
Intermediate stage HCC treatment options: TACE + sorafenib.
44
Intermediate stage HCC treatment options: TACE + sorafenib
Transcript of Intermediate stage HCC treatment options: TACE + sorafenib.

Intermediate stage HCC treatment options: TACE + sorafenib

1. Llovet JM, et al. Lancet. 2002;359:1734-9.2. Lo C-M, et al. Hepatology. 2002;35:1164-71.
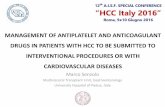
TACE: long-term survival outcomes are unsatisfactory
3-year overall survival (OS): 26%2–29%1
Sustained objective response rate (ORR) (3–6 months): 35%1–39%2
No difference in survival of intention-to-treat (ITT) population between non-responders and control group1
100
80
60
40
20
00 12 24 36 48 60 0 6 12 18 24 30 36 42
ChemoembolizationControl
ChemoembolizationControl
100
80
60
40
20
0
p < 0.0091 p = 0.0022
Time since randomization (months)
Pro
babi
lity
of s
urvi
val (
%)
Pro
babi
lity
of s
urvi
val (
%)
Time since randomization (months)

Hypoxia in the post-TACE tumour micro-environment leads to angiogenesis
HIF-1 responds to hypoxia in tumour
VEGF is a key mediator of tumour neovascularisation (growth and permeability)
Carmeliet P, Jain RK. Nature 2000; 407: 249–57
Angiogenesis
>100μmO2
Hypoxia
HIF-1 HIF-1
Glycolysis Survival/apoptosis
VEGFAng2, NOS
PDGF-β
GeneHRE
HIF = hypoxia inducible factor; HRE = hypoxia response elementAng-2 = angiopoietin-2; NOS = nitric oxide synthasePDGF-β = platelet-derived growth factor-β
Tumour cells become more acidic and more hypoxic further they are from blood vessels
7.4
7.2
7.0
6.8
6.6
Aci
do
sis
(p
H)
14121086420
0 100 200 300 400
Distance of tumour cell from blood vessels (μm)
AcidosisOxygen

VEGF levels in the liver significantly increase after TACE: clinical data
After TACE for HCC, VEGF levels in the tumour increase
Wang B, et al. Acta Radiol 2008; 49: 523–9
Control TACE
Microvessel density (not significant)
VEGF expression:number of VEGF+ cells per 500 tumour cells (p<0.01)
58.57 ± 15.7551.69 ± 18.17
138.26 ± 65.24 243.66 ± 88.88
Microvessels visible in the pericapsular area
VEGF+ cells indicated by brown staining

p=0.018
NS
NS
Plasma VEGF levels significantly increase after TACE: clinical data
Li X, et al. W J Gastroenterol 2004; 10: 2878–82NS = not significant
0
20
40
60
80
100
120
Pla
sma
VE
GF
(n
g/L
)
pre-TACE 1 3 7
64
103
8476
Days post-TACE
(n=45) (n=30) (n=44) (n=18)

High VEGF plasma levels significantly correlate with poor outcomes after TACE
Sergio A, et al. Am J Gastroenterol 2008; 103: 914–21
Plasma VEGF concentration increased following TACE
the increase is greatest in patients who did not respond to TACE
Patients with lower plasma VEGF levels had longer survival than those with higher levels (p=0.008)
130
120
110
100
90
80
70
60
50
VE
GF
(p
g/m
L)
Pre-TACE 3 28
100
75
50
25
0S
urv
ival
pro
bab
ility
(%
)
0 10 20 30 40 50
Time since TACE (months)
RespondersTotalNon-responders
VEGF levels below medianVEGF levels above medianmedian = 43.65pg/dL
Days post-TACE

Combining TAE with an anti-angiogenic agent improves outcomes: preclinical data
Combining embolisation and an anti-angiogenic agent significantly reduced tumour volume and tumour vessel density versus embolisation alone
Jiang H et al. Int J Cancer 2007; 121: 416–24*Significant difference from HCC tumours treated with TAE alone in a rat model (p<0.01); AAV = adeno-associated virus
1,200
900
600
300
0
Tu
mo
ur
volu
me
(mm
3 )
AAV-angiostatin
TAE TAE + AAV- angiostatin
35
30
25
20
15
10
5
0V
esse
l co
un
ts p
er s
urf
ace
area
AAV-angiostatin
TAE TAE + AAV- angiostatin
*
*

Transarterial chemoembolisation leads to central necrosis with a rim of peripheral hypoxia
Dufour J-F and Jonson P. J Hepatology 2009
(A) The surviving tissue exposed to hypoxia releases growth factors such as VEGF which stimulate the growth of the residual tumor lesions. (B) When TACE is performed in combination with a systemic targeted therapy, the growth factor response is blunted preventing the growth of the residual lesions.

