in Brief - University of Missouri System
6
Policy in Brief This is the first edition of the Policy in Brief, a regular publication of the Institute of Public Policy, examining an issue of interest to policy makers. This first edition provides several snapshots of the elderly population, including descriptions of some of the services provided to older adults and some of the circumstances experienced by those 65 years of age and older. As the country and our state experience significant growth in the number of senior citizens, policy makers will increasingly be confronted with issues requiring information- based decision making in order to meet the needs of the elderly. UNIVERSITY OF MISSOURI-COLUMBIA INSTITUTE OF PUBLIC POLICY VOLUME 1 NO. 1 JUNE 2001
Transcript of in Brief - University of Missouri System

Policy in Brief
This is the first edition of the Policy in Brief, a
regular publication of the Institute of Public Policy,
examining an issue of interest to policy makers.
This first edition provides several snapshots of the
elderly population, including descriptions of some
of the services provided to older adults and some
of the circumstances experienced by those 65
years of age and older. As the country and our
state experience significant growth in the number
of senior citizens, policy makers will increasingly
be confronted with issues requiring information-
based decision making in order to meet the needs
of the elderly.
U N I V E R S I T Y O F M I S S O U R I - C O L U M B I AI N S T I T U T E O F P U B L I C P O L I C Y
VOLUME 1 NO. 1 JUNE 2001

During the past century, the percentageof Americans who are age 65 years andolder has more than tripled, from just over4% of the total population in 1900 to nearly13% of the total population in 1999. Older indi-viduals comprise 1 in every 8 Americans, num-bering some 34.5 million persons. Othercharacteristics of the senior population of inter-est include the following:
■ In the next 30 years, the number ofseniors in the U.S. is expected to dou-ble from just under 35 million in 1999 toapproximately 70 million by 2030;
■ While nearly 15% of the white population isage 65 and above, only 8.4% of the AfricanAmerican population and 5.9% of theHispanic population were age 65 andolder in 1999;
■ In 1999, nearly 16% of all elderly indi-viduals, approximately 5.2 million sen-iors, were classified as poor or nearlypoor (up to 125% of the federal povertylevel); among seniors reporting income, justover one-third reported less than $10,000 peryear from all income sources, with an average(median) income reported at $14,425; and
■ Average out-of-pocket expenditures onhealth care among seniors averagedalmost $3,000 in 1998, which reflects a 33%increase since 1990. These expendituresbreak out as follows: $1,528 (52%) for insur-ance, $670 (22%) for drugs, $596 (20%) formedical services, and $142 (5%) for medicalsupplies.
(Source: Administration on Aging, Profile of Older Ameri-cans: 2000; and Current Population Reports, P25-1130Series, February, 1996)
Popu l a t i on Number s
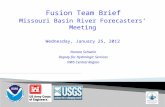
As indicated in Table 1, Missouri has a slightlylarger percentage of individuals age 65 and olderthan the nation as a whole. Overall, Missouriranks 14th among all states in the size of its eld-erly population. In 1999, there were 745,684persons age 65 and older living in Missouri; thisrepresents 13.6% of the state’s total population.By 2010, the number of seniors in Missouri isprojected to increase to 1.137 million, or 20.2%of the state’s population, as the so-called baby-boom generation moves beyond middle age.
Another way of describing the expectedgrowth in Missouri’s elderly population is to
note that between 2000 and 2025, thenumber of Missourians age 65 and olderis projected to increase by 66% to over1.2 million.
(Source: Administration on Aging, Profile of OlderAmericans: 2000; U.S. Census Bureau; andMissouri Department of Social Services)
Urban v s Rura l Res i dence
The majority of Missouri’s elderly residein rural areas. In 1990, the latest year forwhich state-specific information is avail-able, 65% of those 65 years and olderlived in areas classified as rural by theU.S. Census Bureau.
