
INFORMAL CARERS PROJECT (FIRST DRAFT)uir.ulster.ac.uk/24073/1/finalr~1.doc · Web view3.6.2...
267
Informal Carers Research Project Report (3 rd Draft, July 2000) Front Cover Crest – SEHB, W.I.T., and U.U.
Transcript of INFORMAL CARERS PROJECT (FIRST DRAFT)uir.ulster.ac.uk/24073/1/finalr~1.doc · Web view3.6.2...
Informal Carers Research Project Report (3rd Draft, July 2000)
Front Cover
Crest – SEHB, W.I.T., and U.U.
The Health and Social Care Needs of Informal Carers
of Older People:
An Exploratory Study
September 2000
Paula Lane, Research Officer, South Eastern Health Board / Waterford Institute of Technology;
Professor H.P. McKenna, Head of School of Health Sciences, University of Ulster;
Mrs Assumpta Ryan, Lecturer in Nursing, University of Ulster;
Mr Paul Fleming, Lecturer in Health Promotion, University of Ulster.
ACKNOWLEDGEMENTS
The contributions of several people must be acknowledged as central to this research study.
Our deepest thanks are extended to all the carers who consented to partake in the study.
Our appreciation is also conveyed to The Carer’s Association and The Alzheimer’s Disease
Society for their co-operation and support in the project.
Many thanks to Ms. Louise Griffin for her administrative support, patience and good will during
the project.
We are indebted to Mr.Tom Moffat, Minister for State at the Department of Health and Children
who commissioned and funded the project.
Sincere thanks to Mr. J. Magner, Regional Manager at the South Eastern Health Board; who was
instrumental in initiating the project.
We are most grateful to all the public health and community psychiatric nurses whose
participation in the various data collection methods is sincerely appreciated.
Members of the Research Steering Group
Mrs. E. Carroll, Superintendent Public Health Nurse, Waterford Community Care Centre,
Mrs. H. Daniels, Director of Nursing, Waterford Regional Hospital;
Mr. Tony Gyves, Hospital Manager, St. Otterans’ Psychiatric Hospital, Waterford;
Mr. J. Magner, Regional Manager, South Eastern Health Board;
Dr. V. Martin, Head of Research and Development, Waterford Institute of Technology;
Academic Advisory Team
Prof. H. P. McKenna, Head of School of Health Sciences; University of Ulster,
Ms. A. Ryan, Lecturer in Nursing; University of Ulster;
Mr. P. Fleming, Lecturer in Health Promotion; University of Ulster;
Mr. B Cunningham, Statistical Advisor; University of Ulster.
ii

EXECUTIVE SUMMARYIn 1999, the theme of the International Year of Older Persons was “Towards A Society For All
Ages”. This theme fostered the concepts of inclusiveness and human unity, in opening up channels
of multigenerational communication amidst a society where older people and their carers sometimes
experience marginalisation. The designation of 1999 as the United Nations International Year of
Older Persons has raised the profile of issues in relation to these population groups. Despite a
significant growth in the academic literature on care-giving and carers’ needs in the past decade,
many gaps remains at empirical, rational, and conceptual levels (George, 1994; Kellett and
Mannion, 1999). Indeed, a clear understanding of the pertinent issues remains elusive (Gubrium,
1995). In Ireland, there is a dearth of empirical evidence regarding carers’ subjectively percei3ved
needs and experiences. Ruddle et al (1997) highlight the lack of available data in many areas of the
care of older persons, suggesting that a database to underpin policy and practice,
“…must be established through research on assessment of needs, exploratory research on possible services and solutions to address needs and problems and evaluation research on the services provided" (p.324).
Advancing Healthcare Research Initiatives
Recent fundamental changes in health care policy and provision in the U.K. (D.O.H; 1993) and
Ireland (D.O.H; 1994) have emphasised the need for a research culture within the health services.
The argument underpinning this revolves around the assumption that increasing the evidence base
of practice may have a significant impact on the quality of care and consequently quality of life.
Implicit within this cultural change, is the challenge to demonstrate more evidence based effective
and efficient health and social care strategies to meet stakeholder requirements, and to do so in a
flexible responsive manner. As a result, health service providers are becoming more research aware
and more research active.
The South Eastern Health Board in association with Waterford Institute of Technology and The
University of Ulster launched this research study in March 1999. Its aim was to assess perceived
health and social care needs of informal carers of older people. The Board commissioned the project
on the basis that it was both pertinent and timely to explore these issues in an attempt to promote the
basic human rights of older people and their carers, based on independence, participation, self-
fulfilment, care and dignity. The rationale prompting the study stemmed from drives within the
South Eastern Health Board to inform future service plans, with the ultimate aim of using those
inputs and service provision strategies shown to produce effective and efficient outcomes. This
iii
report was written to provide an evidence base for those involved in policy development,
commissioning, planning and operationalising services in support of the carers of older people in
home care settings.
THEMES FROM THE LITERATURE
On analysis of the extant literature, it was found that while some studies have explored carers’
needs, there is a dearth of consultative research exploring carers' subjectively perceived health and
social care needs; particularly in Ireland. Many gaps remain in the evidence base pertaining to
conceptual, rational and humanitarian aspects of care-giving. Specifically, the following points
summarise the main themes identified:
Significant weaknesses were identified in relation to the nature of health and social care services
as well as the planning, organisation and delivery of such services;
Contemporary approaches to determining carers’ needs and experiences are unsystematic, lack
monitoring and evaluation and are predominantly normatively derived without structured
consultation with carers themselves;
The importance of developing flexible, responsive approaches to addressing carers’ needs in
a proactive way, particularly regarding support services is emphasised throughout the
literature;
There is a need for greater flexibility and scope in the way multidisciplinary community care
teams function in order to invoke more effective and efficient care interventions. In this regard,
health promotion and health protection initiatives are central to maintaining and improving
carers’ health and well being, as well as that of the care recipient;
Benefits should be constructed around positive experiences of care-giving, facilitated by
cohesive systems of care and embracing opportunities for services such as respite care, socio-
economic and emotional supports as well as practical assistance;
The segmented, haphazard nature of some areas of service provision reinforce the value of a
thorough exploration and evaluation of current and future service plans in relation to carers’
needs. These needs transcend health and social care boundaries as well as areas such as
education, housing and environmental health;
Measures to enhance communication and collaboration amongst relevant health service
agencies within public, private and voluntary sectors require careful consideration.
RESEARCH AIM AND OBJECTIVES
iv

The project, lies broadly within the thematic programme entitled; “Improving the Quality of Life
and Management of Living Resources” (1998-2002), for research, technology, development and
demonstration under the European Union’s 5th Framework Programme. The aim was to examine
perceived health and social care needs among informal carers of older people, including mentally
infirm persons and to explore their experiences of home care.
Objectives
To determine the prevalence of informal carers according to their geographical location, in an
urban and a rural community;
1. To conduct a comprehensive exploration of the profile, role and needs of informal carers to
map their experience of caring;
2. To identify coping strategies employed by carers;
3. To explore the positive aspects of the caring role/relationship;
4. To establish carers’ satisfaction in relation to:
(a) Quality of life;
(b) Information needs;
(c) Day care and respite care;
(d) Transport;
(e) Emotional support.
In fulfilling these research objectives, rigorous systematic approaches were undertaken at all
stages of the research process. A mixed methodological approach, including focus groups, a self-
administered questionnaire and in-depth interview techniques were undertaken to optimise the
reliability and validity of the research process.
SUMMARY OF METHODOLOGY
Three focus groups were set up to explore informal carers’ subjectively perceived needs and
experiences of caring for general as well as mentally infirm older persons. The issues arising
from these focus groups influenced the content of the questionnaire;
In order to enhance further the development of the questionnaire, an expert panel was asked to
review the questionnaire prior to its use;
v
A postal survey was used to estimate the number of carers known to public health and community
psychiatric nurses;
A pilot study was undertaken with informal carers in a rural/ urban setting (N=40).
In the main study, the pre-tested questionnaire was distributed to informal carers (N=319).
Participants represented a randomised rural/urban population mix from within the Waterford
community care area of the South Eastern Health Board.
In order to obtain a more in-depth understanding of the experience of care-giving, respondents were
asked if they would be willing to participate in a one-to-one interview aimed at eliciting richer
data. This resulted in interviews with 10 informal carers. The purpose of the semi-structured
interviews was to verify and explore further the variables arising from responses to the
questionnaire.
The subsequent qualitative data were analysed through content analysis techniques. Quantitative
data were analysed using the Statistical Package for Social Sciences, version 9 (SPSS, 1997).
FINDINGS
The reasons underlying service deficits are complex and multifaceted. From the data collected, the
following findings emerged:
No evidence of existing registers of informal carers was found;
Inappropriate assumptions are sometimes made regarding carers’ roles, and responsibilities as
well as their availability and ability to provide care. The importance of needs assessment was
clear;
Health and social care boundaries mitigate against effective service provision;
Collaboration, communication and co-operation between carers and statutory and voluntary
services require considerable improvement;
Services are sometimes inflexible, poorly matched to carers' needs, often only becoming a
priority when a crisis occurs;
Lack of availability and reliability of some support services militates against enabling some
carers to continue in their care-giving role;
Shortages exist in terms of practical support structures and resources. Some services display
poor co-ordination and integration, evidenced by both service omissions and duplication;
vi

There is a significant lack of awareness amongst carers regarding health and social care
supports, benefits and entitlements. There is evidence of inequity and access difficulties for
carers seeking information regarding necessary supportive interventions;
Key aspects of carer-dependent relationships expose a variety of perceptions of informal
care. Misconceptions, pride and a sense of diminished independence amongst older people
can result in poor use of support services. Two-thirds (62.7%) of the sample reported that
they did not receive enough information about the availability of support services;
Almost half the sample surveyed (47.9%) reported care-giving as a twenty four-hour job, 89%
of whom provided care seven days a week. The psychological impact of the care-giving role
was quite profound. As one carer states:
“The stress is that you are twenty-four hours looking after them…it can take so much energy out of you, physically…your mind, body and soul”:
A carer in his late seventies, described the intensity of his role caring for his wife; who was
suffering from Alzheimer’s disease stating
" I have to do everything…all day long, day and night. I can't get a decent sleep. I have to be awake at the drop of a hat”.
There is evidence of considerable bureaucracy in the organisation of some services.
Some carers experience a lack of control or power over their care-giving role, primarily where
statutory bodies fail to consult with carers themselves.
Service delivery standards are highly variable with few accountability measures.
The nature and extent of the carers’ role is sometimes poorly understood. One carer encapsulated its
impact stating:
"Slowly but surely, you see your own physical health and radiance going out of yourself... The spark goes out of you, you just get drained slowly."
This carer went on to state that this was:
"not a complaint…just a plea from the heart of the story of carers".
Many carers do not use respite services, citing reasons such as feelings of guilt or a belief that
existing services were unsuitable to themselves or to the care recipient.
Nonetheless, a quarter (24.5%) of respondents related that they never had a break from their
caregiving role. A further two-thirds (66.7%) reported that they had never been offered respite
care.
vii
RECOMMENDATIONS
Reflecting on a variety of findings from the study, a number of recommendations for policy and
practice emerge as essential prerequisites towards assessing and addressing carers’ needs:
Service Issues
From a service perspective, the findings highlight the importance of developing seamless, co-
ordinated total systems of care aimed at facilitating an appropriate range of services in
response to carers’ continuing health and social care needs. The value of a collaborative
approach inclusive of both health and social care provision is important both at
interdisciplinary and interorganisational levels in securing partnerships between statutory,
private and voluntary agencies;
The anticipated continuing demands for family/voluntary care necessitates the integration of
carers’ needs and perspectives in future service planning and decision-making networks, in
partnership with statutory and voluntary bodies. The importance of co-ordination and
partnerships in this regard cannot be overstated;
The need to develop continually an understanding of the effectiveness of specific health and
social care interventions is of paramount importance;
Clarity and vision in required in relation to needs assessment structures for carers, coupled
with explicit service goals tailored to respond to and meet these needs. Subsequent care plans
must be evaluated and monitored, thereby ensuring that care needs are addressed and met;
Rapid response strategies focusing on individual carers’ needs in changing circumstances
such as increasing levels of dependency, illness or potential crises are essential interventions;
The development of considered, systematic and objective care management practice is essential
in order to accurately assess, monitor and evaluate carers' needs. Any such framework must
take account of individual differences such as individual carers' ability, competency and age; as
well as the dependency level of the dependent person;
Efficient evaluative and quality audit measures must be put in place;
Resource inefficiencies and inadequacies must be suitably redressed;
There is a substantial need for shared information systems across services in order to
establish the ‘true’ prevalence of informal carers and meet assessment, planning, and
operational requirements in a structured, systematic manner;
The reasons underpinning many of the problems identified in the study are multifaceted and
require concerted action in order to identify and respond to gaps across a wide spectrum of
issues in home care provision.
viii

Policy Factors
Meaningful practice and policy changes, directed and informed by current advances in the
evidence-base are required in order to redress service practice divides, thereby creating a more
enabling environment in which local service decisions can be made;
The Department of Health and Children and the Department of Social Community and
Family Affairs should commence information initiatives aimed at enabling carers to access
relevant information regarding a range of support services;
Government departments should make explicit their policies in relation to informal carers.
Such policies must recognise and acknowledge carers as unique individuals with distinct
needs and abilities;
The distribution of resources such as economic supports and allowances warrants review and
policy commitment and requires collaborative, cross-sectoral, co-ordinated planning across
categories such as age, illness and social grouping;
The level of interaction between statutory services and carers requires exploration,
monitoring and evaluation;
In acknowledging carers' needs and experiences, it is important that statutory care agencies
develop new and innovative service plans in response to their continuing health and social
care needs;
Education and training programmes should be established for carers in preparation for the care-
giving role;
User-friendly resource centres for carers should be developed at local level;
A co-ordinator of carer support services should be appointed as a link person between carers
and service providers. Such an advocacy service would increase awareness amongst carers as
to the availability of service entitlements and benefits;
The health and social care boundary must be addressed;
Links must be formed across the totality of health and social care services, towards the
development of more integrated, co-ordinated care pathways for carers;
Such approaches may result in the development of more efficient and effective use of
resources in terms of reducing unnecessary institutionalisation. More importantly, since older
people wish to remain at home for as long as possible, these pathways may enhance the
quality of life of both the carer and the older person.
ix

Recommendations for Further Research
Despite the significance of the current study, further research efforts must be encouraged by
commissioning studies that seek to assess and evaluate care interventions and methods of
service delivery;
Ongoing evaluation is required in order to map the quality and outcomes of support
structures and processes aimed at addressing carers' continuing health and social care needs;
A central priority hinges on the need for community-wide, multidisciplinary, multiagency
research, adopting an integrated, collaborative approach in areas of psychosocial, economic
and social research;
Research efforts beyond task orientated aspects of care-giving are warranted as a means of
exploring the humanistic components inherent in the art of caring;
There is a distinct lack of evaluative data on initiatives in the workplace to support carers;
Longitudinal studies are warranted with regard to the different needs and experiences that
carers hold, focusing on gender variability issues, whether caring on a full time basis, or
combining family caring with formal employment;
There is a growing emphasis on ‘second level’ research exploring what can be learnt from
published studies in specific subject areas. Consequently, aggregate analysis of research
findings may be formulated based on cumulative research evidence;
There is a need for improved identification and tracking measures in order to establish the
'complete' picture as to the prevalence of informal carers. New and innovative research
initiatives, coupled with enhanced levels of cross sectoral communication will be required,
particularly in uncovering 'hidden carers' who may be most in need of support services;
Meta analysis and collaborative, multidisciplinary research studies may produce formulae
that reduce methodological or operational difficulties. Such strategies may provide a wealth
of relevant data to better inform health and social care policy and service developments.
CONCLUSIONS
Caring for older people, particularly mentally infirm persons has been described as a
“…neglected area of health and social care in which there is considerable scope for quality improvement” (pp.x.v, Norman et al 1997).
As advocates for older people and their carers, the Department of Health and Children and the
Department of Social Community and Family Affairs hold a responsibility to monitor service
inputs, care processes and outcomes and identify service gaps and deficiencies. Consequently,
x
reliable and valid information bases are required at local and national levels in order to plan
needs-orientated service interventions based on the nature and extent of the care-giving role.
In the context of carer support services, an overarching belief amongst carers was
“that there should be a concerted policy effort to keep people at home, but people need financial assistance to do that” stressing the need for “surveillance”.
One of the most important factors involved in meeting carers' needs includes the provision of
information, enabling them to seek appropriate help and improve the quality of their lives in
order to care more effectively. The results of the current study constitute an informed
contribution to the evidence base regarding experiences of informal carers of an increasingly
ageing population. Since no contemporary systematic analysis of carers' needs has been
undertaken, it is anticipated that these findings may assist policy makers and service planners to
gain insight into the totality of the care-giving experience. Furthermore, these findings may assist
in informing and empowering the expanding number of informal carers of older people in our
communities.
Key Messages
xi
The national profile of carer issues must be raised.
The issues require comprehensive debate at corporate level.
Service providers must ensure that carer support services are made a priority of community
care strategies.
Community care planning and reshaping must reflect the tenets of the community care
reforms, specifically in terms of adequate support services and resources.
Systematic mapping of levels and patterns of carers' need requires structured assessment.
Community service development plans must detail mechanisms by which these needs can be
met proactively, setting out the resources required.
Ongoing monitoring and review of performance must be undertaken.
Carers must be involved actively in all stages of planning, monitoring and evaluation.
Carer support services must be linked to wider social and public health policies.
Problems regarding the health and social care boundary must be resolved.
Comprehensive health and social care strategies for carer support must embrace practical
developments regarding housing, transport, roads, education, training and safety issues.
xii
Contents Page Page No
Acknowledgements...........................................................................................................ii
Members of the Research Steering Group........................................................................ii
Academic Advisory Team.................................................................................................ii
Executive Summary..........................................................................................................iii
Contents Page....................................................................................................................xiii
List of Tables....................................................................................................................xviii
List of Figures...................................................................................................................xx
List of Appendices............................................................................................................xxi
Chapter One: Background to the Research Project
1.0 Introduction and Background to the Report..........................................................1
1.1 The Scale of Demographics..................................................................................1
1.2 Implications for Health and Socio-economic Policy............................................1
1.3 Community Care Reforms-Policy Contexts.........................................................2
1.4 Quality Issues........................................................................................................3
1.5 Profiling Informal Carers......................................................................................3
1.6 Research Aim........................................................................................................4
1.6.1 Research Objectives.....................................................................................4
1.7 Plan of the Report.................................................................................................4
Chapter Two: Research Evidence: A Review of the Literature
2.0 Introduction...........................................................................................................6
2.1 Operational Definition of Terms...........................................................................6
2.2 The Prevalence of Informal Carers.......................................................................6
2.2.1 The Ageing Profile of Informal Carers........................................................7
2.3 The Nature and Extent of the Care-giving Role....................................................8
2.3.1 The Diversity and Complexity of the Care-giving Role..............................8
2.3.2 Exploring the Care-giving Role...................................................................9
2.4 Responsibilities for Care-giving: Policy Contexts................................................10
2.4.1 Irish Policy Objectives.................................................................................10
2.4.2 Carer Participation and Consultation: The Policy-Practice Divide..............11
2.5 Community Care Policies and the Assessment of Carers’ Needs.........................12
xiii
2.5.1 Identifying Carers’ Needs............................................................................12
2.5.2 Assessment and Planning Procedures..........................................................14
2.6 The Health Profile of Carers.................................................................................15
2.7 Conclusion ...........................................................................................................16
Chapter Three: Methodology/Research Design and Procedures
3.0 Introduction...........................................................................................................18
3.1 Research Design Format.......................................................................................18
3.1.1 Summary of Data Collection Approaches....................................................18
3.2 Qualitative and Quantitative Research Perspectives.............................................19
3.3 Procedures: Methods of Investigation...................................................................19
3.4 Section 1: Focus Group Method...........................................................................19
3.4.1 Sample Selection and Size...........................................................................20
3.4.2 Analysing Focus Group Data.......................................................................21
3.5 Section 2: Pre Tested Questionnaire.....................................................................21
3.5.1 Designing and Developing the Questionnaire..............................................22
3.5.2 The Pilot Study.............................................................................................22
3.5.3 Gaining Access to the Pilot Sample.............................................................23
3.6 The Main Study.....................................................................................................24
3.6.1 Prevalence Data - Establishing the Database...............................................24
3.6.2 Defining Urban and Rural Sampling Frames...............................................24
3.6.3 Small Area Statistics....................................................................................25
3.6.4 The Main Sample.........................................................................................25
3.6.5 The Distribution Strategy.............................................................................26
3.7 Validity and Reliability.........................................................................................27
3.8 Analysis Plan for Questionnaire Data...................................................................28
3.8.1 Statistical Applications................................................................................28
3.9 Section Three: In-Depth Interview Technique......................................................29
3.9.1 The Application of Phenomenological Concepts.........................................29
3.10 Sample Selection: Size and Characteristics..........................................................30
3.11 The Interview Process...........................................................................................30
3.12 Data Production.....................................................................................................30
3.12.1 Data Analysis.............................................................................................31
3.13 Ethical Considerations..............................................................................................31
xiv
Chapter Four: Focus Groups, Presentation of Findings and Discussion of Results
4.0 Introduction...........................................................................................................33
4.1 Encapsulating the Totality of the Care-giving Experience ..................................33
4.2 Responsibilities for Care-giving...........................................................................34
4.2.1 Psychosocial Sequalae: Therapeutic Effects of Focus Groups....................35
4.2.2 General Health Issues...................................................................................35
4.2.3 Dependency and Inter-dependency..............................................................36
4.2.4 Support Systems...........................................................................................37
4.2.5 The Significance of Respite Services...........................................................38
4.3 Economic Issues....................................................................................................39
4.4 Family Dynamics..................................................................................................40
4.5 Service Information for Carers.............................................................................41
4.6 Appraising the Adequacy and Efficacy of Services..............................................42
4.7 Education and Training Issues..............................................................................43
4.8 The Physical Components of Care-giving............................................................44
4.9 The Positive Dimensions of Care-giving..............................................................45
4.10 Conclusion............................................................................................................45
Chapter Five: Presentation of Findings
5.0 Introduction...........................................................................................................46
Section One: Presentation of Questionnaire Data.............................................................46
5.1 Socio-Demographic Details of Carers..................................................................46
5.2 Extent of Care-giving Relationships and Responsibilities....................................48
5.3 Carers in the Formal Workplace...........................................................................52
5.4 Responsibilities for Care-Giving..........................................................................52
5.5 Health Profile of Carers........................................................................................53
5.6 Health Profile and Age of the Care Recipient.......................................................57
5.7 Economic and Practical Assistance with Care-giving..........................................58
5.8 Sources of Information Regarding Support Services............................................61
5.9 Carers’ Interaction with Health Care Professionals..............................................64
5.10 Respite and Day Care Services.............................................................................68
5.11 Factor Analysis: Analysing Scale Reliability.......................................................71
5.11.1 Factor Analysis..........................................................................................71
xv
5.12 Reliability..............................................................................................................72
5.12.1 Validity.......................................................................................................72
5.12.2 The Interrelations of the Concepts.............................................................72
5.13 Hypothesis Testing and Tests of Statistical Significance.....................................73
5.13.1 Hypothesis Testing Related to Social Isolation........................................73
5.13.2 Hypothesis Testing Related to Loss of Control........................................74
Section Two: Results of In-depth Interviews....................................................................79
5.14 Key Recommendations.........................................................................................79
5.14.1 Presentation of Results: Thematic Developments......................................79
5.14.2 Statutory, Professional, Voluntary and Familial Roles.............................80
5.14.3 Family Dynamics......................................................................................81
5.14.4 The Care-giving Environment..................................................................81
5.15 The Nature and Extent of the Care-giving Role....................................................82
5.15.1 Psychological Impact of Care-giving.........................................................83
5.15.2 Socio-Economic Factors............................................................................84
5.15.3 Physical Issues...........................................................................................85
5.15.4 Coping Strategies.......................................................................................86
5.16 Positive Aspects of the Carers Role......................................................................87
5.17 Impressions of the Adequacy and Efficacy of Carer Support Services................88
5.18 Care Planning........................................................................................................91
5.19 Education and Training.........................................................................................92
Chapter Six: Discussion of Results
6.0 Introduction...........................................................................................................93
6.1 Carer Language, Definitions and Interpretations..................................................93
6.2 Exploring the Nature and Extent of Care-giving..................................................93
6.2.1 Needs Assessment, Procedures and Policy..................................................94
6.2.2 Support Services..........................................................................................95
6.2.3 Profiling Carers’ Health...............................................................................97
6.2.4 Health Promotion Factors............................................................................98
6.3 Conclusion............................................................................................................99
xvi
Chapter Seven: Recommendations and Conclusions
7.0 Introduction...........................................................................................................101
7.1 Implications for Service Planning.........................................................................101
7.2 Implications for Policy..........................................................................................102
7.3 Recommendations.................................................................................................103
7.4 Implications for Further Research.........................................................................105
References.........................................................................................................................106
Appendices........................................................................................................................115
xvii
List of Tables
Chapter Two
2.1 Projection of Older People and their Need for Care (‘000)........................................8
Chapter Three
3.1 Main Sample Cohorts..................................................................................................26
Chapter Five
5.1 Carers’ Age.................................................................................................................46
5.2 Identifying Carer / Care Recipient Relationships.......................................................47
5.3 Number of Carers Co-residing with the Older Person................................................47
5.4 The Number of Older People being Cared for by each carer......................................49
5.5 Carers’ Time spent Providing Care Daily...................................................................49
5.6 Overnight Care Provided by Carers............................................................................50
5.7 The Extent of Care-giving as Expressed Weekly.......................................................50
5.8 Number of Carers Spending Time Engaged in Activities of Daily Living.................51
5.9 Carers’ Work Profile...................................................................................................52
5.10 Responsibilities for Care-giving...............................................................................53
5.11 Carers’ perceptions of their Physical and Emotional Health....................................54
5.12 Coping Strategies Adopted by Carers.......................................................................56
5.13 Profiling Carer / Care Recipient Relationships.........................................................57
5.14 Carers Receiving Home Help Expressed in Hours Per Week...................................59
5.15 Carers Receiving Home Care Assistance Expressed in Hours Per Week.................59
5.16 Carers’ Expression of their Need for Access to Support Services............................60
5.17 Sources of Practical Support and Assistance............................................................61
5.18 Sources as Identified as Providing Carers with Enough Information about.............63
Relevant Support Service
5.19 Carers’ Reported Interaction with Health Care Professionals..................................64
5.20 Professionals Carers would like more Support and Advice from.............................66
5.21 Professionals Reported as Providing the most Valuable Contribution to Carers......67
5.22 Carers’ Perceptions of People that are there to listen to them..................................68
5.23 Frequency of Breaks from the Care-giving Role......................................................69
5.24 Respite Services Profiling Carers Perspectives.........................................................70
5.25 Transport Problems Associated with Accessing Support Services...........................70
xviii

5.26 Inter-Item Correlations and their Significance..........................................................73
5.27 Mean Scores and Standard Deviations on Social Isolation.......................................74
5.28 Mean Scores and Standard Deviations on Loss of Control.......................................74
5.29 Descriptives for Loss of Control and Confusion......................................................74
5.30 Anova for Loss of Control and Confusion................................................................75
5.31 Anova Results for Loss of Control and Length of Time Caring...............................75
5.32 Descriptives for Loss of Control...............................................................................76
5.33 Loss of Control and Respite Care.............................................................................76
5.34 Descriptives for Self-Fulfilment and Length of Time since Receiving
a Break......................................................................................................................76
5.35 Mean and S.D. for Self-Fulfilment and Length of Time Since Receiving
a Break......................................................................................................................77
5.36 Social Isolation and the Number of Hours Spent Caring Daily................................77
5.37 Mean and S.D. for Social Isolation and the Number of Hours Spent
Caring Daily..............................................................................................................78
xix

List of Figures
Chapter Five
5.1 The Number of Years Spent Caring......................................................................48
5.2 The Number of Older People Suffering from Periods of Confusion....................57
5.3 The Age of the Care Recipient..............................................................................58
xx

List of Appendices
Chapter Two
2.1 Levels of User Involvement..................................................................................115
Chapter Three
3.1 Topic Guide for Focus Group Interviews.............................................................116
3.2 The Questionnaire.................................................................................................117
3.3 PHN Area and Percentage of Older People in Waterford Community Care
Area.......................................................................................................................130
3.4 Pilot Study: Analysis of Response Rates..............................................................131
3.5 Personalised Letter Accompanying Questionnaire...............................................132
3.6 Letter to PHN’s / CPN’s Accompanying Prevalence Register.............................133
3.7 Prevalence Register: Data Collection Form..........................................................134
3.8 Letter Administered to PHN’s / CPN’s Prior to Conducting Main Study............135
3.9 Profile of Non-Respondents in the Main Study....................................................136
3.10 Audit Trail for In-depth Interviews.......................................................................137
3.11 Proposed Interview Topic Guide..........................................................................138
3.12 Information Letter for In-depth Interview Participants.........................................139
3.13 Consent Form........................................................................................................140
3.14 Ethical Approval for the Study.............................................................................141
3.15 Extract From In-Depth Interview..........................................................................142
Chapter Five
5.1 Social Isolation and Loneliness Factor-Frequency of Constituent
Variables...............................................................................................................145
5.2 Self-Fulfilment Factor-Frequency of Constituent variables.................................146
5.3 Loss of control Factor-Frequency of Constituent variables..................................147
5.4 Factor Loading for Loss of Control......................................................................148
5.5 Factor Loading for Social Isolation and Loneliness.............................................148
5.6 Factor Loading for Self Fulfilment.......................................................................148
5.7 Computation of Factor Scores...............................................................................148
xxi
CHAPTER ONE
1.0 Introduction and Background to the Report
The ageing population within Ireland and the European Union represents a crucial challenge to the
development of appropriate health and social service planning for the 21st Century. Consequently,
increasing numbers of high dependency, frail and disabled older people will require new
interventions and improved health and social care inputs. Similarly, health promotion and health
maintenance initiatives will have to address the needs of healthy older people. Hence, greater
credence has been afforded to the importance of examining appropriate and necessary prerequisites
for efficacious care provision in the community and particularly in the family home. Successful
implementation of community care initiatives remains an integral objective for health and social
care agencies as well as interdepartmental policy makers. This introductory chapter contains a
rationale for this study in the form of an overview of pertinent issues surrounding informal care-
giving for older people with and without mental infirmity.
1.1 The Scale of Demographics
In Ireland, approximately 91% of the population aged 65 years and above, live in the community
in private households, 26% of whom are living alone. Of the 26% that live alone, 31% are
females and 20% are males (The Irish National Council on Ageing and Older People, 1997).
Recent demographic projections in Ireland indicate the number of older people is set to double
between 1996 and 2031, during a period in which the overall State population is expected to
remain stable (C.S.O, 1999). Consequently, the projected population of older people (>65 years)
in 2031 will be approximately 850,000 as compared with the 1996 level of 413,882.
Demographic projections within the European Union also indicate that in the next twenty years
the proportion of older people over 65 years will increase by 17 million, and by 5.5 million in
those aged 80 years and above (Eurostat, 1993). Thus, one third of the total population of Europe
will be over 65 years in 2020.
1.2 Implications for Health and Socio-Economic Policy
Clearly, the implications for both health and social care provision are quite profound. Given the
finite financial resources and gross domestic product allocation, in respect of healthcare funding,
demographic trends will impact on fiscal and healthcare policy formulation. This is particularly
pertinent in a global economic climate emphasising allocative efficiency. The question as to how
1

far demographic and social trends have been factored into the forward projections of government
expenditure, both in general and health service planning is an issue that requires further debate.
The Royal Commission on the Funding of Long-Term Care for the Elderly (DOH, 1999)
recommends:
The redefinition of the health and social care divide;
The establishment of a National Care Commission in order to monitor regulate and
standardise the quality of services and the manner in which care needs are assessed and
delivered for older people.
1.3 Community Care Reforms: Policy Contexts
The importance of finding the correct mix of policy priorities is pertinent to the development of
the 1999 UN theme of a society for all ages. Community care reforms in the U.K. (D.O.H,
1989) and Ireland (D.O.H, 1994) prescribed significant changes in health and social care. These
reforms highlight the importance of targeting services at those with the greatest need. They
include the provision for the needs of carers and interprofessional collaboration and co-
ordination. Central to this initiative is the requirement for individually focused assessment
strategies to establish an accurate profile of carers' requirements. As a result, the Irish
government stated that:
“The development and improvement of services for older people is a Government priority,”(D.O.H.A.C. 1998, p. 29).
The Irish report Shaping a Healthier Future: A Strategy for Effective Healthcare in the 1990's
(D.O.H, 1994) sets out targets acknowledging the need to involve people in taking
responsibility for their own health and securing the environmental support necessary to achieve
health and social gain. However, there is increasing evidence that achievements have fallen
short of aspirations (Benson, 1994, Goodwin, 1997, Ruddle et al 1997, Swanwick and Lawlor,
1998, D.O.H, 1999). According to Bowling (1997), the difficulties at policy level stem from the
relative dearth of research data regarding the appropriateness and efficacy of health and social
care policies. The application of scientific research methods through the systematic and rigorous
collection of data may facilitate assessment with regard to the effectiveness of current health
and social care services. This may lead to the achievement of predefined policy objectives
aimed at enabling and empowering carers to provide acceptable standards of care.
2

1.4 Quality Issues
Recent trends in health service planning foster a ‘predict and manage’ case management
approach (Gaucher and Coffey, 1993). Quality improvement and monitoring are at the forefront
of contemporary health service agenda. Fundamental changes in the structures and processes of
healthcare systems are occurring, including, the emergence of voluntary carers of older persons.
The relationship between formal and informal services is seen as increasingly important. This
represents a fundamental change in the manner in which service needs for older people should
be assessed, planned, organised, delivered, and evaluated in the years ahead. A major effect of
the change has been the paradigm shift from a ‘provider’ to a ‘consumer’ orientation.
Consequently, the prioritisation of appropriate carer-focused /needs-based, services underpinned
the South Eastern Health Boards’ philosophy of care in addressing targeted health service
planning and policy developments.
1.5 Profiling Informal Carers
Informal carers are the primary providers for older people in need of varying degrees of care. “Care
in the community has increasingly come to mean care by the community,” (Nolan and Grant, 1992,
p.44). The extent and nature of their multifaceted roles often exacts a wide range of transformational
changes in carers' lives. These include an array of functional dimensions ranging from
psychological, behavioral and socio-economic adaptations to physical modifications. In the main,
these careers are unpaid and they reduce significantly the potential burden of cost incurred by the
State in respect of care for older people. Caring for an older person over a long time will result in
substantial expenditure on transport, household appliances and adaptations, heating, laundry,
equipment and support services (Glendinning, 1988, Ruddle and O’ Connor, 1994).
Despite the significant contribution of carers to society, the evidence suggests that their unique
needs remain largely ignored (Richardson, 1992, Ruddle et al 1997, Henwood, 1998, Warner and
Wexler, 1998). This was also the conclusion of the report entitled: A Review of The Years
Ahead–A Policy for the Elderly (Ruddle et al 1997). Informal carers also constitute a relatively
hidden part of service provision in the care of the mentally infirm, with little thought being given
to their role (Benson, 1994). Furthermore, International and European research findings indicate
that inadequate attention has been paid to the inclusion of older people and their carers in
decision-making processes (Nolan and Grant, 1989, Ruddle et al 1997, Kellett and Mannion,
1999).
3

1.6 Research Aim
The aim of the study was to examine the substantive subjectively perceived health and social care
needs of informal carers of older people including mentally infirm persons, and to explore their
experiences of home care.
1.6.1 Research Objectives
To determine the prevalence of informal carers according to their geographical location, in an
urban and a rural community in the South East of Ireland;
To conduct a comprehensive exploration of the profile, role and needs of informal carers to map
their experience;
To identify coping strategies employed by carers;
To explore the positive aspects of the caring role / relationship;
To establish carers’ satisfaction in relation to:
(a) Quality of life,
(b) Information needs;
(c) Day care and respite care;
(d) Transport;
(e) Emotional support.
1.7 Plan of the Report
The report contains seven chapters:
Chapter one outlines key issues emerging from the extant literature and includes the
findings from the study.
Chapter two reviews some of the most relevant previous research regarding caring for
older people in home care settings.
Chapter three outlines the research methods, design and data collection procedures. The
rationale for selecting both a quantitative and qualitative approach to the research design
is discussed, indicating why a combination of focus groups, survey and in-depth
interview techniques were considered appropriate to achieve the aim and objectives of the
study.
Chapters four to five relate the study’s findings.
4
Chapter six includes a discussion of these results in the context of existing literature,
identifying key issues drawn together in a conclusion which highlights a number of over-
arching themes.
Chapter seven deals with service, policy and research recommendations.
5
CHAPTER TWO
2.0 Introduction
A systematic comprehensive review of relevant literature in the subject area was derived from a
wide range of electronic and manual sources as well as consultation with multidisciplinary
national and international experts in the field. The databases consulted included: CINAHL,
Medline, Bio Medical, EconLit, PsychLit, Socig, B.I.D.S, O.E.C.D and the W.H.O. These
databases were searched from 1990 to date.
2.1 Operational Definition of Terms
Informal carer is a term used in the International literature by researchers and policymakers,
(D.O.H., 1989, Kane and Penrod, 1993, Nolan et al 1996, Goodwin, 1997). This term is often
used as a means of differentiating voluntary care from that provided by a range of
professionals, commonly known as formal carers. Family caregivers include spouses,
siblings, children, close and distant relatives.
By arbitrary convention, older persons, commonly refers to people 65 years or above.
The term mentally infirm is used to describe persons aged 65 years or above, suffering form a
form of dementia or a degree of functional mental illness (W.H.O., 1993).
2.2 The Prevalence of Informal Carers
In the U.K. the term ‘carer’ entered the political vocabulary in the early 1980s, as the prevalence
of informal carers increased and their support as caregivers became acknowledged publicly
(Benson, 1994). Families have traditionally been the primary care-giving institution worldwide,
generally providing unpaid care on an ongoing full time basis. The family remains the main
arena in which care is given and received across Europe (Twigg and Atkin, 1994, Ruddle and
O’Connor, 1994, Levin, 1997, Wackerbarth, 2000). They provide 80-90% of personal and
instrumental assistance to older people, often serving as the link between the older person and
the formal systems (Walker, 1995). Consequently, less than 5% of older people in Ireland reside
in long-stay institutions (National Council on Ageing and Older People: Ageing in Ireland, Fact
File 1, 1997).
However, according to Giddens, (1998) the extended family has disintegrated somewhat and the
nuclear family is reshaping. The changing structure of the family challenges the very fabric of
6
society, calling into question long held family values, care-giving roles, duties and obligations
(Finch and Mason, 1993). McElwee (1999) depicts the family as a rapidly changing, diverse
social unit that reflects our value system. Some trends indicate that family support for older
people may be declining, suggesting that the needs of older people for care have exceeded the
family’s capacity to meet these needs (Brody, 1995). In the main, one family member takes
responsibility for the care of the older person (Nolan et al 1996) and there is evidence of
resentment amidst informal carers who are unsupported in their role by other family members
(Gilhooly et al 1994).
Research findings indicate that female carers are the predominant care givers (Nolan et al 1996).
In particular, carers of suffers of dementia in Ireland, have been reported as being female in 81%
of cases, 71% of whom were spouses (Ruddle and O’Connor, 1994). In Britain, more women are
caring for aged relatives than for children under 16 years (Brody, 1990). The Irish National
Council for the Elderly (1994) reports that since the initial decline in the birth rate, trends in
Ireland are moving in the same direction. However, the contribution of men to the caring role is
increasingly acknowledged in the literature (Whatmore, 1989, Syron and Keane, 1995).
While there are no current databases detailing the prevalence of informal carers in Ireland,
estimates suggest there are in excess of 100,000 (The National Council on Ageing and Older
People, Fact Sheet 9: 1997). However, previous researchers highlight the fact that prevalence
data is often based on those carers who are already in receipt of formal services (O’Connor et al
1988). Since there may be many ‘hidden carers’ unknown to community care services, the
prevalence of informal care-giving is difficult to ascertain accurately (Goodman, 1986),
particularly in rural areas (O’Connor et al 1988).
2.2.1 The Ageing Profile of Informal Carers
British and Irish surveys highlight the large number of carers who are aged themselves, and
unable to continue in the caring role due to poor health (Blackwell et al 1992; Eurobarometer,
1993;Ironside et al 1997). This supports the findings from American studies that caregivers are
often aged or chronically ill (Stevens et al 1993). Maggs and Laugharne (1996), suggest that life
changes and choices by older carers will add strain to the relationships between them and those
for whom they care. They suggest that health and social services need to work more closely with
carers and older people in order to manage the process of ageing more effectively.
7
2.3 The Nature and Extent of the Care-giving Role
The first attempt to quantify the extent and nature of family caring in Ireland was undertaken by
two research teams (O’ Connor et al 1988, O’ Connor and Ruddle, 1997). These surveys
represent innovative attempts to delineate carers of older people at home from the cared for, as
persons with separate personal needs, experiences and identities.
Despite the projections outlined in Table 2.1, important data as to the profile of people with
moderate or high care dependencies are unavailable. It is also uncertain as to how the level of
physical disability and mental infirmity amongst older persons requiring informal care may be
measured and monitored. This is a matter of some concern for the formulation of future service
plans. Indeed, Nolan et al (1996) argue that in order to shape policy at a macro level, an
empirically generated set of care-giving concepts will be necessary.
Table 2.1 Projections of Older People and Their Need for Care (‘000)
YEAR 1996 2016 2036 2056
>65 Yrs 414 584 908 1,018
Some care 50% 70% 109% 122%
A lot of care 29% 41% 64% 71%
Source: Dept. of Social, Community and Family Affairs, (1998)
2.3.1 The Diversity and Complexity of the Care-giving Role
Recognition of the nature and extent of the needs and experiences of carers of mentally infirm older
persons has resulted in a growing body of research (Coope et al 1995, Zarit et al 1999). Older
people suffering from dementia or Alzheimer’s disease commonly require high levels of
supervision, surveillance and assistance with activities of daily living. Goodwin (1997) expounds
upon this point, suggesting that the reality of informal care-giving is such that it tends to result in
significant levels of stress for caregivers. Graham et al (1997) concur with these assertions and
propose that mental healthcare teams need to evaluate their methods of dissemination of knowledge
to carers, devise educational packages and evaluate their effectiveness.
8

