
ACCEPTABILITY of interferon-gamma release assays for use in routine employee TB testing
INT J TUBERC LUNG DIS e-publication ahead of print 8 June 2011© 2011 The Uniondoi:10.5588/ijtld.10.0631
REVIEW ARTICLE
Interferon-gamma release assays and childhood tuberculosis: systematic review and meta-analysis
A. M. Mandalakas,*† A. K. Detjen,†‡ A. C. Hesseling,† A. Benedetti,§¶# D. Menzies§
* Department of Pediatrics, Case Western Reserve University, Cleveland, Ohio, USA; † Desmond Tutu TB Centre, Department of Paediatrics and Child Health, Stellenbosch University, Cape Town, South Africa; ‡ International Union Against Tuberculosis and Lung Disease, New York, New York, USA; § Respiratory and Epidemiology Clinical Research Unit, Montreal Chest Institute, Montreal ¶ Department of Medicine, and # Department of Epidemiology, Biostatistics & Occupational Health, McGill University, Montreal, Quebec, Canada
Correspondence to: Anna Mandalakas, Global Health & Diseases, and Epidemiology & Biostatistics, Case Western Reserve University, Cleveland, Ohio 44106, USA. Tel: (+1) 216 844 6246. Fax: (+1) 216 844 6265. e-mail: [email protected] submitted 14 October 2010. Final version accepted 21 December 2010.
B A C K G R O U N D : Children infected with Mycobacte-rium tuberculosis have signifi cant risk of developing tu-
berculosis (TB) and can therefore benefi t from preven-
tive therapy.
O B J E C T I V E : To assess the value of interferon-gamma
release assays (IGRAs) and the tuberculin skin test (TST)
in the diagnosis of TB infection and disease in children.
M E T H O D S : Thirty-three studies were included, assess-
ing commercial IGRAs (QuantiFERON®-TB [QFT] and
T-SPOT.®TB) and TST. Reference standards for infec-
tion were incident TB or TB exposure. Test performance
for disease diagnosis was evaluated in studies assessing
children with confi rmed and/or clinically diagnosed TB,
compared to children where TB was excluded.
R E S U LT S : Two small studies measured incident TB in
children tested with QFT and found weak positive pre-
dictive value. Association of test response with exposure
—categorized dichotomously or as a gradient—was sim-
ilar for all tests. The sensitivity and specifi city of all tests
were similar in diagnosing the disease. Stratifi ed analysis
suggested lower sensitivity for all tests in young or hu-
man immunodefi ciency virus infected children.
C O N C L U S I O N S : Available data suggest that TST and
IGRAs have similar accuracy for the detection of TB in-
fection or the diagnosis of disease in children. Heteroge-
neous methodology limited the comparability of studies
and the interpretation of results. A rigorous, standard-
ized approach to evaluate TB diagnostic tests in children
is needed.
K E Y W O R D S : tuberculosis; pediatrics; TB infection; IGRAs; tuberculin skin test
THE WORLD HEALTH ORGANIZATION (WHO) estimates that 2 billion people are infected with Myco-bacterium tuberculosis,1 creating a reservoir that leads to 9 million new tuberculosis (TB) cases and 2 mil-lion deaths annually. Children carry approximately 15% of the disease burden, 75% of which occurs in the 22 high-TB-burden countries.2 TB exposure in young children frequently occurs in the household, and the risk of non-household exposure increases with age. Young children not identifi ed for preventive therapy have a disproportionately high risk of early progression to disease and severe forms of TB.3 The global TB epidemic is exacerbated by human immuno-defi ciency virus-1 (HIV) infection, especially in sub-Saharan Africa. HIV-infected children have an up to 24-fold higher risk of developing TB compared to HIV-negative children.4
There is no gold standard for the detection of
S U M M A R Y
M. tuberculosis infection. The tuberculin skin test (TST) has known limitations in terms of sensitivity and specifi city,5–14 which may place children at risk of under- or over-treatment for latent infection. This could unnecessarily burden patients, families and r esource-limited health systems, while potentially failing to identify those children at highest risk of TB disease progression.
The diagnosis of active TB in children is also diffi -cult due to the paucibacillary nature of childhood TB, which makes bacteriological confi rmation chal-lenging. As a result, the diagnosis of active disease in this population often relies on a composite of contact history, clinical symptoms and radiological fi ndings, as well as consideration of the TST reaction.15
The TST and the recently developed interferon-gamma release assays (IGRAs) are immune-based diag-nostic tests. IGRAs measure ex-vivo interferon-gamma (IFN-γ) production by circulating T-lymphocytes when incubated in the presence of highly specifi c AMM and AKD contributed equally to this work.

2 The International Journal of Tuberculosis and Lung Disease
M. tuberculosis antigens (early secreted antigenic tar-get 6 [ESAT-6], culture fi ltrate protein 10 [CFP-10] ± TB7.7). There are two commercially available IGRAs: QuantiFERON®-TB (QFT; QuantiFERON®-TB Gold [QFT-G] and QuantiFERON®-TB Gold In-Tube [QFT-GIT], Cellestis, Carnegie, VIC, Australia) and T-SPOT.®TB (Oxford Immunotec, Oxford, UK). The QFT test incubates whole blood and measures IFN-γ production with an enzyme-linked immunosorbent assay (ELISA), while T-SPOT.TB measures the num-ber of IFN-γ producing peripheral mononuclear cells (PBMCs). Like the TST, IGRAs cannot differentiate between M. tuberculosis infection and active TB.
A growing number of studies have compared the TST and IGRAs in the detection of M. tuberculosis infection and active TB in children. In the absence of a gold standard for infection, some studies have mea-sured sensitivity in populations with active TB as a surrogate for M. tuberculosis-infected persons, while others have used M. tuberculosis exposure as a surro-gate for infection.16,17 The value of IGRAs for the diagnosis of active TB and M. tuberculosis infection in children remains unclear.
We systematically reviewed the existing evidence on the accuracy of IGRAs for the detection of M. tu-berculosis infection and diagnosis of active TB in children in settings with varying incidence of TB. This review was presented at the July 2010 WHO expert meeting where recommendations were drafted for the use of IGRAs in high-burden settings.
METHODS
In collaboration with an experienced librarian at Case Western Reserve University, we systematically searched Medline and Web of Science for articles published in English, French or Spanish from 1998 until January 2010. Search terms included ‘tuber cu-losis infection’, or ‘tuberculosis disease’, AND ‘P e di-atrics’ or ‘child*’, AND ‘QuantiFERON’, or ‘ELISpot’, or ‘interferon-gamma assays’, or ‘interferon-gamma release assays’, or ‘T-cell assays’, AND ‘ESAT-6’, or ‘CFP10’, or ‘RD1 antigens’. We searched reference lists of all articles selected, existing systematic reviews and an existing IGRA database (courtesy of M Pai, McGill University, Montreal, QC, Canada). We also captured new publications identifi ed until 1 June 2010 (Figure 1).
We considered published peer-reviewed studies that included at least 20 children aged <18 years, as-sessing commercially available IGRAs (QFT-G, QFT-GIT and T-SPOT.TB). Studies using in-house assays or pre-commercial IGRA versions were excluded. Case series and case reports were not considered.
Selection of articles for inclusion in this review was performed in two stages. Two reviewers (AM and AD) fi rst screened titles and abstracts, and then performed a full text review to determine eligibility.
Disagreements regarding inclusion were resolved by consensus, or with input from a third reviewer (DM) when consensus could not be reached.
Information was extracted independently from all selected publications by the same two reviewers us-ing a standardized data extraction form, developed, piloted and used specifi cally for this review. Discrep-ancies in extracted data were resolved by consensus.
All reference standards were defi ned a priori: the primary reference standard for M. tuberculosis infec-tion was incident TB in cohorts who were exposed but disease-free and tested for infection at study en-rollment, then followed prospectively with active case fi nding to identify children who subsequently devel-oped active TB. The secondary reference standard for M. tuberculosis infection was TB exposure, defi ned dichotomously (exposed or not) or as a gradient, based on index case microbiologic indicators (sputum smear) or proximity or duration of contact.
Figure 1 Flow of study selection. * See Table 1. ISI = Institute for Scientifi c Information; IGRA = interferon-gamma release assay.

IGRAs and childhood TB: systematic review 3
For the assessment of sensitivity for the diagnosis of active TB, two defi nitions of disease were accepted: defi nite (confi rmed) and probable TB. Defi nite TB was defi ned as the presence of at least one clinical speci-men positive for M. tuberculosis on culture, or posi-tive acid-fast bacilli smear microscopy, or one histol-ogy sample positive for necrotizing granulomas, or nucleic acid amplifi cation test positive for M. tubercu-losis. Probable TB was defi ned as the presence of three or more of the following: 1) chest radiologic fi ndings consistent with active TB; 2) typical symptoms such as cough and weight loss; 3) other radiological evi-dence of active TB, including extra-pulmonary TB (e.g., computed tomography/magnetic resonance im-aging fi ndings consistent with TB meningitis) in con-junction with symptoms; 4) exposure to a case with active infectious TB; and 5) response to appropriate anti-tuberculosis therapy. TST and IGRA could not be included in either case defi nition. For assessment of specifi city in the diagnosis of active TB, we used data from groups of children in whom active TB was systematically excluded: 1) TB suspects with symp-toms suggestive of active TB, or 2) children with ex-posure to a case with active TB. We did not include data from groups if they did not have clear risk fac-tors for active TB or if it was unclear whether active TB was systematically excluded in all subjects.
Data were extracted on the number of positive, negative and indeterminate results for each of the ref-erence standards and tests assessed. Data were also extracted to support stratifi ed and subgroup analysis. We used 13 QUADAS (Quality Assessment of Diag-nostic Accuracy Studies) items for the assessment of study quality and added an additional item on indus-try involvement.18,19
AnalysisData were analyzed using SAS version 9.2 (SAS Insti-tute Inc, Cary, NC, USA) and STATA version 11 (Stata Corporation, College Station, TX, USA). Sev-eral analytic approaches were used to evaluate test performance for the detection of M. tuberculosis in-fection. In studies that measured exposure dichoto-mously, we assessed the association between test re-sult and TB exposure as an odds ratio (OR). These results were pooled using both a fi xed- and a random-effects approach.20 In studies that expressed exposure via a gradient, we measured the correlation between exposure gradients and prevalence of positive tests. We estimated the Spearman correlation between the categorical test result and the outcome and calculated a pooled correlation coeffi cient for each test with both a fi xed- and a random-effects approach.21 Next, we used the OR as the measure of effect to assess performance by calculating the OR for each level of exposure relative to the reference group, and then an overall OR for increasing exposure category. We again used both fi xed- and random-effects ap-
proaches to estimate a pooled exposure effect across studies.22,23 We estimated inter-study heterogeneity via I2 statistics.20
To evaluate test performance for the diagnosis of active TB, we used data from studies that measured IGRAs in children with active TB to estimate test sensitivity and data from studies that included an appropriate group in whom active TB was excluded to estimate test specifi city. We used a random effects meta-analysis to estimate the overall pooled estimates of sensitivity, specifi city and 95% confi dence interval (95%CI; Proc Nlmixed in SAS), and used the exact binomial likelihood approach to approximate the distribution of the outcome of interest.24 We assessed heterogeneity by estimating the I2 statistic and associ-ated 95%CIs.25 To calculate the I2, zero cells were corrected by 0.5. To explore sources of heterogene-ity, we performed sub-group analyses stratifi ed by predefi ned covariates of interest. These included TB incidence, age, World Bank income, bacille Calmette-Guérin (BCG) vaccination rate, HIV prevalence, TST cut-off point and QFT test type (QFT-G or QFT-GIT).
