Information for Patients Undergoing Cataract Surgery · Page 3 This leaflet gives you information...
12
Blackpool Teaching Hospitals NHS Foundation Trust Information for Patients Undergoing Cataract Surgery Ophthalmic Directorate People Centred Excellence Compassion Positive
Transcript of Information for Patients Undergoing Cataract Surgery · Page 3 This leaflet gives you information...

Blackpool Teaching Hospitals
NHS Foundation Trust
Information for Patients Undergoing Cataract
Surgery
Ophthalmic Directorate
People Centred ExcellenceCompassionPositive

Page 2
1. Information for patients 3
The cataract
The operation
After the operation
Likelihood of better vision
Benefits and risks of cataract surgery
Some possible complications during the operation
Some possible complications after the operation
3
3
4
5
5
5
6
2. Checklist: One week before cataract surgery 7
3. Checklist: The day before surgery 7
4. Instructions for the day of surgery 7
5. Post-operative care 8
6. Consent Form for Cataract Surgery (for reading purposes only) 9-10
7. Directions to the Ophthalmic Surgical Unit 11
index

Page 3
This leaflet gives you information that will help you decide whether to have cataract surgery. You might want to discuss it with a relative or carer. Before you have the operation, you will be asked to sign a consent form and so it is important that you understand the leaflet before you decide to have surgery. A copy of the consent form you will be asked to sign can be found on page 9 and 10. Please read this before you arrive at the hospital.
If you have any questions, you may wish to write them down in the box on page 6, so that you can ask one of the hospital staff.
The cataractYour eye surgeon has recommended cataract surgery because the lens in your eye has become cloudy making it difficult for you to see well enough to carry out your usual daily activities. If the cataract is not removed, your vision may stay the same, but it will probably gradually get worse. Waiting for a longer period of time is unlikely to make the operation more difficult, unless your eyesight becomes so poor that all you can see is light and dark.
The operationThe purpose of the operation is to replace the cloudy lens (cataract) with a plastic lens (implant) inside your eye.
• An experienced eye surgeon will carry out the operation or may supervise a doctor in training who also performs some operations.
• Please do not wear any face or eye makeup on the day of surgery
• You will be able to go into theatre wearing your own clothes
• Dentures (if you wear them) need not be removed
• You will come to the Ophthalmic Surgical Unit (OSU) to be prepared for your operation
• In the hour before the operation you will have a series of eye drops instilled to enlarge the pupil. This is in fact a hole in the coloured part of the eye, the iris.
• After this you will be escorted to the anaesthetic room in the theatre where you will be given an anaesthetic to numb the eye. This may consist simply of eye drops or injecting local anaesthetic solution into the tissue surrounding the eye. After the anaesthetic you will not feel any discomfort or pain.

Page 4
With a local anaesthetic you will be awake during the operation. You will not be able to see what is happening, but you will be aware of a bright light.
You will be escorted to theatre where your operation will take place. A peg will be clipped onto one of your fingers to monitor your pulse. The area around your eye is cleaned and then a light sterile drape will cover your face and chest. A tube underneath the drape gently blows out some fresh air therefore you will be able to breathe normally.
During the operation you will be asked to keep your head still, and lie as flat as possible.
A member of the nursing staff is usually available to hold your hand during the operation, should you want them to.
The lids of the eye, to be operated on, will be held open with a small instrument.
You will be asked to refrain from talking during the operation but you can be assured that a nurse will be present to ensure that you are comfortable.
The operation normally takes 15-20 minutes, but may take up to 45 minutes. Most cataracts are removed by a technique called phacoemulsification, in which the surgeon makes a very small cut in the eye, softens the lens with sound waves and removes the cataract through a small tube. The back layer of the lens is left behind. An artificial lens (implant) is then inserted to replace the cataract. Sometimes a small stitch is put in the eye. At the end of the operation, a pad or shield may be put over your eye to protect it.
After the operationIf you have discomfort, we suggest that you take a pain reliever such as paracetamol every 4-6 hours (but not aspirin - this can cause bleeding). It is normal to feel itching, sticky eyelids and mild discomfort for a while after cataract surgery. Some fluid discharge is common. After a few days even mild discomfort should disappear. In most cases, healing will take upto 6 weeks, after which new glasses can be prescribed by your optician. You will be given eye drops to reduce inflammation. The hospital staff will

Page 5
explain how and when to use them. Please don’t rub your eye. Certain symptoms could mean that you need prompt treatment, including:
• Excessive pain
• Loss of vision
• Increasing redness of the eye
You will be given an emergency telephone number to ring in case you develop any of the above, or should you need urgent advice about your eye.