Rationale for adjuvant or combination use of sorafenib to prevent recurrence after TACE
Angiogenesis may play an important role in tumour progression after TACE:– Temporary increases in plasma VEGF levels observed after TACE in patients
with HCC1
– Liver VEGF levels increase after TACE2
– VEGF production correlates with both tumour response and survival after TACE3
Anti-angiogenic activity of sorafenib4 may delay tumour progression after TACE
TACE, transarterial chemoembolization; VEGF, vascular endothelial growth factor .1. Li X, et al. W J Gastroenterol 2004;10:2878–82. 2. Wang B, et al. Acta Radiologica 2008;49:523–9. 3. Sergio A, et al. Am J Gastroenterol 2008;103:914–21. 4. Wilhelm SM, et al. Mol Cancer Ther 2008; 7:3129-3140.
The rationale for combining TACE with sorafenib

Rationale for combining TACE with antiangiogenic therapy for intermediate-stage HCC
Although TACE is effective for the treatment of intermediate-stage HCC, progression is frequent
Angiogenesis may play an important role in tumor survival after TACE1
VEGF reduction correlates with both tumor response and survival after TACE2
There is a rationale for investigating the concomitant use of TACE with antiangiogenic therapy
sorafenib has antiangiogenic and antiproliferative activity3
sorafenib improved overall survival in patients with advanced HCC and is the only agent approved for the treatment of HCC and was well tolerated4,5,6
1. Li et al. W J Gastro(everolienterol 2004;10:2878-82. 2. Sergio et al. Am J Gastroenterol 2008;103:914-21. 3. Wilhelm et al. Mol Cancer Ther 2008;7:3129-40. 4. Llovet et al. New Engl J Med 2008;359:378-90. 5. Cheng et al. Lancet Oncol 2009;10:25-34. 6.Nexavar EU Summary of Product Characteristics.

Sorafenib and TACE combination: different approaches
*Repeat TACE based on efficacy of initial treatment
Sequential schedule standard
TACE, transarterial chemoembolization.1. Strebel BM, Dufour J-F. Expert Rev Anticancer Ther 2008;8:1743–9.
Interrupted schedule
Continuous schedule
TACE SorafenibTime
Sequential schedule efficacy-based*
Interrupted schedule

Systemic therapy with anti-angiogenic properties concomitantly with TACE for the treatment of HCC (1)
Agent Trial phase
Region Trial schema Primary endpoint
Efficacy data Safety data
Sorafenib15 II Asia TACE + sorafenib Safety n = 147CR: 41 patientsPR/SD: 93 patientsPD: 13 patients
Most frequent G3/4 toxicities: Skin reactionHand–foot skin reactionIncreased liver enzymes
Sorafenib16 II Asia TACE + sorafenib (n = 50)
TTP, safety
n = 50TTP 5.1 mo
Hand–foot skin reaction 40%Thrombocytopenia 28%
Sorafenib17 II Europe TACE + sorafenib (n = 72)
TTP n = 44RECIST criteria: CR 0%, PR 2%, SD 26%, PD 3%EASL criteria: CR 2%, PR 15%, SD 11%, PD 3%
45 SAEsFour Grade 5 AEs (progressive disease with liver and multi-organ failure)
Sorafenib18 II Asia TACE vs. TACE + sorafenib (n = 228)
TTUP NA NA
Sorafenib19 II Asia TACE + sorafenib (n = 63)
TTP NA NA
15. START. NCT00990860. Chao et al. ILCA 2011: abstr O-026. 16. COTSUN. NCT00919009. Park et al. J Clin Oncol 29:2011 (Suppl 4); abstr 253.
17. Socrates. NCT00618384. Erhardt et al. J Hepatol 2011;54(Suppl.):S35: abstr. 79. 18. TACTICS. NCT01217034.
19. NCT01170104.