A recent Italian study found that 83% of older persons with some form of cognitive disorder live at
home (Savorani et al 1998). Of these people, 23% live alone and 52% depend on others for support
with activities of daily living. This is compared to 8% of the remaining population. These results
may be reflective of the unique mental health care system in Italy. The researchers analysed 140
family carers used a questionnaire devised by the Italian Association for Research and Assistance
for Dementia (ARAD). This questionnaire was formulated to establish the best approach to improve
quality of life and quality of assistance for the carer-care recipient dyad. Findings showed
behavioural and psychological disturbances of dementia as factors further increasing the
dependency of older people on carers and increasing the carers’ experience of stress. Carers in this
study ranked the most stressful problems arising from the behavioural disturbances of the demented
family member as follows: sleep disturbances, delusions, aggression, agitation and incontinence.
The study identified the need for educational and practical training programmes to improve carers’
quality of life and the quality of assistance afforded to them.
2.3.2 Exploring the Care-giving Experience
The practice of modern healthcare emphasises a holistic perspective, focusing on the human
experience. However, studies in the area of informal care-giving concentrate predominantly on
productive task-oriented components (Kellett and Mannion, 1999). Previous studies have shown
that focusing on tasks and functions alone is simply inadequate. Rather, there is a need to assess the
functional and rational aspects of care-giving so as to predict its effect on personal wellbeing,
lifestyle and behavioural indices (Hermann et al 1993, Waite and Knapman, 1993, Coleman et al
1994, Collins et al 1994, Fink, 1995, Boykin and Winland-Brown, 1995). Therefore, while the
practical elements of care-giving such as, ‘ how to cope’ and ‘ what to do’, are very important, there
is a need to explore conceptualisations of the ‘real’ meaning of family caring. In this way, a deeper
and more meaningful comprehension of what is a multifaceted and complex experience may
emerge.
The literature suggests that little attention has been paid to the rewarding or positive aspects of
caring (Farran et al 1991, Perry, 1995) or the relationships between these aspects (Bulger et al
1993). Much of the extant literature focuses on family ‘burden’, providing a wealth of evidence
of the hardship and health costs that informal carers endure (O’Connor and Ruddle, 1988,
Blackwell et al 1992, Philp et al 1995, Dello Buono et al 1999). Indeed the use of the terms
'need', and ‘burden’ portrays negative stigmatising social constructions (Edmondson, 1997)
9

depicting people in a dependent position and reinforcing the notion that they are problematic
(Caldock, 1994). Doornbos (1996) points out that none of the research studies focusing on the
families of the mentally ill explored family health or family strengths, despite the recognition of
family careers as experts in their relatives’ care management (Harvarth et al 1994).
2.4 Responsibilities for Care-giving: Policy Contexts
It has been suggested that community care policies have shifted the duty and responsibilities for
care from governments to informal caregivers, without the development of appropriate systems
to support and compliment their role (Evers, 1995). This is most evident in older persons who are
also mentally infirm. According to Benson (1994)
“Despite the well documented needs of these families, efforts by policy makers and mental health professionals to provide supportive services to family caregivers, have, until recently, been rare. As a result, many families with mentally ill members have felt virtually abandoned by treatment providers”, (p. 119).
In a recent survey, summarising European policies in relation to supporting family carers, Salvage
(1995) reports that there is no overall policy for supporting family care-giving in Italy. The study
also illuminates a lack of effective policy in the Netherlands, Greece and Spain. In Germany,
limited policies for carers render family members obliged and expected to care without any
remuneration (Pacolet et al 1999). While there are clear indications across Europe that future
Government policies will continue to emphasise enabling older people to remain cared for in their
own homes for as long as possible (Walker et al 1993, Pacolet et al 1999, Dello Buono, 1999), there
is a wide spectrum of differing and opposing views as to the extent to which families should be
expected to care for their aged relatives (Pacolet et al 1999).
2.4.1 Irish Policy Objectives
In Ireland, Government policy continues to place increasing emphasis on maintaining people in
the community, whilst acknowledging the valuable role of carers (Department of Social,
Community and Family Affairs, 1998). The Irish Government’s target, set out in The Strategy
Document is to ensure that at least 90% of persons over 75 years of age live at home (D.O.H,
1994). It highlighted objectives in relation to caring for ill and dependent older people in the
community. These included the maintenance of older people at home in accordance with their
wishes. The strategy also set out to encourage and support the care of older people in their own
community by family, neighbours and voluntary bodies. However, there was no detail as to what
10
services were to be responsible for care and support (Swanwick and Lawlor, 1998). According to
Edmondson (1997)
“Its aims remain in large part aspirational, and exist in a setting of social attitudes to ageing which have not kept pace with contemporary developments in life-course construction”, (p. 161).
Similarly, The Action Programme for the Millennium (DOH, 1997) illustrates the Irish
Government’s commitment to caring for older people, including mentally infirm persons. This
programme includes key priorities such as the provision of higher tax-free allowances for older
people and a new tax allowance for carers. Relaxing the qualifying criteria for the carers’
allowance remains central to increasing its value in real terms. The programme aims to ensure
that health and social services are responsive to carers’ needs providing adequate resources for
respite care. Although there are many complex social realities in relation to health and family
care that are difficult to disentangle, much remains to be done to achieve these objectives.
2.4.2 Carer Participation and Consultation: The Policy-Practice Divide
In Ireland and Europe there is a reorientation towards basing health and social care service
provision on the needs of the population in question (D.O.H, 1989, D.O.H, 1994). Nonetheless,
the absence of coherent policies for caregivers is evident both in the United States (Kane and
Penrod, 1995) and in Britain (Twigg and Atkin, 1994).
Previous studies in Britain (Thornton and Tozer, 1994; Myers and MacDonald, 1996) and
Scotland (Stalker et al 1993) have explored initiatives aimed at consulting with older people and
their carers in strategic planning, assessment and evaluation procedures. Keady and Nolan (1994)
highlight the importance of recognising and valuing the informal caregiver’s expert knowledge
of the care-giving relationship and interfamilial dynamics. Consequently, these authors have
developed the carer-led assessment process (CLASP), which emphasises the expert role of the
carer supported by the enabling role of health care professionals. While such objectives continue
to command widespread support, in practice there is little evidence of a move from prescriptive
to more collaborative care management approaches to defining and addressing carers' needs.
Drawing on interviews from 65 practitioners from four social work departments in Scotland, Myers
and Macdonald (1996) found that the healthcare practitioners' perspectives revealed service gaps
between the 'ideal' of carer empowerment and the 'reality' of everyday practice. This study,
11
undertaken at the Social Work Research Centre at the University of Stirling focused on evaluating
the effectiveness and efficiency of community care processes. The findings indicate that
organisational and resource factors, especially policy and fiscal constraints, are barriers that impede
the progress of carers in the hierarchy of user involvement, particularly at consultative and
empowerment level.
2.5 Community Care Policies and the Assessment of Carers’ Needs
Since 1995, carers in the U.K. have gained a legal right to have their own needs assessed as well as
those of their dependants (D.O.H, 1995). Although informal care-giving is recognised as difficult
and stressful, particularly in relation to mentally infirm persons (Livingstone et al 1996), carers do
not receive a full assessment of their needs (Newens et al 1995). There are methods for functional
assessment of older people to determine the amount and extent of service provision they require.
However, there is no evidence in the literature of a model of assessment to establish whether or not
caregivers possess the necessary skills to provide a multiplicity of care interventions and services. A
key objective embodied in the U.K White Paper Caring for People is that service users and
informal carers should be given a greater individual say in how they live their lives and the services
they need to help them to do so:
“Assessment will need to take account of the support that is available from such carers. They should feel that the overall provision of care is a shared responsibility between them and the statutory authorities and that the relationship between them is one of mutual support” (D.O.H, 1989, p. 28).
More specifically, it refers to the requirement to take account of the wishes of users and their
informal carers and where possible to include their active participation in facilitating flexible
services and consumer choice. User involvement refers to the participation of informal carers as
service users and providers at all levels of service planning and evaluation. Regarding individual
assessment, it relates to the integral role of users and carers as equal partners in the process of
identifying their needs and selecting service measures to meet these needs. Poulton (1997) outlines a
model of user involvement that may be applied to the inclusion of family carers in planning and
evaluating service plans pertaining to the care of older people in the community (Appendix, 2.1).
2.5.1 Identifying Carers’ Needs
Ageing, health and social care requirements are related (Fahey, 1995). In the past decade, the
knowledge base regarding current and future care needs of an ageing population has expanded,
particularly regarding care-giving (George, 1994; Nolan et al 1996). However, despite a
12

significant growth in the academic literature on care-giving and carers’ needs, many gaps
remain, at empirical, rational, and conceptual levels (George, 1994, Kellett and Mannion, 1999,
Zarit et al 1999). A key objective embodied in the White Paper; Caring for People (1989)
emphasises
“The role of an enabling authority is to identify the needs for care among the population it serves, plan how best to meet those needs, set overall strategies, priorities and targets, commission and purchase as well as provide necessary services and ensure their quality and value”(p. 37).
According to Nolan and Grant (1992) carers experience four main types of service need:
Information;
Emotional support;
Skills training;
Regular respite.
The authors suggest that respite services must be in planned in consultation with carers, available
when needed, and acceptable to both the carer and the dependent person. The importance of
obtaining respite care has been detailed in many studies (Nolan et al 1990, Parker, 1997). Mudge
and Ratcliffe (1995) conducted a survey exploring the views of 244 carers in Derbyshire, regarding
the availability of the services they perceived as necessary. This study confirms the importance of
residential and long-term supportive care interventions. These authors suggest that carers were very
keen to put forward their views and propose that more consultative research is necessary in order to
incorporate such perspectives. More recently, The Audit Commission (DOH, 2000) suggests that a
range of high quality support service options should be available to carers.
In a DHSS (1996) survey conducted in Northern Ireland, 42% of respondents reported never having
had a break from the caring role. Of those carers who reported having had a break, 75% of them
stated that another family member provided cover in their absence. Only 10% of carers reported
obtaining respite facilities through statutory or voluntary services. Many carers expressed feelings
of guilt when they suggested respite care to their dependent. In such cases the burden of guilt was
such that respite was just not an option. Only 21% of the carers reported receiving support from
statutory services in the month preceding the study. The uptake of support services was very low,
with only 9% of carers using respite care and 13% using day care services. More than half the carers
in this study reported having no knowledge of financial services or allowances available to them.
Furthermore, carers reported that family and friends were a greater source of information than the
13
media or their family doctor. Many studies suggest a lack of information as the main reason for
non-utilisation of services (Dello Buono et al 1999). Some 70% of carers in the former study
reported feeling isolated in terms of their lack of knowledge regarding available resources, stressing
that they did not obtain enough information on services available to carers. A lack of transport
facilities, predominantly in rural areas was an issue of central concern for carers in the Northern
Ireland study.
Fahey and Murray (1994) report similar findings in an Irish survey where almost 25% of older
people living alone in rural areas had no cars or any access to public transport. The centralisation of
health and public services rendered many of them inaccessible to carers and therefore they were
excluded from some potentially beneficial information and support systems. The authors called for
the planning and implementation of mobile health units for older people in rural areas as an
alternative model of healthcare delivery.
It appears that the uptake of services is just as poor in urban areas. Jennings et al (1997) examined
carers' knowledge, use of and satisfaction with day care services amongst a random sample of 122
informal carers of older people in inner city Dublin. They found that carers continue to shoulder the
considerable ‘burden’ of care. This descriptive study highlights the poor uptake of domiciliary care
and support services by carers and suggests that the care-giving role requires full acknowledgement
by society at large. Furthermore, the study revealed that many carers lacked information and
encouragement to accept domiciliary care where it is needed.
2.5.2 Assessment and Planning Procedures
An official monitoring exercise in the U.K. indicated that in many areas: "assessment procedures
seem to have developed without conceptually clarifying the requirements of assessment of need,"
(Department of Health, 1993 p.5). Previous studies have recommended an individual approach to
carer assessment (Ruddle and O’Connor, 1994, Ironside et al 1997). Twigg and Atkin (1994) assert
that a needs-led assessment assumes that all parties share a clear and unambiguous understanding of
the definition of need. Over the past decade, researchers in the area of family care have highlighted
the importance of developing dynamic assessment structures responsive to carers' needs (Nolan and,
1992, Evers, 1995, Ruddle et al 1997). According to Banks (1999) the sensitivity of the assessment
procedure is central to the implementation of responsive care-giving interventions. Particular
attention should be afforded to the sudden or gradual manner in which carers embark on the care-
14

giving role and the various levels of support that may be required at different points along the care-
giving continuum (DOH, 1999). Community care planning:
“…will be evolutionary. Planning needs to be a dynamic process, tailored to changing circumstances. It should assist health and local authorities as they move towards their role of ‘enabler’, rather than main provider, of all care services. To do this effectively, major providers of care services, service users and their carers, all need to be involved during the planning process” (Department of Health, 1989; p.13).
A British clinical audit on discharge planning between institutional and community nursing services
suggests the need for a thorough review of current policies, procedures and standards (McBride,
1995). Sixty sets of nursing notes were examined, a questionnaire was issued to 27 community
nurses and a total of 60 older people and 26 carers were interviewed. Findings revealed that only
10% of the sample of notes included patient discharge plans that commenced on admission. Most
older people (63%) and carers (81%) reported that neither the carers’ needs or those of the older
person were discussed prior to discharge home. The researchers suggest the establishment of a
multidisciplinary steering group to monitor discharge planning.
Irish and British surveys report that some older people may have to seek institutional care due to
a lack of appropriate supportive services in the community (Blackwell et al 1992; Williams and
Fitton, 1991). The latter researchers indicated that carers' problems often arose as a result of poor
discharge planning, resulting in readmission to hospital. Aside from the principal concerns in
relation to the wellbeing of both the carer and the older person, the potential economic costs and
misuse of funds is a matter of some concern. The researchers recommended that communication
between professionals and informal carers requires substantial improvement. Assessing the
carers' needs prior to discharge of the family member from hospital was proposed. The
researchers in both of these studies suggest failure to adequately recognise carers’ needs has
resulted in care interventions being inappropriate, unavailable or irrelevant. More recently, Zarit
et al (1999) found that carers’ perception of services as inappropriate was a barrier to their
uptake. They suggest that the need to redress this imbalance is the responsibility of the entire
multidisciplinary team as well as the statutory bodies.
2.6 The Health Profile of Carers
A common theme throughout the literature was a sense of loneliness and isolation, linked with
anxiety and depression in caregivers’ lives. The totality of the caring role, and the overwhelming
effect this may have on carers' lives was demonstrated in a study of informal caring in Northern
15
Ireland (DHSS, 1996). For many, caring constituted more than a full-time job with most spending
more than 40 hours a week caring.
Contemporary gerontological policy and practice note that caregiver stress is relieved by
community-based services (Zarit et al 1999). However, there is a dearth of research aimed at
examining the health needs of carers (Sisk, 2000) or determining which interventions are most
effective in alleviating carers’ stress. An American survey of a mixed group of 200 carers of
physically dependent care recipients and those with diagnosed Alzheimer’s disease or related
dementia found that carers’ perception of burden is related to their health related behaviour (Sisk,
2000). The findings suggest that those carers with a lower subjective burden scores engage in more
health promoting behaviours than those with higher subjective burden scores. This supports the
contentions that situational factors such as caregiver burden may affect health promotion (Pender,
1996). Pender suggests that negative perceptions of care-giving may militate against the carers’
ability to participate in various health promoting behaviours. This was also the contention of other
researchers who found that difficulties adjusting to the care-giving role might prevent carers from
attending to their own needs (Graham et al 1997, Hasselkus, 1998). Furthermore, modifying factors
such as the needs of family members, fear and anxiety, lack of knowledge about self-care, disability,
educational level and low income are known to affect health behaviour in a variety of situations
(Miller et al 1995).
British research by Collins and Jones (1997) suggests that carers, particularly spouses of frail older
people at home, experience considerable psychological distress. The researchers conducted a two-
year longitudinal survey of 752 informal carers of frail older people, using semi-structured
interview schedules. The findings suggest the need for greater collaboration between formal and
informal care. This supports the findings of an earlier Irish study (Blackwell et al 1992). Of
particular importance in supporting the health and social wellbeing of older carers and their
dependents is the development of health promotion programmes (The Carnegie Inquiry, 1990). The
inquiry suggests that these programmes need to be applied in association with policies affecting
environmental factors, housing, security, social cohesion and inclusion, accident prevention and
positive mental health.
2.7 Conclusion
16
The absence of rigorous definition means that figures may underestimate the prevalence of carers.
Furthermore, since prevalence data is sometimes incomplete, the ‘true’ extent of informal care-
giving is difficult to estimate. Whilst there are clear indications across Europe that future
Government policies will continue to emphasise enabling older people to remain cared for in their
own homes for as long as possible (Walker et al 1993, Pacolet et al 1999, Dello Buono, 1999), there
is no overall policy for supporting family care-giving. Policy makers sometimes assume that family
members, particularly women, are willing and able to engage in care provision (Banks, 1999, Sisk,
2000). However, socio-demographic changes are impacting upon old age dependency ratios,
influencing demands for ‘long term care’ and the availability of informal carers (Fahey and Murray,
1994, Swanwick and Lawlor, 1998, Department of Social, Community and Family Affairs, 1998).
The importance of empowering carers and developing 'real' partnerships between carers and service
providers has been highlighted (Twigg and Atkins, 1994, DOH, 1999). The provision of
information regarding service availability and eligibility criteria is essential. Previous studies
emphasise the importance of consulting with older people and their carers in strategic planning,
assessment and evaluation procedures (Stalker et al 1993, Keady and Nolan, 1994, Thornton and
Tozer, 1994, Myers and MacDonald, 1996). Contemporary approaches to determining carers’ needs
and experiences are unsystematic, lack monitoring and evaluation and are predominantly
normatively derived without structured consultation with carers themselves. Individually focused
needs assessment strategies are essential in order to establish an accurate profile of carers'
requirements in the determination of appropriate service needs (Twigg and Atkin, 1994, Keady and
Nolan, 1994, Kane and Penrod, 1995, Ruddle et al 1997, D.O.H .2000). The significance of support
and respite has been detailed in many studies (Nolan et al 1990, Mudge and Ratcliffe, 1995, Parker,
1997, DOH, 2000). The need for greater flexibility and scope in the way multidisciplinary
community care teams function in order to invoke more effective and efficient care intervention
measures is evident.
17
CHAPTER THREE
3.0 Introduction
In order to address the research objectives, a systematic and rigorous research approach was
employed, as was a pluralistic approach to data collection. Issues regarding design, sampling,
instrumentation and methods of data analysis are discussed.
3.1 Research Design Format
Firstly, focus group consultations with informal carers were conducted. Emergent themes were
analysed and used subsequently to inform the questionnaire design. A survey approach was
tested in the pilot study, using a triad of distribution strategies aimed at assessing the best
technique for achieving high response rates. In the main study a pre-tested questionnaire,
comprising closed and open questions was used with a stratified, systematically randomised
sample of carers in urban and rural home care settings. Prior to this its validity and reliability
was tested. This was followed up with in-depth interviews. Data were analysed using descriptive
and inferential statistical techniques.
3.1.1 Summary of Data Collection Approaches
1. Three focus groups were set up to explore informal carers’ subjectively perceived needs and
experiences of caring for general as well as mentally infirm older persons. The issues arising
from these focus groups contributed to the formulation of the questionnaire;
2. In order to enhance further the development of the questionnaire, an expert panel were asked
to review it prior to distribution in the main study;
3. A postal survey was also undertaken to estimate the number of carers known to public health
and community psychiatric nurses;
4. A pilot study was undertaken with informal carers in a rural / urban setting (N=40);
5. Using the pre-tested questionnaire, informal carers were surveyed in the main study (N=319).
Participants represented a randomised rural/urban population mix from within the Waterford
community care area of the South Eastern Health Board;
6. To obtain a more in-depth understanding of specific contextual issues related to care-giving,
respondents were asked if they would be willing to participate in a one-to-one interview aimed
at eliciting richer data. This resulted in semi-structured interviews with 10 informal carers. The
purpose of the interviews was to verify and explore further responses to the questionnaire items.
18

3.2 Qualitative and Quantitative Research Perspectives
Researching individual perspectives of care-giving is a complex and arduous exercise,
sometimes fraught with methodological difficulties (Zarit et al 1999). As a result a triangulation
of both quantitative and qualitative research approaches was chosen. Nolan and Behi (1995)
contend that triangulated studies confirm and augment the completeness of the research findings,
and result in richer and deeper research evidence.
Since the mid nineteen-eighties, the value of qualitative methods has received considerable
acknowledgement and recognition in health and social policy research (Denzin and Lincoln,
1994, McKenna, 1997, and Cutcliffe and McKenna, 1999). Qualitative methods have served to
compliment quantitative methods (Tester, 1999). In the present study, the purpose of the
qualitative aspect of the research approach was to describe and interpret the human phenomena
under investigation. One of the central advantages of this approach is the potential to generate
needs assessment data that possess the potential for actionable outcomes.
3.3 Procedures: Methods of Investigation
Three distinct data collection techniques were employed:
Section 1, focus group discussion;
Section 2, pre-tested questionnaire; and
Section 3, interview schedule.
3.4 Section 1: Focus Group Discussion
Kitzinger (1994) defines focus groups as "group discussions organised to explore a specific set
of issues" (p. 103). The focus groups were comprised of carers of older persons with and without
varying degrees of mental infirmity. The purpose of the groups was to gain insight into the ‘felt’
and ‘expressed’ needs and experiences of carers’ of older people in home care settings.
This method is particularly appropriate in population groups who may feel disempowered
(Kitzinger 1994) and provides a safe environment for participants to share their thoughts and
feelings (Kingry et al 1990). Key issues, particularly those of a personal or sensitive nature, are
more likely to be probed successfully in a relaxed research atmosphere (Krueger, 1994). This
technique fosters group synergy and possesses the capacity to gain immediate validation of
information by other group members (Gray-Vickery, 1993). The use and application of the focus
19

group method in gerontological research has been supported because of its potential to gain
insight into participants’: “feelings, opinions, and perceptions about a given problem,
experience, service, programme, or phenomenon” (Gray-Vickery, 1993, p. 27).
The focus group has the potential to bring the researcher closer to the research topic through a
direct and intense encounter with key individuals (Clarke, 1999). However, the breath of
information possible in one group sitting is somewhat limited, despite its inherent content value.
Discussions can be dominated by a couple of people or participants may conform to a perceived
group norm (Macleod et al 1996). Also, data collection and analysis are difficult and time-
consuming. Stewart and Shamdasani (1990) identified three different forms of moderator bias.
Firstly, personal bias may occur whereby comments expressing the moderator’s own points of
view are welcomed. Secondly, the moderator may exhibit an unconscious need to please the
participants. Finally, the moderator may welcome points of view that are internally consistent.
Of particular significance was the fact that data produced in the focus groups facilitated the
development and refinement of the questionnaire, as well as contributing to a theoretical
framework for the study. According to Stewart et al (1990) focus groups are particularly useful
in the development of questionnaires and can be of assistance in establishing the validity of an
instrument. While the researcher in the current study believes that the needs and experiences
detailed by the carers in the focus groups were fairly typical, caution must be taken in
generalising these findings beyond the sample from which they were drawn (Byers and Wilcox,
1991).
3.4.1 Sample Selection and Size
Focus groups usually employ purposive sampling techniques, selecting participants as a group
because of the nature of the research question (Robinson, 1999). Purposive sampling aims to
ascertain insights into the cultural variables of the population and tends to generate rich data.
The focus group sample was accessed following consultation with a combination of statutory and
voluntary agencies. These included a general medical practitioner group, the Waterford Carers
Association, Waterford Community Care and the Waterford Alzheimer’s society. The focus
groups took place between March and May 1999 and were moderated by the researcher. These
groups included a rural and urban mix of informal carers of older people with and without mental
20

infirmity. A total of 17 informal carers were recruited to three focus groups with each group
varying in size from three to eight members.
The ultimate success of data collection often hinges upon careful planning and facilitation
(Roberts, 1997). As a discussion guide, group members were given brief written material on the
research aims and objectives. Topics for inclusion in the discussion were selected based upon
their relevance to the study’s aim and objectives (Appendix 3.1). Discussions began with an
overview of the aim and objectives of the study, followed by general questions. The researcher
probed further with more specific questions until all respondents got an opportunity to express
their views. The sessions ended with a summary of the discussion, seeking verification from the
participants.
3.4.2 Analysing Focus Group Data
The data were transcribed and subsequently analysed by the researcher. Transcriptions were
analysed in accordance with the Framework Analysis approach (Ritchie and Spencer, 1994).
3.5 Section Two: Pre-tested Questionnaire
Ultimately, the choice of one research design over another will depend on the nature of the
phenomena to be investigated, the aim of the research and the amount of the existing knowledge
(Cormack, 1996). The survey approach embodies a non-experimental research strategy focusing
on the retrieval of data on the attitudes, beliefs, preferences and experiences of respondents
through direct questioning of a specific sample (Polit and Hungler, 1991). Within survey design
quantitative and qualitative approaches may be used for the purposes of description, analysis and
comparison (Parahoo, 1994). According to Cormack (1996) the survey design can be applied to
many fields of enquiry and its principles continue to provide an indispensable tool for planners
and policy makers. To address the study’s objectives a questionnaire was employed as a means
of collecting relevant data
Cormack (1996) suggests that compared with interviewer interpretation, questionnaires are less
prone to bias. Nonetheless, the potential for bias is acknowledged; particularly where some
questionnaire items sought to explore the level and quality of interaction between respondents and
health care professionals. Since respondents were aware of attempts to seek their views, the
Hawthorne effect may have modified participants’ responses to questionnaire items. It is further
21
acknowledged that these problems may arise where health care professionals such as public health
nurses distribute and collect the questionnaires. Accepting this, the results from the pilot study
showed that this distribution and collection strategy served to increase response rates and facilitate
access to the target population. Nonetheless, in an attempt to control for bias the questionnaires
were delivered and returned in sealed envelopes and the public health and community psychiatric
nurses were not involved in any other aspect of the study.
There are other problems with the use of questionnaires. For instance, Parahoo (1997) warns that it
may be difficult to ensure that the intended respondent completed the questionnaire and Cormack
(1996) points out that questionnaires may only address the research themes superficially (Cormack,
1996). Consequently, the researchers were aware that the uncritical use of such a technique may
lead to data that provides an incomplete picture of care-giving.
.
3.5.1 Designing and Developing the Questionnaire
The questionnaire approach to collecting data is a simple, rapid and efficient method whereby
relatively vast volumes of data can be obtained from large samples across a wide geographical
area (Sheehan, 1996). In the current study, the questionnaire was designed from the findings
from the literature review, data from the focus group data and expert opinion (Appendix 3.2). An
extensive review of the literature was conducted to ensure the comprehensiveness of each item.
This enhanced its content validity and issues such as sensitivity, appropriateness and
acceptability were given due consideration throughout the entire design. In addition, the content
of the questionnaire reflected the substantive aim and objectives of this study (see Appendix 3.2).
3.5.2 The Pilot Study
The importance of testing all aspects of the questionnaire rigorously as well as potential
distribution formats is a key issue in increasing comprehension or completion (Bell, 1991;
Cormack, 1996). Undertaking a pilot study enhances the quality of the research design since the
feasibility of the planned study, the appropriateness of the instrument, problems with data
collection and analytical strategies can be examined (Richardson, 1994). It assisted in examining
the content and structure of the instrument and in the determination of item clarity and
readability. Furthermore, the questionnaire items were reviewed and amended based on
responses in the pilot study. Amendments were made to items concerning social need, respite
22
service options as well as those relating to psychological disturbances and confusion. These
strategies enhanced the validity of the questionnaire.
3.5.3 Gaining Access to the Pilot Sample
On investigation, no registers of informal carers were found in either the statutory or voluntary
services. Several strategies, such as media advertisements were considered in order to gain
access to the target population. While accessing carers in this way may result in a larger sample,
the nature of such approaches may render the sample over representative in terms of those who
are articulate. Specifically, this may impact negatively upon the opportunity for a wider range of
carers to be selected. Since public health and community psychiatric nurses in the area knew
potential respondents, the researcher sought permission to make contact with carers through
these health care professionals. Billings and Cowley (1995) highlight the potentially vital
position of community nurses in accessing data sources, stating“ has yet to be fully recognised
and taken advantage of”(p.727).
It was intended to select a sample that represented the target population of carers within the South
Eastern Health Board region. Since variations in urban and rural settings, as well as socio-economic
factors may impact upon accessibility to services (D.O.H, 1994), due consideration of geographical
strata differentials was deemed important. Hence, a stratified rural/urban convenience sample of 40
informal carers was selected from the prevalence register detailing carers known to public health
nurses in Area 24, Tramore. The pilot sample was drawn from this area on the basis of its socio-
demographic profile (Appendix 3.3).
In order to explore approaches aimed at enhancing the response rate in the main study, three
different methods of questionnaire distribution were tested. Fifteen questionnaires were posted to
potential respondents for self-completion. For a further fifteen questionnaires, public health
nurses were asked to act as distributors. The remaining ten questionnaires were completed
through face to face interviewing by the researcher. From the high quality of the responses
obtained, it was decided to select the second approach for the main study. An analysis of
response rates is provided in Appendix 3.4.
Burnard and Morrison, (1994) maintain that a full and comprehensive explanation about the
research is likely to encourage people to participate in the study. Therefore, respondents,
23

respondents were well informed and given clear and succinct information. As a means of
introduction, a personalised letter was sent to each potential respondent explaining the purpose of
the study and providing assurances of confidentiality (Appendix 3.5). Only the researcher knew
the encoded names of respondents.
3.6 The Main Study
For the purpose of randomisation a register detailing the prevalence of carers was seen as essential
in order to develop an adequate sampling frame. However, the pilot study showed that no register
of informal carers was found. A prevalence register was set up.
3.6.1 Prevalence Data - Establishing the Database
An outline of public health nursing areas and the percentages of older people in these areas are
included in Appendix 3.3. Letters and prevalence data forms were sent to all 28 public health nurses
as well as the 5 community psychiatric nurses (Appendices 3.6 and 3.7). The prevalence register was
closed three months after the initial written contact in order to commence the process of
randomisation and selection of potential respondents. The total number of informal carers identified
by public health nurses and community psychiatric nurses amounted to 566 and 44 persons
respectively representing a total of 610 informal carers on the prevalence register.
Whilst the prevalence data obtained is clearly incomplete, it represents a ‘snapshot’ of the extent of
informal care-giving within the overall Waterford community care area. Nonetheless, the ‘true’ extent
of informal care-giving is difficult to project, not least because of a paucity of documentation but also
because many carers do not link with statutory or voluntary health care organisations. Consequently,
health or social care providers may not know of their existence. Furthermore, tracking non-
respondents in the pilot study revealed that some potential respondents do not identify themselves as
informal carers. Thus, the process of attempting to ascertain an accurate picture of the prevalence of
informal careers of older people in a given demographic area was exceedingly difficult.
3.6.2 Defining Urban and Rural Sampling Frames
Since community healthcare areas do not always correspond to the District Electoral Division,
(D.E.D.) it was not possible to structure the geographical areas in this way. Furthermore, because
the distribution of carers recorded on the prevalence register was found to be disproportionate
24
across D.E.Ds, it was not possible to randomise the sample solely on the basis of D.E.D.
location.
The most recent comprehensive review of rural / urban areas was carried out as part of the
processing phase of the 1996 census (C.S.O, 1996). It is acknowledged that a further limitation
of determining urban and rural areas from census data is that there may be differences depending
on the location of a specific area from the centre point of the area. This may impact further on
proximity to services, despite the classification of an area as rural or urban. In order to augment
the accuracy of the reporting of areas as urban or rural for the stratification process, personal
communication was made with the relevant planning authorities and county councils. This was
also considered to be important in the light of the changing geographical profiles in Ireland,
arising from urbanisation and the demise of rural Ireland. Indeed, the scale of development is
such that some areas need ongoing reclassification (Sinclair, 1999).
3.6.3 Small Area Statistics
Many questions concerning health status, population needs, healthcare delivery and use are
sensitive to both scale and location (Sinclair, 1999). Since many healthcare issues are addressed
at relatively high levels of aggregation, for example at national and health board level, any
significant variations between different regions may be hidden. Interestingly, the Department of
Health’s strategy document (1994) acknowledged this phenomenon and reported that: “pilot
work on local information systems has proven that there can be significant variations in health
needs within relatively small areas”(p. 24).
According to Sinclair (1999), area based measures of deprivation are invaluable tools in
examining differentials related to issues such as mortality and health service use by small area.
Such measures are potentially useful in identifying specific areas of need for priority funding,
health promotion and service development. The application of a needs-orientated approach based
on the analysis of small area data may harvest the best interests of a particular population group.
3.6.4 The Main Sample
In order to achieve representativeness, the main study sample was selected via a process of
systematic randomisation. Parahoo, (1997) illustrates how every nth number on a list may be
chosen until the required sample is reached. Thus, within the sampling frame every carer on the
25
frame had an equal chance of being selected. Consequently, the sample was stratified into
categories of carers of older people with and without mental infirmity. A further stratification
related to rurality or urbanisation.
The total number of general category carers as outlined above amounted to 566 persons.
Concurrent with standard research practice, those carers included in the pilot study were
excluded from the main study. Thus, the total number of general category carers included in the
randomisation process was 526. Prior to the stratification, the 44 carers of mentally infirm
persons, identified by community psychiatric nurses were combined with the general categories
of urban and rural carers. On analysis, the numbers of informal carers submitted by public health
nurses and community psychiatric nurses was geographically disproportionate, since a greater
proportion of carers were drawn from rural areas. However, it was difficult to avoid this due to
the reliance on these professionals in obtaining the sample. Following urban/rural stratification,
four cohorts emerged where the total sample was N=319. The final breakdown of carer
categories included in the main study is set out in Table 3.1 below.
Table 3.1 Main Sample Cohorts
Category of Carer Numbers Randomised
Percentage of Sample
1 General carers in urban areas n=141 43.9% (44%)
2 General carers in rural areas n =178 55.6% (56%)
3 Carers of mentally infirm persons in rural areas n=11 3.44 %(3.4%)4 Carers of mentally infirm persons in urban
areasn=15 4.70% (4.7%)
3.6.5 The Distribution Strategy
Since it proved to be the most effective and efficient distribution strategy in the pilot study,
public health and community psychiatric nurses were selected to distribute and collect the
questionnaires. A personalised letter was sent to each public health and community psychiatric
nurse (Appendix 3.8). Individual personal contact was also maintained throughout the research
process.
26
It was acknowledged that while many of the respondents may have a willingness to respond to
the questions, they were often aged themselves. These factors coupled with the demands of the
care-giving role may reduce the potential response rate or the level of completed responses.
Where possible a log of returns was held in order to track and obtain a profile of non-respondents
(Appendix 3.9). On tracking initial non-returns, 5 carers stated that despite their interest in
participating in the study they could not do so due to literacy/ writing difficulties. Following
informed consent, face-to-face administration of the questionnaire occurred in these cases.
3.7 Validity and Reliability
The psychometric properties of the questionnaire were tested in terms of two essential criterion,
validity and reliability. Validity means that the questionnaire measures what it is intended to
measure, while reliability means that it does so consistently (Polit and Hungler, 1991). Face
validity, was tested to establish whether or not the questionnaire appeared to measure the
appropriate constructs. The appropriateness of each item in the questionnaire was assessed, and
items unrelated to the characteristics under investigation removed. Content validity pertaining to
the questionnaire items was sought from a panel of experts who had researched and published
internationally in the subject area. Subjecting the instrument to the scrutiny of such experts is a
measure of considerable worth (Burns and Grove, 1987).
Key aspects regarding the reliability of a questionnaire relate to its consistency, dependability and
stability as a measuring tool. The stability of a measure relates to:“the extent to which the same
results are achieved following repeated administrations of the instrument” (Polit and Hungler,
1991, p. 412). In this way, reliability focuses upon the instrument’s susceptibility to extraneous
factors from one administration to the next. The reliability of the questionnaire as a data collecting
instrument, is a criterion of immense importance in assessing its adequacy and quality. The extent to
which the questionnaire scores are free from measurement error is a measure of its external
reliability (Sternberg, 1993). External reliability was examined at the item level, through the test-
retest process. At time one, (T1) and time two, (T2) (two week interval) the same questionnaire was
administered to selected respondents in the pilot study. Interestingly, the reliability co-efficient for
these variables was at the 0.01 level; with a significance level of 0.883 at post-test. This high
correlation indicated a favourable degree of reliability, supporting the consistency and value of the
questionnaire as an appropriate data collection tool.
27

The internal reliability of the questionnaire was estimated in terms of its repeatability and
consistency as an empirical measure by the application of Cronbachs' alpha procedure (Cronbach,
1951). Coefficients, detailing computations of factor scores were used a measure of equivalence. In
the current study, Cronbachs' alpha was greater than 0.70 indicating a high level of internal
consistency (Polit and Hungler, 1991).
3.8 Analysis Plan for Questionnaire Data
According to Parahoo (1994), questionnaires may provide a most reliable method of data collection
since all respondents are asked the same standardised questions. Before engaging in the data
analysis process, data were checked, cleaned, screened for mistakes and missing items in line with
recommended good practice (Polit and Hungler, 1991). Individual carers served as the unit of
analysis. Descriptive and inferential statistics were used to describe and analyse relevant data
generated from the collated questionnaire data. Though largely a quantitative instrument, analysis of
the qualitative aspects of the questionnaire involved a process of making sense of the findings. This
qualitative element served to strengthen and augment quantitative findings.
3.8.1 Statistical Applications
All questionnaire items were coded and the results in relation to each variable were analysed using
the Statistical Package for Social Sciences Windows, version 9 (SPSS, 1997). Tables of frequency,
bar and pie charts were used to illustrate relevant descriptive data. The valid percent is a measure of
all valid responses expressed in tables since this figure takes account of responses coded as non-
applicable or missing. Where results do not equate to 100% (N=215) this was due to rounding,
multiple answers, non-applicable or missing data. As stated above in 3.9, a statistical profile of
significant bivariate correlations was conducted on the test-retest data generated in the pilot study.
Bivariate analysis of questionnaire items was applied to explore relationships between variables as
part of the test-retest process. Statistical significance was generally accepted at 0.05%. On test-
retest, Spearmans’ correlation coefficients (two-tailed) were computed between the variables to test
the relationship between them. These findings verify the stability of the instrument with acceptable
test-retest data, 0.05% internal consistency reliabilities and comparable patterns of significance.
Since reliability co-efficients produced values 0.01, the difference between the two sets of data
(T1 and T2) could have occurred by chance only one in a hundred times.
28
Additionally, 20 Likert scale items, presented in section three of the questionnaire, were factor
analysed using maximum likelihood estimates with Equamax rotation. Assumptions for
parametric tests were met since the distribution of scores for each subscale was approximately
normal, involved the estimation of at least one parameter and lay at the interval scale of
measurement. Parametric statistical tests using t-tests and Anova were used.
3.9 Section Three: In-Depth Interview Technique
This qualitative approach to investigating carers’ perceptions of their needs and experiences, and
the meaning they attach to their personal situations, have been described in research literature as:
“a promising area of research” (Rose 1996, p.73). The rationale underpinning the use of in-
depth interviews was based on eliciting the carers’ perspective of contextual phenomena of
interest. Empirical literature reviewed in chapter two illustrates clearly the dilemma regarding
the application of appropriate research methods to the study of informal care-giving. Such
research challenges prompted the application of a qualitative method underpinned by the
phenomenological approach.
3.9.1 The Application of Phenomenological Concepts
A central premise of hermeneutic phenomenological inquiry lies in the search for deeper
meaning, understanding and insight into human experience (Robertson-Malt, 1999). This
qualitative approach emphasises subjectivity and values experiences as a route to theory
development. In-depth interviews grounded in phenomenology were particularly appropriate for
gaining a more comprehensive and explicit picture of carers’ personal experiences. In this way, it
was possible to augment and build upon the questionnaire data, journeying from general to more
specific experiences. The narrative method is akin to storytelling. According to Tilley et al
(1999)“ a story framework can help researchers to reflect on a process of social scientific
investigation, and to consider how to ‘go on’ in that process, (p.1221)”.
Consequently, there is considerable potential in delving beneath the surface responses explored
in the questionnaire, in order to elicit ‘true’ meaning in complex issues pertaining to attitudes,
behaviour and experiences. Issues can be probed, answered and clarified in an open non-
directive relaxed atmosphere. Furthermore, this approach enhances the rigorous nature of the
data collection process in its totality thereby authenticating the veracity of the findings.
29
3.10Sample Selection: Size and Characteristics
A sample of carers were selected on a voluntary basis, from those respondents to the
questionnaire who indicated a wish to share their personal needs and experiences in a more
detailed format. Since they had already taken part in the completion of the questionnaire, this
sample was relatively easy to recruit, near at hand and likely to respond. Out of the total sample,
51.7% (N=111) volunteered to partake in further research and were therefore systematically
randomised. Upon interviewing, the optimum sample size was reached when data saturation
occurred after 10 interviews.
3.11 The Interview Process
In narration the story is created during the interview (Sandleowski, 1991). Respondents were
reminded of the aim of the study, and the process whereby their names were selected. An audit
trail detailing how the interview guide was formulated is presented in Appendix 3.10. A sample
topic guide regarding phenomena of interest was developed from a data matrix drawn from focus
group and survey data as well as evidence from the extant literature. Subsequently, participants
were contacted in writing and consulted with regard to the relevance of suggested items in the
topic guide. Additionally, respondents were asked to suggest relevant topics for inclusion in the
interview schedule. The timeframe for interviews ranged between 1-1.5 hours. From the pilot
study, it was felt that this was long enough to afford the carer the opportunity to share their
experiences with the researcher. Attention was also paid to linguistic and extra-linguistic
behaviour, elements of ‘paralanguage’, voice inflection and quality, silences and body language.
The quality of the interview is highly dependent on interview/respondent rapport. The
researchers were aware that what people ‘say’ is not always what people ‘ do’. Furthermore,
respondents’ deliberate social desirability bias may limit the credibility of the data (Bowling,
1997). Yet, another weakness of this method is the effect the researcher may have in the
interview situation Therefore, questions must be asked in a non-biasing and non-leading way,
through the use of neutral probes (Bowling, 1997).
3.12 Data Production
The choice of the narrative method provided the study with rich material for analysis. The in-
depth interviews yielded vivid comprehensive data illustrating the meaning that carers attributed
to a wide range of complex issues. The stories, derived from carers’ experiences were coloured
30
by personal attitudes, beliefs, values and perceptions. In the main, the data stemmed from the
topic guide provided to all participants (Appendix 3.11). These guides accompanied by
explanatory letters (Appendix 3.12.) were posted to all participants two weeks before the
interview process.
3.12.1 Data Analysis
Analysis of the qualitative data was related to findings arising from quantitative data analysis.
Von Post and Eriksson (1999) suggest that the relevance of a story lies within the potential of the
narrative language to portray a certain understanding of reality. Data were analysed using the
framework analysis format detailed in the genesis of focus group data (see 3.6). However, there
are potential pitfalls to be avoided when analysing qualitative data. Member checks were
performed with interviewees to verify the researchers’ interpretation of responses obtained in the
interviews. Furthermore, in-depth interviews are only feasible with small numbers and therefore
possess limited representativeness. The process is also labour intensive, time consuming and
expensive.
3.13 Ethical Considerations
Ethical standards were adhered to throughout this research project. Issues of importance
including beneficence, sensitivity, human dignity, human justice and respect for persons
permeated all aspects of the research process (Polit and Hungler, 1991; Cormack, 1996, Parahoo,
1997). Written consent was obtained from respondents (Appendix 3.13) and explicit assurance
was given in relation to their right to withdraw from the process at any time. The application of
ethical principles was outlined in the letters sent to respondents prior to the commencement of
the study. In addition to the personalised letters, the researcher set out a weekly timeframe during
which potential respondents were invited to seek any information or assistance if required.
Ethical approval for the study was sought and obtained from both the South Eastern Health
Board and University of Ulster (Appendix 3.14).
Respondents have the right to expect that any information they provide will be treated in
confidence (Bell, 1991). Therefore, issues regarding privacy, confidentiality, and the disclosure
of potentially sensitive information were discussed with individual carers prior to
commencement of the interviews. The anonymity of respondents was protected and maintained
by the allocation of a respondent number. However, the nature of the interview or focus group
approach is such that true anonymity cannot be assured.
31

