel The pill
Hepatitis vacc. Polio vacc. Chickenpox vacc. Palladium Ecbolic substances
Hepatitis pathogen Polio pathogen Chickenpox pathogen Mercury Tocolytic substances
Allergic Exposure
Food chemistry 1 Barley Lectin Horses Fish Nut mix
Bacterial influence 2 Oat Phasin Beef Poultry Sweeteners ok
Toxins in living spaces Carbohydrates Bee/wasp Sheep Veal Colourings
Viral influence 4 Sweet corn Animal hair gen. Pollen gen. Lamb Wood preserver
Heavy metal contamination 5 Rice Goose feathers House dust Beef Food flavourings
Fungal infection 6 Rye Dogs Hay dust Pork meat Metals
Stress 7 Wheat Insects Milk Pip fruit Detergents
Genetic cause 8 Grain flour Rabbits Lactose int. Stone fruit penicillin
Major allergen 9 Gliadin Cats Egg white Citrus fruits Cold urticaria
Basic foods 10 Gluten Guinea Pigs Chicken eggs Fructose Sun allergy

Summary Page 62
14 Summary of Results
The 20 patients chosen for the study were aged between 6 months and 15 years. 12 patients out of this group had received previous allopathic treatment with a steroid and had come into contact with a steroid over a period over about 6 to 12 months. The other 8 patients of the same age group were administered only allergy medication as allopathic pre-treatment, in roughly the same time frame. The selection of patients for this study was carried out on the basis of illness criteria in accordance with atopic eczema from the perspective of different stages of the disease, taking into consideration also family history.
The analyses which were carried out clearly demonstrate that, as well as allergic familial predisposition, a peri-natal intestinal candidosis is almost always present as a result of dysbacteriosis. The first signs of a yeast infection appear with pronounced cradle cap, oral thrush (with and without visible infection) and perianal eczema. This preceding exposure subsequently helps the allergic predisposition to take hold. If action is taken at this point with a steroid, the transfer to atopic dermatitis (neurodermatitis) almost always follows immediately with all the known concomitant symptoms and a high recurrence rate. Further developments depend on the ensuing therapy; if treatment with steroid medication continues, then nothing bars the way to further allergies such as rhinopathia pollinosa and bronchial asthma. In no situation is it possible to talk about spontaneous healing by "growing out" of the condition, if there is an endogenous disposition due to family (allergies, cumulation of the same disease) or a perinatal candidosis. At least one of these conditions was confirmed in all study cases.
The problem for the cases treated in this study, as well as for other cases, is how to convince parents to renounce treatment with cortisone. In cases of severely affected children, this becomes very difficult. Their constantly scratched and bloodied bodies, the long nights during which children cannot sleep due to intense itching wear the entire family out and often leave exhausted parents with no other choice.
The conclusion is that damage to the intestinal mucosa, caused by mycoses, antibiotics, allergies, is always present and can be viewed as the main reason. This is in fact the cause of immune deficiency, recurring toxicity and additional burdens on the skin, as confirmed by the reaction to gamma-Linolenic acid, since after their administration the skin immediately improved in almost all study cases.
14.1 The following treatment regimen has resulted from the study
1) Immediate administration of gamma-Linolenic acid in high dosage 6000mg per unit 2x1 daily, in infants and toddlers 1x1 capsule (can be opened).
2) Immediate stool culture to detect any mycoses and parasites, with consequent required therapy for the intestine.
3) Treatment of parasites, helminths, mycoses and germs with Frequency Specific Microcurrent
Therapy (FSMT).
4) Concomitant start of therapy with Bioresonance Therapy (BRT) to treat removal and allergies.
5) Concomitant homoeopathic therapy to treat the state of the skin and in conclusion miasmatic (negative genetic information) treatment.