Monday-Friday, 9am-5pm 01253 957420
Out of hours and weekends - Ward 15A Tel. 01253 953415. For all ophthalmic queries, help and advice.
Likelihood of better visionAfter the operation you may read or watch TV almost straight away, but your vision may be blurred. The healing eye needs time to adjust so that it can focus properly with the other eye, especially if the other eye has a cataract.
The vast majority of patients have improved eyesight following cataract surgery
Please note that if you have another condition such as diabetes, glaucoma or age-related macular degeneration your quality of vision may still be limited even after successful surgery.
Benefits and risks of cataract surgery The most obvious benefits are greater clarity of vision and improved colour vision. Because lens implants are selected to compensate for existing focusing problems, most people find that their eyesight improves considerably after surgery but you will need to replace your glasses. Reading glasses are usually needed after cataract surgery.
However, you should be aware that there is a small risk of complications, either during or after the operation.
Some possible complications during the operation• Tearing of the back part of the lens capsule with disturbance of the gel inside the eye
that may sometimes result in reduced vision.
• Loss of all or part of the cataract into the back of the eye requiring a further operation which may require a general anaesthetic.
• Bleeding inside the eye.

Page 6
Some possible complications after the operation• Bruising of the eye or eyelids.
• High pressure inside the eye.
• Clouding of the cornea.
• Incorrect strength or dislocation of the implant.
• Swelling of the retina - macular oedema.
• Detached retina which can lead to loss of sight.
• Infection in the eye - endophthalmitis - which can lead to loss of sight, or even loss of the eye.
• Allergy to the medication used.
• Several complications listed above may result in permanent sight loss.
Complications are rare and in most cases can be treated effectively. In a small proportion of cases, further surgery may be needed. Very rarely some complications can result in blindness.
The most common complication is called ‘posterior capsular opacification’. It may come on gradually after months or years after cataract surgery. When this happens, the back part of the lens capsule, which was left in the eye to support the implant, becomes cloudy. This prevents light from reaching the retina. To treat this, the eye specialist uses a laser beam to make a small opening in the cloudy membrane in order to improve the eyesight. This is a painless outpatient procedure which normally takes only a few minutes.
We hope this information is sufficient to help you decide whether to go ahead with surgery.
Please use the space below to write down any further questions to ask the doctor or nurse when you come to the hospital for your appointment. Don’t worry about asking questions. Our staff will be happy to answer them.

Page 7
Checklist: One week before cataract surgery
1. Ensure that your blood glucose levels are stable if you are diabetic (below 21mmol/l).
2. Ensure your blood pressure is below 200/110 if you suffer from high blood pressure.
3. Check your warfarin blood levels and ensure these are within the therapeutic range.
4. Take all medications as normal upto and including the day of surgery.
5. Arrange transport to arrive in time for your appointment.
6. If you develop any illnesses, coughs, colds or any medical or eye conditions please let us know by phoning 01253 957420. This will prevent you being cancelled on the day and the operation slot can be offered to someone else.
7. You will not be able to drive home yourself so please ensure you have someone with you and a means of transport home.
Checklist: The day before surgery1. Ensure the above are completed.
2. You can eat or drink as normal.
3. Bring with you a list of your medication. It maybe that the doctor will wish to see this.
4. Take your normal medication. If you take warfarin, and you know your levels are abnormal you must ring the department as soon as you can.
5. Have the telephone number with you of the person taking you home.
Instructions for the day of surgery1. Report to the reception desk upon arrival to the hospital
2. If you are having a local anaesthetic you can have a light meal prior to the surgery.
3. You should continue to take all medications for blood pressure, heart problems, asthma and epilepsy with sips of water up to 2 hours prior to surgery. Please bring your daily medications with you (in their original containers) on the day of your operation.
4. Leave all jewellery and large sums of money at home. Bring just enough money for a taxi ride home. The hospital assumes no responsibility in the case of loss.
5. You will be asked to remove all make-up and hair ornaments. Rings that cannot be removed will be secured with tape. Please remember to bring your contact lens container.
6. If you are to have a general anaesthetic, an intravenous drip may be started before your procedure.

Page 8
Use black biro to complete form.
File in Section 3
Patient agreement to investigation or treatment(Designed in compliance with the Department of Health consent form 1)
CONSENT FORM 1Responsible health professional ....................................................