Parahoo (1997) cautions that a one-to-one interview may have the effect of altering participants’
perspectives and raising their expectations (Parahoo, 1997). In the present study, carers spoke
openly and freely about intimate issues and experiences of care-giving. The course of this
interaction may be evidenced in the audiotapes and transcripts (Appendix 3.15). The need to be
sensitive to participants' feelings both during and following completion of the interview process
is important (Smith, 1995). The responsibilities of the researcher extended to providing comfort,
support and advise (Reed and Proctor, 1995). This is particularly relevant where the researcher is
a nurse.
Three £50 prizes were offered in a raffle to respondents as a token of gratitude for completing
the questionnaire. It was thought that this might also enhance the response rate.
32

CHAPTER FOUR
4.0 Introduction
This chapter includes a presentation and discussion of the findings of the focus groups, outlined
in chapter three. Overall themes identified focused on carers needs and experiences, attitudes
and perceptions, levels of user involvement and appraisal of service adequacy and efficacy.
4.1 Encapsulating the Totality of the Care-Giving Experience
Participants in the course of all three focus groups cogently expressed the totality of the caring
role and the overwhelming effects this may have on carers’ lives. One carer in focus group one
FG 1, described her role as "a labour of love " which was "constant" in nature, stating that:
"It never goes out of your mind, you never sleep, you never relax.”
Another carer in his late seventies in FG3, described the intensity of his role in caring for his
wife; who was suffering from Alzheimer’s’ disease:
" I have to do everything…all day long, day and night. I can't get a decent sleep. I have to
be awake at the drop of a hat. She gets out of bed and she roams around. In case she goes
astray in the night, I have to be there ".
A participant in FG1, who was caring for her mother with Alzheimer's disease, summed up the
impact of cognitive and behavioural changes on their relationship:
"The saddest thing about it is that a mother that you've loved to bits all your life and …
because you're the one spending so much time with her, you are ending up at
loggerheads, because there's great personality changes…it's not the person there
anymore and you are not the person you were anymore, because you never argue with
your mother, but patience runs out and you are pushed to the max”.
Previous studies identified the correlation between the degree of carer stress and strain and
deterioration in the care recipients’ state (Livingstone et al 1996). Clearly, the intensity and
33
duration of psychological strain are closely linked with an individual’s ability to cope with
inordinate emotional stress.
4.2 Responsibilities for Care-giving
In the current study, carers across all focus groups felt that ultimately the burden of responsibility
for caring lay with the family, primarily female members. A carer in FG1 illustrated this point
stating:
"it is the families responsibility up to a point, but I mean there has to be some help lined
out".
Yet another participant in this focus group was annoyed with what she perceived as the
inadequacy of the statutory services stating:
“They [the statutory services] want to put more care on the family, and yet there is no
facilities there for the family…the government have to take some responsibility, they have
to help out.”
A carer in FG2 highlighted the fact that in many cases the families are no longer available or
willing in some instances; to provide care and stated:
“They do stress all the time on the family, they do say they have to be there, and they are
not there.”
Another young carer in FG1, proposed that informal care-giving should be called 'payback time',
commenting that:
"Your parents gave everything for you and I think in turn all the family should pull
together. I think that would make it easier".
There is certainly previous evidence reporting that family support for older people remains as
strong and as effective as ever (Sundstrom, 1994). In the current study, the loyalty and
compassion expressed by many carers for the older persons in their care was quite remarkable,
34
with many examples of utter selflessness and dedication to their caring role. One carer in FG3,
summed up her commitment to caring for her mother as follows:
"I'd be very reluctant to let her into a home, it would have to come to the stage that
literally my health would go".
4.2.1 Psychosocial Sequalae: Therapeutic Effects of Focus Groups
Previous researchers have noted the therapeutic element of focus groups (Gale, 1992). A
considerable number of participants commented on the supportive nature of the focus groups and
suggested that it would be useful:
"if there was more meetings, just meetings to share with one another,"FG3.
Many of the participants thanked the researcher for affording them the opportunity to express
their experiences and difficulties through interaction with other carers. Some of the carers
exchanged information and advice. One carer in FG3, suggested:
"We should set up our own support, so that someone could step in and take the strain".
4.2.2 General Health Issues
A significant proportion of participants asserted that their personal health and social wellbeing
had deteriorated as a direct result of the care-giving experience. One carer in FG1, summed up
the these changes as follows:
"Slowly but surely, you see your own physical health and radiance going out of yourself,
which is minor, but it is probably major to maybe your husband. The spark goes out of
you, you just get drained slowly."
This carer went on to state that this comment was "not a complaint…just a plea from the heart of
the story of carers".
Carers described changes in their psychological health as being considerably more profound than
any other aspect of their overall health. Previous research evidence suggests that carers,
35

particularly spouses of frail older people at home experience considerable psychological distress
(Buck et al 1997). A participant in his seventies, in FG3, described the impact of stress and
sleeplessness stating how:
"There is only so much that you can take…there are times when people will snap…as you
get older what tolerance do you have to deal with problems like that...up all night.
Sometimes I blow up and let off steam. I hate to say it but sometimes I really blow up on
her…. You can only take so much. You can't be the nice fella the whole time, there is no
way, no way. "
A fellow carer, also within FG3; concurred with these experiences, suggesting that:
"It’s stress, that's what it is, you can't cope…. and it's day and night, every day and every
night for years, you know. "
In the same way, a daughter in FG1 caring for her mother with Alzheimer's disease, related how
the intensity of her role was such that she had a baby monitor plugged in all the time, and made
the following comments
"It nearly drove me mad. She'd call me every night at the same time, it was the confusion,
the head swinging and the face snapping and glaring. The same thing night in, night out.
You just end up cracking up yourself".
4.2.3 Dependency and Interdependency
A considerable number of carers expressed feelings of guilt regarding respite care intimating that
respite services were just not an option. A carer in FG2, explained that when she did go on a
holiday after caring for her mother for almost twenty years, she received phone calls from her
mother where
“she was giving out, saying that she was getting depressed, I should have stayed at
home”.
36
One woman in FG1, who was caring for her highly dependent mother, illustrated the extent of
her sense of responsibility for her mother; explained how leaving her mother in a respite service
left her feeling that she had abandoned her stating how
“People try to say to switch off, but how do you leave somebody you have loved all your
life? I just couldn’t turn my back on her .”
4.2.4 Support Systems
In the present study, there were many references to carers reliance on informal supports,
primarily family, friends and voluntary agencies. In some instances, this was due to a lack of
awareness and information among carers regarding accessing and obtaining essential services, as
well as dependency factors that rendered the care recipient unwilling to avail of services.
Previous researchers have identified the need to evaluate methods of dissemination of knowledge
to carers and evaluate their effectiveness (Coope et al 1995, Graham et al 1997). A participant in
FG2 emphasised the need for "a home help- you need backup."
Groups felt that in order to enable the valuable work of the voluntary agencies to be extended
and expanded, the government should provide support and assistance.
As one carer in FG3 put it:
"The real big help is the day-care…it's a help, brilliant. Extend the day care if it's
possible".
All the carers in FG3 praised the work of the Alzheimer’s’ day care services as a source of
respite care, information and education. Previous studies, found that carers of older people
suffering from dementia made significantly greater use of day-care services (Philp et al 1995).
They were also the most knowledgeable when compared with carers that had been in contact
with statutory mental health services and those who had no prior contact with any care agency
(Graham et al 1997) One aged carer, in FG3 commented that:
"It is a blessing when they come along with the van [The Alzheimer's Association] and
take her off. The minute they are gone I go back up and lie down for another two hours
and I get a peaceful sleep."
37
4.2.5 The Significance of Respite Services
Interestingly, psychological sequalae and the need for day-care and respite services were found
to be interlinked in the current study. As one carer in FG1explained:
"Now the respite help is being offered to us this year, and we’re going to whether we
want to or not, we have to take it because we just can't cope any longer. Were going to
take it because we are at the end of our tether".
However, this carer expressed a common phenomenon amongst other focus group members
pertaining to feelings of guilt regarding accepting respite care:
"We were just thinking, you see if she dies, you see it never goes away, after all our care
to try and keep her happy that if she got in such a state and died, we would never forgive
ourselves and that's the other end of it. You spend your whole life giving and then will
you spend your whole life if she died in that situation bearing guilt like”
Another carer in FG1, caring for her blind mother with Alzheimer’s disease emphasised her
plight in quite profound terms stating that:
“There is a definite need for a break for people. You have to be a prisoner in your own
home, day and night and you cannot leave until somebody comes to relieve you. I don’t
really think that if you are to live a normal life at all, you could be expected to exist like
that whether you are 70, 35 or whatever. You had to get out the door and go because that
was like your freedom. It's’ like leaving a bird out of the cage.”
A daughter caring for her frail aged mother, in FG3 echoed the need for support to combat an
intense sense of isolation stressing that:
“You need to have somebody in the house with you. To be there, to help you along the
way. Even if you had somebody coming in for a few hours a day. You are so alone.”
A daughter caring for her frail aged mother summed up the benefits of the carer obtaining some
form of respite:
38
"The more breaks you get, the more stamina and the fresher outlook on the whole thing,
to go back to a person and be fresh…if it's just ongoing it's, you're dragged down."
4.3 Economic Issues
Numerous carers believed that the benefits and allowances available were grossly inadequate to
cover the underestimated economic costs of caring for an older person. A considerable lack of
awareness and knowledge of financial benefits and entitlements was evidenced across all focus
groups. One aged carer, who had been caring for his wife for many years, referred to the carers
allowance stating:
"I never heard that word said, I don't know nothing about that."
A common experience that emerged across all the discussion groups was a scenario whereby
carers often obtained information regarding benefits such as the carers allowance by chance or
on the advise of a fellow carer, friend or family member. A carer in FG1, caring for her mother
stated that:
"There shouldn't be such a tight reign on the carers allowance because it would enable
you to pay some help as well…it's costing a lot , heating is a major problem with an old
person. If you were getting a carers allowance, you could say, well I could put that to
some paid help."
A carer in FG2 described how her employment opportunities had been curtailed since engaging
in caring for her mother stating she
“…was working full time, but now I have had to cut my work down to two days".
This highlights the potential impact that such issues may exact on the carers’ economic status,
social life, emotional wellbeing and overall quality of life.
39

4.4 Family Dynamics
Many carers referred to the fact that the caring role was often left to one member of the family,
often a female carer. A carer in FG1, explained how although there were ten siblings in her
family:
"It just doesn't work out that way when it comes to helping. People switch off. It's a
terrible strain when it comes to one person", unfortunately, you are let down by family
members, who won't give the time or the money".
Another participant in this group concurred with these assertions stating:
"It is always left to one at the end".
A carer in FG1, caring for her mother who was suffering from Alzheimer's disease explained the
impact multiple caring roles:
"I don't think for a person with their husband and child, I really don't think it's possible
to include an aged parent that is in that condition without something snapping
somewhere".
Furthermore, a carer in FG2 caring for her school-going children as well as her frail father stated
that her role in caring for her father
"...does affect the whole family ".
This point emphasises the importance of considering the rational elements of care-giving as well
as the inherent tasks, in order to hear and understand carers concerns (Kellett, 1996). As one
carer in FG2 put it:
"It is not only what you are doing, take time and listen to them, because they really want
to talk".
This finding was echoed by other group members and across other focus groups.
40

4.5 Service Information for Carers
Some carers related feeling of frustration and hopelessness in relation to attempting to access and
receive services. A carer in FG2 who was caring for her father following a stroke stated:
"…that no one gives you any information for one thing", even if you are entitled to
something, you have to go through so much I’d say to even get something.”
A fellow carer in the same focus group proclaimed that:
“If you don't know what you're entitled to, you have no hope at all of getting it", adding
that:" there should be an information leaflet for everybody caring for the aged."
Similarly, carers across other groups reported that they often did not know who to ask or what to
ask for. A previous longitudinal study of carers of demented and non-demented older people
found that they needed to be facilitated in seeking help and support (Gafstrom and Winblad,
1995). A recent Irish study, Jennings et al (1997) identified the need for primary healthcare
practitioners to become more active in their role as informants and facilitators of support services
for carers.
A carer in FG3 suggested that:
"The Health Board need to promote themselves, their information, I mean they’re a
Government body and should be either going through Eirtell on the television and the
media, there should be publications, they have books out there, there should be somebody
there, if you have a problem, that you could go and sit down and talk to them".
4.6 Appraising the Adequacy and Efficacy of Services
McBride (1995) highlighted the importance of standards of care in discharge planning between
institutional and community nursing services. A carer in FG3, contended that:
"The government doesn't seem to care. They are not providing enough. There would
want to be more and more people in the Health Board."
41
Carers, across different focus groups; described the management of services for carers as a
process of "crisis management" arising from restrictive eligibility criteria. A participant in FG3,
caring for his wife who was suffering from Alzheimer's disease, emphasised that in order to get
any help:
" the situation has to reach crisis, that's the main thing, that would be my gripe at the
moment".
Previous studies report a tendency amongst carers to only seek supportive services when they are
unavailable to continue care-giving or can no longer sustain the strain of care provision
(Nankervis et al 1997, Dello Buono et al 1999). Indeed, a carer in FG3, described the plight of
her mother who was looking after her father, and stressed the reactive nature of community
statutory service interventions, stating:
"When my mother got sick…then the nurse came, and then they got her home help,
somebody to come in and bath my father, twice a week, but she [the main carer] had to
get sick before that happened, that is the biggest point that I want to make, we will have
all sorts of problems then because we will have two sick people".
A carer referring to the need to assess the carer proposed that:
"The whole situation should change, people should be coming to the house, they should
be checking on the carers as well as the patient you know…see how the carer is doing,
what needs to be done from here, what is going to need to be done in two months time.
They should take into consideration their age, what are they on, how are they going. They
are no longer young".
Another carer in FG3 referred specifically to the need for service monitoring, suggesting the
importance of statutory service providers:
"Who look at the need of people and not just now, but in six months time… Can they
[carers] manage in six months time, in twelve months time, what is the situation going to
be and give the feedback to someone…they should know the duration of the patient and
start preparing the family then for what's coming, not waiting 'till the day…"
42
Another carer in FG1, was of the opinion that service shortages and follow up care in the
community stemmed from a lack of financial resources, stating:
"I'm not running down the health board at all because they're stretched".
However, this carer asserted that some of the economic problems arose out of a poor distribution
of funds and could be curtailed if carers were given some financial incentives and supports to
enable them to sustain their carer role at home.
She concluded that:
"The Health Board, I know there are tight reigns on their money, but think of the amount
of people it's keeping out of hospital [ home care] and what it would cost a person. It's
costing them nothing for her to be sitting at home, but yet they refuse the very small
minimum [the Carers Allowance] it's like a vicious circle. If they don't help you in the
initial stages, it's going to cost them in the long run."
4.7 Education and Training Issues
Implications for the provision of services by carers in regard to the need for education, training,
supervision and support have been evidenced (Wardell and Chesson, 1998). A considerable lack
of training for carers in relation to lifting and handling older people was identified. Moreover,
there was no evidence of any agreed service standards, accreditation, regulation or monitoring
procedures. Concerns were also voiced in regard to a lack of communication, monitoring and
support for carers, from the relevant professionals where new or altered medication had been
introduced.
A carer in FG1, whose mother was blind and living with poorly controlled diabetes mellitus,
expressed serious concerns about the lack of information and support for carers trying to
administer medication. She expressed the view that the health care services for older people
living at home are such that:
43
"You are left with the responsibility…really at the end of the day there is nobody there to
help, and at the end of the day, you are there on your own … you had to go and look for
things yourself, you need somebody to take control of the medical end of things, you know
the drugs."
4.8 The Physical Components of Care-giving
A number of carers referred to the fact that many carers do not possess the physical skills and
capacities necessary to undertake certain aspects of the caring role. Many were unsure as to how
to access supportive equipment and appliances. One aged carer in FG3 caring for his wife, who
was suffering from Alzheimer's disease, explained that he received no help from the statutory
services, commenting:
"I'm the one who's on tablets. I'm nearly crippled".
No members of any discussion group reported ever having received a physical assessment of the
home care environment, or any structural modifications to the home to facilitate caring. A carer
in FG3, looking after her mother commented that:
"Old people should be supplied with a shower with a seat…devices anything that makes
life easier."
A male carer in FG3, caring for his mother commented that without help:
"The hygiene problem… is at times very awkward".
4.9 The Positive Dimensions of Caring
A daughter, commenting on caring for her father related how important it was to her to have
been afforded the opportunity to care for somebody she was very close to, stating:
“I did what I would like someone to do for me and it was very fulfilling. I felt it was
closeness, and when he died, I said well you did your best for me and I have done that for
you. So, that was comfort for me and I wouldn’t change it”.
44
This carer went on to convey the comfort she derived from her role in caring for her parents,
while assuring a fellow carer who was caring for her father:
" You will always say to the day you die I have given him the most precious thing and that
is my time".
4.10 Conclusion
A diverse range of needs and experiences were related in the course of these focus groups. The
magnitude and complexity of carers' roles and responsibilities is clearly illustrated. These
contentions portray clearly the importance of exploring and responding to defined gaps in health
and social care services to support rather that militate against the maintenance of informal care-
giving. The findings support the thesis that we cannot lightly refute the possibility that:
‘We are in danger of needing more and more ambulances downstream to fish people out
of the river for want of fences upstream to stop them falling in' (Harding, 1997).
45
CHAPTER FIVE
5.0 Introduction
The results of the main study and a discussion of its findings are presented in this chapter.
Survey data were collected between mid November 1999 and mid February 2000. A total of 215
completed questionnaires were returned out of a total of 319, representing a response rate of
69%. This study was undertaken during a period of considerable industrial unrest in Irish
nursing, which culminated in strike action. Given the impact of these issues on the distribution
mechanism coupled with the significant workload of many carers, this was considered a
reasonably acceptable response rate.
Section One: Presentation of Questionnaire Data
5.1 Socio-Demographic Details of Carers
Carers in this study were drawn from a wide geographical spread representative of carers residing in
rural (54.2%) and urban (45.8%) areas. In relation to gender, almost three-quarters of carers
identified were female. 71.2% (n=153) were female and 28.8 % (n=62) were male.
Table 5.1: Carers’ Age
Description Frequency Valid Percent Cumulative Percent
20-30 years
31-40 years
41-50 years
51-60 years
61-70 years
over 70 years
5
19
50
61
39
41
2.3
8.8
23.3
28.4
18.1
19.1
2.3
11.2
34.4
62.8
80.9
100.00
Total 215 100
It can be observed from Table 5.1, that almost 20% of carers are over the age of 70 years, 37%
over the age of 60, and 65% are over the age of 50 years. Thus, consistent with previous studies
detailed in chapter two, a significant number of carers were older persons themselves. A small
minorities of carers, 2.3% were aged between twenty and thirty years while most carers in the
46
study were aged between fifty-one and sixty years (28.4%). The mean age of carers was
estimated at 56 years (range=20-70+years).
Table 5.2: Identifying Carer/Care Recipient Relationships
Description Frequency Valid Percent Cumulative PercentCarers caring for a parent/ parent-in-law
Carers caring for a spouse
Caring for an aunt/uncle
Sister/Brother
Brother/Sister-in-law
Neighbour/Friend
Granddaughter
121
48
16
15
5
6
2
56.8
22.5
7.4
7.1
2.4
2.8
0.9
56.8
79.3
86.7
93.8
96.2
99.0
99.9Total 213 100
As indicated in Table 5.2, 56.8% of principal carers were caring for a parent, and 35.2% of the
main carers were daughters. This confirms the carer profile portrayed in numerous other studies
where the caregiver role traditionally fell upon female family members. While 22.5% of carers
were caring for a spouse, other family members were also engaged in the care-giving role. In
general, care-giving lay within the domain of one family member.
Table 5.3: Number of Carers Co-Residing with the Older Person, by Age (N=215)
What age are you?
Do you live in the same household as the older person / persons you care for?
Yes No20 – 30 Years 5 031 – 40 Years 15 441 – 50 Years 34 1651 – 60 Years 43 1861 – 70 Years 34 5Over 70 Years 38 3
47

Table 5.3 above shows that at the time of the survey 78.6% (n =169) of the sample were living in
the same household as the older person. Older carers, particularly males were found to be more
likely to be living with the care recipient.
5.2 Extent of Care-giving Relationships and Responsibilities
Figure 5.1 below, shows that only 10 (4.7%) of respondents had been a carer for less than a year,
while 34 (15.8%) of the total sample reported care-giving for twenty years or more (range I-20
years+). Most of the carers (26.5%) n=57, reported engaging in the care-giving role for greater than
five but less than ten years.
Figure 5.1: The Number of Years Spent Caring (N=214)
48
How long have you been a carer?
Cou
nt
60
50
40
30
20
10
0
34
45
5754
15
10
Table 5.4: The number of older people being cared for by each carer (N=214)
What Age are you?
How many people over 65 years do you care for?
1 2 3 4
20 – 30 Years 4 1 0 0
31 – 40 Years 18 1 0 0
41 – 50 Years 39 10 0 1
51 – 60 Years 53 4 1 0
61 – 70 Years 36 3 0 0
Over 70 Years 39 2 0 0
Table 5.4 above, illustrates that a significant majority of carers (88.3%: n=189) engage in the
care of one older person while (11.7%) indicated that they cared for two or more people. Those
caring for one or more person tended to be in middle or old age themselves. A further 23.3% had
other care-giving responsibilities as mothers of school-going children, housewives and carers of
chronically ill children or adults.
Table 5.5: Carers’ Time Spent Providing Care Daily
Description Frequency Valid Percent Cumulative Percent
Carers’ time spent providing care daily:
0-3 Hours4-8 Hours9-15 Hours16-24 Hours
374232102
17.419.715.047.9
17.437.152.1
100.00Total 213 100
As illustrated in Table 5.5, the average time spent care-giving was between 16 and 24 hours daily
(47.9%) or less providing care supporting previous studies that reported care-giving as a twenty
four-hour job (see chapter 2). Only 17.4% reported spending three hours or less.
49
Table 5.6: Overnight Care Provided by Carers
Description Frequency Valid Percent Cumulative Percent
Provision of overnight care:
1 -3 Times nightly4 -6 Times nightly> 6 Times nightly
Sometimes
881173
80.410.36.52.8
80.490.797.2
100.00Total 109 100
Table 5.6 shows that more than half the sample (50.5%) reported providing care overnight with
80.4% reported having to get up 1-3 times nightly while 16.8% reported having to get up more often
to provide care.
Table 5.7: The Extent of Care-Giving as Expressed Weekly
Description Frequency Valid Percent Cumulative Percent
Provision of daily care:
4 Week days or less
All seven days
24
190
11.2
88.8
11.2
100.00
Total 214 100
Table 5.7 shows that 88.8% of respondents reported providing care across all seven days of the
week, illustrating the continuous nature of the carers’ role.
Table 5.8 below, profiles the many labour intensive dimensions of the care-giving role,
illustrating the diversity and intensity of some of its many components. These aspects of care-
giving are based on an activity of living model and are by no means all-inclusive.
50
Table 5.8: Number of Carers Spending Time Engaged in Activities of Daily Living
Number of Carers engaged in each activity
None 1-6 hours
7-12 hours
13-18 hours
19-24 hours
Washing and bathing 94 105 3 1 6Dressing 110 90 3 1 7Eating and drinking 137 57 4 1 7Cooking 48 138 13 4 8Toileting 123 67 4 3 9Lifting and moving 118 71 6 5 8Incontinence 130 57 4 4 10Medication 56 132 12 1 8Household tasks 35 133 21 6 14Shopping 33 156 6 3 10Personal safety 35 107 19 10 37
Through open-ended questionnaire items, many carers expressed key concerns, which lay within
the following areas:
A lack of official acknowledgement regarding the financial impact of care-giving;
Difficulty in obtaining the carers allowance despite carers needs;
Deterioration in their quality of life, as a result of care-giving;
Deterioration in the older persons physical and psychological state;
Concerns regarding future coping strategies as the dependency of the older person increases;
Issues surrounding the aged profile of carers themselves;
Carers and older people living in poor social conditions;
Social isolation, and an associated lack of independence;
Issues surrounding loneliness and a lack of social interaction;
A lack of practical support services, particularly home helps and home care attendants;
The lack of flexibility and continuity in terms of day-care and respite care, since care-giving
is a twenty four hour job;
51
5.3 Carers in the Formal Workplace
Tables 5.9 shows that 33.5% of carers were also engaged in employment outside the home. A
further 37.7% indicated that they would like to be in paid employment while 20.3% stated that
they had given up paid employment to engage in care-giving responsibilities.
Table 5.9: Carers’ Work Profile
Description Frequency Valid Percent Cumulative Percent
Full-time paid employment
Part-time paid employment
Work in the home only
26
24
164
12.1
11.2
76.6
12.1
23.4
100.00
Total 214 100If not, would you like to be in paid employment?
YesNo
63104
37.762.3
37.7100.00
Total 167 100Did you give up paid employment to become a carer?
YesNo
43169
20.379.7
20.3100.00
Total 212 100
5.4 Responsibilities for Care-giving
Table 5.10 shows that 77.7% of the sample felt that caring for the older person was primarily the
responsibility of both the family and the Health Board collectively. Some 19.1% believed that
this responsibility rested with the family alone, while only 3.3% of respondents indicated that the
responsibility rested solely with the Health Board. Of considerable significance was the
consistent evidence suggesting that 93.8% of carers feel that the Department of Health should do
more for the carers of older people.
52
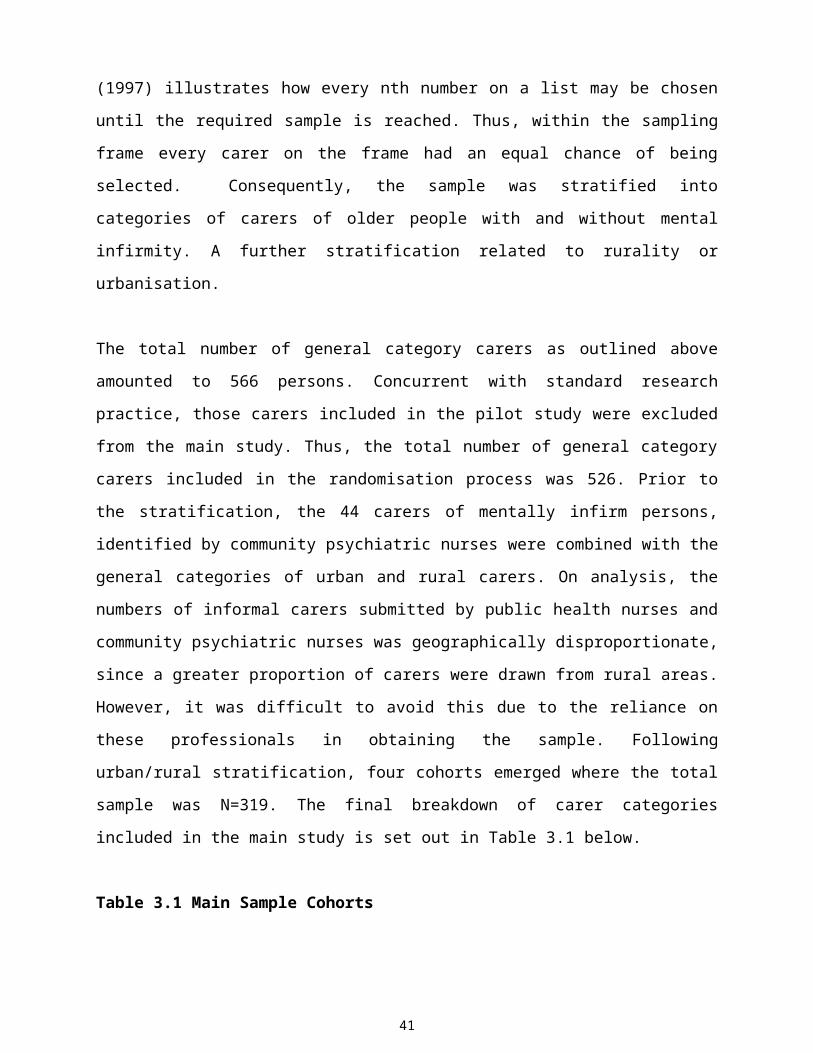
Table 5.10: Responsibilities for Care-giving
Description Frequency Valid Percent
Cumulative Percent
Do you believe that caring for the older person is primarily the responsibility of:
Family?Health Board?
Both?
417
167
19.13.377.7
19.122.3
100.00
Total 215 100Do you feel the Department of Health should do more for the carers of older people?
Yes No
19712
93.85.7
93.899.5
Total 210 100
5.5 Health Profile of Carers
More than half of the total sample reported that they worried about their present health (53.3%
n=114), while 70.3% (n=149) expressed concerns regarding their future health. Furthermore,
more than two thirds of respondents, 68% (n=138) stated that they worried about becoming
unwell and unable to continue as a carer, while 26.6% (n=57) indicated that they did not usually
have enough energy to fulfil their role as a carer. Additionally, 24.3% (n=52) reported that they
did not get enough sleep to meet their own needs. A total of 25.7% (n=55) indicated that they
did not find life satisfying, while 30% (n=64) no longer felt cared for as a person. 55.1% (n=118)
related a deterioration in their social life since undertaking the care-giving role.
53
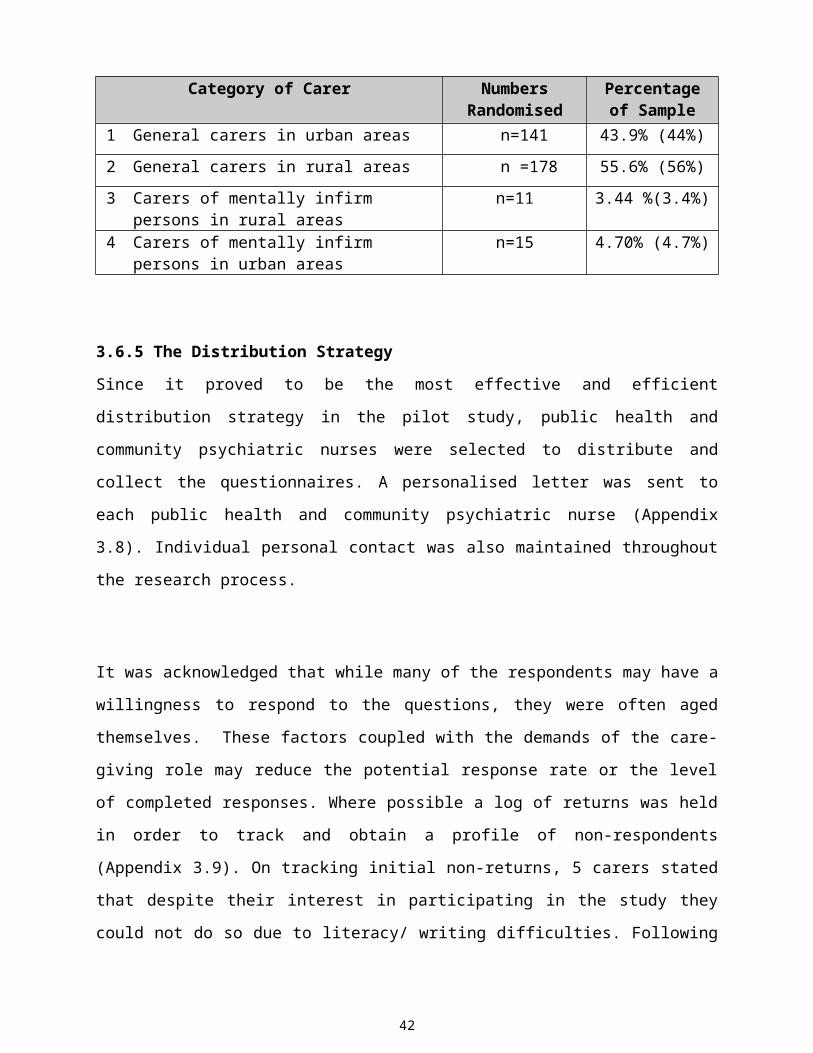
Table 5.11: Carers’ Perceptions of their Physical and Emotional Health
Description Frequency Valid Percent
Cumulative Percent
How would you describe your physical
health before becoming a carer?
Very Good
Good
Fair
Poor
Very Poor
97.0
81.0
34.0
2.0
0.0
45.3
37.9
15.9
0.9
0.0
45.3
83.2
99.1
100
100
Total 214 100How would you describe your physical
health since becoming a carer?
Very Good
Good
Fair
Poor
Very Poor
47.0
74.0
71.0
17.0
4.0
22.1
34.7
33.3
8.0
1.9
22.1
56.8
90.1
98.1
100
Total 213 100How would you describe your emotional
health before becoming a carer?
Very Good
Good
Fair
Poor
Very Poor
87.0
104.0
23.0
0.0
0.0
40.7
48.6
10.7
0.0
0.0
40.7
89.3
100
100
100
Total 214 100How would you describe your emotional
health since becoming a carer?
Very Good
Good
Fair
Poor
Very Poor
41.0
87.0
64.0
10.0
12.0
19.2
40.7
29.9
4.7
5.6
19.2
59.8
89.7
94.4
100
Total 214 100
54
As illustrated in Table 5.11, a significant proportion of carers reported deterioration in their
physical health since partaking in the care-giving role. While 83.2% described their physical
health as very good (45.3%) or good (37.9%) prior to becoming a carer, only 56.8% collectively
reported the same positive expressions of physical health since becoming a carer. Moreover,
89.3% expressed their emotional health as very good (40.7%) or good (48.6%) before becoming
a carer; these figures fell to 19.2% and 40.7% respectively (59.9% collectively) following
engagement in the care-giving role, suggesting a significant deterioration in carers’
psychological wellbeing. While carers’ expressions of poor or very poor physical or emotional
health were almost non-existent prior to becoming a carer, carers perceived their physical health
as poor (8%) or very poor (1.9%) since becoming a carer. Some carers also perceived their
emotional health as poor (4.7%) or very poor 5.6% since becoming a carer.
It can be observed from Table 5.12, that 68.6% of the sample reported that they relied on past
experiences to help them cope with their care-giving role, while 66.0% were of the opinion that
they coped better when they reflected upon good times they shared with the care recipient in the
past. Similarly, three quarters of respondents (75.0%) believed that the good parts of caring
enabled them to cope with their role. Half the sample (48.7%) were of the opinion that more
information and training in relation to their role would enable them to cope. Furthermore, in
order to cope 51.0% felt the need to discuss their problems as a carer. A sizeable majority 77.9%
(n=166) felt that religious / spiritual beliefs helped them to cope with their care-giving role.
55
Table 5.12: Coping Strategies Adopted by Carers
Description Frequency Valid Percent Cumulative PercentI rely on past experiences to help me copeStrongly AgreeAgreeNeither Agree nor DisagreeDisagreeStrongly Disagree
3110932266.0
15.253.415.712.72.9
15.268.684.397.1100
Total 204 100I cope better when I reflect on good times I had in the past with the person I care forStrongly AgreeAgreeNeither Agree nor DisagreeDisagreeStrongly Disagree
2811238223.0
13.855.218.710.81.5
13.869.087.798.5100
Total 203 100The good parts of caring help me to copeStrongly AgreeAgreeNeither Agree nor DisagreeDisagreeStrongly Disagree
2212933137.0
10.863.216.26.43.4
10.874.090.296.6100
Total 204 100If I had more information and training for this role, I feel I could cope betterStrongly AgreeAgreeNeither Agree nor DisagreeDisagreeStrongly Disagree
237650486.0
11.337.424.623.63.0
11.348.873.497.0100
Total 203 100I need someone to discuss my problems as a carer, in order to copeStrongly AgreeAgreeNeither Agree nor DisagreeDisagreeStrongly Disagree
287533579.0
13.937.116.328.24.5
13.951.067.395.5100
Total 202 100
As illustrated in Table 5.13, a total of 95% (n=303) of respondents described their past
relationship with the care recipient as very good (76.2%) or good (18.7%), while 77.7% (n=185)
described their current relationship with the person they care for as very good (65.4%) or good
(22.3%). Although, 3.7% described their past relationship as fair, poor or very poor (1%) some
10.9% expressed their current relationship as fair or poor 0.9%. Therefore, some deterioration in
the carer / care recipient relationship was noted following engagement in the care-giving role.
56
Table 5.13: Profiling Carer/Care Recipient Relationships
Description Frequency Valid Percent Cumulative PercentHow would you describe your PAST relationship with the person you care for?Very GoodGoodFairPoorVery Poor
163.040.08.01.01.0
76.218.73.70.50.5
96.294.998.699.199.5
Total 214 100How would you describe your CURRENT relationship with the person you care for?Very GoodGoodFairPoorVery Poor
138.047.023.02.00.0
65.422.310.90.90.0
65.487.798.699.5100
Total 211 100
5.6 Health Profile and Age of the Care Recipient
74.6% of older people suffered from general health related conditions, while 25.4% were known to
have varying degrees of mental infirmity ranging from Alzheimer’s disease to differing forms of
dementia, confusional states and functional depression. Although 8.2% were known to be caring
for a mentally infirm person on commencement of the study, on analysing the health profile of the
total sample, a further 17.2% were identified.
Figure 5.2: The Number of Older People Suffering from Periods of Confusion
57
Does the person suffer from any periods of confusion?
NeverOccasionallyFrequently
Perc
ent %
50
40
30
20
10
0
30
47
23
As illustrated in Figure 5.2 above, 70.3% of carers stated that the older person experienced
periods of confusion, (23.3%) frequently and (47.0%) occasionally. Figure 5.3 below, shows
that the average age of the care recipients lay between 81 and 85 years (27.2%), with an age
range of between 65 and 102 years. This is consistent with previous research (see chapter 2)
evidencing the increasing longevity of older people.
Figure 5.3: The Age of the Care Recipient
5.7 Economic and Practical Assistance with Care-giving
82.8% (N=178) of carers indicated that they were not in receipt of the carers’ allowance, while
89.9% did not endorse the means testing of the carers’ allowance. Although 38.5% (n=82)
related experiencing financial worries that resulted from providing home care, only 13.1% of the
sample reported experiencing concerns about their pension as a consequence of having given up
paid employment to become a carer.
As indicated in Tables 5.14 and 5.15, (80.6%) are not receiving the support of a home help or
home care attendant (87.7%). Furthermore, many carers who do receive these support services
receive very few hours weekly. Several carers reported that they supplemented the payment
which the home help / home care attendant received, expressing the view that the payment rates
were too low to attract or maintain these support personnel. In addition, carers expressed
58

dissatisfaction with the lack of these support services at night or at weekends, particularly where
the older person required high levels of care-giving interventions.
Table 5.14: Carers Receiving Home Help Expressed in Hours Per Week (n=201)
Description Frequency Valid Percent Cumulative Percent
None1-2 Hours3-4 Hours5-6 Hours7-8 Hours9-10 Hours
Over 10 Hours
1628.07.06.05.04.09.0
80.64.03.53.02.52.04.5
80.684.688.191.093.595.5
100.00Total 201 100
Table 5.15: Carers Receiving Home Care Assistance Expressed in Hours Per Week (n=195)
Description Frequency Valid Percent Cumulative Percent
None
1-2 Hours
3-4 Hours
5-6 Hours
7-8 Hours
Over 10 Hours
171
7.0
7.0
3.0
3.0
4.0
87.7
3.6
3.6
1.5
1.5
2.1
87.7
91.3
94.9
96.4
97.9
100.00
Total 195 100
As shown below in Table 5.16, 45.8% of the sample claimed to need the assistance of a home
help, while a further 37.4% claimed to require the services of a home care attendant.
59

