Integrating Public Health into Emergency and Disaster Risk ...
19
© UNDRR – United Nations Office for Disaster Risk Reduction With the support of Integrating Public Health into Emergency and Disaster Risk Reduction Planning Session 2: National to Local Governance for Effective Health Emergency Management.
Transcript of Integrating Public Health into Emergency and Disaster Risk ...

© UNDRR – United Nations Office for Disaster Risk Reduction
With the support of
Integrating Public Health into Emergency and Disaster Risk Reduction Planning
Session 2: National to Local Governance for Effective Health
Emergency Management.

© UNDRR – United Nations Office for Disaster Risk Reduction
Disaster Resilience
In the Context of Cities:
“the ability to withstand and bounce back from both acute shocks (natural and manmade) such as floods, earthquakes, hurricanes, wild-fires, chemical spills, power outages, as well as chronic stresses occurring over longer time scales, such as groundwater depletion or deforestation, or socio-economic issues such as homelessness and unemployment.”
Roly-poly toy
- the Sendai Framework for DRR 2015-2030

© UNDRR – United Nations Office for Disaster Risk Reduction
What makes the fictional city of Drecca-Susdev resilient?
The Global Assessment Report on Disaster Risk Reduction (GAR), 2019
Fictional delta city of Drecca-Susdev - some elements of integrated risk governance

© UNDRR – United Nations Office for Disaster Risk Reduction
• City is made up of different
systems
• These systems have multiple
connections and interactions
• Causal
• Resources
• Data
• Because each system will have
different owners and
stakeholders, resilience is a
multi-organizational endeavor.
Resilience must embrace “systems of systems”
Energy, Fuel
Water, sanitation
Protective infrastructure
Telecommuni-cations, data
Food storage and delivery
Healthcare, public health
Ecosystem services
Social systems
Public safety
Mass & private transportation,

© UNDRR – United Nations Office for Disaster Risk Reduction
Resilience is a process, with multiple timescales
Some resilience functions play out over many years. Others require real time
response.
Multi-Decade
sDecade
Sub-decade →
Years
Months →Wee
ks
Days→ Hours
Hours→ Days
Weeks→
Months
Years→ Sub
decade
Long run risk prediction (egclimate impacts, earthquake risk
Long run exposure predictions –eg urban boundaries
Land use decisions
Consumption patterns
Major infrastructure hardening and duplication
Production methods
Building code revisions
Emergency planning and simulation
Corporate risk assessment and mitigation
Building public awareness, drills
(Monitoring of famines, droughts)
Seasonal weather forecasting (eghurricanes)
Pre-positioning supplies
Pre-event maintenance (egstorm drains)
Evacuation and property securing
Enhanced law and order presence
Event tracking and alerts
Impact tracking
First response
Survivor search
Debris removal
Emergency shelter, food, first aid, power
Restarting infrastructure
Loss adjustments, insurance payments
Short run economic reboot
Rebuilding, economic recovery
Finding the “new normal” – changed social norms, business methods, transport methods etc.
Learn and improve

© UNDRR – United Nations Office for Disaster Risk Reduction
The resilience process for diseases (examples)
As with other disasters, some disease management functions play out over many years.
Others require real time response.
Multi-Decade
sDecade
Sub-decade
→ Years
Months →Wee
ks
Days→ Hours
Hours→ Days
Weeks→
Months
Years→ Sub
decade
Long run exposure predictions –eg urban boundaries, population densities
Land use decisions
“Surge capacities”
Healthcare infrastructure hardening and duplication
Supply chain scanning and “topping up”
Pandemic planning and simulation
Corporate risk assessment and mitigation
Building public awareness, drills
(Monitoring of disease onset)
First lockdowns, social distancing as required
Pre-event maintenance (equipment, facilities), pre-positioning of supplies
Contact tracing for first cases
Enhanced law and order presence
Disease trend analysis, hotspot detection
Unwind lockdowns and social distancing
Continued trend analysis
Re-boot business
Short run economic support -business and personal bailouts
Economic recovery
Learn and improve
Attitudes to collective action vs individual rights
Continuous public awareness and comms
Treat the sick
Understand disease biology, pathology
Continuous public awareness and comms
Create vaccines
Support families
Finding the “new normal” – changed social norms, business methods, transport methods etc.
© UNDRR – United Nations Office for Disaster Risk Reduction
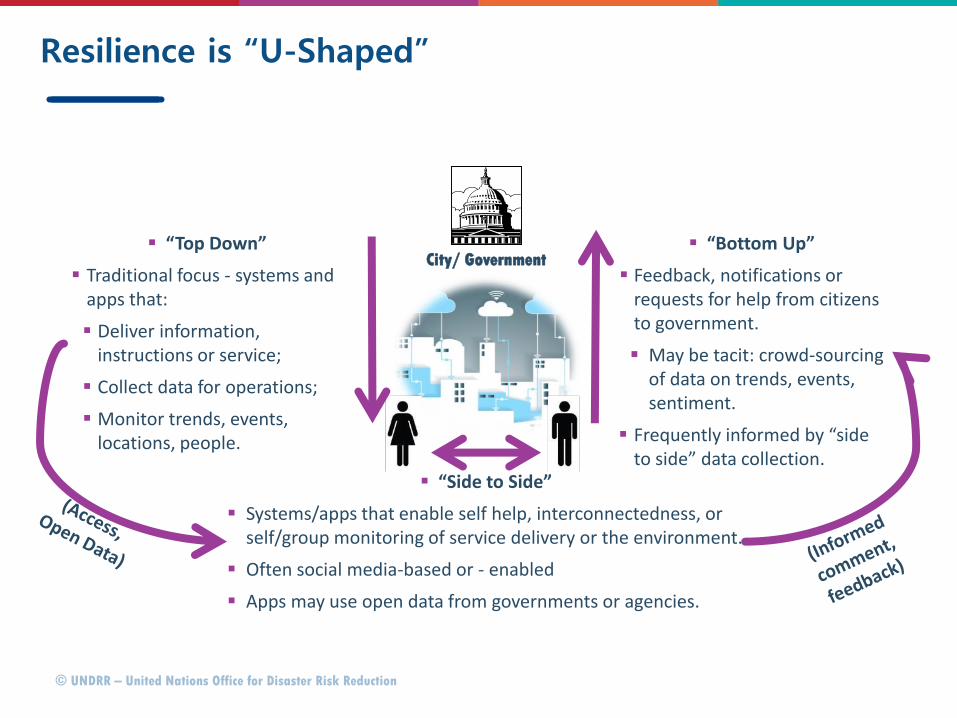
Resilience is “U-Shaped”
“Top Down”
Traditional focus - systems and apps that:
Deliver information, instructions or service;
Collect data for operations;
Monitor trends, events, locations, people.
“Bottom Up”
Feedback, notifications or requests for help from citizens to government.
May be tacit: crowd-sourcing of data on trends, events, sentiment.
Frequently informed by “side to side” data collection.
City/ Government
“Side to Side”
Systems/apps that enable self help, interconnectedness, or self/group monitoring of service delivery or the environment.
Often social media-based or - enabled
Apps may use open data from governments or agencies.