Job title ............................................................................................Special requirements: ........................................(eg other language/other communication method)
All patients about to undergo any elective or emergency surgical or endoscopic procedure likely to involve contact with tissuesof medium or low level infectivity should be asked the question:-‘’Have you ever been notified that you are at increased risk of Creutzfeldt-Jakob disease (CJD) or variant Creutzfeldt-Jakobdisease (vCJD) for public health purposes?’’ If the patient’s response is No, proceed using normal infection prevention measures. If the answer is Yes, please ask the patient to explain further and consult the Infection Prevention Team for advice. If the procedure is likely to involve contact with tissues of potentially high level infectivity (Brain, spinal cord, implanted duramater grafts prior to 1992, cranial nerves and ganglia, pituitary gland and posterior eye (specifically: posterior hyaloid face,retina, retinal pigment epithelium, choroid, sub retinal fluid and optic nerve) the following questions should be asked:-1. Have you a history of CJD or other prion disease in your family? 2. Have you ever received growth hormone or gonadotrophin treatment? 3. Have you ever had surgery on your brain or spinal cord? If the answer to any of these questions is Yes, please discuss with the consultant in charge of the case and consult the InfectionPrevention Team for advice.
Approved by the Health Records Committee 00/00/2014 VS335 (R2)
Contact Details (if patient wishes to discuss optionslater)
Statement of interpreter (where appropriate)
I have interpreted the information above to the patient tothe best of my ability and in a way in which I believe s/hecan understand.
Signed ....................................................................................
Date........................................................................................
Name (PRINT) ........................................................................
Statement of patientPlease read this form carefully. If your treatment has been planned in advance, you should already haveyour own copy of page 1 which describes the benefits and risks of the proposed treatment. If not, you willbe offered a copy now. If you have any further questions, do ask - we are here to help you. You have theright to change your mind at any time, including after you have signed this form.
I agree to the procedure or course of treatment described on this form.
I understand that you cannot give me a guarantee that a particular person will perform the procedure.The person will, however, have appropriate experience.
I understand that I will have the opportunity to discuss the details of anaesthesia with an anaesthetistbefore the procedure, unless the urgency of my situation prevents this. (This only applies to patientshaving general or regional anaesthesia).
I understand that any procedure in addition to those described on this form will only be carried out if it isnecessary to save my life or to prevent serious harm to my health.
I have been told about additional procedures which may become necessary during my treatment. I havelisted below any procedures which I do not wish to be carried out without further discussion.
................................................................................................................................................................................
................................................................................................................................................................................
................................................................................................................................................................................
Patient’s signature ...................................................................... Date ..................................................................
Name (PRINT) ..........................................................................................................................................................
A witness should sign below if the patient is unable to sign but has indicated his or her consent. Young people/children may also like a parent to sign here (see notes).
Signed .......................................................................................... Date ..................................................................
Name (PRINT) ..........................................................................................................................................................
Confirmation of consent (to be completed by a health professional when the patient is admitted forthe procedure, if the patient has signed the form in advance).
On behalf of the team treating the patient, I have confirmed with the patient that s/he has no furtherquestions and wishes the procedure to go ahead.
Right eye Name/signature................................................................ date ................................................
Left eye Name/signature................................................................ date ................................................
Important notes: (tick if applicable)� See also advance directive/living will (eg Jehovah’s Witness form)
� Patient has withdrawn consent (ask patient to sign/date here ....................................................................
Bottom copy accepted by patient: yes / no (please ring) Patients Notes
Name of proposed procedure or course of treatment: Right eye / left eyeCataract extraction and intraocular lens insertion including photography/video for teachingand publicationStatement of health professional (to be filled in by health professional with appropriate knowledge ofproposed procedure, as specified in consent policy)
I have explained the procedure to the patient. In particular, I have explained:The aim of the cataract operation is to improve the quality of your vision. Surgery may also improve the doctors'view of the back of the eye. We will try to reduce your dependence on spectacles as much as possible, but youmay require distance glasses for best vision and will probably need reading glasses. Your glasses prescription willchange after the operation.
