Anaesthesia for Cataract Surgery
19
Anaesthesia for Cataract Surgery Emmanuel Nouvellon, 1 Philippe Cuvillon, 1 Jacques Ripart 1,2 and Eric J. Viel 1 1 Anaesthesia Service and Pain Clinic, University Hospital Caremeau, Nı ˆmes, France 2 Montpellier-Nı ˆmes Medical School, Montpellier I University, Montpellier, France Contents Abstract .................................................................................. 21 1. Anaesthesia in the Elderly Patient: Specific Considerations .................................... 22 1.1 Concomitant Diseases ............................................................... 23 1.2 Continuation of Usual Treatment or Not? ............................................... 23 2. Requests from the Surgeon ............................................................... 24 3. Anatomical Considerations .............................................................. 24 4. Regional Anaesthesia (RA): Conventional Blocks ............................................ 25 4.1 Complications of Needle Blocks ....................................................... 25 4.2 Retrobulbar Anaesthesia (RBA) ....................................................... 26 4.3 Peribulbar Anaesthesia (PBA) ......................................................... 26 4.4 RBA versus PBA Controversy .......................................................... 28 5. Recent RA Techniques ................................................................... 28 5.1 Topical Anaesthesia ................................................................. 28 5.2 Perilimbal (Subconjunctival) Anaesthesia ............................................... 29 5.3 Sub-Tenon’s Block ................................................................... 29 5.3.1 Needle Technique ............................................................. 30 5.3.2 Surgical Approach with a Blunt Cannula .......................................... 30 5.4 Local Anaesthetics and Adjuvant Agents for Eye Blocks .................................. 31 5.5 Controversy: Who Should Perform the Block? ........................................... 32 5.6 Supporting Therapies ................................................................ 32 6. Controversy: General Anaesthesia versus RA................................................ 33 7. Future of Cataract Anaesthesia........................................................... 34 8. Conclusion ............................................................................ 34 Abstract Cataract surgery is the most frequent surgical procedure requiring anaes- thesia in developed countries. It is performed mainly in elderly patients, who present with many coexisting diseases that induce subsequent hazards from general anaesthesia. Cataract anaesthesia is performed following various techniques of regional anaesthesia, which are detailed in this review. Needle block carries a low but real risk of complications, mainly because of needle misplacement. Correct teaching and training are mandatory to prevent complications. The main patient risk factor for inadvertent globe perforation is the presence of a myopic staphyloma. Retrobulbar block has been pro- gressively phased out and replaced by peribulbar block, sub-Tenon’s block (STB) or topical anaesthesia (TA). The requirement for very deep block with total akinesia has greatly decreased with the use of phacoemulsification for cataract surgery, allowing for use of TA or low-volume STB. However, REVIEW ARTICLE Drugs Aging 2010; 27 (1): 21-38 1170-229X/10/0001-0021/$49.95/0 ª 2010 Adis Data Information BV. All rights reserved.
-
Upload
rido-banar-ekaputra -
Category
Documents
-
view
136 -
download
6
Transcript of Anaesthesia for Cataract Surgery
Anaesthesia for Cataract SurgeryEmmanuel Nouvellon,1 Philippe Cuvillon,1 Jacques Ripart1,2 and Eric J. Viel1
1 Anaesthesia Service and Pain Clinic, University Hospital Caremeau, Nımes, France
2 Montpellier-Nımes Medical School, Montpellier I University, Montpellier, France
Contents
Abstract. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 211. Anaesthesia in the Elderly Patient: Specific Considerations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22
1.1 Concomitant Diseases. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 231.2 Continuation of Usual Treatment or Not? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23
2. Requests from the Surgeon . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 243. Anatomical Considerations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 244. Regional Anaesthesia (RA): Conventional Blocks . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25
4.1 Complications of Needle Blocks. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 254.2 Retrobulbar Anaesthesia (RBA) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 264.3 Peribulbar Anaesthesia (PBA) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 264.4 RBA versus PBA Controversy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28
5. Recent RA Techniques . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 285.1 Topical Anaesthesia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 285.2 Perilimbal (Subconjunctival) Anaesthesia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 295.3 Sub-Tenon’s Block . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29
5.3.1 Needle Technique . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 305.3.2 Surgical Approach with a Blunt Cannula . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30
5.4 Local Anaesthetics and Adjuvant Agents for Eye Blocks . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 315.5 Controversy: Who Should Perform the Block? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 325.6 Supporting Therapies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 32
6. Controversy: General Anaesthesia versus RA. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 337. Future of Cataract Anaesthesia. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 348. Conclusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 34
Abstract Cataract surgery is the most frequent surgical procedure requiring anaes-thesia in developed countries. It is performed mainly in elderly patients, whopresent with many coexisting diseases that induce subsequent hazards fromgeneral anaesthesia. Cataract anaesthesia is performed following varioustechniques of regional anaesthesia, which are detailed in this review. Needleblock carries a low but real risk of complications, mainly because of needlemisplacement. Correct teaching and training are mandatory to preventcomplications. The main patient risk factor for inadvertent globe perforationis the presence of a myopic staphyloma. Retrobulbar block has been pro-gressively phased out and replaced by peribulbar block, sub-Tenon’s block(STB) or topical anaesthesia (TA). The requirement for very deep block withtotal akinesia has greatly decreased with the use of phacoemulsificationfor cataract surgery, allowing for use of TA or low-volume STB. However,
REVIEW ARTICLEDrugs Aging 2010; 27 (1): 21-38
1170-229X/10/0001-0021/$49.95/0
ª 2010 Adis Data Information BV. All rights reserved.

non-akinesia techniques may give rise to impaired surgical conditions, whichhave the potential to result in surgical complications. A surgical approach toaccessing sub-Tenon’s space avoids needle block, but does not totally preventcomplications. When deep anaesthesia is required, low-volume STB, performedusing either the needle technique or a surgical approach, appears to be thetechnique of choice in terms of efficacy. Increasing the anaesthetic volumeprovides reproducible akinesia. Various local anaesthetics may be used, de-pending on their availability and respective properties. Themost useful adjuvantto local anaesthetic is hyaluronidase.
Ophthalmic surgery is the most frequent sur-gical procedure requiring anaesthesia in devel-oped countries. Each year, cataract surgery isperformed on more than 300 000 patients in theUK, about 500 000 patients in France and nearly2 million patients in the US.[1] The vast majorityof procedures are performed in a 1-day surgerysetting, under regional anaesthesia (RA), alsocalled ‘eye block’.[1-3]
Eye block has historically been limited to retro-bulbar anaesthesia (RBA) performed by the sur-geon alone with monitored anaesthesia care orwithout any anaesthesiologist’s assistance at all.Anaesthesiologists are now increasingly becom-ing involved in ophthalmic RA. As surgicalpractice evolves following widespread use of thephacoemulsification (PKE) technique, requestsfrom surgeons for total akinesia and loweredintraocular pressure (IOP) have decreased.[4] Atthe same time, the complications of conventionalRBA have been extensively described, and theneed for greater safety during eye block has beenemphasized. This has resulted in the developmentof alternative techniques such as peribulbar, low-volume sub-Tenon’s block (STB) and topicalanaesthesia (TA), the aim of which is to improvesafety, albeit at the price of imperfect akinesia.However, some surgeons still express a need fora more efficient block, providing total globeakinesia and anaesthesia of the globe, for somedifficult procedures and certain patients. A greaterknowledge of anatomy and of the various tech-niques will enable the anaesthesiologist to choosethe best technique to match each situation.
Whether anaesthesia influences patient out-comes has been the topic of many publications,and these cannot be extensively detailed here. The
controversy over the choice of anaesthesia tech-nique – i.e. general anaesthesia (GA) versus RA –
suffers from a lack of well designed comparativestudies. Moreover, non-ophthalmic complica-tions of cataract surgery are so rare that theoutcome does not significantly differ betweenthose patients who have been operated on andthose who have not.
This review briefly discusses anaesthesia in el-derly patients and the condition of the eye request-ed by the surgeon, but focuses particularly on RA,i.e. the relevant anatomy, classical (retrobulbar andperibulbar) needle block techniques together withtheir efficacies and complications, emerging tech-niques and their relative ‘pros’ and ‘cons’, choice oflocal anaesthetics and adjuvant agents and, finally,some ongoing controversies. In addition, the de-bate between GA and RA is developed.
Literature searches were conducted on MED-LINE and EMBASE from 2000 to 2009 using thefollowing keywords: cataract surgery, phako-emulsification, intraocular lens replacement, eyesurgery, anesthesia, regional anesthesia, generalanesthesia, and elderly patient. We also searched acumulative personal database based on monthly is-sues of the following journals published since 1994:Anesthesiology, Regional Anesthesia and Pain Medi-cine, Anesthesia & Analgesia, British Journal of An-aesthesia, Journal of Cataract & Refractive Surgery,Ophthalmology, American Journal of OphthalmicSurgery, Eye and Archives of Ophthalmology.
1. Anaesthesia in the Elderly Patient:Specific Considerations
The topic of anaesthesia in the elderly patient issufficiently large in itself as to require a separate
22 Nouvellon et al.
ª 2010 Adis Data Information BV. All rights reserved. Drugs Aging 2010; 27 (1)

review, which can be found elsewhere (e.g. Cohendyet al.[5]). This discussion is limited to the mostimportant points.
1.1 Concomitant Diseases
Cataract is mainly an elderly patient’s healthconcern. In a series of >55 000 cases, the medianpatient age was 75 years.[6]
As in all elderly patients, cataract patients mayhavemultiple concomitant diseases. Kelly observedthat up to 63% of cataract patients have a signifi-cant underlying disease.[7] Stupp et al. observed a97% rate of pre-existing risk factors for intra-operative adverse events requiring medical inter-vention in patients undergoing cataract surgery.[8]
The most frequently described co-morbidity is car-diovascular disease, but neurological or metabolicdiseases or conditions, including diabetes mellitusor chronic corticosteroid therapy, are also reported.In a prospective study, Sharwood et al. reported thefollowing incidences: hypertension (51%), gastro-oesophageal reflux (19%), angina and myocardialinfarction (14%), diabetes (13%) and asthma(9%).[9] Indeed, diabetes and corticosteroid therapyare classical causes of cataracts.
The elderly have also specific characteristicsthat may interfere with anaesthetic agents, parti-cularly GA, to produce exaggerated adverseeffects:
� Decreased drug elimination may lead to accu-mulation, relative overdosage and subsequentlydelayed recovery or prolonged residual effectwith mental dysfunction.
� Increased susceptibility to anaesthetic agentsmay lead to more pronounced drug effectsthan in healthy adults with the same dosage(e.g. deeper hypotension induced by GA ordelayed wakening).
� Effects of anaesthesia such as arterial hypo-tension may be less well tolerated in theelderly patient because of multiple under-lying diseases (e.g. myocardial or cerebralinfarction resulting from coronary or carotidstenosis).
� Polymedication may lead to significant druginteractions with anaesthetic agents, especiallyin patients given GA.