Summary Page 63
14.2 Treatment Results for All 20 Study Patients
Total of patients treated and healed 18 out of 20 = 85%
Total of patients treated and improved 2 out of 20 = 10%
Total of patients treated and unchanged 1 out of 20 = 5%
Out of 17 healed patients, there were 4 with quick relapse 4 out of 20 = 25%
Table 9: Recurrence Rate in all 20 study patients after 8 weeks of treatment
At the beginning of the treatment, all 20 patients presented severe pain and symptoms, which were always updated at the 14-day treatment intervals. In some cases, the pain and itching diminished already after the first 2 weeks, solely due to the administration of gamma-Linolenic acid. At the end of the 8-week therapy period, all but one of the patients were practically free of symptoms and pain.
Table 10: Pain and symptom burden in all 20 patients during treatment
Healed 17 patients
Improved 2 patients
Unchanged 1 patient
Healed 4 patients with relapse
The Recurrence Rate in the Study
18
16
14
12
17
8
6
4
2
0
4
2 1
Patients Treated Over 8 Weeks
20
strong symptoms
moderate symptoms
hardly noticeable symptoms
no more symptoms
Chronological Representation of Pain and Symptom Burden
25 20 18 17
15 11
10 9
5 6 5
4 2 3
1 2
0
1 2 4 6 8
Study Progress Over 8 Weeks

References Page 64
15 References
IMU International College: Faculty of Biomagnetic Medicine. Study Materials (2003).
Keymer M.: Bicom. Resonanz Therapie (BRT). Karl F. Haug Verlag. Heidelberg (1996). 4th improved edition. ISBN 3-7760-1552-7.
Keymer M.: Dermatologisches Privatinstitut GmbH. D-Preetz (1996)
Lifeline: Fundamentals of the treatment of atopic eczema (Neurodermatitis) www.lifeline.de (26. 04. 2003).
Prof. Dr. med. Johannes D. Schnell: Vaginalmykosen und perinatale Pilzinfektion.
Karger Verlag Prattelen (1982) (1982). ISBN 3-8055-2854-X.
[a] Morel F.: Mora Therapie. Karl F. Verlag. Heidelberg (1987).
[b] Ludger Mersmann: www.biophysik.de/images/Book-USA-3.
[c] Pischinger A.: Das System der Grundregulation. Karl F. Verlag. Heidelberg (1976). 2nd edition.
[d] Wiener N.: Cypernetics Düsseldorf. Vienna (1963) 2nd edition.
[e] Keymer M.: Bicom. Resonanz Therapie (BRT). Karl F. Haug Verlag. Heidelberg (1996). 4th improved edition. ISBN 3-7760-1552-7.
[f] P. G. Valeske: Biophysicalischer Resonanz-Test auf dem Prüfstand vom Vergleich: IgE/IgG. Information booklet no. 13. pp. 93-97 by the Institut für Regulative Medizin. Kolloquium des Internationalen Medizinischen Arbeitskreises (1993).
[g] Benirschke, K; Raphael S.I.: Candida albicans of the amniotic sac. Am J. Obstet Gynec. 75: pp. 200-202 (1958).
[h] Epstein, A.: Über Soor bei Kindern. Prag med. Wschr. 5: pp. 43-87 (1880).
[i] Gavaller, B. de: Contribution a la pathogénidad de las Monilias en recién nacidos a bas de los hallazgos anatomo-pathologicos. Revta sudam. Morf. 10: pp. 117 -140 (1952).

List of Tables Page 65
16 List of Tables
Table 1 Detection of Food and Food Component Allergies in the 20 Test Patients ............................ 8
Table 2 Comparative Study between Biotensor and IgG Immunoglobulin Grid ................................ 19
Table 3 Pathogen detection in the 1st Patient Group from Blood and Stool ..................................... 21
Table 4 Pathogen detection in the 2nd Patient Group from Blood and Stool .................................... 21
Table 5 Specific Survey of Allergic Condition in All 20 Patients ....................................................... 22
Table 6 Analysis of the 20 Stool Samples for Intestinal Mycoses and Fermentative Dyspepsias ..... 22
Table 7 Analyses of Chewing Gum and Blood Drops for Heavy Metals ........................................... 23
Table 8 Yeast Infection in the Child Directly Post Partum
Table 9 Treatment Results for All 20 Study Patients ........................................................................ 63
Table 10 Chronological Representation of Pain and Symptoms ...................................................... 63
17 List of Figures
Figure 1 The Magnetic Field of the Bicom Electrodes ...................................................................... 11
Figure 2 The Separator ................................................................................................................... 12
Figure 3 The Regulating Cycle ........................................................................................................ 13
Figure 4 Pischinger's Ground Regulation System ............................................................................ 14
Figure 5 How the Cybernetic Regulatin Cycle Functions ................................................................. 16
Figure 6 Representation of the Cybernetic Regulating Cycle Between Bicom and Patient .............. 17
Figure 7 The Biotensor .................................................................................................................... 18
Figure 8 Germination of Yeast Spores (Candida Albicans) .............................................................. 24
Figure 9 Oral Thrush at 4 Days of Age ............................................................................................ 26
Figure 10 Inguinal and Genital Area Thrush at 5 Days of Age ......................................................... 26
Figure 11 Extensive Nappy Rash at 4 Weeks of Age....................................................................... 26
Figure 12 Candida Bronchopneumonia ........................................................................................... 26
Figure 13 Patient S. B. at 1 Year of Age .......................................................................................... 29
Figure 14 Patient S. B. at 13 Months of Age With Full-Blown Atopic Eczema .................................. 29
Figure 15 Patient S. B. After 8 Weeks of Treatment ........................................................................ 29
Figure 16 Patient I. M. at 3 Months of Age ....................................................................................... 39
Figure 17 Patient I. M. with Full-Blown Atopic Dermatitis ................................................................. 39
Figure 18 Patient I. M. at 2 Months of Age with Healthy Skin ........................................................... 39