Systemic therapy with anti-angiogenic properties concomitantly with TACE for the treatment of HCC (2)
Agent Trial phase
Region Trial schema Primary endpoint
Efficacy data Safety data
Sorafenib20 II USA DC Bead™ TACE + sorafenib (n = 50)
Safety n = 36EASL criteria: PR 54%, SD 46%RECIST criteria: SD 96%, PD 4%
Most frequent Grade 3/4 toxicities: FatigueRUQ painIncreased liver enzymes
Sorafenib21 III USA TACE or DC Bead™ TACE + placebo vs. TACE or DC Bead™ TACE + sorafenib (n = 400)
PFS NA NA
Sorafenib22 III Europe DC Bead™ TACE + placebo vs. DC Bead™ TACE + sorafenib (n = 412)
Efficacy NA NA
Sorafenib23 II Europe, Asia,
USA
DC Bead™ TACE + placebo vs. DC Bead™ TACE + sorafenib (n = 300)
TTP NA NA
20. Johns Hopkins Study. NCT00844883. Prof. J-F. Geschwind (personal communication). 21. ECOG. NCT01004978. 22. TACE-2. EudraCT: 2008-005073-36. UKCRN ID 5347. 23. SPACE. NCT00855218.

www.clinicaltrials.gov/ct2/show/NCT00478374.Dufour et al. Oncologist 2010;15:1198.
(n = 21)
Eligibility criteria
• ECOG PS 0–1
• Child–Pugh A/B (<10)
• No prior systemic treatment
• BCLC Ba
Primary endpoint
• Safety
Secondary endpoints
• VEGF levels in blood prior to and after treatment
aIn July 2008, the protocol was amended by restricting inclusion to patients with BCLC stage B disease to ensure a more homogenous patient population
Phase I trial: TACE + sorafenib (continuous) in patients with HCC
Sorafenib(dose escalation from 200 mg BID
to 400 mg BID) Initiated 1 week before first TACE,
without a pause for TACE treatment+
TACE with doxorubicin (50 mg)

Continuous administration of TACE in combination with sorafenib in patients with HCC: results
Results from May 2007 to January 2009
21 patients screened for inclusion: 14 patients received sorafenib with TACE Median age: 63.5 years 78% male 93% ECOG PS 0 93% Child–Pugh A
No dose-limiting toxicities in first three patients receiving sorafenib 200 mg BID
Subsequent patients received sorafenib 400 mg BID
27 TACE procedures performed (median of two per patient; range 1–4)
Two SAEs after first TACE: one cholecystitis, one hospitalization with thigh pain
Median duration sorafenib therapy: 246 days (range 14–547 days)
Sorafenib-related AEs Grade ≥3: hand–foot skin reaction (n = 3), weight loss (n = 2), diarrhea (n = 1), abdominal pain (n = 1), thrombocytopenia (n = 3)
VEGF levels significantly decreased after sorafenib + TACE treatment (from 93 to 67 ng/L)
Dufour et al. Oncologist 2010;15:1198.

Dufour et al. Oncologist 2010;15:1198.
Continuous administration of sorafenib in combination with TACE in patients with HCC: results
Author conclusionsContinuous administration of sorafenib 400 mg BID + TACE
was tolerableThe AE profile was similar to that of sorafenib monotherapy,
except for thrombocytopenia, which may be more frequent with this combination
There were no increases in circulating VEGF levels after TACE

Phase II trial of sorafenib + doxorubicin eluting bead-transarterial chemoembolization (DEB-TACE) for patients with HCC
Selected entry criteria:
Unresectable HCC
ECOG 0–1
Child-Pugh A–B7
50 Patients
Single arm
Continuous sorafenib for as long as is beneficial
DEB-TACE up to 4 times/year
Sorafenib held 3d pre and post DEB-TACE in the first 8 pts, then continuous schedule
EASL, European Association for the Study of the Liver; ECOG, Eastern Cooperative Oncology Group; HCC, hepatocellular carcinoma; RECIST, Response Evaluation Criteria in Solid Tumours TACE, transarterial chemoembolization. 1. Reyes et al. AASLD 2009; abstr LB9; 2. Reyes et al. ASCO-GI 2010, abstr. 254. 3. Reyes et al. CIRSE 2010, abstr. 254. www.ClinicalTrial.gov NCT00844883.
Interim results:1, 2, 3
• 4% decrease at 3 weeks in tumor size (p=0.79)
• 49% decrease at 3 weeks in tumor enhancement (p<0.0001)
• 25% increase at 3 weeks in apparent diffusion coefficient (p=0.01)
• RECIST: partial response 1/24 (4%), stable disease 23/24 (96%)
• EASL: partial response 14/24 (58%), stable disease 10/24 (42%)
Findings: Combination did not result in greater toxicities than that reported for either therapy alone