To assess the impact of indeterminate IGRA re-sults, sensitivity estimates were calculated with inde-terminates considered as false-negatives; the relation-ship between the frequency of IGRA indeterminate results and important covariates was described.
RESULTS
Selection and quality of studiesOur search strategy identifi ed 240 studies. From these, 67 articles were selected for full text review, of which 31 articles describing 32 studies (one arti-cle describing two studies conducted in two coun-tries was included; Figure 1, Table 1).26–93 Thirty-six studies that completed full text review were excluded for a number of reasons, including data not available;27,42,47,48,61,62,64,80,81,83,91 no exposure gradient used;31,34,71,74,86,89,90 pre-commercial IGRAs used;29,37,40,66,76,85 fewer than 20 children in-cluded;28,60,65,70,77 IGRA testing completed in TST-positive children only, precluding a comparison group;46,56,78,93 study population overlapped with an included study;39,84 and children with positive TST referred preferentially to the study, creating incorpo-ration bias.63
Studies were performed in 18 countries; the inci-dence of smear-positive TB was >25 per 100 000 population in 10. Nineteen studies (59%) were per-formed in high-income countries; these included 11% to 100% immigrant children. The 32 studies de-scribed results in 5525 children; our analysis included 4122 of these children, as some sub-groups did not meet the criteria for any reference standard. The mean age of the children was 7.6 years (range 1.9–14.6); BCG coverage ranged between 8% and 100%. Six studies included HIV-infected children (range

4 The International Journal of Tuberculosis and Lung Disease
Table 1 Characteristics of included studies sorted by World Bank income index
Author, year, reference Country
World Bank
income index
TB incidence*
Included for analysis/total study
n/N
Mean or median age,
yearsBCG%†
Immigrants%†
HIV-infected
%†
Immune suppressed
%†
Adetifa, 201026‡ The Gambia LIC 113 225/285 7.3 77 NR 1 NROkada, 200879 Cambodia LIC 219 195/217 2.5 88 NR NR NRPetrucci, 200882‡§ Nepal LIC 77 146/145 8.5 94 NR NR NRDogra, 200744‡ India LMIC 75 105/105 6¶ 92 NR 1 57Nakaoka, 200673 Nigeria LMIC 131 207/207 7.4 90 NR NR NRWarier, 200992 India LMIC 75 100/143 6.7 NR NR NR NRHansted, 200951 Lithuania UMIC 30 120/120 13.9 100 NR 0 NRHesseling, 200954‡ South Africa UMIC 358 29/29 2.9 100 NR 0 0Mandalakas, 200869‡ South Africa UMIC 358 23/23 4.4 91 NR 100 0Nicol, 200975 South Africa UMIC 358 214/243 2.6 100 NR 0.5 NRPetrucci, 200882‡§ Brazil UMIC 26 113/113 8.4 100 NR NR NRStavri, 200987 Romania UMIC 51 36/36 15 100 NR 100 67Stefan, 201088 South Africa UMIC 358 34/34 7¶ NR NR 0 100Bamford, 200930‡ UK HIC 6.8 195/195 8.5 53 42 NR NRBergamini, 200932‡ Italy HIC 3.3 480/480 10.9 38 71 0 0Bianchi, 200933‡ Italy HIC 3.3 16/336 4.5¶ 52 97 0 0Chun, 200835 Korea HIC 40 162/227 3.2 100 NR 0 NRConnell, 200636‡ Australia HIC 2.8 9/101 3.9¶ 33 78 NR NRConnell, 200838‡ Australia HIC 2.8 9/100 8.2 23 89 NR NRDetjen, 200741‡ Germany HIC 2.7 50/73 3.3¶ 8 52 0 0Diel, 200843‡ Germany HIC 2.7 168/168 13.3 41 24 0 0Dominguez, 200845‡ Spain HIC 13 134/134 9.6 64 66 0 0Girardi, 200749 Italy HIC 3.3 9/161 13 9 11 NR NRGrare, 201050‡ France HIC 6.2 7/51 6.5 43 100 NR NRHaustein, 200952‡ UK HIC 6.8 27/253 7.3 51 NR 0.9 24Herrmann, 200953 France HIC 6.2 62/129 7¶ 92 27 0 0Higuchi, 200957‡ Japan HIC 9.5 313/313 9.6 99 NR NR NRHiguchi, 200855‡ Japan HIC 9.5 102/102 14.6 100 NR NR NRHiguchi, 200958 Japan HIC 9.5 10/61 8.6 80 NR NR NRKampmann, 200959 UK HIC 6.8 91/209 9.2 60 33 0 NRLighter, 200967‡ USA HIC 1.8 207/207 9 36 34 0 0Lucas, 201068‡ Australia HIC 2.8 524/524 7.4¶ 69 100 NR NR
* Incidence of smear-positive TB per 100 000 population reported by the WHO in 2007.† These data indicate the proportion of BCG-vaccinated/immigrants/HIV-infected or immune-suppressed children within the sub-group used for analysis. If the subgroup data were not available, data for the whole group were used.‡ Author contacted to ensure that there was no data overlap with other publications or to provide clarifi cation/re-analysis of data.§ Data provided in the published manuscript were analyzed as two independent studies.¶ Median age used as mean age was not reported.TB = tuberculosis; BCG = bacille Calmette-Guérin; HIV = human immunodefi ciency virus; LIC = low-income country; NR = not reported; LMIC = low- and middle-income countries; UMIC = upper-middle-income country; HIC = high-income country; WHO = World Health Organization.
0.5–100),26,44,52,69,75,87 and three studies included chil-dren with non-HIV-related immune suppression.52,87,88
Two studies reported incident TB in cohorts, 18 described the association of tests with exposure (Ta-ble 2), 21 assessed test sensitivity in children with ac-tive TB, and nine provided data that could be used to estimate test specifi city for active TB. Studies evalu-ated one or more index tests, including T-SPOT.TB (n = 15), QFT-G (n = 10) and QFT-GIT (n = 21). Thirty studies provided TST data that could be used for analysis (Table 1).
Assessment of the study quality using QUADAS showed that only a minority of studies clearly re-ported on sampling methods or included a spectrum of subjects representative of patients in whom the tests might be used clinically. Blinding of clinicians to IGRA results was reported in 29% of the studies as-sessing active TB. Of 32 studies, 11 (33%) were sup-ported by either or both IGRA manufacturers, mainly through donation of test kits. In 43% of the studies assessing active TB, it remained unclear whether the reference standard was applied to all subjects in-
cluded (i.e., whether active TB was excluded in all subjects). Seventeen of 21 studies (81%) described their defi nition of the reference standard in detail suf-fi cient to support replication. However, there was still wide variation among studies regarding the criteria used and data provided on the defi nition of confi rmed or probable TB.
Test failure was infrequently reported. IGRA test failure was defi ned as technical errors, failed phlebot-omy or insuffi cient peripheral blood mononuclear cells (T-SPOT.TB). For the TST, failure was defi ned as unread tests. Failure rates ranged from 0% to 7% for QFT-GIT (n = 19), 0% for QFT-G (n = 6), 0% to 21% for T-SPOT.TB (n = 15) and 0% to 11% for TST (n = 20). Average rates of indeterminate results across all studies were respectively 6.5% for QFT-GIT, 6.4% for QFT-G and 3.5% for T-SPOT.TB. In several stud-ies, indeterminate rates >10% were associated with multiple factors such as young age, helminth co-i nfection and immune suppression.32,50,54,68,36,52,87,88,92 In our analysis, a signifi cant correlation of indetermi-nate results with specifi c risk factors could not be

IGRAs and childhood TB: systematic review 5
Table 2 Characteristics of dichotomous and graded expression of M. tuberculosis exposure, sorted by World Bank income index
Author, year, reference
Dichotomous comparison groups
Description ‘exposed’ Description ‘unexposed’
LMIC Hansted, 200951 Household or school contact No TB contact, no symptoms, chest radiography normalHesseling, 200954 Known TB contact No known TB contactMandalakas, 200869 Known household contact No known household contactStefan, 201088 Known TB contact No known TB contact
HIC Bianchi, 200933 TB contacts, Italian and immigrant Immigrants without TB contactChun, 200835 Household contacts Contact outside householdDominguez, 200845 Children from contact investigations TST-positive children detected during routine screening*Higuchi, 200957 Same class as index case (contact ⩾90 h) Same school, different classes from index case (contact
<18 h)Lighter, 200967 Close contact to TB index case No risk factors for TB exposureLucas, 201068 Immigrants with household contact Immigrants without household contact
Graded exposure comparison groups (characteristics of exposure)
Grade 0 Grade 1 Grade 2 Grade 3
LMIC Adetifa, 201026 Different house Different room Same room —Nakaoka, 200673 Community controls Smear− TB Smear+ TB —Okada, 200879 Smear− TB Smear+ TB Smear++ TB Smear+++ TBPetrucci, 200882 Scanty TB Smear+ TB Smear++ TB Smear+++ TB
HIC Bergamini, 200932 Probable TB Smear/culture+ TB Smear+ TB —Diel, 200843 40–59 h exposure 60–99 h exposure 100–199 h exposure ⩾200 h exposureGirardi, 200749 Other students Activities with index case Attending class with index case —
* TST was not used for analysis due to incorporation biasLMIC = low- and middle-income countries; TB = tuberculosis; HIC = high-income countries; − = negative; + = positive; TST = tuberculin skin test.
