Intentions to Care for Children Orphaned by HIV/AIDS: A Test of the Theory of Planned Behavior
22
Intentions to Care for Children Orphaned by HIV/AIDS: A Test of the Theory of Planned Behavior Loraine Townsend 1 Medical Research Council and Department of Psychiatry and Mental Health University of Cape Town Cape Town, South Africa Andrew Dawes Child and Family Development Human Sciences Research Council and University of Cape Town Cape Town, South Africa HIV/AIDS has added an unparalleled number of children to South Africa’s orphan population. The theory of planned behavior (TPB) was used to investigate the decision-making processes of potential substitute caregivers of children orphaned by AIDS. Existing foster and adoptive parents (n = 175) completed a self-report postal survey. Of the sample, 76.0% reported willingness to care for an HIV-negative child and 62.2% an HIV-positive child. Analyses of the theory’s components reveal con- tradictory and disappointing results. While the theory is most useful in conceptual- izing the factors that bear on fostering and adoption, the current study suggests that the TPB is limited in its ability to address the complexity of decisions that attend fostering and adoption of children orphaned by HIV/AIDS. Orphaning is not new to Africa. High rates of maternal mortality, politi- cal conflict, and natural disasters persist in many African countries (Madha- van, 2004). The HIV/AIDS pandemic, however, has added an unprecedented number of children to the orphan population. In 2003, it was estimated that there were close to 1 million maternal orphans under the age of 18 in South Africa (Mbambo, 2005). Prior to the South African government’s 2004 announcement to roll out anti-retroviral therapy (ARVT) to all HIV-positive people, it was estimated that by the year 2015, a total of 4 million children (representing roughly 10% of South Africa’s entire population) would be orphaned (Whiteside & Sunter, 2000). Close to 2 million of these children would have lost both parents (Mbambo, 2005). The provision of ARVT will reduce these projected numbers, but a very substantial number will still require care. It is likely that the majority will be taken in by family members. However, substantial 1 Correspondence concerning this article should be addressed to Loraine Townsend, Post Office Box 240, Plumstead 7801, South Africa. E-mail: [email protected] 822 Journal of Applied Social Psychology, 2007, 37, 4, pp. 822–843. © 2007 Copyright the Authors Journal compilation © 2007 Blackwell Publishing, Inc.
-
Upload
loraine-townsend -
Category
Documents
-
view
216 -
download
1
Transcript of Intentions to Care for Children Orphaned by HIV/AIDS: A Test of the Theory of Planned Behavior

Intentions to Care for Children Orphaned by HIV/AIDS:A Test of the Theory of Planned Behavior
Loraine Townsend1
Medical Research Counciland
Department of Psychiatry andMental Health
University of Cape TownCape Town, South Africa
Andrew DawesChild and Family Development
Human Sciences Research Counciland
University of Cape TownCape Town, South Africa
HIV/AIDS has added an unparalleled number of children to South Africa’s orphanpopulation. The theory of planned behavior (TPB) was used to investigate thedecision-making processes of potential substitute caregivers of children orphaned byAIDS. Existing foster and adoptive parents (n = 175) completed a self-report postalsurvey. Of the sample, 76.0% reported willingness to care for an HIV-negative childand 62.2% an HIV-positive child. Analyses of the theory’s components reveal con-tradictory and disappointing results. While the theory is most useful in conceptual-izing the factors that bear on fostering and adoption, the current study suggests thatthe TPB is limited in its ability to address the complexity of decisions that attendfostering and adoption of children orphaned by HIV/AIDS.
Orphaning is not new to Africa. High rates of maternal mortality, politi-cal conflict, and natural disasters persist in many African countries (Madha-van, 2004). The HIV/AIDS pandemic, however, has added an unprecedentednumber of children to the orphan population. In 2003, it was estimated thatthere were close to 1 million maternal orphans under the age of 18 in SouthAfrica (Mbambo, 2005).
Prior to the South African government’s 2004 announcement to roll outanti-retroviral therapy (ARVT) to all HIV-positive people, it was estimatedthat by the year 2015, a total of 4 million children (representing roughly 10%of South Africa’s entire population) would be orphaned (Whiteside & Sunter,2000). Close to 2 million of these children would have lost both parents(Mbambo, 2005). The provision of ARVT will reduce these projectednumbers, but a very substantial number will still require care. It is likely thatthe majority will be taken in by family members. However, substantial
1Correspondence concerning this article should be addressed to Loraine Townsend, PostOffice Box 240, Plumstead 7801, South Africa. E-mail: [email protected]
822
Journal of Applied Social Psychology, 2007, 37, 4, pp. 822–843.© 2007 Copyright the AuthorsJournal compilation © 2007 Blackwell Publishing, Inc.

numbers will require placement using more traditional forms of foster careand adoption.
Accessing caregivers who are willing to care for children orphaned byHIV/AIDS will present some unique challenges. Wild (2001) pointed to anumber of stressors that face these children: economic deprivation, disruptedschooling, multiple losses, uncertainty, lack of adequate care and supervi-sion, stigma, and social isolation. In these circumstances, it is not surprisingthat a number of studies have described elevated levels of depression, anxiety,and adjustment problems among these children (Freeman, 2004). These poormental health outcomes will follow them into whatever alternative care situ-ation they may enter, which may negatively impact potential caregivers’willingness to care for them. Orphaned children who are themselves HIV-positive will have the double burden of poor mental health and decliningphysical health. The fact that these children will become progressively sickerand may eventually die could further reduce their chances of having peoplewilling to care for them.
Caring for Children Orphaned by HIV/AIDS
The burden of care for orphans in AIDS-afflicted populations continuesto lie with the extended family system, which is likely to become overwhelmedas the pandemic progresses (Foster, 2000; Halkett, 1999; Nyambedha, Wan-dibba, & Aagaard-Hansen, 2003; Nyamukapa & Gregson, 2005; Smart,2000). As the numbers of children requiring alternative parental careincreases, alternative approaches to care and the pool of willing and ablecaregivers will need to be expanded (Desmond, Gow, Loening-Voysey,Wilson, & Stirling, 2002). An option is to consider the potential of statutoryfoster care and adoption.
Historically, in South Africa, alternative parenting for orphans—andindeed for all children in need of alternative parenting within familycontexts—has been provided by adoption, foster care, and kinship carewithin the extended family. In the past, adoption was strongly influenced bypractice and policy developed in the West, and thus was confined to theadoption of young infants by childless, White, middle-class, married couples(Harber, 1999; Brink, 1998; Quintin, Rushton, Dance, & Mayers, 1998).More recently, criteria for eligibility to adopt have changed in South Africa(Brink, 1998; Halkett, 1999; Harber, 1999). Single parents, gay and lesbianparents, parents of different cultures, and poor people—all previouslythought to be unsuitable—now are being considered as adoptive parents.Active promotion of adoption among Black people has found some success,prompting Harber to conclude that previous obstacles to adoption of Blackchildren are not insurmountable.
HIV/AIDS ORPHANS AND THE THEORY OF PLANNED BEHAVIOR 823