Phase II trial of study in Asia of the combination of TACE with sorafenib in patients with hepatocellular carcinoma (START)
Repeated every 6 to 8 weeks
Sorafenib 400 mg twice daily will be initiated on Day 4 (up to Day 7) after 1st TACE (Day 1).
Sorafenib will be interrupted after the evening dose 4 days before next TACE cycle and restarted on Day 4 (up to Day 7) of the new TACE cycle.
A prospective trial investigating the combination of TACE and sorafenib in patients with unresectable HCC
www.clinicaltrials.gov/ct2/show/NCT00990860.
HCC patients
• BCLC B
• ECOG PS 0,1
• Child–Pugh score ≤ 7
• Size of largest tumor ≤ 10 cm
• TACE naive
TACE (Lipiodol and 30–60 mg
doxorubicin)+
Sorafenib(400 mg b.i.d)
Abdominal CT scan and AFP
assessed 4 weeks after
TACE to determine need
for further TACE
Primary end-point
• Child–Pugh safety (NCI–CTCAE v. 3.0)
Secondary end-point
• Efficacy

Phase II START 3rd interim analysis:baseline patient characteristics
Patient characteristics (n = 166)
Patients, n 166
Median age, years (range) 56.4 (48–64)
BCLC Staging system A/B/C, % 17.3/80.9/1.9
Child–Pugh A/B, % 91.6/7.7
HBV related, % 82
Previous treatment (n =146)
Surgical resection for primary HCC No/Yes, %
89.7/10.3
Loco-regional treatment for HCC No/Yes, %
89.0/11.0
• An interim safety analysis was performed at the end of 2010 when a total of 166 patients had received one or more doses of sorafenib
Adapted from Chao Y et al. Oral presentation, ILCA Hong Kong, 2011 (abstr O-026).

• TACE + sorafenib was associated with good response rates:– Complete response in 41 patients – Partial response or stable disease in 93 patients– ORR was 52.4%
• Median PFS: 270 days; TTP: 280 days; OS probability of >90% after 2 years follow up
0
5
10
15
20
25
30
35
40
45
Completeresponse
Partial reponse Stable disease Progressivedisease
Pat
ient
s (%
)P
atie
nts
(%) 27.927.9
24.524.5
38.838.8
8.88.8
Adapted from Chao Y et al. Oral presentation, ILCA Hong Kong, 2011 (abstr O-026).
Phase II START 3rd interim analysis: efficacy (n = 147)

Phase II START 3rd interim analysis: safety (n = 166)
Number of patients with drug-related adverse events (%)
All Grades Grades 3/4
Skin/subcutaneous tissue disorders
62.6 10.2
Gastrointestinal disorders 23.8 3.4
General/administration site events
8.8 0.7
Abnormal lab investigations
8.8 7.5
Respiratory/thoracic/mediastinal disorders
7.5 0
Nervous system disorders
3.4 0
Vascular disorders 3.4 0
• Skin and gastrointestinal adverse events were most common drug-related adverse events
Adapted from Chao Y et al. Oral presentation, ILCA Hong Kong, 2011 (abstr O-026).

Phase II START 3rd interim analysis: top Grade 3/4 AEs (non-laboratory) (n = 166)
• Top 5 Grade 3/4 drug-related AEs (non-laboratory) were skin reaction, hand-foot skin reaction, diarrhea/vomiting, and blister
Number of patients with drug-related adverse events (%)
Grade 3 Grade 4 Grades 3/4
Skin reaction 4.1 0 4.1
Hand-foot skin reaction
2.7 0 2.7
Diarrhoea 1.4 0 1.4
Vomiting 1.4 0 1.4
Blister 1.4 0 1.4
Chao et al. Oral presentation, ILCA Hong Kong, 2011 (abstr O-026).