Table 5.16: Carers Expression of their Need for Access to Support Services
Description Frequency Valid Percent Cumulative Percent
Do you feel you need the assistance of a home help?
YesNo
98116
45.854.2
45.8100.00
Total 214 100Do you feel you need the assistance of a home help?
YesNo
80134
37.462.2
45.8100.00
Total 214 100
With regard to other support networks, it can be seen in Table 5.17 that 62.1% of carers
described the practical support and assistance they receive from family as very good (40.3%) or
good (21.8%). However, 11.8% described it as fair, while 3.8% indicated that family support
was poor or very poor (8.1%). Interestingly, 14.2% stated that they did not expect any practical
support from family. Similarly, 12.5% of carers did not expect practical support from
professionals/health services. Although those in receipt of practical support from professional
health service agents described it as very good (27.9%) or good (31.3%); 16.3% felt that this
service was fair, poor (6.3%) or very poor (5.8%). In addition, 66% stated that they did not
expect voluntary bodies to provide practical support. In relation to friends and neighbours,
40.6% of respondents claimed that they did not expect any support or assistance from them.
However, those in receipt of practical support from friends and neighbours (59.4%) described it
as very good (17.4%) or good 21.3%.
60
Table 5.17: Sources of Practical Support and Assistance
Description Frequency Valid Percent
Cumulative Percent
FamilyGood / Very GoodFairPoor / Very PoorDon’t expect any support / assistance
131252530
62.111.811.814.2
62.173.985.8
100.00Total 211 100
Professionals/ Health ServicesGood / Very GoodFairPoor / Very PoorDon’t expect any support / assistance
131252530
59.216.312.112.5
59.275.587.6
100.00Total 208 100
Voluntary OrganisationsGood / Very GoodFairPoor / Very PoorDon’t expect any support / assistance
23639132
11.53.019.566.0
11.514.534.0
100.00Total 200 100
Friends/ NeighboursGood / Very GoodFairPoor / Very PoorDon’t expect any support / assistance
80232084
38.711.19.740.6
38.749.859.4
100.00Total 207 100
5.8 Sources of Information Regarding Support Services
Almost two-thirds (62.7%) of the sample reported that they did not receive enough information
about the availability of support services in their care-giving role. Table 5.18 below, illustrates
key sources identified regarding accessing relevant information about available services to
support the carers’ role. Primarily, information was sourced from public health nurses (77.9%)
family doctors (63.4%) and friends and neighbours (17.4%). Almost two thirds of respondents
indicated that this information was not obtained from community psychiatric nurses. With
regard to the information received from health care professionals, some carers expressed the
view that the public health nurse and the family doctor did not offer information voluntarily,
claiming that obtaining relevant information was generally initiated by the carers themselves, as
a reaction to a problem situation.
61
A total of 30% of carers reported upon the value of books, newspapers and magazines as a source of
information regarding accessing support services while others reported media such as radio,
(20.7%) television, (22.1%) or the internet (4.2%) as being instrumental in retrieving the necessary
information.
62
Table 5.18: Sources Identified as Providing Carers with Information about Relevant
Support Services
Description Frequency Valid Percent Cumulative Percent
DoctorYesNo
13578
63.436.6
63.4100.00
Total 213 100Community Psychiatric NurseAgreeDisagree
2133
38.961.1
38.9100.00
Total 54 100Public Health NurseYesNo
16647
77.922.1
77.9100.00
Total 213 100FamilyYesNo
69144
32.467.6
32.4100.00
Total 213 100Friends/NeighboursYesNo
37176
17.482.6
17.4100.00
Total 213 100FamilyYesNo
69144
32.467.6
32.4100.00
Total 213 100RadioYesNo
47166
22.177.9
22.1100.00
Total 213 100Books, Newspapers and magazinesYesNo
64149
3070
30100.00
Total 213 100TelevisionYesNo
47166
22.177.9
22.1100.00
Total 213 100InternetYesNo
9.0204
4.295.8
4.2100.00
Total 213 100
63

5.9 Carers Interaction with Health Care Professionals
As can be observed from Table 5.19 below, 59.1% of respondents reported that they received a
visit from the public health nurse at least monthly, while 8.6% claimed that they had never seen
him/her. Some 19% claimed that the public health nurse only called to them when asked to do
so. Although 25.4% of the overall sample was caring for a mentally infirm person, only 35.2%
indicated that were seen by a community psychiatric nurse, at varying intervals. A sizeable
number of carers (49.8%) reported that they only saw the family doctor when asked or needed.
Some 89.7% of participants stated that they had never seen an occupational therapist, social
worker (94.8%) or a physiotherapist (84.5%) in their home or at a clinic. Additionally, a
significant number of carers indicated that they had never met with a chiropodist (69%) or
counsellor (98.4%). However, of the 31% of the sample that reported having been seen by a
chiropodist, many stated that this was by private consultation.
Table 5.19: Carers Reported Interaction with Health Care Professionals
Description Frequency Valid Percent
Cumulative Percent
Meets the Public Health Nurse1-3 WeeklyMonthly2-6 Monthly9-12 MonthlyOnly when asked/neededNever
3094270.04018
14.344.812.90.0
19.08.6
14.359.172.072.091.099.0
Total 213 100Meets the Community Psychiatric Nurse1-3 WeeklyMonthly2-6 Monthly9-12 MonthlyOnly when asked/neededNever
1.012.04.00.02.035
1.922.27.40.03.7
64.8
1.924.131.531.535.2100
Total 54 100Meets the Family Doctor1-3 WeeklyMonthly2-6 Monthly9-12 MonthlyOnly when asked/neededNever
2.064300.010611
0.930
14.10.05.2
49.8
0.930.94545
50.2100
Total 213 100
64
14/05/23 04:43
Table 5.19 (cont.): Carers Reported Interaction with Health Care Professionals
Description Frequency Valid Percent
Cumulative Percent
Meet the Social Worker1-3 WeeklyMonthly2-6 Monthly9-12 MonthlyOnly when asked/neededNever
0.00.02.00.08.0183
0.00.01.00.04.1
94.8
0.00.01.01.05.199.9
Total 193 100Meet the Chiropodist1-3 WeeklyMonthly2-6 Monthly9-12 MonthlyOnly when asked/neededNever
0.010.0180.034
138
0.05.09.00.0
17.069.0
0.05.014.014.031.0
100.00Total 200 100
Meets the Occupational Therapist1-3 WeeklyMonthly2-6 Monthly9-12 MonthlyOnly when asked/neededNever
0.00.02.00.018.0
175.0
0.00.01.00.09.2
89.7
0.00.01.01.010.299.9
Total 195 100Meet the Counsellor1-3 WeeklyMonthly2-6 Monthly9-12 MonthlyOnly when asked/neededNever
0.01.01.00.01.0190
0.00.50.50.00.5
98.4
0.00.51.01.01.599.9
Total 193 100Meet the Physiotherapist1-3 WeeklyMonthly2-6 Monthly9-12 MonthlyOnly when asked/neededNever
0.07.02.00.020
163
0.03.61.00.0
10.484.5
0.0-3.64.64.615.0
100.00Total 193 100
While 68.4% indicated that the healthcare professionals they interacted with understood carers’
specific health and social care needs, almost one third of the sample did not share this view.
Furthermore, 45.3% indicated that they would like more support from healthcare professionals.
65

14/05/23 04:43
Table 5.20:Professionals Carers Would Like More Support and Advice From
Description Frequency Valid Percent
Cumulative Percent
Which professionals would you like more support and advice from?Public Health NurseYesNo
43162
2179
21100.00
Total 205 100Community Psychiatric NurseYesNo
1232
22.277.8
22.2100.00
Total 44 100Occupational TherapistYesNo
22183
10.789.3
10.7100.00
Total 205 100PhysiotherapistYesNo
19186
9.390.7
9.3100
Total 205 100Social WorkerYesNo
18187
8.891.2
8.8100
Total 205 100DoctorYesNo
44161
21.578.5
21.5100
Total 205 100CounsellorYesNo
19186
9.390.7
9.3100
Total 205 100ChiropodistYesNo
30175
14.685.4
14.6100
Total 210 100
66
14/05/23 04:43
As shown in Table 5.20 above, nearly one fifth of respondents expressed a preference for further
support and advice from both public health and community psychiatric nurses. Interestingly,
evidence detailed in Table 5.19, illustrates that public health nurses interact with and support
carers more than any other health care agent. These findings are supported by data illustrated in
Table 5.18, where almost four fifths (77.9%) of carers identified public health nurses as key
health care professionals in the provision of adequate information for carers regarding relevant
support services.
Table 5.21: Professionals Reported as Providing the Most Valuable Contribution to Carers
Description Frequency Valid Percent Cumulative PercentPublic Health NurseYesNo
12769
64.835.2
64.8100
Total 196 100Family DoctorYesNo
90.0106
45.954.1
45.9100
Total 196 100Community Psychiatric NurseYesNo
13.037
26.074
26.0100
Total 50 100PhysiotherapistYesNo
4.0191
2.097.4
2.099.5
Total 195 100Social WorkerYesNo
3192
1.598
1.599.5
Total 195 100Occupational TherapistYesNo
5190
2.696.9
2.699.5
Total 196 100ChiropodistYesNo
11184
5.693.9
5.693.9
Total 195 100CounsellorYesNo
4191
297.4
299.4
Total 195 100
67
14/05/23 04:43
Table 5.21 above highlights health care professionals identified by carers as providing the most
valuable contribution in supporting carers. Public health nurses were seen as providing the
single most valued contribution to carers (64.8%). A further 45.9% indicated the value of the
family doctor in providing caregiver support. Interestingly, a quarter of respondents (26%)
specified the contribution of community psychiatric nurses. This may be explained by the fact
that only 35.2% reported meeting with a community psychiatric nurse, while 22.2% of carers of
mentally infirm persons expressed a preference for further support and advice from community
psychiatric nurses (see Table 5.19).
Table 5.22: Carers’ Perceptions of People There to Listen to Them
Description Frequency Valid Percent Cumulative PercentFamilyAgreeDisagree
15948
76.823.2
76.8100.00
Total 207 100Professionals / Health ServicesAgreeDisagree
15851
75.624.4
75.6100.00
Total 209 100Voluntary OrganisationsAgreeDisagree
36169
17.682.4
17.6100.00
Total 205 100Friends/NeighboursAgreeDisagree
106102
51.049.0
51.0100.00
Total 208 100
As shown in Table 5.22 carers felt that the people that are there to listen to them include family
(76.4%); professional / health services (75.6%); voluntary organisations (17.6%) and friends/
neighbours (51.0%). Therefore, nearly a quarter of respondents felt that neither professionals /
health service agents nor other family members were available to listen to them.
5.10 Respite and Day Care Services
68

14/05/23 04:43
66.7% of carers reported that they had never been offered respite care, while 32.6% (n=104) who
had been offered respite care did not avail of it. Although 58.9% (n=126) of respondents were
aware of day-care services only 13.1% (n=28) indicated that they availed of these services.
An open-ended questionnaire item revealed reasons that may be best illustrated by the following
carers’ experiences
“All outside help is refused and discouraged, (by the care recipient) neither or nurses or nuns
can persuade her; all have tried and failed”. (Carer no. 215)
“We live in a remote rural area.” (Carer no. 149)
“The problem of getting out, plus mobility problem…living in an isolated area.
“Don’t know of any Day-care services, nor have I been made aware of any….no transport.”
(Carer no. 181)
“Would not be able, as he is physically and mentally unwell”. (Carer no. 104)
“Unable to go out due to mental confusion”. ( Carer no. 1)
“Very independent and proud”. (Carer no. 95)
As shown in Table 5.23 below, 75.5% of respondents stated that they had received a break,
defined as a period of a week or more away from their care-giving role. Of those who reported
receiving a break, family (58.5%) and friends (22.3%) were cited as caring for the care recipient
in their absence. Approximately one third (36.8%) of respondents reported that they had
received a break in the proceeding 6 to 12 months. A further, 22.2% reported that they had not
received any break in the preceding 1 to 5 years, while 11.3% indicated that they had not
received a break for between 5 and 10 years. Interestingly, 5.2% reported not having had a break
in over 10 years, while a quarter (24.5%) of respondents related that they never had a break from
their care-giving role.
69
14/05/23 04:43
Table 5.23: Frequency of Breaks from the Care-Giving Role
Description Frequency Valid Percent
Cumulative Percent
How long is it since you had a break, lasting a week or more away from your care-giving
role?
Less than 6 monthsBetween 6 and 12 monthsBetween 1 and 5 yearsBetween 5 and 10 yearsOver ten yearsNever
572147241152
26.99.922.211.35.224.5
26.936.859.070.375.5100
Total 212 100
Table 5.24 below illustrates the respite services from which carers felt they would benefit.
Almost 44% of respondents indicated a preference for respite services provided for a few hours
weekly, on a regular basis. Many indicated a preference for in-home services. Almost one fifth
of respondents (18.5%) suggested that they could not avail of some respite services since the care
recipient wished to remain at home. This is consistent with carers’ comments in relation to the
poor uptake of day-care services. Many older people saw support services such as respite care as
a challenge to their independence. 13% of carers expressed a preference for day-care services in
the local community. However, a quarter of respondents expressed the view that they would
benefit from a week respite care twice yearly in a facility for the care of older people.
Table 5.24: Respite Services-Profiling Carers’ Perspectives
Description Frequency Valid Percent
Cumulative Percent
Which Respite Services would you benefit from if available?
A couple of hours a week on a regular basisDay-care facilities in the local communityOne week twice a year in a facility for the care of older people Wouldn’t go, only happy at home
8726
5337
43.513.0
26.518.5
43.556.5
83.0101.5
Total 200 100
Table 5.25 shows that 12.1% of carers claimed to experience transport problems in accessing
services aimed at supporting the care-giving role, a significant majority of carers (69.6%) stated
that they used their own private transport facilities in order to access necessary services.
70
14/05/23 04:43
Table 5.25: Transport Problems Associated with Accessing Support Services
Description Frequency Valid Percent Cumulative Percent
Do you experience transport problems in accessing services to support you in your caring role?
YesNo
Transport has to be provided by family/self
2639149
12.118.269.6
12.130.3
100.00
Total 214 100
71
14/05/23 04:43
5.11 Factor Analysis: Analysing Scale Reliability
The primary purpose of factor analysis was to reduce sets of Likert scale variables into smaller
more manageable sets of measures. In terms of concept development this procedure reduces
large sets of variables into smaller variable sets with common characteristics or underlying
dimensions (Polit and Hungler, 1991). These factors represent the weights on each factor and
were derived from inter-correlations in the correlation matrix.
5.11.1 Factor Analysis
Factor analysis, a multivariate statistical technique for assessing evidence of internal association
between sets of variables, is a powerful measurement assessment and measurement reliability
tool (Polit and Hungler, 1991). It is the most appropriate and commonly used inferential
statistical technique for assessing empirical evidence regarding internal consistency, association
and subsequent reliability (Zeller and Carmines, 1986). The use of the factor analysis model is
consistent with similar previous research by leading researchers in the field in the exploration of
issues such as carer burden (Nolan and Grant, 1992).
Factor frequencies are shown in Appendices 5.1 to 5.3. Interrelationships between the variables
underpinning each concept were identified and banded together as unified concepts. Following
this process of identifying underlying theoretical constructs, the following factors emerged:
loss of control,
self-fulfilment,
social isolation and loneliness.
Factor analysis was engaged in, as a process of establishing the discriminant validity of these
concepts. The factor loadings shown in Appendices 5.4 to 5.6 were condensed from larger
variable sets and extracted following computation from a rotated factor matrix, using the
Statistical Package for Social Sciences, (SPSS, 1997). Similar to correlation co-efficients, factor
loadings range from –1.00 to = +1.00 and represent the correlation between individual factors or
underlying dimensions (Polit and Hungler, 1991).
72
14/05/23 04:43
5.12 Reliability
Since the factor loading is analogous to a correlation coefficient, it can be inferred from Figures
6.19 to 6.21 that there are significantly strong factor / variable relationships. Thus, intercorrelations
amongst variables contained within the questionnaire responses were clarified. The repeatability
and consistency of these factors as empirical measurements was estimated by the application of
Cronbachs' alpha procedure (Cronbach, 1951). Coefficients, detailing computations of factor scores
are presented in Appendix 5.7 as a measure of internal consistency or equivalence. In the current
study, when reliabilities was carried out, each of the subscales had Cronbach’s alpha greater than
0.70. The criterion for acceptability was taken at the level of 0.30-0.40 (Polit and Hungler, 1991).
Since the distribution of scores of each subscale was approximately normal, it was possible to apply
parametric tests in subsequent data analysis procedures.
5.12.1 Validity
Despite the mathematically robust properties of factor analysis, its value is commonly estimated
in terms of the degree to which it is conceptually meaningful (Norusis, 1985, Alt, 1990; Nolan
and Grant, 1992). Since factor analysis does not include a technique to ensure validity, it is
essential to ensure that it is possible to make sense of the factors (Norusis, 1985, Alt 1990). The
factors were validated against accompanying data external to the analysis process. This practice
is widely deemed as an appropriate and essential component of data validation (Child, 1970, Alt,
1990, Nolan and Grant, 1992). In the current study, validation of the emergent factors was
derived from independent qualitative data. This loaned considerable weight to the level of
confidence that may be attributed to these findings.
5.12.2 The Interrelations of the Concepts
The theoretical model for loss of control, self-fulfilment, and social isolation and loneliness
would suggest that as social isolation increased there is a corresponding increase in loss of
control, and a decrease in self-fulfilment. Thus, there is evidence of a positive correlation
between loss of control and social isolation and loneliness, and an inverse relationship between
loss of control and self-fulfilment.
73
14/05/23 04:43
Table 5.26: Inter-item Correlations and their Significance
Inspection of Table 5.26 shows that the relationships are indeed as may be expected. The
correlation between loss of control and social isolation and loneliness is 0.41 (p.= 0.0001).
Although this is just outside the level of significance at the 0.05 level, it is significant at the 0.01
level. Thus, it may be deduced with 90% certainty that this result did not occur by chance. This
shows that as social isolation increases, there is increased potential for loss of control. The
correlation between loss of control and self-fulfilment is negative; as would be expected with a
coefficient of r=-0.134. There is no relationship between self-fulfilment and social isolation.
Clearly, there is no theoretical reason as to why there should be such a relationship.
5.13 Hypothesis Testing and Tests of Statistical Significance
Theoretical distributions were used to establish probable and improbable values for test (t)
statistics, based on acceptance or rejection of the null hypothesis (Polit and Hungler, 1991). By
way of determining the range of improbable values, the means at both ends of the sample were
tested through the application of two-tailed tests.
5.13.1 Hypothesis Testing Related to Social Isolation
It can be hypothesised that carers who live in rural areas are more likely to experience social
isolation than those who live in urban areas. This hypothesis was tested using t test, a parametric
procedure for testing differences in group means. The computations of the t-statistic for
independent samples detailing these results are shown in Table 5.27. The mean score for those
74
1.000 -.134 .418**-.134 1.000 -.090.418** -.090 1.000
. .063 .000.063 . .217.000 .217 .197 194 190194 197 190190 190 194
TOTNLOCTOTNSFTOTSOCISTOTNLOCTOTNSFTOTSOCISTOTNLOCTOTNSFTOTSOCIS
PearsonCorrelation
Sig.(2-tailed)
N
TOTNLOC TOTNSF TOTSOCIS
Correlations
Correlation is significant at the 0.01 level (2-tailed).**.

14/05/23 04:43
in rural areas is higher than in urban areas. However, the mean difference is not statistically
significant.
Table 5.27: Mean Scores and Standard Deviations on Social Isolation
(t=1.22. df =192, p.=ns)
5.13.2 Hypotheses Testing Related to Loss of Control
It can be hypothesised that carers of the mentally infirm sample are more likely to experience
loss of control than those who care for general categories. This hypothesis was tested using t
test. The results are shown in Table 5.28. Although loss of control was shown to be higher
amongst carers of mentally infirm persons, it was not statistically significant.
Table 5.28: Mean Scores and Standard Deviations on Loss of Control
Table 5.29 Descriptives for Loss of Control and Confusion
75
106 19.6321 5.7127 .554988 18.5227 6.8414 .7293
GeographicalLocationRuralUrban
TOTSOCISN Mean
Std.Deviation
Std. ErrorMean
Group Statistics
145 13.4483 3.5958 .298649 13.8571 3.7639 .5377
GroupingGeneralEMI
TOTNLOCN Mean
Std.Deviation
Std. ErrorMean
Group Statistics
46 14.0217 3.6239 .5343 12.9456 15.0979 5.00 20.0097 13.1753 3.8757 .3935 12.3941 13.9564 4.00 20.0054 13.9444 3.0863 .4200 13.1021 14.7868 4.00 20.00
197 13.5838 3.6210 .2580 13.0750 14.0925 4.00 20.00
FrequentlyOccasionallyNeverTotal
Does the person you care forsuffer fromconfusion?
TOTNLOCN Mean
Std.Deviation Std. Error
LowerBound
UpperBound
95% ConfidenceInterval for Mean
Minimum Maximum
Descriptives
14/05/23 04:43
As indicated in Table 5.29, those who care for older people who frequently experience periods of
confusion are more likely to experience loss of control. However, as seen in Table 5.30,
statistical analysis reveals no significant difference.
Table 5.30 Anova for Loss of Control and Confusion
Table 5.31: Anova Results for Loss of Control and Length of Time Caring
Inspection of descriptives Table 5.32; shows that carers with the highest score on loss of control
were those caring for twenty years or more and carers who had embarked on the care-giving role
within the preceding one to two years. This indicates a trend regarding initial problems of
adaptation to the role. There is also a trend towards greater loss of control in parallel with the
increasing duration of the care-giving role. As shown in Table 5.31; this trend is statistically
significant at the 0.01 level (p. = 0.669). Therefore, it can be deduced with 90% certainty that
this result was not due to chance.
76
32.036 2 16.018 1.224 .296
2537.832 194 13.082
2569.868 196
BetweenGroupsWithinGroupsTotal
TOTNLOC
Sum ofSquares df
MeanSquare F Sig.
ANOVA
42.381 5 8.476 .641 .669
2527.487 191 13.233
2569.868 196
BetweenGroupsWithinGroupsTotal
TOTNLOC
Sum ofSquares df
MeanSquare F Sig.
ANOVA

14/05/23 04:43
Table 5.32 Descriptives for Loss of Control N Mean Std. Deviation Std. Error
TOTNLO How long have you been a carer?
Up to one yearMore than one year but less than twoBetween two and five yearsBetween five and ten yearsBetween ten and twenty yearsTwenty years or moreTotal
13
52
52
40
32197
14.00
13.730
13.019
13.300
14.25013.583
4.3780
3.5431
3.7127
3.8310
2.96213.6210
1.2142
.4913
.5149
.6057
.5236
.2580
Table 5.33 Loss of Control and Respite Care
The degree to which loss of control was ameliorated by respite care was also examined.
Although those carers who received respite care experienced less loss of control, the result was
not statistically significant. The mean and S.D. for loss of control for those who received respite
care can be seen in Table 5.33.The t value = 0.68 df = 194 p = 0.49.
Table 5.34 Descriptives for Self Fulfilment and Length of Time Since Receiving a Break
N Mean Std. Deviation Std. Error
TOTNSF How long is
it since you
had a break,
lasting a
week or more
away from
your caring
role?
Less than six months
Between six and twelve
months
Between one and five years
Between five and ten years
Over ten years
Never
Total
55
18
44
20
11
49
11.1455
10.7778
9.7045
10.1500
9.5455
9.0612
3.3245
3.2998
2.2473
3.2650
2.4643
2.6802
.4483
.7778
.3388
.7301
.7430
.3829
77
66 13.3333 3.8042 .4683130 13.7077 3.5469 .3111
Has thepersonyou carefor everbeenoffered'RespiteCare'?
YesNo
TOTNLOCN Mean
Std.Deviation
Std. ErrorMean
Group Statistics
14/05/23 04:43
197 10.0812 2.9784 .2122
It can be observed on examination of Table 5. 34 that those carers who did not receive breaks of
a week or more experienced less fulfilment than those in receipt of a break from the care-giving
role. Self-fulfilment was most evident amongst those carers who received a break within the
preceding six months. Those who reported never receiving a break experienced the lowest levels
of self-fulfilment. The mean levels of self-fulfilment fall as the period since receiving a break
from care-giving increases. The lowest mean score of 9.06 was amongst those respondents who
claimed that they never had a break from their care-giving role. An inverse relationship was
found in that the longer a person cares without a break, the greater the loss of self-fulfilment.
This is indicated by the decrease in mean scores for self-fulfilment, shown in Table 5.35. This
result was statistically significant at the .010 level. Hence, there is 95% certainty that this result
was not due to chance.
Table 5.35 Mean and S.D. for Self-Fulfilment and the Period of Time Without a Break
The t value = DF=5 p=. 010 (p.0.05)
Table 5.36. Social Isolation and the Number of Hours Spent Care- giving Daily
95% Confidence Interval for Mean
Lower Bound
Upper Bound
Minimum Maximum
TOTSOCIS How many 0 – 3 19.2104 23.4348 8.00 33.00
hours a day 4 – 8 17.7410 21.6108 7.00 30.00
do you spend 9 – 15 18.1284 23.0440 9.00 35.00
caring? 16 - 24 16.4162 18.9380 7.00 32.00
Total 18.1968 19.9690 7.00 35.00
78
131.500 5 26.300 3.126 .010
1607.200 191 8.415
1738.701 196
BetweenGroupsWithinGroupsTotal
TOTNSF
Sum ofSquares df
MeanSquare F Sig.
ANOVA
14/05/23 04:43
Table 5.36. shows that the greater the number of hours spent caring daily, the more likely the
carer is to experience social isolation. As shown in Table 5.37, this result was statistically
significant at the .011 level. Therefore, it can be deduced with 95% certainty that this result was
not due to chance.
Table 5.37 Mean and S.D. for Social Isolation and the Number of Hours Spent Caring
Daily
79
423.767 3 141.256 3.784 .011
7054.906 189 37.328
7478.674 192
BetweenGroupsWithinGroupsTotal
TOTSOCIS
Sum ofSquares df
MeanSquare F Sig.
ANOVA

14/05/23 04:43
Section Two: Results of In-Depth Interviews
5.14 Key Considerations
Although the findings of the in-depth interviews alone prohibit generalisations, due to the
relatively small sample size; many of the findings are consistent with those evidenced through
the process of triangulation. Hence, these findings will be related to focus group and survey data,
where correlations were found across the three data sets. As outlined in chapter three,
comparison analysis was conducted between the manual thematic analytical process and the
application electronic software, using similar techniques to those invoked in the analysis of focus
group data. Consequently, theoretical constructs emerged from a process of thematic analysis.
Theoretical issues can then be tested in order to enhance understanding of the data.
5.14.1 Presentation of Results: Thematic Developments
Data were collected from carers, in their own environment and language. In presenting the
results of the analysis of the ten in-depth interviews, issues arising from the topic guide will be
dealt with first (see Appendix, 3.13). Further unsolicited topics are also discussed where carers
identified topics as a priority for discussion. Analysis of the content of these interviews
uncovered conceptual similarities between focus group and survey data. Consequently, common
themes emerged between focus group, survey and in-depth interview data. The thematic
foci/categories derived from the in-depth interview data are portrayed through the use of pertinent
quotes within the text. Congruence between the results of both the analysis of the qualitative and
the quantitative results contributed significantly to the validity of both.
A thematic framework made up of key categories was developed, based on carers’:
Needs and experiences;
Education and training requirements;
Perceptions of statutory, professional, voluntary and familial roles and responsibilities;
Impressions of the adequacy and efficacy of carer’ support services;
Levels of user involvement;
Overall health, wellbeing and quality of life.
Specific care-giving dynamics are separated for ease of presentation. However, it can be seen
that there are strong similarities between the multidimensional aspects of the care-giving
experience, which are often inextricably linked.
80
14/05/23 04:43
5.14.2 Statutory, Professional, Voluntary and Familial Roles
The current analysis shows that many carers feel that the responsibility for caring primarily rests
on one female family member. However, “sometimes it is not possible…women are out
working” (No. 237, p.1-2). It was suggested that in Ireland there exists a:
“Strong culture that we should look after our parents, with extended families is no longer
the case, usually the family is totally dispersed” (No. 86,p.4).
This correlates with survey and focus group data as well as similar research (Twigg and Atkin,
1994, Kane and Penrod, 1995, Jennings et al 1997). While considerable family loyalty was
evidenced, “I have the strong sense of duty to my mother” (No. 86, p.16) many carers were of
the opinion that the responsibility for caregiving was such that it was often “left to one”, (No.
122, p. 3) family member. Other respondents expressed the importance of their responsibilities
suggesting
“I was the oldest in my family, the only girl, I was the one who was left”(No. 237, p.14).
Regarding governmental responsibilities, carers believed that “they should be doing more”
(No.181, p. 1) and “look after carers properly” since “carers are vulnerable, and can feel very
isolated”, (No. 86, p. 1) describing the governments’ attitude as “negative” (No. 181, p. 38).
Many carers believed that
“the Health Board should give you help…somebody to come in for an hour, if you wanted
to go away for an evening” (No. 237, p. 30).
However, “it is very hard to get a home help”, particularly in rural areas (No. 158, p. 27), where
the service was described as “inadequate” (No. 86, p. 3). While respondents believed that the
Health Boards had a clear responsibility to support the care of older people, he believed that the
Board were “over stretched” (No. 122, p. 5) financially and have not been awarded the
necessary funding. A common belief was that the government “should provide more money to
the Health Boards, give them more scope and leave them decide what they want” (No. 158, p.
10). This carer called for “some kind of investigation, then bring it to the notice of the Health
Board” (p.13) citing examples such as assessing “our ability to get around, and to know are you
doing the right thing” (p.13) regarding the care-giving role. Many carers felt that the individual
needs of older people are not considered by State managed care agencies
81

14/05/23 04:43
“I feel the main responsibility does rest with the family, wherever possible…giving over
responsibility to the State is not a good thing…that does not take into account the
individual needs of the person”.
5.14.3 Family Dynamics
Tensions were sometimes borne out of misperceptions amongst family members regarding the
role of the primary care giver, “There are times when it would cause tensions…my mother can
be a demanding woman” (No. 122, p. 8). According to one respondent “they didn’t realise
exactly what I was doing…there was a lot of falling out” (No. 68, p. 26). Yet another carer, felt
that the minimal support he receives from his family suggested to him that “they just take it for
granted” posing the question “who cares about the carer…people like carers are not thought
of…not acknowledged” (No. 318, pp. 15-16).
“You do feel sad when you are sitting in the house on your own at night-time, you have
so much family and none of them coming near you” (No. 318, p. 32).
5.14.4 The Care-giving Environment
A willingness to engage in family care provision was evidenced. All carers interviewed
expressed the view that home care settings were the optimal environment for the care of older
people
“I think it is great if they can be looked after in the family home, it improves their life
anyway, there is no doubt about that” (No. 122, p. 16).
Furthermore, home care was associated with a sense of future “that is why I feel the hope, while
she is in her home” (No. 246, p. 26).
In particular, this assertion was portrayed in relation to the care of mentally infirm persons
“…if they were in an institutionalised place they would clam up and just sit there” (No. 5, p. 2)
“she loves her home, she knows she is in her home, she is happiest” (No. 68, p. 16).
Furthermore, respondents expressed a preference for in-home respite care “I would only be
happy if she was looked after in the home” (No. 68, p. 24). Participants suggested that carers
could be further enabled to avail of respite services
82
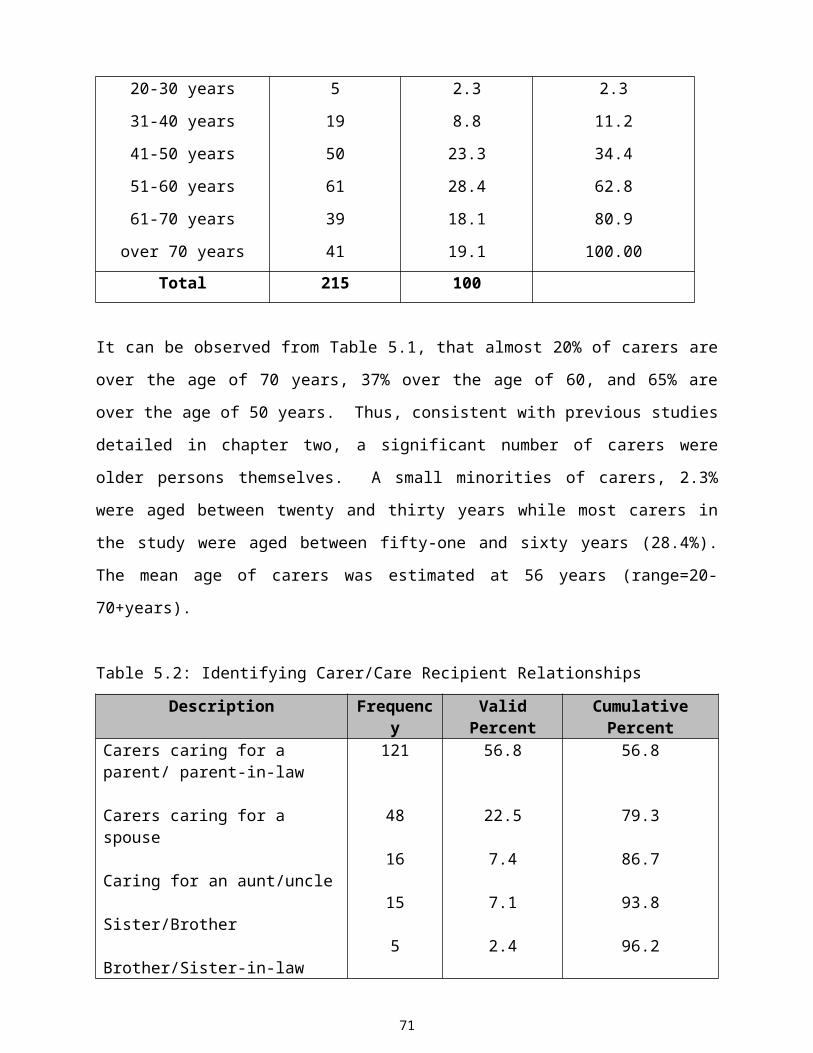
14/05/23 04:43
“If someone came here to look after her for the week or two weeks and give them the
money rather than put her into [an institution]” (No. 181, p. 21).
Survey data further supports these findings. Similarly, Nolan and Grant (1992) found that many
carers perceived institutional care are unacceptable and derived satisfaction from their ability to
provide home care, “I have given everything…I can be fulfilled” (No. 68, p. 19). Another carer
recommended the development of “a carers’ panel, someone who would come in for three or
four hours” (No. 246, p. 10). One carer summed up the sentiments of many carers as follows
“a lot of people want to do it but they can’t afford it financially, instead of having the
capital expense of more buildings and employing more nurses, why not give some
financial incentive to people to keep a person at home out of hospital” (No. 86, p. 19).
5.15 The Nature and Extent of the Care-giving Role
As evidenced in focus group and survey data, the carers’ role is often multifaceted embracing
transformational changes in carers' lives. In many cases, the care interventions required by the
older person led to psychosocial, economic and behavioural modifications, impacting on the
carers' quality of life. One male carer, profiling the extent of his involvement stated “I moved
my bed up to her room, so I am there in the night-time when she calls me” (No. 181, p. 9) adding
“If she wasn’t here now, I would be in town living with my own family…I miss them and
they miss me…if more people called into her, I might have more time for my family” (No.
181, p. 33).
Some carers who were also older persons expressed concerns about their ability to provide care
in the future
“the thing that really worries me at times…suppose I was lying in bed and got a heart
attack or something, what would happen” (No. 318, p. 10)
Sometimes older people do not see themselves as having a carer
83
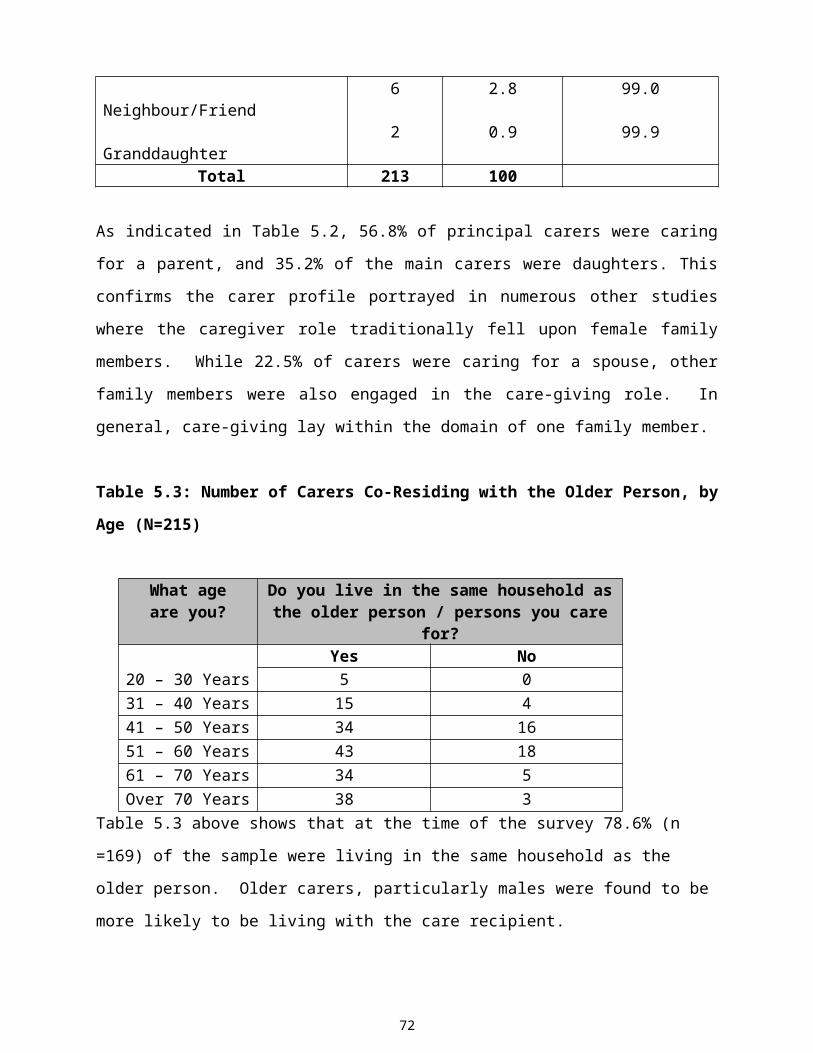
14/05/23 04:43
“They are not really aware of their dependency, although the dependency is there it is not
acknowledged by them”(No. 5, p. 9). Conversely, some carers illustrated the level of
interdependency that can exist between the carer and the care recipient “she helps me and I help
her” (No. 158, p. 33).
5.15.1 Psychological Impact of Care-giving
Many examples of stress among participants throughout the current study reflected the impact of
the care-giving role on carers’ psychological morbidity. Carers described changes in their
psychological well-being as considerably more profound than other aspects of their health. In the
current study, many assertions in previously presented data regarding the magnitude of the
carers’ role found resonance in the present analysis
“The stress is that you are twenty-four hours looking after them” (No. 68, p. 11). This
respondent reported that: “when they are battling with you…you could call them a name…you
could shake them” (No. 68, p. 34). This experience graphically illustrates potential conflicts that
may ensue due to the complexity and intensity of the care-giving relationship. Correlations
between survey and interview data indicate a trend regarding initial problems of adaptation to the
caregiving role (see Table 5.31).
“The first two years were just…I nearly had a breakdown, I was a total wreck trying to
come to terms with it…I would just cry…she wouldn’t even know you sometimes… you
would even turn against them, that’s how bad it can be” (No. 68, pp.5-7), “Now, I can
deal with any situation, so it is not as bad as in the beginning”(No. 68, p. 36).
Throughout this study the level of stress experienced by carers was alarming, “I react and fly off
the handle at times”(No. 122, p. 15). Sleep deprivation was depicted as a particularly
“desperate” factor in the genesis of psychological stress. Also, carers suggested that cognitive
disorders exacerbated the difficulties, sometimes resulting in a loss of control “It is hard to strike
the balance” (No. 237, p. 18). Deterioration in the dependent persons psychological state gave
rise to feelings of social isolation, loneliness, sadness and loss of persons they held dear
throughout their lives
“There is a certain sadness and loneliness, you can’t carry on a conversation, I find that
stressful… I find myself looking back to the days when they were strong and healthy…full
84

14/05/23 04:43
of life, full of joy…I know that is gone forever, but there is a certain sadness there, and
then I kind of feel a bit isolated, a bit lonely” (No. 5, pp. 17-18).
Another carer described the latter scenario as the “worst part of being on your own with the
person” (N. 246, p.27). Other respondent described “not seeing other people, loneliness” (No.
246, p. 23) as a central concern. A carer in his eighties reported feeling
“A bit isolated… depending on neighbours, because they are all working. we are like
passing strangers, you have no transport, that way you cannot see people, so you are
here all night” (No. 158, pp. 5-6).
Throughout the interviews, physical care demands; hygiene issues and increasing care
dependencies were described as stressful
“I look at her not able to get out of the chair to do anything, that is the most upsetting
part of it…nobody kind of cares”, which rendered this carer “very sad and angry at
times” (No. 318, p. 12).
“What worries me most, and I suppose every carer worries about this, how am I going to
cope with a bedridden situation” (No. 5, p. 23).
5.15.2 Socio-Economic Factors
Some carers believed that socio-cultural factors in contemporary society had negatively impacted
on the care of older people in the community:
“It is not like years ago, you would have people coming into your house, neighbours and
so on, but that is all gone, nobody has time anymore” (No. 318, p. 13).
Despite the social constraints associated with care-giving, the loyalty and dedication expressed
by many carers was quite profound. As a lady caring for two brothers explained “I do it not
because I am a carer, but because I am their sister and they need me” (No. 5, p. 29). Another
very young carer reported “I had to give up my job…I would do it anyway for my mother” (No.
68, pp. 3-4). However, this carer believed that “a little more money would help” (p. 13)
particularly for young carers in such circumstances. Similarly, another carer described how her
employment opportunities had been curtailed “I wouldn’t mind a part-time job” (No. 44, p. 6)
stating that “some allowance really is important” (No. 44, p. 38).
85

