Incident Management Policy 2016 V2 - Doncaster CCG
34
1 INCIDENT MANAGEMENT POLICY Last Review Date October 2018 Approving Body Quality and Patient Safety Committee Date of Approval Date of Implementation 3 January 2019 Next Review Date 12 February 2019 September 2021 Review Responsibility Chief Nurse / Head of Corporate Governance Version 1.1
Transcript of Incident Management Policy 2016 V2 - Doncaster CCG

1
INCIDENT MANAGEMENT POLICY
Last Review Date
October 2018
Approving Body Quality and Patient Safety Committee
Date of Approval Date of Implementation
3 January 2019
Next Review Date 12 February 2019
September 2021
Review Responsibility Chief Nurse / Head of Corporate Governance
Version 1.1

2
REVISIONS/AMENDMENTS SINCE LAST VERSION (IF APPLICABLE)
Date of Review
Amendment Details
January 2015 • The original PCT document has been revised to reflect the Clinical Commissioning Group establishment
• Reflect the Clinical Commissioning Group Structure February 2016 • Updated definition of an Incident and Serious Incident.
• Updated list of guidance documents used in development of this policy and procedure.
• Useful Contacts updated. • Reportable External Bodies updated in line with guidance.
February 2018 • Useful Contacts updated • Updated job titles throughout document
October 2018 • Health and Safety incident guidance • Updated definitions • Serious Incident (SI) & Never Event (NE) management
process • The new incident reporting template • Incident flowchart • Equality Impact Assessment • NHS Protect amended to NHS Counter Fraud Authority

3
CONTENTS
PAGE
DEFINITIONS / TERMINOLOGY 4
SECTION A – DEFINITIONS 6
Definition of an Incident and Serious Incident 6
SECTION B – POLICY 9
1. Policy Statement, Aims and Objectives 9
2. Legislation and Guidance 11
3. Scope 12
4. Accountabilities and Responsibilities 12
5. Dissemination, Training and Review 15
SECTION C – PROCEDURE 17
1. Procedure in the event of an Incident (including serious incidents) 17
2. Procedure in relation to Serious Incident 17
3. Trends and Lessons Learnt 18
4. Serious Incidents involving a Doncaster CCG Commissioned Service 19
SECTION D – NHS DONCASTER CCG SERIOUS INCIDENT
PERFORMANCE MANAGEMENT PROCEDURES
20
1. Performance monitoring the management of Serious Incidents (except child safeguarding incidents)
20
2. Performance monitoring the management of child safeguarding Serious Incidents
21
3. Monitoring Serious Incident Trends, Themes and Patterns 21
4. Obtaining Assurance of Action Plan Completion 22
5. Reporting on Never Events 22
APPENDICES 23
A Useful Contacts 23
B Reportable External Bodies 24
C Serious Incident Performance Monitoring Flowchart 27
D NHS Doncaster CCG Incident Reporting Form 28
E Incident Reporting Flow Chart 31
F Equality Impact Assessment 32

4
DEFINITIONS / TERMINOLOGY
Term Definition
Abuse Abuse is a violation of an individual’s human rights by any other person or persons.
Consequence A result or effect of some previous occurrence.
Harm Physical or mental injury, moral evil or wrongdoing, to injury physically, morally or mentally.
Information Governance Serious Incident
Any incident involving the actual or potential loss of personal information that could lead to identity fraud or have other significant impact on individuals should be considered as serious.
Investigation The act or process of investigating, careful search or examination in order to discover the truth.
NHS Doncaster Clinical Commissioning Group
NHS Doncaster Clinical Commissioning Group is the Commissioning Organisation for Health in Doncaster.
NHS Funded services and care
The treatment of patients in: NHS establishments or services; in independent establishments including private healthcare; or the patient’s home or workplace. Either all or part of the patient’s care in these settings is funded by the NHS.
Permanent harm Directly related to the incident and not related to the natural cause of the patient’s illness or underlying condition, permanent lessening of bodily functions, sensory, motor, physiologic or intellectual, including removal of the wrong limb or organ, or brain damage.
RIDDOR Reporting of Injuries, Diseases and Dangerous Occurrences Regulations 1995.
Never Event Serious, largely preventable patient safety incidents that should not occur if the available preventative measures have been implemented. Incidents that fall within this category are defined nationally.
Approval The act of approving, of formal agreement.
Policy A deliberate plan of action adopted or pursued by an individual organisation to guide decisions and achieve rational outcomes. A policy is a statement of intent, describing the approach or course of action the organisation is taking in respect of a particular issue. Policies are underpinned by relevant evidence based procedures and guidelines and enable management and staff to make correct decisions, work effectively and comply with relevant legislation and organisational aims and objectives.

5
Term Definition
Procedure A set of step-by-step instructions that describe the appropriate method for carrying out tasks or activities to achieve the highest standard possible and to ensure efficiency, consistency and safety.
Procedural document
An overarching term for the full range of strategies, policies and procedures.
Strategy A long term plan designed to achieve particular goals or objectives. A strategy is often a broad statement of an approach to accomplishing these desired goals or objectives and can be supported by policies and procedures.
6
SECTION A – DEFINITIONS DEFINITION OF AN INCIDENT AND SERIOUS INCIDENT For the purpose of this policy an incident is any incident / accident, near miss or untoward event, which had, or may have had the potential to cause harm, dissatisfaction or injury to persons, loss or damage to property i.e. result in an adverse outcome. This definition includes hazards, accidents, ill health, dangerous occurrences and near misses. Examples of Incidents can include: • A slip or trip in the office • A Road traffic collision whilst driving for work • A scald from a dripping tap • A fire alarm activation that wasn’t pre planned. • Finding a report containing private information on the photocopier • Theft of a laptop • Loss of an ID card This list is meant as guidance and is not designed as an exhaustive list. What is a Serious Incident? In broad terms, serious incidents are events in health care where the potential for learning is so great, or the consequences to patients, families and carers, staff or organisations are so significant, that they warrant using additional resources to mount a comprehensive response. Serious incidents can extend beyond incidents which affect patients directly and include incidents which may indirectly impact patient safety or an organisation’s ability to deliver ongoing healthcare. The occurrence of a serious incident demonstrates weaknesses in a system or process that need to be addressed to prevent future incidents leading to avoidable death or serious harm to patients or staff, future incidents of abuse to patients or staff, or future significant reputational damage to the organisations involved. Serious incidents therefore require investigation in order to identify the factors that contributed towards the incident occurring and the fundamental issues (or root causes) that underpinned these. Serious incidents can be isolated, single events or multiple linked or unlinked events signalling systemic failures within a commissioning or health system. There is no definitive list of events/incidents that constitute a serious incident and lists should not be created locally as this can lead to inconsistent or inappropriate management of incidents. Where lists are created there is a tendency to not appropriately investigate things that are not on the list even when they should be investigated, and equally a tendency to undertake full investigations of incidents where that may not be warranted simply because they seem to fit a description of an incident on a list. The definition below sets out circumstances in which a serious incident must be declared. Every incident must be considered on a case-by-case basis using the description below. Inevitably, there will be borderline cases that rely on the judgement of the people involved. Serious Incidents in the NHS include: Acts and/or omissions occurring as part of NHS-funded healthcare (including in the: • Unexpected or avoidable death of one or more people. This includes
o suicide/self-inflicted death; and