In South Africa, formal or statutory foster care is an established practicethat involves the legal transfer of guardianship of the child to a foster parent(or foster parents), as well as financial assistance from the government in theform of a foster-care grant. However, this form of foster care has a historicallegacy of not being available to nor having been provided for a large numberof children in need of alternative family care, most notable Black Africanchildren. In these circumstances, relatives customarily have incorporatedchildren in need of alternative family care (including orphans) into theirfamilies (as noted by Preble, 1990, in Madhavan, 2004). In this form ofkinship care or social parenting, arrangements for the care and upbringing ofchildren are the concern of both the biological parents and an extensivenetwork of relatives (Nyambedha et al., 2003). Recent steep increases in thenumber of foster-care placements reported by the child welfare movement(Halkett, 1999) have suggested that formal, statutory foster care is becomingmore accessible and better known to Black African caregivers. It is also likelythat kinship caregivers are now accessing foster-care grants to assist them incaring for their kin.
While recognizing that statutory adoption and foster care remain under-promoted and underutilized by the majority of South Africans, they dopresent viable options for increasing the pool of potential caregivers(Townsend & Dawes, 2004). Given South Africa’s legacy, however, the poolof adoptive parents may remain wealthier and, therefore, White. The pool offoster parents may include those who are merely attracted by the foster-caregrant. Nevertheless, selecting appropriate caregivers who would providecomprehensive, continuous, and sustained care for orphaned children iscritical (Ansell & Young, 2004).
An exploration of factors that influence decisions to care for children whoare orphaned as a result of HIV/AIDS would be important in guiding prac-tice and childcare placement. The theory of planned behavior (TPB) providesan opportunity to inform interventions and possible avenues for behaviorchange (Ajzen, 1991). In the current paper, we focus on a specific section ofa larger study (Townsend, 2001) that employed the TPB to explore intentionto care for children orphaned by HIV/AIDS.
Theory of Planned Behavior
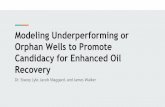
As originally proposed by Ajzen (1991), a brief description of the TPBmodel follows (see Figure 1). Central to the TPB is the concept of inten-tion. Intention provides the motivation necessary to engage in a particularbehavior and, therefore, is the principal predictor of that behavior (Ajzen,1991).
824 TOWNSEND AND DAWES

The TPB proposes three conceptually independent determinants or prin-cipal predictors of intention to perform a given behavior. The first of these isattitudes toward performing the behavior in question. Attitudes refer toeither favorable or unfavorable evaluations or judgments about the givenbehavior. The second determinant is subjective norm, which refers to per-ceived social pressure to either perform or not perform the given behavior.The third determinant is perceived behavioral control, which refers to theperceived ease or difficulty of performing the behavior.
The determinants are measured using a number of 5- or 7-point semanticdifferential items. A mean of each respondent’s scores on the items is used asthe direct or global measure of the determinants of intentions. The relativeimportance of each of these three direct measures is expected to vary frombehavior to behavior and across situations (Ajzen, 1991).
The TPB also explores the antecedents of each of the principal predictorsof intention, allowing for an explanation of, rather than merely the prediction
Belief that behavior leads to
certain outcomes
Evaluation of outcomes
Belief that specific referents
think behavior should/should not
be performed
Motivation to comply with
referents
Belief of volitional control
over behavior
Perceived power over behavior
ATTITUDE TOWARD
BEHAVIOR
SUBJECTIVE NORM
PERCEIVED BEHAVIORAL
CONTROL
INTENTION TO PERFORM
BEHAVIOR BEHAVIOR
Figure 1. Theory of planned behavior (Ajzen, 1991).
HIV/AIDS ORPHANS AND THE THEORY OF PLANNED BEHAVIOR 825

of, human behavior (Ajzen, 1991). The structures underlying each of theprincipal predictors of intention to perform a behavior are envisioned ascomposites of expectancy and value (Hewstone, 1986). For example, arespondent’s attitude toward caring for a child orphaned by HIV/AIDS isproposed to be a function of the belief that caring for such a child wouldprovide him or her with a loving home (expectancy), multiplied by the beliefthat this would be a very good thing to do (value). These composites arereferred to as the belief-based measures of the principal predictors of inten-tion. They are equally important in determining intention—and, therefore,behavior—and revolve around salient beliefs and information pertinent tothe behavior in question.
Ajzen and Fishbein (1980) provided guidelines as to how these constructsshould be developed and measured. Preparatory work should be conductedeither with respondents themselves or with a representative group from thepopulation to be studied. Their salient beliefs along each of the theory’sdimensions should be elicited. Items are constructed from the most fre-quently mentioned salient beliefs.
Together with the theory of reasoned action (TRA) (Fishbein & Ajzen,1975), the TPB is the most validated and extensively researched of the socialcognitive models that seek to predict behavior (Bandawe, 2000). Theapproach has been used in a number of international contexts to predict arange of diverse behaviors. Most recently, these behaviors have includedhealthy eating and physical activity/exercise (Armitage, 2005; de Bruijn,Kremers, Schaalma, Van Mechelen, & Brug, 2005; Payne, Jones, & Harris,2005), sexual behavior (Chitamun & Finchilescu, 2003; Collazo, 2004),contraception (Kridli & Newton, 2005), smoking (McMillan, Higgins, &Connor, 2005), volunteerism (Greenslade & White, 2005), and spelling(Sideridis, 2005), to name a few.
To our knowledge, the TPB has not been used to investigate decisions tocare for orphaned children. In the present study, the TPB was used toinvestigate the decision-making processes of potential substitute caregivers ofchildren orphaned by AIDS, including their attitudes toward caring for sucha child, the influence of respected others in their decision-making process,and the effects of their perceived control over their decisions.
Method
Research Instrument
Ajzen and Fishbein (1980) provided clear guidelines as to how the con-structs relevant to the TPB should be measured. In order to develop thequestions for participants in the present study in accordance with the TPB, a
826 TOWNSEND AND DAWES