Phase II START 3rd interim analysis: top Grade 3/4 AEs (laboratory) (n = 166)
• Top 5 Grade 3/4 drug-related AEs (laboratory) were elevated liver transferases (ALT / AST) and decreased neutrophil / platelet / white blood cell counts
Number of patients with drug-related adverse events (%)
Grade 3 Grade 4 Grades 3/4
Alanine aminotransferase increased
6.8 0 6.8
Aspartate aminotransferase increased
4.1 1.4 5.5
Neutrophil count decreased
4.1 0 4.1
Platelet count decreased 3.4 0 3.4
White blood cell count decreased
3.4 0 3.4
Chao Y et al. Oral presentation, ILCA Hong Kong, 2011 (abstr O-026).

Phase II START 3rd interim analysis
Author conclusions
TACE and sorafenib combination therapy was effective: 52.4% of patients had CR/PR through RECIST assessment
Clinical progression of disease in 8.8% of patients after the first cycle of TACE+ sorafenib treatment
This combination therapy achieved a median PFS of 270 days, TTP of 280 days and an OS probability of >90% after 2 years follow up
No un-expected or new safety signals from this study
Adapted from Chao Y et al. Oral presentation, ILCA Hong Kong, 2011 (abstr O-026).

Primary endpoints
• TTP
• Safety and tolerability
Secondary endpoints
• PFS
• ORR
N = 50Sorafenib 400 mg BID
+ TACE
Lipiodol + doxorubicin30–60 mg → Gelfoam
Eligibility criteria• ≥1 bi-dimensional lesion
(CT or MRI)
• Child–Pugh A or B ≤7
• ECOG PS ≤1
www.clinicaltrials.gov/ct2/show/NCT00919009.
• Sorafenib on day 3 after first TACE• Sorafenib continuous up to 24 weeks• TACE every 4–6 weeks on demand
Phase II COTSUN Korea trial: TACE + sorafenib (continuous)
interim analysis (n = 50) Patient characteristics: Mean age: 61.5 years82% BCLC B18% BCLC C56% HBV16% HCVMedian follow-up: 5.3 months (range 1.0–13.1 months)Median number of TACE sessions: 1 (range 1–4 sessions)

Phase II COTSUN Korea trial: interim analysis (n = 50)
Results
AEs more severe than NCI–CTCAE Grade 3: Hand–foot skin reaction (40%) Thrombocytopenia (28%) ALT/AST increase (38/34%) Dose reduction of sorafenib in 50% of patients, mostly due to hand–foot
skin reaction
Median TTP was 5.1 months (range 3.8–6.3 months)
Author conclusions
Interim analysis showed that a combination of TACE and sorafenib was well tolerated and the trial could be continued
Preliminary evidence of anti-tumor activity was observed
Park J-W et al. Poster presented at ASCO GI 2011, San Francisco USA (abstr. 253).

Primary endpoint
• TTP
Secondary endpoint
• Safety
Sorafenib 400 mg BID
n = 72
Phase II SOCRATES study: TACE + sorafenib (interrupted)
Adapted from Erhardt A et al. Poster presented at ASCO 2011, Chicago, IL, USA (abstr. 4107). www.clinicaltrials.gov/ct2/show/NCT00618384.
Sorafenib administered for ≥14 days
TACE TACE
Eligibility criteria
• Unresectable HCC
• Measurable disease (RECIST)
• ECOG PS 0–2
• Child–Pugh <B8
TACE repeated every 6 weeks*
Sorafenib withheld
3 days pre- TACE
Sorafenib withheld
3 days post- TACE
*One cycle = 6 weeks*One cycle = 6 weeks

Phase II SOCRATES study:baseline patient characteristics
Erhardt A et al. Poster presented at ASCO 2011, Chicago, IL, USA (abstr. 4107).
Baseline Patient Characteristics
Sorafenib + TACE (n = 43)
Female/male, % (n) 14 (6) /86 (37)
Mean age, years (SD) 69 (9)
Etiology HCV/HBV/other, %
30/16/64
Child–Pugh A/B, % 81/19
Tumor size 4.5 cm (1.526)
BCLC B/C, % 84/16
AFP µg/L, mean (SD) 205 (807)
ALT U/L, mean (SD) 54 (30)
Platelets x103 µl 194 (94)