1.2 Continuation of Usual Treatment or Not?
As with any other surgical procedure, the goldenrule is not to change apatient’s usual treatment if heorshe is stable on it. This is especially true for antihyper-tensive agents, and moreover for b-adrenoceptorantagonists (b-blockers) in particular, because of therisk of a rebound effect.[10] Therefore, the patient’susual treatment should be given on the morning ofsurgery. Concerning insulin treatment of diabeticpatients, when the patient is fasted, two options arepossible: (i) as for any other surgery, because thepatient is fasting, the normal insulin dose is given asusual under the cover of an intravenous glucose in-fusion (glucose 50g/L, 1mL/g/h); or (ii) the morn-ing insulin dose is avoided. When the patient is notfasting, the usual insulin is continued.
The most debated problem is whether to con-tinue anticoagulants/antiplatelet therapy. On theone hand, continuing such treatments is frequentlythought to increase both the risk for surgicalbleeding and the risk of haematoma from eye blockpuncture. On the other hand, discontinuing thosetherapies may unacceptably increase the risk forthrombosis in at-risk patients, for example, thosewith atrial fibrillation, non-tissue prosthetic heartvalves, carotid stenosis or coronary drug-elutingstents. These risks include cerebral ischaemicstroke, myocardial infarction and death. In fact,cataract surgery is a totally ‘bloodless’ procedureand can be performed safely in patients taking anyanticoagulant/antiplatelet agents.[11] So these drugsshould generally be continued. When choosing theeye block, the option of TA must be taken intoaccount. All deep blocks (both needle block andcannula STB) carry a low risk for haematoma.Most of them are benign with only short-termaesthetic consequences (i.e. subconjunctival orpalpebral haematoma), the exception being theclassical but very infrequent compressive retro-bulbar haemorrhage.[12,13] However, it appears thatanticoagulants/antiplatelets do not significantly in-crease the risk of such a haemorrhage.[14] There-fore, discontinuation of anticoagulant/antiplatelettherapy for a deep block is no longer routinely re-commended. British guidelines state that, ‘‘the INR[international normalized ratio] should be withinthe therapeutic ratio which is determined by the
Anaesthesia for Cataract Surgery 23
ª 2010 Adis Data Information BV. All rights reserved. Drugs Aging 2010; 27 (1)
condition for which the patient is being anti-coagulated’’,[15] and French guidelines recommendcontinuation of aspirin (acetylsalicylic acid).[16]
Canadian practice appears to be similar.[17] Theonly drug for which there are no recommendationsis clopidogrel. In this case, a decision must be takenon an individual basis.
2. Requests from the Surgeon
Classically, for cataract surgery, as with anyother open globe surgery, the request from thesurgeon is for analgesia, akinesia and hypotonia ofthe eyeball. This remains true for the traditionalextracapsular cataract extraction (ECE) technique,which requires a large (6–8mm) incision to removethe entire lens. By contrast, with the development ofPKE, methods have radically changed.[4] This pro-cedure consists of fragmentation of the lens nucleuswith an ultrasound probe and evacuation of thefragments by an irrigation-aspiration system. Asmall incision (3–4mm) is sufficient to allow afoldable prosthetic lens to be introduced. Becausethe small incision is self-sealing, there is no need forany suture and the duration of the procedure is re-duced to as little as 3–5minutes in easy cases. As thesmall incision is obturated by the ultrasound probe,PKE can be considered a ‘closed eye’ procedure,meaning lowering the IOP is much less important.Akinesia is rarely if ever required, because theultrasound probe allows immobilization of the eye-ball. Finally, as the lens is free of any sensory in-nervation, only the corneal incision may be painful,and this only rarely. Indeed, PKE is possible forselected patients without any anaesthesia at all.[18]
The surgeon may also require that other generalconditions be prevented. Acute peak arterial hyper-tension, for instance, may cause catastrophicchoroidal expulsive haemorrhage. Tremor orrestlessness may impair the procedure, for ob-vious reasons. Coughing gives rise to very acuteand high peak IOP, which can impair surgery andtherefore must be prevented.
3. Anatomical Considerations
The orbit is a cavity in the shape of a truncatedsquare pyramid, with its apex posterior and its
base corresponding to the anterior aperture. Theorbit is filled mainly by adipose tissue, and theglobe is suspended in its anterior part. The fourrectus muscles of the eye are inserted anteriorlynear the equator of the globe. Posteriorly, theyare inserted together, at the apex, on the Zinntendinous annulus, through which the optic nerveenters the orbit. The four rectus muscles delimitthe retrobulbar cone, which is not sealed by anyintermuscular membrane.[19,20] Sensory innerva-tion of the globe is supplied by the ophthalmicnerve, the first branch of the trigeminal nerve(cranial nerve [CN] V), which passes through themuscular cone. The trochlear nerve (CN IV)provides the motor command to the superioroblique muscles, the abducens nerve (CN VI)does the same to the lateral rectus muscle, and theoculomotor nerve (CN III) provides motor sig-nals to all the other extraocular muscles. All thesenerves except the trochlear nerve pass throughthe muscular conus. Therefore, injecting localanaesthetic inside the cone can logically be ex-pected to provide anaesthesia and akinesia of theglobe and of the extraocular muscles. Only themotor command of the orbicularis muscle of theeyelids has an extraorbital course, arising as itdoes from the superior branch of the facial nerve(CN VII). Many major structures are located inthe muscular conus and are therefore vulnerableto the risk of needle injury; these include the opticnerve with its meningeal sheaths, most of the ar-teries of the orbit, and the autonomic, sensoryand motor innervation of the globe.
The facial sheath of the eyeball – also calledTenon’s capsule – is a fibroelastic layer that sur-rounds the entire scleral portion of the globe. Itdelimits the episcleral space or sub-Tenon’sspace, a potential space with no actual volume,although fluid can be injected into it. Some au-thors assimilate it into the articular capsule of theglobe. Near the equator, Tenon’s capsule is per-forated by the tendons of the oblique and rectusmuscles before they insert into the sclera. At thispoint there is a continuity between Tenon’s cap-sule and the fascial sheath of the muscles. Ante-riorly, Tenon’s capsule merges with the bulbarconjunctiva before both insert together into thecorneal limbus.
24 Nouvellon et al.
ª 2010 Adis Data Information BV. All rights reserved. Drugs Aging 2010; 27 (1)

4. Regional Anaesthesia (RA):Conventional Blocks
As all needle blocks can be used for cataractsurgery, the choice of needle is largely based onefforts to prevent complications.
4.1 Complications of Needle Blocks
The most common cause of needle blockcomplications is needle misplacement. Althoughsome anatomical features may increase the risk ofcomplications, the main risk factor is poortraining and limited experience of the physicianperforming the block.
Spread of anaesthesia in the CNS may involvetwo mechanisms. Firstly, an inadvertent intra-arterial injection may reverse blood flow in theophthalmic artery up to the anterior cerebralor the internal carotid artery,[21] such that aninjected volume as small as 4mL can produceseizures. In such cases, symptomatic treatment(oxygen supply, injected antiepileptic drugs suchas thiopental sodium or benzodiazepine, facemask ventilation, and, if required, tracheal in-tubation for mechanical ventilation with musclerelaxants) usually allows rapid recovery withoutafter-effects. Secondly, an inadvertent injectionunder the dura mater sheath of the optic nerve ordirectly through the optic foramen may result insubarachnoid spread of the local anaesthetic.This causes partial or total, progressive, brain-stem anaesthesia.[22,23] Katsev et al. have de-monstrated that the apex of the orbit may bereached with a 40mm long needle.[24] Dependingon the dose and volume of local anaestheticspreading towards the brainstem, possibilitiesinclude bilateral block, CN palsy with sympa-thetic activation, confusion and restlessness, ortotal spinal anaesthesia with tetraparesis, arterialhypotension, bradycardia and eventually respi-ratory and cardiac arrest. Symptomatic treatment(oxygen supply, vasopressors, and, if required,tracheal intubation and ventilation) should resultin total recovery within hours.
Inadvertent globe perforation and rupture isthe most devastating complication of eye blocks.The complication has a poor prognosis, particu-
larly in cases of delayed diagnosis. The incidenceis between 1/350 and 7/50 000 cases.[25,26] Riskfactors are classically inexperience of the physi-cian and a highly myopic eye (i.e. long eyeball).[26]
In a series of 50 000 cases, Edge and Navon ob-served that myopic staphyloma was the greatestrisk factor for scleral perforation.[25] This sug-gests that isolated high myopia may not be a riskfactor per se, but acts as a confounding factor, asmyopic staphyloma occurs only in myopic eyes.Using ultrasound imaging, Vohra and Goodobserved that the probability of staphyloma isgreater in highly myopic than slightly myopiceyes.[27] Moreover, staphyloma is more fre-quently located at the posterior pole of the globe(accounting for perforations after RBA) or in theinferior area of the globe (accounting for per-forations after inferior and temporal punctures,both peri- or retrobulbar). As a result, at least inmyopic patients and ideally in all patients, ultra-sound measurement of the axial length of theglobe (biometry) should be performed. A highlymyopic eye (axial length >26mm) remains theclassical contraindication to eye block. However,this contraindication may be circumvented ifB-mode ultrasound is conducted to assess thepresence and location of a staphyloma.
Injury to an extraocular muscle may causediplopia and ptosis. Several mechanisms can beinvolved: direct injury by the needle resulting inintramuscular haematoma, high pressure due toinjection into the muscle sheath, or myotoxicityof the local anaesthetic.[28] The injury may pro-gress in three steps: initially the muscle is para-lysed, then it appears to recover, and finally, aretractile scar develops.
Retrobulbar haemorrhage results from an in-advertent arterial puncture. This complicationmay lead to a compressive haematoma, whichcan threaten retinal perfusion. Surgical decom-pression may be required, but, in most cases,all that is needed is postponement of surgery.[12]
The main risk factor is arterial fragility (diabetesand atheroma), rather than clotting disorders.Venous puncture leads to noncompressive hae-matoma, the consequences of which are muchless severe, so that, in most cases, surgery can becontinued.
Anaesthesia for Cataract Surgery 25
ª 2010 Adis Data Information BV. All rights reserved. Drugs Aging 2010; 27 (1)
Direct optic nerve trauma by the needle is veryrare but causes blindness. CT scan imaging usual-ly shows optic nerve enlargement due to intra-neural haematoma.[29]
4.2 Retrobulbar Anaesthesia (RBA)
Historically, RBA has been the gold standardof eye block and is achieved by injecting a smallvolume of local anaesthetic agent (3–5mL) insidethe muscular cone.[30] The main hazard of RBA isthe risk of injury to the globe or one of the manyvulnerable elements located in the muscular cone.Near the apex, these structures are packed in avery small volume and are fixed by the tendon ofZinn, which prevents them from moving awayfrom the needle. The resulting potential compli-cations are detailed in section 4.1. To preventsuch complications, some authors have proposedavoiding introduction of a needle into the mus-cular cone, and prefer to keep the needle in theextraconal space, a technique that is theoreticallyless hazardous.[31,32]
Although used from the beginning of the twen-tieth century, RBA was formally described only in1936.[30] An additional facial nerve block is re-quired to prevent blinking, with the technique thatis most frequently used being the van Lindt eyelidblock.[33] The Atkinson ‘up and in’ position of thegaze was abandoned after Liu et al.[34] and Unsoldet al.[35] confirmed that this increases the risk ofoptic nerve injury. RBA is used less frequentlynowadays because of its complications.