pilot study was conducted with 14 women who were caring for nonbiologicalchildren and, therefore, who were considered similar to the population to bestudied in the main research. Their salient beliefs along each of the dimen-sions of the theory were solicited by means of open-ended, self-reportresponses to 14 questions.
Respondents were asked to specify what they thought would be the mostimportant advantages and disadvantages in caring for either an HIV-negative or an HIV-positive child, both for the child and for themselves. Theyalso were asked what they thought would make it easy/difficult for them tocare for the child. Questions asked respondents to indicate which people, whoare important to them, would approve/disapprove should they care for thechild. Finally, respondents were asked, if they were already caring for anonbiological child, what they liked or disliked about such an arrangement.The responses were simply listed and tallied. Those that were mentioned mostfrequently by all respondents were incorporated into the construction of thefinal TPB questionnaire.
Questionnaires
Two questionnaire booklets were developed. One assessed the opinions ofrespondents’ willingness to care for an HIV-negative orphan (Form A), whilethe other assessed willingness to care for an HIV-positive orphan (Form B).The questionnaires were constructed following consultation with researchcolleagues, staff in the Non-Government Organisation (NGO) that assistedin accessing participants, and a group of foster parents (who were notincluded in the final sample). The questionnaires were then translated intoAfrikaans and isiXhosa (the languages of many probable participants). Theywere then back-translated, and discrepancies were corrected in consultationwith translators and back-translators.
Participant Instructions
The section of the questionnaire pertinent to the current paper describesa particular orphaning situation:
The child in this part of the questionnaire is orphaned becausehis or her mother has died of AIDS.2 It is unknown whether the
2It is more correct to speak of a person dying from “an AIDS-related illness.” We acknowl-edge the incorrect phrasing used here. However, the phrase used in the questionnaire reflects acommon understanding that AIDS is a fatal illness in itself, rather than a condition that rendersa patient vulnerable to life-threatening illnesses (i.e., the actual cause of death).
HIV/AIDS ORPHANS AND THE THEORY OF PLANNED BEHAVIOR 827

child has other family members who would be willing or evenable to care for him or her. The child appears to have no one tolook after him or her and nowhere to go.
Participants were also alerted to the following (it was necessary to be specificas to the basis of their hypothetical decisions):
In the questionnaire, you will see that I ask a number of ques-tions about caring for an orphaned child. Caring for anorphaned child would mean taking the child into your own homeand treating him or her as you would your own children; pro-viding him or her with food, shelter, and clothing; schoolingand medical care; and love, support, and guidance.
These instructions provide the necessary target (child orphaned by HIV/AIDS), action (caring, as described previously), context (within one’s ownhome), and time (imminent) of the behavioral criterion required for ananalysis of behavioral intention in the TPB (Ajzen & Fishbein, 1980).
Items that measure TPB variables followed these instructions. A descrip-tion of the items follows.
Intention. Respondents were given the option to respond Yes or No to thefollowing statement (their response was used as an indicator of intention toperform the target behavior): “I would be willing to care for the childdescribed in the scenario if the child is HIV-negative and does not haveAIDS” (in Form A of the questionnaire); or “I would be willing to care forthe child described in the scenario if the child is HIV-positive and does haveAIDS and is likely to become ill and will eventually die” (in Form B of thequestionnaire).
All of the other items were measured by means of a 5-point scale rangingfrom 1 (coded as -2) to 5 (coded as +2) for each item. Positive scores reflectpositive beliefs, states, or actions (in terms of caring for the hypotheticalchild); and negative scores reflect the opposite. Although the convention inmost research employing the TPB is to use a 7-point scale, other reasonedaction research had used this variation without any apparent disadvantage(e.g., Bandawe, 2000; Godin & Kok, 1996).
Attitude. Attitude was measured directly by means of a three-item scale. Asingle statement was divided into three sections, allowing for a responsealong cognitive, affective, and general components of attitudes (Povey,Connor, Sparks, James, & Shepherd, 2000). The statement began “For me tocare for this child would be . . . ,” which was followed by the anchors “a verygood thing to do/a very bad thing to do”; “a wise thing to do/a foolish thing todo”; and “an enjoyable thing to do/an unenjoyable thing to do.” Cronbach’s
828 TOWNSEND AND DAWES

alpha coefficients for this scale were .85 and .82 for Form A and Form B,respectively.
Behavioral beliefs and outcome evaluations. Behavioral beliefs corre-sponded to affective and instrumental components of attitudes (Ajzen &Driver, 1991; Connor & Armitage, 1998). Following the procedure forcomputing a belief-based measure of attitude (Ajzen, 1991; Ajzen & Fish-bein, 1980), this measure was computed as the sum of the products of thescores for behavioral beliefs, multiplied by the corresponding outcomeevaluations of those beliefs. There were five items in this measure. A samplebehavioral belief item is “I would be able to provide this child with a lovingand stable home” (strongly agree to strongly disagree). Assessing the cor-responding outcome evaluation for this item was constructed as follows:The statement “To give this child a loving and stable home would be” wasrated on a scale ranging from a very good thing to do to a very bad thing todo. Cronbach’s alphas for the behavioral beliefs scales were .80 (Form A)and .71 (Form B); and for the outcome evaluation items were .70 (Form A)and .46 (Form B).
Subjective norm. Much of the criticism of the subjective norm constructhas revolved around the traditional use of a single-item to measure it(Connor & Armitage, 1998; Povey et al., 2000). Povey et al.’s example wasfollowed, and three items were constructed, including notions of significantothers’ approval and sanction. A mean of the three items was used as a globalmeasure of subjective norms. The three statements were as follows: “PeopleI respect would think that I should care for this child” (strongly agree tostrongly disagree); “If I were to care for this child, people I respect would . . .”(strongly approve to strongly disapprove); and “People I respect would wantme to care for this child” (strongly agree to strongly disagree). Cronbach’salphas for these items were .92 and .94 for Form A and Form B, respectively.
Normative beliefs and motivation to comply. Normative beliefs and moti-vation to comply were measured by means of three items based on the mostfrequently reported salient referents (husband/partner, family, and friends) inthe preparatory study. Following the procedure for computing a belief-basedmeasure of subjective norm (Ajzen, 1991; Ajzen & Fishbein, 1980), thismeasure was computed as the sum of the products of the scores for normativebeliefs, multiplied by the corresponding motivation to comply with thosebeliefs. A sample normative belief item is “If I were to care for this child, myhusband/partner would . . . ,” which was rated on a scale ranging from defi-nitely approve to definitely disapprove. The corresponding motivation tocomply for this item is “With most things in life, I do what my husband/partner wants me to do” (always to never). Cronbach’s alphas for the nor-mative beliefs scale were .90 (Form A) and .87 (Form B); and for themotivation to comply items were .72 (Form A) and .59 (Form B).
HIV/AIDS ORPHANS AND THE THEORY OF PLANNED BEHAVIOR 829