Table 3 Concordance of tests for M. tuberculosis infection with dichotomized exposure to tuberculosis
TestAuthor, year,
reference
Exposedpositive/
total
Unexposedpositive/
total OR*
Pooled effects OR (95%CI)
Fixed Random
TST 5 mm Bianchi, 200933 19/38 154/289 4.4 1.5 (1.03–2.1) 1.3 (0.7–2.7)Chun, 200835 26/42 16/29 1.3Hansted, 200951† 33/45 36/52 1.2Higuchi, 200957 20/38 186/268 0.5Lucas, 201068 12/26 83/278 2.0Mandalakas, 200869† 0/6 4/17 0.2Stefan, 201088† 0/4 4/30 0.7
TST 10 mm Bianchi, 200933 16/38 31/289 6.0 2.0 (1.4–2.8) 1.9 (0.98–3.8)Chun, 200835 14/42 7/29 1.6Hansted, 200951† 27/45 34/52 0.8Hesseling, 200854† 14/26 1/2 1.2Higuchi, 200957 13/38 77/268 1.3Lighter, 200967‡ 5/13 8/30 4.4Lucas, 201068 8/26 48/278 2.1Stefan, 201088† 0/4 4/30 0.7
TST 15 mm Bianchi, 200933 9/38 16/289 5.3 1.7 (1.00–3.0) 1.8 (0.7–5.0)Hansted, 200951† 11/45 21/52 0.5Lucas, 201068 4/26 18/278 2.6
QuantiFERON®-TB Bianchi, 200933 17/38 35/287 5.8 3.4 (2.3–5.1) 3.5 (1.9–6.7)Chun, 200835 8/42 2/27 2.9Dominguez, 200745 28/64 16/61 3.0Hesseling, 200854† 8/16 0/2 5.0Higuchi, 200957 3/41 3/265 6.9Lighter, 200967‡ 8/13 0/30 94Lucas, 201068 7/33 38/387 2.5Mandalakas, 200869† 0/3 2/9 0.4Stefan, 201088† 0/3 3/26 0.96
T-SPOT®.TB Dominguez, 200745 32/63 13/61 3.8 3.0 (1.8–4.9) 1.3 (0.8–2.3)Hansted, 200951† 8/45 5/52 2.0Hesseling, 200854† 24/25 1/2 24.0Lucas, 201068 6/30 32/382 2.7Mandalakas, 200869† 2/6 4/17 1.6Stefan, 201088† 1/3 5/20 1.5
* In the calculation of ORs, a value of 0.5 was added to all cells if one cell had a 0 value.† Indicates country classifi ed as low-, low and middle or upper middle-income country according to the World Bank. ‡ Three exposure groups defi ned by Lighter et al. However, results from the intermediate group were excluded from analysis, as their exposure was judged too heterogeneous. OR = odds ratio; CI = confi dence interval; TST = tuberculin skin test.
6 The International Journal of Tuberculosis and Lung Disease
shown; there was no difference in the frequency of IGRA indeterminate results in stratifi ed analysis.
Results of review: latent TB infectionTwo longitudinal studies assessed incident active TB.43,57 A school outbreak investigation in Japan as-sessed 313 children with TST and QFT-G tests.57 QFT-G-positive children and QFT-G-indeterminate/TST-positive children received preventive chemother-apy. One year after the index case was reported, all children underwent chest radiography; no child de-veloped active TB during the 3-year follow-up (posi-tive predictive value [PPV] 0%, 95%CI 0–35, nega-tive predictive value [NPV] 100%, 95%CI 0–1.5). German contact investigations assessed 168 children with QFT-GIT and completed approximately 2 years of follow-up.43 Three of seven QFT-GIT-positive chil-dren developed probable TB (PPV 43%, 95%CI 16–75), whereas none of the 161 QFT-GIT-negative chil-dren developed active TB (NPV 100%, 95%CI 0–3).
As seen in Table 3, the pooled ORs (random ef-fects model) for the association of positive TST using respectively 5, 10 or 15 mm cut-offs, with dichoto-mous exposure, was 1.34 (95%CI 0.66–2.72), 1.93 (95%CI 0.98–3.77) and 1.83 (95%CI 0.67–5.02). For QFT-G/QFT-GIT, the pooled OR was 3.51 (95%CI 1.85–6.66) and for T-SPOT.TB it was 1.31 (95%CI 0.76–2.27; Table 3). When the analysis was restricted
to low- and middle-income countries (LMICs), QFT and T-SPOT.TB results were positively correlated with exposure (OR 1.30 and 2.24, respectively), but TST was not (OR 1.04 [95%CI 0.46–2.36], 0.81 [95%CI 0.38–1.74] and 0.48 [only one study] for cut-offs of 5, 10 and 15 mm, respectively).
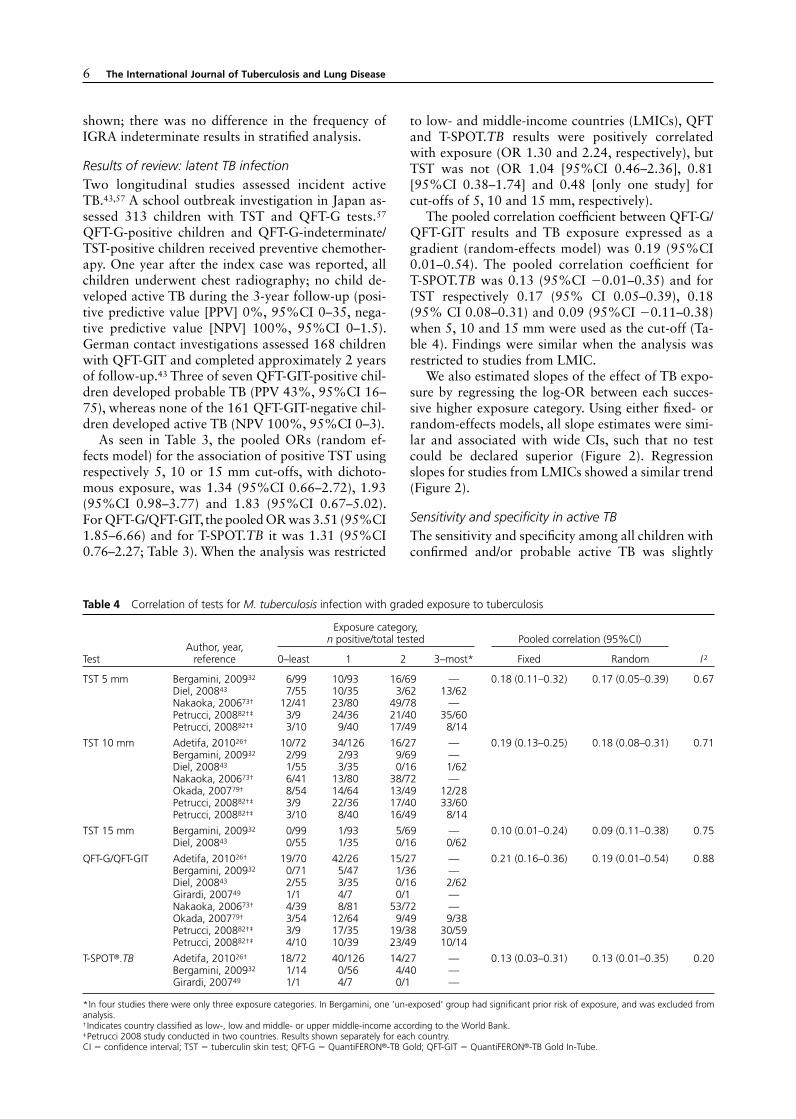
The pooled correlation coeffi cient between QFT-G/ QFT-GIT results and TB exposure expressed as a gradient (random-effects model) was 0.19 (95%CI 0.01–0.54). The pooled correlation coeffi cient for T-SPOT.TB was 0.13 (95%CI −0.01–0.35) and for TST respectively 0.17 (95% CI 0.05–0.39), 0.18 (95% CI 0.08–0.31) and 0.09 (95%CI −0.11–0.38) when 5, 10 and 15 mm were used as the cut-off (Ta-ble 4). Findings were similar when the analysis was restricted to studies from LMIC.
We also estimated slopes of the effect of TB expo-sure by regressing the log-OR between each succes-sive higher exposure category. Using either fi xed- or random-effects models, all slope estimates were simi-lar and associated with wide CIs, such that no test could be declared superior (Figure 2). Regression slopes for studies from LMICs showed a similar trend (Figure 2).
Sensitivity and specifi city in active TBThe sensitivity and specifi city among all children with confi rmed and/or probable active TB was slightly
Table 4 Correlation of tests for M. tuberculosis infection with graded exposure to tuberculosis
TestAuthor, year,
reference
Exposure category, n positive/total tested Pooled correlation (95%CI)
I 20–least 1 2 3–most* Fixed Random
TST 5 mm Bergamini, 200932 6/99 10/93 16/69 — 0.18 (0.11–0.32) 0.17 (0.05–0.39) 0.67Diel, 200843 7/55 10/35 3/62 13/62Nakaoka, 200673† 12/41 23/80 49/78 — Petrucci, 200882†‡ 3/9 24/36 21/40 35/60Petrucci, 200882†‡ 3/10 9/40 17/49 8/14
TST 10 mm Adetifa, 201026† 10/72 34/126 16/27 — 0.19 (0.13–0.25) 0.18 (0.08–0.31) 0.71Bergamini, 200932 2/99 2/93 9/69 —Diel, 200843 1/55 3/35 0/16 1/62Nakaoka, 200673† 6/41 13/80 38/72 —Okada, 200779† 8/54 14/64 13/49 12/28Petrucci, 200882†‡ 3/9 22/36 17/40 33/60Petrucci, 200882†‡ 3/10 8/40 16/49 8/14
TST 15 mm Bergamini, 200932 0/99 1/93 5/69 — 0.10 (0.01–0.24) 0.09 (0.11–0.38) 0.75Diel, 200843 0/55 1/35 0/16 0/62
QFT-G/QFT-GIT Adetifa, 201026† 19/70 42/26 15/27 — 0.21 (0.16–0.36) 0.19 (0.01–0.54) 0.88Bergamini, 200932 0/71 5/47 1/36 —Diel, 200843 2/55 3/35 0/16 2/62Girardi, 200749 1/1 4/7 0/1 —Nakaoka, 200673† 4/39 8/81 53/72 —Okada, 200779† 3/54 12/64 9/49 9/38Petrucci, 200882†‡ 3/9 17/35 19/38 30/59Petrucci, 200882†‡ 4/10 10/39 23/49 10/14
T-SPOT®.TB Adetifa, 201026† 18/72 40/126 14/27 — 0.13 (0.03–0.31) 0.13 (0.01–0.35) 0.20Bergamini, 200932 1/14 0/56 4/40 —Girardi, 200749 1/1 4/7 0/1 —
* In four studies there were only three exposure categories. In Bergamini, one ‘un-exposed’ group had signifi cant prior risk of exposure, and was excluded from analysis.† Indicates country classifi ed as low-, low and middle- or upper middle-income according to the World Bank. ‡ Petrucci 2008 study conducted in two countries. Results shown separately for each country. CI = confi dence interval; TST = tuberculin skin test; QFT-G = QuantiFERON®-TB Gold; QFT-GIT = QuantiFERON®-TB Gold In-Tube.