7
o homicide by a person in receipt of mental health care within the recent past • Unexpected or avoidable injury to one or more people that has resulted in serious
harm;
• Unexpected or avoidable injury to one or more people that requires further treatment by a healthcare professional in order to prevent:— o the death of the service user; or o serious harm;
• Actual or alleged abuse; sexual abuse, physical or psychological ill-treatment, or acts of omission which constitute neglect, exploitation, financial or material abuse, discriminative and organisational abuse, self-neglect, domestic abuse, human trafficking and modern day slavery where: o healthcare did not take appropriate action/intervention to safeguard against
such abuse occurring; or o Where abuse occurred during the provision of NHS-funded care. This includes abuse that resulted in (or was identified through) a Serious Case Review (SCR), Safeguarding Adult Review (SAR), Safeguarding Adult Enquiry or other externally-led investigation, where delivery of NHS funded care caused / contributed towards the incident.
• A Never Event - all Never Events are defined as serious incidents although not all
Never Events necessarily result in serious harm or death. • An incident (or series of incidents) that prevents, or threatens to prevent, an
organisation’s ability to continue to deliver an acceptable quality of healthcare services, including (but not limited to) the following: o Failures in the security, integrity, accuracy or availability of information often
described as data loss and/or information governance related issues o Property damage; o Security breach/concern; o Incidents in population-wide healthcare activities like screening and
immunisation programmes where the potential for harm may extend to a large population;
o Inappropriate enforcement/care under the Mental Health Act (1983) and the Mental Capacity Act (2005) including Mental Capacity Act, Deprivation of Liberty Safeguards (MCA DOLS);
o Systematic failure to provide an acceptable standard of safe care (this may include incidents, or series of incidents, which necessitate ward/ unit closure or suspension of services); or
o Activation of Major Incident Plan (by provider, commissioner or relevant agency).
• Major loss of confidence in the service, including prolonged adverse media
coverage or public concern about the quality of healthcare or an organisation Near Misses • An example could constitute a system failure, the result of which is
incorrect/delayed diagnosis. This may not have any serious consequences for some patients, but for others could lead to the wrong treatment/serious delay in treatment and ultimately to death.

8
Information Governance Serious Incidents • Any incident involving the actual or potential loss of personal information that
could lead to identity fraud or have other significant impact on individuals irrespective of media involvement should be considered as serious;
• An information governance incident that leads to damage of service, organisation or NHS reputation;
• Refer to Checklist Guidance for Reporting, Managing and Investigating Information Governance Serious Incidents requiring Investigation (IG SIRI) available from the Health and Social Care Information Centre.
Safeguarding Children Serious Incidents • Any case where there is initial indications that a child has sustained a potentially
life threatening injury which may be through abuse or neglect or
• serious sexual abuse, or sustained serious and permanent impairment of health or development through abuse or neglect. A case where a child dies (including death by suicide) and abuse or
• neglect is known or suspected to be a factor in the child’s death and there will be a Serious Case Review (Working Together 2013)
This list is NOT exhaustive nor in any order of importance. Personal judgement will need to be exercised when deciding whether or not to report and manage an incident as a Serious Untoward Incident. If in doubt report or contact the Chief / Deputy Nurse, Quality and Patient Safety Manager and Designated Nurse for Safeguarding Children and Looked After Children (LAC), for advice.
9
SECTION B - POLICY 1. Policy Statement, Aims and Objectives 1.1 This Policy represents the agreed Policy and Procedure of NHS Doncaster Clinical
Commissioning Group (the CCG) in relation to the reporting and management of Incidents. It also represents the agreed policy and procedure in relation to the CCGs responsibility to performance manage the Serious Incidents that occur within the services it commissions.
1.2 The aim of this policy is to ensure that the organisation captures all incidents
(including serious incidents and never events), learns and shares lessons from them to reduce the chance of similar incident happening again and takes appropriate action to protect patients, staff, contractors, volunteers and members of the public from harm. The policy also relates to the performance management of Serious Incidents within commissioned services.
By following the procedures outlined the organisation will:-
• Document the organisation’s commitment to a fair blame culture to encourage
reporting of all incidents (including serious incidents and ‘Never Events’) to enable the organisation to learn and share lessons learnt across the wider health community.
• Ensure all incidents are captured through early identification in a timely manner, irrespective of whether they caused actual harm.
• Ensure that all reported incidents are appropriately reviewed, managed and investigated based on their severity within the CCG and commissioned services.
• Describe the arrangements for serious incident management, investigation and follow up action.
• Learn, make changes and ensure improvements, as a result of all incidents in order to improve safety for patients, staff, visitors and contractors.
• Use qualitative and quantitative data analysis to highlight any trends which may be occurring and uncover any further need for intervention.
• Ensure individual and organisational responsibilities are defined and followed for incident and serious incident reporting.
• Ensure the organisation complies with all current legislation and performance management.
• Identify the assurance process in place for monitoring and reviewing serious incidents involving services commissioned by the CCG.
• Ensure all commissioned services adhere to contractual performance requirements.
1.3 The purpose of this document is to provide guidance to the CCG Staff in relation to
the reporting of Incidents and Serious Incidents. It will also provide guidance as to how these Incidents should be managed.
1.4 The document also provides guidance to CCG staff in relation to the performance
management of Serious Incidents that occur within commissioned services. 1.5 The aims of this procedural document policy are:

10
• To ensure that incidents that occur within the CCG are reported and managed in a timely effective manner that is in line with national requirements, guidance and legislation.
• To ensure that the CCG meets its obligations to performance manage Serious Incidents that occur within the services it commissions and that in meeting this obligation, all national and local guidelines and legislation is followed.
• To ensure that there are robust processes in place to disseminate appropriate learning from incidents and reduce the risk of reoccurrence through a positive culture of learning and continuous quality improvement.
• To ensure that there are strong governance arrangements in place within the CCG in relation to patient safety and the management of incidents across the health community and within the organisation.
1.6 To ensure continuous improvement in risk management, the organisation has a
range of key performance indicators (KPIs) which it uses for monitoring purposes:
No. Key Performance Indicator Method of Assessment
1. Serious Incident Reporting Performance and Analysis
I. Incident Management Group minutes and performance management records.
II. Contract monitoring and
reports to IMG and relevant committees
2. Internal Incident Reporting and analysis. I. Quarterly Corporate Assurance Report.
3. Production of trends, themes and patterns reports based on information from Providers
I. Receipt of annual reports from Providers.
II. Quarterly and annual
reporting within Doncaster CCG Governance structures.
4. Monitor performance of providers in relation to learning and progress of action plans to ensure they are completed in accordance with original plan
I. Through information schedule and reporting to NHS Doncaster CCG.
II. Minutes and papers
considered through Clinical Quality Review Group.

11
2. LEGISLATION AND GUIDANCE 2.1 The following legislation has been taken into consideration in the development of
this policy and procedure:
• Health and Safety at Work Act 1974 • The Management of Health & Safety at Work Regulations 1999 • Mental Health Act 1983 and 2007 • Reporting of Injuries, Diseases and Dangerous Occurrences Regulations
2013 • Human Rights Act 1998 • Current Data Protection Legislation (Data Protection Act 2018 and EU General
Data Protection Regulations 2016) • The Children Act 2004 • Mental Capacity Act 2005
2.2 The following guidance has been used in the development of this policy
and procedure:
• An Organisation with a Memory – DOH 2000 • Doing Less Harm – DOH and NPSA 2001 • Seven Steps to Patient Safety – NPSA • Building a Safer NHS for patients – Implementing An Organisation with a
Memory – DOH 2001 • Learning from Bristol – DOH 2002 • Design for Patient Safety – DOH 2005 • Safety First: A report for patients, clinicians and healthcare managers –
DOH 2006 • Reporting of Injuries, Diseases and Dangerous Occurrences Regulations
2013 (RIDDOR) • Information Commissioner Guidance Documents. • Reporting Safety Problems for Medicines, Blood and Devices – MHRA.
www.mhra.gov.uk • Health and Safety Executive (HSE) Reporting – www.hse.gov.uk • Safety Problems for medicines, Blood and Devices – medicines Healthcare
products Regulatory Agency (MHRA) Reporting, www.mhra.gov.uk • Counter Fraud and Security Management Services (CFSMS) - Physical
assault reporting • NHS Estates – Reporting fire related incidents • NHS Litigation Authority (NHSLA) Requirements • Procedure for the management of Serious Incidents (SIs) Framework –
NHS Commissioning Board March 2013. • Being Open When Patients are Harmed NPSA September 2005 (re-
launched 2009) • The Private and Voluntary Health Care (England) Regulations 2001 • Statutory Notifications Guidance HCC) 2006 • A guide to Good Practice in the Management of Controlled Drugs in
Primary Care (England) February 2007 • Memorandum of Understanding - Investigating Patient Safety incidents

12
involving unexpected death and serious harm: a protocol for liaison and effective communications between the NHS, Association of Chief Police Officers and Health and Safety Executive February 2006
• Guidelines for the NHS in support of the Memorandum of Understanding November 2006
• Working together to Safeguard Children 2013 • No Secrets – Guidance on developing and implementing multi-agency
procedures to protect vulnerable adults from abuse • Francis Report – report of the Mid Staffordshire NHS Foundation Trust
2013. • Keogh Report – Review into the quality of care and treatment provided by
14 Trusts in England 2013. • Winterbourne Report – Transforming Care: A National response to
Winterbourne View Hospital 2012 • Berwick Report - A promise to learn – A commitment to act: Improving the
safety of patients in England 2013 • Serious Incident Framework – NHS England 2015. • Revised Never Event Policy and Framework 2015 • Checklist Guidance for Reporting, Managing and Investigating Information
Governance Serious Incidents requiring Investigation (IG SIRI) – HSCIC 2014. 2.3 The Essential Standards of Quality and Safety (March 2010) consist of 28
regulations (and associated outcomes) that are set out in two pieces of legislation: the Health and Social Care Act 2008 (Regulated Activities) Regulations 2010) and the Care Quality Commission (Registration) Regulations 2009.
3. SCOPE 3.1 This policy applies to those members of staff that are directly employed by the
CCG and for whom the CCG has legal responsibility. For those staff covered by a letter of authority/honorary contract or work experience this policy is also applicable whilst undertaking duties on behalf of the CCG or working on the CCG premises and forms part of their arrangements with the CCG. As part of good employment practice, agency workers are also required to abide by the CCG policies and procedures, as appropriate, to ensure their health, safety and welfare whilst undertaking work for the CCG.
4 ACCOUNTABILITY AND RESPONSIBILITIES 4.1 Overall accountability for incident management within the organisation lies with the
Chief Officer who has responsibility for establishing and maintaining an effective risk management system within the organisation including sharing lessons learnt. This is formally delegated at follows:
Chief Nurse (or equivalent)
Has delegated responsibility for: Leading the development of appropriate systems and processes to manage Serious Incidents in line with the CCGs responsibilities.