(Source: Missouri Census Data Center)
28.48
22.55
17.69
13.64
6.54
1.79
27.27
21.24
16.52
12.67
5.99
1.53
0 5 10 15 20 25 30
50+
55+
60+
65+
75+
85+
Old
er P
opul
atio
n by
Sel
ecte
d A
ge G
roup
s
Percentage of total population
US TotalMissouri
Table 11999 US Census Estimates of Older Population for StatesJuly 1, 1999
Policy in Brief
Introduction
2I N S T I T U T E O F P U B L I C P O L I C Y

Househo ld I n come
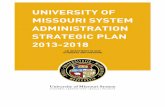
According to the 1990 U.S. Census,14.8% of Missourians who are 65 years ofage and older have incomes below thefederal poverty level. Looking at specificincome levels for Missouri seniors we find:
■ 34.11% report annual incomes of lessthan $10,000
■ 50.95% report annual incomes of lessthan $15,000
■ 72.66% report annual incomes of lessthan $25,000
■ 84.39% report annual incomes of lessthan $35,000
(Source: 1990 U.S. Census Bureau)
Hea l th I n su rance
Health insurance, while an issue of con-cern for all Missourians, is especiallyimportant for elderly persons due toincreased medical needs. As shown inTable 3, nearly all Missourians age 65and older are covered by some form ofinsurance. Not surprisingly, the near uni-versal health insurance coverage is duelargely to enrollment in Medicare. Cen-sus information for 1998 shows thatwhile 16.3% of the total U.S. populationlacked health insurance, only 1.1% ofAmericans age 65 and older were notcovered by some type of health insur-ance plan.
In addition to Medicare and privatehealth insurance, a relatively small num-ber of Missouri seniors receive healthinsurance coverage through Medicaid,the public health insurance program forlow-income individuals. In December,2000, 77,111 elderly Missourians, or justover 10% of the total senior population,were enrolled in Medicaid; this repre-
sents 9.25% of all Missourians receivingMedicaid. An additional 9,500 seniors,just over 1% of all Missouri seniors, quali-fied for Medicaid through the spend-down program during calendar year2000. The spenddown program allowsindividuals who would otherwise not
qualify to become eligible for Medicaidcoverage once they have incurred suffi-cient medical expenditures.
(Source: U.S. Census Bureau: Statistical Abstract ofthe United States: 2000; Missouri Department ofSocial Services)
Missouri’s Senior Population: The Facts
0.00%
5.00%
10.00%
15.00%
20.00%
25.00%
Less
than $
5,000
$5,00
0 to
$9,99
9
$10,0
00 to
$14,9
99
$15,0
00 to
$24,9
99
$25,0
00 to
$34,9
99
$35,0
00 to
49,9
99
$50,0
00 to
$74,9
99
$75,0
00 to
$99,9
99
$100
,000
or m
ore
Household Income
Per
cen
tage
of
Ind
ivid
ual
s 6
5 Y
ears
an
d O
lder
Table 2Percentage of Individuals 65 Yearsand Over by Household Income, 1990
Missouri
United States
3P O L I C Y I N B R I E F : J U N E 2 0 0 1
Table 3Health Insurance for Missourians 65 years and Older
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
1999 1998 1997 1996 1995 1994 1993 1992 1991 1990 1989
Total Private Insurance
Medicaid
Medicare
Covered by SomeInsurance

Policy in Brief
Pres c r i p t i on Drug Cos t s
The rising costs of pharmaceuticals and lack ofaccess to affordable prescription drugs can resultin financial hardships and diminished health sta-tus for senior citizens. Although elderly personscomprise only about 14% of the total popula-tion, they account for approximately one-thirdof the expenditures on prescription drugs.
While most seniors have public, private orboth types of health insurance, estimates arethat approximately one-third of this population,some 11 million older Americans, lack any typeof prescription drug insurance coverage. TheMissouri Department of Insurance reports thatfor Missouri seniors covered by private “Medi-gap” plans, only 5.2% of these plans offer effec-tive prescription drug coverage.