Patients were evaluated by central radiology
Patients, n (%)
CR PR SD PD Only baseline
RECISTEASL
03 (7.0)
2 (4.7)18 (41.9)
32 (74.4)11 (25.6)
2 (4.7)4 (9.3)
7 (16.2)7 (16.2)
• Patients received:– a mean of 2.6±2.2 [range 0–10] TACE applications– a mean of 8.3±7.4 [range 0–28] cycles
Erhardt A et al. Poster presented at ASCO 2011, Chicago, IL, USA (abstr. 4107).Erhardt A et al. Poster presented at ASCO 2011, Chicago, IL, USA (abstr. 4107).
Phase II SOCRATES study:final response data (ITT: n = 43)

RECIST criteriaDiscontinuation before a radiological progression was censored
Events: 12 × progression5 × death2 × LTX3 × TACE not possible7 × only baseline•2 × TACE not possible•2 × sorafenib not tolerated•2 × death (diverticulitis, progression)•1× progression (Child B to C)
TTP: 18.9 mo (568 days)(95% CI: 515)
Phase II SOCRATES study:final TTP data (ITT: n = 43)*
Erhardt A et al. Oral presentation at EASL 2011, Berlin, Germany (abstr. 79).
*According to RECIST; data for 3 patients under investigation

OS: 20.1 months (603 d)(95% CI: 527, 741)
Phase II SOCRATES study:final overall survival data (ITT: n = 43)*
Erhardt A et al. Poster presented at ASCO 2011, Chicago, IL, USA (abstr. 4107).Erhardt A et al. Poster presented at ASCO 2011, Chicago, IL, USA (abstr. 4107).
*As by April 2011: 15 out of 43 patients still alive

Phase II SOCRATES study final analysis: safety
Erhardt A et al. Poster presented at ASCO 2011, Chicago, IL, USA (abstr. 4107).Erhardt A et al. Poster presented at ASCO 2011, Chicago, IL, USA (abstr. 4107).
Frequent Adverse events (>10%)
TACE + sorafenib (n = 43)
n Cycle 1 Cycle 2Cycle 3 Cycle 4
Diarrhea 25 13 8 3 1
Hand–foot skin reaction 20 8 9 3 0
Anorexia 14 9 5 0 0
Asthenia 12 10 2 0 0
Weight loss 9 6 3 0 0
ALT elevation 7 2 2 3 0
Hepatic encephalopathy 7 1 2 3 1
Thrombocytopenia 6 2 2 2 0
Ascites 6 1 4 1 0
Nausea 6 4 2 0 0
Hoarseness 6 5 1 0 0

Phase II SOCRATES study final analysis: conclusions
Combination of TACE plus Sorafenib allowed an acceptable tumor control
Combination of TACE plus Sorafenib resulted in an increased TTP and OS
Side effects were tolerable and in part related to the combination treatment compared to the monotherapeutic approaches
Present results have to be confirmed by the ongoing phase III study (SPACE Trial)
Erhardt A et al. Poster presented at ASCO 2011, Chicago, IL, USA (abstr. 4107).Erhardt A et al. Poster presented at ASCO 2011, Chicago, IL, USA (abstr. 4107).

Johns Hopkins University phase II trial of doxorubicin-eluting LC Bead® TACE plus sorafenib in patients with unresectable HCC
Primary end-point: safety
Secondary end-point: tumor response (EASL, RECIST), TTP, OS
Continue until tumor progression or
toxicity
*Absolute neutrophil count > 1,500 /mm3, platelets > 50,000 /mm3, normal creatinine, total bilirubin ≤ 3, AST and ALT < 5 x upper limit of normal.
NCT00844883.Geschwind et al. J Clin Oncol 2011 [in press]
(n = 50)
Sorafenib 400 mg b.i.d. initiated
1 week before first TACE
Up to 4 treatments/6 months: TACE with doxorubicin-LC
Bead® 100 mg doxorubicin
Eligibility criteria
• Unresectable HCC (beyond Milan)
• > 18 years old
• ECOG PS 0/1
• Child–Pugh A/B (< 8)
• Adequate end organ function*
+