Serious or frequently occurring risksIt is possible for cataract surgery to leave you worse off than you are now. One person in every 1000 will go blindin that eye as a direct result of the operation. One in 10,000 will lose the eye. There is virtually no risk to theother eye. Details on the most common specific complications are given below.Ecchymosis - Bruising of eye or eyelids (quite common).Posterior capsule rupture and / or vitreous loss - a split in the thin back wall of the cataract which can allowcommunication between front and back compartments of the eye.Post operative glaucoma - raised pressure in the eye for the first day or so (common). This may require treatment.Posterior capsular opacification - clouding of the membrane behind the implant causing blurred vision.Cystoid macular oedema - inflammatory fluid in the centre of the retina. This is commonly mild and needs notreatment. It can be severe and require prolonged treatment.Refractive surprise - unexpectedly large (or different from expected) need for glasses.Allergy - to drops given after the operation, causing an itchy swollen eye until the drops are stopped or changed.Dropped nucleus - part or all of the cataract falls into the back part of the eye, needing another operation toremove it.Corneal decompensation - clouding of the normally clear front window of the eye.Detached retina - peeling off of the seeing layer of cells within the eye.Endophthalmitis - severe (usually painful) infection inside the eye.Dislocation of the implant - movement out of position of the lens implant.Complications are rare and in most cases can be treated effectively. In a small proportion of cases, a furtheroperation may be required. If you decide against a cataract operation, your vision will probably slowly worsen.
Individual additional risks - (e.g. deterioration of diabetic retinopathy, corneal oedema, unexpected refractiveoutcome particularly post laser patients)
Extra procedures that may be necessary during the procedure - Vitrectomy
..........................................................................................................................................................................................
..........................................................................................................................................................................................� The following leaflet/tape has been provided: Cataract Surgery information leafletThis procedure will involve: � general and/or regional anaesthesia � local anaesthesia � sedation
Signed .......................................................................................... Date ..........................................................................
Name (PRINT................................................................................Job title ......................................................................
Write patient details or affixIdentification label
Hospital Number:Name:Address:
Date of Birth:NHS Number:
7. You are NOT TO DRIVE after receiving a general anaesthetic or sedation. You must arrange for a responsible adult to drive you to and from the hospital. You must not operate hazardous machinery, drive a car or sign important documents for 48 hours.
8. Wear loose, comfortable clothing.
After your surgery, you may return to the hospital recovery area for a short time, where you will be given something to eat and drink.
Post-operative care After your surgery we would like you to go home and take it easy.
You are NOT to use any eye drops that evening.
Please do not rub or touch the eye.
It is normal for your eye to feel some itching and mild discomfort after surgery.
Some discharge is also common and your eye may be sensitive to lights.
If there is slight discomfort you can use a mild pain reliever (paracetamol).
If you experience a lot of pain or a decrease in your vision, you should contact the hospital. This is not normal.
1. Avoid lifting anything over 20 lbs. or 9 kilos in weight for two weeks (Children, groceries etc.).
2. Avoid water sports or swimming for two weeks.
3. You can have a shower but avoid getting water or soap into the operated eye.
4. You can wash your hair by tilting your head backward as at the hairdressers.
i. Certain sport activities need to be avoided (i.e. bowling, swimming) for a time, usually 2 weeks.
ii. If you still work, it will depend upon your job when it would be safe to go back to work. Please discuss with your doctor.
iii. You may drive if you are legally able to do so. Some patients may need to wait 3-4 weeks until they have new glasses prescribed.
Please discuss any activities you would like to participate in with the doctor.

Use black biro to complete form.
File in Section 3
Patient agreement to investigation or treatment(Designed in compliance with the Department of Health consent form 1)
CONSENT FORM 1Responsible health professional ....................................................
Job title ............................................................................................Special requirements: ........................................(eg other language/other communication method)
All patients about to undergo any elective or emergency surgical or endoscopic procedure likely to involve contact with tissuesof medium or low level infectivity should be asked the question:-‘’Have you ever been notified that you are at increased risk of Creutzfeldt-Jakob disease (CJD) or variant Creutzfeldt-Jakobdisease (vCJD) for public health purposes?’’ If the patient’s response is No, proceed using normal infection prevention measures. If the answer is Yes, please ask the patient to explain further and consult the Infection Prevention Team for advice. If the procedure is likely to involve contact with tissues of potentially high level infectivity (Brain, spinal cord, implanted duramater grafts prior to 1992, cranial nerves and ganglia, pituitary gland and posterior eye (specifically: posterior hyaloid face,retina, retinal pigment epithelium, choroid, sub retinal fluid and optic nerve) the following questions should be asked:-1. Have you a history of CJD or other prion disease in your family? 2. Have you ever received growth hormone or gonadotrophin treatment? 3. Have you ever had surgery on your brain or spinal cord? If the answer to any of these questions is Yes, please discuss with the consultant in charge of the case and consult the InfectionPrevention Team for advice.