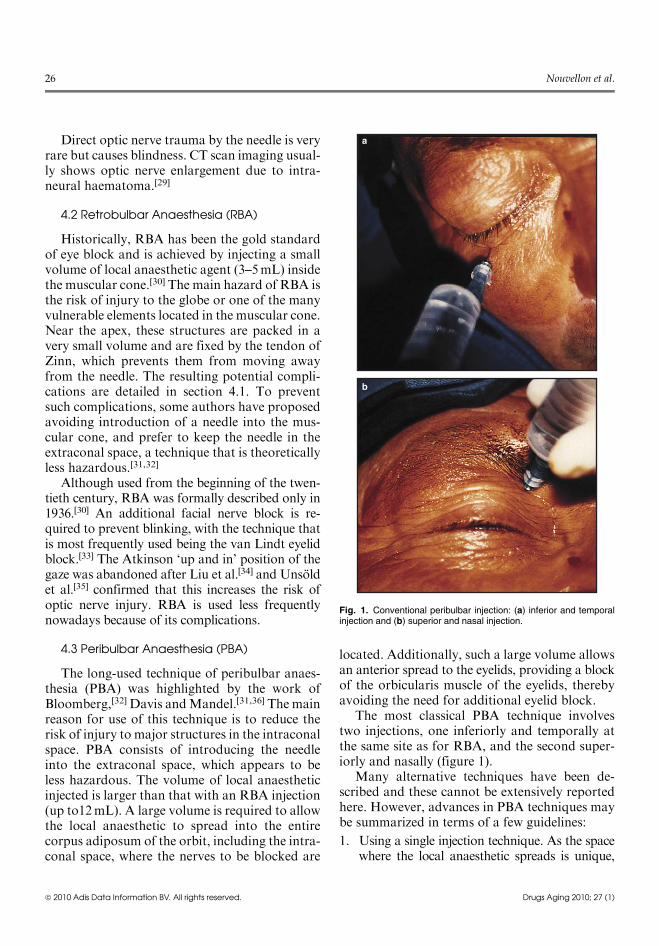
4.3 Peribulbar Anaesthesia (PBA)
The long-used technique of peribulbar anaes-thesia (PBA) was highlighted by the work ofBloomberg,[32] Davis andMandel.[31,36] The mainreason for use of this technique is to reduce therisk of injury to major structures in the intraconalspace. PBA consists of introducing the needleinto the extraconal space, which appears to beless hazardous. The volume of local anaestheticinjected is larger than that with an RBA injection(up to12mL). A large volume is required to allowthe local anaesthetic to spread into the entirecorpus adiposum of the orbit, including the intra-conal space, where the nerves to be blocked are
located. Additionally, such a large volume allowsan anterior spread to the eyelids, providing a blockof the orbicularis muscle of the eyelids, therebyavoiding the need for additional eyelid block.
The most classical PBA technique involvestwo injections, one inferiorly and temporally atthe same site as for RBA, and the second super-iorly and nasally (figure 1).
Many alternative techniques have been de-scribed and these cannot be extensively reportedhere. However, advances in PBA techniques maybe summarized in terms of a few guidelines:
1. Using a single injection technique. As the spacewhere the local anaesthetic spreads is unique,
a
b
Fig. 1. Conventional peribulbar injection: (a) inferior and temporalinjection and (b) superior and nasal injection.
26 Nouvellon et al.
ª 2010 Adis Data Information BV. All rights reserved. Drugs Aging 2010; 27 (1)
increasing the injected volume is sufficient toprovide efficient anaesthesia. Comparative stud-ies have confirmed that, provided the injectedvolume is sufficient, the single injection tech-nique is as effective as the double injection tech-nique.[37] Moreover, as the first injection mayimpair identification of anatomical landmarks,it has been suggested that the second injectionmay lead to complications more frequentlythan the first.[38] A second injection should beperformed only as a supplement when the firstinjection has failed.
2. Limiting the depth of needle insertion (usually25mm). Posteriorly to the globe, the rectusmuscles are in contact with the orbital walls,so that the extraconal space totally disappearsand becomes virtual. Increasing the depth ofneedle insertion is expected to change a peri-bulbar into a retrobulbar injection.[39] Some‘posterior PBAs’ are in fact inadvertent retro-bulbar injections. This fact probably explainsthe occurrence of complications such as opticnerve injury after an attempted peribulbarinjection. Moreover, a long needle introducedtotally into the orbit may reach the apex of theorbit, a hazardous zone.[40] In an anatomicalstudy, Katsev et al. demonstrated that insert-ing the needle up to a 40mm depth will resultin an injection directly through the opticalforamen in 11% of cases.[24] More recently,limiting the needle insertion to a 15mm depthwas proposed; this has a similar efficacy to a25mm depth.[41]
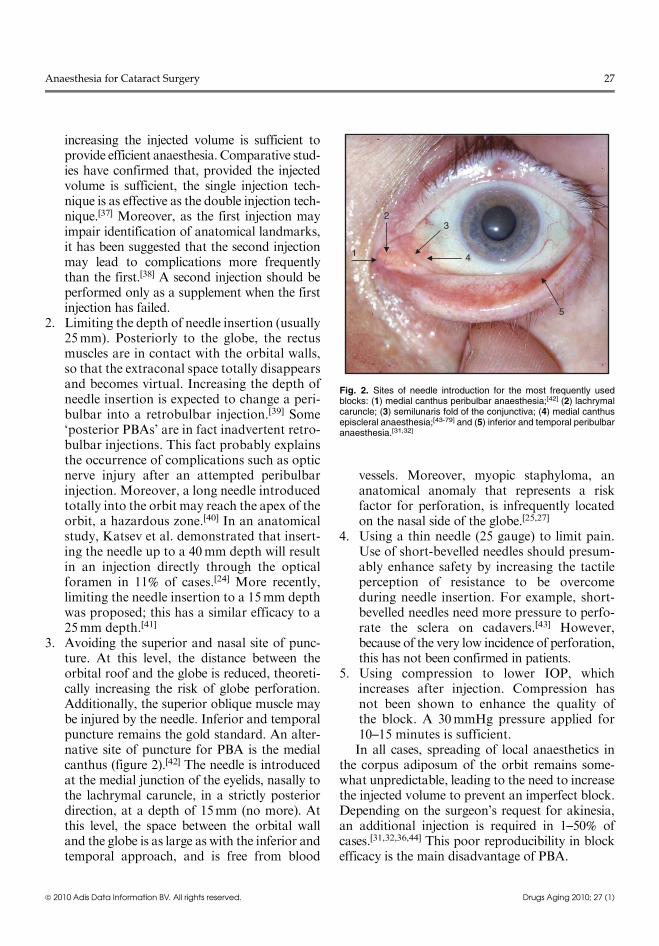
3. Avoiding the superior and nasal site of punc-ture. At this level, the distance between theorbital roof and the globe is reduced, theoreti-cally increasing the risk of globe perforation.Additionally, the superior oblique muscle maybe injured by the needle. Inferior and temporalpuncture remains the gold standard. An alter-native site of puncture for PBA is the medialcanthus (figure 2).[42] The needle is introducedat the medial junction of the eyelids, nasally tothe lachrymal caruncle, in a strictly posteriordirection, at a depth of 15mm (no more). Atthis level, the space between the orbital walland the globe is as large as with the inferior andtemporal approach, and is free from blood
vessels. Moreover, myopic staphyloma, ananatomical anomaly that represents a riskfactor for perforation, is infrequently locatedon the nasal side of the globe.[25,27]
4. Using a thin needle (25 gauge) to limit pain.Use of short-bevelled needles should presum-ably enhance safety by increasing the tactileperception of resistance to be overcomeduring needle insertion. For example, short-bevelled needles need more pressure to perfo-rate the sclera on cadavers.[43] However,because of the very low incidence of perforation,this has not been confirmed in patients.
5. Using compression to lower IOP, whichincreases after injection. Compression hasnot been shown to enhance the quality ofthe block. A 30mmHg pressure applied for10–15 minutes is sufficient.In all cases, spreading of local anaesthetics in
the corpus adiposum of the orbit remains some-what unpredictable, leading to the need to increasethe injected volume to prevent an imperfect block.Depending on the surgeon’s request for akinesia,an additional injection is required in 1–50% ofcases.[31,32,36,44] This poor reproducibility in blockefficacy is the main disadvantage of PBA.
1
23
4
5
Fig. 2. Sites of needle introduction for the most frequently usedblocks: (1) medial canthus peribulbar anaesthesia;[42] (2) lachrymalcaruncle; (3) semilunaris fold of the conjunctiva; (4) medial canthusepiscleral anaesthesia;[43-79] and (5) inferior and temporal peribulbaranaesthesia.[31,32]
Anaesthesia for Cataract Surgery 27
ª 2010 Adis Data Information BV. All rights reserved. Drugs Aging 2010; 27 (1)
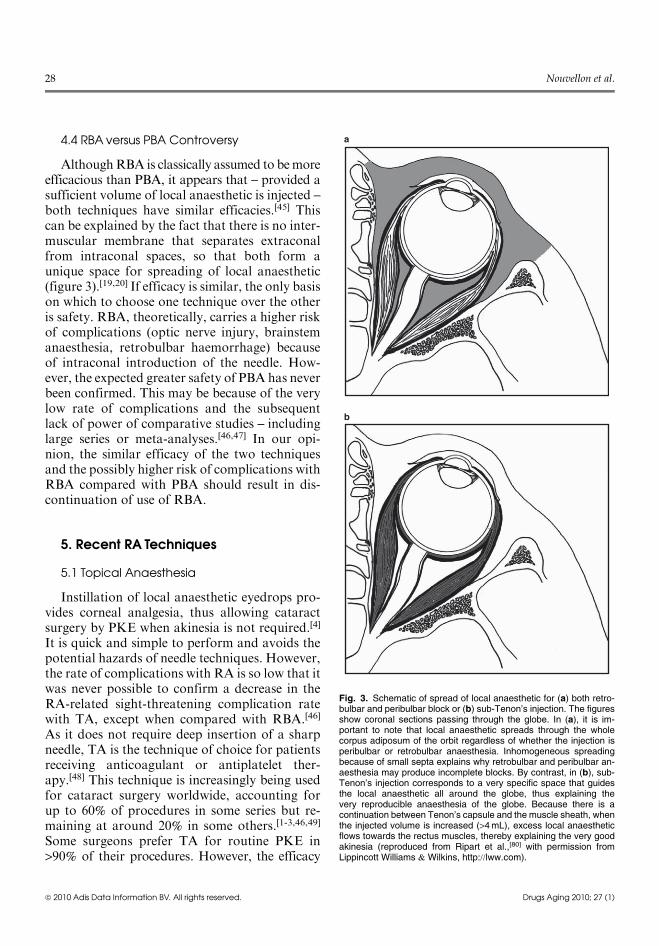
4.4 RBA versus PBA Controversy
AlthoughRBA is classically assumed to bemoreefficacious than PBA, it appears that – provided asufficient volume of local anaesthetic is injected –
both techniques have similar efficacies.[45] Thiscan be explained by the fact that there is no inter-muscular membrane that separates extraconalfrom intraconal spaces, so that both form aunique space for spreading of local anaesthetic(figure 3).[19,20] If efficacy is similar, the only basison which to choose one technique over the otheris safety. RBA, theoretically, carries a higher riskof complications (optic nerve injury, brainstemanaesthesia, retrobulbar haemorrhage) becauseof intraconal introduction of the needle. How-ever, the expected greater safety of PBA has neverbeen confirmed. This may be because of the verylow rate of complications and the subsequentlack of power of comparative studies – includinglarge series or meta-analyses.[46,47] In our opi-nion, the similar efficacy of the two techniquesand the possibly higher risk of complications withRBA compared with PBA should result in dis-continuation of use of RBA.