13
Associate Director of HR and Corporate Services (or equivalent)
Has delegated responsibility for the development and implementation of non-clinical incident management. This is the Senior Information Risk Owner (SIRO) for NHS Doncaster CCG.
Chief Finance Officer (or equivalent)
Has delegated responsibility for the development and implementation of financial risk management and financial governance.
Data Protection Officer (DPO)
Has responsibility for assisting in implementing essential elements of the General Data Protection Regulation including the security of processing and notification and communication of data breaches. The DPO must be promptly consulted once a data breach or another incident has occurred Nominated Head of
Quality in Contracts and Designated Nurse for Safeguarding Children and Looked After Children (LAC)
Has delegated responsibility for the day to day management of the serious incident reporting, reviewing and performance monitoring process. Will liaise with the Quality and Patient Safety Manager and Heads of commissioned services to ensure that incidents will be managed appropriately. Also acting as liaison between Doncaster CCG and Rotherham, Doncaster and South Humber Mental Health NHS Foundation Trust (RDaSH) and Doncaster and Bassetlaw Hospitals NHS Foundation Trust (DBTHFT) with respect to clinical incidents.
Quality Support Officer (or equivalent)
Has delegated responsibility for the logging, updating and extracting information on the Serious Incident Database. Said person will provide the Incident Management Group and Quality and Safety Committee with the relevant reports and will liaise with the NHS England Area Team to ensure information is received/provided and recorded accurately.
Staff Responsibilities of Staff (including all employees, whether full/part time, agency, bank or volunteers) are: Complying with all procedural documents of the organisation. Identifying any gaps in Incident management Policies and identifying these to the document authors / responsible officers.
4.2 The day-to-day operation of commissioned service incident reporting has been delegated to the Designated Nurse for Safeguarding Children and LAC, unless otherwise agreed. Said person (or their delegates) will provide the CCG Quality and Patient Safety Committee (Q&PSC) relevant information in respect of all types of incidents.

14
4.3 All staff – must take charge of the immediate situation until a more senior person is available and ensure that all potential/actual incidents (including serious incidents) are reported, that the incident report is fully completed and that the requirements of this policy and procedure are met. In the first instance, the incident must be reported within 24 hours. Where appropriate staff members may be involved in the review of incidents and implementing actions.
4.4 All staff must ensure they book on and attend any mandatory or statutory training
sessions on Risk Management, Incident Reporting and Health and Safety. 4.5 All Managers – All managers are responsible for ensuring that all incidents
(including serious incidents), which occur in their areas of responsibility, are reported immediately through the agreed reporting systems. Said incidents must also be reviewed by the appropriate Chief of service to ensure that:
• The incident report is fully and accurately completed; • The incident severity has been correctly categorized; • Reports to External Agencies are completed and sent; • Where appropriate managers must ensure an investigation is carried out.
Managers are responsible for ensuring staff at all levels understand the need to report all incidents, accidents and near misses as per this policy and procedure and to ensure compliance with the CCG’s legal obligations. In order to discharge this duty managers are required to ensure that members of staff attend any mandatory or statutory training sessions on risk management and health and safety. It is recognised that many incidents; especially more serious incidents (Serious Incidents) may have a significant impact upon staff affected by the incident. Arrangements should be made by Line Managers to ensure that any member of staff involved in incidents receives the necessary support and counselling (if required).
4.6 A Nominated Lead Investigator – has delegated responsibility for undertaking
the investigation using the NPSA Root Cause Analysis (RCA) model and submitting a full report within the specified timescales. http://www.nrls.npsa.nhs.uk/resources/type/toolkits/
4.7 All Chiefs – are collectively and individually responsible for the management of risk and for implementing this policy and procedure. It is each and all, Chiefs responsibility to ensure that departmental inductions outline the organisation’s requirements of staff in respect of this policy and procedure. Chiefs also have responsibility for cascading information to staff regarding updates or amendments to the policy and procedure.
4.8 Committees – The CCG Governing Body has delegated responsibility for
reviewing the development and implementation of incident management systems to the Q&PSC. In order to discharge this duty the Q&PSC must ensure that appropriate sub- committees and groups exist to support the process.
The following group provide assurance that incidents are being managed and confirm action plans resulting from incidents (including serious incidents),

15
complaints or claims are followed up and lessons learnt are disseminated: - 4.9 Incident Management Group (IMG) – Reports to Q&PSC. Reviews, quality
assures and on completion of required actions and agrees closure of all serious incidents reported by the CCG commissioned services. The IMG may also undertake this role under a memorandum of understanding when incidents occur in services commissioned by others including Public Health and NHS England.
4.10 Clinical Quality Review Group – Reports to the relevant Strategic Contracting
meeting with our main providers. Reviews themes and trends and any recommendations from the IMG to escalate any issues / concerns identified.
4.11 Information Governance Group - Reports to Executive Committee.
Receives and considers reports into information incidents and risks, including cyber security incidents, and ensure appropriate action is taken for reporting to Executive Committee.
4.12 Health and Safety Manager - Provides advice and support to staff whenever
necessary: • Investigation of accidents / incidents and near misses; • Advising Managers with regards RIDDOR Reporting; • Ensures that all managers are kept up to date with any changes in legislation; • Discusses any recommendations with managers if necessary.
5. DISSEMINATION, TRAINING AND REVIEW 5.1 Dissemination 5.1.1 The effective implementation of this policy will support openness and
transparency. The CCG will ensure that the policy is implemented through the publication of this policy, supporting any training needs and also the monitoring of the key performance indicators.
5.1.2 A set of hardcopy Procedural Document Manuals are held by the Governance
Team for business continuity purposes and all procedural documents are available via the organisation’s website. Staff members are notified by email of new or updated procedural documents.
5.2 Training 5.2.1 All staff will be offered relevant training commensurate with their duties and
responsibilities. Staff requiring support should speak to their line manager in the first instance. Support may also be obtained through the HR Department. Managers should contact the Governance Team if there are specific training needs.
5.2.2 It is important that all staff working for the organisation are familiar with this policy
and that it is well understood and that the associated procedures are rigorously applied. Some staff have been trained in the NPSA Root Cause Analysis techniques by the organisation, this will be dependent on their role in incident

16
investigation 5.3 Review 5.3.1 This policy will be reviewed every three years and in accordance with the
following on an as and when required basis:
• Legislative changes • Good practice guidance • Case law • Significant incidents reported • New vulnerabilities • Changes to organisational infrastructure
This policy is located on the Website. A number of other procedural documents and policies are related to this policy and should be read in conjunction as shown below:
• Relevant Health and Safety Policies • Claims Management Policy • Whistleblowing Policy • Risk Management Strategy, Policy and Procedure • Security Policy including Lone Working Procedure • Complaints Policy • Disciplinary Policy • Relevant Infection Prevention and Control Policies • Freedom of Information and Environmental Regulations Policy • Practice Guidance for Safeguarding Children
This list is not exhaustive and other CCG policies may relate to this policy.