14/05/23 04:43
Many carers supported an argument for increased economic benefits for carers referring to
government savings where dependants are cared for in home care rather than institutionalised
settings “I must surely be saving expenses in the hospital” (No. 237, p. 1). An overarching
belief amongst carers was “that there should be a concerted policy effort to keep people at home,
but people need financial assistance to do that” stressing the need for “surveillance” (No. 86, p.
23) in the context of carer support services.
5.15.3 Physical Issues
The importance of obtaining an appropriate assessment of carers' skills, abilities, roles and
responsibilities, in consultation with the carer, emerged as an issue of immense importance.
Many carers received “no assessment” (No. 5, p. 22) and found the physical aspects of care-
giving particularly challenging
“It can take so much energy out of you, physically…your mind, body and soul” (No. 68,
pp. 25-26).
Another respondent felt that “there were times when you would be exhausted” claiming that
even at night “you are aware of every sound and every movement” (No. 246, pp. 20-21).
The nature and extent of the physical aspects of care-giving can be particularly difficult for
carers who experience chronic health problems or are older persons themselves. A male carer in
his late seventies profiled his situation stating:
“I have a heart complaint and am a diabetic. My wife is in nappies; she has to be lifted
up in bed in the mornings, washed, cleaned and dressed. I organise her hair and put a bit
of make up on her face. I take her out to the car, lift her in and go to the Priory, where
she goes to church, she has to be lifted into bed like a baby, I do everything on my own”
(No. 318, pp. 4-5).
This man had been providing care for his wife since 1994 and had received no education or
training.
5.15.4 Coping Strategies
86
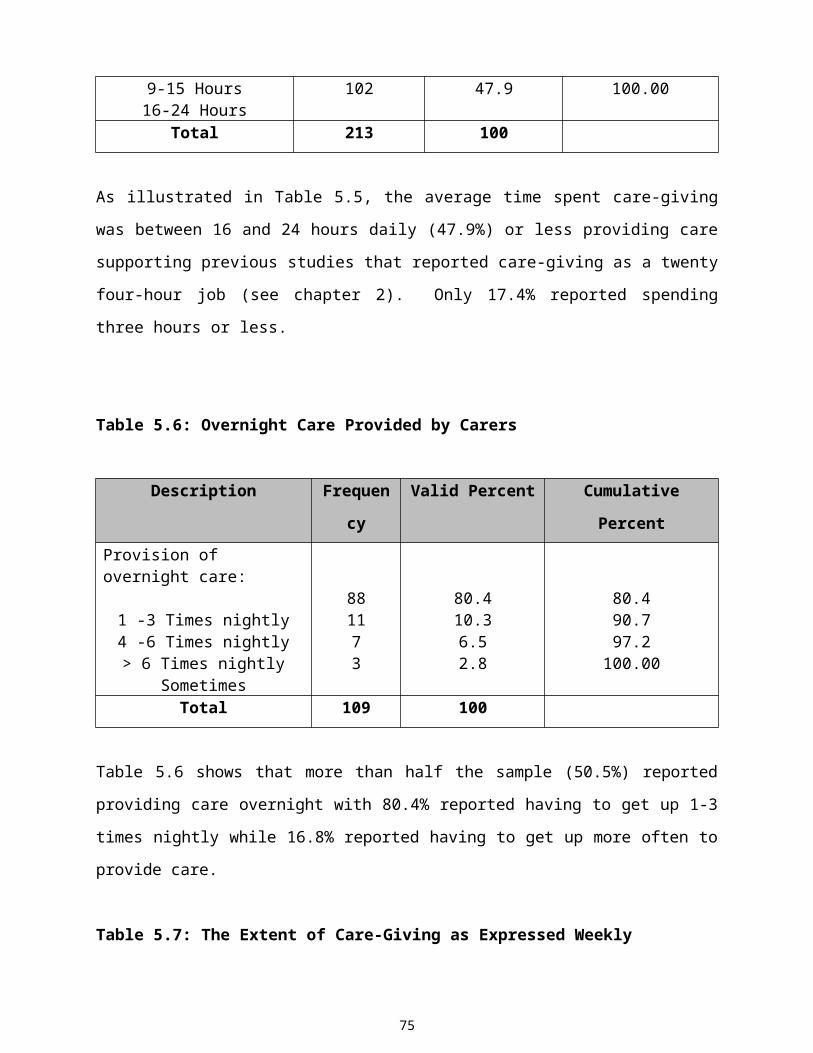
14/05/23 04:43
Many carers suggested that “the support of family” (No. 44, p. 21) was central to coping with
challenges in care-giving, suggesting “You couldn’t do it without them” (No. 246, p. 8). The
latter respondent stressed that in order to cope “to ask for help is probably the best thing you
could do” (No. 246, p. 28).
Carers’ emotional responses and coping strategies were particularly challenged when the older
person appeared unappreciative of their efforts
“Ingratitude is a little bit stressful, I find that hurts…so, I think patience is a virtue that
you need” (No. 5, p. 17).
Such ingratitude is compounded by the fact that many older people refuse to attend support
services “he wouldn’t go to the day-care centre” (No. 237, p. 12) or accept help from anybody
except the carer
“I mentioned would they be interested in having a district nurse on a regular basis, they
don’t want that…they only want me” (No. 5, p. 25).
Similarly, another carer explained that his wife would not accept outside help since “she still
thinks of me as the only one” (No. 319, p. 9). The following explanation was suggested as
contributing to such behaviour
“When they were growing up, all the elderly had no care except for the family…there
was no such thing as respite care or social services…they are all alien things to those
(older) people, intruders into their world” (No. 5, pp. 26-27).
Many participants suggested that “Patience is a thing you would want to have in abundance”
(No. 44, p. 32). This respondent reported the benefits of enabling the older person to live
somewhat separately in an extension of the family home
“You still feel you have your privacy, it’s like two separate houses. I don’t know how I
would cope if she was here all the time I don’t think I would be able to manage” (No.44,
pp. 33-34).
5.16 Positive Aspects of the Carers’ Role
87
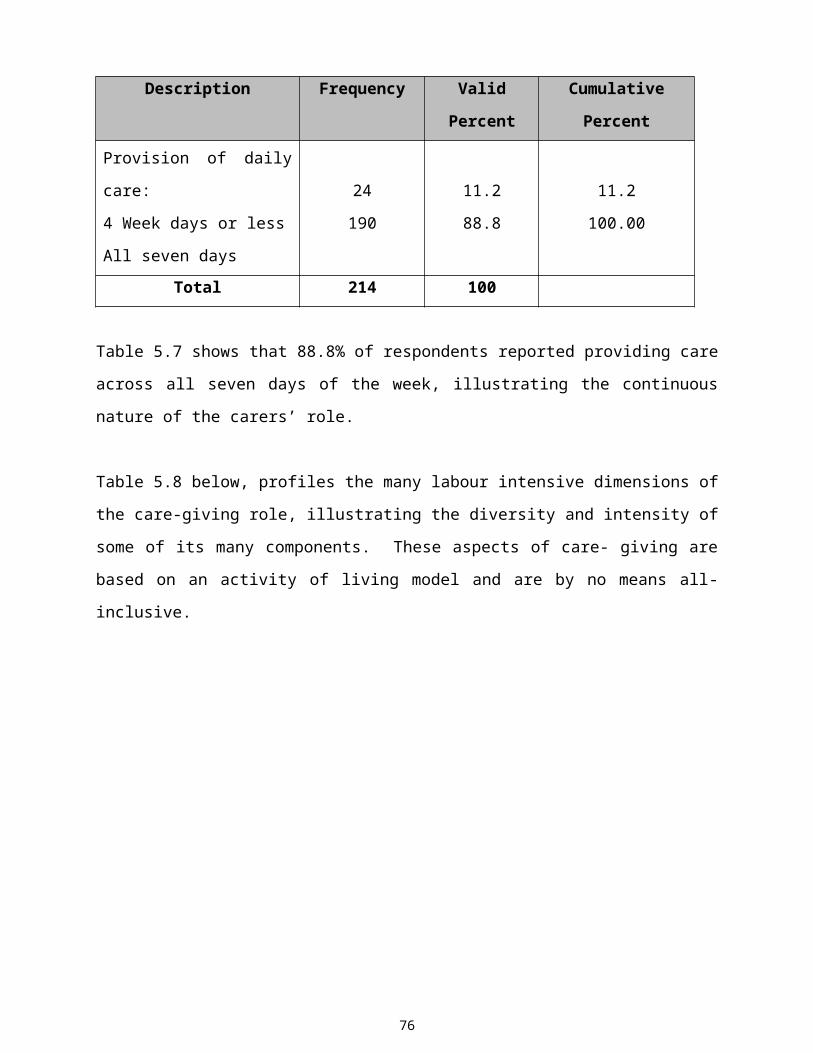
14/05/23 04:43
Despite the high levels of stress evidenced in the present sample, undertaking the caregiving role
was associated with a sense of personal worth and was not necessarily a burden.
“I don’t feel she is a burden” (No. 44, p. 11) adding “I am sure they [the children] will see it
was nice to know their grandparents…being so near to them” (No.44, p. 31). A significant
degree of satisfaction was experienced by the act of giving of oneself
“I am happy to be doing it” (No. 181, p. 6) “she looked after me when I was only a child, and I
am returning the complement…to me, it is important” (No. 181, p. 10). Other carers echoed
these sentiments, especially where institutionalisation could be avoided
“The good side is that you are doing it and you want to do it. Would you rather do that
for your mother or would you rather see her go into hospital…that is my contention…
they are happier in their own environment” (No. 318, pp. 23-24) adding “it has brought
us closer together” (p. 29).
In some ways, the care-giving role enabled carers to gain a deeper understanding of the human
condition,
“It gives me a purpose…I feel it keeps me going…the fact that I have to do something, I find it an
advantage even though sometimes I feel a bit overwhelmed…the demands on me might be fairly
strong…it is part of the fabric of my life” (No. 5, p. 15).
Despite its challenges, feelings of self-fulfilment rendered the care-giving role less onerous and
somewhat rewarding, “I feel I have made a difference to their lives” (No. 5, p. 31).
“I know myself if my mother passed on, I have given everything…I can be fulfilled” (No. 68, p.
19). Similarly, another participant felt that
“ I did my best for her...that would be the big thing...you owe them something and I
wouldn’t have any regrets” (No. 44, pp. 23-24).
In summary, it was thought that “there are more positive than negative, at least you are doing
something for someone” (N158, p. 22). These data correlates well with other results in the
current study as well as recent research findings (Yamashita, 1998, Kellett and Mannion, 1999).
5.17 Impressions of the Adequacy and Efficacy of Carer’ Support Services
88
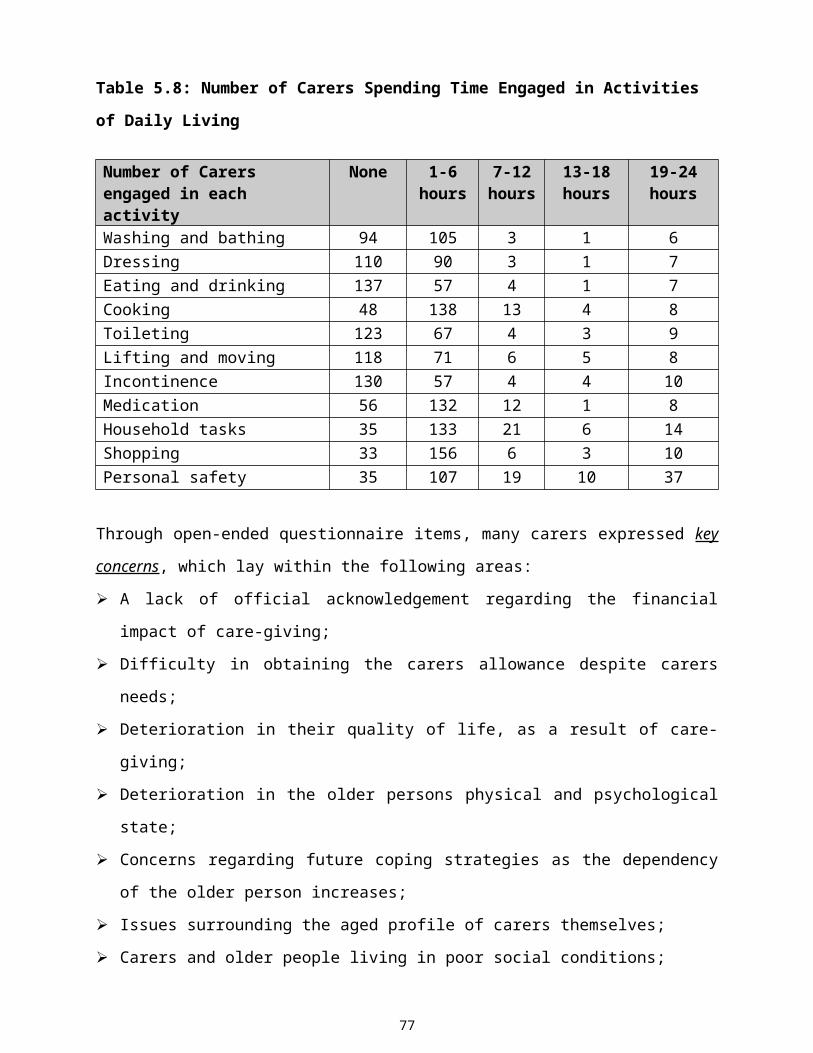
14/05/23 04:43
Interaction with health care professionals was perceived as a matter of considerable importance.
Carers paid tribute to the support received from healthcare professionals
“I find them very, very willing” (No.5, p.6). Although many respondents valued the support of
public health nurses, “she was super, excellent” (No.246, p.2); the need to make “more
resources available to them” (No. 122, p. 14) was recommended, since respondents did not
“think they were calling enough, just to see how you are” (No.318, p.7) and “should call more
often” (No.181, p.3). Nonetheless, public health nurses were seen as “very approachable”,
providing “the main contact” between carers and health care services (No.158, p.14).
“The nurse is very good to her…if I needed anything there would be no problem…it is
fantastic to have her calling” (No. 44, pp. 8-9).
Conversely, the support provided by some health care professionals was described as “minimal”
(No. 86, p. 6). Some carers described the management of services for carers as a process that
lacked proactivity and health promotional opportunities
“The specialist said I thought it was agreed that you would only come back to us if you
couldn’t cope or if there was a major problem” (No. 86, p. 12).
Services primarily targeted at increasing dependencies may indicate a lack of preventative
measures directed at promoting the health of both the carer and the older person. The
contribution of the voluntary services was acknowledged. Consistent with focus group and
survey data, the importance of supporting and promoting voluntary agencies was clear
“They deserve support…they are the people who deal with old people…they know what
appeals to old people” and should be “consulted” (No. 122, p. 19-20)
The significance of respite care, residential and long-term supportive care interventions was
highlighted across all interviews. Respite services were described as “vital” (No. 122, p. 12) in
enabling carers to maintain and sustain their care-giving role. This carer expressed the view that
respite care enabled him to exercise more control over his life “at least you would be free to get
up whenever you wanted…just small things like that” (No. 122, p. 12). Another carer stated that
without respite care
89

14/05/23 04:43
“I would say I would go nuts… I may not go, but I like to know I can go” (No. 246, p. 21).
Yet, many carers reported that they had “never” been offered respite care. Where carers did
avail of a break, some claimed that they “depend on our neighbours” (No. 44, p. 18) to do so.
However, there was evidence of reluctance to take a break when
“all she wants is to see me walking in the door and I do feel kind of guilty” (No. 318, p.10).
Some carers believed that current services were “limited” (No. 122, p. 27) and should be more
flexible, thereby providing “another bit of freedom” (p. 28) for carers experiencing social
isolation or loss of control over their personal lives. Other carers in similar situations conveyed
feelings of being trapped both physically and emotionally, in their care-giving role
“It is devastating really…you are bound and you are caught” (No. 68, p. 8) “… you feel
hemmed in and trapped at times” (p. 23) “…I am still young…it affects your social life” (pp.
30-31).
“Your privacy is gone ...I find that very hard.” (No. 44, p. 3) “…you are very tied”, (No. 44, p.
9) suggesting that loss of privacy and independence can impact negatively on family dynamics.
These feelings were exacerbated when carers felt isolated and abandoned by a system, which
failed to provide any meaningful acknowledgement or recognition of their efforts.
“I think it is just taken for granted…this job is done by families and in the end it is
forgotten by people in authority” (No. 44, p. 40).
Consistent with the previously detailed analyses, stressful aspects of the financial aspects of care-
giving were evident. A number of carers reported a lack of awareness regarding the carers’
allowance and related eligibility criteria
“I find nobody tells you anything, what you are entitled to” (No. 318, p. 25), while another carer
asked, “would you have to pay for them” [day-care services] (No. 181, p. 19).
A carer in his eighties, thought the means test was “disgraceful,” (No. 158, p. 2) adding
90
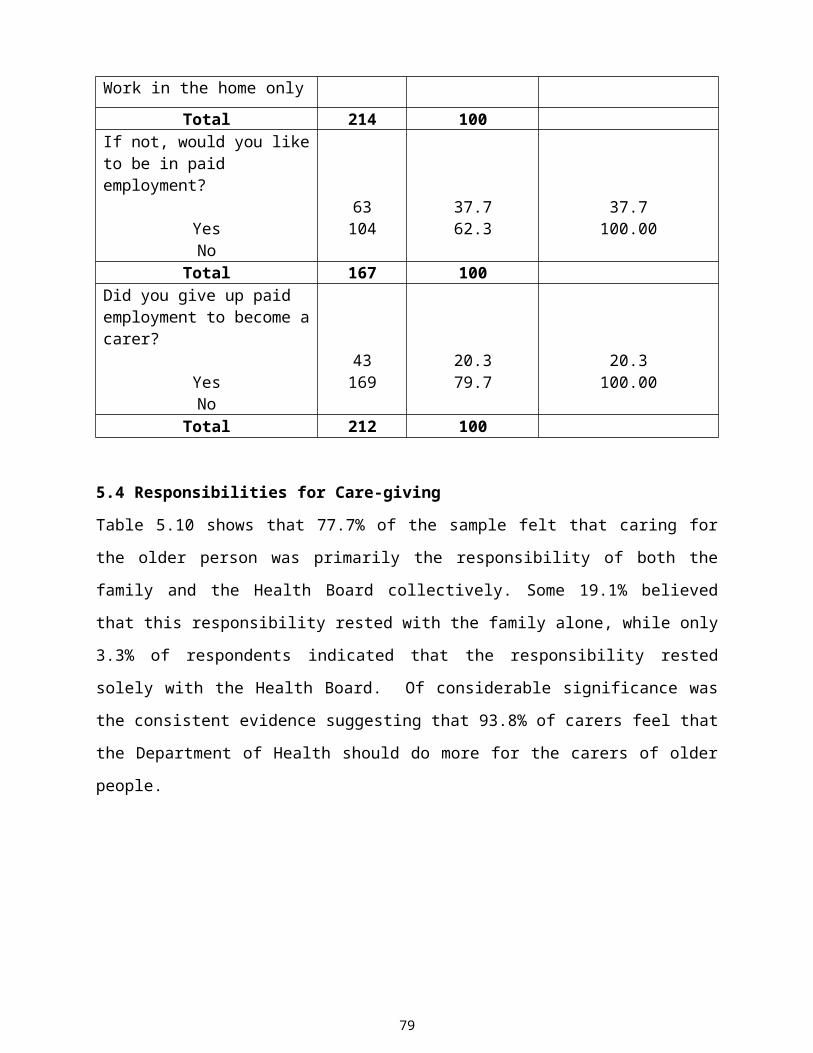
14/05/23 04:43
“You should be entitled to facilities and I don’t think that is too much to be asking of any
government in your old age, having made their contribution to society” (pp. 30-31).
Carers expressed frustration and hopelessness arising from a lack of information and the
inadequacy of statutory respite care and other support services
“I have asked before, what kind of help is available and I still haven’t got any real
answers, there are lots of things I believe that you can get that you don’t know about”
(No.318, pp.7-8); recommending “there should be leaflets given out every so often…just
to show them that there is someone around” (No. 181, pp. 26-27).
“I think a local authority or government should be there in a back-up situation…a
consultative type role would be good, where you can get guidelines” (No. 5, p. 2).
The lack of statutory support services was such that carers reported that “anything you want you
have to look for” (No. 158, p.4). Furthermore, “transport is the main thing” (No. 158, p. 33) that
mitigates against accessing support services, in rural areas.
Some carers felt that obtaining essential appliances and supports was laden with bureaucracy,
“red tape and hassle, I was told there was a twenty four month waiting list for an Occupational
Therapist to come to an eighty year old” (No. 246, p. 2) adding “I made seventeen phone calls
before I eventually got an answer” (p. 5).
Many carers found that involvement in this research study raised their awareness of the
significance of their role
“I am thankful for this opportunity of being able to identify myself” (No. 5, p. 35), while another
respondent felt that the research indicated to him “that there was someone starting to do
something for us” (No. 181, p. 25). It was thought that the current research project assisted in
making carers
“more aware…I suppose I wouldn’t have thought anything about this until you sent out
the questionnaire. we wouldn’t really have known where to turn…” (No. 44, pp. 35-36).
91
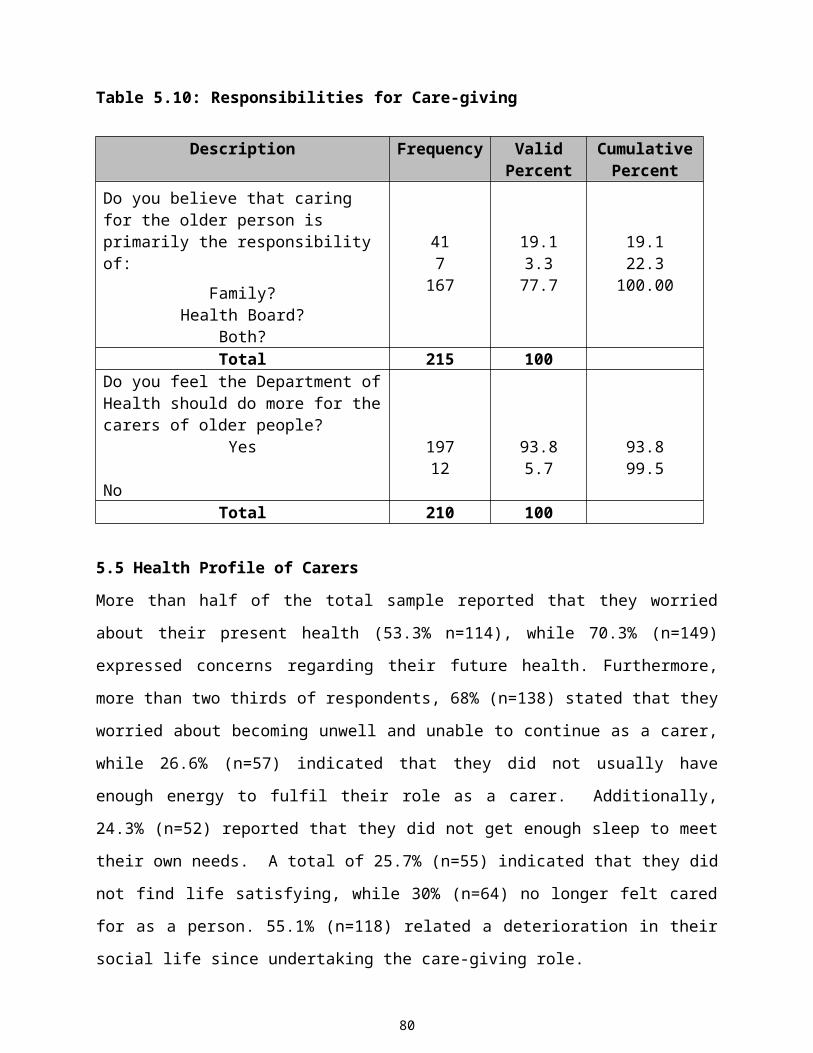
14/05/23 04:43
5.18 Care Planning
All three data collection procedures reported no evidence of discharge planning or any form of
needs assessment in order to secure the successful transfer of care from institutionalised to home
care settings. The latter findings found support in the present analysis,
“I think people should be assessed” (No. 68, p. 37).
Another respondent portrayed somewhat fragmented, uncoordinated service links
“There is no correlation between the hospital care and being put back out into the home” (No.
86, p. 13).
Additionally, the importance of planning the provision of care amongst family members was
emphasised, suggesting that forward planning could enable family members
“To lay out a routine from the beginning…if you could have time beforehand to discuss it with
other family members…” rather than having “it thrust upon us” (No. 120, p. 170).
“If you can anticipate and you can plan, I think it is half the battle” (No. 5, p. 24). Other carers,
referred to the need for “a more proactive role” (No. 86, p. 22) to be taken by statutory bodies.
In consulting with and assessing carers’ needs, “there should be an effort to find out the carers’
point of view” (No. 86, p. 14). Other carers suggested that
“If somebody did call, ask them how they are coping. of their own accord …just the fact
that somebody called, you feel somebody cared about the person looking after them”
(No. 44, pp. 36-37).
“For the government to move forward, they need plenty of information…every
household, every carer and every older persons’ circumstances are different…so, they
have to be surveyed” (No. 68, p. 38).
5.19 Education and Training
A considerable lack of training for carers in relation to lifting and handling skills was identified.
The need “ for somebody to come along and show them [carers] what to do and what not to do”
92

14/05/23 04:43
(No. 246, p. 30) was deemed important, particularly in “families where they wouldn’t know how
to cope in a particular situation”(No. 86, p. 22).
Concerns were also voiced regarding a lack of monitoring and support for carers, where new or
altered medication had been introduced, “there is always a danger on tablets, if you got a bit of
guidance it would help” (No. 122, p. 18).
93

14/05/23 04:43
CHAPTER SIX
6.0 Introduction
This study represents the first attempt to study a sample of informal carers within the South
Eastern Health Board area. Since the self-administered questionnaire was distributed to a sample
drawn randomly from a limited geographical area, results may only be generalised to similar
populations. Furthermore, interview results are not generalisable. Nonetheless, this study
presents substantial information in an area of health and social care, the extent of which has not
been previously investigated comprehensively in Ireland. This chapter includes a discussion of
these results.
6.1 Carer Language, Definitions and Interpretations
Issues surrounding the identification, definition and language used in reference to carers requires
further clarification amongst health care professionals and carers themselves. Perceptions of the
role do vary, giving rise to considerable ambiguity. This highlights the importance of identifying
inclusion criteria that constitute a common approach to the identification of carers. However,
such a definition will not clarify varying perceptions amongst informal carers who see their role
as a 'duty' or responsibility that does not ‘fit’ with their perceptions of the ‘informal carer’ label.
From a sociological perspective, the culture of care-giving was found to be a factor across rural
and urban care settings, influencing how both carers and care recipients perceived care-giving
roles and responsibilities as well as the relevance and significance of supportive services.
Therefore, the meaning that carers and older people attributed to care-giving in all its dimensions
was influenced significantly by the culture of the study population. The service implications of
such cultural sequelae require careful planning in terms of development and supportive
interventions.
6.2 Exploring the Nature and Extent of Care-giving
Analysis of the data sets reveals a correlation between factors such as loss of control, social
isolation, loneliness and self-fulfilment. The tiring nature of the physical aspects of care
provision was a key concern. Ongoing elevated levels of psychological arousal, particularly at
night may exacerbate carers’ stress levels. Indeed, mental frailty was deemed a matter of greater
concern than physical dependency. Evidence of increasingly older carers, decreases in the
numbers of available carers, coupled with changes in family structure and responsibilities for
94
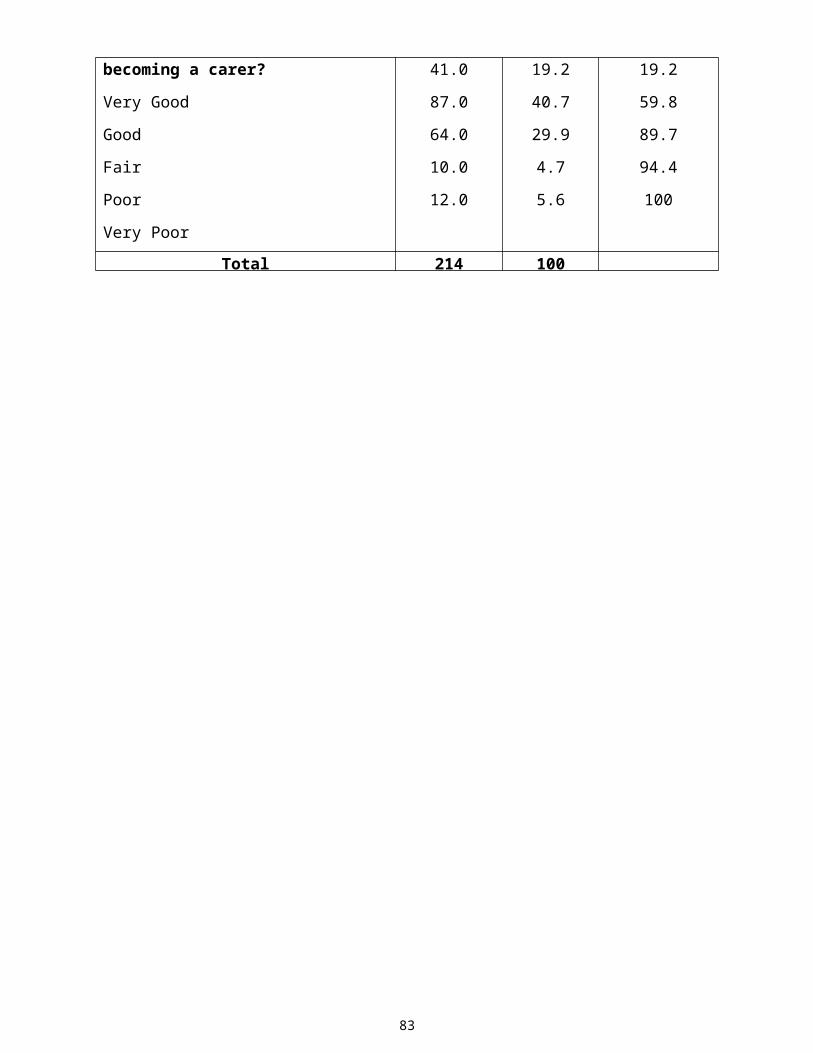
14/05/23 04:43
care-giving may impact negatively upon the feasibility of home care in some areas. One carer
suggested the need to advocate so that families “share the care”, in an effort to reduce the so-
called burden of care upon individual family members.
These findings illustrate the nature and extent of informal care-giving, highlighting the
magnitude of the care-giving role, the impact of which can exert transformational changes in
carers' lives. Positive aspects of the care-giving role suggest that it is not perceived in
predominantly negative terms. However, carers’ perceptions of their caregiving role impact upon
the negative and or positive perspectives they attribute to it. The central factors underpinning the
direction of carers’ perspectives include:
The demanding nature of the carers’ role;
The quality of the carer/care dependent relationship;
Changes in the carers’ personal life;
Feelings of guilt;
Loss of control;
Family dynamics- the level of supportive interventions;
The adequacy and appropriateness of professional and statutory supports.
6.2.1 Needs Assessment: Procedures and Policy
In the interest of the common good, issues regarding carers in the community must be held in
balance with broader issues such as individual human rights, citizenship and ethico-legal matters.
Carers are part of a much more extensive system in society made up of many marginalised
groups. Yet, many felt that their own unique needs had become somewhat subsumed and
overshadowed by those of the care recipient.
Consistent with similar research, clear indications emerged as to the importance of identifying
and applying structured, holistic approaches in determining the type of support carers received.
This was essential in order to inform service plans and deliver timely and appropriate supportive
interventions. The importance of assessment measures is clear, given the broad spectrum of
dependency levels and caregiver needs. The assessment process defines needs and determines
carers' eligibility for support as indicated by predetermined stated policy criteria. However, there
is evidence of widespread failure in the conceptualisation of the care needs of older people;
95
14/05/23 04:43
especially the very frail (Nolan et al 1996). Furthermore, there was no evidence in the present
study of any guidelines or structures in relation to addressing carers’ needs. Specifically,
evidence of involving carers in care planning initiatives; setting targets towards the development
of appropriate service plans and evaluation processes was negligible.
The findings portray the importance of assessing carers’ needs in a structured co-ordinated
manner, amongst the multidisciplinary team. Exploring the interplay between carers perceived
stressors; expressed needs and coping mechanisms are key factors associated with maintaining
and sustaining the care-giving relationship. This is an issue of considerable importance both in
terms of the quality of services provided and health economics in respect of the balance of care
between primary and secondary care sectors However, there are clear indications of tensions
between fulfilling carers’ perceived needs for supportive services where conflicts emerge
between the carers’ perspective and that of the care recipient. Such differences and resistance
from older people themselves may militate against carers’ options in seeking health and social
supports that they perceive as necessary in order to sustain and maintain the care-giving role.
6.2.2 Support Services
Many innovations in home care have lacked evaluation (Challis, 1992). The principle of
providing appropriate levels of practical, psychological and socio-economic support was
evidenced by the findings of this study. It is a matter of substantial importance in the
development of a service distinctly orientated towards carers' needs. Indeed, the success of such
initiatives may influence carers’ capacity to continue care-giving; a matter on which the bulk of
community care policy depends.
The introduction of strategically planned interventions aimed at providing carers with effective
support systems may emerge from exploration and understanding of the impact which care-
giving exerts on carers’ lives. There was a general consensus among carers that the management
culture within the statutory services was such that there was a lot of 'red tape' and bureaucracy
associated with obtaining services. Carers’ perceptions of the degree to which statutory
healthcare agents understand their needs resulted in a wide range of sometimes disparate opinion.
While one survey respondent commented, “I don’t think they understand the commitment we
undertake”, yet another expressed the view that “professionals should present a package of
information carers need”. However, another carer stated that “any professionals we meet are
96

14/05/23 04:43
sympathetic to our case”, while another believed that although professionals understand carers’
needs “they don’t have the resources to provide the level of care that they know is required”. A
considerable reorientation of service structures would appear to be warranted if carers are to
receive the support they require.
Almost half the sample indicated that they would like more support from healthcare
professionals. Carers’ perceptions as to the most valuable contributions of health care
professionals highlight the perceived importance of interactions with public health nurses.
Some carers indicated that they were unclear about the differing roles of home helps and home
care assistants. The lack of availability, flexibility and continuity in terms of day-care and respite
care was a key concern since care-giving was widely expressed as a twenty four hour job, by
almost half the respondents surveyed, 89% of whom provided care seven days a week. Of those
surveyed, 41% were unaware of day-care services. In relation to respite care, two-thirds of carers
reported that they had never been offered respite care, while a further third who had been offered
respite care but did not avail of it, expressed the following reasons for non-acceptance:
The care recipient would refuse to go as they wished to remain in their own home;
Some carers stated that they were able to cope with the help of family and wished to maintain
the management of care within the family unit;
A common theme that emerged related to the carers’ belief that the older person envisaged
staying in their home as synonymous with retaining their independence and dignity;
Some carers stated that they were unwilling to allow the older person to avail of respite care
due to feelings of guilt, where they felt the older person might feel unwanted.
These findings have significance for the provision of respite care to carers. Carer stress may be
exacerbated rather than reduced where carers’ perspectives regarding supportive interventions are
ignored. Consistent with previous research, high quality support and respite services must be
planned in consultation with carers, and acceptable to both the carer and the dependent person
(Nolan and Grant, 1992; The Audit Commission , DOH; 2000). Reported low levels of service use
may be further explained by a lack of awareness of services coupled with a lack of knowledge as to
how to access such services. In a DHSS (1996) survey conducted in Northern Ireland, 42% of
respondents reported never having had a break from the caring role. Many carers expressed feelings
of guilt when they suggested respite care to their dependent. In such cases the burden of guilt was
such that respite was just not an option.
97

14/05/23 04:43
More than half the carers in the current study reported having no knowledge of financial services or
allowances available to them. Furthermore, carers reported that family and friends were a greater
source of information than the media or their family doctor. Many studies suggest a lack of
information as the main reason for non-utilisation of services (Dello Buono et al 1999). Some 70%
of carers in the former study reported feeling isolated in terms of their lack of knowledge regarding
available resources, stressing that they did not obtain enough information on services available to
carers. A similar rationale may underpin the poor uptake of services in the present study since two-
thirds of the sample claimed that they did not receive enough information to support them in their
care-giving role. The general experience was that services had to be sought after rather than offered
in a user-friendly manner.
Importantly, the more hours spent caring daily and the longer carers engage in the care-giving role
without a break, the more social isolation they are likely to experience. Feelings of social isolation
and loneliness may decrease the carers’ potential to continue in their role. Furthermore, carers who
did not receive breaks of a week or more experienced less fulfilment than those in receipt of a break
from the care-giving role. This is an issue of extreme importance since one third of respondents
indicated that they had never received a break from their care-giving role. Clearly, due consideration
must be afforded to these factors if effective, appropriate respite services are to be offered.
6.2.3 Profiling Carers' Health
The magnitude of the care-giving role exerts a significant impact upon the carers’ life, often
requiring substantial adaptations in response to a range of transformational changes. Physical,
psychosocial and economic demands influenced carers' responses to the caregiving role. Feelings
of stress were most commonly encountered where carers felt isolated, trapped or unsupported.
Carers reported deterioration in their physical and emotional health. Profound effects were also
expressed in areas of social and family life. More than half the sample expressed concerns about
their current health, while more than two thirds were concerned about their future health and
their ability to continue care-giving. While there were perceived effects upon these aspects of
carers' lives, it is difficult to determine the precise strength of association since other
confounding factors such as personal changes in the carers' life pattern may have influenced
these findings.
Carers adopt a broad range of coping behaviours including, problem-solving techniques and
cognitive coping mechanisms in attempting to manage stress and psychological burden.
98

