in Adults With Mental Retardation Fitness and Work ... · PDF fileADAPTED PHYSICAL ACTIVITY...
31
ADAPTED PHYSICAL ACTIVITY QUARTERLY, 1992, 9, 148-178 Effects of Reinforcement Based Exercise on Fitness and Work Productivity in Adults With Mental Retardation Ronald Croce Michael Horval University of New Hampshire University of Georgia The present study evaluated the effects of a reinforcement based aerobic and resistance exercise progratn on three obese men with mental retardation and below average fitness levels. A multiple-baseline-across-subjects design was employed to evaluate treatment effectiveness and retention of treatment effects on five dependent measures: body weight, percent body fat (body composition), oxygen consumption (predicted max VO, in ml/kg/min), composite isometric strength (in kg of force), and work productivity (pieces of work completed). Subjects improved during treatment from their baseline scores on cardiovascular fitness, strength, and work productivity mcasure- ments (1~.05); however, retention of gains made during treatment were inconsistent and the data that indicated subjects' scores were regressing back toward baseline tneasurements. There were no significant differences for body wcight and percent body fat lneasiiretnents for treatment and rctcntion phases (11>.05). Results indicated that adults with mental retardation respond to a progressive exercise program in much the same tnanncr as thcir nonretarded peers and that such an exercise progratn can facilitatc job performance. Due to recent trends in the general population to exercise for health and psychological benefits, researchers are focusing on systelnatically evaluating the fitness of individuals with mental retardation (Coleman, Ayoub, & Friedrich, 1976; Reid, Montgomery, & Seidl, 1985) as well as the effects exercise programs have on various behavioral (Schurrer, Weltman, & Bramtnell, 1985; To~nporow- ski & Ellis, 1984, 1985), psychological (Brown, 1977; Tomporowski & Ellis, 1984, 1985),and physiological (Bennett, Eisenman, French, Henderson, & Shultz, 1989; Croce, 1990; Combs & Jansma, 1990) parameters. Researchers have consistently reported that individuals with mental retardation exhibit low exercise performance and work capacity levels (Reid et a]., 1985; Schurrer et a!., 1985); however, in spite of initial low physical work capacity and fitness levels, they Ronald Croce is with the Pediatric Exercise and Motor Behavior Laboratory at the University of New Hampshire, Durham, NH 03824. Michael Horvat is with the Pediatric Exercise and Motor Development Clinic at the University of Georgia, Athens, GA 30602.
Transcript of in Adults With Mental Retardation Fitness and Work ... · PDF fileADAPTED PHYSICAL ACTIVITY...

ADAPTED PHYSICAL ACTIVITY QUARTERLY, 1992, 9, 148-178
Effects of Reinforcement Based Exercise on Fitness and Work Productivity in Adults With Mental Retardation
Ronald Croce Michael Horval University of New Hampshire University of Georgia
The present study evaluated the effects of a reinforcement based aerobic and resistance exercise progratn on three obese men with mental retardation and below average fitness levels. A multiple-baseline-across-subjects design was employed to evaluate treatment effectiveness and retention of treatment effects on five dependent measures: body weight, percent body fat (body composition), oxygen consumption (predicted max VO, in ml/kg/min), composite isometric strength (in kg of force), and work productivity (pieces of work completed). Subjects improved during treatment from their baseline scores on cardiovascular fitness, strength, and work productivity mcasure- ments ( 1 ~ . 0 5 ) ; however, retention of gains made during treatment were inconsistent and the data that indicated subjects' scores were regressing back toward baseline tneasurements. There were no significant differences for body wcight and percent body fat lneasiiretnents for treatment and rctcntion phases (11>.05). Results indicated that adults with mental retardation respond to a progressive exercise program in much the same tnanncr as thcir nonretarded peers and that such an exercise progratn can facilitatc job performance.