Approved by the Health Records Committee 00/00/2014 VS335 (R2)
Contact Details (if patient wishes to discuss optionslater)
Statement of interpreter (where appropriate)
I have interpreted the information above to the patient tothe best of my ability and in a way in which I believe s/hecan understand.
Signed ....................................................................................
Date........................................................................................
Name (PRINT) ........................................................................
Statement of patientPlease read this form carefully. If your treatment has been planned in advance, you should already haveyour own copy of page 1 which describes the benefits and risks of the proposed treatment. If not, you willbe offered a copy now. If you have any further questions, do ask - we are here to help you. You have theright to change your mind at any time, including after you have signed this form.
I agree to the procedure or course of treatment described on this form.
I understand that you cannot give me a guarantee that a particular person will perform the procedure.The person will, however, have appropriate experience.
I understand that I will have the opportunity to discuss the details of anaesthesia with an anaesthetistbefore the procedure, unless the urgency of my situation prevents this. (This only applies to patientshaving general or regional anaesthesia).
I understand that any procedure in addition to those described on this form will only be carried out if it isnecessary to save my life or to prevent serious harm to my health.
I have been told about additional procedures which may become necessary during my treatment. I havelisted below any procedures which I do not wish to be carried out without further discussion.
................................................................................................................................................................................
................................................................................................................................................................................
................................................................................................................................................................................
Patient’s signature ...................................................................... Date ..................................................................
Name (PRINT) ..........................................................................................................................................................
A witness should sign below if the patient is unable to sign but has indicated his or her consent. Young people/children may also like a parent to sign here (see notes).
Signed .......................................................................................... Date ..................................................................
Name (PRINT) ..........................................................................................................................................................
Confirmation of consent (to be completed by a health professional when the patient is admitted forthe procedure, if the patient has signed the form in advance).
On behalf of the team treating the patient, I have confirmed with the patient that s/he has no furtherquestions and wishes the procedure to go ahead.
Right eye Name/signature................................................................ date ................................................
Left eye Name/signature................................................................ date ................................................
Important notes: (tick if applicable)� See also advance directive/living will (eg Jehovah’s Witness form)
� Patient has withdrawn consent (ask patient to sign/date here ....................................................................
Bottom copy accepted by patient: yes / no (please ring) Patients Notes
Name of proposed procedure or course of treatment: Right eye / left eyeCataract extraction and intraocular lens insertion including photography/video for teachingand publicationStatement of health professional (to be filled in by health professional with appropriate knowledge ofproposed procedure, as specified in consent policy)
I have explained the procedure to the patient. In particular, I have explained:The aim of the cataract operation is to improve the quality of your vision. Surgery may also improve the doctors'view of the back of the eye. We will try to reduce your dependence on spectacles as much as possible, but youmay require distance glasses for best vision and will probably need reading glasses. Your glasses prescription willchange after the operation.
Serious or frequently occurring risksIt is possible for cataract surgery to leave you worse off than you are now. One person in every 1000 will go blindin that eye as a direct result of the operation. One in 10,000 will lose the eye. There is virtually no risk to theother eye. Details on the most common specific complications are given below.Ecchymosis - Bruising of eye or eyelids (quite common).Posterior capsule rupture and / or vitreous loss - a split in the thin back wall of the cataract which can allowcommunication between front and back compartments of the eye.Post operative glaucoma - raised pressure in the eye for the first day or so (common). This may require treatment.Posterior capsular opacification - clouding of the membrane behind the implant causing blurred vision.Cystoid macular oedema - inflammatory fluid in the centre of the retina. This is commonly mild and needs notreatment. It can be severe and require prolonged treatment.Refractive surprise - unexpectedly large (or different from expected) need for glasses.Allergy - to drops given after the operation, causing an itchy swollen eye until the drops are stopped or changed.Dropped nucleus - part or all of the cataract falls into the back part of the eye, needing another operation toremove it.Corneal decompensation - clouding of the normally clear front window of the eye.Detached retina - peeling off of the seeing layer of cells within the eye.Endophthalmitis - severe (usually painful) infection inside the eye.Dislocation of the implant - movement out of position of the lens implant.Complications are rare and in most cases can be treated effectively. In a small proportion of cases, a furtheroperation may be required. If you decide against a cataract operation, your vision will probably slowly worsen.