5. Recent RA Techniques
5.1 Topical Anaesthesia
Instillation of local anaesthetic eyedrops pro-vides corneal analgesia, thus allowing cataractsurgery by PKE when akinesia is not required.[4]
It is quick and simple to perform and avoids thepotential hazards of needle techniques. However,the rate of complications with RA is so low that itwas never possible to confirm a decrease in theRA-related sight-threatening complication ratewith TA, except when compared with RBA.[46]
As it does not require deep insertion of a sharpneedle, TA is the technique of choice for patientsreceiving anticoagulant or antiplatelet ther-apy.[48] This technique is increasingly being usedfor cataract surgery worldwide, accounting forup to 60% of procedures in some series but re-maining at around 20% in some others.[1-3,46,49]
Some surgeons prefer TA for routine PKE in>90% of their procedures. However, the efficacy
a
b
Fig. 3. Schematic of spread of local anaesthetic for (a) both retro-bulbar and peribulbar block or (b) sub-Tenon’s injection. The figuresshow coronal sections passing through the globe. In (a), it is im-portant to note that local anaesthetic spreads through the wholecorpus adiposum of the orbit regardless of whether the injection isperibulbar or retrobulbar anaesthesia. Inhomogeneous spreadingbecause of small septa explains why retrobulbar and peribulbar an-aesthesia may produce incomplete blocks. By contrast, in (b), sub-Tenon’s injection corresponds to a very specific space that guidesthe local anaesthetic all around the globe, thus explaining thevery reproducible anaesthesia of the globe. Because there is acontinuation between Tenon’s capsule and the muscle sheath, whenthe injected volume is increased (>4 mL), excess local anaestheticflows towards the rectus muscles, thereby explaining the very goodakinesia (reproduced from Ripart et al.,[80] with permission fromLippincott Williams & Wilkins, http://lww.com).
28 Nouvellon et al.
ª 2010 Adis Data Information BV. All rights reserved. Drugs Aging 2010; 27 (1)

of TA is limited. Firstly, analgesia may be in-complete. Patients randomly subjected to RBAor TA for one eye and the other technique forthe other eye preferred RBA (71% vs 10%).[50]
Intraoperative comfort is more consistentlyobtained with RBA[50-52] or sub-Tenon’s[53,81]
than with TA, which appears to be no more ef-fective than no anaesthesia at all in selected casesinvolving an experienced surgeon.[18] Secondly,the lack of akinesia and IOP control associatedwith the short duration of the procedure maytheoretically make surgery more hazardous.[52,54]
Only one study has observed an advantage for TAin terms of the surgical complication rate. In arandomized, non-blind, comparative study ofunselected patients, Jacobi et al. observed onlyone significant difference between TA and RBA,namely, a surprising decrease in vitreous issuerate in the TA group (0.4% vs 2.5%).[55] At thesame time, the investigators observed a non-significant increase in iris prolapse (1.7% vs0.4%), possibly reflecting eye hypertonia due tothe lack of akinesia in the TA group. In a 2382-case survey, Shaw et al. observed an acceptablylow rate of surgical complications of cataractsurgery performed under TA.[56] By contrast, amore recent meta-analysis has shown that, whencompared with STB, TA is associated with a2-fold increase in posterior capsule rupturerequiring anterior vitrectomy.[54] Similarly, TAwas identified as a risk factor for displacement ofnuclear fragments into the vitreous.[57] Therefore,TA should be limited to planned easy proceduresperformed by experienced surgeons in selectedpatients. For manual ECE, akinesia is still re-quired and TA is questionable.[4] This may be thecase in institutions where PKE is not available fortechnical reasons.[58,59]
Efforts have been made to improve TA effi-cacy in many ways. Use of long-acting local an-aesthetics such as levobupivacaine or ropivacaineappears more efficacious than lidocaine (ligno-caine).[60,61] Intracameral injection of localanaesthetic has been proposed to enhance an-algesia.[62] This entails injecting small volumes(0.1mL) of local anaesthetic in the anteriorchamber at the beginning of surgery. The safetyof this technique in relation to local anaesthetic
toxicity to corneal endothelium, which is not ableto regenerate, has been confirmed,[63,64] but anysignificant analgesic benefit of intracameral in-jection versus simple TA has never been estab-lished by properly designed trials.[18,64-68] This isnot surprising, as analgesia is not correlated withintracameral local anaesthetic concentration.[69]
For these reasons, intracameral injection cannotbe recommended. The efficacy of sponges soakedwith local anaesthetic inserted into the con-junctival fornices and soluble local anaestheticinserts needs further documentation.[70,71] Instil-ling lidocaine jelly instead of eyedrops appearsto clearly enhance the quality of analgesia ofthe anterior segment,[53,69,72] and is being in-creasingly used. However, lidocaine jelly hasbeen associated with an increase in postoperativeincidence of endophthalmitis, as described bythe French sanitary agency in 2004.[73] This mightexplain why TA has been associated with a3.8-fold increase in endophthalmitis rate com-pared with RBA.[74] The most plausible explana-tion for these cases is that if the jelly was appliedfirst on the eye, it would have acted as a barrier,preventing disinfectant applied later from reach-ing the conjunctiva, thereby resulting in insufficienteye disinfection. Thus, the problem is probablythe wrong sequence of application rather thanthe jelly itself. Specifically designed topical lido-caine or tetracaine jellies should replace currentjellies, which were originally designed for use inurology.[75,76]
5.2 Perilimbal (Subconjunctival) Anaesthesia
Subconjunctival injection of local anaestheticmay provide analgesia of the anterior segmentwithout any akinesia,[77] but has not gained widepopularity.
5.3 Sub-Tenon’s Block
Also called episcleral or parabulbar anaesthesia,STB is achieved by injecting into the episcleralspace. This allows the local anaesthetic to spreadcircularly around the scleral portion of theglobe, thereby achieving high-quality analgesiaof the whole globe with injection of relatively
Anaesthesia for Cataract Surgery 29
ª 2010 Adis Data Information BV. All rights reserved. Drugs Aging 2010; 27 (1)
low volumes (usually 3–5mL) [figure 3].[78,79] Inaddition, use of a larger volume (up to 8–11mL)means the local anaesthetic will spread to theextraocular muscle sheaths, producing an effectiveand reproducible akinesia (figure 3).[44,78,79,82,83]
Chemosis (subconjunctival spread of the local an-aesthetic) occurs frequently after injection of suchlarge volumes[81,83,84] and is easily explained byanatomical features. Its occurrence confirms thesub-Tenon’s location of the injection and mayrequire compression to be resolved.
Sub-Tenon’s space may be injected usingeither a needle technique or surgical dissectionfollowed by introduction of a blunt cannula.
5.3.1 Needle Technique
In the needle technique,[44,78,79,83] the needle isintroduced into the fornix between the semilunarisfold of the conjunctiva and the globe, tangentiallyto the globe (figure 2). After it has encroached onthe conjunctiva, the needle is slightly shiftedmedially and advanced strictly posteriorly, therebypulling on the globe, which results in directing thegaze medially. At a 10–15mm depth, after a smallloss of resistance (‘click’) is perceived, the globereturns to its primary gaze position. This serves asa depth marker, thus allowing injection.
Using a large volume (5–10mL) with this tech-nique results in good globe and lid akinesia, andthe results are more reproducible than with clas-sical PBA.[44] This technique is simple to learnand perform, with acceptable safety of use. In ourexperience of 2000 cases, we encountered no ser-ious complications.[83] However, as with all nee-dle techniques, the risk of misplacement of theneedle and its subsequent complications must bekept in mind. This technique has not been widelyused outside France.
A variant technique using only forceps and a‘pencil-point’ needle instead of scissors and can-nula was recently proposed by Allman et al.[85]
This technique might be considered as a blend ofneedle and cannula techniques. It remains to beassessed on a large scale.
5.3.2 Surgical Approach with a Blunt Cannula
Use of a blunt cannula was first proposed as anintraoperative complement to RBA.[86] This tech-
nique has subsequently been proposed as a soleanaesthetic technique,[87] and has been used in upto 50% of cases in the UK.[3] Under TA, the bulbarconjunctiva is grasped with a small forceps,5–10mm away from the limbus. Blunt Wescottscissors are used to open a small buttonhole intothe conjunctiva and Tenon’s capsule to gain accessto the episcleral space. A blunt cannula is theninserted into the episcleral space to allow the in-jection. Several types of cannulas have been pro-posed: smooth curvedmetallic cannulas, ultrashortmetallic cannulas, and silicon or plastic cannu-las.[88,89] When no specific cannula is available, ashort intravenous catheter (18 or 20 gauge) withoutits needle can be used.