Résumé Page 66
18 CURRICULUM VITAE
Name JAKOB Daniel Bruno
Address Schornäglenstr. 26, 8623 Wetzikon ZH (CH)
Personal telephone 01/930 65 38
Mobile 079/ 694`76`74
Medical practice telephone 01/970 30 55 Medical practice Fax: -56
Date of birth 26.11.1957
Home town Trub BE (CH)
Mother Dora Jakob born Lyrenmann, married at the time to
Stepfather Dr. med. Rudolf Gerner, Senior Physician at the University of Vienna
Siblings Sonja Jakob, Renè Jakob, Thomas Gerner
Marital Status Married
Background:
1974- 1978 Medical studies (8 semesters), specialisation in orthopaedics
1976 - 1980
Study of HAMO-Therapy at Private University College (8 semesters) with Prof. Dr. med. M. Mochitsuki, Dipl.
med. HAMO-Therapeuten certification Thesis: "Die Meridiane und ihre Verläufe" ("The Meridians and Their Courses")
1977 - 1979
Internship with Prof. Dr. med. univ. Wasilewski in laboratory diagnostics/determination of parameters, infiltrations, injections and microbiology.
1980 - 1981
Assistant in orthopaedic surgery and emergency medicine under the direction of Prof. Dr. med. Wasilewski,Vienna General Hospital
1990 -1991
Assistant in orthopaedics (Dr. med. A. Rüegg/Orthopaedic surgery) in Wetzikon ZH, speciality acupuncture and specialised "HAMO" acupuncture for the treatment of myogeloses and traumas of the entire locomotor system.
1990 - 1991
Assistant in orthopaedic surgery under the direction of Dr. med. A. Rüegg and in emergency medicine under the direction of Prof. Dr. med. Wasilewski.
1999
Opened own complementary medical practice at Buchgrindelstrasse 15, 8621 Wetzikon ZH
2000 - 2004
Study of bioenergetic medicine (11 semesters) at the International Mediterranean University (I.M.U.) College in Malta Faculty of Bioenergetic Medicine. Dissertation and State Examination: Atopic Dermatitis (Neurodermatitis)
and Bioresonance Therapy, under the direction of private lecturer M. Keymer.
2001- 2004
Trained at the FNH Zürich (8 semesters) to obtain certification of Dipl. med. Naturarzt FNH (Föderatio Naturopathika Helvetia)
2003
Trained at the International College für Posturologie under the direction of Dr. med. Bricot, (orthopaedic

Résumé Page 67
Surgery)
Spec. reprogramming postural tonus.
2005 - 2007
Study of chiropractic at the I.M.U. College for Holistic Health. State Examination: Certified chiropractor.
2006 Reopening of the complementary medicine practice in Wetzikon at Schlossbachstrasse 2, 8620 Wetzikon ZH.
2006
Advanced training and graduation in TCM at the I.Y.U. (Internationalen Youth University) School of Traditional Chinese Medizine in Beijing. (the 8 Semesters of HAMO were taken into account)
2006 - 2008
Doctoral study and dissertation at the Szent István University in Budapest (orthopaedics and holistic medicine). Dissertation theme: Atopic eczema and Bioresonance Therapy. Graduated summa cum laude under
the direction of Dr. László Villányi as Doctor of Holistic Medicine and Doctor of Orthopaedics.