17
SECTION C - PROCEDURE 1. PROCEDURE IN THE EVENT OF AN INCIDENT (INCLUDING SERIOUS
INCIDENTS) OCCURRING WITHIN THE CCG 1.1 Immediate action should be taken to ensure the health needs of the individuals
affected are dealt with in order to minimise harm and limit the impact of the incident if safe to do so. The most senior relevant person should also be informed.
1.2 Should any situation pose imminent danger to others, attempts should be made to
reduce the risk to the environment, staff patients and the public (i.e. first aid, emergency services, administering drugs, isolation of area, wearing protective clothing etc).
1.3 Immediate notification to external agencies such as the Police or Coroner should be
considered when appropriate and following advice from the Chief Nurse or Head of Corporate Governance.
1.4 Documenting and reporting the incident is done by completing the Incident
Reporting Form (Appendix D). This form should be completed within 24 hours of the incident taking place.
1.5 The completed form is reviewed by the Corporate Governance Manager and an initial
risk assessment is undertaken. This initial assessment will include any immediate actions required and also if the incident has met the threshold to be considered a Serious Incident. Advice is available from the Chief Nurse or the Designated Nurse for Safeguarding Children and LAC.
1.6 If the incident has not reached the threshold to be considered a Serious Incident, the
Corporate Governance Manager will determine what further actions are required to investigate the incident and identify any appropriate learning.
1.7 Learning from incidents will be used to make any necessary changes within the
CCG and to mitigate the risk to individuals and the organisation. 1.8 If the incident has met the threshold to be considered a Serious Incident, the
process to be followed should be in line with the NHS England Serious Incident Framework 2015.
2. PROCEDURES IN RELATION TO SERIOUS INCIDENTS 2.1 Any incident considered as a serious Incident will need to be recorded on Strategic
Executive Information (STEIS). This recording will be carried out by the Quality and Safety Team.
2.2 Certain Government agencies or statutory bodies require notification of certain
incidents. The main agencies that require notification are listed below:
• Health & Safety Executive (HSE) - RIDDOR • NHS Property Services Limited / Community Health Partnerships Limited • Medicines and Healthcare Regulatory Agency (MHRA)

18
• Police • Fire • Coroner • Environment Agency • NHS Counter Fraud Authority • Doncaster CCG Quality Team • Information Commissioner’s Office • It is recommended that specialist advice regarding external reporting is sought
from the Head of Health, Safety and Security and Associate Director of Corporate Services.
2.3 NHS England will also need to be informed of any Serious Incident reported by the CCG. NHS England has the responsibility of performance managing any CCG Serious Incident.
2.4 A person responsible for contacting relevant parties (i.e. staff, patient(s), carer(s),
relative(s), public, visitor, and contractor) should be identified. It must be noted that any individuals involved in incidents, including relatives, must be informed. (Duty of Candour).
2.5 Appropriate support and information should be made available to those involved in
the incident. 2.6 The Incident will be investigated and managed in line with the NHS Serious
Incident Framework and follow Root Cause Analysis or NHS Counter Fraud Authority methodology.
2.7 The appropriate people or person to lead and undertake any investigation will be
identified by the CCG Senior Management Team after considering the nature of the incident, skills required to investigate and any potential conflicts of interest.
2.8 The CCG will ensure that it has access to appropriately skilled and relevant staff
to be able to undertake robust and transparent investigations. 2.9 The Incident Management Group of the CCG will provide internal assurance of
the Incident report within the required timescales. 2.10 Final CCG sign off will be by the Chief Nurse or Head of Corporate Governance. 2.11 A final report will be made to NHS England within the time scales identified within
the NHS England Serious Incident Framework. 2.12 Any learning from the investigation and subsequent action plans will be monitored
through the Q&PSC. 3. TRENDS AND LESSONS LEARNT 3.1 Serious incident trends, themes, patterns and lessons learnt will be analysed and
reported to the appropriate committees. Lessons learnt will be disseminated appropriately across the health community and to other relevant groups to minimise the risk of reoccurrence.

19
4. SERIOUS INCIDENTS INVOLVING A DONCASTER CCG COMMISSIONED SERVICE
4.1 The CCG has the responsibility for ensuring that serious incidents are appropriately
reported and managed for any service which it commissions for NHS patients. This responsibility is discharged through continued arrangements with providers.
4.2 All incidents considered Serious Incidents should be reported in line with the
current NHS England Serious Incident Framework. 4.3 Full report, including Root Cause Analysis or other similar investigation process
and action plan will be provided in line with the Framework. There may be occasions when more time is required e.g. awaiting the outcome of a criminal investigation, but this will be decided on a case by case basis.
4.4 All providers are contractually required to report all Serious Incidents occurring
within their organisation on STEIS. 4.5 If the provider does not have access to STEIS, they are required to inform the
CCG of the incident and the Quality and Safety Team can input the incident on STEIS.
4.6 It is important that the organisation appropriately responds to the potential for media
interest in a particular incident. A Serious Incident may trigger the preparation of a media response based on the available information by the appropriate Chairperson, Chief Nurse and the Head of Communications and Engagement. All media communications must be led by and approved by the Head of Communications and Engagement.
4.7 Where potential media interest exists, the appropriate Chief should be notified
even if the incident was not previously considered to be a Serious Incident.