Perceived behavioral control (PBC). PBC was measured directly by meansof four items. Although Ajzen (1991) views self-efficacy and PBC as synony-mous, more recently researchers have examined the distinction betweenand the relative importance of these two constructs in the TPB (Armitage& Connor, 1999; Armitage, Connor, Loach, & Willetts, 1999; Connor &Armitage, 1998; Giles & Rea, 1999; Povey et al., 2000). These studies provideevidence for separating the two dimensions of PBC as independent predictorsof intentions or behavior. In line with this recent debate, two of the itemsassess aspects of personal control, and the other two encompass aspects ofself-efficacy. An example of the former is “If I cared for this child, it would beentirely my own decision” (strongly agree to strongly disagree). And anexample of the latter is “I would feel very capable of caring for this child”(strongly agree to strongly disagree).
In order to assess whether to employ a mean of the four items as a globalmeasure of PBC, or whether the personal control and self-efficacy itemswould be used separately as predictors of behavioral intention, the items weresubjected to a principal components factor analysis. All items loaded ontoone factor, with loadings ranging from .87 to .91 with an eigenvalue of 3.15.The factor explained 79% of the variance in Form A, and 76% of the variancein Form B (loadings from .81 to .92 with an eigenvalue of 3.03). The itemsclearly did not discriminate between self-efficacy and personal control. Amean computed for the four items was used as a direct measure of PBC.Cronbach’s alphas for these items were .90 and .89 for Form A and Form B,respectively.
Control beliefs and power of control beliefs. The preparatory studyparticipants—who were asked what makes caring for a child easy ordifficult—were of assistance in identifying perceptions of control. Affective aswell as instrumental constraints/facilitators were included in the items.Again, following the procedure for computing a belief-based measure of PBC(Ajzen, 1991), this measure was computed as the sum of the products of thescores for control beliefs, multiplied by the corresponding measure of thepower of those beliefs. An example of a control belief item is “If I were to carefor this child, I would need the support of my family and friends” (stronglyagree to strongly disagree). Assessing the corresponding power of this controlbelief was worded as follows: “If I have the support of my family and friends,this would make it . . . to care for this child” with the response options ratedon a scale ranging from much easier to much more difficult. Cronbach’s alphasfor the three-item control beliefs scale were .81 (Form A) and .83 (Form B);and for the power of control beliefs scale were .65 (Form A) and .55 (FormB).
With reference to Cronbach’s alpha coefficients reported for each of thementioned scales, Aiken (1982) suggested that attitude scales should show a
830 TOWNSEND AND DAWES

reliability of between .79 (median) and .98 (high). Despite the removal of anumber of items in the scales to improve their reliability, some alpha coeffi-cients remained below .79. Although the majority of the alphas were high,giving credibility to the results that emerged from the questionnaires, somecaution must be exercised when interpreting results.
Sample
A group of foster and adoptive mothers on the registers of two branchesof a child welfare NGO were asked to participate in the study. The NGOoffers welfare services to children and their families as well as foster-care andadoption placements throughout South Africa. In addition, the editor of anational newsletter sent to adoptive parents (largely confined to the Gautengarea of South Africa) agreed to include the questionnaire in a posting of oneof their quarterly newsletters.
Those who were mailed a questionnaire included 513 foster parents and395 adoptive parents who resided in two South African cities (Cape Townand Johannesburg) and one large town (George). One hundred and seventy-five questionnaires were returned (a 19.3% response rate).
The final study sample consisted of 70 adoptive and 96 foster mothers (Mage = 41.7 and 51.6 years for the adoptive and foster mothers, respectively).Between them, the adoptive families were caring for 49 biological and 105adopted children younger than 16 years. The fostercare families were caringfor 21 biological, 56 biologically related, and 118 non-kin children youngerthan 16 years. It is not known whether any of these children were orphanedby AIDS.
Procedure
All of the participants provided informed consent, and data for the studywere gathered by means of a self-report postal survey. The questionnaireswere mailed directly from the NGO office and the editorial office of thenewsletter. In this way, respondents’ anonymity was ensured.
A randomly selected half of the sample from each source received FormA, and the other half received Form B. All of the booklets included aself-addressed stamped envelope for ease of return. As the inclusion of anincentive has been documented as having a positive effect on response rates(Bailey, 1987), respondents had a chance to receive a R100 shopping voucherredeemable at a leading supermarket chain, which was offered to 10 ran-domly drawn respondents who had completed the questionnaire.
HIV/AIDS ORPHANS AND THE THEORY OF PLANNED BEHAVIOR 831