14/05/23 04:43
Understanding the coping strategies employed in dealing with challenges in care-giving is central
to the development of carer-oriented support services. Analysis of positively and negatively
perceived aspects of care-giving evidenced significant correlations. The dimensions explored
embraced carers’ expressions of self-fulfilment, loss of control and social isolation and
loneliness. Consistent with a similar Swedish study, receiving more information and training for
the care-giving role was perceived as enhancing carers' ability to cope (Lundh, 1999).
Furthermore, a cognitive factor which influenced carers ability to cope, both in the latter and
current study was their ability to reflect on good past experiences with the care recipient. This is
consistent with UK research by Nolan et al (1996) who examined multidimensional aspects of
care-giving and coping. They found that carers reported that obtaining as much professional help
as possible was a particularly useful problem solving approach. However, in the present study,
there was a tendency to report relatively low expectations from professional services. This
phenomenon was also reported by Lundh (1999) who postulated that such low expectations may
occur as a result of a sense of independence amongst carers or a relative lack of available
professional support structures. In the present study, data detailing the frequency of interactions
with health professionals provides considerable evidence in support of the latter contention.
Furthermore, such low levels of interaction reduce opportunities for engaging in health
promotional and carer empowerment initiatives.
6.2.4 Health Promotion Factors
A client-centred approach is crucial to the promotion of health and social gain for carer and
dependent alike. This is in order to support the autonomy of the older person and their carer and
to remain supported in their own home with dignity and independence. Health promotional
initiatives may enable carers to attain a sense of identity and self esteem. Raising the profile of
the role, responsibilities and the meaning of family caregiving may enhance carers’ self belief
and confidence. This will help support the continuity of the home caring process and embrace the
protection of family life. Whilst there are stresses and strains inherent in family caregiving, there
are also therapeutic aspects of the role that may nurture carers’ ability to cope with the more
demanding components of family care. Indeed, some carers valued and enjoyed their role.
Nonetheless, the need for health professionals to provide adequate emotional support and
personal contact is imperative, in addressing a wide range of emotional responses.
99
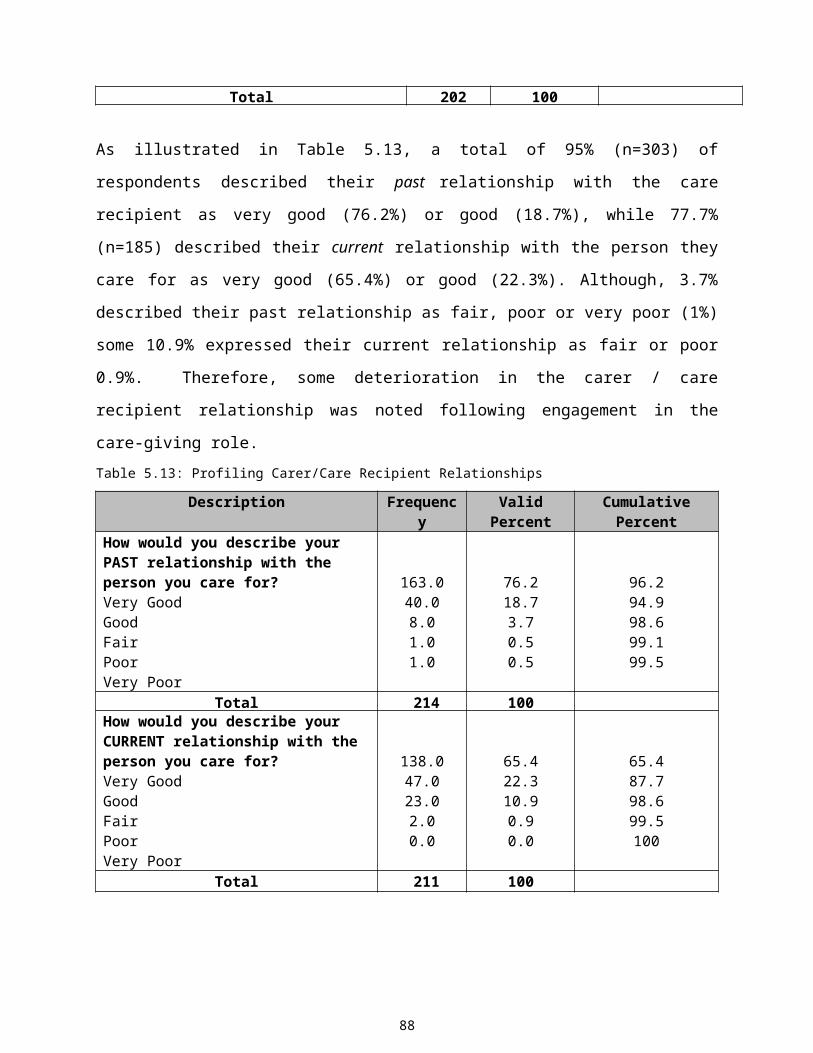
14/05/23 04:43
Advancing the health and social care needs of carers and the recipients of care requires this level
of willingness and engagement. Concerted action, targeted resources and clear policy must be
enacted, within a clear framework. Successful needs assessment measures will require sensitive
eclectic approaches that reflect the perspectives and perceived needs of both the carer and the
older person. Mechanisms for collaborating with and empowering family carers is the ultimate
objective in terms of user/carer involvement in service planning and evaluation and may enable
family carers to ascribe new meaning to their experiences.
6.3 Conclusion
The main themes and categories arising from the data analysis were similar across all three data
sets. They also found resonance with findings in the main care-giving literature. These data
indicate trends in relation to carers’ needs and experiences as well as coping and mediating
factors pertaining to health, wellbeing and stress related outcomes.
This high degree of consensus across the data sets, coupled with the pluralistic approach to
research enquiry engendered greater confidence in the relevance and empirical value of the
findings. Given the distinct differences inherent in both the qualitative and quantitative
methodologies, the congruence between the analyses of the three data sets, further augments the
validity and reliability of the overall findings.
The need to raise awareness of carers’ issues among private and public service providers, media,
government and social partners is of considerable importance. Attitudes to carers need to be
examined, so that caring may be seen as a normal feature of many people’s lives. Voluntary and
non-governmental organisations can play a significant role at local level in promoting awareness
and information, using campaigns tailored to local circumstances. This is important in the
context of the decentralisation of services to delivery at local level, based on agreed national
standards. The balance between formal and family care must shift. There is a need for change
that reflects continuity and diversity in a co-ordinated and integrated manner. The challenge is to
establish and introduce appropriate and meaningful health and social policy initiatives to support
that shift.
Strategic assessment and monitoring of such important issues may enable the publishing of
functional and comparative benchmarks, which set out a clear view of the available services.
100
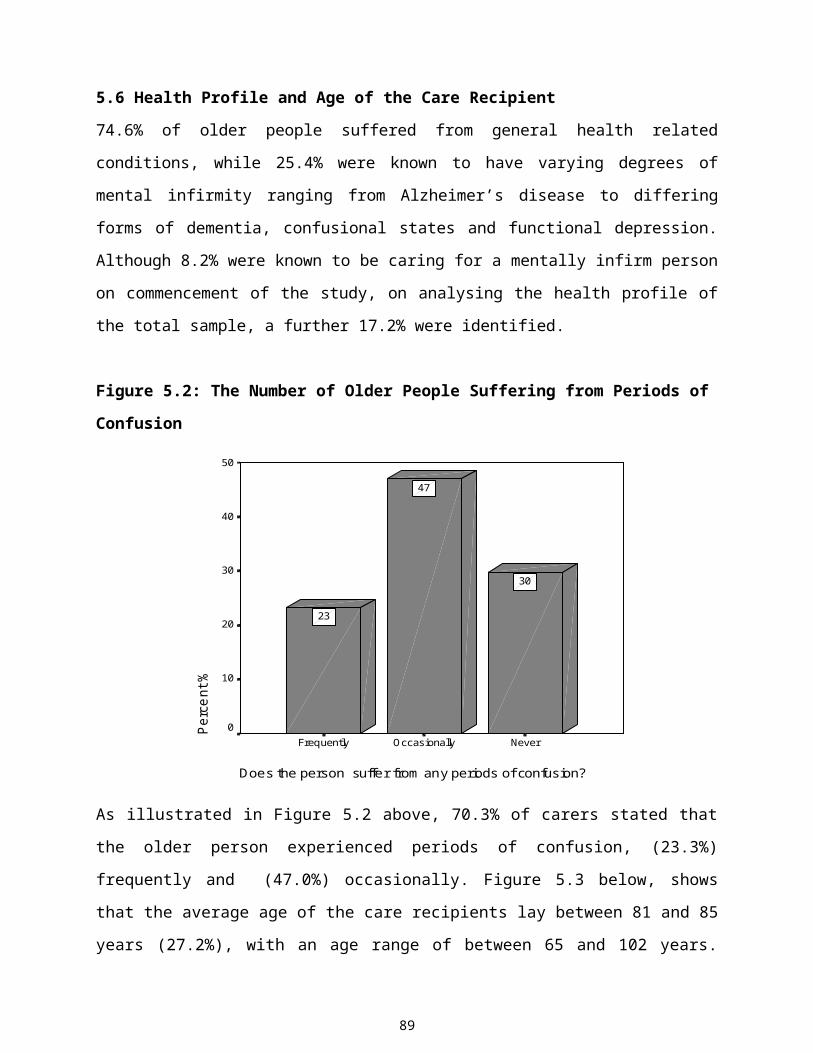
14/05/23 04:43
Policy development ought to possess sensitivity such that it can inform interventions for
individual caregivers and their dependants. This is an important issue in regard to addressing the
diversity of need amongst carers and those they care for, in an effort to adopt a more inclusive,
eclectic approach towards prospective innovations in health and social care policy formulation.
This study is not without its weaknesses and limitations. It is acknowledged that there may be a
number of ‘hidden’ carers with significant health and social care needs that have not been
explored. As discussed in chapter three, accessing hidden carers proved extremely difficult.
101
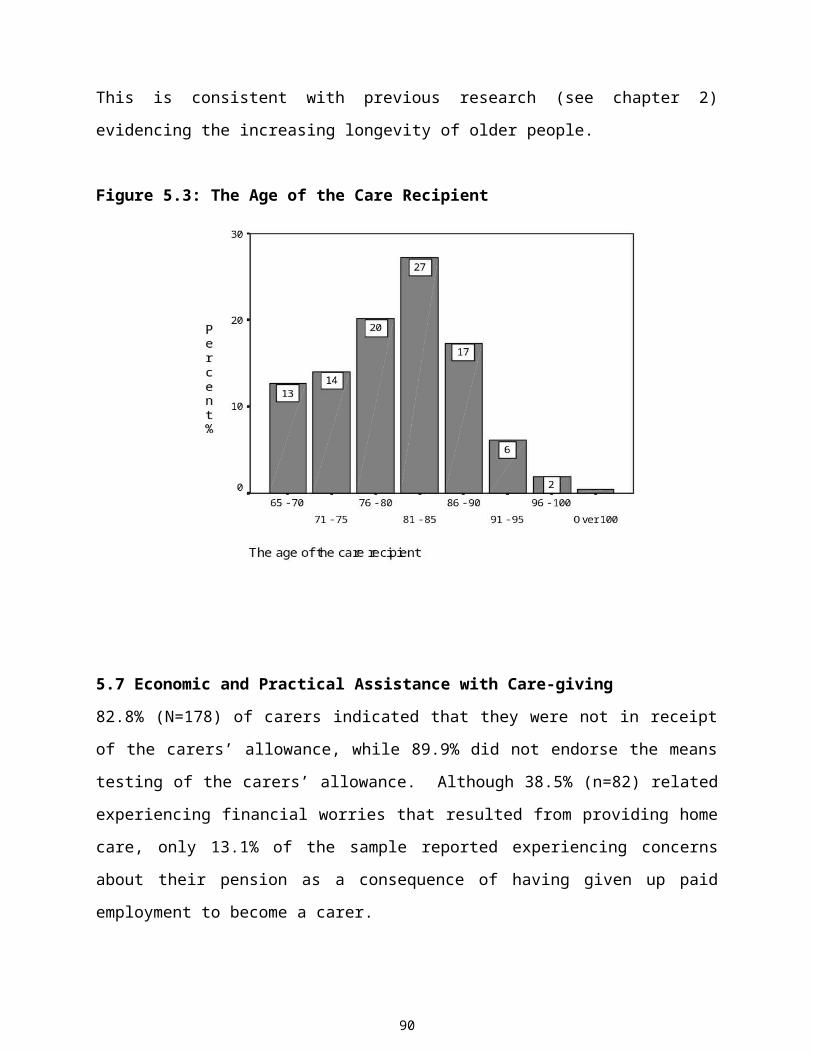
14/05/23 04:43
CHAPTER SEVEN
7.0 Introduction
The final chapter outlines conclusions and recommendations from the results of the study in
association with previous research findings. Central to the understanding of carers' needs and
experiences is an appreciation this diverse group with individual abilities, tolerance levels, values
and approaches to caring for older people. Their own needs and wishes display a similar degree
of disparity. Informal carers have been and continue to be hugely significant partners in the
totality of the health and social services provided to older persons. Nonetheless, consistent with
previous research, formal support services are often only employed when a crisis is reached,
informal support is unavailable (Fine and Thompson, 1993, Nankervis et al 1997) and the strain
of care provision becomes unbearable. Evidently, the ability of healthcare providers to convey
their understanding of the needs, experiences and significance of family care-giving is a key
issue in determining carers’ perceptions of the involvement of statutory and professional bodies,
as empowering and supportive or intrusive and negating (Nolan et al 1995).
The consultative nature of the current study led to the production of reliable and valid data on
which appropriate needs-orientated health service plans may be based. Attempts to consult with,
and take guidance from the carers themselves may help to build the trust and co-operation of the
respondents, thereby enhancing the potential value of this research project. It is anticipated that
the data produced will enable carers to make a valuable contribution to service planning at local
level, through having a voice at the corporate table.
7.1 Implications for Service Planning
The need for improvement and change is evident and may encourage a more positive vision of
ageing and caring for older persons. Both qualitative and quantitative data produced
corroborating evidence as to the complex and diverse nature of carers’ needs and experiences.
Contributory factors in the genesis of care giver burden as well as carer satisfaction indicators as
central to understanding the totality of the care-giving experience. In order to maintain and
sustain the future of informal care-giving, carers’ needs must be explored and addressed locally,
at service and policy level in an effort to promote their health and social gain.
Analysis of the main study findings produced comprehensive data, which may inform the
planning, and delivery of services for older people and their carers, towards benchmarking
102
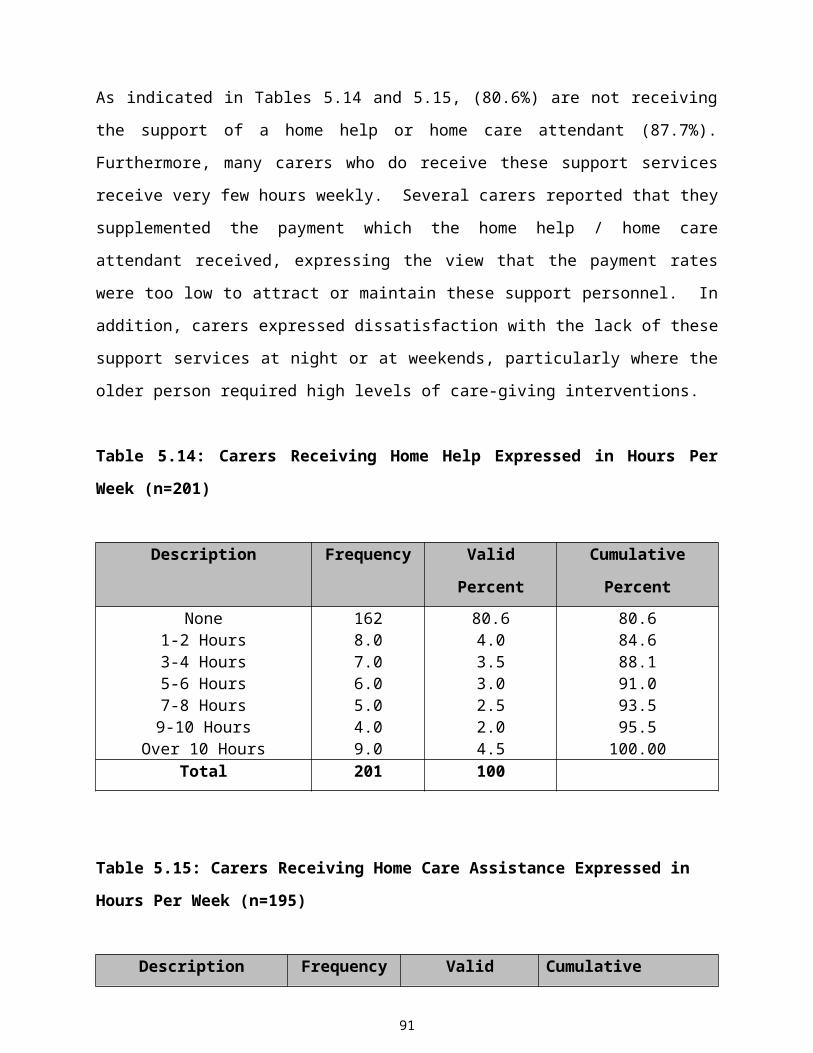
14/05/23 04:43
models of best practice. A major theme that emerged from this study uncovers the magnitude of
the care-giving role, the totality of which exerts significant effects on carers' health and
wellbeing. To this end, 94% of respondents felt that the government should do more for the
carers of older people. The identification of carers’ needs and experiences of existing health and
social care services suggests the importance of ongoing monitoring and evaluation of the
efficacy of service structures, delivery processes and outcome measures. Assessing carers' needs
encompasses a range of needs including biological, psychosocial, economic, technological, and
informational and health promotional issues as well as palliative and terminal care concerns.
There are clear indications that health and social care service planners and providers must re-
orientate service delivery strategies in order to meet user needs and subsequently, avoid or delay
the unnecessary institutionalisation of older people.
Despite the sometimes incessant demands of the care-giving role, most carers reported a lack of
support services and respite care. The need for appropriate supportive interventions was widely
expressed. Most carers wish to delay or avoid the institutionalisation of older people, perceiving
home care settings as the optimal care-giving environment. Many welcome supportive initiatives
in the community, expressing preferences for greater scope and flexibility in the development of
supportive interventions. Specifically, carers’ preferences for in-home respite services were
conveyed. Furthermore, health service planners and providers need to take cognisance of carers
coping patterns in attempting to develop appropriate support services. The level of interaction
between statutory services and carers requires exploration, monitoring and evaluation. In
acknowledging carers' needs and experiences, it is important that statutory care agencies develop
new and innovative service plans in response to their continuing health and social care needs.
Education and training programmes should be established for carers in preparation for the care-
giving role. Clearly targeted policy embracing systematic tracking, assessment, planning,
intervention and evaluation processes is integral to the development of proactive service plans
that address carer centred needs.
7.2 Implications for Policy
These finding contribute significantly to the evidence base exploring carers’ needs and
experiences. The data has policy implications for the targeting and delivery of services. The
implications of an aging population, for both living and working conditions, require careful
consideration. Considering and consulting with the service user in planning, monitoring and
evaluation processes is crucial to the promotion of informed and realistic choices. The
103
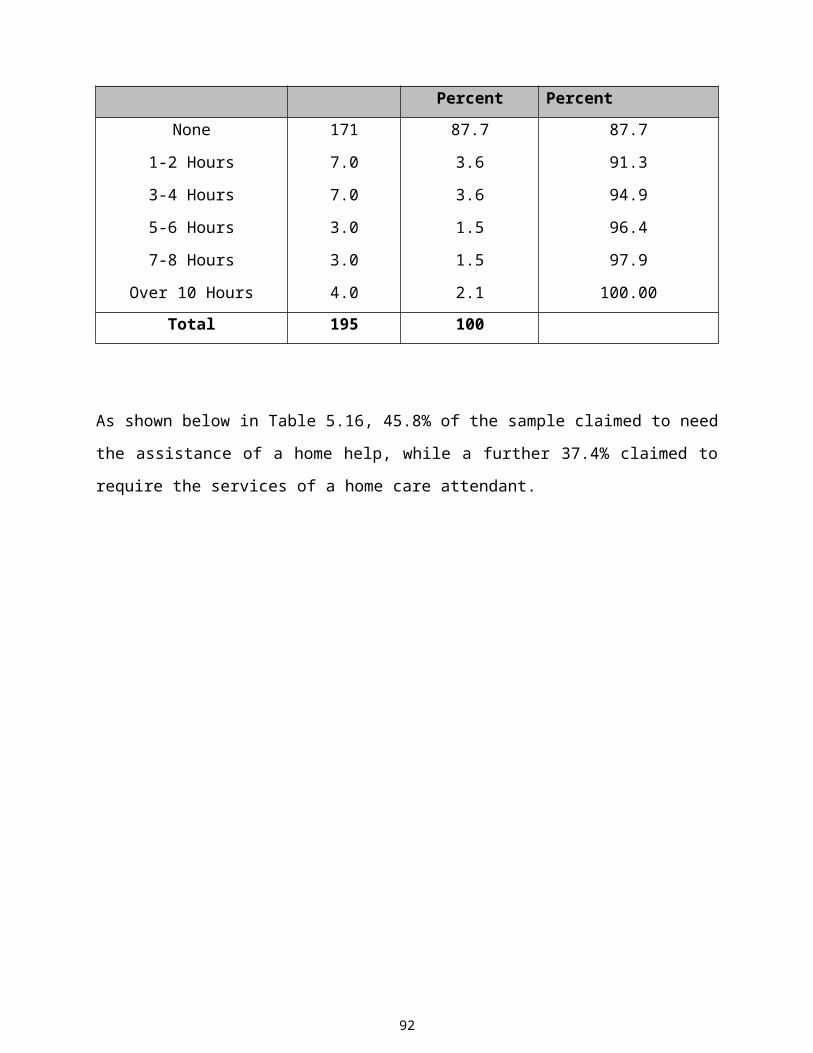
14/05/23 04:43
development of ‘shared purposes’ is an issue of central importance in enhancing and improving
informal carers’ personal well-being and quality of life, in the promotion of healthier
communities and in the development of public health policy. The interface between health care
and social care is an integral component of planning, assessment, care management,
commissioning, and service delivery strategies (Department of Health, 1989). Relevant
government departments should make explicit their policies in relation to informal carers. Such
policies must recognise and acknowledge carers as individuals with distinct needs and abilities.
Inadequacies at various points of the care spectrum can inhibit choice about care options,
resulting in inappropriate care placements, over medicalisation and institutionalisation (Dello
Bruno et al 1999). The distribution of resources requires collaborative, cross-sectoral, co-
ordinated planning across categories such as age, illness and social grouping. The distribution of
resources such as economic supports and allowances warrants further policy review. The
anticipated continuing demands for family care, necessitate the integration of carers’ needs and
perspectives in future service planning and decision making networks, in partnership with
statutory and voluntary bodies. Cross-sectoral co-ordination and partnerships are imperative in
this regard. Furthermore efforts to redress the health and social care divide are required. The
primary objective of ‘adding life to years’ as well as adding ‘years to life’, as set out by The
World Health Organisation (1996) must prevail as a matter of the utmost importance in creating
a vision of caring for older people in the years ahead. One of the most profound challenges of the
next century will be to extend the ‘ health span’ as the ‘life span’ increases. Improving the health
span of older people may promote the independence of older people for as long as possibly,
thereby reducing the demand upon family carers in terms of intensity and dependency levels.
7.3 Recommendations
Meaningful practice and policy changes, directed and informed by current advances in the
evidence-base world-wide are required in order to redress service practice divides. If the meeting
of needs is to be democratic, open debate on the subject of carers’ needs is imperative. This
means that the process of needs assessment must be conducted in a manner where carers are
enabled to participate fully in decision-making about services. One of the most important factors
involved in meeting the needs of carers include the provision of information, which enables them
to seek appropriate help and improve the quality of their lives in order to care more effectively.
There was profound lack of awareness amongst carers regarding entitlements, benefits and
104

14/05/23 04:43
support services. This highlights the importance of opening information channels of
communication to reach people in most need of support services since many people don’t realise
what forms of support are available, or what services may be of benefit. Furthermore, some
carers experienced an inability to articulate their needs. The right to and the provision of
information in a user-friendly readable form, is clear since some respondents reported being
unable to access and understand written information. Similar studies suggest personal contact as
the optimal mechanism of giving and explaining information (Tester, 1996). The Department of
Health and Children and the Department of Social Community and Family Affairs should initiate
information initiatives aimed at enabling carers to access relevant information regarding a range
of support services. User-friendly resource centres for carers should be developed at local level.
In relation to health promotional factors influencing the promotion of health and social gain, these
results suggest that psychological and emotional aspects of care-giving such as sadness, loneliness,
loss, guilt and burden may mitigate against individual perspectives of personal health and wellbeing.
Carers often have limited opportunities to leave the home care setting and partake in health
promoting activities and therefore must be seen as potentially at risk of developing health problems
that may be averted by the introduction of relevant health promoting initiatives. These results are
consistent with similar research illustrating the complexity of the relationship between challenging
aspects of the care-giving relationship and health promotion (Sisk, 2000). Therefore, emotional and
social care interventions afforded to carers constitute an important component of service provision.
Clearly, a significant requirement of carer support services includes the provision of information
and education, dealing with their anxieties and concerns, bereavement counselling and crisis
emotional support. The importance of advocating for carers requires further consideration, based on
the belief that people should have a say in what happens to them thereby enabling carers to make
informed choices about the provision made for them and for whom they are responsible. Tailoring
respite services in response to carers needs is an essential service requirement. A co-ordinator of
carer support services should be appointed a link person between carers and service providers. Such
an advocacy service would increase awareness amongst carers in relation to the availability of
service entitlements and benefits. The implicit value of family caregiving must be seen in context,
as an aspect of living which any one of us may become a part of in the course of our mortal lives.
Community care systems must ensure that the healthcare environment in the community does not
emerge as a disseminated condensed version of institutional settings, further isolating the carer and
their dependants. To do so would be to overlook the enriching potential of a diverse society
105
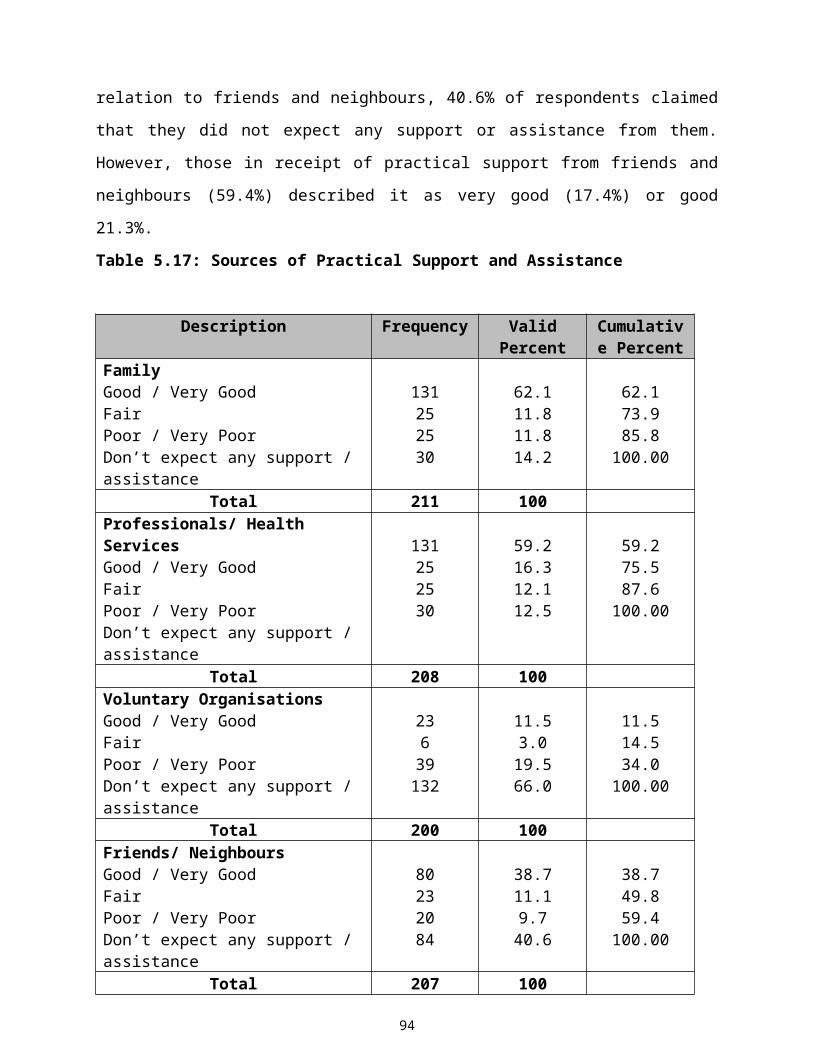
14/05/23 04:43
fostering intergenerational solidarity and partnership with fellow citizens towards a strategy of
social inclusion.
7.4 Implications for Further Research
It is important to establish databases regarding the prevalence of informal caring, that may be
used by carers and service providers alike, based on systematic research findings in regard to
carers’ needs, may provide a useful resource for investigating and analysing periods of care-
giving. There is a distinct lack of information on the prevalence of working carers, the duration,
intensity, and nature of their family care-giving. Since caring is a multifaceted dynamic process,
important changes in experiences or patterns of behaviour, require further investigation.
The manner in which carers perceive themselves is a somewhat neglected area of research.
Although many see their role as having evolved from personal duty, responsibility and personal
attachment to the older person, others see themselves as irritable, resentful and passive in their
role (Askham et al 1992). Specifically, studies exploring caregiver perceptions of burden and
lack of control are required to examine relationships between these cognitive factors and health-
promoting behaviours. From a psychological perspective, specific links between this or other
stress related human emotions and carers' ability to engage in behaviours supporting health-
promotion and health maintenance are areas that require further inquiry. The relationship
between the carer and the person being cared for requires further focusing particularly on how
different forms of care might be developed to best suit the needs of both the carer and the care
recipient.
106
14/05/23 04:43
ReferencesAlt, M. (1990). Exploring Hyperspace: A non-mathematical consideration of multivariate analysis,
McGraw Hill, Berkshire, UK.
Askham, J.E. (1992) Caring: The importance of Third Age carers. Age concern. Institute of
Gerontology, Kings College, University of London.Audit Commission (2000) Forget Me Not: Mental Health Services for Older People. Audit
Commission, London.
Banks, P. (1999) Carer Support: Time for a Change of Direction. King’s Fund, London.
Bell, J. (1991) Doing your Research Project. Open University Press, Milton Keynes.
Benson, P. (1994) Deinstitutionalisation and Family Caretaking of the Seriously Mentally Ill: the
Policy Context. International Journal of Law and Psychiatry, 17, (2) 199 - 138.
Blackwell, J, O'Shea, E, Moare G, Murray P. (1992) Care Provision and Cost Measurement:
Dependent Elderly People at Home and in Geriatric Hospitals. The Economic and Social Research
Institute, Dublin.
Bowling, A. (1997) The effects of illness on quality of life: Findings from a survey of households
in Great Britain. Journal of Epidemiology and Community Health, 50, 149-155.
Brody, E. M. (1990) Women in the Middle: Their parent care years. Springer, New York.
Brody, E. M. (1995) Prospects for family care giving: Response to change, continuity, and diversity,
In: Kane, R.A. and Penrod, J.D. (1995) Family Care giving in an Ageing Society: Policy
Perspectives, Sage Publications, New York.
Buck, D., Gregson, B. A., Bamford, C. H., McNamee, P., Farrow, G. N. and Bond, J. (1997)
Psychological distress among informal supporters of frail older people at home and in
institutions. International Journal of Geriatric Psychiatry, 12, 7 737 - 744.
Burnard, P., Morrison, P. (1994) Nursing Research and Action (2nd Ed) MacMillan, London.
Burns, N., Grove, S. (1987) The Practice of Nursing Research: Conduct, Critique and Utilisation:
W.B. Saunders Company, Philadelphia.
Burr, J.A. and Mutchler, J.E. (1999) Race and ethnic variations in normal or filial responsibility
among older persons. Journal of Marriage and the Family, 61 (3) 674-687.
Byers, P.Y., Wilcox, J.R. (1991) Focus groups: a qualitative opportunity for researchers. The
Journal of Business Communication 28(1), 63-78.
Caldock, K. (1994) Policy and practice, fundamental contradictions in the conceptualisation of
community care for elderly people. Health and Social Care in the Community, 2, 131-141.
107
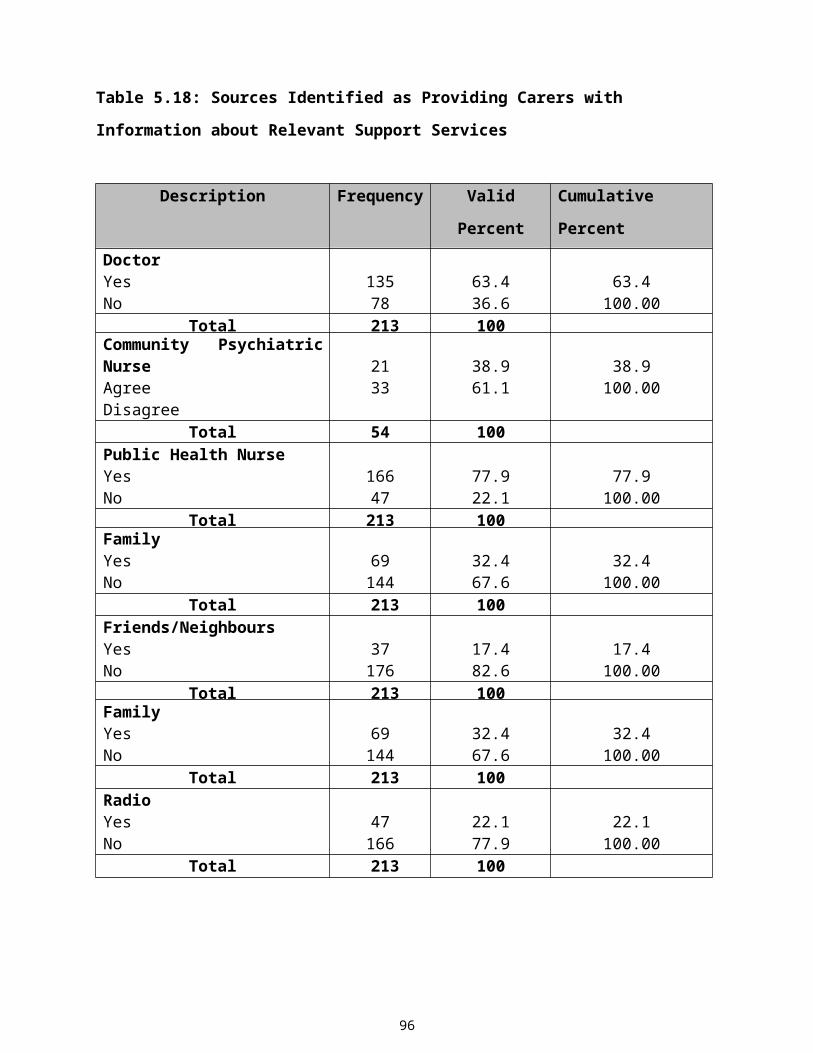
14/05/23 04:43
Carnegie Trust, U.K. (1990) Carnegie Inquiry into the Third Age of Life. Carnegie Trust, U.K.
Central Statistics Office (1999) Population and Labour Force Projections, 2001 – 2031. Dublin
Stationery Press: Dublin.
Central Statistics Office (1997) Women in the Workforce. Statistical Release, Ireland.
Central Statistics Office (1997) Population and Labour Force Projections 1996 - 2026. Stationery
Press, Dublin.
Challis, D. (1992) Providing alternatives to long stay hospital care for frail elderly patients: is it cost
effective? International Journal of Geriatric Psychiatry 7, 773-781
Clarke, A. (1999) Focus group interviews in health-care research. Professional Nurse, 14, 6 395.
Collins, C. Jones R., (1997). Emotional Distress and Morbidity in Demential Carers: a Matched
Comparison of Husbands and Wives. International Journal of Geriatric Psychiatry 12, 1168-1173
Compton, S. A., Flanagan, P. and Gregg, W. (1997) Elder Abuse in People with Dementia in
Northern Ireland; Prevalence and Predictors in Cases Referred to a Psychiatry of Old Age Service.
International Journal of Geriatric Psychiatry, 12, 6 632 - 635.
Coope, B. B., C; Saad, K; Patel, A; Bentham, P; Bannister, C; Graham, C; and Wilcock, G. (1995)
The prevalence of depression in the carers of dementia suffers. International Journal of Geriatric
Psychiatry, 10, 237-242.
Cormack, D (1996) The Research Process in Nursing. 3rd Edition, Blackwell Scientific, Oxford.
Cronbach, L.J. (1951) Coefficient Alpha and the Internal Structure of Tests. Pychometrika, 16, 297
– 334.
Cutcliffe, J.R., McKenna, H.P. (1999) Establishing the credibility of qualitative research findings:
the plot thickens. Journal of Advanced Nursing, 30 (2) 374-380
Dello Buono, M., Busato, R., Mazzetto, M., Paccagnella, B., Aleotti, F., Sanetti, O., Bianchetti, A.,
Trabucchi, M. De Leo, D. (1999) Community Care for Patients with Alzheimer’s Disease and non-
demented elderly people: Use and satisfaction with services and unmet needs in family caregivers.
International Journal of Geriatric Psychiatric 14, 915-924.
Denzin, N., Lincoln, Y.S. (1994) Introduction: entering the field of qualitative enquiry. In
Handbook of Qualitative Research (Denzin N., Lincoln, Y.S. Ed’s) Sage, London.
Department of Health, U. (1989) Caring for People: Community Care in the next decade and
beyond. HMSO. London.
Department of Health, (1993) Research for Health. HMSO. London.
Department of Health (1994) Shaping a Healthier Future: A Strategy for Effective Healthcare in the
1990's. Stationery Press: Dublin.
108
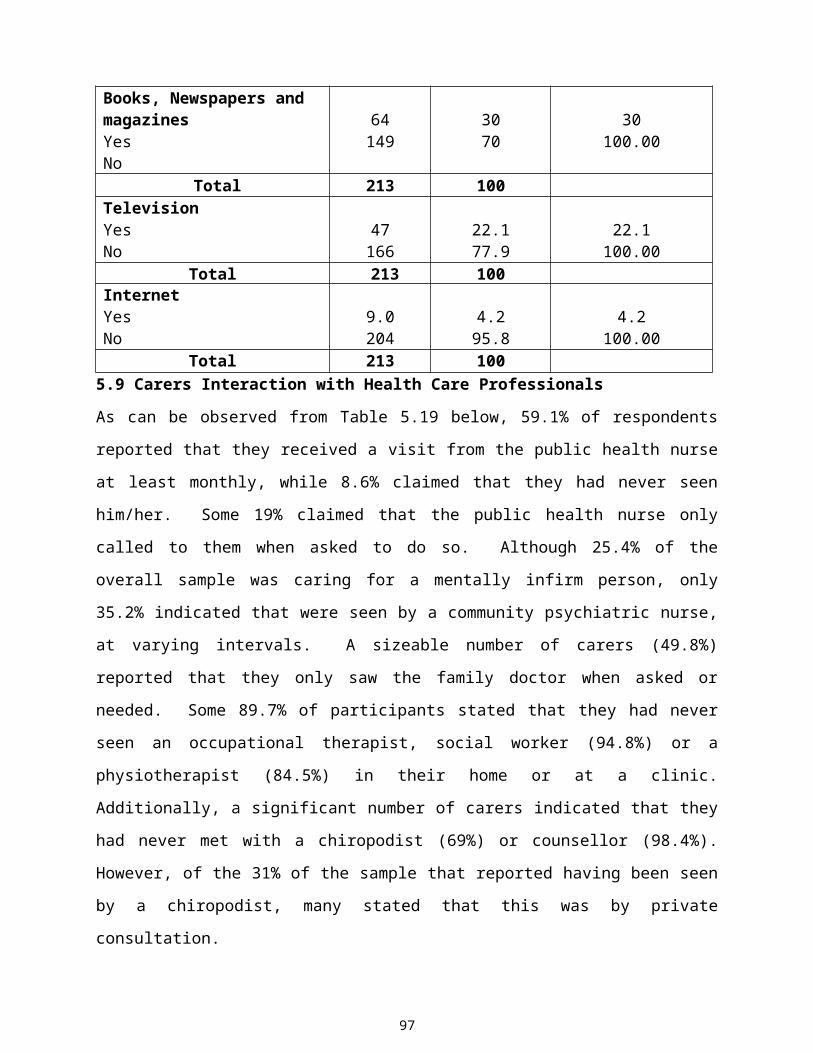
14/05/23 04:43
Department of Health (1995) Carers’ Recognition and Service Act. Practice Guide, Department of
Health, London.
Department of Health (1997) An Action Programme for the Millennium. Stationery Office, Dublin.
Department of Health and Children (1998) Working for Health and Well-being Strategy Statement
1998-2001. Department of Health and Children, Dublin.
Department of Social, Community and Family Affairs (1998) Inclusion, Innovation and
Partnership. Strategy Statement 1998 – 2001, Department of Social, Community and Family
Affairs, Dublin.
Department of Health (1999) Carers National Strategy, Department of Health, London.
DHSS (1996) The Prevalence and Experience of Informal Caring within the Eastern Health and
Social Services Council Area. Eastern Health and Social Services Council, UK.
Doornbos, M. M. (1996) The Strengths of Families Coping with Serious Mental Illness. Archives of
Psychiatric Nursing, 4, 214-220.
Edmondson, R. (1997) Older people and Life Course Construction in Ireland. In Cleary, A. and
Eurobarometer (1993) Age and Attitudes: Main Results of a Eurobarometer Survey, Director
General 5, European Commission, Brussels.
Eurostat (1993) Demographic Statistics, Statistical Office of the European Communities,
Luxembourg.
Evers, A. (1995) The Future of Elderly Care in Europe: Limits and Aspirations. In: Scharf T.,
Wenger GC. Eds. International Perspectives on Community Care for Older People. Avebury,
Aldershot.
Fahey, T. (1995) Health and Social Care Implications of Population Ageing in Ireland 1991 - 2011.
National Council for the Elderly, Dublin.
Fahey, T., Murray, P. (1994) Health and Autonomy among the over 65's in Ireland. National
Council for the Elderly. Report No. 39. National Council for the Elderly: Dublin.
Finch, J. and Mason, J. (1993) Negotiating Family Responsibilities. Routledge, London.
Fowler, F.J., (1993) Survey Research Methods (2nd Ed) Sage, Newbury Park.
Gafstrom, M. and Winblad, B. (1995) Family burden in the care of the demented and nondemented
elderly: A longitudinal study. Alzheimer’s Disease Association Disorder 2, 78 - 86.
Gaucher, E. J. and Coffey, R. J. (1993) Total Quality in Healthcare: From Theory to Practice. Josse
Bass, San Francisco.
George, L. K. (1994) Caregivers burden and well being: An elusive distinction. The Gerontologist,
34, 1 6-7.
109
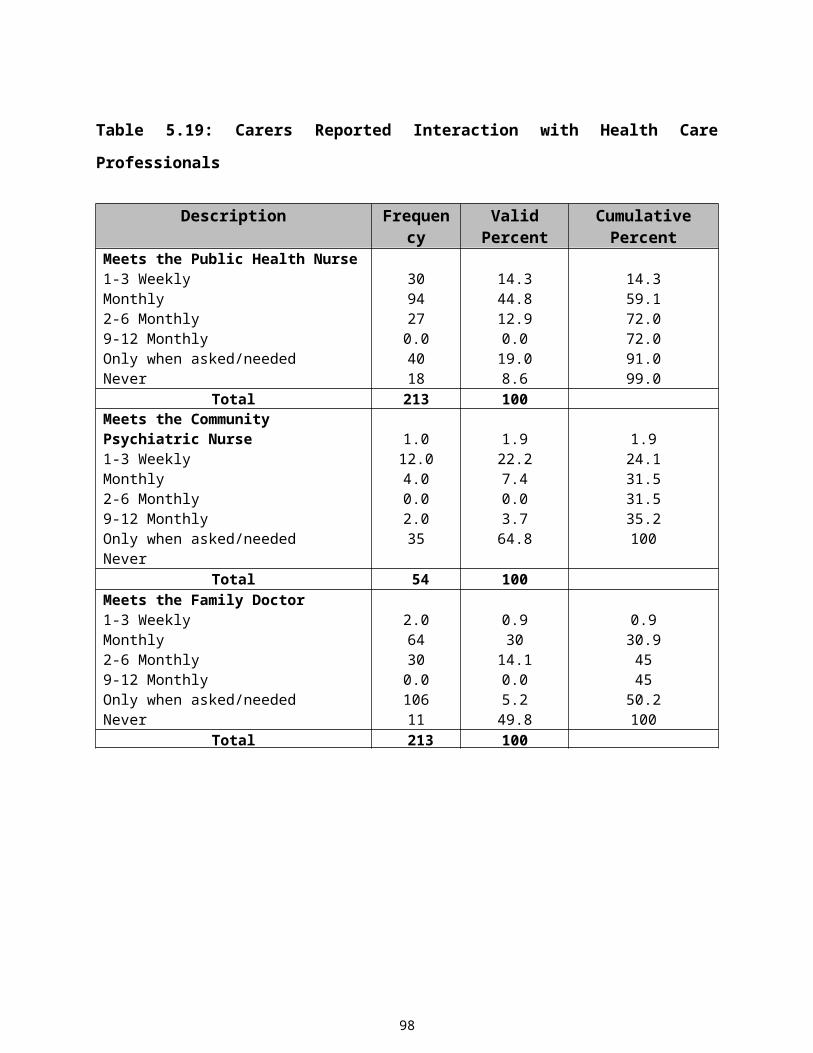
14/05/23 04:43
Giddens, A. (1998) Sociology. Polity Press, Cambridge.
Gilhooly, M.M.L., McKee, K.S., Whittick, J.E., Ballinger, B.B., Gordon, D.S., Mutch, W.J. and
Philp, I. (1994) Coping in family supporters of elderly people with dementia. Paper presented at
the British Society of Gerontology Annual Conference, September, Royal Holloway.
Glendinning, D. (1988) Formal Services and Informal Help: The Costs and Benefits of Informal
Careers. SPRU Discussion Paper, New York.
Goodman, C. (1986) Research on the Informal Carer: A Selected Literature Review. Journal of
Advanced Nursing 11:765-712.
Goodwin, S. (1997) Comparative Mental Health Policy: From Institutional to Community Care.
Sage Publications, California.
Graham, C., Ballard, C., Sham, P. (1997). Carers' knowledge of dementia, their coping strategies
and morbidity. International Journal of Geriatric Psychiatry 12, 931 - 936.
Gray-Vickery (1993) Gerontological Research: Use and Application of Focus Groups. Journal of
Gerontological Nursing, 19, 5 21 - 27.
Gubrium, J. (1995) taking Stock. Qualitative Health Research, 5, 3 267 - 269.
Harding, T. (1997) A life worth living: the independence and inclusion of older people. Help the
aged, London.
Harvarth, T. A. and Archbold Stewart, B. J. (1994) Establishing Partnerships with Family
Caregivers: Local and Cosmopolitan Knowledge. Journal of Gerontological Nursing, 20, 29 - 35.
Hasselkus, B. R. (1998) Meaning in family care giving: perspectives on caregiver/progressive
relationships. The Gerontologist, 28, 686 - 691.
Henwood, M. (1998) Ignored and Invisible? Carers’ Experience of the NHS Report of a UK
Research Survey. Carers National Association, London.
Ironside, J., McMahon, M., Barron, B. (1997) The Balance of Care. A study of carers needs in Co.
Clare, Ireland. Soroptomist International, Unpublished, Republic of Ireland.
Jennings, S., Sayers, G., Doorley, P. and Deehan, A. (1997) Carers of the Elderly, Knowledge, Use
or and Satisfaction with Daycare Services. Irish Journal of Medical Science, 166, 1 28 - 31.
Kane, R. A. and Penrod, J. D. (1995) Family Care giving Policies: Insights from an Intensive
Longitudinal Study, In S.H. Zarit, L.I. Pearlin and Schaie K.W. Care giving systems: Informal and
formal helpers, 273 - 292.
Keady, J. and Nolan, M. (1996) Behavioural and Instrumental Stressors in Dementia (B.I.S.I.D.):
Refocusing the Assessment of Care giving Need in Dementia. Journal of Psychiatric and Mental
Health Nursing, 3, 136-172.
110