Individual additional risks - (e.g. deterioration of diabetic retinopathy, corneal oedema, unexpected refractiveoutcome particularly post laser patients)
Extra procedures that may be necessary during the procedure - Vitrectomy
..........................................................................................................................................................................................
..........................................................................................................................................................................................� The following leaflet/tape has been provided: Cataract Surgery information leafletThis procedure will involve: � general and/or regional anaesthesia � local anaesthesia � sedation
Signed .......................................................................................... Date ..........................................................................
Name (PRINT................................................................................Job title ......................................................................
Write patient details or affixIdentification label
Hospital Number:Name:Address:
Date of Birth:NHS Number:
FOR
INFO
RMAT
ION
PU
RPO
SES
ON
LY

Use black biro to complete form.
File in Section 3
Patient agreement to investigation or treatment(Designed in compliance with the Department of Health consent form 1)
CONSENT FORM 1Responsible health professional ....................................................
Job title ............................................................................................Special requirements: ........................................(eg other language/other communication method)
All patients about to undergo any elective or emergency surgical or endoscopic procedure likely to involve contact with tissuesof medium or low level infectivity should be asked the question:-‘’Have you ever been notified that you are at increased risk of Creutzfeldt-Jakob disease (CJD) or variant Creutzfeldt-Jakobdisease (vCJD) for public health purposes?’’ If the patient’s response is No, proceed using normal infection prevention measures. If the answer is Yes, please ask the patient to explain further and consult the Infection Prevention Team for advice. If the procedure is likely to involve contact with tissues of potentially high level infectivity (Brain, spinal cord, implanted duramater grafts prior to 1992, cranial nerves and ganglia, pituitary gland and posterior eye (specifically: posterior hyaloid face,retina, retinal pigment epithelium, choroid, sub retinal fluid and optic nerve) the following questions should be asked:-1. Have you a history of CJD or other prion disease in your family? 2. Have you ever received growth hormone or gonadotrophin treatment? 3. Have you ever had surgery on your brain or spinal cord? If the answer to any of these questions is Yes, please discuss with the consultant in charge of the case and consult the InfectionPrevention Team for advice.
Approved by the Health Records Committee 00/00/2014 VS335 (R2)
Contact Details (if patient wishes to discuss optionslater)
Statement of interpreter (where appropriate)
I have interpreted the information above to the patient tothe best of my ability and in a way in which I believe s/hecan understand.
Signed ....................................................................................
Date........................................................................................
Name (PRINT) ........................................................................
Statement of patientPlease read this form carefully. If your treatment has been planned in advance, you should already haveyour own copy of page 1 which describes the benefits and risks of the proposed treatment. If not, you willbe offered a copy now. If you have any further questions, do ask - we are here to help you. You have theright to change your mind at any time, including after you have signed this form.
I agree to the procedure or course of treatment described on this form.
I understand that you cannot give me a guarantee that a particular person will perform the procedure.The person will, however, have appropriate experience.
I understand that I will have the opportunity to discuss the details of anaesthesia with an anaesthetistbefore the procedure, unless the urgency of my situation prevents this. (This only applies to patientshaving general or regional anaesthesia).
I understand that any procedure in addition to those described on this form will only be carried out if it isnecessary to save my life or to prevent serious harm to my health.
I have been told about additional procedures which may become necessary during my treatment. I havelisted below any procedures which I do not wish to be carried out without further discussion.
................................................................................................................................................................................
................................................................................................................................................................................
................................................................................................................................................................................
Patient’s signature ...................................................................... Date ..................................................................
Name (PRINT) ..........................................................................................................................................................
A witness should sign below if the patient is unable to sign but has indicated his or her consent. Young people/children may also like a parent to sign here (see notes).
Signed .......................................................................................... Date ..................................................................
Name (PRINT) ..........................................................................................................................................................
Confirmation of consent (to be completed by a health professional when the patient is admitted forthe procedure, if the patient has signed the form in advance).
On behalf of the team treating the patient, I have confirmed with the patient that s/he has no furtherquestions and wishes the procedure to go ahead.
Right eye Name/signature................................................................ date ................................................
Left eye Name/signature................................................................ date ................................................
Important notes: (tick if applicable)� See also advance directive/living will (eg Jehovah’s Witness form)
� Patient has withdrawn consent (ask patient to sign/date here ....................................................................