In addition, the annual rate of increase in pre-scription drug spending nationwide, estimated at18.4% for 1999, is more than three times theaverage annual increase in overall health-relatedspending (5.3%). Retail sales of prescriptiondrugs increased from $68.6 billion in 1995 to$121.7 billion in 1999.
As of December, 2000, 22 states havepassed some form of pharmacy assistance law; anumber of initiatives at both the federal andstate level continue to be proposed to addressthe problems posed by rising prescription drugscosts. Of particular interest are the following:
■ The state of Maine instituted pharmaceuticalprice controls in 2000;
■ A number of states require pharmacies thatserve Medicaid beneficiaries to provide a dis-count similar to that offered toMedicare beneficiaries;
■ Several states have obtained or are seekingwaivers by which to qualify additional low-income elderly in full Medicaid coverage orpartial Medicaid coverage for prescriptiondrugs only;
■ State bulk purchasing arrangements(and multi-state regional buying pools) havebeen implemented in a handful of states, inorder to achieve greater discounts for eligiblegroups; and
■ Federal proposals include providing pre-scription drug insurance coverage for thosewho are eligible for Medicare and who haveeither catastrophic drug expenses or familyincome at or below 175% of the federalpoverty level, or both, until a prescriptionbenefit is implemented as part of overallreform of the Medicare program.
(Source: National Conference of State Legislatures, “StateSenior Pharmaceutical Assistance Programs, 2/5/01; U.S.Census Bureau, Statistical Abstract of the United States2000).
Long-Te rm Ca re
The long-term care facilities regulated by thestate are categorized by the level of care theyprovide and the acuity or functioning level ofresidents. Information on fiscal year 2000 bedcapacity and census count by facility type is pro-vided in Table 4.
The occupancy rate during Fiscal Year2000 for all long-term care facilities in Missouriwas 79.2%.
In 1994, MissouriCare Options (MCO)was implemented by theDivision of Aging, as away to offer home andcommunity-based alterna-tives to long-term facility-based care. In addition tooffering senior citizens theindependence and com-fort of remaining in theirhomes and communities, MCO provides consid-erable savings by way of avoiding or postponingcostlier institutional care. For example, in FiscalYear 2000, nursing facility care averaged$32,385 per participant per year, as compared toan average annual cost of $3,914 per participantfor home and community-based care. Alterna-tives to facility-based care in Fiscal Year 2000resulted in an estimated cost avoidance to thestate of nearly $82.5 million. One of these alter-natives is adult day care; there are 72 suchfacilities in Missouri, which served 1,401 partici-pants in Fiscal Year 2000. These alternatives take
4M I S S O U R I ’ S E L D E R L Y P O P U L A T I O N
467 51,313 39,582
79 4,948 3,865
684 22,261 14,376
1,230 78,522 57,823
Table 4Long-Term Care Facilities in Missouri (FY2000)
Number of Beds Number of Facilities Census
Skilled NursingFacilities
IntermediateCare Facilities
Residential CareFacilities
Total

5
Policy in Brief
I N S T I T U T E O F P U B L I C P O L I C Y
on increased significance in light of the nation-wide projections that by the year 2030, some10.8 million seniors will require some type oflong-term care services, compared with nearly 7million in 2000.
(Source: Missouri Division of Aging: State Fiscal Year2000 Service Operations Summary)
Elderly Abuse, Neglect and Exploitation
Missouri has implemented a number of adminis-trative and statutory provisions aimed at protect-ing the elderly from abuse and neglect. TheDivision of Aging maintains a toll-free, 24-hour hotline for the reporting of abuse andneglect of seniors (1-800-392-0210). Missourilaw requires individuals who provide certaintypes of services to the elderly, including healthcare, social service, and law enforcement profes-sionals, to report suspected instances of abuse,neglect or exploitation to the Division of Aging.In addition, long-term care facilities are requiredto obtain criminal background checks onprospective employees, and are prohibited fromknowingly employing anyone who is listed onthe Division of Aging’s employee disqualifi-cation list (EDL). The Division is authorizedto place persons on the EDL for a number ofillegal or inappropriate actions. Elder care work-ers hired after 12/31/00 are also required to reg-ister with the Family Care Safety Registrymaintained by the Department of Health, forpurposes of obtaining criminal and related back-ground checks for such individuals; this registryalso documents whether elder care facilitieshave experienced licensure suspensions, revoca-tions or denials.