IGRAs and childhood TB: systematic review 7
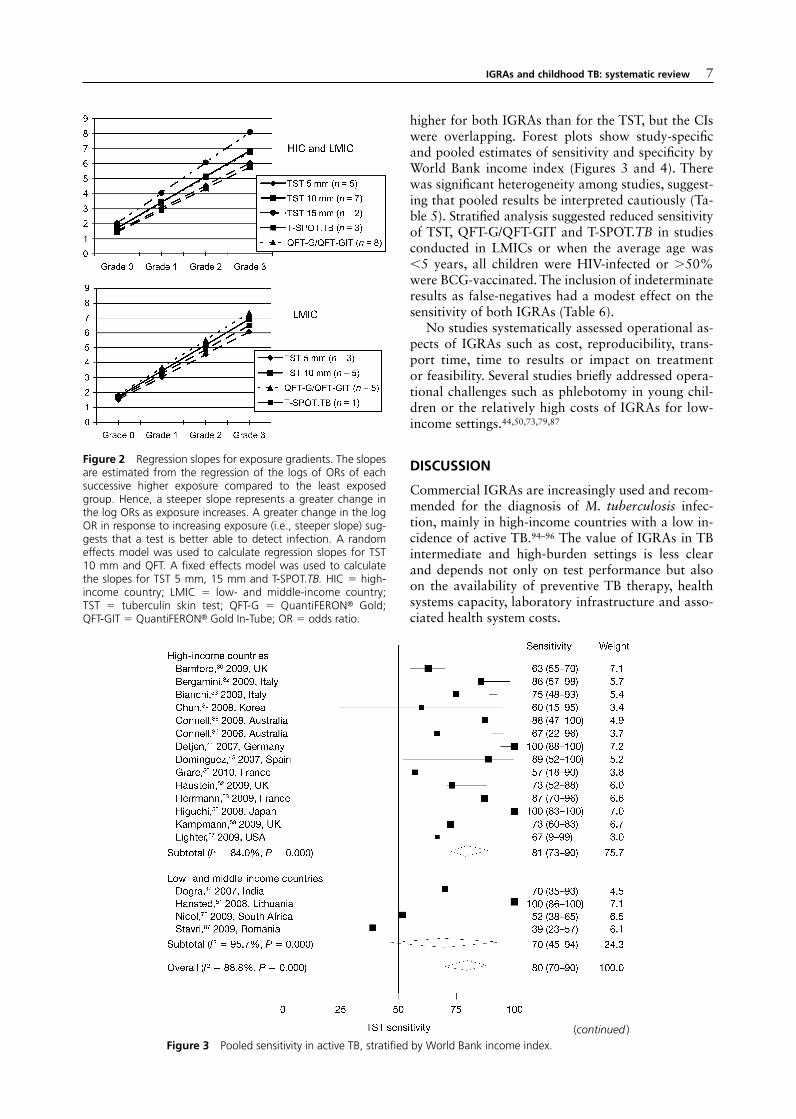
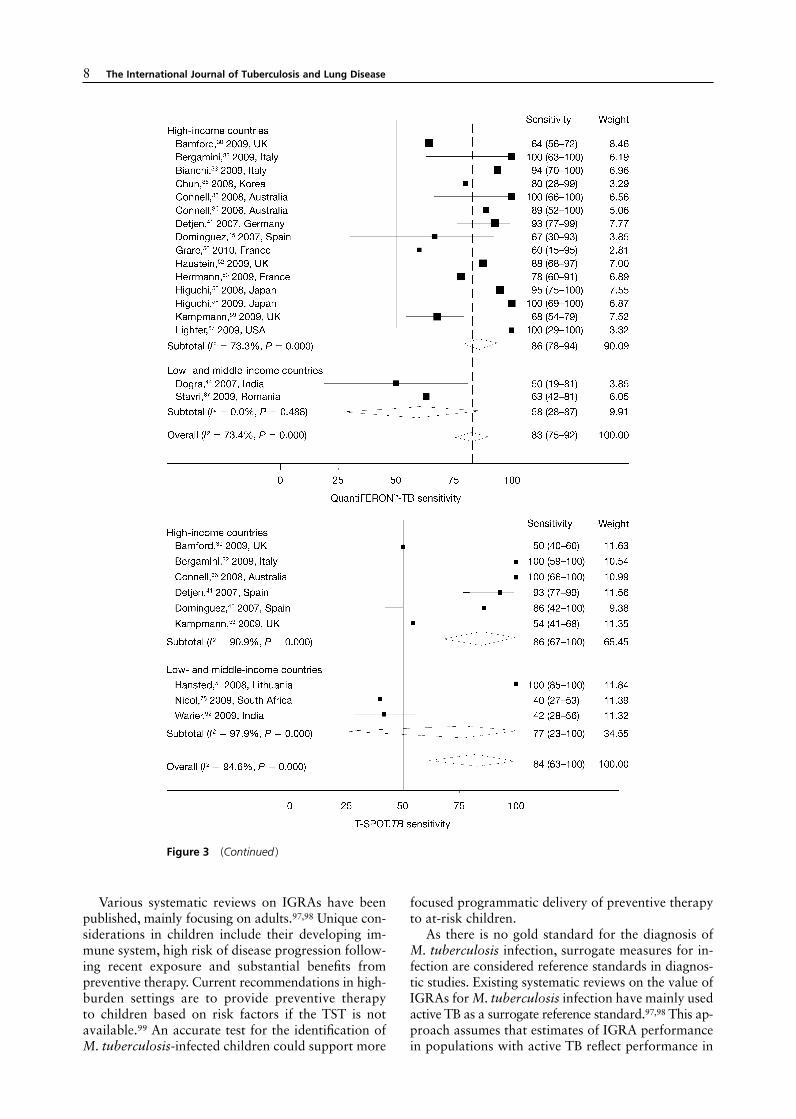
higher for both IGRAs than for the TST, but the CIs were overlapping. Forest plots show study-specifi c and pooled estimates of sensitivity and specifi city by World Bank income index (Figures 3 and 4). There was signifi cant heterogeneity among studies, suggest-ing that pooled results be interpreted cautiously (Ta-ble 5). Stratifi ed analysis suggested reduced sensitivity of TST, QFT-G/QFT-GIT and T-SPOT.TB in studies conducted in LMICs or when the average age was <5 years, all children were HIV-infected or >50% were BCG-vaccinated. The inclusion of indeterminate results as false-negatives had a modest effect on the sensitivity of both IGRAs (Table 6).
No studies systematically assessed operational as-pects of IGRAs such as cost, reproducibility, trans-port time, time to results or impact on treatment or feasibility. Several studies briefl y addressed opera-tional challenges such as phlebotomy in young chil-dren or the relatively high costs of IGRAs for low-income settings.44,50,73,79,87
DISCUSSION
Commercial IGRAs are increasingly used and recom-mended for the diagnosis of M. tuberculosis infec-tion, mainly in high-income countries with a low in-cidence of active TB.94–96 The value of IGRAs in TB intermediate and high-burden settings is less clear and depends not only on test performance but also on the availability of preventive TB therapy, health systems capacity, laboratory infrastructure and asso-ciated health system costs.
Figure 2 Regression slopes for exposure gradients. The slopes are estimated from the regression of the logs of ORs of each successive higher exposure compared to the least exposed group. Hence, a steeper slope represents a greater change in the log ORs as exposure increases. A greater change in the log OR in response to increasing exposure (i.e., steeper slope) sug-gests that a test is better able to detect infection. A random effects model was used to calculate regression slopes for TST 10 mm and QFT. A fi xed effects model was used to calculate the slopes for TST 5 mm, 15 mm and T-SPOT.TB. HIC = high-income country; LMIC = low- and middle-income country; TST = tuberculin skin test; QFT-G = QuantiFERON® Gold; QFT-GIT = QuantiFERON® Gold In-Tube; OR = odds ratio.
Figure 3 Pooled sensitivity in active TB, stratifi ed by World Bank income index.(continued )
8 The International Journal of Tuberculosis and Lung Disease
Figure 3 (Continued )
Various systematic reviews on IGRAs have been published, mainly focusing on adults.97,98 Unique con-siderations in children include their developing im-mune system, high risk of disease progression follow-ing recent exposure and substantial benefi ts from preventive therapy. Current recommendations in high-burden settings are to provide preventive therapy to children based on risk factors if the TST is not available.99 An accurate test for the identifi cation of M. tuberculosis-infected children could support more
focused programmatic delivery of preventive therapy to at-risk children.
As there is no gold standard for the diagnosis of M. tuberculosis infection, surrogate measures for in-fection are considered reference standards in diagnos-tic studies. Existing systematic reviews on the value of IGRAs for M. tuberculosis infection have mainly used active TB as a surrogate reference standard.97,98 This ap-proach assumes that estimates of IGRA performance in populations with active TB refl ect performance in

IGRAs and childhood TB: systematic review 9
Figure 4 Pooled specifi city in active TB, stratifi ed by World Bank income index.

10 The International Journal of Tuberculosis and Lung Disease
populations with infection. Not only does the im-mune status of diseased persons differ from that of infected persons, but populations evaluated for active TB differ greatly from populations evaluated for in-fection. For M. tuberculosis i nfection, this review therefore used two reference standards, incident TB and TB exposure, which were considered superior surrogate measures of infection.
A test identifying individuals at highest risk for disease progression would greatly aid in the selection of individuals who would most benefi t from preven-tive therapy. Longitudinal studies using incident TB as the reference standard are therefore ideal. We iden-tifi ed two studies completed in high-income countries that employed this reference standard using commer-cial IGRAs. These studies, which included very small sample sizes of QFT-positive children, showed a weak association between positive QFT assays and sub-sequent active TB, suggesting low PPVs.43,57 Non-commercial ELISpot assays (not included in this re-view) have also shown performance similar to the TST in longitudinal studies assessing incident TB.29,100
Exposure to M. tuberculosis increases the likeli-hood of infection. A strong correlation of the index test with exposure therefore suggests that the index test can identify people most likely to benefi t from preventive therapy. We compared the performance of the IGRAs and the TST in exposed vs. unexposed in-dividuals as well as across a gradient of exposure and found comparable performance between all tests us-ing both methodological approaches.