Due to recent trends in the general population to exercise for health and psychological benefits, researchers are focusing on systelnatically evaluating the fitness of individuals with mental retardation (Coleman, Ayoub, & Friedrich, 1976; Reid, Montgomery, & Seidl, 1985) as well as the effects exercise programs have on various behavioral (Schurrer, Weltman, & Bramtnell, 1985; To~nporow- ski & Ellis, 1984, 1985), psychological (Brown, 1977; Tomporowski & Ellis, 1984, 1985), and physiological (Bennett, Eisenman, French, Henderson, & Shultz, 1989; Croce, 1990; Combs & Jansma, 1990) parameters. Researchers have consistently reported that individuals with mental retardation exhibit low exercise performance and work capacity levels (Reid et a]., 1985; Schurrer et a!., 1985); however, in spite of initial low physical work capacity and fitness levels, they
Ronald Croce is with the Pediatric Exercise and Motor Behavior Laboratory at the University of New Hampshire, Durham, NH 03824. Michael Horvat is with the Pediatric Exercise and Motor Development Clinic at the University of Georgia, Athens, GA 30602.

Reinforcement Based Exercise 149
respond to exercise regimens physiologically in much the same way as their nonretarded peers (Croce, 1990; Halle, Silverman, & Regan, 1983; Tomporow- ski & Ellis, 1984, 1985; Tomporowski & Jameson, 1985). More important, researchers have reported that individuals with mental retardation can leam to perform specific exercises and generalize learned exercises to participate in group conditioning programs (Coleman & Whitman, 1984; Stainback, Stainback, Wehman, & Spangiers, 1983).
In conjunction with low physical work capacity, researchers have also reported a high prevalence of obesity in this population (Fox & Rotatori, 1982; Kelly, Rimmer, & Ness, 1986; Polednak & Auliffe, 1976). For example, Kelly et al. examined the prevalence of obesity in 553 adults who were institutionalized; they reported that 45.2% of the males and 50.5% of the females were obese. Given the adverse effects of obesity on health and longevity (Larsson, Bjomt- orp, & Tibblin, 1982), this problem requires immediate attention by health-care and physical education professionals.
There is a trend to ascertain the economic impact of fitness and sport programs on employees' work performance and job satisfaction (Shephard, 1989). Likely benefits to a company include gains in the quality and quantity of work produced (Danielson & Danielson, 1982; Shephard, 1985, 1986a, 1986b), decreased worker absenteeism (Baun, Bernacki, & Tsai, 1986) and worker turnover, which in the long run increases program effectiveness (Leatt, Hattin, West, & Shephard, 1988; Shephard, 1986a, 1986b), and reduced incidence of industrial injuries (Shephard, 1986a, 1986b). While current evidence is limited, the link between fitness and physical work capacity in the general population suggests that worksite exercise programs are both cost effective and cost beneficial (Shephard, 1989, 1990).
Although the effect of exercise on the physical work capacity of individuals with mental retardation has been demonstrated, few studies have empirically investigated the relationship between fitness parameters and job performance (Nordgren, 1970; Nordgren & Backstrom, 1971) or improvements in work performance resulting from exercise programs (Beasley, 1982; Maurer, Hussey, & Schofield, 1976) in this population. No experimental studies were discovered that assessed retention of fitness levels and worker productivity (work output) after treatment termination.
Since researchers have demonstrated that individuals with mental retarda- tion perform substantially lower on physical skills when compared to their nonretarded peers (Winnick, 1979), and since they are most typically required to use physical rather than cognitive skills in the work place, enhanced physical capacities can make a significant contribution to the overall vocational and social development of these individuals (Williams, 1977). According to Cohen (1963), it is imperative that individuals with mental retardation be successful in their first employment opportunity. Failure to adequately match job requirements with occupational capabilities often contributes to the worker's failure on the job and has a negative impact on future occupational independence; moreover, fitness programs are required for individuals with mental retardation to qualify for and maintain employment on most occupational tasks (Coleman et a]., 1976).
Verification of the link between physical conditioning programs and improvements in job related skills for individuals with mental retardation, in particular those individuals having below average fitness levels, can significantly

4 50 Groce and Norvat
enhance the rationale for adapted physical education and physical training programs in the public schools. The Back o f empirical research demonstrating such a relationship prompted the present investigation. Accordingly, the purpose o f the present study was to determine the effects o f a reinforcement based exercise program on body weight, percent body fat (body composition), oxygen consumption (predicted max V 0 2 in m8/kg/min), conapposite isometric strength (in kg o f force), and work pmductivity (pieces o f work completed) in men with mental retardation and below average fitness levels. Retention o f fitness parameters and job related behaviors once treatment was withdrawn was also detemined.