Patient characteristics: Phase II Trial of DEB-TACE plus Sorafenib
Variable Value
Patients enrolled 35
Mean age, years (range) 64 (31–88)
Male/female 26/9
Child–Pugh status A/B 31/4
ECOG Performance Status 0/1 16/19
HBV/HCV/other etiology 2/13/20
Portal vein Thrombosis (yes/no) 11/24
BCLC B/C 12/23
Mean index tumor size, cm (SD) 7.7 ±4.2
Geschwind et al. J Clin Oncol 2011 [in press]

*ADC = apparent diffusion coefficient measured by functional diffusion weighted MR.
Tumor Response: Phase II Trial of DEB-TACE plus Sorafenib
EASLPartial response:14/26 (54%)Stable disease: 12/26 (46%)
36 patients treated to date, 35 patients completed Cycle 1 (n = 26 evaluated for efficacy)Tumor response by MR imaging
FeaturesPre-
DEB-TACEPost-
DEB-TACE
Change at 3 weeks
(%)p value
Tumor Size ± SD (cm) 7.9 ± 4.3 7.6 ± 4.5 – 4 0.79
Tumor Enhancement (%) 85 43.5 – 49 < 0.01
*ADC (x 10–3 mm2/sec) 1.2 1.54 + 25% 0.01
RECIST Stable disease: 25/26 (96%)Progressive disease: 1/26 (4%)
Geschwind et al. J Clin Oncol 2011 [in press]

Tumor Response: Phase II Trial of DEB-TACE plus Sorafenib
68-year-old male, right lobe lesion2 cycles of DEB-TACE and sorafenibBridged to surgical resection 3 months after end of second cycle
TACE #1 TACE #2
Baseline 21 Days Post-treatment
10.3 cm, 90% enhancement
10.2 cm, 30% enhancement
Geschwind J-F et al. Presented at 2nd Asia–Pacific Primary Liver Cancer Expert Meeting, 1–3 July 2011, Osaka, Japan.

Baseline:8.1 cm, 90% enhancement
3 weeks post DEB-TACE:6.3 cm, 10% enhancement
20 months post DEB-TACE:5.7 cm, <10 % enhancement
73-year-old male, right lobe lesion 1 cycle of DEB-TACE and sorafenib Stable for 20 months
Geschwind J-F et al. Presented at 2nd Asia–Pacific Primary Liver Cancer Expert Meeting, 1–3 July 2011, Osaka, Japan.
Tumor Response: Phase II Trial of DEB-TACE plus Sorafenib

Incidence of Grade 3/4 Toxicities:Phase II Trial of DEB-TACE plus Sorafenib
All remaining toxicities were Grade 1/2 (no unexpected events)
60
50
40
30
20
10
0
All Grade 3/4 toxicities (any cause)
Pain-a
bd-RUQ
Fatigue
Incre
ased liver e
nzym
e
Lymphopenia
HFSR
Hyperbilir
ubinem
ia
Pain (o
ther)
Hypertensio
n
Incre
ased lipase
Pain in
chestDOE
PE / >coagulo
pathy
Rash /mucositi
s
Encephalopath
y
Cycle 1 (n = 27)
Cycle 2 (n = 19)
Cycle 3 (n = 12)
Pain-abd-RUQ = abdominal pain, right upper quadrantDOE = Dyspnea on exertion; PE = pulmonary embolism
Per
cen
tag
e
Geschwind J-F et al. Presented at 2nd Asia–Pacific Primary Liver Cancer Expert Meeting, 1–3 July 2011, Osaka, Japan.