Our analysis compared differences in exposure
gradients (our gold standard comparison) rather than absolute exposure. Although studies used different selection methods and measure of exposure, we ana-lyzed studies collectively by defi ning study-specifi c gradients that progressed from the least to highest exposure. In theory, a steeper slope in the regression analysis is associated with a greater change in odds across exposure categories, indicating increased abil-ity of the test to distinguish infection across expo-sure categories. Of note, differences between expo-sure grades were sometimes subtle (e.g., exposure to smear+ vs. smear++ TB); the expected magnitude of the test effect is therefore unclear. Despite the meth-odological heterogeneity of study groups, we found a positive and increasing correlation between each test and each progressive grade of exposure. This correla-tion would be stronger if studies used a standard-ized tool to measure TB exposure. However, despite the heterogeneous nature of the studies, our analysis clearly illustrates that both the IGRAs and the TST have the ability to detect M. tuberculosis infection.
In studies reviewed for dichotomous exposure, the overall odds of a positive QFT-G or QFT-GIT was higher in exposed than unexposed children (OR 3.51, 95%CI 1.85–6.66). QFT may differentiate be-tween these two groups more accurately than the TST (10 mm cut-off) and T-SPOT.TB (OR 1.93, 95%CI 0.98–3.77 and OR 1.31, 95%CI 0.76–2.27, respectively). Nevertheless, the wide and overlapping CIs preclude identifi cation of a superior test and highlight the signifi cant heterogeneity among studies. Studies were performed in countries and populations
Table 5 Characteristic of comparison groups for active TB, sorted by World Bank income index
Author, year, reference Active TB category* No TB category†
LMIC Dogra, 200744 Defi nite/probable TB combined Hospitalized children with clinical suspicion of TB or TB contact, TB disease was ruled out
Warier, 200992 Defi nite TB, probable TB Hospitalized children with other diagnosis, no TB contactHansted, 200951 Defi nite TB Reported group not usedNicol, 200975 Defi nite/probable TB combined Children admitted for either clinically suspected TB or TB
contact, active TB ruled out by CXR and cultureStavri, 200987 Defi nite TB No group reported
HIC Bamford, 200930 Defi nite TB, probable TB No group reportedBergamini, 200932 Defi nite/probable TB combined Reported group not usedBianchi, 200933 Defi nite/probable TB combined Reported group not usedChun, 200835 Probable TB TB ruled out, other diagnosisConnell, 200636 Defi nite/probable TB combined Reported group not usedConnell, 200838 Probable TB Reported group not usedDetjen, 200741 Defi nite TB Children with other respiratory illness, low risk for TBDominguez, 200845 Defi nite/probable TB combined Reported group not usedGrare, 201050 Defi nite/probable TB combined Reported group not usedHaustein, 200952 Defi nite TB, probable TB Reported group not usedHerrmann, 200953 Defi nite/probable TB combined Children hospitalized for any other disease, no TB contactHiguchi, 200855 Defi nite/probable TB combined
(detected in school outbreak)School outbreak investigation, active TB excluded by CXR
Higuchi, 200958 Defi nite/probable TB combined Reported group not usedKampmann, 200959 Defi nite TB, probable TB Children with risk factors for TB but disease ruled out,
other diagnosis madeLighter, 200967 Defi nite/probable TB combined Reported group not used
* Defi nite TB = culture-confi rmed disease, probable TB = diagnosis made on the basis of symptoms and radiologic fi ndings, no culture result. Defi nite/probable combined = some cases confi rmed but others diagnosed on clinical and radiological criteria only, and results not stratifi ed by method of diagnosis. † No TB = active TB systematically excluded in either TB suspects with symptoms suggestive of active TB, or TB contacts. No group reported = study assessed active TB group only. Reported group not used = reported control group did not meet review criteria for an appropriate control group.TB = tuberculosis; LMIC = low- and middle-income countries; CXR = chest radiography; HIC = high-income countries.

Table 6 Diagnostic accuracy of TST, QFT and T-SPOT.TB for defi nite and/or probable active TB stratifi ed by key variables
Sensitivity (true-positives) Specifi city (false-positives)
n
Positive/testedn/N
Sensitivity % (95%CI) n
Positive/testedn/N
Specifi city % (95%CI)
TST Overall* 18 373/534 80 (70–90) 6 105/362 85 (63–100) TST, mm 5 13 220/265 91 (84–98) 4 104/217 70 (17–100) 10 15 248/321 84 (75–93) 5 86/276 88 (62–100) 15 11 246/389 67 (50–83) 3 44/131 92 (71–100) World Bank income index HIC 14 299/407 81 (73–90) 4 94/217 79 (39–100) LMIC 4 74/127 70 (45–94) 2 11/145 93 (77–100) TB incidence†
<25 13 296/402 83 (73–93) 3 75/131 75 (36–100) ⩾25 5 77/132 68 (39–84) 3 30/231 76 (71–100) BCG vaccination, %‡
<50 6 57/66 85 (70–100) 1 0/22 100 (85–100) ⩾50 12 316/468 77 (65–90) 5 105/340 77 (50–100) Age, years <5 5 77/113 77 (57–98) 3 27/158 92 (75–100) ⩾5 13 296/421 81 (69–93) 3 78/204 74 (35–100) HIV prevalence, % <15† 17 359/498 81 (73–90) 6 105/362 85 (63–100) 100 1 14/36 39 (0–92) 0 — —
QFT (QFT-G and QFT-GIT unless otherwise specifi ed) Overall 17 320/431 83 (75–92) 6 71/323 91 (78–100) Overall, indeterminates§ 17 320/462 82 (71–92) — — — QFT test type QFT-G 5 63/74 92 (82–100) 1 53/82 35 (0–80) QFT-GIT 13 272/393 77 (65–88) 6 66/568 92 (86–100) World Bank income index HIC 15 298/394 86 (78–94) 5 65/228 91 (74–100) LMIC 2 22/37 58 (28–87) 1 6/95 94 (71–100) TB incidence†
<25 14 294/389 86 (78–93) 4 64/157 82 (59–100) ⩾25 3 26/42 68 (34–78) 2 6/166 72 (19–100) BCG vaccination, %‡
<50 6 57/62 93 (85–100) 1 0/21 100 (84–100) ⩾50 11 263/369 78 (68–87) 5 71/302 87 (69–100) Age, years <5 4 54/58 94 (86–100) 2 1/92 99 (57–100) ⩾5 13 266/373 81 (69–92) 4 70/231 79 (66–100) HIV prevalence, %¶
<15† 16 303/404 84 (76–92) 6 71/323 91 (78–100) 100 1 17/27 63 (16–100) 0 0 — T-SPOT.®TB Overall 9 194/336 84 (63–100) 4 12/143 94 (87–100) Overall, indeterminates§ 9 194/347 81 (59–100) — — — World Bank income index HIC 6 126/202 86 (67–100) 2 3/46 95 (84–100) LMIC 3 68/134 77 (23–100) 2 9/97 93 (83–100) TB incidence†
<25 6 126/202 87 (68–100) 2 3/46 95 (86–100) ⩾25 3 68/134 73 (29–100) 2 9/97 93 (83–100) BCG vaccination, %‡
<50 3 42/44 97 (92–100) 1 0/21 100 (84–100) ⩾50 5 130/239 69 (45–93) 3 11/75 87 (53–100) Age, years <5 2 49/86 74 (23–100) 2 8/71 92 (80–100) ⩾5 7 145/250 86 (65–100) 2 4/72 95 (88–100) HIV prevalence, %¶
<15† 9 194/336 84 (63–100) 4 12/143 94 (87–100) 100 0 0 — 0 0 —
* For overall and stratifi ed analysis, a TST cut-off of 10 mm was preferentially used; for two studies, TST 5 mm data were used and for one study, TST 15 mm data were used as these were the only data available; one of these studies was conducted in HIV-infected children.† Incidence of smear-positive TB per 100 000 population reported by the WHO in 2007.‡ These data indicate the proportion of BCG-vaccinated within the subgroup used for analysis. BCG vaccination information not provided in one study; study was categorized as >50% BCG vaccinated as national guidelines recommend neonatal.§ Indeterminate results were included as false-negative in this analysis of the all TB group. Indeterminates were excluded for all other analysis.¶ HIV prevalence in study population. If HIV status of subjects not reported, study was categorized as having <15% of subjects HIV-infected.TST = tuberculin skin test; QFT = QuantiFERON®-TB; TB = tuberculosis; CI = confi dence interval; BCG = bacille-Calmette Guerin; HIV = human immuno-defi ciency virus; QFT-G = QuantiFERON®-TB Gold; QFT-GIT = QuantiFERON®-TB Gold In-Tube; WHO = World Health Organization.

12 The International Journal of Tuberculosis and Lung Disease
with different annual risk of TB infection and other factors modifying the risk of infection, such as diag-nostic delay and strain type. The categories ‘unex-posed’ and ‘exposed’ therefore describe very different populations in each study. Sub-group analysis, in-cluding World Bank income status, did not suggest possible explanations for differences in estimates of test performance. By comparing studies with similar methodological approaches and comparable study populations, the correlation of either test with expo-sure would be stronger and differences between tests might become apparent.
For the diagnosis of active TB, the overall sensi-tivity of both IGRAs and the TST was similar when assessed in children with all categories of active TB combined. Our results suggest that TST and QFT sensitivity may be higher in children with defi nite TB compared to children with defi nite and probable TB. Although estimates of test sensitivity are most certain in the defi nite TB group, study-specifi c case defi ni-tions of probable TB varied considerably and might have introduced differential bias among studies. The assessment of test performance in children with all categories of active TB is thus most representative of clinical practice and provides useful insight upon which to base clinical guidelines. Overall, the ability of either TST or IGRAs was suboptimal to ‘rule in’ or ‘rule out’ active TB, reinforcing the appropriate use of these tests as adjuncts in the clinical diagnosis of active TB.
Young children have an increased risk of develop-ing active TB after infection, which may indicate dif-ferences in the pediatric immune system compared to adults. Individual studies have suggested poorer sen-sitivity and higher rates of indeterminate results in children aged <5 years, who could most benefi t from accurate detection of M. tuberculosis infection.32,50,54,59 Similarly, our stratifi ed analysis found a trend towards lower sensitivity of all tests in studies assessing children younger than vs. older than 5 years. Nevertheless, the small number of studies completed in younger chil-dren and the lack of data reported by age strata lim-ited our ability to demonstrate a statistically signifi -cant difference. Our review clearly highlights the need for more data on test performance in young children.