© UNDRR – United Nations Office for Disaster Risk Reduction
A “U-Shaped” response to pandemics and disease management
“Top Down”
Shelter in place, business opening instructions.
Data on pandemic progress by locale.
Advice on symptoms and staying healthy.
Locations of treatment facilities.
Projections for resuming normal activity.
“Bottom Up”
Centralized contact tracing.
Crowd-sourcing of data on events, sentiment, how people are coping.
Applications for help (financial and other).
Questions, comments, concerns.
City/ Government
“Side to Side”
Community awareness/ability to activate mitigation options
Disaggregated contact tracing
Data on neighborhood help resources – local Q & A.
Requests/offers for help

© UNDRR – United Nations Office for Disaster Risk Reduction
The “Ten Essentials” MCR2030
Pros: Relatively holistic, complete coverage of the field, and allows “systems of systems” (technological, social, economic) to be addressed: great for making connections between these.
Con: public health system issues don’t emerge clearly from this structure.

© UNDRR – United Nations Office for Disaster Risk Reduction
Resilience embraces chronic stresses and acute events

© UNDRR – United Nations Office for Disaster Risk Reduction
Examples of chronic stress and acute event interactions in a pandemic
Chronic stresses
Drive acute events where:
– Economic stress (poverty) leads to higher risk of contracting diseases such as COVID-19, through population density, poor sanitation and underlying ill-health;
– Lack of open space makes it harder to exercise and maintain social distancing.
– Air pollution increases susceptibility to the disease.
Acute event (pandemic)
Exacerbate chronic stresses where:
– Enforced closures force local businesses such as food stores and cafes and to close, so causing social and economic stress through lack of facilities and unemployment.
– Public transportation is forced to close – so preventing people who may not have cars from getting to work.
May predispose to, or worsen acute eventsMay hinder recovery
May exacerbate chronic stresses
Interactions

© UNDRR – United Nations Office for Disaster Risk Reduction
can be downloaded for free from: https://www.unisdr.org/campaign/resilientcities/home/toolkitblkitem/?id=4
A further version of the Scorecard, for industrial and commercial buildings was recently published and is available for free from: https://www.preventionweb.net/publications/view/69845.
The Disaster Resilience Scorecard for Cities

© UNDRR – United Nations Office for Disaster Risk Reduction
Multisectoral mechanism for supporting pandemic management
WHO guidance on
Health Emergency and
Disaster Risk
Management
Disaster Resilience Scorecard for
Cities
Public health system resilience scorecard
Pandemic/disaster risk management
MCR2030

© UNDRR – United Nations Office for Disaster Risk Reduction
Available for use from: https://www.unisdr.org/campaign/resilientcities/toolkit/article/public-health-system-resilience-scorecard
The Public Health System Resilience Scorecard

© UNDRR – United Nations Office for Disaster Risk Reduction
Structure of the Public Health System Resilience Scorecard
Hospitals – local, regional;
Isolation facilities;
Residential facilities, nursing homes, assisted living facilities;
Community health clinics, doctors’ offices, outpatient care facilities;
EMS systems;
Mental health facilities;
Health laboratory and testing facilities;
Public sector health departments.
Water and sanitation systems;
Food distribution systems;
Pharmaceutical and medical supply distribution systems, drug stores;
Environmental health systems;
Community information, engagement and outreach processes and facilities;
Skills, staff, assets, facilities and equipment required to function –availability post-disaster.
Tele-medicine/tele-health systems.
Created to address the one obvious weakness in the “Ten Essentials”.
Uses the same “Ten Essentials” structure as the City scorecard – in the context of a pandemic, focuses on the wider issues of management and recovery
It is NOT a medical or epidemiological tool, although these disciplines will inform answers given.
Addresses the “non-medical” issues of a medical emergency.