Bottom copy accepted by patient: yes / no (please ring) Patients Notes
Name of proposed procedure or course of treatment: Right eye / left eyeCataract extraction and intraocular lens insertion including photography/video for teachingand publicationStatement of health professional (to be filled in by health professional with appropriate knowledge ofproposed procedure, as specified in consent policy)
I have explained the procedure to the patient. In particular, I have explained:The aim of the cataract operation is to improve the quality of your vision. Surgery may also improve the doctors'view of the back of the eye. We will try to reduce your dependence on spectacles as much as possible, but youmay require distance glasses for best vision and will probably need reading glasses. Your glasses prescription willchange after the operation.
Serious or frequently occurring risksIt is possible for cataract surgery to leave you worse off than you are now. One person in every 1000 will go blindin that eye as a direct result of the operation. One in 10,000 will lose the eye. There is virtually no risk to theother eye. Details on the most common specific complications are given below.Ecchymosis - Bruising of eye or eyelids (quite common).Posterior capsule rupture and / or vitreous loss - a split in the thin back wall of the cataract which can allowcommunication between front and back compartments of the eye.Post operative glaucoma - raised pressure in the eye for the first day or so (common). This may require treatment.Posterior capsular opacification - clouding of the membrane behind the implant causing blurred vision.Cystoid macular oedema - inflammatory fluid in the centre of the retina. This is commonly mild and needs notreatment. It can be severe and require prolonged treatment.Refractive surprise - unexpectedly large (or different from expected) need for glasses.Allergy - to drops given after the operation, causing an itchy swollen eye until the drops are stopped or changed.Dropped nucleus - part or all of the cataract falls into the back part of the eye, needing another operation toremove it.Corneal decompensation - clouding of the normally clear front window of the eye.Detached retina - peeling off of the seeing layer of cells within the eye.Endophthalmitis - severe (usually painful) infection inside the eye.Dislocation of the implant - movement out of position of the lens implant.Complications are rare and in most cases can be treated effectively. In a small proportion of cases, a furtheroperation may be required. If you decide against a cataract operation, your vision will probably slowly worsen.
Individual additional risks - (e.g. deterioration of diabetic retinopathy, corneal oedema, unexpected refractiveoutcome particularly post laser patients)
Extra procedures that may be necessary during the procedure - Vitrectomy
..........................................................................................................................................................................................
..........................................................................................................................................................................................� The following leaflet/tape has been provided: Cataract Surgery information leafletThis procedure will involve: � general and/or regional anaesthesia � local anaesthesia � sedation
Signed .......................................................................................... Date ..........................................................................
Name (PRINT................................................................................Job title ......................................................................
Write patient details or affixIdentification label
Hospital Number:Name:Address:
Date of Birth:NHS Number:
FOR
INFO
RMAT
ION
PU
RPO
SES
ON
LY

Page 11
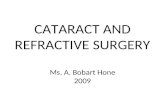
Directions to the Ophthalmic Surgical Unit (OSU)How to get here
The hospital is adjacent to Blackpool Zoo. From the A583 Preston New Road turn onto South Park Drive, which becomes East Park Drive.
For the Southern entrance to the Hospital, turn right at the set of traffic lights after the entrance to the Zoo.
For the Northern entrance, carry on to Four Lane Ends roundabout. Take the fourth exit and turn right into Whinney Heys Road.
Hospital policySmoking- the Trust operates a no smoking policy and your cooperation with this is appreciated
Health and Safety- our patients may have poor vision, please consider their safety by cooperating with the following:-
• Try not to obstruct the corridor.
• To reduce the risk of injury to you and other patients, please avoid assisting others.
Facilities available on the unit• Music via CD player or radio in the postoperative area.
• Telephone for making out going calls.
• Chilled water fountain.