Trends in subgroup and stratifi ed analysis suggest that the sensitivity of all tests for the diagnosis of dis-ease may be dependent on the study setting and pop-ulation. The sensitivity of all tests may be higher in high-income countries, and T-SPOT.TB could be the most sensitive in LMICs, although more robust data are needed.
In contrast, all tests may have lower sensitivity in HIV-infected children. Indeterminate results may lower the sensitivity of IGRAs slightly. Most interest-ing was a tendency towards lower sensitivity of all tests in study populations with >50% BCG coverage. Although BCG vaccination can explain differences in specifi city between TST and IGRAs, BCG is not ex-
pected to infl uence sensitivity. We note that BCG cov-erage is high in countries with higher TB burden or among immigrants in low-burden settings. Popula-tions with higher BCG coverage rates may also have higher rates of underlying conditions that may impair test accuracy, such as co-infections with helminths and malnutrition.68 Although small subgroup sample sizes limited our ability to demonstrate statistically signifi cant differences, trends in sub-group analysis highlight important factors to consider when choos-ing a preferred testing strategy in different settings or patient groups or targeting research areas.
Operational aspects and feasibility are important considerations when contemplating the programmatic implementation of a diagnostic test, particularly in resource-constrained settings. We aimed to assess some important aspects such as cost, transport times, re-producibility and feasibility in this systematic review, but studies rarely addressed operational aspects of study implementation or test performance. Future studies should assess operational aspects and feasibil-ity of IGRAs to comprehensively inform guidelines regarding their use in children.
Our review had limitations. In addition to those previously discussed, the studies included assessed very different populations in diverse settings. Sample sizes were less than 10 in some subgroup analyses, limiting our ability to generalize these subgroup re-sults. The tremendous variation in methodological approaches and the use of non-uniform reference stan-dards led to signifi cant analytic heterogeneity. Never-theless, we used a variety of analytic approaches to improve the robustness of our fi ndings. A limited num-ber of studies employed an acceptable defi nition of the non-diseased group, limiting our power to esti-mate specifi city.
Although additional data in children exist on in-house assays and pre-commercial versions of current IGRAs, this review focused on two standardized com-mercial IGRAs, which are the most widely used and have recently been considered for policy guidance and programmatic implementation.
This review found that TST, QFT and T-SPOT.TB had similar accuracy for the diagnosis of M. tubercu-losis infection and active TB in children. Diverse study methodologies limited the comparability of studies and interpretation of results, emphasizing the importance of rigorous, standardized approaches for the evaluation of TB diagnostic tests in children. Well-defi ned exposure gradients serve as a good surrogate reference standard for M. tuberculosis infection and patient-important outcomes. Based on the evidence generated by this review, the WHO’s Strategic and Technical Advisory Group for TB (STAG-TB) has dis-couraged the use of IGRAs for the diagnosis of active TB and M. tuberculosis infection in children living in LMICs.101
There is a clear need for more coordinated re-search on the value of IGRAs in different pediatric

IGRAs and childhood TB: systematic review 13
populations in settings with high burden of TB and HIV. Although we were not able to determine a supe-rior test, our analysis confi rms that the TST and both IGRAs are able to identify children with M. tubercu-losis infection. In settings with high burdens of TB, accurate identifi cation of children with M. tuberculo-sis infection may help guide the targeted delivery of isoniazid preventive therapy (IPT), and might im-prove the cost-effectiveness of IPT. Children of all ages, but particularly very young and HIV-infected children with the highest risk of disease progression, stand to benefi t most from TB preventive therapy. Al-though the limited available data did not support a meaningful comparison of test performance for the TST and the commercial IGRAs in these subgroups of vulnerable children, more high-quality diagnostic studies and cost-effectiveness analyses are needed to inform recommendations regarding IGRA use in these high-risk groups.
There was suffi cient data to assess test perfor-mance in the diagnosis of active TB. Our analysis demonstrated that neither the TST nor the IGRAs perform suffi ciently to ‘rule in’ or ‘rule out’ active TB as a single test. Our fi ndings reinforce the acceptable use of these tests as adjuncts in the clinical diagnosis of active TB where resources are suffi cient to support the use of a test for infection.
AcknowledgementsThe authors thank the studies’ authors for kindly providing ad-ditional information upon request, including I Adetifa, S Arend, P Beffa, A Bose, T Connell, R Diel, G Dixon, J Dominguez, M Grare, K Higuchi, Y Kang, Y Kobashi, B Kampman, Y Lee, W Lew, M Losi, M Lucas, P Mantegani, B McKinnon, A Nienhaus, R Petrucci, H Pollack and E Tavast. The authors thank M P McGraw, Case Western Reserve University, for support to com-plete their electronic literature search and K Steingart for helpful discussions on QUADAS. This systematic review was made possi-ble by the generous support of the American people through the United States Agency for International Development (USAID) un-der Cooperative Agreement GHN-A-00-08-00004-00. The con-tents are the responsibility of the authors and do not necessarily refl ect the views of USAID or the United States Government. DM and AB receive salary support from Fond de la recherche en Santé de Québec. AM receives salary support from the US Department of State Fulbright Senior Scholars program. The funding agencies had no role in the preparation or submission of this report.
References 1 Dolin P J, Raviglione M C, Kochi A. Global tuberculosis inci-
dence and mortality during 1990–2000. Bull World Health Organ 1994; 72: 213–220.
2 Corbett E L, Watt C J, Walker N, et al. The growing burden of tuberculosis: global trends and interactions with the HIV epi-demic. Arch Intern Med 2003; 163: 1009–1021.
3 Marais B J, Gie R P, Schaaf H S, et al. The natural history of childhood intra-thoracic tuberculosis: a critical review of liter-ature from the pre-chemotherapy era. Int J Tuberc Lung Dis 2004; 8: 392–402.
4 Hesseling A C, Cotton M F, Jennings T, et al. High incidence of tuberculosis among HIV-infected infants: evidence from a South African population-based study highlights the need for improved tuberculosis control strategies. Clin Infect Dis 2009; 48: 108–114.
5 Anastos K, Kalish L A, Palacio H, et al. Prevalence of and risk factors for tuberculin positivity and skin test anergy in HIV-1-infected and uninfected at-risk women. Women’s Interagency HIV Study (WIHS). J Acquir Immune Defi c Syndr 1999; 21: 141–147.
6 Anonymous. CDC changing position on anergy testing, ther-apy. Centers for Disease Control and Prevention. AIDS Alert 1997; 12: 117–118.
7 Graham N M, Nelson K E, Solomon L, et al. Prevalence of tu-berculin positivity and skin test anergy in HIV-1-seropositive and -seronegative intravenous drug users [Comment]. JAMA 1992; 267: 369–373.
8 Huebner R E, Schein M F, Hall C A, Barnes S A. Delayed-type hypersensitivity anergy in human immunodefi ciency virus-i nfected persons screened for infection with Mycobacterium tuberculosis. Clin Infect Dis 1994; 19: 26–32.
9 Karalliedde S, Katugaha L P, Uragoda C G. Tuberculin re-sponse of Sri Lankan children after BCG vaccination at birth. Tubercle 1987; 68: 33–38.
10 Klein R S, Flanigan T, Schuman P, Smith D, Vlahov D. Criteria for assessing cutaneous anergy in women with or at risk for HIV infection. HIV Epidemiologic Research Study Group [Comment]. J Allergy Clin Immunol 1999; 103: 93–98.
11 Lavin J, Haidorfer C. Anergy testing⎯a vital weapon. RN 1993; 56: 31–32; quiz 3.
12 Miller W C, Thielman N M, Swai N, et al. Delayed-type hyper-sensitivity testing in Tanzanian adults with HIV infection. J Acquir Immune Defi c Syndr Hum Retrovirol 1996; 12: 303–308.
13 Pesanti E L. The negative tuberculin test. Tuberculin, HIV and anergy panels. Am J Respir Crit Care Med 1994; 149: 1699–1709.
14 Wright P W, Crutcher J E, Holiday D B. Selection of skin test antigens to evaluate PPD anergy. J Fam Pract 1995; 41: 59–64.
15 Hesseling A C, Schaaf H S, Gie R P, Starke J R, Beyers N. A critical review of diagnostic approaches used in the diagnosis of childhood tuberculosis. Int J Tuberc Lung Dis 2002; 6: 1038–1045.
16 Hesseling A C, Mandalakas A M, Kirchner L H, et al. Highly discordant T-cell responses in individuals with recent house-hold tuberculosis exposure. Thorax 2008; 64: 840–846.
17 Lienhardt C, Sillah J, Fielding K, et al. Risk factors for tubercu-losis infection in children in contact with infectious tuberculo-sis cases in the Gambia, West Africa. Pediatrics 2003; 111: e608–614.
18 Whiting P, Rutjes A W, Reitsma J B, Bossuyt P M, Kleijnen J. The development of QUADAS: a tool for the quality assess-ment of studies of diagnostic accuracy included in systematic reviews. BMC Med Res Methodol 2003; 3: 25.
19 Reitsma J B, Rutjes A W S, Whiting P, Vlassow V V, Leefl ang M M G, Deeks J J. Chapter 9: Assessing methodological qua-lity. In: Deeks J J, Bossuyt P M, Gatsonis C, eds. Cochrane hand-book for systematic reviews of diagnostic test accuracy version 1.0.0. London, UK: Cochrane Collaboration, 2009.
20 Higgins J P, Thompson S G. Quantifying heterogeneity in a meta-analysis. Stat Med 2002; 21: 1539–1558.
21 Diener M J, Hilsenroth M J, Weinberger J. A primer on meta-analysis of correlation coeffi cients: the relationship between patient-reported therapeutic alliance and adult attachment style as an illustration. Psychother Res 2009; 19: 519–526.
22 Schlattmann P. Medical applications of fi nite mixture models, statistics for biology and health. Chapter 7: Investigating and analyzing heterogeneity in meta-analysis. Berlin, Heidelberg: Springer Verlag, 2009.
23 Greenland S, Longnecker M P. Methods for trend estimation from summarized dose-response data, with applications to meta-analysis. Am J Epidemiol 1992; 135: 1301–1309.
24 Hamza T H, van Houwelingen H C, Stijnen T. The binomial distribution of meta-analysis was preferred to model within-study variability. J Clin Epidemiol 2008; 61: 41–51.

14 The International Journal of Tuberculosis and Lung Disease
25 Higgins J P, Thompson S G. Controlling the risk of spurious fi ndings from meta-regression. Stat Med 2004; 23: 1663–1682.