Results
Descriptive Statistics and Intercorrelations
It was expected that more respondents would be willing to care for anHIV-negative child than an HIV-positive child, as caring for an HIV-positivechild is likely to be financially, physically, and emotionally taxing. Althoughmore respondents reported their willingness to care for an HIV-negative child(76.5%) than an HIV-positive child (62.2%), a chi-square analysis reveals thatthis difference was not statistically significant.
The mean scores for each variable, their reliabilities, and the correlationsamong the variables are shown in Table 1. Irrespective of the HIV status ofthe hypothetical child, respondents reported a positive attitude toward takingon a substitute parent role. Scores on subjective norms were also positive,suggesting that the specific referents identified in the preparatory study didinfluence respondents’ reported willingness to care for the child. Respondentsalso reported positive levels of control over their intention to care for thechild. Moderate to high intercorrelations between the components of theTPB were evident. All correlations were higher than .30. Ajzen and Fishbein(1980) regarded this level as adequate to confirm the links between thecomponents of the theory.
Table 1
Descriptive Statistics, Alpha Coefficients, and Intercorrelations
Variable M SD a 1 2 3
1. Intention — — — —2. Attitude
HIV-negative child 1.39 0.89 .85 .41** —HIV-positive child 0.89 1.04 .82 .52** —
3. Subjective normHIV-negative child 1.16 1.08 .92 .43** .75** —HIV-positive child 0.53 1.38 .94 .48** .69** —
4. PBCHIV-negative child 1.13 1.20 .90 .48** .53** .62**HIV-positive child 0.77 1.31 .89 .49** .62** .58**
Note. PBC = perceived behavioral control.** p < .01.
832 TOWNSEND AND DAWES

Zero-Order Correlations Between Direct and Belief-Based Measures
Exploring the intercorrelations between the direct measures and belief-based measures of the components of the TPB reveals that correlationsbetween the belief-based measures of subjective norm and its correspondingdirect measures were adequate to confirm the link between this componentsof the theory. This was irrespective of the child’s HIV status (Ajzen &Fishbein, 1980; r = .32 and .56 for an HIV-negative child and an HIV-positive child, respectively).
The links between the direct measure of attitude and its correspondingbelief-based measures were confirmed only in the case of an HIV-negativechild (r = .39). The same cannot be said for the links between the belief-basedand direct measures of PBC (r = .20 and .06 for an HIV-negative child and anHIV-positive child, respectively), and between the belief-based measure ofattitudes and its corresponding belief-based measures in the case of an HIV-positive child (r = .07). This may be indicative of the difficulty of constructingbelief-based measures of some dimensions of the theory to adequately tap thedirect measure. Caution must be exercised when interpreting results for per-ceptions of PBC.
Multiple Linear Regression to Predict Intentions
Employing forward, stepwise linear regression, intention to care for thehypothetical child was regressed against attitude, subjective norm, and PBC(HIV-negative child, N = 61; HIV-positive child, N = 73). The results aredepicted in Table 2.
Attitudes and subjective norms were entered into the model first andexplained 20.3% of the variance in intention to care for an HIV-negativechild, F(2, 59) = 7.38, p < .01; and 29.7% of the variance in intention to carefor an HIV-positive child, F(2, 70) = 14.81, p < .01. PBC was entered next andincreased the amount of variance in intention to care for an HIV-negativechild by 6% (R Δ́ = .06), F(3, 57) = 6.86, p < .01; and by 3% (R Δ́ = .33),F(3, 69) = 11.32, p < .01, in the case of an HIV-positive child.
Beta-weight analysis of measures contributing to intention to care for anHIV-negative child indicate that PBC was the only significant contributor(b = .32, p < .05). Neither attitude nor subjective norms contributed signifi-cantly to intention to care for an HIV-negative child (b = .15 and .12, respec-tively). For this subsample, therefore, intention to care for the child wasinfluenced by the extent to which the respondents perceived that the decisionto care was something over which they had personal control. Despite certaincomponents of the theory not having good predictive ability, the model as a
HIV/AIDS ORPHANS AND THE THEORY OF PLANNED BEHAVIOR 833

whole did predict intention to care for an HIV-negative child, F(3, 57) = 6.86,p < .01.
In the case of an HIV-positive child, beta-weight analysis indicates thatneither attitude nor subjective norms nor PBC contributed significantly tointention to care for the child (b = .26, .17, and .24 respectively). For thissubgroup, then, none of the components of the theory influenced intention tocare for the child, although, on the whole, intention was predicted signifi-cantly by the TPB model, F(3, 69) = 11.32, p < .01. These models are depictedin Figure 2.
In an effort to understand why the majority of the direct measures did notsignificantly contribute to intention to care, a further investigation of pos-sible multicollinearity between the independent variables was undertaken.All bivariate correlations were below .80, and none of the R2 values wereclose to 1.00 when regressing each independent variable on the other two.According to Berry and Feldman (1985), these findings suggest that multi-collinearity was not present.
Correlations Between Individual Belief-Based Items and Their CorrespondingDirect Measures
In an attempt to investigate which of the belief-based items contributedmost to the corresponding direct measure, correlations between the two wereundertaken. The results are depicted in Table 3.
Table 2
Prediction of Willingness (Intention) to Care
Step/predictor R R2 R2D F Final beta
HIV-negative childAttitude .149Subjective norm .45 .20 .20 7.38** .118PBC .52 .27 .06 6.86** .322*
HIV-positive childAttitude .257Subjective norm .55 .30 .03 14.81** .165PBC .57 .33 .03 11.32** .238
Note. PBC = perceived behavioral control.* p < .05. ** p < .01.
834 TOWNSEND AND DAWES

Respondents’ attitudes toward caring for an HIV-negative child seem tobe strongly child-centered and altruistically motivated. Although all correla-tions were low, they were positive and significant. In the case of an HIV-positive child, respondents’ attitudes toward caring for the child seem to berelated to the possibility of incurring financial costs. The more positive theirattitudes toward caring for the child were, the less they felt they would beplacing themselves and their families at risk of cross-infection.
Not surprisingly, respondents felt that their husbands/partners had aninfluence on their intentions to care for both an HIV-negative and an HIV-positive child. The correlations were significant and high in both cases. It isonly when expressing an intention to care for an HIV-positive child thatrespondents’ families (other than their partners) appeared to exert someinfluence on their intentions.
Friends had little influence. The greater respondents’ willingness, the lessinfluence friends seemed to have on them (low but negative and nonsignifi-cant correlations).
In sum, the evidence indicates that individual commitment outweighsconformity to the wishes of others in the case of an HIV-negative child. In thecase of an HIV-positive child, however, family members may well exert someinfluence on intentions.
The two most important contributors to the control that respondents feltthey had over their intention to care for an HIV-negative child were whetherthey had adequate time and energy and whether contact with other familiescaring for a similar child was available. In the case of an HIV-positive child,none of the items were significantly related to the expressed intention to carefor the child.
Behavioral Attitude beliefs and (a) r = .39 * toward caring outcome (b) r = .07 for an orphaned evaluations child
(a) β = .15 (b) β = .26
Normative Subjective Intention beliefs and (a) r = .32 * norms regarding (a) β = .12 (a) R = .52** to care for motivation (b) r = .56 ** intention to care (b) β = .17 (b) R = .57** orphaned to comply for an orphaned child
child
(a) β = .32* (b) β = .24
PBC and power of behavioral (a) r = .20 control (b) r = .06
Perceived controlover intention tocare for anorphaned child
Figure 2. Theory of planned behavior model to predict intention to care for a child orphaned byHIV/AIDS. (a) = HIV-negative child. (b) = HIV-positive child. *p < .05. **p < .01.
HIV/AIDS ORPHANS AND THE THEORY OF PLANNED BEHAVIOR 835