It was hypothesized that a rigorous exercise program emphasizing aerobic activities arad general muscle strength training would have a significant ianpact on cardiovascu!ar fitness, muscle strength, and work productivity and that these behaviors would be maintained above baseline levels 5 weeks posttreatilnent. la was further hypothesized chat since this investigation did not incorporate caloric restriction as part o f the i~atervelition, the fitnless program employed w o ~ ~ l d only have a modest iinpact on body weight ant8 percent bcpcly kit (Buono, MclCenzie, 8r McKenzie, 1988; Hagan, 8988).
Subjects
Three obese men with mental retardation (nnean CA = 24.66 f 3.50, r:unge 2 1--28; mean HQ [WSSC-R] = 52.33 t- 4.40, range 88-56] from a sheltered wol.ltshop in the northeastern region o f the Ui~iied states participated in thc stucly. Since the primary purpose o f this investigation was to determine wlaether aim excrcisc program could improve the physical fitness and work productivity in meal with mental retartlation who 17;1d below average fitness levels, a primary crilcrio~r iiw participation i n the current investigation was that subjects hacP bclow :ivei-;igc fitness levels (see below). In aclclition, to cnnatrol for secontlary v:arialacc (i.c., conli)untlinmg vari:tbles) nmtl ro ensure tipat the treatment alone ancl not [lie s~~t),jeccs' obesity, fitness, ancl/oi- lQ levels lecl 20 the concornitand changes in the tlcpenclcnl measures, subjects were matched as closely as possible on these measures.
Subjects were able to lipllow verbal clirectioaas, were free I'ronl any chronic disease iund motor tlisability, were not cjn any medication that coi~lcl i~tlversePy influence their- physiological responses to exercise and, accortling ro their inslr~ic- tors at tile workshop, were highly motivated individi~als (see 'I'ahle 1 I'or sul?jcct characteristics). Sub.jecils were chosen la-om an origi~lal pool 01' P4 wor8\crs :it thc slaelies-ed worltshop, anati were given medical clearance by their Family physicii~ns prior- to participation.
Sublects were cl:issifiecl as having low (Se~bjcct I ) to Fair (Sill?jccts :! ;inti 3 ) fitness levels. Fitness levels were based om nomas I'or cvalualing Asirantl bicycle test perfo'onnance (Preventive Medicine Center, Palo Alto, CA, cilctl in Adams, I990). Because there ccuueaably is no stal~tlartl by which obesity lu~:ty he clearly defined or ill ensured (BusliirIc, 1987)- the clns:;ificatios~ sy:;lc.sra of' O:o:.,:; and Strehie ( i 91N) was used lo deteraa~ine obesity levels in sarbjecis. klsaclcr tliis system, three 11?;4jor categories of obesity may be considei-oci: slighi ( I?-O(ZJ ol' ideal body weight), moderate ( 1 3 0 8 o f ideal body weight), ancl e:ttrerne ( 150'%1 o f ideal body weight).

Reinforcement Based Exercise
Table 1
Physical Characteristics of Subjects
Characteristics Subject
1 2 3 Mean SD
Age Height (cm) Weight (kg) Percent ideal weight Percent body fatC Max VO? (ml/kglmin)d Compos~te strength kg 'f )e Fitness classification
48.00 21 .oo
179.30 94.96
128.00 31.56 22.26 68.88 Low
56.00 53.00 52.33 4.04 25.00 28.00 24.66 3.5
172.20 170.80 174.10 4.55 86.67 91.44 91.02 4.16
121 .OO 126.00 125.00 3.60 23.00 26.29 26.95 4.31 28.56 25.91 25.57 3.16 91.46 78.34 79.56 11.33 Fair Fair n.a. n.a.
Note. Body weight, percent body fat, max \lo2, and composite isometric strength values represent the mean of baseline measurements. a~ased on WISC-R intelligence scale; bbased on standard tables from the Metropolitan Life Insurance Co. (1983). 'based on sum of three skinfolds (chest, abdomen, and thigh) and age (Pollock et al., 1980); 'values predicted from heart rate at a submaximal workload based on the Astrand bicycle test (1960); escores represent the sum of elbow extension, elbow flexion, shoulder abduction, shoulder transverse adduction, and thoracic flexion isometric strength in kilograms; fbased on norms from the Preventive Medicine Center, Palo Alto, CA (cited in Adams, 1990).