20
SECTION D – NHS DONCASTER CCG SERIOUS INCIDENT PERFORMANCE MANAGEMENT PROCEDURES 1. PERFORMANCE MONITORING THE MANAGEMENT OF SERIOUS
INCIDENTS (EXCEPT CHILD SAFEGUARDING INCIDENTS) 1.1 As a lead commissioning organisation, the CCG has a specific duty to provide
assurance for the reporting and management of serious incidents occurring at their main providers, commissioned services, foundation trusts, independent care providers etc. This will be discharged through the following procedure:
• The Serious Incident notification is received via STEIS and logged on the
Doncaster CCG Serious Incident Database. • Ensure local NHS England Area team have been notified in the case of the
following types of incident:- • Outbreaks of infectious diseases including Pandemic Flu outbreak
• Child aged 17 or under being admitted to adult mental health bed
• Serious incidents involving Trainee Doctors
• Never Events
• Homicide involving a service user
• Incidents relating to NHS England commissioned services • Identify Trust Lead for investigation and advise the service involved of the target
for submission of investigation report and the need to update on a monthly basis. • Exceptions will only be considered in the case of a Police, Coroner etc.
investigation and extenuating circumstances. Requests for extensions should be submitted in writing/email.
• If an interim report is submitted, ensure monthly updates are received until a final
report is submitted (even if it is to say there is no further progress). • Once a full report is received, submit to Incident Management Group who will
review the report. The report will be reviewed appropriately and any feedback will be provided to the lead investigator.
• If the Incident Management Group agrees the report as being unsatisfactory it is
returned to the local trust lead for further information within a specified timescale. • If the Incident Management Group recommends the report for closure it is ‘closed
on STEIS. All associated actions are monitored through the Acute Clinical Quality

21
Review Group (unless otherwise agreed by the Incident Management Group). • Lessons learnt need to be included within the STEIS form prior to closure to allow
for shared learning across the Regional teams. 1.2 In principle the CCG should share information with NHS England in an open and
transparent way to facilitate appropriate management and communication. 1.3 In the case of a Serious Incident involving mental health service users committing
homicide, the CCG will follow the NHS England Single Operating Framework in relation to Investigating Mental Health Homicides.
1.4 The CCG will work with NHS England as required to facilitate and support any
independent investigations that are required. 2. PERFORMANCE MONITORING THE MANAGEMENT OF CHILD
SAFEGUARDING SERIOUS INCIDENTS 2.1 Where the incident involves a child or younger person, considerations should be
given to raising the alert as a Serious Incident. The following process should be undertaken by the CCG when monitoring the management of child safeguarding serious incidents that have occurred within Doncaster.
• The child safeguarding serious incident is received and logged on STEIS using the
notification report and the CCG Serious Incident database within 24 hours of being alerted.
• Identify and log the investigator on the Serious Incident database. • Inform the Designated Nurse of the target for completion of investigation report
date in writing and the need to update on a monthly basis. • Ensure the Designated Nurse updates in relation to any significant developments. • Once the Safeguarding process is complete and relevant reports produced, the
CCG will consider the closure of the incident through the Incident Management Group.
• If the Incident Management Group agrees the report as being unsatisfactory it is
returned to the local trust lead for further information within a specified timescale. • If the Incident Management Group recommends the report for closure it should be
submitted to NHS England Local Team via the Safe Haven e-mail address. A request to close the Serious Incidents is submitted to the Area Team.
3. MONITORING SERIOUS INCIDENT TRENDS, THEMES AND PATTERNS 3.1 Serious incident trends, themes, patterns and lessons learnt will be analysed and
reported to the appropriate committees and NHS England local Team via STEIS.

22
3.2 In cases where there is evidence that the incident is part of a worrying trend or where the circumstances or consequences of the incident are exceptionally serious, the CCG may need to instigate a wider investigation.
• The CCG may ask the Trust to undertake further inquiries or suggest a particular
course of action. • Or may decide that a more independent investigation of the incident in required
and work with the Trust to facilitate this.
4. OBTAINING ASSURANCE OF ACTION PLAN COMPLETION 4.1 The CCG will gain assurance by exception on each Provider’s serious incident
action plans to determine whether all actions have been completed in accordance with the plan.
4.2 Performance management of Provider action plans will take place within the
existing contractual and governance structures and process. 5. REPORTING ON NEVER EVENTS 5.1 The CCG will monitor the occurrence of Never Events within the services they
commission. Providers are required to publish information on the occurrence of never events as part of their annual Quality Account. The reporting of Never Events and associated actions will be in line with the current published guidance at the time.

23
USEFUL CONTACTS
APPENDIX A
Doncaster CCG
Directorate of Quality and Patient Safety
Chief Nurse 01302 566211 Head of Corporate Governance 01302 566216 Corporate Governance Manager 01302 566216 Deputy Chief Nurse 01302 566276 Designated Nurse for Safeguarding Adults 01302 566099 Quality & Patients Safety Manager 01302 566056 Quality Support Officer 01302 566054
Safe Haven Fax
Doncaster CCG 01302 556321
Other agencies / bodies Reporting Safety Problems for Medicines, Blood and Devices – MHRA www.mhra.gov.uk
Health and Safety Executive (HSE) Reporting including RIDDOR – www.hse.gov.uk or 0845 300 99 23 NHS Commissioning Board Special Health Authority www.england.nhs.uk/
Local Counter Fraud Specialist (LCFS) Reporting fraud – 360 Assurance NHS Counter Fraud Authority for Fraud and Security issues - https://cfa.nhs.uk/
Report fraud - https://www.reportnhsfraud.nhs.uk - 0800 028 4060
Legal Advice via Corporate Services / Head of Corporate Governance Care Quality Commission – www.cqc.org.uk or 03000 616161
NHS Property Services- www.property.nhs.uk/
Monitor - www.gov.uk/government/organisations/monitor Information Commissioner Office www.ico.gov.uk email: [email protected]

24
Appendix B - Reportable External Bodies
Type of Incident
Method
Report To / From
Timescales
RIDDOR: Reporting of Injuries, Diseases and Dangerous Occurrences Regulations 1995
On-line / by telephone. Information to be supplied to the Head of Specialist Advice, Health and Safety who will contact external agencies. http://www.hse.gov.uk/riddor/report.htm 0345 300 9923 (opening hours Monday to Friday 8.30 am to 5.00 pm).
Line Manager to Head of Health and Safety / Corporate Services Head of Health and Safety / Corporate Services to report to Health and Safety Executive. Health and Safety Executive Foundry House 3 Millsands Riverside Exchange SHEFFIELD S3 8NH
Line Manager to report: Deaths / Major injuries / Dangerous occurrences/ Diseases – immediately (within 10 days of the incident occurring) Injury resulting in absence from work for over 7 days –within 15 days Admission of a patient/visitor into A&E from your premises due to an injury- immediately (within 10 days of the incident occurring) Guidance can be found http://www.hse.gov.uk/riddor/reportable- incidents.htm
Incidents that may lead to litigation
Telephone Line Manager to report to Head of Corporate Governance / Corporate Services (Claims) Head of Corporate Governance (Claims) to: NHS Litigation Authority 2nd Floor 151 Buckingham Palace Road London SW1W 9SZ
Line Manager: Head of Corporate Governance / Corporate Services (Claims) As soon as risk of possible litigation identified Head of Corporate Governance (Claims): NHS Litigation Authority Within 48 hours of notification