Table 3
Correlations Between Belief-Based Items and Attitudes, Subjective Norm,and PBC
HIV-negative child
r
HIV-positive child
rAttitudes Attitudes
For me to care for this childwould mean that . . .
For me to care for this childwould mean that . . .
1. I would provide the childwith a loving and stablehome.
.36** 1. I would be rejected byfamily and friends.
.20
2. I would provide the childwith a sense of belongingand security.
.27* 2. I would incur financialburden.
.27*
3. I would provide the childwith a chance for anormal life.
.31* 3. The child would havedifficulty in adjusting tonew life.
.15
4. I would help a needychild.
.31* 4. I would place self andfamily at risk of infection.
-.32**
5. I would be unsure aboutunknown medical andfamily background.
.18 5. I would endure emotionalstrain.
-.09
Subjective norm Subjective norm
Salient referents Salient referents1. Husband/partner .65** 1. Husband/partner .70**2. Friends -.09* 2. Friends -.033. Family .10 3. Family .32*
Perceived BehavioralControl
Perceived BehavioralControl
1. I would need support offamily and friends.
-.04 1. I would need health careexperience.
.18
2. I would need time andenergy.
.27* 2. I would need someoneelse to pay medical bills.
-.18
3. I would need contact withother (adoptive) families.
.25* 3. I would need supportfrom family and friends.
.16
* p < .05. ** p < .01.
836 TOWNSEND AND DAWES

Discussion
There are no studies to date that have used the TPB to explore intentionto care for children orphaned as a result of HIV/AIDS. As such, the presentinvestigation not only adds to the literature on the TPB, but also extends thelimited literature on caring options for children orphaned by HIV/AIDS.
Data from an exploration of the TPB as a possible appropriate anduseful model to investigate behavior relating to caring for childrenorphaned by HIV/AIDS may be explored along two dimensions. First, andtraditionally, the usefulness of the model can be investigated. This wouldencompass exploration of its predictive utility, the link between the compo-nents of the theory, and various methodological and statistical concerns.However, as the TPB has not been used to explore alternative parentingintentions, comparisons to existing research necessarily would be excluded.Much of the discussion, therefore, will revolve around the TPB as it relatesto the current study.
Second, analysis of individual items in the TPB battery can be used tocomplement much of the literature surrounding caring options for childrenorphaned as a result of HIV/AIDS. Particular attitudes toward caring for anorphaned child, influences of others in deciding to care for such a child, andperceptions regarding facilitators or hindrances to caring for an orphanedchild can be explored.
As a model to predict intention to perform specific behaviors, the results ofthe current study appear to confirm the potential of the TBP in limitedrespects. Intention to care for an orphaned child, irrespective of his or her HIVstatus, was predicted significantly by the three determinants of such an inten-tion: participant’s attitude toward the behavior, subjective norm, and PBC.However, of concern is the fact that the relative contribution of each of thedeterminants was not defined clearly. The only significant contributor tointention to care was PBC, and then only in the case of an HIV-negative child.Although the correlations between each of the direct measures and themeasure of intention were significant—suggesting a strong relationshipbetween them—the correlations did not corroborate the evidence from themultiple regression. Therefore, our evidence suggests that multicollinearitybetween the independent variables was not responsible. Post hoc factor analy-ses show that items measuring attitude and subjective norms loaded onto onefactor, and items measuring PBC loaded onto another, irrespective of thechild’s HIV status. Lack of discriminant validity between these two variablesis a likely explanation for their insignificant contribution to the regression.
Another concern is the relatively low correlations found between thebelief-based measures of each of the constructs and their respective directmeasures. As suggested by Hankins, French, and Horne (2000), the
HIV/AIDS ORPHANS AND THE THEORY OF PLANNED BEHAVIOR 837

Belief ¥ Expectancy multiplicative operationalization of control beliefs isonly a representation of the processes involved, and not necessarily a usefulmeasure of it. A suggestion has been to provide a simple measure based onself-reported beliefs, rather than a multiplicative composite (Eagly &Chaiken, 1993, as reported in Hankins et al., 2000). Self-reports of respon-dents’ own beliefs would not require an expectancy component, as expect-ancies would be high. Future studies that employ the TPB to investigateintention to care for orphaned children, therefore, should document respon-dents’ own beliefs about caring for the child.
Ajzen (1991) provided another explanation to account for “the generallymoderate correlations between belief-based indices and other, more globalmeasures of each variable” (p. 197). He suggested that global measures mayprovoke a more automatic response from respondents, as opposed to a morereasoned response that belief-based items require. The different responseprocesses—automatic or reasoned—may induce different responses and thuscontribute to the poor correlation results.
One important way in which the TPB contributes to our understanding ofthe decision-making processes involved in intention to care for orphanedchildren can be seen from exploration of the correlations between individualbelief-based items and their corresponding global measures. Although, wheresignificant, the correlations were mostly low, the findings may be useful tofuture researchers wishing to explore elements of potential caregivers’ deci-sion making. For example, items that correlated positively and significantlywith the direct measure of attitudes toward caring for an HIV-negative childwere those that demonstrate strong child-centeredness: providing the childwith a loving and stable home, a sense of belonging, and a chance for anormal life; and providing respondents with the opportunity to help a needychild. These beliefs appear to be strongly indicative of respondents’ motiva-tions, which are routinely investigated by both adoption and foster-carepractitioners (Scholtz, 1997; South African National Council for Child andFamily Welfare, 1996). Child-centered motivations are considered necessaryfor the successful placement of children in either of these groups’ care. In thecase of an HIV-positive child, however, none of the child-centered attitudebelief items remained after the exclusion of those that were necessary toimprove reliability of the measure.
Clearly, the expectation of incurring financial hardship is an issue andcorresponds to the reported need for assistance with medical care and finan-cial aid should adoption or fostering be considered. Of note is the fact that ofthose who are more positive about caring for the child, the less they fearcross-infection. This finding suggests that accurate knowledge about HIV—particularly modes of transmission—would assist in reducing resistance tocare.
838 TOWNSEND AND DAWES