26 Adetifa I M, Ota M O, Jeffries D J, et al. Commercial inter-feron gamma release assays compared to the tuberculin skin test for diagnosis of latent Mycobacterium tuberculosis infec-tion in childhood contacts in the Gambia. Pediatr Infect Dis J 2010; 29: 439–443.
27 Adetifa I M O, Lugos M D, Hammond A, et al. Comparison of two interferon gamma release assays in the diagnosis of Myco-bacterium tuberculosis infection and disease in The Gambia. BMC Infect Dis 2007; 7: 122.
28 Arend S M, Thijsen S F, Leyten E M, et al. Comparison of two interferon-gamma assays and tuberculin skin test for tracing tuberculosis contacts. Am J Respir Crit Care Med 2007; 175: 618–627.
29 Bakir M, Millington K A, Soysal A, et al. Prognostic value of a T-cell-based, interferon-gamma biomarker in children with tu-berculosis contact. Ann Intern Med 2008; 149: 777–787.
30 Bamford A R, Crook A M, Clark J, et al. Comparison of i nterferon-gamma release assays and tuberculin skin test in pre-dicting active tuberculosis (TB) in children in the UK—a paedi-atric TB network study. Arch Dis Child 2010; 95: 180–186.
31 Beffa P, Zellweger A, Janssens J P, Wrighton-Smith P, Zellweger J P. Indeterminate test results of T-SPOTTM.TB performed un-der routine fi eld conditions. Eur Respir J 2008; 31: 842–846.
32 Bergamini B M, Losi M, Vaienti F, et al. Performance of commer-cial blood tests for the diagnosis of latent tuberculosis infection in children and adolescents. Pediatrics 2009; 123: e419–e424.
33 Bianchi L, Galli L, Moriondo M, et al. Interferon-gamma re-lease assay improves the diagnosis of tuberculosis in children. Pediatr Infect Dis J 2009; 28: 510–514.
34 Bruzzese E, Bocchino M, Assante L R, et al. Gamma interferon release assays for diagnosis of tuberculosis infection in immune-compromised children in a country in which the prevalence of tuberculosis is low. J Clin Microbiol 2009; 47: 2355–2357.
35 Chun J K, Kim C K, Kim H S, et al. The role of a whole blood interferon-gamma assay for the detection of latent tuberculosis infection in bacille Calmette-Guerin-vaccinated children. Diagn Microbiol Infect Dis 2008; 62: 389–394.
36 Connell T G, Curtis N, Ranganathan S C, Buttery J P. Perfor-mance of a whole blood interferon gamma assay for detecting latent infection with Mycobacterium tuberculosis in children. Thorax 2006; 61: 616–620.
37 Connell T G, Davies M A, Johannisen C, et al. Reversion and conversion of Mycobacterium tuberculosis IFN-gamma ELISpot results during anti-tuberculous treatment in HIV-infected chil-dren. BMC Infect Dis 2010; 10: 138.
38 Connell T G, Ritz N, Paxton G A, Buttery J P, Curtis N, Ranga-nathan S C. A three-way comparison of tuberculin skin testing, QuantiFERON-TB Gold and T-SPOT.TB in children. PLoS One 2008; 3: e2624.
39 Connell T G, Tebruegge M, Ritz N, Bryant P A, Leslie D, Cur-tis N. Indeterminate interferon-gamma release assay results in children. Pediatr Infect Dis J 2010; 29: 285–286.
40 Davies M A, Connell T, Johannisen C, et al. Detection of tu-berculosis in HIV-infected children using an enzyme-linked immunospot assay. AIDS 2009; 23: 961–969.
41 Detjen A K, Keil T, Roll S, et al. Interferon-gamma release as-says improve the diagnosis of tuberculosis and nontuberculous mycobacterial disease in children in a country with a low inci-dence of tuberculosis. Clin Infect Dis 2007; 45: 322–328.
42 Dewan P K, Grinsdale J, Kawamura L M. Low sensitivity of a whole-blood interferon-gamma release assay for detection of active tuberculosis. Clin Infect Dis 2007; 44: 69–73.
43 Diel R, Loddenkemper R, Meywald-Walter K, Niemann S, Nienhaus A. Predictive value of a whole blood IFN-gamma as-say for the development of active tuberculosis disease after re-cent infection with Mycobacterium tuberculosis. Am J Respir Crit Care Med 2008; 177: 1164–1170.
44 Dogra S, Narang P, Mendiratta D K, et al. Comparison of a whole blood interferon-gamma assay with tuberculin skin test-ing for the detection of tuberculosis infection in hospitalized children in rural India. J Infect 2007; 54: 267–276.
45 Dominguez J, Ruiz-Manzano J, De Souza-Galvao M, et al. Comparison of two commercially available gamma interferon blood tests for immunodiagnosis of tuberculosis. Clin Vaccine Immunol 2008; 15: 168–171.
46 Eisenhut M, Paranjothy S, Abubakar I, et al. BCG vaccination reduces risk of infection with Mycobacterium tuberculosis as detected by gamma interferon release assay. Vaccine 2009; 27: 6116–6120.
47 Ferrara G, Losi M, D’Amico R, et al. Use in routine clinical practice of two commercial blood tests for diagnosis of infec-tion with Mycobacterium tuberculosis: a prospective study. Lancet 2006; 367: 1328–1334.
48 Ferrara G, Losi M, Meacci M, et al. Routine hospital use of a new commercial whole blood interferon-gamma assay for the diagnosis of tuberculosis infection. Am J Respir Crit Care Med 2005; 172: 631–635.
49 Girardi E, Loffredo M, Alessandrini A, Anzidei G, Goletti D. A two-step approach for screening contacts of active tuberculo-sis. Infection 2007; 35: 122–123.
50 Grare M, Derelle J, Dailloux M, Laurain C. QuantiFERON®-TB Gold In-Tube as help for the diagnosis of tuberculosis in a French pediatric hospital. Diagn Microbiol Infect Dis 2010; 66: 366–372.
51 Hansted E, Andriuskeviciene A, Sakalauskas R, Kevalas R, Sit-kauskiene B. T-cell-based diagnosis of tuberculosis infection in children in Lithuania: a country of high incidence despite a high coverage with bacille Calmette-Guerin vaccination. BMC Pulm Med 2009; 9: 41.
52 Haustein T, Ridout D A, Hartley J C, et al. The likelihood of an indeterminate test result from a whole-blood interferon-gamma release assay for the diagnosis of Mycobacterium tuberculosis infection in children correlates with age and immune status. Pediatr Infect Dis J 2009; 28: 669–673.
53 Herrmann J L, Belloy M, Porcher R, et al. Temporal dynamics of interferon gamma responses in children evaluated for tuber-culosis. PLoS One 2009; 4: e4130.
54 Hesseling A C, Mandalakas A M, Kirchner H L, et al. Highly discordant T-cell responses in individuals with recent exposure to household tuberculosis. Thorax 2009; 64: 840–846.
55 Higuchi K, Harada N, Fukazawa K, Mori T. Relationship be-tween whole-blood interferon-gamma responses and the risk of active tuberculosis. Tuberculosis (Edinb) 2008; 88: 244–248.
56 Higuchi K, Harada N, Mori T, Sekiya Y. Use of QuantiFERON-TB Gold to investigate tuberculosis contacts in a high school. Respirology 2007; 12: 88–92.
57 Higuchi K, Kondo S, Wada M, et al. Contact investigation in a primary school using a whole blood interferon-gamma assay. J Infect 2009; 58: 352–357.
58 Higuchi R, Mori M, Ozawa R, et al. Whole blood interferon-gamma assay for tuberculosis in children in Japan. Pediatr Intern 2009; 51: 97–102.
59 Kampmann B, Whittaker E, Williams A, et al. Interferon-gamma release assays do not identify more children with active tuber-culosis than the tuberculin skin test. Eur Respir J 2009; 33: 1374–1382.
60 Kang Y A, Lee H W, Hwang S S, et al. Usefulness of whole-blood interferon-gamma assay and interferon-gamma enzyme-linked immunospot assay in the diagnosis of active pulmonary tuberculosis. Chest 2007; 132: 959–965.
61 Kobashi Y, Mouri K, Miyashita N, et al. QuantiFERON TB-2G test for patients with active tuberculosis stratifi ed by age groups. Scan J Infect Dis 2009; 41: 841–846.
62 Kobashi Y, Mouri K, Obase Y, Fukuda M, Miyashita N, Oka M. Clinical evaluation of QuantiFERON TB-2G test for immunocompromised patients. Eur Respir J 2007; 30: 945–950.

IGRAs and childhood TB: systematic review 15
63 Latorre I, De Souza-Galvao M, Ruiz-Manzano J, et al. Quanti-tative evaluation of T-cell response after specifi c antigen stimu-lation in active and latent tuberculosis infection in adults and children. Diagn Microbiol Infect Dis 2009; 65: 236–246.
64 Lee J Y, Choi H J, Park I N, et al. Comparison of two com-mercial interferon-gamma assays for diagnosing Mycobacte-rium tuberculosis infection. Eur Respir J 2006; 28: 24–30.
65 Lew W J, Jung Y J, Song J W, et al. Combined use of Quanti-FERON®-TB Gold assay and chest computed tomography in a tuberculosis outbreak. Int J Tuberc Lung Dis 2009; 13: 633–639.
66 Liebeschuetz S, Bamber S, Ewer K, Deeks J, Pathan A A, Lal-vani A. Diagnosis of tuberculosis in South African children with a T-cell-based assay: a prospective cohort study. Lancet 2004; 364: 2196–2203.
67 Lighter J, Rigaud M, Eduardo R, Peng C H, Pollack H. Latent tuberculosis diagnosis in children by using the QuantiFERON-TB Gold In-Tube Test. Pediatrics 2009; 123: 30–37.
68 Lucas M, Nicol P, McKinnon E, et al. A prospective large-scale study of methods for the detection of latent Mycobacterium tuberculosis infection in refugee children. Thorax 2010; 65: 442–448.
69 Mandalakas A M, Hesseling A C, Chegou N N, et al. High level of discordant IGRA results in HIV-infected adults and children. Int J Tuberc Lung Dis 2008; 12: 417–423.
70 Mantegani P, Piana F, Codecasa L, et al. Comparison of an in-house and a commercial RD1-based ELISpot-IFN-gamma as-say for the diagnosis of Mycobacterium tuberculosis infection. Clin Med Res 2006; 4: 266–272.
71 Moilicotti P, Bua A, Mela G, et al. Performance of Quanti-FERON-TB testing in a tuberculosis outbreak at a primary school. J Pediatrics 2008; 152: 585–586.