25
Type of Incident
Method
Report To / From
Timescales
For incidents relating to buildings, plant and non-medical equipment (dependent on type and severity)
Head of Specialist Advice, Health and Safety NHS Property Services Ltd Oak House Moorhead Way Bramley Rotherham S66 1YY T: 01709 302119
Head of Specialist Advice, Health and Safety Immediately Head of Specialist Advice, Health and Safety to report to: NHS Property Services Ltd Within 24 hours
Physical Assault Online reporting system Head of Health, Safety & Security) via reception to: NHS Counter Fraud Authority https://cfa.nhs.uk/
Head of Specialist Advice, Health and Safety via reception to: NHS Counter Fraud Authority Within 5 working days of notification of the incident report
Fire - any incident, no matter how small, involving fire or fire warning systems, or false alarm, resulting in Fire Brigade attendance should also be reported using the Fire Safety Policy.
Online reporting system & documentation in the fire manual. A copy of the latter should be sent to the fire officer with the original kept in the fire log book
Discovery of a fire or fire alarm sounding, anyone via (9)999 to the fire service All false alarms (including unwanted fire signals) should be reported annually as part of Estates Return Information Collection (ERIC) returns. (although CCG’s do not have to complete an ERIC return). Head of Specialist Advice, Health and Safety
Line Manager to report to: Head of Corporate Governance Immediately Head of Specialist Advice, Health and Safety to: Fire Officer Within 24 hours

26
Type of Incident
Method
Report To / From
Timescales
Information Governance Incidents
Online reporting system and telephone If it is likely to be a Serious Incident (IG SIRI) then the Head of Corporate Governance / Corporate Services should be consulted. Head of Corporate Governance / Corporate Services to report to the Information Commissioners Office as appropriate.
Line Managers to report Serious Incidents to: Head of Corporate Governance / Corporate Services Immediately
Fatality - apparent or potentially as a consequence of alleged patient action; self-harm or contributory action by staff.
Online reporting system and Email or in case of very serious incident telephone
STEIS NHS Doncaster, Patient Safety Team
Within 24 hours of incident
Within 1 working day

APPENDIX C
Serious Incident Performance Monitoring – Flowchart
NHS DONCASTER DBHTFT Independent Care
Providers RDaSH
Local Trust leads the investigation
NHS Doncaster generate reminder or request further information
NHS Doncaster inform the Trust in writing of target date for completion
of investigation and report
Investigation report to Incident Management Group (IMG)
Full Report Exception Report No Available report
Serious incident reported and logged Clock Starts
Unsatisfactory Report with no
evidence of sharing and
learning outcomes
Satisfactory report with evidence of sharing learning outcomes Reporting in line
with NHS England Serious Incident Framework
IMG to agree closure where appropriate
Closure request for NHS Doncaster CCG Serious Incidents to be agreed by NHS England Area Team.
Cont
inua
l mon
itorin
g by
Qua
lity
Team

28
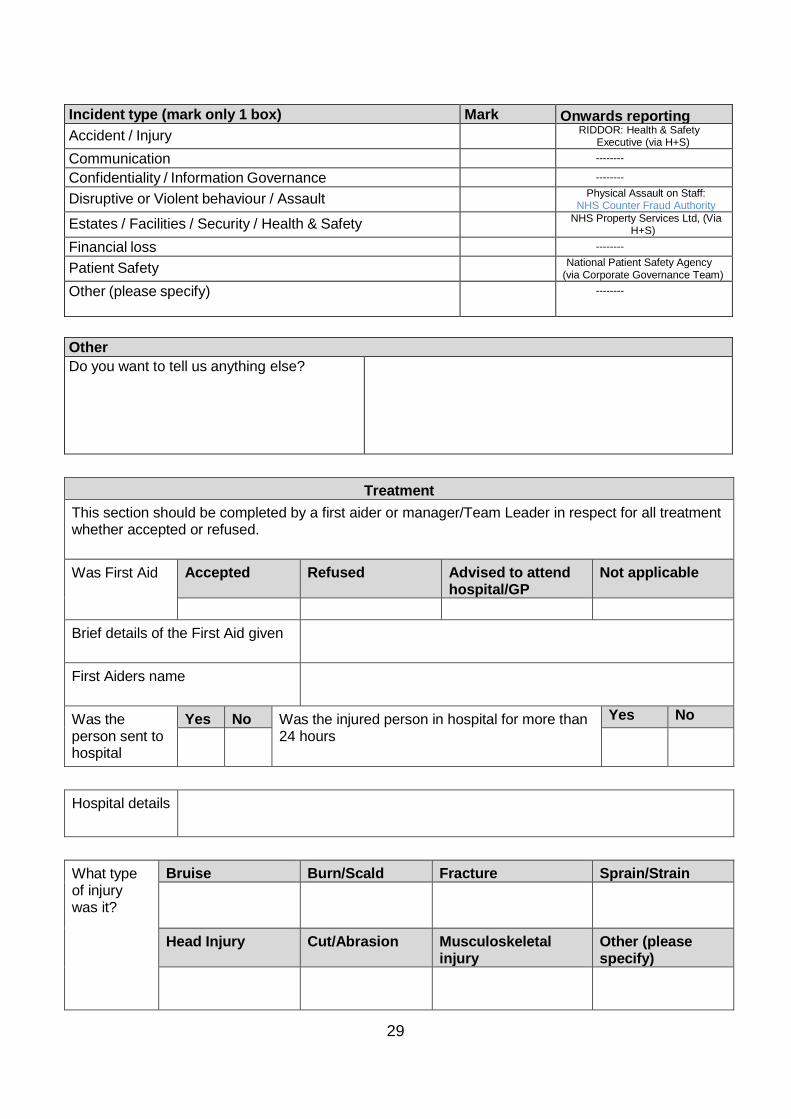
APPENDIX D
NHS DONCASTER CCG INCIDENT REPORTING FORM
Incident reporter details Name: Role: Date reported:
Incident description Date / Time of Incident?
Name of person(s) involved in the incident.
What happened? Describe the Incident, exact events leading up to and including the incident. (please record facts only, not opinion or second hand information.)
Where did the incident happen? (describe the location)
Name of witness(es) to the incident.
Were there any adverse effects / factors which may have played a part in the incident? (weather conditions, traffic, floor surface condition, record injuries, financial costs, loss of service, reputational impact etc)
29
Incident type (mark only 1 box) Mark Onwards reporting Accident / Injury RIDDOR: Health & Safety
Executive (via H+S) Communication --------
Confidentiality / Information Governance --------
Disruptive or Violent behaviour / Assault Physical Assault on Staff: NHS Counter Fraud Authority
Estates / Facilities / Security / Health & Safety NHS Property Services Ltd, (Via H+S)
Financial loss --------
Patient Safety National Patient Safety Agency (via Corporate Governance Team)
Other (please specify)
--------
Other Do you want to tell us anything else?
Treatment
This section should be completed by a first aider or manager/Team Leader in respect for all treatment whether accepted or refused. Was First Aid Accepted Refused Advised to attend
hospital/GP Not applicable
Brief details of the First Aid given
First Aiders name
Was the person sent to hospital
Yes No Was the injured person in hospital for more than 24 hours
Yes No
Hospital details
What type of injury was it?
Bruise Burn/Scald Fracture Sprain/Strain
Head Injury Cut/Abrasion Musculoskeletal injury
Other (please specify)