Irrespective of the child’s HIV status, husbands/partners were found toinfluence respondents’ intentions to care for an orphaned child. Given themagnitude of a decision to care for an orphaned child, this finding points tothe need to involve both partners equally in decision-making processes. Theconsequences of this type of decision will affect (adult) members of a familymost. Therefore, the decision is likely to need both partners’ deliberation andagreement/disagreement with a final commitment. With respect to the influ-ence of family members, it was only in the case of an HIV-positive child thatfamilies were instrumental in respondents’ decision to care for the child. Theneed to include family members in decision making may be the result ofanticipating the need for emotional or instrumental support from them:support that may not be as necessary when caring for a presumably healthychild.
With respect to caring for an HIV-negative child, the present study’srespondents reported only potential facilitators to their sense of control overtheir intention to care for the child: needing time and energy, and havingcontact with other families in similar situations. The first of these facilitators,however, could be said of anyone caring for a child. The second could be saidof anyone caring for an adopted child. However, neither of these facilitatorscould be said to be specific to caring for a child orphaned by HIV/AIDS.Caring for any child arguably requires time and energy; the uniqueness ofcaring for an adopted child may be managed better with the support given byothers in similarly unique parenting situations.
The present study showed that existing foster and adoptive parents area potential recruiting ground for caregivers of children orphaned by HIV/AIDS. Those who are strongly child-centered and who wish to provideneedy children with a loving home, a sense of belonging, and a chancefor a normal life are likely to be particularly willing to take on thechallenge.
Perceived support of the husband or partner is important in predicting theintention to care for these children (regardless of their HIV status). In thecase of HIV-positive children, the support of other family members appearsto be important as well. The intention to care is dependent, in part, on theprobable burden of the caregiver’s role. In the case of the HIV-positive child,support for medical costs is an important factor. At the end of the day, it isthe strength of the commitment of the potential caregiver that outweighs allother considerations.
The present study has several limitations. The sample cannot be consid-ered representative of foster and adoptive parents or the general population.The sample realized was smaller than had been hoped because of a relativelylow response rate (though not untypical of postal surveys). The refusals mayhave produced a systematic bias in participants. For example, those who
HIV/AIDS ORPHANS AND THE THEORY OF PLANNED BEHAVIOR 839

were already predisposed to care for a child with HIV/AIDS also may havebeen more likely to respond to the questionnaire.
Despite respondents being unaware of the cooperation provided by theNGO, the possibility exists that they may have suspected as much. Thus, theymay have provided answers to the questions that would put them in afavorable light as potential foster parents, adoptive parents, or both. Clearly,a better response rate and a larger number of respondents would have addedsubstantial weight to the conclusions. We believe that our choice of a foster/adoptive sample was appropriate, as they are a likely pool of caregivers forchildren orphaned by HIV/AIDS (i.e., they have already made the decision tocare for vulnerable children). Nonetheless, the study must be replicated inother populations.
While the model showed some promise for the present purpose, analysisof the components of the theory as well as their interrelationships in thisstudy raised some contradictory and, at times, disappointing results. As noother research has been conducted using the TPB to explain alternativeparenting intentions, these are difficult to unravel at this point. While theTPB seems to make a contribution to our understanding of the decision-making processes involved in intention to care for orphaned children, thepresent data proved less powerful than we had hoped. This could be a resultof the questions and scales used. However, we suggest that the outcome ismore likely a result of the model not being up to the complexity of thedecision process that attends fostering and adoption. Both pose major life-changing consequences for caregivers and their families. This is in contrastto the focused health-promotion endeavors (e.g., smoking cessation) inwhich the TPB has been used successfully. Whether the TPB is or is not auseful model for the exploration of behavior of this complexity must beresolved through further investigations and possible elaboration of themodel itself.
References
Aiken, L. R. (1982). Psychological testing and assessment (4th ed.) Boston:Allyn and Bacon.
Ajzen, I. (1991). The theory of planned behavior. Organizational Behaviorand Human Decision Processes, 50, 179–211.
Ajzen, I., & Driver, B. L. (1991). Prediction of leisure participation frombehavioral, normative, and control beliefs: An application of the theoryof planned behavior. Leisure Sciences, 13, 185–204.
Ajzen, I., & Fishbein, M. (1980). Understanding attitudes and predicting socialbehavior. Englewood Cliffs, NJ: Prentice-Hall.
840 TOWNSEND AND DAWES