SpeechTherapy
Home
Restaurant(1st Floor)
DROP OFF & SHORT STAYPOINT
EducationCentre
Breast CareCentre
Women andChildren’s Unit
Urgent CareCentre Entrance
7
Surgical Centre
Whinpark 1Car Park
Whinpark 2Car Park
OccupationalHealth
MAIN ENTRANCECAR PARK
Exit
Entrance
Staff Parking Only
Drop Off Point 2Disabled Parking
Drop Off Point 3
Disabled &
Staff Parking Only
Drop OffPoint 5
Disabled &Staff Parking
Only
Drop Off Point 4Disabled Parking
Suggested Car Parkfor Main Outpatients
appointments subject to availability – alternative Main Entrance Car Park
Drop Off Point 1
MainEntrance
Drop Off Point 3Disabled &
Staff Parking Only
Motorcycle
RING ROAD
CYCLEPARKING
Staff Parking, Car Sharers
and On Call Only
Department Area FloorA&E Entrance 3 GAccident & Emergency (A&E) 3 GAccounts Office 1 GAcute Medical Unit 3 1stAdolescent Ward 8 1stAmbulance Liaison Office 1 GBereavement Office 2 GBirth Centre 8 GBlue Skies Shop 1 GBreast Care Centre 2 GCaféteria 12 G
Caféteria 1 GCardiac Reception 12 GCardiac ITU 12 2ndCardiac Investigation Unit 12 GCardiology Day Ward 12 GCar Parking Office 16 GChapel 3 GChildren’s Assessment 8 1stChildren’s Wards 8 1stCombined Assessment and Treatment Unit (CAT) 3 1stCoronary Care Unit 12 1stDiabetic Resource Centre 4 GDietetics & Nutrition 4 GEducation Centre 14 GEntrance East Park Drive 2 GGastroenterology 6 GHaematology & Oncology Day Unit 5 GHome 15Intensive Therapy Unit 3 GInformation Desk 5 GLancashire suite 12 1stMain Entrance 16 GMain Entrance Outpatients 1 GMcMillan Windmill Unit 8 1stMedical Retina Unit 5 GMedical Photography 5 GMortuary 2 GNeonatal Unit 8 1stOccupational Health 13 GOccupational Therapy 1 GOphthalmic Surgical Unit 5 GOrthotic Department 1 GPathology 2 GPharmacy 5 GPhysiotherapy 1 GPrimary Care Dept 3 G
Department Area FloorReception A 1 GReception B 1 GReception - Blue 4 1stReception - Cardiac 12 GReception - Women & Children’s 8 GResearch & Development 5 2ndRestaurant 5 1stRetail Units 16 GSecurity Office 1 GSimulation & Skills Centre 2 2ndSpeech Therapy 14 GSurgical Appliances 1 GSurgical Centre 7 GSurgical Rapid Access Unit (SRAC) 3 1stTrust Headquarters 16 2ndUrgent Care Centre 3 GUrology 7 GVictoria Centre 8 GWard C 8 2ndWard D 8 3rdWard E (Haem Ward) 8 4thWard 1 (HDU) 4 GWard 2 4 1stWard 3 4 2ndWards 5 & 7 5 1stWard 6 5 1stWard 8 5 2ndWard 10 5 GWard 11 5 1stWard 12 5 2ndWard 14 (Surgical Centre) 7 1stWard 15 (Surgical Centre) 7 1stWard 16 (Surgical Centre) 7 1stWard 18 3 1stWard 19 3 1stWard 23 3 2ndWard 24 3 2ndWard 25 3 2ndWard 26 3 2ndWard 32 (Stroke) 11 GWard 33 (Stroke) 11 GWard 34 (Orthopaedic) 11 1stWard 35 (Orthopaedic) 11 1stWard 37 12 1stWard 38 12 1stWard 39 12 1stX-Ray Central 4 GX-Ray North 3 G
Information correct at the time of printing

Patient Relations DepartmentThe Patient Relations Department offer impartial advice and deal with any concerns or complaints the Trust receives. You can contact them via:
Tel: 01253 955589 email: [email protected]
You can also write to us at: Patient Relations Department, Blackpool Victoria Hospital, Whinney Heys Road, Blackpool FY3 8NR
Further information is available on our website: www.bfwh.nhs.uk
ReferencesThis leaflet is evidence based wherever the appropriate evidence is available, and represents an accumulation of expert opinion and professional interpretation.
Details of the references used in writing this leaflet are available on request from: Procedural Document and Leaflet Coordinator 01253 953397
Useful contact details
Hospital Switchboard: 01253 300000
Monday-Friday, 9am-5pm 01253 957420
Out of hours and weekends - Ward 15A Tel. 01253 953415. For all ophthalmic queries, help and advice.
People Centred Positive
ExcellenceCompassion
Our Four Values:
Blackpool Teaching Hospitals
NHS Foundation Trust
Author: Approved by:
Date of Publication:Reference No: Review Date:
Mr Rahman Opthalmic Directorate
26/08/2016BFWH143 - PL/502 v3 01/08/2019
Options available If you’d like a large print, audio, Braille or a translated version of this booklet then please call: 01253 955588