30
Type of incident
Near miss Minor injury
Major injury
Ill Health Road Traffic Collision
Post-incident actions What actions were taken after the incident?
Are any further actions planned?
Please return the completed form as soon as possible after the incident to:
Corporate Governance Team, Sovereign House, Heavens Walk, Doncaster, DN4 5HZ Or by email to [email protected]
Office use only Date received
Logged

31
APPENDIX E - Incident Reporting Flow Chart
Near Miss Accident
Incident Occurs
Health & Safety Incident Near Miss Accident
Dangerous Occurrence
Patient Identifiable Information (PID)
Information Governance Incident
For “Provider” Serious Incidents or Never Events please refer to appendix C
IMMEDIATE ACTION Inform:
Data Protection Officer Caldicott Guardian SIRO IMMEDIATE ACTION
The immediate needs of those involved are dealt with The environment is made safe – seek Health & Safety advice if required All evidence is retained intact Any defective equipment is withdrawn from m use Witness details are taken
PID passed to Caldicott support officer
Complete incident report form and assess incident against the HSCIC Serious Incident requiring investigation checklist to determine whether Level 1 or Level 2
Breach responded to as appropriate by secure email, verbal, letter
Level 2 incident identified – treat as serious incident – record on IG Toolkit (for notification to DH & ICO within 24 hours)
All information logged onto DCCG Caldicott log master
Level 1 incident identified (follow process below)
If the accident/dangerous occurrence is reportable under RIDDOR. Inform the health and safety team RIDDOR report is completed and submitted by the responsible person/person in control of premises with assistance from the health & safety team
Log presented at the monthly information Governance meetings
Complete an Incident Report Form Manager to complete relevant section of the form Investigate the incident and develop an action plan (if required) Implement the action plan Ensures learning from incident is shared with staff

32
Appendix F Equality Analysis Form
Subject of equality analysis
Incident Management Policy
Type Tick Policy √ Strategy Business case Commissioning service redesign Contract / Procurement Event / consultation
Owner Name: Helen Harris Job Title: Head of Corporate Governance
Date 17 October 2018 Assessment Summary
The overall purpose of the policy is to set out the CCG’s approach to Incident Management Policy within the workplace. The policy will also set out guidance to staff and managers about their responsibilities in relation to the reporting of serious incidents. NHS Doncaster CCG (the CCG) has a responsibility to ensure that the investigation and management of serious incidents in services which they have commissioned is effective and are responsible for holding providers to account for managing responses to serious incidents. This document demonstrates and provides assurance that the CCG has systematic measures in place to respond to incidents requiring investigation and has robust performance management arrangements in place to ensure serious incidents are managed and investigated by providers according to best practice. These measures must protect patients and result in organisations learning from serious incidents to minimise the risk of the incident happening again. When an incident occurs it must be reported to all relevant bodies.
Stakeholders
Tick Staff √ General public √ Service users Partners Providers Other
Data collection and consultation
Please note that due to the small number of staff employed by the CCG, data with returns small enough to identity individuals cannot be published. However, the data should still be analysed as part of the EIA process, and where it is possible to identify trends or issues, these should be recorded in the EIA. Consultation on the updated policy has taken place locally.

33
Other policies related to or referred to as part of this analysis:
Protected characteristic Positive Neutral Negative
Negative: What are the risks?
Positive: What are the benefits / opportunities?
Age
x
This policy applies to all regardless of age
Disability
x
This policy applies to all regardless of disability.
This policy is not currently available in other formats. The assumption is that all staff will have the correct
physical equipment on their desktops to ensure that
they will be able to view this document. The CCG
website does provide the facility to view documents in
larger fonts.
Gender
x
This policy applies to all regardless of gender
Race
x
This policy applies to all staff regardless of
race/ethnicity. Analysis of employee data
indicates that the percentage of white
employees is reflective of the local population.
However, the proportion of BME staff is lower than that
of the local population it serves
All staff require competencies which
include the ability to read and understand English or
to request the information in another format available to
them.
Religion & Belief
x
This policy applies to all regardless of religion or
belief
Sexual
Orientation
x
This policy applies to all, regardless of sexual
orientation

34
Protected characteristic Positive Neutral Negative
Negative: What are the risks?
Positive: What are the benefits / opportunities?
Gender
reassignment
x
This policy applies to all regardless of
transgender/gender reassignment
Pregnancy & Maternity
x
This policy applies to all regardless of pregnancy or
maternity
Marriage & Civil
Partnership
x
This policy applies to all regardless of marriage or
civil partnership
Social Inclusion / Community Cohesion
x This policy applies to all.
Conclusion & Recommendations including any resulting action plan
As the policy is written in English there is a potential impact on employees whose first language is not English and therefore may struggle reading the policy. The CCGs internal ‘portal’ and external website signpost individuals to alternative formats such as large print, braille or another language. Responsible lead: CCG Communications.
Review date October 2020