Ansell, N., & Young, L. (2004). Enabling households to support successfulmigration of AIDS orphans in southern Africa. AIDS Care, 16, 3–10.
Armitage, C. J. (2005). Can the theory of planned behavior predict mainte-nance of physical activity? Health Psychology, 24, 235–245.
Armitage, C. J., & Connor, M. (1999). The theory of planned behaviour:Assessment of predictive validity and “perceived control.” British Journalof Social Psychology, 38, 35–54.
Armitage, C. J., Connor, M., Loach, J., & Willetts, D. (1999). Differentperceptions of control: Applying an extended theory of planned behaviorto legal and illegal drug use. Basic and Applied Social Psychology, 21,301–316.
Bailey, K. D. (1987). Methods of social research (2nd ed.) New York: FreePress.
Bandawe, R. C. (2000). A schistosomiasis health education intervention amongrural Malawian children: Lessons learned. Unpublished doctoral thesis,University of Cape Town, South Africa.
Berry, W. D., & Feldman, S. (1985). Multiple regression in practice. BeverlyHills, CA: Sage.
Brink, P. (1998). Adoption practice in the AIDS era: A South African per-spective. Retrieved June 2000, from http://www.togan.co.za.cindi/papers/paper1.htm
Chitamun, S., & Finchilescu, G. (2003). Predicting the intention of SouthAfrican female students to engage in premarital sexual relations: Anapplication of the theory of reasoned action. South African Journal ofPsychology, 33, 154–161.
Collazo, A. A. (2004). Theory-based predictors of intention to engage inprecautionary sexual behavior among Puerto Rican high school adoles-cents. Journal of HIV/AIDS Prevention in Children and Youth, 6, 91–120.
Connor, M., & Armitage, C. (1998). Extending the theory of planned behav-ior: A review and avenues for further research. Journal of Applied SocialPsychology, 38, 195–222.
de Bruijn, G. J., Kremers, S. P., Schaalma, H., Van Mechelen, W., & Brug,J. (2005). Determinants of adolescent bicycle use for transportation andsnacking behavior. Preventive Medicine, 40, 658–667.
Desmond, C., Gow, J., Loening-Voysey, H., Wilson, T., & Stirling, B. (2002).Approaches to caring: Essential elements for quality service and cost-effectiveness in South Africa. Evaluation and Program Planning, 25, 447–458.
Fishbein, M., & Ajzen, A. (1975). Beliefs, attitudes, intentions, and behavior:An introduction to theory and research. Reading, MA: Addison-Wesley.
Foster, G. (2000). The capacity of the extended family safety net for orphansin Africa. Psychology, Health, and Medicine, 5, 55–62.
HIV/AIDS ORPHANS AND THE THEORY OF PLANNED BEHAVIOR 841

Freeman, M. (2004). HIV/AIDS in developing countries: Heading towards amental health and consequent social disaster? South African Journal ofPsychology, 34, 139–159.
Giles, M., & Rea, A. (1999). Short research note. Career self-efficacy: Anapplication of the theory of planned behavior. Journal of Occupationaland Organizational Psychology, 72, 393–398.
Godin, G., & Kok, G. (1996). The theory of planned behavior: A review ofits application to health-related behaviors. American Journal of HealthPromotion, 11, 87–98.
Greenslade, J. H., & White, K. M. (2005). The prediction of above-averageparticipation in volunteerism: A test of the theory of planned behaviorand the Volunteers Functions Inventory in older Australian adults.Journal of Social Psychology, 145, 155–172.
Halkett, R. (1999). HIV/AIDS and the care of children. Braamfontein, SouthAfrica: South African National Council for Child and Family Welfare.
Hankins, M., French, D., & Horne, R. (2000). Statistical guidelines forstudies of the theory of reasoned action and the theory of planned behav-ior. Psychology and Health, 15, 151–181.
Harber, M. (1999). Models of care for AIDS orphans: Lessons from Sub-Saharan Africa. Durban, South Africa: University of Natal, Centre forSocial and Development Studies.
Hewstone, M. (1986). Towards a social psychological analysis of “Euro-peanism.” In Hewstone M. (Ed.), Understanding attitudes to the Europeancommunity: A social psychological study in four member states (pp. 51–94).Cambridge, UK: Cambridge University Press.
Kridli, S. A.O., & Newton, S. E. (2005). Jordanian married Muslim women’sintentions to use oral contraceptives. International Nursing Review, 52,109–114.
Madhavan, S. (2004). Fosterage patterns in the age of AIDS: Continuity andchange. Social Science and Medicine, 58, 1443–1454.
Mbambo, B. (2005). HIV/AIDS: Thief of childhood. ChildrenFirst, 9, 36–37.McMillan, B., Higgins, A. R., & Connor, M. (2005). Using an extended
theory of planned behavior to understand smoking among schoolchil-dren. Addiction Research and Theory, 13, 293–306.
Nyambedha, E. O., Wandibba, S., & Aagaard-Hansen, J. (2003). Changingpatterns of orphan care due to the HIV epidemic in western Kenya. SocialScience and Medicine, 57, 301–311.
Nyamukapa, C., & Gregson, S. (2005). Extended family’s and women’s rolesin safeguarding orphans’ education in AIDS-afflicted rural Zimbabwe.Social Science and Medicine, 60, 2155–2167.
Payne, N., Jones, F., & Harris, P. R. (2005). The impact of job strain onpredictive validity of the theory of planned behaviour: An investigation of
842 TOWNSEND AND DAWES

exercise and healthy eating. British Journal of Health Psychology, 10,115–131.
Povey, R., Connor, M., Sparks, P., James, R., & Shepherd, R. (2000). Appli-cation of the theory of planned behaviour to two dietary behaviours:Roles of perceived control and self-efficacy. British Journal of HealthPsychology, 5, 121–139.
Quintin, D., Rushton, A., Dance, C., & Mayers, D. (1998). Joining newfamilies: A study of adoption and fostering in middle childhood. New York:John Wiley & Sons.
Scholtz, S. (1997). Draft discussion on foster care guidelines. Pretoria, SouthAfrica: Department of Welfare.
Sideridis, G. D. (2005). Attitudes and motivations of poor and good spellers:Broadening planned behavior theory. Reading and Writing Quarterly:Overcoming Learning Difficulties, 21, 87–103.
Smart, R. (2000). Children living with HIV/AIDS in South Africa: A rapidappraisal. Pretoria, South Africa: National AIDS and Children TaskTeam.
South African National Council for Child and Family Welfare. (1996). Aguide to adoption practice in the child welfare movement: South Africa.Braamfontein, South Africa: Author.
Townsend, L. (2001). Decisions to care for HIV/AIDS orphans. Master’sThesis, Department of Psychology, University of Cape Town, SouthAfrica.
Townsend, L., & Dawes, A. (2004). Willingness to care for children orphanedby HIV/AIDS: A study of foster and adoptive parents. African Journal ofAIDS Research, 3, 69–80.
Whiteside, A., & Sunter, C. (2000). AIDS: The challenge for South Africa.Cape Town, South Africa: Human & Rousseau.
Wild, L. (2001). The psychosocial adjustment of children orphaned by AIDS.Southern African Journal of Child and Adolescent Mental Health, 13, 3–22.
HIV/AIDS ORPHANS AND THE THEORY OF PLANNED BEHAVIOR 843