14/05/23 04:43
Keady, J., Nolan, M. (1994) The Carer led Assessment Process (CLASP): a Framework for the
Assessment of Need in Dementia Caregivers. Journal of Clinical Nursing. 3: 103-108.
Kellett (1996) Families as caregivers: the long-term aged care experience. Paper presented at the
National Geriaction Conference, Brisbane, August.
Kellett, M., Mannion, J. (1999) Meaning in Caring: Reconceptualising the nurse-family carer
relationship in community practice. Journal of Advanced Nursing, 29 (3) 697.
Kellett, U. M. (1997) The human experience of family caring in Nursing Homes. Paper presented at
the XVIth Congress of the International Association of Gerontology, Adelaide, August.
Kitzinger, J. (1994) The methodology of Focus Groups: the importance of interaction between
research participants. Sociology of Health and Illness, 16, 1 105.
Levin, E. (1997) Carers- problems, strains, and services, In: Jacob, R. and Oppenheimer, C. (eds.).
Psychiatry of the Elderly, University Press, Oxford.
Livingstone, G., Manela, M. and Katona, C. (1996) Depression and other Psychiatric Morbidity in
carers of elderly people living at home. British Medical Journal, 312, 7024 153 - 156.
Lundh, U. (1999) Family Carers: Coping strategies among family carers in Sweden. British Journal
of Nursing 8, 11, 735-746.
Maggs, C. and Lougharne, C. (1996) The Relationship Between Elderly Carers and the Older Adult
with Learning Disabilities, An Overview of the Literature. Journal of Advanced Nursing, 23, (2)
243 - 245.
Macleod Clarke, J. Maben, J. Jones, K. (1996) The use of focus group interviews in Nursing
Research; issues and challenges. Nursing Times Research 1: 2, 143-153.
McBride, R. C. (1995) An audit of Current Discharge Planning Arrangements and their
Effectiveness on Elderly Care Wards and Community Nursing Services, together with Aspects of
Client Satisfaction. Journal of Nursing Management, 3, 1 19-24.
McElwee, C.N. (1999) Centre for Social Care Research. Conceptualising families into the New
Millennium. Phd. Thesis unpublished.
McKenna H.P. (1997) Nursing Theories and Models. Routledge, London.
Miller, D.C. (1991) Guides to Methods and Techniques of Collecting Data in Library, Field and
Laboratory. Sage, Newbury Park.
Miller, B., Campbell, R.T., Farran, C.J., Kaufman, J.E., Davis, L., (1995). Race, Control, Mastery
and Caregiver Distress. Journal of Gerontology B 50, S374-S382.
Mudge, K. and Ratcliffe, I. (1995) Considering the needs of carers: a survey of their views on
services. Nursing Standard, 9, 30 29 - 31.
111
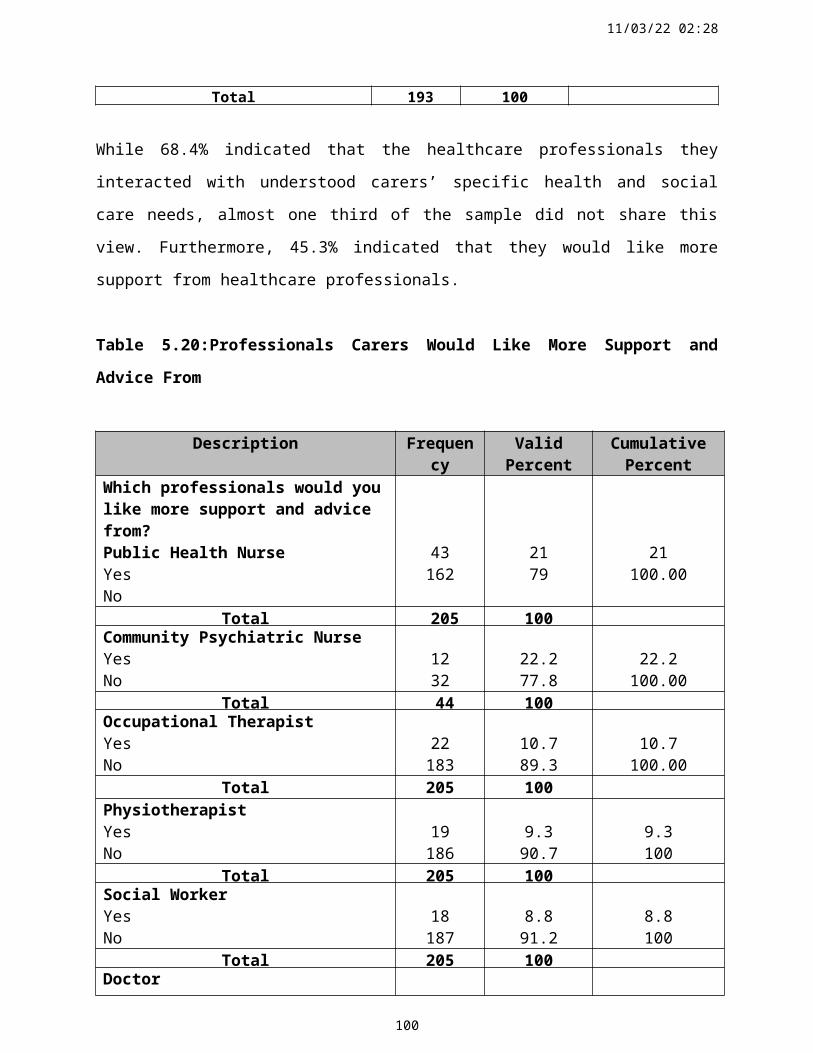
14/05/23 04:43
Myers, F. and MacDonald, C. (1996) Power to the People. Involving Users and Carers in Needs
Assessments and Care Planning-Views from the Practitioner. Health and Social Care in the
Community, 4, 2 86-95.
Nankervis, J., Schofield, H., Herrman, H. and Bloch, S. (1997) Homebased Assessment for Family
Carers: A Preventative Strategy to Identify and Meet Service Needs. International Journal of
Geriatric Psychiatry, 12, 193 – 201
National Council for Aging and Older People (1997). Aging in Ireland, Fact File 1.
National Council for the Elderly (1997) Fact Sheet 9, National Council for the Elderly, Dublin.
National Council for the Elderly (1994) Older People in Ireland: Social Problem or Human
Resource. A Submission to the National Economic and Social Forum. Report No. 37, National
Council for the Elderly, Dublin.
Newens, A. J., Forster, D. P. and Day, D. W. K. (1995) Dependency and community care in
presenile Alzheimer’s disease. British Journal of Psychiatry, 166, 777 - 782.
Nolan, M.R. and Grant. G. (1989) Addressing the Needs of Informal Carers: A Neglected Area
of Nursing Practice. Journal of advanced nursing 14 (11) 950-61.
Nolan, M. and Grant, G. (1992). Regular Respite: An Evaluation of a hospital rota bed scheme
for elderly people. Age Concern Institute of Gerontology, Research Paper No. 6, London.
Nolan, M. & Behi. R. (1995) Triangulation: the best of all worlds? British Journal of Nursing
14(14), 829-832.
Nolan, M., Keady, J., and Grant, J. (1995) A basis for assessment and support with family carers.
British Journal of Nursing 4 (14) 822-826.
Nolan, M. and Caldock, K. (1995b) Assessment: Identifying the Barriers to Good Practice.
Health Social Care in the Community, 4, 2 77 - 85.
Nolan, M., Grant, G. and Keady, J. (1996) Understanding Family Care: A Multidimensional
Model of Caring and Coping. Open University Press: Buckingham.
Norman, I.J., Redfern, S.J., Greengrass, S. (1997) Mental Health Care for Elderly People.
Churchill Livingstone: New York
Norusis, M.J. (1985) SPSSX Advanced Statistics Guide, McGraw Hill, New York.
O'Connor, J., Smyth, E. and Whelan, B. (1988) Caring for the Elderly. Part 1: A Study of
Carers at Home and in the Community. National Council for the Aged. Report Number 18.
Dublin: National Council for the Aged.
Central Statistics Office (1996) Population and Labour Force Projections 1996 - 2026. Dublin:
Stationery Press
112
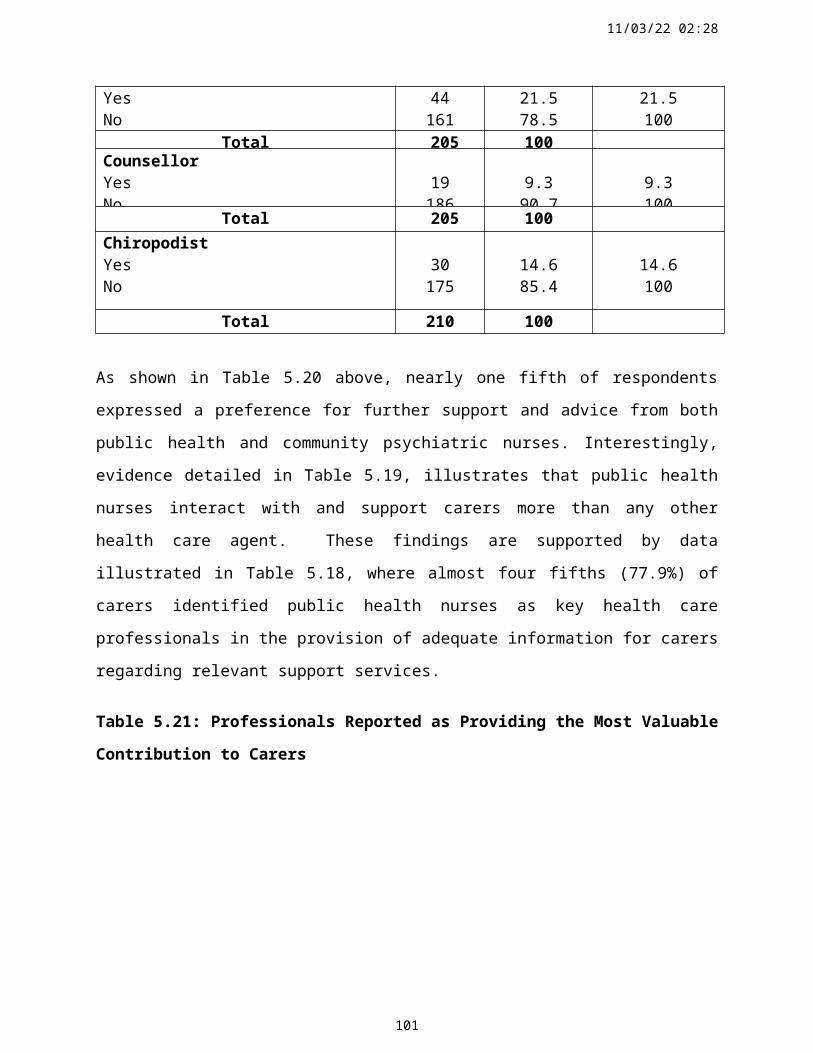
14/05/23 04:43
Pacolet, J., Bouten, R., Lanoye, H. and Versieck, K. (1999) Social Protection for Dependency in
Old Age in the 15 EU Member States and Norway. Office for Official Publications of the European
Communites, Luxembourg.
Parahoo, K. (1994) Questionnaires: use, value and limitations. Nurse Researcher 1 (2) 4-15
Parahoo, K. (1997) Nursing research: Principles, process and issues. MacMillan, London.
Parker, G. (1997) Coping with Caring for a Person with Dementia. In: (Ed) Hunter, S. Dementia,
Challenges and New Directions. Jessica Kingsley Publishers, London.
Pender, N.J. (1996). In: Health Promotion in Nursing Practice, 3rd ed. Appleton and Lange,
Stamford, CT.
Perry, J. (1995) A study of women care giving to husbands who have Alzheimer’s Disease: Family
know-how as a process of interpretative caring. Unpublished doctoral dissertation, University of
Washington.
Philp, I., McKee, J. J., Meldrum, P., Ballinger, R., Gilhooley, M. L., Gordon, D. S., Mutch, W. J.
and Whittick, J. G. (1995) Community care for demented and non-demented elderly people: a
comparison study of financial burden, service use and unmet needs in family supporters. British
Medical Journal, 310, 6993 1503 - 1506.
Polit, D.F., Hungler, B.P. (1991) Nursing Research. 6th Edition, Lippincott, Philadelphia.
Poulton, B. (1997) Consumer feedback and determining satisfaction with services. Achieving
Quality in Community Health Care Nursing Services, Macmillan Press, London.
Roberts, P. (1997) Planning and running a focus group. Nurse Researcher. Qualitative data
analysis 4 (4) 79, Royal College of Nursing, Middlesex.
Robinson, N. (1999) The use of focus group methodology - with selected examples from sexual
health research. Journal of Advanced Nursing 29 (4), 905 - 913
Richardson, A. (1992) A ten Point Plan for Meeting Carers Needs. World Health Organisation, 44,
235 – 239, Geneva.
Richardson, A. (1994) Piloting a study. In Buckeldee, J. and McMahon, R. (eds.) The Research
Experience in Nursing. Chapman and Hall, London.
Ritchie, J. and Spencer, L. (1994) Qualitative data analysis for applied policy research. In: Bryman
A., and Burgess R. Analysing Qualitative Data. Routledge, London.
Robertson-Malt, Susie (1999) Listening to them and reading me: a hermeneutic approach to
understanding the experience of illness. Journal of Advanced Nursing, 29 (2) 290 – 297.
113
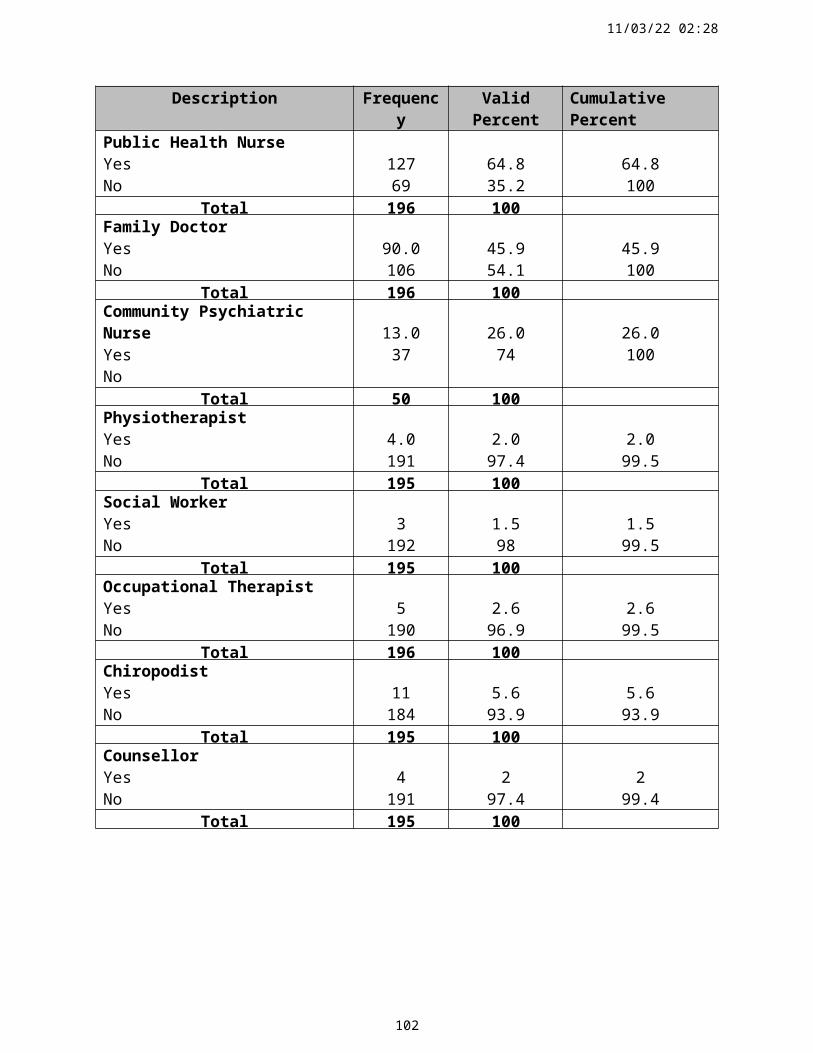
14/05/23 04:43
Rose, L. E. (1996) Families of Psychiatric Patients: a critical review and future research directions.
Archives of Psychiatric Nursing, 2, 67 - 76.
Royal Commission on Long Term Care (1999) With Respect to Old Age: Long Term Care – Rights
and Responsibilities, Stationery Office. London.
Ruddle H., O'Donoghue, F. and Mulvihill, R. (1997) The Years Ahead Report; A Review of the
Implementation of Its Recommendations. National Council on Ageing and Older People: Dublin.
Ruddle, H., O'Connor, J. (1994) Caring without Limits? Suffers of Dementia / Alzheimer’s Disease:
A study of their Carers. The Alzheimer's Society of Ireland and Policy Research Centre, Dublin.
Salvage, A. V. (1995) Who will Care? Future Prospects for Family Care of Older People in the
European Union. European Foundation for the Improvement of Living and Working Conditions,
Dublin.
Sandleowski, M. (1991) Telling stories: narrative approaches in qualitative research. Journal of
Nursing Scholarship, 3, 23 161 - 166.
Savorani, G., Vulcano, V., Boni, S., Sarte, G., Ravaglia, G. (1998) Archives of Gerontology and
Geriatrics. 5, 6 1.
Sheehan, J (1996) Aspects of research methodology. Nurse Education Today 6, 193-202.
Sinclair, H. (1999) The application of small area analysis in the planning and provision of primary
and secondary care services. Conference proceedings. Health Service research conference.
Unpublished work, University College Cork.
Sisk, R.J. (2000) Caregiver Burden and Health Promotion. International Journal of Nursing Studies
37 (2000) 37-43.
Sternberg, R.G. (1993) The Psychologists Companion (3rd Ed) Cambridge University Press, New
York.
Stewart, D. W., Shamdasani P.N., (1990) Focus groups: Theory and Practice. Sage, Newbury Park.
Stevens, G,L, Walsh, R.A., Baldwin, B.A., 1993. Family Caregivers of Institutionalised and Non-
Institutionalised Elderly Individuals. Nursing Clinics of North America, 28 349 – 362, New York.
Sundstrom, G. (1994) Care by Families; An overview of trends, in caring for frail elderly people.
New Directions in Care, OECD Paris.
Swanwick, G.R.J., Lawlor, B.A. (1998) Services for Dementia sufferers and their carers:
Implications for future development, in: Leahy, A.L., Wiley, M.M. (Eds.) The Irish Healthcare
System in the 21st Century, Oak Tree Press, Dublin.
Syron, M., Keane, Y. (1995) A study of the informal carers in the Ballyconnealy area. Milupa
Education and Research Review 1 (18) 4-7, Dublin.
114
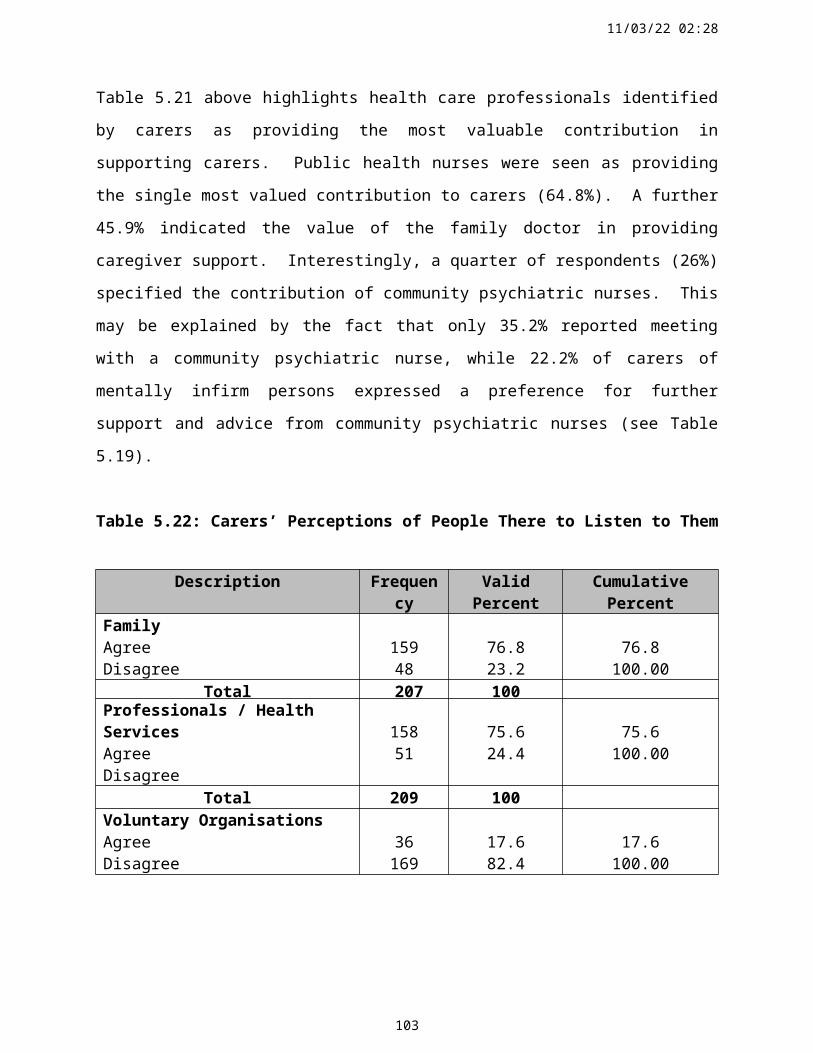
14/05/23 04:43
The Health Forum (1994) What created health? Individuals and communities respond. A National
Study conducted by DYG inc., for the Healthcare Forum, San Francisco.
Tester, S. (1996) Community Care for Older People: A comparative Perspective. Macmillan,
Basingstoke.
Tester (1999) Commentary - Useful services for families; research findings and directors.
International Journal of Geriatric Psychiatry 14, 165-181.
Thornton, P. and Tozer, R. (1994) Involving Older People in Planning and Evaluating Community
Care: A Review of Initiatives. Social Policy Research Unit, New York.
Tilley, S., Pollack, L., Ross, L., Tait, L. (1999) Progress’s Pilgrim: A critical narrative of research in
progress. Journal of Advanced Nursing 29 (5) 221 – 227.
Twigg, J. and Atkin, M. (1994) Carers Perceived: Policy and Practice in Informal Care. Open
University Press, Buckingham.
Wackerbarth, S (2000) Caregivers of Family Members with Dementia were involved in a dynamic
decision making process to maintain tolerable situations. Evidence Based Nursing, 3, 32-33.
Walker, A. (1995) Integrating the Family in the Mixed Economy of Care. In: Allan, I., Perkins, E.
eds. The Future of Family Care for Older People. HMSO, London.
Wardell, F. and Chesson, R. (1998) Volunteering a Healthy Choice. Elderly Care. 10, (6) 12.
Warner, C., Wexler, S. (1998) Eight Hours a Day and Taken for Granted ? The Princess Royal
Trust for Carers, London.
Williams, E. I. and Fitton, F. (1991) Survey or Carers of Elderly Patients Discharge from Hospital.
British Journal of General Practice, 41, 344 105 - 108.
World Health Organisation (1993) The ICD-1 Classification of Mental and Behavioural Disorders;
Diagnostic criteria for research. World Health Organization, Geneva.
Zarit, S. H., Gaungler, J., Jarrott, S.E (1999) Useful Services for Families: Research Findings and
Directions. International Journal of Geriatric Psychiatry 14, 165-181.
Zeller, R.A. and Carmines, E.G. (1986) Measurement in the social sciences, Cambridge University
Press, Cambridge.
115
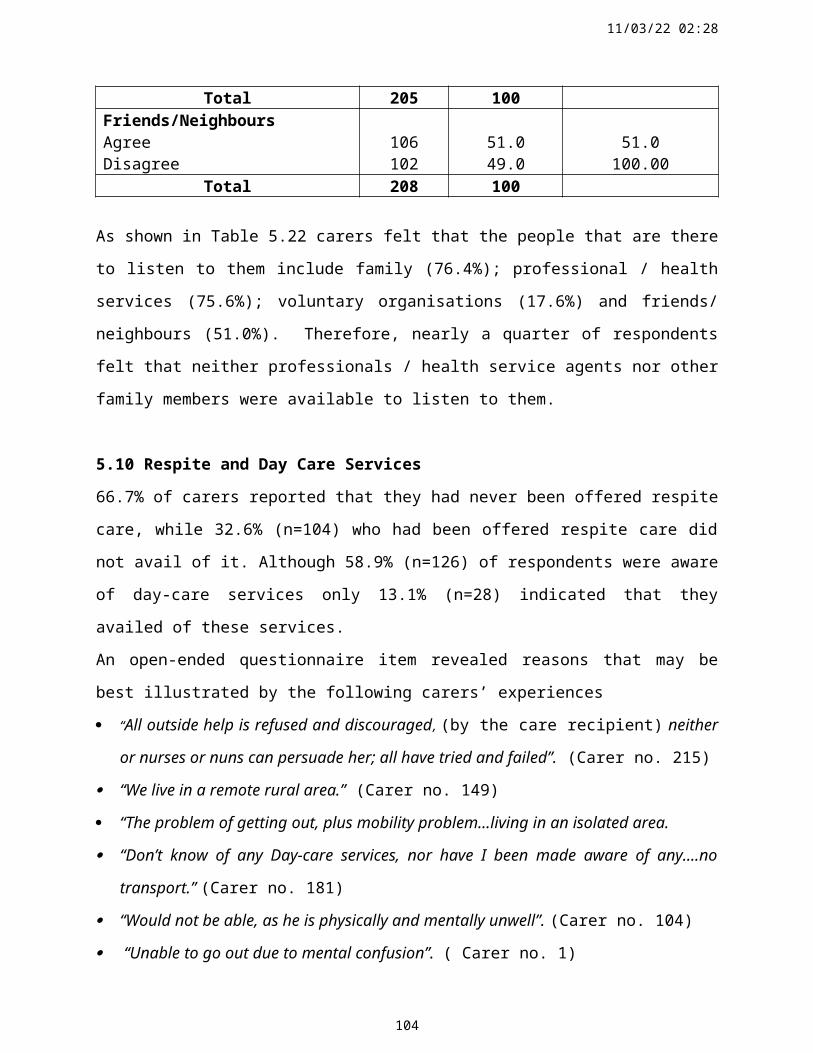
14/05/23 04:43
AppendicesAppendix 2.1: Levels of User Involvement
Empowerment
Participation
Consumer Satisfaction
Consultation
Health Education
Information Giving
Source: Poulton, B, 1997. Consumer Feedback and Determining Satisfaction with Services.
In: Achieving Quality in Community Health Care Nursing Services. Macmillan Press, London.
116
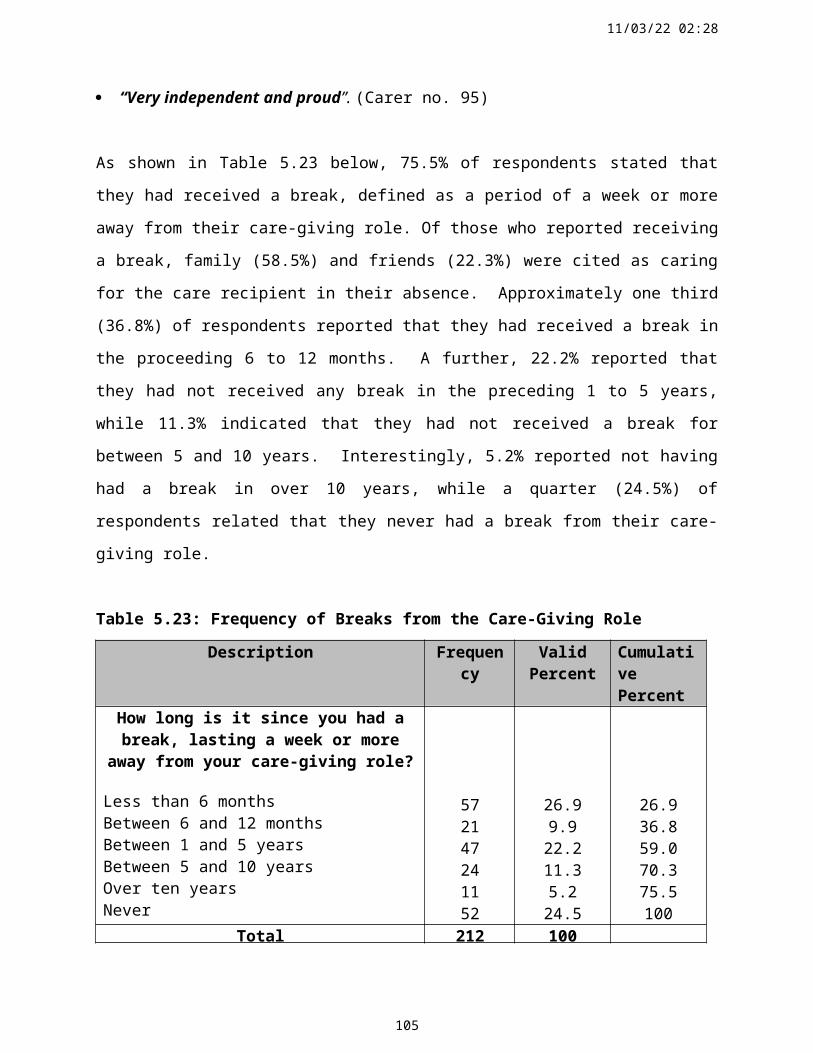
14/05/23 04:43
Appendix 3.1 Topic Guide for Focus Group Interviews
Explore of the profile, role and needs of informal carers in order to map their experience of
caring for older persons.
Discuss responsibilities for care-giving: government, health board, statutory and voluntary
services.
Explore the role of the family in the provision of home care for older people.
Discuss support services for carers;
Professional supports;
Physical structures (appliances etc);
Psychological (stress related matters);
Social (carers allowance, financial issues, respite services).
Discuss the need for education and training for carers.
Identify coping strategies employed by carers.
Explore the positive aspects of the caring role/relationship.
Discuss the effects of care provision on the carers’ health, wellbeing and quality of live.
Establish carers’ satisfaction in relation to the following indices:
1. quality of life,
2. information needs,
3. day care and respite care,
4. transport,
5. Emotional support.
117
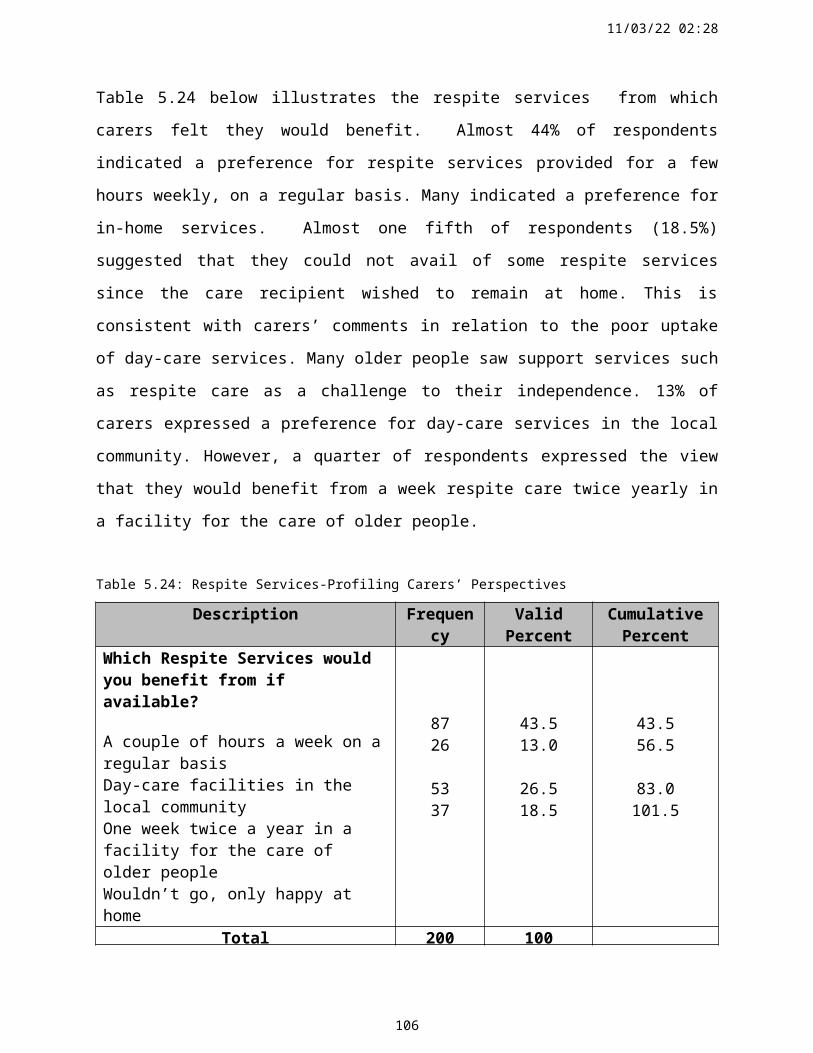
14/05/23 04:43
Appendix 3.2: The Questionnaire
This Questionnaire is Strictly ConfidentialQuestionnaire No.
NEEDS ASSESSMENT QUESTIONNAIRE FOR CARERS OF OLDER PEOPLE (OVER 65 YEARS)
PLEASE COMPLETE EACH QUESTION BY TICKING THE APPROPRIATE BOX / BOXES OR WRITING IN THE SPACE PROVIDED.
Official Use OnlyRuralCity
1.1 Are you 1 Male 2 Female
1.2 What age are you?1 Less than 20 years2 20 – 30 years3 31 – 40 years4 41 – 50 years5 51 – 60 years6 61 – 70 years7 Over 70 years
1.3 How many people over 65 years do you care for?
1.4 Do you live in the same household asthe older person/persons you care for? 1 Yes 2 No
1.5 How long have you been a carer?
1 Up to 1 Year 4 5 years but less than 102 More than 1 year, but less than 2 5 10 years but less than 203 2 years but less than 5 6 20 years or more
118
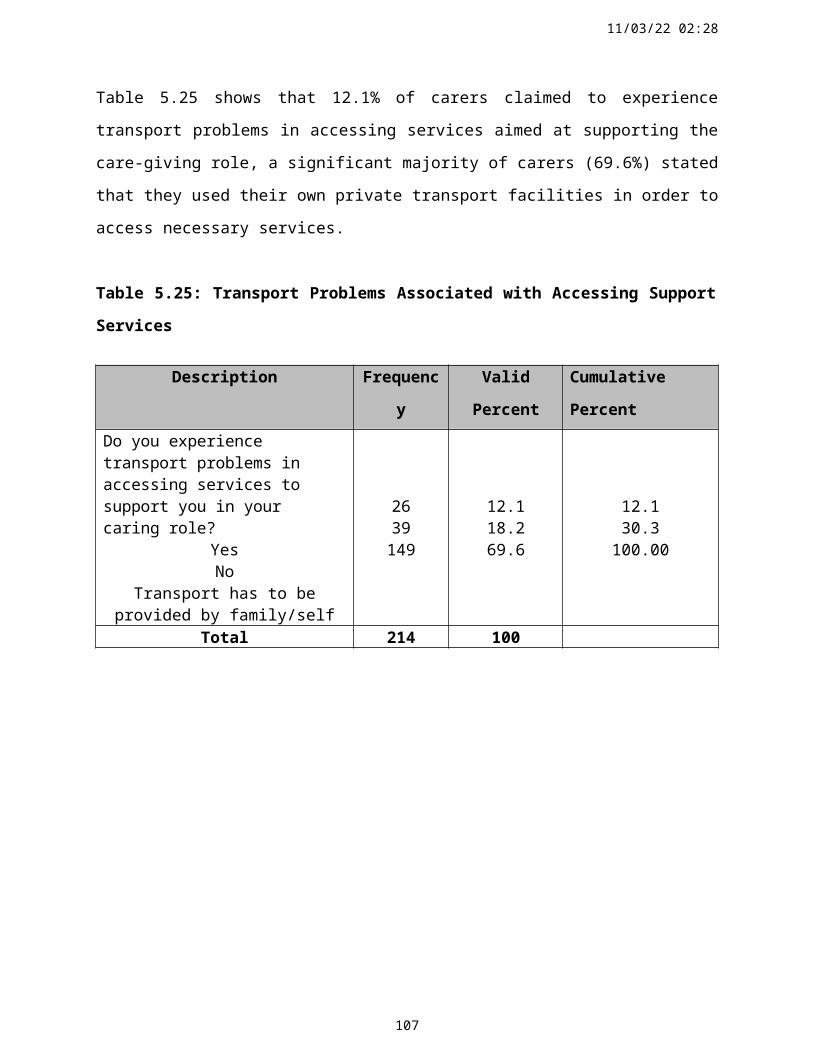
14/05/23 04:43
Section 1 Cont’d
1.6 With regard to the older person / persons you care for, please indicate;
1st Person 2nd Person 3rd Person1.6.1 Your relationship1.6.2 Their age1.6.3 Any condition/s the person
suffers from
1.7 Does the older person / persons you care for suffer from any periods of confusion?
1 Frequently 2 Occasionally 3 Never
1.8 Do you also care for any other persons / family members who are not over 65 years?
1 Yes 2 No
If yes, please answer question 1.8 below
1.9 Please indicate the other family members or persons you care for.
1.10 Are you in paid employment?
1 Full-time 2 Part-time 3 No
1.11 If not, would you like to be in paid employment? 1 Yes 2 No
1.12 Did you give up paid employment to become a carer? 1 Yes 2 No
Please answer all relevant questions on this page
119
14/05/23 04:43
SECTION 2: CARING ACTIVITIES AND SUPPORTS
2.1 Apart from the condition that the older person / persons suffers from, what concerns you most about their health and welfare?
2.2 How many hours a day do you spend caring?
1 0 – 3 hours 2 4 – 8 hours 3 9 – 15 hours 4 16 – 24 hours
2.3 When do you provide care? Please tick as many as are appropriate;
1 Morning 2 Afternoon 3 Evening 4 Overnight
2.4 If overnight, how often do you get up?
1 1 – 3 times nightly2 4 – 6 times nightly3 More than 6 times nightly
2.5 Please state what days (Monday to Sunday) you provide care. Please tick as many as are appropriate
5.1 Monday5.2 Tuesday5.3 Wednesday5.4 Thursday5.5 Friday5.6 Saturday5.7 Sunday
Please answer all relevant questions on this page
120
14/05/23 04:43
Section 2 Cont’d
2.6 What amount of assistance does the person / persons you care for need with the following activities? Please tick one box for each caring activity
None Between 1 and 6 hours
daily
Between 7 and 12 hours
daily
Between 13 and 18 hours
daily
Between 19 and 24 hours
daily6.1 Washing & Bathing6.2 Dressing6.3 Eating & Drinking6.4 Cooking6.5 Toileting6.6 Lifting & Moving6.7 Incontinence6.8 Medication6.9 Household Tasks6.10 Shopping6.11 Personal SafetyPlease specify any other activities
2.7 Do you receive the carers allowance? 1 Yes 2 No
2.8 Do you agree with the means testing of the carers’ allowance?
1 Yes 2 No
2.9 Please specify the average number of hours per week that you receive assistance from either or both of the following people.Home helpHome care assistant
2.10 Do you feel you need assistance from either or both of the following peopleHome help 1 Yes 2 NoHome care assistant 1 Yes 2 No
Please answer all relevant questions on this page
121
14/05/23 04:43
Section 2 Cont’d
2.11 How would you describe the practical support and assistance you receive in your caring role from each of the following:
Very Good
Good Fair Poor Very Poor
Don’t expect any help
11.1 My Family11.2 Professional / Health Services11.3 Voluntary Organisations11.4 Friends / Neighbours
2.12 With regard to the following statements, please indicate your agreement / disagreement.
The people that are there to listen to me
include
The people who provide me with information and direction when I need it
include:Agree Disagree Agree Disagree
12.1 My Family12.2 Professional / Health Services12.3 Voluntary Organisations12.4 Friends / Neighbours
2.13 How would you describe your PAST and CURRENT relationship with the person / persons you care for? Tick one box in Past and Current sections.
Past Relationship Current Relationship
Person 1 Person 2 Person 3 Person 1 Person 2 Person 31 Very Good2 Good3 Fair4 Poor5 Very Poor
2.14 Do you believe that caring for the older person is primarily the responsibility of:
1 Family2 Health Board 3 Both
Please answer all relevant questions on this page
122
14/05/23 04:43
Section 2 Cont’d
2.15 Has the person you care for ever been offered ‘Respite Care’? This is where the person you care for is looked after in a Nursing Home, Hospital or a Voluntary Organisation in order to give you a break.
1 Yes 2 No
2.16 If ‘Respite Care’ has been offered but you did not avail of it, please indicate why?
2.17 How long is it since you had a break, lasting a week or more; away from your caring role?
1 Less than six months 4 Between 5 & 10 years2 Between 6 & 12 months 5 Over 10 years3 Between 1 & 5 years 6 Never
2.18 Which respite services would you benefit from it available? Please tick one or more if you so wish.
1. A couple of hours a week on a regular basis;2. Day-care facilities in the local community;3. One week respite care twice a year in a care of the elderly facility;4. Please specify any other suggestions;
2.19 Has any family member or friend looked after the person you care for in order to give you a break?
Family 1 Yes 2 No
Friend 1 Yes 2 No
Please answer all relevant questions on this page
123
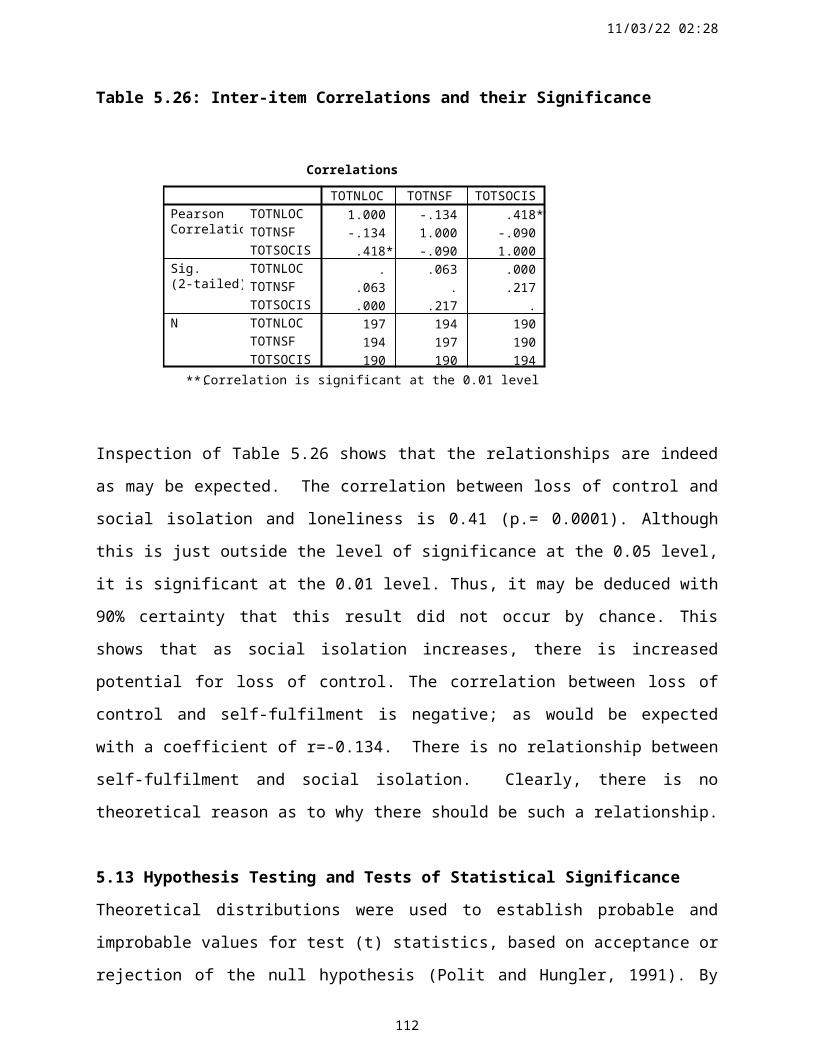
14/05/23 04:43
Section 2 Cont’d
2.20 Are you aware of any Day-care Services that are available to the person you care for?
1 Yes 2 No
2.21 Does the person you care for avail of Day-care Services?
1 Yes 2 No
If not, why?
2.22 Do you experience transport problems in accessing services to support you in your caring role?
1 Yes 2 No 3 Transport provided by family / self
2.23 Do you receive enough information about services available to support you in your role as a carer?
1 Yes 2 No
2.24 Do you receive the information you require from any one or more of the following? Please tick all that are applicable.
1 Family Doctor 6 Family7
2 Public Health Nurse 7 Friends / Neighbours3 Community Psychiatric Nurse 8 Radio4 Voluntary Organisations 9 Television
87
5 Books, Newspapers & Magazines 10 Internet / Computer
2.25 Please specify which Voluntary Organisations, if any provide support for you as a carer.
Please answer all relevant questions on this page
124
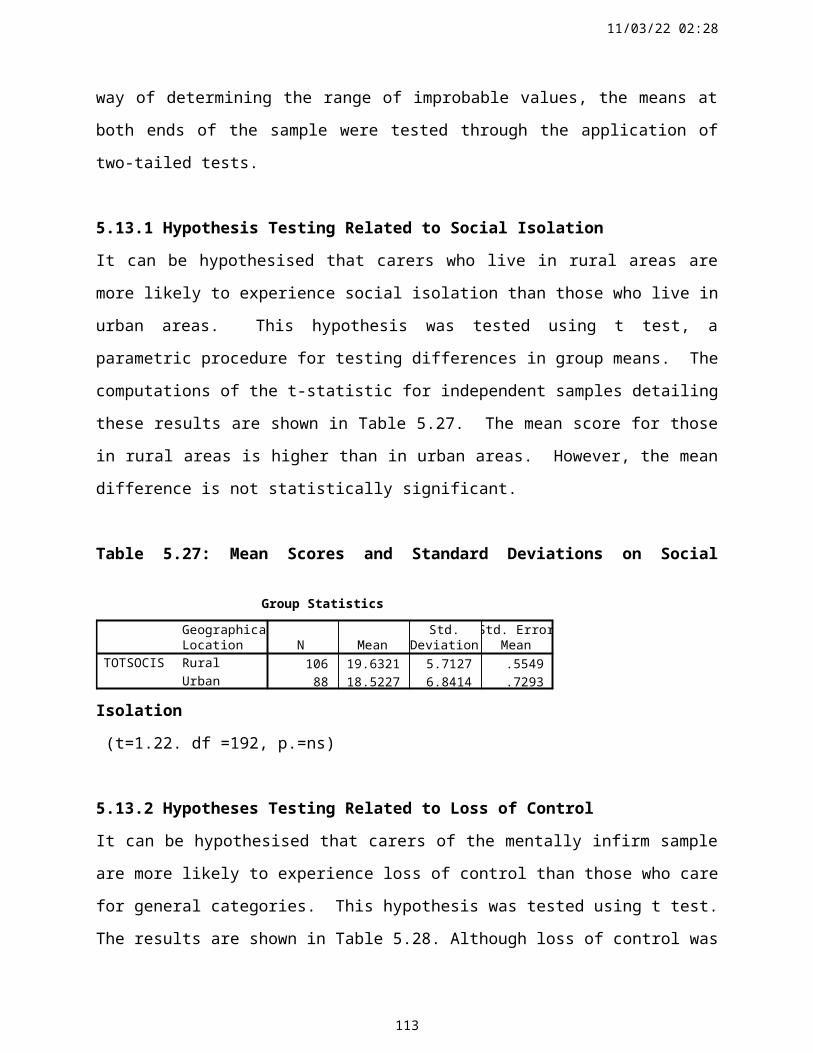
14/05/23 04:43
Section 2 Cont’d
2.26 Please indicate how often per month the person you care for sees any of the following Health Board Professionals in the home or at a clinic.
Once Monthly
Once every 2-6 months
Only when asked / needed
Never
26.1 Public Health Nurse26.2 Community Psychiatric Nurse26.3 Occupational Therapist26.4 Physiotherapist26.5 Social Worker26.6 Family Doctor26.7 Counsellor26.8 Chiropodist
2.27 Please specify which professionals, if any, from the above list (in question 2.26) have provided the most valuable contribution/s to you as a carer.
2.28 Would you like more support from any of the professionals listed in question 2.26.
1 Yes 2 No
If yes, please answer question 2.29.
2.29 Which professionals would you like more support and advise from?
Please answer all relevant questions on this page
125
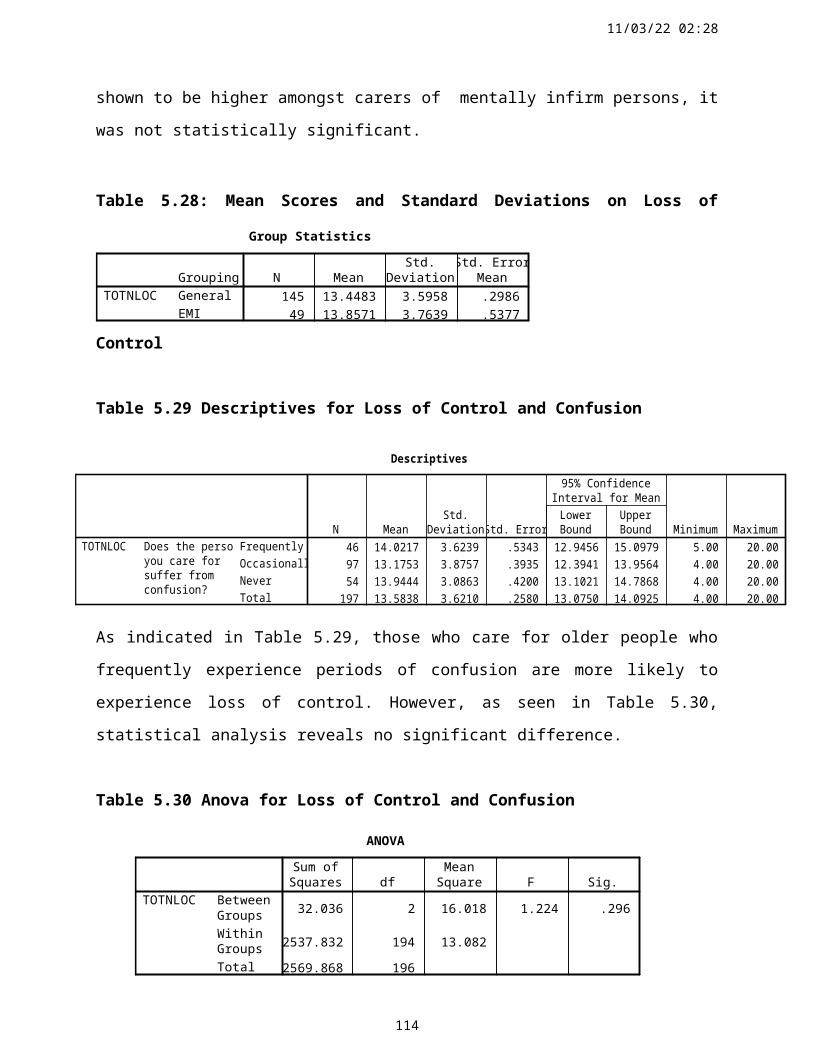
14/05/23 04:43
Section 2 Cont’d
2.30 In your experience do the professionals you meet understand your health and social care needs, as a carer?
1 Yes 2 No
Please elaborate if you so wish.
2.31 Do you feel the Department of Health should do more for the carers of older people
1 Yes 2 No
Please answer all relevant questions on this page
126
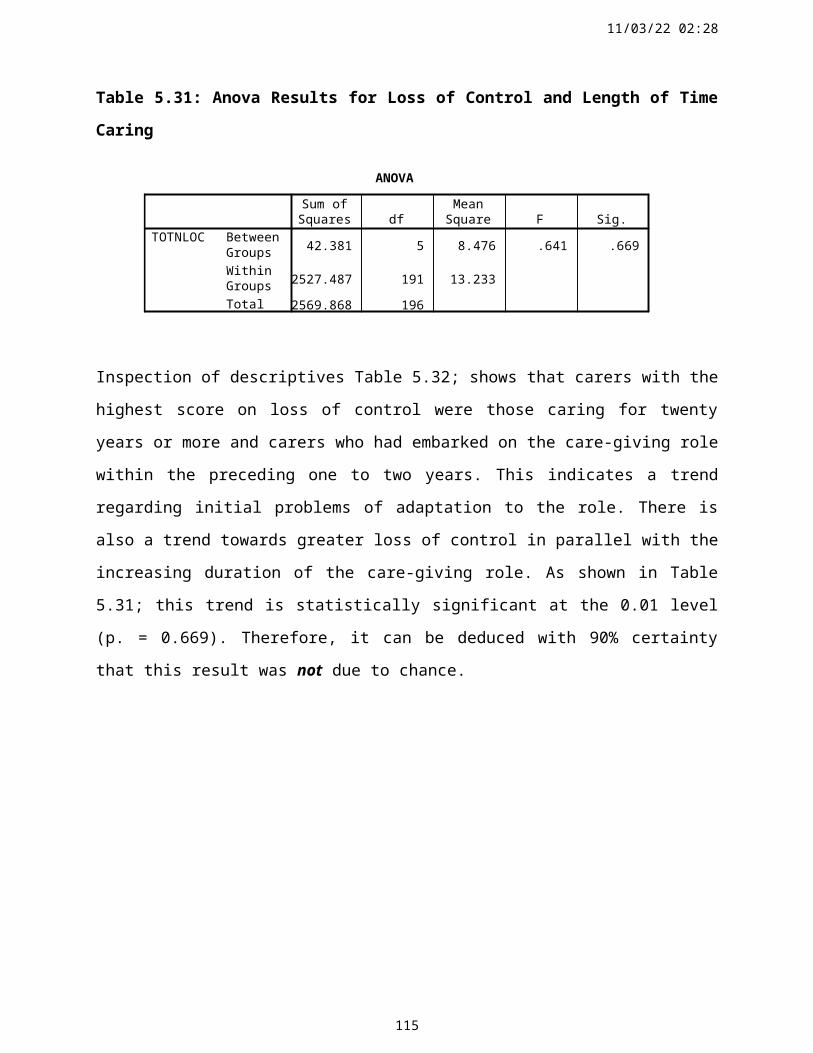
14/05/23 04:43
SECTION 3: COPING STRATEGIES, NEGATIVE AND POSITIVE DIMENSIONS
Please indicate how much you agree or disagree with the following statements by ticking one column for each statement.
Strongly Agree
Agree Neither agree nor disagree
Disagree Strongly Disagree
3.1 I feel trapped in my care giving role3.2 I rely on past experiences to help me
cope3.3 I feel isolated from others as a carer3.4 I seem to have no free time for
myself3.5 Caring makes me feel needed and
fulfilled3.6 I feel sad and lonely at times3.7 I feel content in my role as a carer3.8 I sometimes lose my temper with the
person I care for3.9 I cope better when I reflect on good
times I had in the past with the person I care for
3.10 I worry about becoming unwell and unable to continue as a carer
3.11 Emotionally, I feel supported3.12 Sometimes I resent the person I care
for3.13 The good parts of caring help me to
cope 3.14 I feel burdened by my roles and
responsibilities as a carer3.15 I lose my patience with the person I
care for regularly.3.16 If I had more information and
training for this role I feel I could cope better
3.17 I need someone to discuss my problems as a carer, in order to cope
3.18 There are times when I feel I could lose control
3.19 Caring has strengthened family relationships
3.20 I feel powerless as a carerPlease answer all relevant questions on this page
127