This technique is usually used with injection oflow volumes (2–5mL) of local anaesthetic, whichprovides good globe analgesia but only partialakinesia of the globe and lids. To obtain acceptableakinesia, the injected volumemust be increased to11mL.[82] Being a non-akinesia technique, low-volume STB carries the same limitations as TA.Indeed, it has been identified as a risk factor fordisplacement of nuclear fragments into the vitre-ous.[57] Another limitation is the relatively highrate of minor incidents, with a 2.3-fold increasecompared with RBA and PBA having been ob-served.[3] In a 6000-case series, Guise reportedthat 6% of cases had chemosis and 7% had sub-conjunctival haematoma, with only one case re-quiring cancellation of surgery.[84] However, STBefficacy is excellent for globe analgesia: 96% ofthe blocks were scored as perfect or good. More-over, use of small volumes causes a very smallincrease in IOP, such that preoperative com-pression of the globe may be unnecessary. Simi-larly, episcleral injection of a small volume oflocal anaesthetic may be used for an open globe.Therefore, it is the technique of choice as a sup-plemental injection when required intraopera-tively. Finally, the main advantage of the techniqueis its safety, because it avoids the blind introduc-tion of a needle in the orbit. Some complicationsof STB, although rare, have been described. Nev-ertheless, despite its proven safety record in largeseries, any needle block complication may occurafter STB, including strabismus, eyeball perfora-tion and sepsis.[13] One inadvertent perforation
30 Nouvellon et al.
ª 2010 Adis Data Information BV. All rights reserved. Drugs Aging 2010; 27 (1)

occurred during dissection, possibly due to syne-chias between the sclera and Tenon’s capsule in apreviously operated eye.[90] However, in largeseries, complications of STB are very rare. Guisereported no serious complication in 6000 cases.[84]
In the series of 375 000 procedures by Eke andThompson, STB appeared to cause a lower in-cidence of serious complications than RBA andPBA, although this difference was significantonly for life-threatening (not sight-threatening)complications.[46] In the British database series of>55 000 cases, STB was associated with a 2.5-folddecreased risk in serious complications comparedwith needle techniques.[3] Sub-Tenon’s anaes-thesia also leads to higher patient and surgeonsatisfaction than RBA and TA,[91,92] but is onlyslightly superior to PBA in this respect.[93]
5.4 Local Anaesthetics and AdjuvantAgents for Eye Blocks
All available local anaesthetics have been usedfor eye block, either alone or as a mixture of twoagents. Many publications have compared variouslocal anaesthetic mixtures and concentrations, andthese cannot be detailed here. The choice of localanaesthetics should be based on the pharmaco-logical properties and availability of the drugs,taking into account particularly the requirementfor quick onset (lidocaine, mepivacaine, articaine),prolonged effect, postoperative residual block foranalgesia (ropivacaine, bupivacaine) and akinesia(higher concentration). The most frequently usedlocal anaesthetics are lidocaine, bupivacaine, ropi-vacaine and mepivacaine, or a combination of twoof these.[94] The main differences found betweenthese local anaesthetic combinations are in accor-dance with their known pharmacological properties.Articaine, usually used more by dental surgeonsthan anaesthesiologists, has also been proposedfor both PBA and STB because of its quick onsetand short duration.[95,96] Articaine is also con-sidered to cause less myotoxicity and diplopiathan other drugs.[97] There is no definitive ‘magicbullet’ in terms of the ideal local anaesthetic foreye block. As the volume of local anaestheticinjected is usually small (3–10mL), systemictoxicity is not a major concern.
Hyaluronidase is an enzyme that facilitateswider spreading of local anaesthetics.[98] The onlysignificant, although very rare, complication ofhyaluronidase administration is immediate ordelayed allergy. This may cause orbital oedemaor a pseudotumoural orbitopathy, with a sub-sequent rise in IOP that may mimic an expulsivechoroidal haemorrhage[99] or lead to surgicalcomplications (posterior capsule rupture or vitre-ous loss).[100-104] As it is probably not due tohyaluronidase itself, this problem should beprevented by more effective purification[105] or,ideally, by use of recombinant hyaluronidase,which is available in the US. Use of hyaluroni-dase is classically assumed to shorten the onsetof the block and enhance its quality.[106] How-ever, the literature is somewhat controversial,showing a limited magnitude of benefit concern-ing akinesia.[107] This may be because of use ofvarying concentrations in different studies. Dosesvarying from 3.75 to 300 IU/mL of local anaes-thetic have been reported, with only a tendencytowards a greater benefit with higher doses.[108]
Given the wide range of concentrations used andthe absence of clear dose-efficacy ranging data,25–50 IU/mL can be proposed. Use of hyaluron-idase also permits a decrease in the amount oflocal anaesthetic required to achieve the sameefficacy.[109] Other benefits of hyaluronidaseinclude a smaller intraoperative increase in IOP,which may otherwise dramatically hinder sur-gery.[108] The last consideration in terms of thebenefits of hyaluronidase is its ability to decreasethe incidence of postoperative strabismus, possi-bly by limiting local anaesthetic myotoxicitybecause of a quicker spread.[110,111]
Other adjuvants are less frequently used.Clonidine, for instance, enhances intraoperativeand postoperative analgesia when added to localanaesthetic. At a dose of 0.5–1 mg/kg, clonidinedoes not increase the incidence of systemicadverse events such as hypotension or excessivesedation.[112] Moreover, clonidine may help toprevent intraoperative arterial hypertension andmay lower IOP. Adrenaline (epinephrine) issometimes added to increase the duration ofeye block. However, postoperative pain is not amajor concern after cataract surgery and the
Anaesthesia for Cataract Surgery 31
ª 2010 Adis Data Information BV. All rights reserved. Drugs Aging 2010; 27 (1)

availability of a new long-acting local anaesthetichas become the focus of less interest. Alkalinizationhas been proposed to decrease pain during injec-tion and to accelerate block onset, but has limitedefficacy. The optimal concentration of bicarbon-ate is difficult to determine because of the largepH range of local anaesthetic solutions providedby pharmaceutical firms. Moreover, the localanaesthetic may precipitate when there is ex-cessive alkalinization.[113] Small doses of musclerelaxant may enhance akinesia, but concern hasbeen expressed about their potential risk for sys-temic effects.[114] Opioids do not appear to bemore efficient when administered via a regionalophthalmic route than by systemic administra-tion.[115] Warming the local anaesthetic maydecrease pain on injection and enhance block effi-cacy, but no clinically relevant benefits appear tooccur.[116]
5.5 Controversy: Who ShouldPerform the Block?
Since the 1980s, anaesthesiologists have becomeincreasingly involved in eye blocks that werepreviously undertaken by surgeons. However,there are very great differences in anaesthesiolo-gists’ involvement in eye blocks both between andwithin countries. In some institutions, anaes-thesiologists are not available, and surgeons haveto manage the block themselves.[117,118] In otherareas, anaesthesiologists provide only monitoredanaesthesia care while the surgeon performs theblock. Finally, in many countries, such as Franceand the UK, anaesthesiologists are increasinglyperforming the blocks. Some reports have em-phasized complications after blocks performedby ‘‘anesthesia personnel’’.[119] In fact, some ofthese complications were associated with blocksperformed by nurse anaesthetists or operatingroom nurses directly supervised by surgeons. Itmust be stressed that eye blocks are, like anyother RA, relatively safe but potentially danger-ous. Anaesthesiologists should theoretically bethe most appropriate persons to perform eyeblocks, provide monitored anaesthesia care andmanage life-threatening complications. Providedthat they have been correctly taught and trained,
anaesthesiologists have demonstrated their abil-ity to perform eye blocks, as with other RAtechniques.[3,42,83,84] However, anaesthesiologistsare not available for eye block everywhere. Thecost effectiveness of this practice may vary amongvarious institutions, depending on the paymentsystem.
5.6 Supporting Therapies
Eye surgery, especially cataract surgery, hasvery little impact on perioperative morbidity andmortality.[120,121] Eye block is associated withlower perioperative morbidity than GA for oph-thalmic surgery, provided that no heavy sedationis added.[121-125] As a result, some standard safetymeasures such as monitoring, fasting and pre-operative evaluation, which are considered basicrecommendations for other types of block, aresometimes circumvented for eye blocks.[126]
The role of preoperative fasting remains contro-versial. When complications occur or there is aneed to convert to GA, a full stomach may con-stitute an aggravating factor. On the other hand,strict fasting is uncomfortable and may be con-sidered too heavy-handed given the very low in-cidence of such situations. Practices appear tovary widely among different countries.
Old patients undergoing eye surgery frequentlyhave coexisting disease. Therefore, a preoperativeassessment to ensure coexisting diseases are prop-erly controlled appears well advised.
Premedication is frequently used but should beutilized cautiously so as not to prevent early dis-charge because of residual excessive sedation in anambulatory setting. The most frequently useddrugs include benzodiazepines, hydroxyzine, clo-nidine, dexmedetomedine and melatonin.[127-130]
Antibacterial prophylaxis is limited to sepsis high-risk situations such as in the treatment of diabeticpatients, in which situation the antibacterial will bechosen for its intraocular penetration properties.A fluoroquinolone is a standard choice.[131] Shortsedation for performing the block might includesmall amounts of propofol or opioids.[44,83] Caremust be taken in patients with mental confusionand restlessness attributable to benzodiazepines orany other drug overdosage. Excessive sedation and
32 Nouvellon et al.
ª 2010 Adis Data Information BV. All rights reserved. Drugs Aging 2010; 27 (1)

subsequent mental confusion have been claimed tohave caused patient movement during performanceof RA with subsequent eyeball perforation.[132]
Because perioperative systemic adverse eventsof supporting therapies are so rare that their in-cidence cannot be measured, some physiciansadvise against any intraoperative monitoring ormonitored anaesthesia care.[133] However, giventhe underlying co-morbidities in many patients,adverse events are possible.[134] Even if their in-cidence is low, in the context of the very largeamount of cataract surgery performed each year,the absolute value of such events is probablysignificant. In the authors’ opinion, as in Frenchpractice, intraoperative monitoring should in-clude basic monitoring, i.e. ECG, pulse oximetryand automated noninvasive blood pressure mea-surement. Various British guidelines are less strictand recommend only continuous monitoring ofventilation and circulation by clinical observa-tion and pulse oximetry.[15,135] In patients withlife-threatening complications, the ability to per-form resuscitation is essential, and the sameguidelines recommend that ‘‘there should alwaysbe at least one person present who has AdvancedLife Support (ALS) training or equivalent’’.Intravascular access is clearly required.
Patient immobility is required during surgery.Anxiety and residual pain occur relatively fre-quently during eye surgery under local anaes-thesia, and the presence of drapes over the headmay increase anxiety. Therefore, the patientshould be positioned as comfortably as possible,with sufficient space to allow free breathing.Additional fresh air flow is preferable to oxygenas a means of improving ventilation in a confinedatmosphere. Intraoperative sedation can be usedto limit anxiety and pain, in addition to or insteadof premedication. However, heavy sedation hasbeen associated with an increase in complicationssuch as restlessness or hypoxia, and has even beenassociated with increasedmortality.[122] Excessivesedation can be avoided by cautious use of seda-tives (if needed), which are titrated before thepatient is draped. The most frequently used drugsare small doses of propofol or remifentanil infu-sion.[136,137] Continuous infusion of dexmedeto-medine or midazolam has also been proposed,
without enjoying widespread use.[138] To avoidexcessive sedation, patient-controlled or patient-target-controlled infusion have been proposed,again without achieving great popularity.[137,139]
6. Controversy: General Anaesthesiaversus RA
Anterior segment ophthalmic surgery is theonly human surgical procedure that has no de-tectable impact on patient survival.[123] There is alack of well conducted prospective large studiescomparing GA and RA for cataract surgery.Light planes of GA may lead to eye divergencywith subsequent eccentric eye position and im-paired surgical access to the globe.[140]
Postoperative cognitive dysfunction (POCD)in the elderly patient remains an unsolved pro-blem after GA for major surgery and is a pre-dictive factor for mortality.[141] Both anaesthesiaduration and the technique used for postopera-tive analgesia (particularly avoidance of RA, i.e.continuous epidural or peripheral nerve blocks)may play a role in increasing POCD.[5] This is anargument for avoiding GA for cataract surgery,which typically is totally painless postoperatively.