© UNDRR – United Nations Office for Disaster Risk Reduction
Examples of What is Covered in the Public Health Addendum
Essential Examples in Healthcare Addendum
1. Organization & Governance • Are public health and medical professionals involved in disaster planning and management?• Are other professionals (e.g. sanitation, water, energy, comms) involved in public health planning?
2. Risk understanding • Inclusion of a pandemic scenario in risk planning.• Inclusion of pandemics (and pre-existing chronic health stresses – malaria, malnutrition) as a complexity factor,
alongside “disasters as usual” – floods, earthquakes, fire etc.
3. Financial architecture • Adequacy and protection of of funding• Resilience “dividends” – other benefits that arise from resilience spending
4. Land use and building codes • Code and zoning compliance of key facilities
5. Ecosystem services • Protection of ecosystem services with health benefits - natural water filtration, tree cover, recreation space
6. Capacity • Availability of public health skills – medical and other• Availability and sharing of required data with (that is, to and from) other stakeholders
7. Social capacity • Community engagement processes and effectiveness• Community trust of information provided• Community mental health and mental stress management
8. Infrastructure • Resilience of key health infrastructures• Resilience of other relevant infrastructures– water, power, communications, sanitation, trash collection.• Surge capacity• Continuity of care facilities for those already sick
9. Disaster response • Early warning systems• Integration with emergency management• Education, rehearsals, drills, public health supplies
10. Recovery planning • Offsetting long run impacts on health• Learning and improving.

© UNDRR – United Nations Office for Disaster Risk Reduction
Scorecard indicators relevant to pandemic/disease outbreak
No Assesses*
A1.1/9.2 Governance mechanisms for disaster risk and emergency management include public health professionals
• Emergency care, primary care, environmental heath, epidemiology, medical supplies, other government entities, etc.
A2.1 Disaster risk planning includes public health emergencies
• Pandemics/outbreaks and other public health disasters are included in risk scenarios adopted by the city.
A2.2 Consideration of public health impacts arising from other disasters
• Trauma and post-trauma care, treatment of chronic conditions, water and food-borne illnesses, quarantine facilities, emergency shelters, psychological care, etc.
A3.1 Funding earmarked for addressing public health implications of disasters
• Essential hospital services, alternate care sites, emergency medical supplies, etc.
A6.1 Sufficient, skilled health professionals to maintain public health around disasters
• Doctors, nurses, allied health professionals, pharmacists, environmental health, epidemiologists, supply chain
managers, laboratory technicians, etc.
A6.2 Public health data shared with all stakeholders that need it
• Awareness of public health assets and facilities needs pre and post disaster.* Questions have been summarized

© UNDRR – United Nations Office for Disaster Risk Reduction
Disaster Risk Reduction Terminology: http://www.preventionweb.net/english/professional/terminology/
Sendai Framework for Disaster Risk Reduction 2015-2030, UN: http://www.preventionweb.net/drr-framework/sendai-framework
The Global Assessment Report & Global Risk Atlas: http://www.preventionweb.net/gar/
Understanding Disaster Risk – based upon GARs 2009, 2011, 2013, 2015, UNISDR – including risk models, viewers and data:
http://www.preventionweb.net/risk and http://risk.preventionweb.net/capraviewer
The Global Risks Report 2019, 14th Edition, World Economic Forum: http://www3.weforum.org/docs/WEF_Global_Risks_Report_2019.pdf
Unbreakable, GFDRR, World Bank: https://www.gfdrr.org/sites/default/files/publication/Unbreakable_FullBook_Web-3.pdf
Making Cities Resilient Campaign Website: https://www.unisdr.org/campaign/resilientcities/
A Handbook For Local Government Leaders [2017 Edition]: https://www.unisdr.org/campaign/resilientcities/toolkit/article/a-handbook-for-local-
government-leaders-2017-edition
10 Essentials for Making Cities Resilient: https://www.unisdr.org/campaign/resilientcities/toolkit/article/the-ten-essentials-for-making-cities-resilient
Health Emergency and Disaster Risk Management Framework, WHO : https://www.who.int/hac/techguidance/preparedness/health-emergency-and-
disaster-risk-management-framework-eng.pdf?ua=1
Key Resources

© UNDRR – United Nations Office for Disaster Risk Reduction
With the support of
Thank YouUNDRR
Global Education and Training Institute (GETI)
4F Songdo G-Tower,
175 Art Center-daero,
Yeonsu-gu, Incheon
Republic of Korea