SECTION 4: QUALITY OF LIFE ISSUES
4.1 How would you describe your own physical health?
Very Good
Good Fair Poor Very Poor
1 Before becoming a carer2 Since becoming a carer
4.2 How would you describe how you feel emotionally within yourself?
Very Good
Good Fair Poor Very Poor
1 Before becoming a carer2 Since becoming a carer
4.3 Do you worry about your own health? At Present In the Future1 Yes 1 Yes2 No 2 No
4.4 Do you feel you usually have the energy to fulfil your role as a carer?
1 Yes 2 No
4.5 Do you usually get enough sleep to meet your own needs?
1 Yes 2 No
4.6 Do you find life satisfying?
1 Yes 2 No
4.7 Do you feel cared for yourself as a person?
1 Yes 2 No
4.8 Do you feel that your religious / spiritual beliefs help you to cope with your caring role?
1 Yes 2 No 3 Not Applicable
Please answer all relevant questions on this page
129
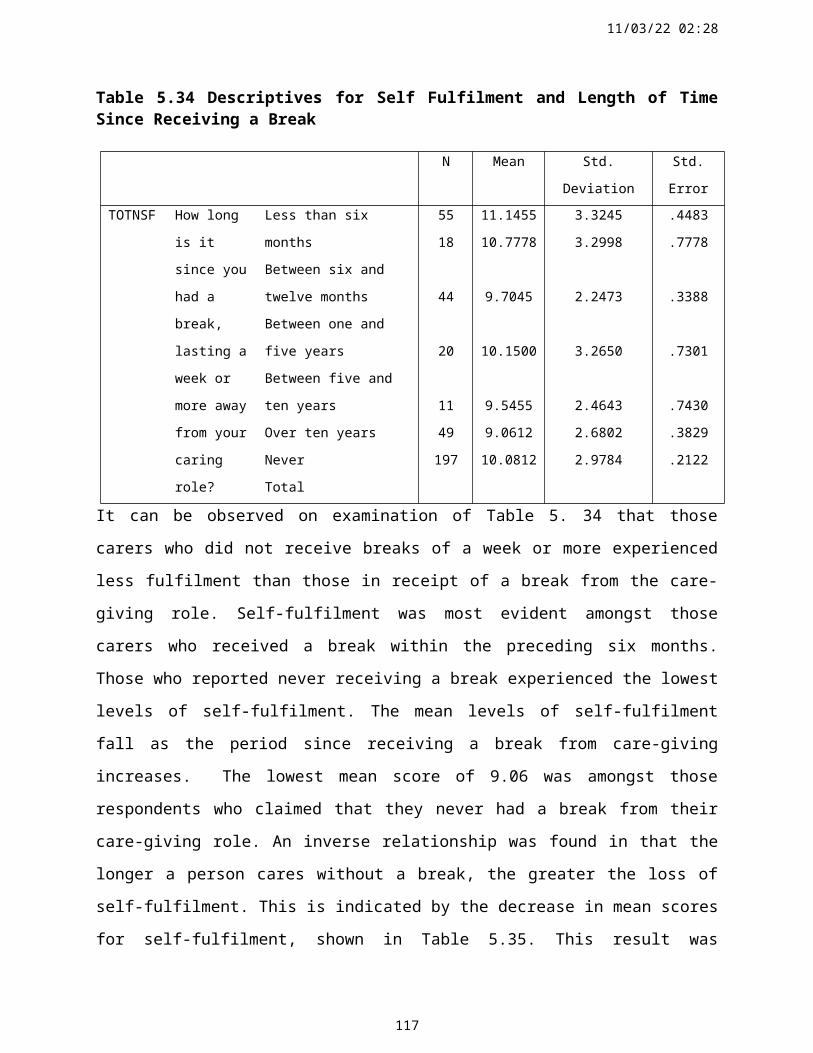
Section 4 Cont’d
4.9 Has your social life deteriorated since becoming a carer?
1 Yes 2 No
4.10 Do you experience financial worries that result from providing home care?
1 Yes 2 No
4.11 If you have given up paid employment to become a carer, do you experience concerns about your own pension?
1 Yes 2 No 3 Not Applicable
4.12 If there are any comments / recommendations that you wish to make regarding any aspect of providing care for older people, please do so in the space provided below.
4.13 Please indicate if you would be willing to take part in a discussion with the research officer regarding your views in relation to your caring role?
1 Yes 2 No
If yes, please provide your:
Name:
Address:
Phone:
Thank you most sincerely for taking the time to complete this questionnaire.
130

131
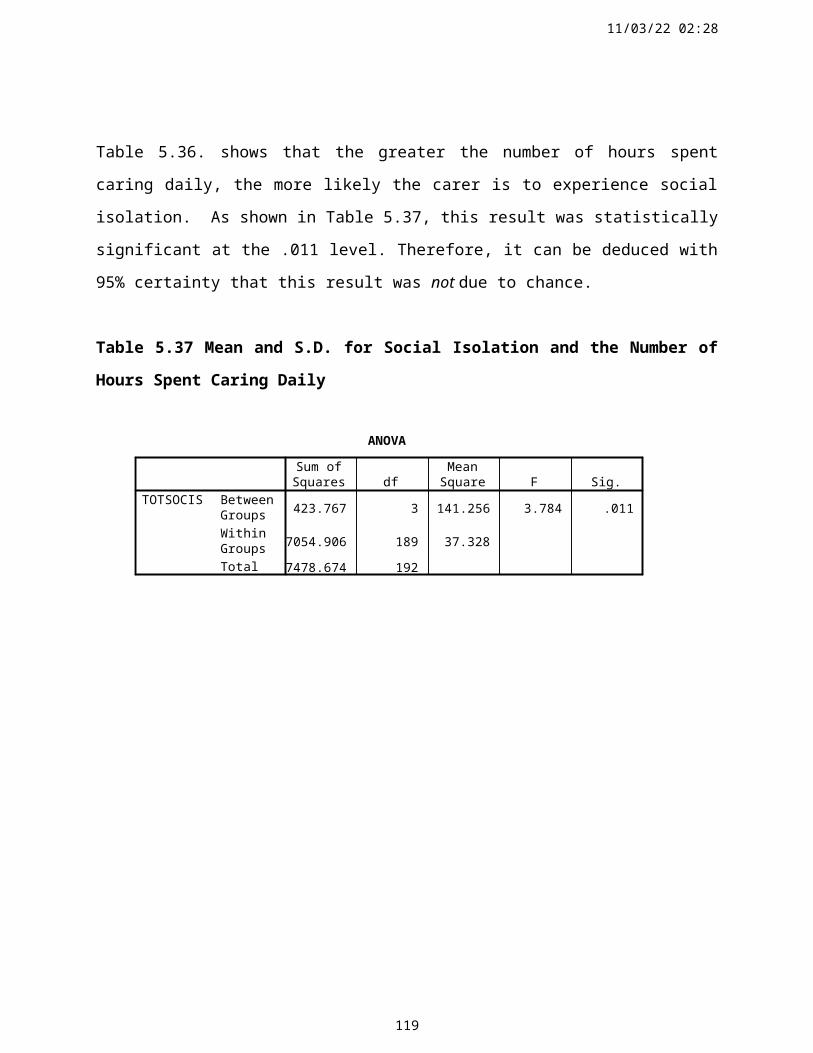
Appendix 3.3
PHN Area and Percentage of Older People, Over 65 Years in Waterford Community Care Area.
Public Health Nurse Area 1991 Pop. 1996 Pop. % change 65 – 74 Years
75 – 84 Years
85+ Years
1. Newtown 4717 5275 11.8% 6.39% 5.18% 1.97%
2. Johns Park 4497 4409 1.9% 11.15% 5.03% 1.31%
3. Kilcohan, 2058 3235 57.2% 1.95% 0.96% 0.48%
4. Ballybeg 3573 3307 7.4% 1.2% 0.4% 0.1%
5. Larchville, Lisduggan 5836 4962 14.9% 8.05% 4.16% 1.43%
6. Slievekeale, Lismore Park 5158 5180 0.4% 3.54% 1.95% 0.64%
7. Hillview 4448 4631 4.1% 10.27% 5.07% 1.16%
8. City Centre 4257 4441 4.3% 11.50% 5.23% 1.33%
9. Ardmore 2850 2879 1% 7.96% 5.6% 1.14%
10. Bonmahon 3073 3185 3.6% 8.10% 5.04% 0.84%
11. Lismore 2567 2550 0.7% 8.35% 6.15% 1.65%
12. Cappoquin 2802 2795 0.2% 8.84% 5.72% 1.11%
13. Dungarvan 3590 4665 29.9% 6.39% 3.59% 0.56%
14. Dungarvan 3688 4160 12.8% 9.32% 3.42% 1.80%
15. Kilmacthomas 2977 2885 3.1% 7.80% 3.33% 0.63%
16. Kilmeaden 3224 2983 8.1% 5.47% 2.43% 0.90%
17. Mooncoin 3654 3602 1.4% 7.36% 3.50% 0.64%
18. Piltown 3621 3613 0.2% 6.92% 4.29% 1.05%
19. Portlaw 1968 2161 9.8% 7.69% 5.18% 1.39%
20. Ring (Old Parish) 2924 2695 7.9% 6.39% 2.40% 0.93%
21. Slieverue 3990 3837+ 3.8% 10.42% 6.40% 1.02%
22. Seskinane 2748 2358 14.2% 7.63% 5.40% 1.14%
23. Tallow 2894 2787 3.7% 8.70% 5.23% 0.84%
24. Tramore 1 (Pilot Site) 3536 4951 40% 6.84% 3.14% 0.62%
25. Tramore 2 3449 2864 16.9% 6.22% 2.35% 0.50%
26. Dunmore East 3673 4167 13.4% 7.27% 3.26% 0.62%
28. Ferrybank 4144 4839- 16.8% 8.01% 4.65% 0.76%
29. Dunmore Road 3383 4736 40% 2.35% 0.89% 0.06%
132
Appendix 3.4 Pilot Study: Analysis of Response Rates
Test (N =35)
Respondent Number Distribution Method Total response rate 88%
Respondents 1-11 Face-to-face (n=11) 100%
Respondents 12-26 Public Health Nurse (n=15) 100%
Respondents 27-40 Postal (n=9 out of 14) 64%
Re-Test (N =28)
Respondent Number Distribution Method Total response rate 71%
Respondents 1-11 Face-to-face (n=11) 100%
Respondents 12-26 Public Health Nurse (n=12) 82%
Respondents 27-40 Postal (n=5) 32%
133

Appendix 3.5 Personalised Letter Accompanying Questionnaire
22nd November 1999
Dear
The South Eastern Health Board in association with Waterford Institute of Technology and the University of Ulster have set up a working group aimed at assessing the needs and experiences of carers of older people.
In order to identify these needs, we are carrying out a survey of people involved in the care of an older person. Your name was selected at random from Health Board records to take part in the study.
In an effort to hear and understand your experiences, as a carer, I would be grateful if you would complete the enclosed questionnaire by 15th December 1999. While I fully appreciate the demands on your time, this is an opportunity to have your voice heard. Although, the questionnaire is quite lengthy, your involvement is crucial to developing a clear understanding of important issues. The information you provide will be treated as strictly confidential. No-one other than the Research Team will have access to the completed questionnaires.
Please feel free to address any questions on any part of the questionnaire that seem unclear. I can be contacted at the number below if you require assistance. I have assigned Mondays and Tuesdays from 9.00am to 5.00pm to addressing any queries you may have. However, you may call the number below at any time and I will speak with you as soon as possible.
Your time and co-operation in completing this questionnaire is sincerely appreciated.
Yours sincerely,
__________________________
Paula LaneResearch Officer
Phone: (051) 302803E-Mail: [email protected]
134
Appendix 3.6 Letter to PHN’S/CPN’S, Accompanying Prevalence Register
15th July 1999
Ms. Community Care CentreCork RoadWaterford
Dear
The South Eastern Health Board in association with Waterford Institute of Technology and the University of Ulster are currently undertaking a study aimed at identifying the needs and experiences of family and lay carers of people over 65 years of age. This study will also include mentally infirm persons in home care settings in both urban and rural areas of the Waterford Community Care Region.
In order to estimate the prevalence of informal caring, I would appreciate if you would provide me with information regarding the number of carers providing all levels of care for an older person. The specific data required includes the carers’ name, address, and age category. Please specify the Barthel Index or Mental Test Score of the persons being cared for by each informal carer. Please indicate if the person being cared for is known to be on the at risk register.
There may be more than one carer involved in providing care for an individual older person. All these carers are relevant, irrespective of the amount of time spent providing care.
Please do not hesitate to contact me at the address or phone number provided if you have any queries. I would be grateful if I may have this information before 9 th August 1999. While I appreciate the immense constraints on your time, this important information must be detailed in order to examine support services for carers and older people. Your time and co-operation is sincerely appreciated.
Yours sincerely
_________________________Paula LaneResearch Officer
135
Appendix 3.7 Prevalence Register: Data Collection FormIn order to assist you in providing this data, I would be grateful if you would follow the format below, in relation to all family / lay carers of older people (>65 years) in your area.
Carers Name Address Phone Care Recipient Barthel
Index
At Risk
Register1
2
3
4
5
6
7
8
9
10
11
12
13
14
136
Appendix 3.8
Letter Administered to Public Health/Community Psychiatric Nurses Prior to Conducting the Main Study
Dear
As you know, the South Eastern Health Board in association with Waterford Institute of Technology and the University of Ulster are currently undertaking a study aimed at identifying the needs and experiences of family / informal carers of people over 65 years of age. This study will also include mentally infirm persons in home care settings in both urban and rural areas of the Waterford Community Care Region.
Thank you for submitting details in relation to carers known to you in your area. A register of informal / family carers has now been set up on a database. Carers have been randomly selected from this database, to partake in the main study. The Steering Group for the project have proposed that each Public Health Nurse / Community Psychiatric Nurse will distribute and collect the questionnaire for the purposes of the main study. Your co-operation and contribution is therefore very important, as you are aware, a good response rate is essential in order to adequately reflect the views of carers.
Please do not hesitate to contact me at the address or phone number provided if you have any queries. I will be available from 9.00am to 5.00pm each Monday and Tuesday on the number below. However, please feel free to contact me on any other weekday and I will return your call as soon as possible. I would be grateful if you would return the completed questionnaire by 10 th
December 1999. While I appreciate the immense constraints on your time, your support is central to researching in this area of health and social care.
Yours sincerely
_________________________Paula LaneResearch OfficerWaterford Institute of TechnologyCollege Street Campus
Phone: (051) 302803 Fax: (051) 302293 E-Mail: [email protected]
137
Appendix 3.9: Profile of Non-Respondents in Main Study
Relevant Details Respondent Number
Moved out of study site – only known after closing date of study 164, 200
Refused – Says she / he is not a carer 304, 216, 85, 66, 60
255, 203, 170, 145
177, 118
Care recipient objected, says she / he has no carer 137, 235, 75, 53
Refused – no reason given 160, 206, 308, 213
113, 92, 230, 305
240, 244, 37, 273
Carer feels too stressed to partake 236, 247, 93, 14, 281,
140, 78, 125, 247, 93,
14, 281, 140, 78, 244,
175
Sampling error – age did not meet inclusion criteria 263, 212, 48, 114,
248, 65
Carer ill – hospitalised 49
Refused – too upset following recent death 169
Refused – not interested in partaking 204
Too busy to partake 179, 251
Refused – says there is no point 260, 191
138
Appendix 3.10 Audit Trail For In-Depth Interviews
Literature Review Main Study – Questionnaire Data
Emergent Subject Guide for in-depth Interviews
1 Responsibilities for care giving: varying perspectives in relation to DOH / Government responsibilities.Salvage; 1995;Wardell et al; 1997;Pacelot; 1998;Dello Buono; 1999.
Items 2.14, 2.30, 2.31 Carers perceived responsibilities: Government; Health Board; Other Statutory Bodies.
2 Family dynamics – the impact upon carers’ roles and responsibilities. DOH, 1989, 1994, 1997.Twig & Atkin; 1994;Ruddle & O’Connor; 1994;Levin; 1997.
Items 2.11, 2.12, 2.19 The role of the family in care giving
3 The importance of support service planning & interventions.Martin & White, 1988;Thompson; 1993;Alexy & Elnitsky; 1996;Cooper, 1997;Nankervis et al; 1997;Riordan & Bennett; 1998;Vetter et al; 1998;Dello Buono; 1999.
Items 2.7, 2.9, 2.11 – 2.12, 2.15 – 2.16, 2.18 – 2.31
Support services for carers; Physical Psychosocial Dimensions
4 Health & stress related aspects of care giving;Navid; 1992;Kelleher; 1993;O’Loughlin; 1994;Twig & Atkin; 1994;Coope et al; 1995;Livingstone et al; 1996;Goodwin; 1997;Cullen et al; 1997;Buck et al; 1997;Brown & Mulley; 1997; (Health and Wellbeing).Donaldson et al; 1998;Zarit et al; 1999 (stress)
Item 2.13, Sections 3 & 4
Caring – the effects on carers’ health, wellbeing and quality of life.
5 Education & training requirements for carers.Erkert; 1991;Blackwell et al; 1992;Poulton; 1997;Wardell & Chesson; 1998;Savorani et al; 1998.
Section 3,Items 4.1 – 4.3, 4.10, 2.26, 2.11
Education and Training for Carers.
139

Appendix 3.11 Proposed Interview Topic Guide
*Please tick the boxes where you consider the topic to be relevant.
Relevant Irrelevant
1. Responsibilities for care giving; Government, Health Board and Statutory Services;
2. The role of the family;
3. Support services for carers; Professional Supports; Physical structures (appliances etc); Psychological (stress related matters); Social (Carers allowance, financial issues, respite services)
4. Caring – the effects on the carers health and wellbeing;Quality of life.
5. Education and training for carers.
Any other suggested topics for discussion:
Please specify date and time available to meet with Researcher
Date: _________________________
Time: _________________________
Please do not hesitate to contact me at the number below if you have any queries.
Phone: (051) 302803Fax: (051) 302293
140
Appendix 3.12 Information Letter for In-Depth Interview Participants
Title of research project:
The Needs and Experiences of Family or Lay Carers of Older People
Explanation
Thank you for completing the questionnaire and indicating your willingness to take further part in this research project. Your contribution to this research is very valuable and much appreciated.
. As you may recall, the project is about exploring the health and social care needs of people who provide varying amounts of care for an older person living at home. Research in other countries has shown that caring for an elderly family member can at times be difficult and at other times rewarding. However, there is little research done on this in Ireland.
Therefore, the purpose of meeting with you is to gain greater understanding of the experiences and needs of caring from the carers' point of view. This will provide information that may contribute to future health service plans to support carers in the South East. The interview should last about 45 minutes.
I am based at the Waterford Institute of Technology and this work is in association with the South Eastern Health Board and the University of Ulster. The highest standards of professional and ethical practice shall be adhered to at all times. All the information you provide will be treated in the strictest confidence. The anonymity of all who take part will also be protected. You can of course withdraw from the study at any time.
Your participation is sincerely valued and very much appreciated. If you have any queries, please do not hesitate to contact the researcher.
Yours sincerely
_____________________
Paula LaneResearch OfficerPhone: (051) 302803E-mail: [email protected]
141
Appendix 3.13 Consent Form
Title of Project:
The needs and experiences of family and lay carers of older people
I, ……………………………………………………..
of ……………………………………………………………………………………………
………………………………………………………………………………………………
have read and understood the “Information for Participants” sheet which describes the research project, a copy of which I have been given to keep. I have been given ample time to decide whether or not I wish to take part.
I willingly declare my consent to participate in this study.
Signed:
(Participant) ………………………………………………………………………………
(Researcher) ………………………………………………………………………………
Date …………………………………………
142
Appendix 3.14 Ethical Approval for the Study
Advancing Knowledge through Teaching, Learning and ResearchCampuses: Belfast, Coleraine, Jordanstown, Magee College

Advancing Knowledge through Teaching, Learning and ResearchCampuses: Belfast, Coleraine, Jordanstown, Magee College
Newtownabbey
County Antrim
BT37 0QB
Northern Ireland
Telephone: Belfast (01232) 365131

7th October 1999
Ms. Paula LaneResearch OfficeWITWATERFORDIreland
Dear Paula
Research Ethical Committee
Project 99/43 The needs and experiences of family or lay carers of older people
Thank you for the additional materials provided for the Committee.
You may now proceed with the project.
Yours sincerely
Advancing Knowledge through Teaching, Learning and ResearchCampuses: Belfast, Coleraine, Jordanstown, Magee College
Advancing Knowledge through Teaching, Learning and ResearchCampuses: Belfast, Coleraine, Jordanstown, Magee College

NICK CURRYResearch Office
Advancing Knowledge through Teaching, Learning and ResearchCampuses: Belfast, Coleraine, Jordanstown, Magee College
Appendix 3.15 Extract From In-Depth Interview
R…..in the beginning it was all new to me, I had to find out what was happening to my mother.
I just went ballistic, I didn’t know what was happening and now I have become accustomed to it
and I know her needs and em, I came the long hard road learning myself ….. (p. 5)
I. Was that difficult.
R. Oh it was yeah, because I had to give up my job then as well and you know she was, it gradually
took about, it was happening over a period of three years and she got really bad, so I, it was all new
to me and I was, had to get accustomed to this and I did then slowly but now I know where I stand
with it and you know, I came the, it just didn’t happen overnight, my, with my mother it, slow,
week by week she was deteriorating and so I was learning as well and….
I. You said there, you had to give up your job.
R. Yeah, yeah, eventually.
I. How did it, how did it come to be that you were the one do you think, you know.
R. Looking after her.
I. Yeah, you know how some…
R. Well, I am the youngest in the family, the three others are married.
I. Right, OK.
R. And em, I was here with my mother anyway, living with my mother, my father died when I
was twenty, so em, like I had been with her, like we had been together then for a few years just
in the house, so, like the rest were married and they have children and…
148
do you mind telling me, say about the experience, of what it was like for you, you know, when in
the beginning when you found yourself in the role and your mother became iller over that
timeframe. Like you say it was gradual, but…
R. Yeah, em, gradual, I went.
I. But how you felt yourself.
R. I was totally, I just couldn’t em, it was very hard she was doing things that, yet you think that
she was normal and you would come home and you would find em, she could be walking the
roads or she could be, the doors could be left open. She would get up at night, em, leaving things
in funny places, doing funny…
I. Not herself.
R. Not herself, yeah, em, couldn’t communicate with her and she would totally go against you and
there was a stage in the beginning which was very hard where she wouldn’t leave you wash her, she
had some, you know, she wouldn’t leave you touch her, so you know that was a battle to get her
into the bath and wash her and all, you know, so I started to overcome that and then her bowels
started to deteriorate and her, she got constipated and she still had some faculties, but you couldn’t
tell her to go to the toilet and then to the bathroom, she wouldn’t go, she would soil herself and that
was the first two years were just, I nearly had a breakdown, now I will be honest with you and I
could show you photographs of myself, I was a total wreck, trying to come to terms with it and she
would be going against you, because she had some bit of a mind then, but em, her whole system
was breaking down and mine was breaking down on top of it, so, yet you have to do it. The first
stages were absolutely just terrible, I just wouldn’t wish it on anybody now, em, oh, I broke down, I
mean I just broke down, I mean I used to have breakdowns, I would just cry, you know yourself…
I. Yeah.
R. And you would even turn against them, you would even, that’s how bad it can be, you know.
I. It affects your relationship with the person.
149
R. Oh totally, totally, but that’s part of you know, I was able to, there is one very good friend I
have and she em, was going through similar stages and my other sister, X, she is a Nurse and she
was actually helping me out, her husbands’ father an elderly person there and she was going
through a little bit of the same stages, she was telling me, you know but, she would look after my
mother, her own mother as well, but we were able to relate, you know and she knew I had it
very, very hard here, so em, it was bad, it was absolutely, I will never, ever forget it. It was very
bad, my whole system just broke down…
150

Appendix 5.1: Social Isolation and Loneliness Factor-Frequency of Constituent Variables
Description Frequency Valid Percent Cumulative PercentI feel trapped in my care giving roleStrongly AgreeAgreeNeither agree nor disagreeDisagreeStrongly Disagree
4159385514
19.828.518.426.66.8
19.848.366.793.2100
Total 207 100I feel isolated from others as a carer
Strongly AgreeAgreeNeither agree nor disagreeDisagreeStrongly Disagree
2861267514
13.729.912.736.86.9
13.743.656.493.1100
Total 204 100I seem to have no free time for myself
Strongly AgreeAgreeNeither agree nor disagreeDisagreeStrongly Disagree
436129648.0
21.029.814.131.23.9
21.050.764.996.1100
Total 205 100I feel sad and lonely at times
Strongly AgreeAgreeNeither agree nor disagreeDisagreeStrongly Disagree
4172324612
20.235.515.822.75.7
20.255.771.494.1100
Total 205 100I worry about becoming unwell and being unable to continue as a carerStrongly AgreeAgreeNeither agree nor disagreeDisagreeStrongly Disagree
558324347.0
27.140.911.816.73.4
27.168.079.896.6100
Total 203 100I feel burdened by my roles and responsibilities as a carerStrongly AgreeAgreeNeither agree nor disagreeDisagreeStrongly Disagree
2465366513
11.832.017.732.06.4
11.843.861.693.6100
Total 203 100I feel powerless as a carerStrongly AgreeAgreeNeither agree nor disagreeDisagreeStrongly Disagree
2342407916
11.521.020.039.58.0
11.532.552.592.0100
Total 200 100151

Appendix 5.2: Self-Fulfilment Factor-Frequency of Constituent Variables
Description Frequency Valid Percent Cumulative PercentCaring makes me feel needed and fulfilledStrongly AgreeAgreeNeither agree nor disagreeDisagreeStrongly Disagree
278556289.0
13.241.529.313.74.4
13.254.682.095.6100
Total 205 100I cope better when I reflect on good times I had in the past with the person I care forStrongly AgreeAgreeNeither agree nor disagreeDisagreeStrongly Disagree
2811238223
13.855.218.710.81.5
13.869.087.798.5100
Total 205 100The good parts of caring help me to copeStrongly AgreeAgreeNeither agree nor disagreeDisagreeStrongly Disagree
2212933137
10.863.216.26.43.4
10.874.090.296.6100
Total 204 100Caring has strengthened family relationshipsStrongly AgreeAgreeNeither agree nor disagreeDisagreeStrongly Disagree
1579434221
7.539.521.521.010.5
7.547.068.589.5100.0
Total 200 100
152

Appendix 5.3: Loss of Control Factor-Frequency of Constituent Variables
Description Frequency Valid Percent Cumulative PercentI sometimes lose my temper with the person I care forStrongly AgreeAgreeNeither agree nor disagreeDisagreeStrongly Disagree
1569187625
7.434.08.937.412.3
7.441.450.287.2100
Total 203 100Sometimes I resent the person I care forStrongly AgreeAgreeNeither agree nor disagreeDisagreeStrongly Disagree
1241179536
6.020.48.547.317.9
6.026.434.882.1100
Total 201 100I lose my patience with the person I care for regularlyStrongly AgreeAgreeNeither agree nor disagreeDisagreeStrongly Disagree
82834
10327
4.014.017.051.513.5
4.018.035.086.5100
Total 200 100There are times when I feel I could lose controlStrongly AgreeAgreeNeither agree nor disagreeDisagreeStrongly Disagree
1743289023
8.521.413.944.811.4
8.529.943.888.6100
Total 201 100
153

Appendix 5.4: Factor Loading for ‘Loss of Control’
Description of Variable Factor Loading
I sometimes lose my temper with the person I care for 0.61Sometimes I resent the person I care for 0.63I lose my patience with the person I care for regularly 0.75There are times when I feel I could lose control 0.75
Appendix 5.5: Factor Loading for Social Isolation and Loneliness
Description of Variable Factor Loading
I feel trapped in my care giving role 0.77I feel isolated from others as a carer 0.77I seem to have no free time for myself 0.76I feel sad and lonely at times 0.58I worry about becoming unwell and unable to continue as a carer 0.43I feel burdened by my roles and responsibilities as a carer 0.64I feel powerless as a carer 0.57
Appendix 5.6: Factor Loading for Self-Fulfilment
Description of Variable Factor Loading
Caring makes me feel needed and fulfilled 0.73I cope better when I reflect on good times I had in the past with the person I care for
0.55
The good parts of caring help me to cope 0.78Caring has strengthened family relationships 0.62
Appendix 5.7: Computation of Factor Scores
Scale Mean S.D. No. of Items AlphaSocial Isolation 19.12 6.25 7 0.86Loss of Control 13.58 3.6 4 0.80Self-Fulfilment 10.1 2.9 4 0.74
154


