Most cataract surgeries are performed underRA, a choice based on the assumption that this isless hazardous to elderly patients. Although thisassumption seems logical for many, it is based onvery weak evidence or none at all. In a 20-yearnoncomparative survey, Quigley was not able todemonstrate any difference in mortality rate be-tween GA and RA.[124] Similarly, Hoskings et al.were not able to show any difference in short-termmortality and morbidity between GA and RA inelderly patients (age >90 years).[125] However, inthis series, patients’ age was greater in the RAgroup, possibly because physicians more fre-quently chose elderly and disabled patients, beingconvinced that RA is safer for fragile patients.Only Glantz et al. observed fewer myocardialischaemic events after RA than after GA.[121]
However, trying to impose use of RA in allcases is probably pointless. Neurological dis-eases and psychiatric disorders (e.g. deafness,Parkinson’s disease or mental confusion) mayimpair patient cooperation and the ability to lie
Anaesthesia for Cataract Surgery 33
ª 2010 Adis Data Information BV. All rights reserved. Drugs Aging 2010; 27 (1)
supine quietly during surgery under RA. Similarly,rheumatic pain or prostate adenoma dysuria mayprevent the patient from lying immobile underRA. The required time of immobility is around15 minutes, but may be longer, depending on thesurgeon’s skill and the characteristics of the catar-act. Sedation is frequently presented as a solutionbut excessive sedation may lead to restlessness,sleeping and snoring, or to respiratory depression,which, in the absence of any airway access, may becatastrophic. In cases where intraoperative im-mobility cannot be guaranteed, GA might be con-sidered as a first choice, rather than RA combinedwith hazardous heavy sedation.
7. Future of Cataract Anaesthesia
Cataract anaesthesia in the elderly is achievedmainly by RA or TA. Research should continuethe quest for the ‘Holy Grail’ that will provideanalgesia (PKE) and total akinesia when required(other surgical techniques), enabling proceduresto be carried out in absolute safety. In terms ofefficacy, STB appears to be the gold standard.However, most anaesthesiologists are unfamiliarwith cannula techniques, which require two-handexperience. Because of safety considerations,needle techniques will probably continue to losepopularity in the future. TA prevents anaesthesiacomplications but some concerns may still be ex-pressed over surgical difficulties caused by theabsence of akinesia. Specific local anaestheticjelly mixtures for TA should be developed. Hya-luronidase, although useful, is not available inmany countries, and further efforts should bemade to make it – including the recombinantform – more available.
8. Conclusion
Cataract surgery is the most frequent surgicalprocedure requiring anaesthesia in developedcountries. Over the last 20 years, anaesthesiolo-gists have played an increasing role in performingeye blocks. RBA is being progressively replacedby PBA. The requirement for very deep blockwith total akinesia has greatly decreased with theuse of PKE for cataract surgery, expanding the
place for TA or low-volume STB. Needle blockcarries a low but real risk of complications,mainly due to needle misplacement. Correctteaching and training are required to preventcomplications. The main patient risk factor forinadvertent globe perforation is the presence of amyopic staphyloma. Use of a surgical approachto gain access to sub-Tenon’s space avoids needleblock, but does not totally prevent complications.When deep anaesthesia is required, STB, per-formed either by the needle technique or usinga surgical approach, appears to be the techniqueof choice.
Acknowledgements
No sources of funding were used to assist in the prepara-tion of this review. Jacques Ripart has acted as a consultant toAstraZeneca, France, and Air Liquide Sante, France. Theother authors have no conflicts of interest that are directlyrelevant to the content of this review. The authors acknowl-edge Serge Albertini for his English editing of the article.
References1. Leaming DV. Practice styles and preferences of ASCRS
members: 2003 survey. J Cataract Refract Surg 2004; 30:892-900
2. Pick ZS, Leaming DV, Elder MJ. The fourth New Zealandcataract and refractive surgery survey: 2007. Clin Experi-ment Ophthalmol 2008; 36: 604-19
3. El-Hindy N, Johnston RL, Jaycock P, et al., UK EPRUserGroup. The Cataract National Dataset electronic multi-centre audit of 55 567 operations: anaesthetic techniquesand complications. Eye 2009; 23: 50-5
4. Schutz JS, Mavrakanas NA. What degree of anaesthesia isnecessary for intraocular surgery? It depends on whethersurgery is ‘‘open’’ or ‘‘closed’’. Br J Ophthalmol. In press
5. Cohendy R, Brougere A, Cuvillon P. Anaesthesia in theolder patient. Curr Opin Clin Nutr Metab Care 2005; 8:17-21
6. Narendran N, Jaycock P, Johnston RL, et al. The CataractNational Dataset electronic multicentre audit of 55 567operations: risk stratification for posterior capsule rup-ture and vitreous loss. Eye 2009; 23: 31-7
7. Kelly JM. Preoperative assessment and medication. In:Mostafa SM, editor. Anaesthesia for ophthalmic surgery.New York: Oxford University Press, 1991: 95-105
8. Stupp T, Hassouna I, Soppart K, et al. Systemic adverseevents: a comparison between topical and peribulbar an-aesthesia in cataract surgery. Ophthalmologica 2007; 221:320-5
9. Sharwood PL, Thomas D, Roberts TV. Adverse medicalevents associated with cataract surgery performed under
34 Nouvellon et al.
ª 2010 Adis Data Information BV. All rights reserved. Drugs Aging 2010; 27 (1)
topical anaesthesia. Clin Experiment Ophthalmol 2008;36: 842-6
10. Landoni G, Zambon M, Zangrillo A. Reducing peri-operative myocardial infarction with anesthetic drugs andtechniques. Curr Drug Targets. In press
11. Jonas JB, Pakdaman B, Sauder G. Cataract surgery undersystemic anticoagulant therapy with coumarin. Eur JOphthalmol 2006; 16: 30-2
12. Edge KR, Nicoll MV. Retrobulbar hemorrhage after 12500retrobulbar blocks. Anesth Analg 1993; 76: 1019-22
13. Ruschen H, Bremner FD, Carr C. Complications after sub-Tenon’s eye block. Anesth Analg 2003; 96: 273-7
14. Kumar N, Jivan S, Thomas P, et al. Sub-Tenon’s anesthe-sia with aspirin, warfarin, and clopidogrel. J CataractRefract Surg 2006; 32: 1022-5
15. The Royal College of Anaesthetists and the Royal Collegeof Ophthalmologists. Local anaesthesia for intraocularsurgery. London: Royal College of Anaesthetists, 2001[online]. Available from URL: http://www.rcoa.ac.uk/docs/RCARCOGuidelines.pdf [Accessed 2009 Sep 29]
16. Societe Francaise d’Anesthesie et de Reanimation et SocieteFrancaise d’Hematologie. Antiplatelet agents and the peri-operative period, 2001 [online]. Available fromURL: http://www.sfar.org/pdf/aapconfexp.pdf [Accessed 2009 Sep 29]
17. Ong-Tone L, Paluck EC, Hart-Mitchell RD. Periopera-tive use of warfarin and aspirin in cataract surgery byCanadian Society of Cataract and Refractive Surgerymembers: survey. J Cataract Refract Surg 2005; 31: 991-6
18. Pandey SK, Werner L, Apple DJ, et al. No-anesthesia clearcorneal phacoemulsification versus topical and topicalplus intracameral anesthesia: randomized clinical trial.J Cataract Refract Surg 2001; 27: 1643-50
19. Koornneef L. Details of the orbital connective tissue in theadult: the architecture of the musculo-fibrous apparatusin the human orbit. Acta Morphol Neerl-Scand 1977; 15:1-64
20. Ripart J, Lefrant JY, de La Coussaye JE, et al. Peribulbarversus retrobulbar anesthesia for ophthalmic surgery: ananatomical comparison of extraconal and intraconalinjections. Anesthesiology 2001; 94: 56-62
21. Aldrete JA, Romo-Salas F, Arora S, et al. Reverse arterialblood flow as a pathway for central nervous system toxicresponses following injection of local anesthetics. AnesthAnalg 1978; 57: 428-33
22. Nicoll JMV, Acharya PA, Ahlen K, et al. Central nervoussystem complication after 6000 retrobulbar blocks.Anesth Analg 1987; 66: 1298-302
23. Loken RG, Mervyn Kirker GE, Hamilton RC. Respira-tory arrest following peribulbar anesthesia for cataractsurgery: case report and review of the literature. Can JOphthalmol 1998; 33: 225-6
24. Katsev DA, Drews RC, Rose BT. Anatomic study of retro-bulbar needle path length. Ophthalmology 1989; 96: 1221-4
25. Edge R, Navon S. Scleral perforation during retrobulbarand peribulbar anesthesia: risk factor and outcome in50 000 consecutive injections. J Cataract Refract Surg1999; 25: 1237-44
26. Duker JS, Belmont JB, Benson WE, et al. Inadvertentglobe perforation during retrobulbar and peribulbar an-esthesia. Ophthalmology 1991; 98: 519-26
27. Vohra SB, Good PA. Altered globe dimensions of axialmyopia as risk factors for penetrating ocular injury duringperibulbar anaesthesia. Br J Anaesth 2000; 85: 242-5