72 Moyo S, Isaacs F, Gelderbloem S, et al. Tuberculin skin test and QuantiFERON assay in young children investigated for tuber-culosis in South Africa. Int J Tuberc Lung Dis. [In press]
73 Nakaoka H, Lawson L, Squire S B, et al. Risk for tuberculosis among children. Emerg Infect Dis 2006; 12: 1383–1388.
74 Neira-Munoz E, Smith J, Cockcroft P, Basher D, Abubaker I. Extensive transmission of Mycobacterium tuberculosis among children on a school bus. Pediatr Infect Dis J 2008; 27: 836–837.
75 Nicol M P, Davies M A, Wood K, et al. Comparison of T-SPOT.TB assay and tuberculin skin test for the evaluation of young children at high risk for tuberculosis in a community setting. Pediatrics 2009; 123: 38–43.
76 Nicol M P, Pienaar D, Wood K, et al. Enzyme-linked immuno-spot assay responses to early secretory antigenic target 6, cul-ture fi ltrate protein 10, and purifi ed protein derivative among children with tuberculosis: implications for diagnosis and moni-toring of therapy. Clin Infect Dis 2005; 40: 1301–1308.
77 Nienhaus A, Schablon A, Diel R. Interferon-gamma release assay for the diagnosis of latent TB infection−analysis of discordant results, when compared to the tuberculin skin test. PLoS One 2008; 3: e2665.
78 Nsutebu E, Moffi tt S J, Mullarkey C, Schweiger M S, Collyns T, Watson J P. Use of QuantiFERON-TB Gold test in the inves-tigation of unexplained positive tuberculin skin tests. Public Health 2008; 122: 1284–1287.
79 Okada K, Mao T E, Mori T, et al. Performance of an interferon-gamma release assay for diagnosing latent tuberculosis infec-tion in children. Epidemiol Infect 2008; 136: 1179–1187.
80 Ozekinci T, Ozbek E, Celik Y. Comparison of tuberculin skin test and a specifi c T-cell-based test, T-Spot®.TB, for the diag-nosis of latent tuberculosis infection. J Intern Med Res 2007; 35: 696–703.
81 Pai M, Joshi R, Dogra S, et al. T-cell assay conversions and re-versions among household contacts of tuberculosis patients in rural India. Int J Tuberc Lung Dis 2009; 13: 84–92.
82 Petrucci R, Amer N A, Gurgel R Q, et al. Interferon gamma,
interferon-gamma-induced-protein 10, and tuberculin re-sponses of children at high risk of tuberculosis infection. Pediatr Infect Dis J 2008; 27: 1073–1077.
83 Piana F, Ruffo Codecasa L, Baldan R, Miotto P, Ferrarese M, Cirillo D M. Use of T-SPOT.TB in latent tuberculosis infec-tion diagnosis in general and immunosuppressed populations. New Microbiol 2007; 30: 286–290.
84 Ruhwald M, Petersen J, Kofoed K, et al. Improving T-cell as-says for the diagnosis of latent TB infection: potential of a diagnostic test based on IP-10. PLoS One 2008; 3: e2858.
85 Soysal A, Millington K A, Bakir M, et al. Effect of BCG vac-cination on risk of Mycobacterium tuberculosis infection in children with household tuberculosis contact: a prospective community-based study. Lancet 2005; 366: 1443–1451.
86 Soysal A, Turel O, Toprak D, Bakir M. Comparison of posi-tive tuberculin skin test with an interferon-gamma-based as-say in unexposed children. Jpn J Infect Dis 2008; 61: 192–195.
87 Stavri H, Ene L, Popa G L, et al. Comparison of tuberculin skin test with a whole-blood interferon gamma assay and ELISA, in HIV-positive children and adolescents with TB. Roum Arch Microbiol Immunol 2009; 68: 14–19.
88 Stefan D C, Dippenaar A, Detjen A K, et al. Interferon-gamma release assays for the detection of Mycobacterium tuberculo-sis infection in children with cancer. Int J Tuberc Lung Dis 2010; 14: 689–694.
89 Taylor R E B, Cant A J, Clark J E. Potential effect of NICE tuberculosis guidelines on paediatric tuberculosis screening. Arch Dis Child 2008; 93: 200–203.
90 Tsiouris S J, Austin J, Toro P, et al. Results of a tuberculosis-specifi c IFN-gamma assay in children at high risk for tuber-culosis infection. Int J Tuberc Lung Dis 2006; 10: 939–941.
91 Wang J Y, Chou C H, Lee L N, et al. Diagnosis of tuberculosis by an enzyme-linked immunospot assay for interferon-gamma. Emerg Infect Dis 2007; 13: 553–558.
92 Warier A, Gunawathi S, Venkatesh S, John K R, Bose A. T-cell assay as a diagnostic tool for tuberculosis. Indian Pediatr 2009; 47: 90–92.
93 Winje B A, Oftung F, Korsvold G E, et al. School-based screening for tuberculosis infection in Norway: comparison of positive tuberculin skin test with interferon-gamma release assay. BMC Infect Dis 2008; 8: 140.
94 Diel R, Forssbohm M, Loytved G, et al. [Recommendations for background studies in tuberculosis]. Pneumologie 2007; 61: 440–455. [French]
95 Mazurek M, Jereb J, Vernon A, LoBue P, Goldberg S, Castro K. Updated guidelines for using interferon gamma release as-says to detect Mycobacterium tuberculosis infection—United States, 2010. MMWR Recomm Rep 2010; 59: 1–25.
96 Updated recommendations on interferon gamma release as-says for latent tuberculosis infection. An Advisory Committee Statement (ACS). Can Commun Dis Rep 2008; 34: 1–13.
97 Pai M, Zwerling A, Menzies D. Systematic review: T-cell-based assays for the diagnosis of latent tuberculosis infection: an update. Ann Intern Med 2008; 149: 177–184.
98 Menzies D, Pai M, Comstock G. Meta-analysis: new tests for the diagnosis of latent tuberculosis infection: areas of uncer-tainty and recommendations for research. Ann Intern Med 2007; 146: 340–354.
99 World Health Organization. Guidance for national tuber-culosis programmes on the management of tuberculosis in children. WHO/HTM/TB/2006.371. WHO/FCH/CAH/2006.7. Geneva, Switzerland: WHO, 2006.
100 Hill P C, Jackson-Sillah D J, Fox A, et al. Incidence of tuber-culosis and the predictive value of ELISPOT and Mantoux tests in Gambian case contacts. PloS ONE 2008; 3: e1379.
101 World Health Organization. Report of the Tenth Meeting of the Strategic and Technical Advisory Group for Tuberculosis (STAG-TB). Geneva, Switzerland: WHO, 2010.

IGRAs and childhood TB: systematic review i
C O N T E X T E : Les enfants infectés par Mycobacterium tuberculosis encourent un risque signifi catif de déve-
lopper une tuberculose (TB) et une thérapie préventive
leur est bénéfi que.
O B J E C T I V E : Evaluer la valeur des tests de libération de
l’interféron-gamma (IGRA) et des tests cutanés tubercu-
liniques (TST) pour le diagnostic de l’infection et de la
maladie TB chez les enfants.
M É T H O D E S : On a inclus 33 études évaluant les IGRA
commerciaux (QuantiFERON-TB [QFT] et T-SPOT.®TB)
ainsi que le TST. Les standards de référence de l’infection
ont été la TB incidente ou l’exposition à la TB. On a
évalué la performance des tests pour le diagnostic de la
maladie dans les études évaluant des enfants ayant une
TB confi rmée et/ou diagnostiquée cliniquement par com-
paraison aux enfants où la TB a été exclue.
R É S U LTAT S : Deux petites études ont mesuré la TB inci-
dente chez les enfants au moyen de QFT et ont trouvé
une faible valeur prédictive positive. L’association de la
réponse au test avec l’exposition (caractérisée soit de
manière dichotomique, soit sous forme d’un gradient) a
été similaire pour tous les tests. Pour le diagnostic de la
maladie, la sensibilité et la spécifi cité de l’ensemble des
tests ont été semblables. Une analyse stratifi ée a suggéré
une sensibilité plus faible de l’ensemble des tests chez les
jeunes enfants infectés par le virus de l’immunodéfi cience
humaine.
C O N C L U S I O N S : Les données disponibles suggèrent que
le TST et les IGRA ont une précision similaire pour la
détection de l’infection TB ou pour le diagnostic de la
maladie chez les enfants. L’hétérogénéité des méthodolo-
gies limite le caractère comparable des études et l’inter-
prétation des résultats. Une approche rigoureuse et stan-
dardisée de l’évaluation des tests diagnostiques de la TB
s’impose chez les enfants.
M A R C O D E R E F E R E N C I A : Los niños infectados por
Mycobacterium tuberculosis presentan un riesgo im-
portante de padecer tuberculosis (TB) y se benefi cian
con el tratamiento preventivo.
O B J E T I V O : Evaluar la utilidad de las pruebas de libera-
ción de interferón gama (IGRA) y de la reacción cutánea
a la tuberculina (TST) en el diagnóstico de la infección
y de la enfermedad tuberculosa en los niños.
M É T O D O S : Se incluyeron en el análisis 33 estudios de
evaluación de las IGRA (QuantiFERON-TB® [QFT] y
la prueba T-SPOT®.TB) y de la reacción TST. Se usaron
como criterios de referencia de infección un caso nuevo
de TB o la exposición a la TB. El rendimiento diagnós-
tico de las pruebas se evaluó en los estudios que incluye-
ron niños con TB clínica o confi rmada, comparados con
niños en quienes se había descartado el diagnóstico de
enfermedad tuberculosa.
R E S U LTA D O S : En dos estudios pequeños se midieron
los casos nuevos de TB en niños en quienes se practicó
una prueba QFT y se encontró un bajo valor pronóstico
del resultado positivo. La asociación entre la respuesta a
la prueba y la exposición (por categorías dicotómicas o
como un gradiente) fue equivalente con todas las prue-
bas. La sensibilidad y la especifi cidad con respecto al
diagnóstico de la enfermedad fueron análogas con todas
las pruebas. El análisis estratifi cado indicó una menor sen-
sibilidad en los niños de <5 años de edad y en los niños
infectados por el virus de la inmunodefi ciencia humana.
C O N C L U S I O N E S : Los datos existentes indican que la
prueba TST y las pruebas IGRA ofrecen una exactitud
equivalente en la detección de la infección y la enferme-
dad tuberculosa en los niños. La heterogeneidad de los
métodos limitó la comparabilidad de los estudios y com-
plicó la interpretación de los resultados. Es preciso defi -
nir una estrategia normalizada rigurosa que permita
evaluar las pruebas diagnósticas de la TB en los niños.
R É S U M É
R E S U M E N


