The Division of Aging reports that during Fis-cal Year 2000, 8,704 investigations of allegedabuse and neglect were completed; 28% ofthese, or 2420 allegations, were found to bevalid. Among the reports found to be substanti-ated, the most common type of abuse in institu-tional settings is physical abuse. This contrastswith the most common type of abuse in homeand community settings, where physical neglectand emotional neglect are much more fre-
quently found. Penalties for elderly abuse andneglect range from a Class A misdemeanor to aClass A felony.
(Source: Division of Aging, State Fiscal Year 2000 ServiceOperations Summary; Missouri Revised Statutes)
Services for the Elderly in Other States
Currently, Missouri’s Division of Aging is one offive divisions within the Department of SocialServices. While this administrative structure innot uncommon, 17 states have established exec-utive departments or commissions that workexclusively with aging-related issues. Those states are:
AlabamaCaliforniaFloridaIdahoIllinoisIowaKansasMarylandMassachusetts
New MexicoNew YorkOhioPennsylvaniaRhode IslandTexas VirginiaWest Virginia
(Source: Administration on Aging, “State Agencies onAging”)

6
Policy in Brief
I N S T I T U T E O F P U B L I C P O L I C Y
Administration on Aging. 1999 Census Estimates ofthe Older Population for States: Older Population bySelected Age Groups. Data as of July 1, 1999.Retrieved January 11, 2001 from the World WideWeb: http://www.aoa.dhhs.gov.
Administration on Aging. State Agencies on Aging.Retrieved January 11, 2001 from the World WideWeb: http://www.aoa.dhhs.gov.
Administration on Aging, Profile of Older Americans:2000
Current Population Reports, P25-1130 Series,February, 1996
Missouri Census Data Center, 1990 CensusSummary Tape File 3. February 15, 2001.
Missouri Department of Social Services, Divisionof Aging. Abuse, Neglect and Exploitation of Seniorsand Adults with Disabilities: Annual Report, Fiscal Year1999. May 2000.
Missouri Department of Social Services, Division of Aging. Plan on Aging. RetrievedFebruary 8, 2001 from the World Wide Web:http://www.dss.state.mo.us/da/plan/demog.htm
Missouri Department of Social Services, Divisionof Aging: State Fiscal Year 2000 Service OperationsSummary
Missouri Department of Social Services, Researchand Evaluation Unit. Missouri Medicaid Eligibility.December 31, 2000.
National Conference of State Legislatures, “StateSenior Pharmaceutical Assistance Programs”,2/5/01
U.S. Census Bureau. Health Insurance CoverageStatus and Type of Coverage by State, All People: 1987to 1999.
U.S. Census Bureau, Statistical Abstract of the UnitedStates: 2000
U.S. Census Bureau. Tiger Mapping Service DigitalMap Database. Age of Householder by HouseholdIncome in 1989, 1990 US Census Data: UnitedStates. Retrieved January 11, 2001 from the WorldWide Web: http:// venus.census.gov
U.S. Census Bureau. Tiger Mapping Service DigitalMap Database. Age of Householder by HouseholdIncome in 1989, 1990 US Census Data: Missouri.Retrieved January 11, 2001 from the World WideWeb: http:// venus.census.gov
The information in the Policy
In Brief is compiled by the
Institute of Public Policy at
the University of Missouri -
Columbia. The Policy In
Brief may be freely photo-
copied or otherwise distrib-
uted with attribution.
Please contact us at:
Institute of Public PolicyUniversity of Missouri-
Columbia265 McReynolds HallColumbia, MO 65211Phone: (573) 884-3381Fax: (573) 884-4872E-mail: [email protected]
Refe rence s