28. Carlson BM, Rainin EA. Rat extraocular muscle re-generation: repair of local anesthetic-induced damage.Arch Ophthalmol 1985; 103: 1373-7
29. Hersch M, Baer G, Diecker JP, et al. Optic nerve enlarge-ment and central retinal-artery occlusion secondary toretrobulbar anesthesia. Ann Ophthalmol 1989; 21: 195-7
30. Atkinson WS. Retrobulbar injection of anesthetic withinthe muscular cone (cone injection). Arch Ophthalmol1936; 16: 495-503
31. Davis DB, Mandel MR. Posterior peribulbar anesthesia:an alternative to retrobulbar anesthesia. J Cataract Re-fract Surg 1986; 12: 182-4
32. Bloomberg LB. Administration of periocular anesthesia.J Cataract Refract Surg 1986; 12: 677-9
33. Van Lindt M. Paralysie palpebrale transitoire provoqueedans l’operation de la cataracte. Ann Ocul 1914; 151:420-4
34. Liu C, Youl B, Moseley I. Magnetic resonance imaging ofthe optic nerve in the extremes of gaze: implications forthe positioning of the globe for retrobulbar anaesthesia.Br J Ophthalmol 1992; 76: 728-33
35. Unsold R, Stanley JA, Degroot J. The CT topography ofretrobulbar anesthesia: anatomical correlation of implica-tions and suggestion of a modified technique. AlbrechtVon Graefes Arch Klin Exp Ophthalmol 1981; 217: 125-36
36. Davis DB, Mandel MR. Efficacy and complication rate of16 224 consecutive peribulbar blocks: a prospective multi-center study. J Cataract Refract Surg 1994; 20: 327-37
37. Demirok A, Simsek S, Cinal A, et al. Peribulbar anesthesia:one versus two injections. Ophthalmic Surg Lasers 1997;28: 998-1001
38. Ball JL, Woon WH, Smith S. Globe perforation by thesecond peribulbar injection. Eye 2002; 16: 663-5
39. Sarvela J, Nikki P. Comparison of two needle lengths inregional ophthalmic anesthesia with etidocaine and hya-luronidase. Ophthalmic Surg 1992; 23: 742-5
40. Karampatakis V, Natsis K, Gisgis P, et al. The risk of opticnerve injury in retrobulbar anesthesia: a comparativestudy on 35 and 40mm retrobulbar needles in 12 cadavers.Eur J Ophthalmol 1998; 8: 184-7
41. Riad W, Ahmed N. Single injection peribulbar anesthesiawith a short needle combined with digital compression.Anesth Analg 2008; 107: 1751-3
42. Hustead RF, Hamilton RC, Loken RG. Periocular localanesthesia: medial orbital as an alternative to superiornasal injection. J Cataract Refract Surg 1994; 20: 197-201
43. Waller SG, Taboada J, O’Connor P. Retrobulbar an-esthesia risk: do sharp needles really perforate the eyemore easily than blunt needles? Ophthalmology 1993; 100:506-10
44. Ripart J, Lefrant JY, Vivien B, et al. Ophthalmic regionalanesthesia: canthus episcleral anesthesia is more efficientthan peribulbar anesthesia: a double blind randomizedstudy. Anesthesiology 2000; 92: 1278-85
45. Demediuk OM, Dhaliwal RS, Papworth DP, et al.A comparison of peribulbar and retrobulbar anesthesia
Anaesthesia for Cataract Surgery 35
ª 2010 Adis Data Information BV. All rights reserved. Drugs Aging 2010; 27 (1)
for vitreoretinal surgical procedures. Arch Ophthalmol1995; 113: 908-13
46. Eke T, Thompson JR. Serious complications of local an-aesthesia for cataract surgery: a 1 year national survey inthe United Kingdom. Br J Ophthalmol 2007; 91: 470-5
47. Alhassan MB, Kyari F, Ejere HO. Peribulbar versusretrobulbar anaesthesia for cataract surgery. CochraneDatabase Syst Rev 2008; 16 (3): CD004083
48. Barequet IS, Sachs D, Priel A, et al. Phacoemulsification ofcataract in patients receiving coumadin therapy: ocularand hematologic risk assessment. Am J Ophthalmol 2007;144: 719-72
49. Wagle AA, Wagle AM, Bacsal K, et al. Practice prefer-ences of ophthalmic anaesthesia for cataract surgery inSingapore. Singapore Med J 2007; 48: 287-90
50. Boezaart A, Berry R, Nell M. Topical anesthesia versusretrobulbar block for cataract surgery: the patient’sperspective. J Clin Anesth 2000; 12: 58-60
51. Rebolleda G, Munoz-Negrete FJ, Gutierrez-Ortiz C.Topical plus intracameral lidocaine versus retrobulbaranesthesia in phacotrabeculectomy: prospective random-ized study. J Cataract Refract Surg 2001; 27: 1214-20
52. Gombos K, Jakubovits E, Kolos A, et al. Cataract surgeryanaesthesia: is topical anaesthesia really better than ret-robulbar? Acta Ophthalmol Scand 2007; 85: 309-16
53. Sekundo W, Dick HB, Schmidt JC. Lidocaine-assistedxylocaine jelly anesthesia versus one quadrant sub-Tenoninfiltration for self-sealing sclero-corneal incision routinephacoemulsification. Eur J Ophthalmol 2004; 14: 111-6
54. Davison M, Padroni S, Bunce C, et al. Sub-Tenon’s an-aesthesia versus topical anaesthesia for cataract surgery.Cochrane Database Syst Rev 2007; 18 (3): CD006291
55. Jacobi PC, Dietlein TS, Jacobi FK. A comparative study oftopical vs retrobulbar anesthesia in complicated cataractsurgery. Arch Ophthalmol 2000; 118: 1037-43
56. Shaw AD, Ang GS, Eke T. Phacoemulsification compli-cation rates. Ophthalmology 2007; 114: 2101-2
57. Mahmood S, von Lany H, ColeMD, et al. Displacement ofnuclear fragments into the vitreous complicating phaco-emulsification surgery in the UK: incidence and risk fac-tors. Br J Ophthalmol 2008; 92: 488-92
58. Waddell KM, Reeves BC, Johnson GI. A comparison ofanterior and posterior chamber lenses after cataract ex-traction in rural Africa: a within patient randomized trial.Br J Ophthalmol 2004; 88: 734-9
59. Bourne RR,MinassianDC, Dart JK, et al. Effect of cataractsurgery on the corneal endothelium: modern phacoemulsi-fication compared with extracapsular surgery. Ophthalmo-logy 2004; 11: 679-85
60. Borazan M, Karalezli A, Akova YA, et al. Comparativeclinical trial of topical anaesthetic agents for cataractsurgery with phacoemulsification: lidocaine 2% drops,levobupivacaine 0.75% drops, and ropivacaine 1% drops.Eye 2008; 22: 425-9
61. Fernandez SA, Dios E, Diz JC. Comparative study of to-pical anaesthesia with lidocaine 2% vs levobupivacaine0.75% in cataract surgery. Br J Anaesth 2009; 102: 216-20
62. Karp CL, Cox TA, Wagoner MD, et al. Intracameral an-esthesia: a report by the AmericanAcademy ofOphthalmo-logy. Ophthalmology 2001; 108: 1704-10
63. Heuerman T, Hartman C, Anders N. Long term endo-thelial cell loss after phacoemulsification: peribulbar an-esthesia versus intracameral lidocaine 1%: prospectiverandomized study. J Cataract Refract Surg 2002; 28:638-43
64. Boulton JE, Lopatazidis A, Luck J, et al. A randomizedcontrolled trial of intracameral lidocaine during phaco-emulsification under topical anesthesia. Ophthalmology2000; 107: 68-71
65. Roberts T, Boytell K. A comparison of cataract surgeryunder topical anaesthesia with and without intracamerallignocaine. Clin Experiment Ophthalmol 2002; 30: 19-22
66. Pang MP, Fujimoto DK, Wilkens LR. Pain, photophobia,and retinal and optic nerve function after phacoemulsifi-cation with intracameral lidocaine. Ophthalmology 2001;108: 2018-25
67. Ezra DG, Nambiar A, Allan BD. Supplementary intra-cameral lidocaine for phacoemulsification under topicalanesthesia: a meta-analysis of randomized controlledtrials. Ophthalmology 2008; 115: 455-87
68. Ezra DG, Allan BD. Topical anaesthesia alone versus to-pical anaesthesia with intracameral lidocaine for phaco-emulsification. Cochrane Database Syst Rev 2007 Jul18; (3): CD005276
69. Bardocci A, Lofoco G, Perdicaro S, et al. Lidocaine 2% gelversus lidocaine 4% unpreserved drops for topical an-esthesia in cataract surgery: a randomized controlled trial.Ophthalmology 2003; 110: 144-9
70. Aziz ES. Deep topical fornix nerve block versus peribulbarblock in one-step adjustable suture horizontal strabismussurgery. Br J Anaesth 2002; 88: 129-32
71. Mahe I, Mouly S, Jarrin I, et al. Efficacy and safety of threeophthalmic inserts for topical anaesthesia of the cornea:an exploratory comparative dose-ranging, double-blind,randomized trial in healthy volunteers. Br J Clin Phar-macol 2005; 59: 220-6
72. Barequet IS, Soriano ES, Green WR, et al. Provisionof anesthesia with single application of lidocaine gel.J Cataract Refract Surg 1999; 25: 626-31
73. Agence Francaise pour la Securite Sanitaire et des Produitsde Sante (AFSSAPS): Mesusage de Xylocaıne� 2%, geluretral en seringue pre-remplie: endophtalmies rapporteeslors du traitement chirurgical de la cataracte. Vigilances2004 Oct; (2): 2 [online]. Available from URL: http://www.afssaps.fr/var/afssaps_site/storage/original/application/9095a6c4be02687266bd4b042dad2229.pdf [AccessedSep 29]
74. Garcia-Arumi J, Fonollosa A, Sararols L, et al. Topicalanesthesia: possible risk factor for endophthalmitisafter cataract extraction. J Cataract Refract Surg 2007;33: 989-92
75. Perone JM, Popovici A, Ouled-Moussa R, et al. Safety andefficacy of two ocular anesthetic methods for phaco-emulsification: topical anesthesia and viscoanesthesia(VisThesia). Eur J Ophthalmol 2007; 17: 171-7
76. Amiel H, Koch PS. Tetracaine hydrochloride 0.5% versuslidocaine 2% jelly as a topical anesthetic agent in cataractsurgery: comparative clinical trial. J Cataract RefractSurg 2007; 33: 98-100