Phase II TACTICS randomized trial: TACE vs. TACE + sorafenib in patients with HCC
www.clinicaltrials.gov. NCT01217034.
(n = 228)
Eligibility criteria
•ECOG PS 0–1
•Child–Pugh A
•No prior systemic treatment
Primary endpoint
• TTUP
Secondary endpoints
• TTP
• Overall survival
• ORR
• Tumor markers
• Safety
Sorafeniba
+TACE
TACE repeated when tumor increases
TACE
TACE repeated when tumor increases
a400 mg OD stopped 2 days before first TACE; resumption of sorafenib 3–21 days after TACEWhen tolerability is confirmed at 1 week after resumption, sorafenib is increased to 400mg BID
Status: recruiting

Phase II, randomized, double-blind, placebo-controlled study of sorafenib in intermediate-stage HCC in combination with DEB-TACE using beads loaded with doxorubicin
Study start date: March 2009
Estimated completion date: Dic 2011
DEB, drug-eluting bead; ECOG, Eastern Cooperative Oncology Group; EHS, extrahepatic spread; HCC, hepatocellular carcinoma; MVI, macrovascular invasion; OS, overall survival; TACE, transarterial chemoembolization; TTP, time to progression; TTUP, time to untreatable progression.www.ClinicalTrial.gov, NCT00855218 - EudraCT: 2008-005056-24
Endpoints
Primary TTP
Secondary OS TTUP Time to vascular
invasion Time to EHS
Eligibility criteria Unresectable HCC Multinodular HCC Child–Pugh A ECOG PS 0
Exclusion criteria EHS/MVI Contraindication to
TACE
DEB-TACE +
sorafenib 400 mg bid
DEB-TACE + placebo
SPACE: Sorafenib or Placebo in combination with TACE for intermediate stage HCC
Ra
nd
om
iza
tio
n
1:1
(n=
30
7)

Primary end-point• PFS
Secondary end-points• OS• Toxicity
www.clinicaltrials.gov/ct2/show/NCT01004978.
Sorafenib 400 mg b.i.d.
and TACE (doxorubicin,
mitomycin C and cisplatin)
Placebo and TACE
(doxorubicin,
mitomycin C and cisplatin)
Randomization1:1
(n = 400)
Eligibility criteria• Unresectable HCC• Child–Pugh A -B7• ECOG PS 0-1
Exclusion criteria• EHS• Main portal vein
invasion• Ascites
A phase III randomized, double-blind trial of TACE with or without sorafenib in patients with unresectable HCC
– status: recruiting– contact information: ECOG Group Chair’s Office (Robert L. Comis)
ECOG: phase III study investigating the combination of sorafenib with TACE

QoL = quality of life. EudraCT: 2008-005073-36 ; ISRCTN: 93375053; UKCRN ID 5347
Eligibility criteria Unresectable HCC At least 1 unidimensional CT/MRI-measurable lesion Child–Pugh A ≤6 ECOG PS ≤1
Exclusion criteria EHS Contraindication to TACE Child–Pugh B ≥7 or C Prior embolization, systemic or radiation tx
1º endpoint PFS
2º endpoints
OS Toxicity QoL Number of TACE performed Health economics
Investigator-sponsored, randomized, placebo-controlled, double-blinded, Phase III trial evaluating sorafenib in combination with TACE in unresectable HCC
– Study start date: August 2010– Estimated completion date: 07 January 2013– Target recruitment: 412 patients (UK, Ireland, France and Italy)– Status: recruitment opened November 2010
TACE-2: Phase III study investigating the combination of sorafenib with TACE
Sorafenib 400 mg BIDcontinuous
Placebo PO BID
continuous
2-5 weeks
initiate TACE
DEB-TACE with
doxorubicin (150 mg)
1:1
Ran
do
miz
ati
on
(n =
412
)

Adjuvant Sorafenib after TACE to prevent Recurrence of Hepatocellular CarcinOma (ASTRO)
Italy, phase II, double-blind, randomised, placebo-controlled adjuvant trial after TACE-based treatments
Prior treatment• TACE ± RFA/PEI
Eligibility criteria• Child–Pugh
score 5–7 • Radiological CR
Primary endpoint• Time to recurrence
Secondary endpoints• RFS• OS• Other
Sorafenib 400 mg b.i.d.
Placebo
Randomisation 1:1(n=216)
Stratification• Unifocal vs. Multifocal















![F]FDG PET imaging evaluation on non-alcoholic fatty liver disease … · 2018-11-09 · Conclusion: Sorafenib shows promise 18as a treatment for reducing the aggressiveness of HCC](https://static.fdocuments.in/doc/165x107/5ecaf77331e6bc613a32fe63/ffdg-pet-imaging-evaluation-on-non-alcoholic-fatty-liver-disease-2018-11-09-conclusion.jpg)