36 Nouvellon et al.
ª 2010 Adis Data Information BV. All rights reserved. Drugs Aging 2010; 27 (1)
77. Cagini C, De Carolis A, Fiore T, et al. Limbal anaesthesiaversus topical anaesthesia for clear corneal phacoemulsi-fication. Acta Ophthalmol Scand 2006; 84: 105-9
78. Ripart J, Prat-Pradal D, Charavel P, et al. Medial canthussingle injection episcleral (sub-Tenon) anesthesia ana-tomic imaging. Clin Anat 1998; 11: 390-5
79. Ripart J, Metge L, Prat-Pradal D, et al. Medial canthussingle injection episcleral (sub-Tenon) anesthesia com-puted tomography imaging. Anesth Analg 1998; 87: 43-5
80. Ripart J, Benbabaali M, L’Hermitte J, et al. Ophthalmicblocks at the medial canthus (reply). Anesthesiology 2001;95: 1533-5
81. Zafirakis P, Voudouri A, Rowe S, et al. Topical versus sub-Tenon’s anesthesia without sedation in cataract surgery.J Cataract Refract Surg 2001; 27: 873-9
82. Li HK, Abouleish A, Grady J, et al. Sub-Tenon’s injectionfor local anesthesia in posterior segment surgery. Oph-thalmology 2000; 107: 41-7
83. Nouvellon E, L’Hermite J, Chaumeron A, et al. Ophthal-mic regional anesthesia: medial canthus episcleral (sub-Tenon’s) single injection block. Anesthesiology 2004; 100:370-4
84. Guise P. SubTenon’s anesthesia: a prospective study of6000 blocks. Anesthesiology 2003; 98: 964-8
85. Allman KG, Theron AD, Byles DB. A new technique ofincisionless minimally invasive sub-Tenon’s anaesthesia.Anaesthesia 2008; 63: 782-3
86. Mein CE, Flynn HW. Augmentation of local anesthesiaduring retinal detachment surgery. Arch Ophthalmol1989; 107: 1084
87. Stevens JD. A new local anaesthesia technique for cataractextraction by one quadrant sub-Tenon’s infiltration. Br JOphthalmol 1992; 76: 670-4
88. Kumar CM, Mac Neela BJ. Ultrasonic localization of an-aesthetic fluids using sub Tenon’s cannulae of three dif-ferent lengths. Eye 2003; 17: 1-5
89. MacNeela BJ, Kumar CM. Sub-Tenon’s block using ultra-short cannula. J Cataract Refract Surg 2004; 30: 858-62
90. Friedman BJ, FriedbergMA. Globe perforation associatedwith sub-Tenon’s anesthesia. Am JOphthalmol 2001; 131:520-1
91. Rodrigues PA, Vale PJ, Cruz LM, et al. Topical anesthesiaversus sub-Tenon block for cataract surgery: surgicalconditions and patient satisfaction. Eur J Ophthalmol2008; 18: 356-60
92. Ryu JH, Kim M, Bahk JH, et al. A comparison of retro-bulbar block, sub-Tenon block, and topical anesthesiaduring cataract surgery. Eur J Ophthalmol 2009; 19: 240-6
93. Budd JM, Brown JP, Thomas J, et al. A comparison of sub-Tenon’s with peribulbar anaesthesia in patients under-going sequential bilateral cataract surgery. Anaesthesia2009; 64: 19-22
94. Borazan M, Karalezli A, Oto S, et al. Comparison of abupivacaine 0.5% and lidocaine 2% mixture with levobu-pivacaine 0.75% and ropivacaine 1% in peribulbar an-aesthesia for cataract surgery with phacoemulsification.Acta Ophthalmol Scand 2007; 85: 844-7
95. Ozdemir M, Ozdemir G, Zencirci B, et al. Articaine versuslidocaine plus bupivacaine for peribulbar anaesthesia incataract surgery. Br J Anaesth 2004; 92: 231-4
96. Gouws P, Galloway P, Jacob J, et al. Comparison ofarticaine and bupivacaine/lidocaine for sub-Tenon’s an-aesthesia in cataract extraction. Br J Anaesth 2004; 92:228-30
97. Raman SV, Barry JS, Murjaneh S, et al. Comparison of 4%articaine and 0.5% levobupivacaine/2% lidocaine mixturefor sub-Tenon’s anaesthesia in phacoemulsification cat-aract surgery: a randomised controlled trial. Br J Oph-thalmol 2008; 92: 496-9
98. Khandwala M, Ahmed S, Goel S, et al. The effect of hya-luronidase on ultrasound-measured dispersal of local an-aesthetic following sub-Tenon injection. Eye 2008; 22:1065-8
99. Minning CA. Hyaluronidase allergy simulating expulsivechoroidal hemorrhage. Arch Ophthalmol 1994; 112: 585-6
100. Agrawal A, Mclure HA, Dabbs TR. Allergic reaction tohyaluronidase after a peribulbar injection [letter]. Anaes-thesia 2003; 58: 814-5
101. Etesse B, Beaudroit L, Deleuze M, et al. Hyaluronidase:here we go again. Ann Fr Anesth Reanim 2009; 28: 658-65
102. Kumar CM, Dowd TC, Dodds C, et al. Orbital swellingfollowing peribulbar and sub-Tenon’s anaesthesia. Eye2004; 18: 418-20
103. Quhill F, Bowling B, Packard RB. Hyaluronidase allergyafter peribulbar anesthesia with orbital inflammation.J Cataract Refract Surg 2004; 30: 916-7
104. Ahluwalia HS, Lukaris A, Lane CM. Delayed allergic re-action to hyaluronidase: a rare sequel to cataract surgery.Eye 2003; 17: 263-6
105. Eberhart AH, Weiler CR, Erie JC. Angioedema relatedto the use of hyaluronidase in cataract surgery. Am JOphthalmol 2004; 138: 142-3
106. Remy M, Pinter F, Nentwich MM, et al. Efficacy andsafety of hyaluronidase 75 IU as an adjuvant to mepiva-caine for retrobulbar anesthesia in cataract surgery.J Cataract Refract Surg 2008; 34: 1966-9
107. Alwitryy A, Chaudhary S, Gopee K, et al. Effect of hya-luronidase on ocular motility in sub Tenon’s anesthesia:randomized controlled trial. J Cataract Refract Surg2002; 28: 1420-3
108. Dempsey GA, Barrett PJ, Kirby IJ. Hyaluronidase andperibulbar block. Br J Anaesth 1997; 78: 671-4
109. Schulenburg HE, Sri-Chandana C, Lyons G, et al. Hya-luronidase reduces local anaesthetic volumes for sub-Tenon’s anaesthesia. Br J Anaesth 2007; 99: 717-20
110. Brown SM, Coats DK, Collins MLZ, et al. Second clusterof strabismus cases after periocular anesthesia withouthyaluronidase. J Cataract Refract Surg 2001; 27: 1872-5
111. Hamada S, Devys JM, Xuan TH, et al. Role of hyalur-onidase in diplopia after cataract surgery. Ophthalmology2005; 112: 879-82
112. Bharti N, Madan R, Kaul HL, et al. Effect of additionof clonidine to local anaesthetic mixture for peribulbarblock. Anaesth Intens Care 2002; 30: 438-41
113. Hinshaw KD, Fiscella R, Sugar J. Preparation of pH-adjusted local anesthetics. Ophthalmic Surg 1995; 26: 194-9
114. Kucukyavuz Z, Arici MK. Effects of atracurium added tolocal anesthetics on akinesia in peribulbar block. RegAnesth Pain Med 2002; 27: 487-90
Anaesthesia for Cataract Surgery 37
ª 2010 Adis Data Information BV. All rights reserved. Drugs Aging 2010; 27 (1)
115. Hemmerling TM, Budde WM, Koppert W, et al. Retro-bulbar versus systemic application of morphine duringtitratable regional anesthesia via retrobulbar catheter inintraocular surgery. Anesth Analg 2000; 91: 585-8
116. Krause M, Weindler J, Ruprecht KW. Does warming ofanesthetic solutions improve analgesia and akinesia inretrobulbar anesthesia? Ophthalmology 1997; 104: 429-32
117. Hansen TE. Practice styles and preferences of Danishcataract surgeons: 1995 survey. Acta Ophthalmol Scand1996; 74: 56-9
118. Royal College of Anaesthetists Guidance on the provisionof ophthalmic anaesthesia services [online]. Availablefrom URL: http://www.rcoa.ac.uk/docs/GPAS-Ophth.pdf[Accessed 2009 Sep 29]
119. Grizzard WS, Kirk NM, Pavan PR, et al. Perforatingocular injuries caused by anesthesia personnel. Ophthal-mology 1991; 98: 1011-6
120. Eke T, Thompson JR. The national survey of local an-esthesia for ocular surgery II: safety profile of local an-esthesia techniques. Eye 1999; 13: 196-204
121. Glantz L, Drenger B, Gozal Y. Perioperative myocardialischemia in cataract surgery patients: general vs local an-esthesia. Anesth Analg 2000; 91: 1415-9
122. Katz J, Feldman MA, Bass EB. Adverse intraoperativemedical events and their association with anesthesiamanagement strategies in cataract surgery. Ophthalmol-ogy 2001; 108: 1721-6
123. Edwards AE, Seymour DG, McCarthy JM, et al. A 5-yearsurvival study of general surgical patients aged 65 yearsand over. Anaesthesia 1996; 51: 3-10
124. Quigley HA. Mortality associated with ophthalmic sur-gery: a 20-year experience at the Wilmer institute. Am JOphthalmol 1974; 77: 517-24
125. Hoskings MP, Warner MA, Lobdell CM, et al. Outcomesof surgery in patients 90 years of age and older. JAMA1989; 261: 1909-15
126. Eke T, Thompson JR. The national survey of local an-esthesia for ocular surgery: survey methodology and cur-rent practice. Eye 1999; 13: 189-95
127. Filos KS, Patroni O, Goudas LC, et al. A dose-responsestudy of orally administered clonidine as premedicationin the elderly: evaluating hemodynamic safety. AnesthAnalg 1993; 77: 1185-92
128. Barioni MF, Lauretti GR, Lauretti-FO A, et al. Cloni-dine as a coadjuvant in eye surgery: comparison of peri-bulbar vs oral administration. J Clin Anaesth 2002; 14:140-5
129. Erdurmus M, Aydin B, Usta B, et al. Patient comfort andsurgeon satisfaction during cataract surgery using topical
anesthesia with or without dexmedetomidine sedation.Eur J Ophthalmol 2008 May-Jun; 18 (3): 361-7
130. Ismail SA, Mowafi HA. Melatonin provides anxiolysis,enhances analgesia, decreases intraocular pressure, andpromotes better operating conditions during cataractsurgery under topical anesthesia. Anesth Analg 2009; 108:1146-51
131. Societe Francaise d’Anesthesie et de Reanimaation. Re-commandations pour la pratique de l’antibioprophylaxieen chirurgie [online]. Available from URL: http://www.sfar.org/antibiofr.html [Accessed 2009 Sep 29]
132. Schaack E, Diallo B, Devys JM. Inadvertent globe per-foration during peribulbar anaesthesia and sedation withpropofol. Ann Fr Anaesth Reanim 2006; 25: 43-5
133. Rocha G, Turner C. Safety of cataract surgery under to-pical anesthesia with oral sedation without anestheticmonitoring. Can J Ophthalmol 2007; 42: 288-94
134. Quantock CL, Goswami T. Death potentially secondary tosub-Tenon’s block. Anaesthesia 2007; 62: 175-7
135. The Royal College of Ophthalmologists. Commissioningcataract surgery: an outline of good practice. 2004 [on-line]. Available fromURL: http://www.rcophth.ac.uk/docs/publications/published-guidelines/CommissioningCataractSurgery-April2004.pdf [Accessed 2009 Sep 29]
136. Yun MJ, Oh AY, Kim KO, et al. Patient-controlled seda-tion vs anaesthetic nurse-controlled sedation for cataractsurgery in elderly patients. Int J Clin Pract 2008; 62: 776-8
137. Akgul A, Aydin ON, Dayanir V, et al. Usage of re-mifentanil and fentanyl in intravenous patient-controlledsedo-analgesia. Agri 2007; 19: 39-46
138. Alhashemi JA. Dexmedetomidine vs midazolam formonitored anaesthesia care during cataract surgery. Br JAnaesth 2006; 96: 722-6
139. Pac-Soo CK, Deacock S, Lockwood G, et al. Patient-controlled sedation for cataract surgery using peribulbarblock. Br J Anaesth 1996; 77: 370-4
140. Rossiter JD, Wood M, Lockwood A, et al. Operatingconditions for ocular surgery under general anaesthesia:an eccentric problem. Eye 2006; 20: 55-8
141. Steinmetz J, Christensen KB, Lund T, et al., and the ISPOCDGroup. Long-term consequences of postoperative cogni-tive dysfunction. Anesthesiology 2009; 110: 548-55
Correspondence: Prof. Jacques Ripart, Departement d’Anesthesie-Douleur, Centre Hospitalier Universitaire deNımes, Hopital Caremeau, Place du Pr Debre, 30029 Nımes,CEDEX 09, France.E-mail: [email protected]
38 Nouvellon et al.
ª 2010 Adis Data Information BV. All rights reserved. Drugs Aging 2010; 27 (1)

Copyright of Drugs & Aging is the property of ADIS International Limited and its content may not be copied or
emailed to multiple sites or posted to a listserv without the copyright holder's express written permission.
However, users may print, download, or email articles for individual use.