Ideal weight refers to the most recent standard tables published by the Metropolitan Life Insurance Company (1983) (Table 1). It is important to note that this system does not look at actual body composition measurements (i.e., percent body fat) as a means of determining obesity but rather at percent over ideal body weight. Although this method is an arbitrary one, its ease of interpretation and comparability to other studies incorporating these standards has led to its popularity in research (Foss & Strehle, 1984). Based on this classification system, subjects were classified as being slightly obese.
Experimental Design
Since there is sufficient evidence of inconsistent performance by individuals with mental retardation, one may question typically used pretest to posttest research designs. Moreover, due to the large individual differences in persons with mental retardation and the individualized nature of instructional programs used with this population, group research designs often are inappropriate in physical activity research (Figoni, 1990; Watkinson & Wasson, 1984). To alleviate this problem, a multiple-baseline-across-subjects design was used (Ottenbacher, 1986), with body weight, percent body fat (body composition), oxygen consumption (predicted max V02 in ml/kg/min), composite isometric strength (in kg of force), and work productivity (pieces of work completed) as the dependent measures.

152 Croce and Hon/at
In multiple-baseline strategies, data collected during baseline are used to establish a pretreatment rate of pkrfomance that is used as a comparison against data in treatment (intervention) and retention phases. Threats to internal and external validity, which are controlled for by random assignment of subjects to groups in traditional group-comparison designs, are controlled for in single- subject designs by each subject serving as his or her own control and by the systeaaaadic application and withdrawal of treatment. If the application, withdrawal, or manipulation of treatment is linked with systematic changes in the dependent variables, one can then infer that treatment produced the observed changes (Hersen & Barlow, 1976).
During baseline data collection, subjects participated in their normal daily activities. Treatment consisted of a I -hour exercise program 3 days per weel< and a 40-minute exercise program 1 day per week (the decreased length of one of the exercise sessions was because the resistance exercise component was per- formed only 3 days per week). Exercise sessions were scheduled for 10 minutes of warm-up, 20 minutes of isotonic strength training (which was omitted during one of the exercise sessions), 20 vni~a~ntes of aerobic exercise (s-un~ming/wollcing or pedaling on a cycle ergometer), and a BO-minute cool down. All conaapolraents of the exercise program adhered to guidelines establishecl by the Avnerican College of Sponas Medicine (ACSM) (1991) and Pollock and Wilmore (1990).
Exercise and testing sessions were scheduled each afternoon 5 days per week and were closely nnonitorecB by a research assistant antl/or one of the experimenters. The research assistant had an undergraduate degree in1 physical education, had receattiy connpletecl a course in medical :enc% exercise issues in disability, and was skilled in ad~ninisterilag and evaluating exercise programs according to guideliraes established by tlae ACSM (199%). Prior to initiation of the study, tlae research assistant was additionally trained in the reinforcement system and testing and exercise proiocols ~rsed. Exercises wcs-o pc:rk)rtaaed in a secluded quiet room nt the worksite. Tlae rnnn~ing/walkinag conapocietmt of the exercise program was performed ah a nearby park and recreation cou~aplex.
Tlne was-111-up po1-tiu11 01' ~ O P C exel-cise program consistecl oi'static sis-etching of the shoulder girdle, quadriceps, hamstring, Iower back, and c~zli' muscles to prevent potential nne~scle icjuries that naaiglat havc arisen from the exercise progrann. Stretching exercises adhered to the guidelines of Shelliocli xacE Prentice ( 1985).
Wou-EiBoads in the aerobic phase of the exercise program were based on heart rate a r ~ 9 whether or not tlae subject showed signs of undue fatigue (e.g labored breathing and an inarability to nnaiaaiain exercise intensity). As each participant adapted to the exercise regimen, exercise intensity was gradually increasecl. Pzogressiom rates followed the first two stages of exercise progressioi~i as o~atlined by tlae ACSM ( B 99 1 ).
During Stage I , thc initial co~aditioniaag stage, Bovv levels of aerobic aceiviay were incorporated so that participanats woetld expes-ien~ce a nlcniniuaa~.tun of rnuscll soreness ant! avoid debilitziting ir~jtrsies. The %engiBa of Stage U was dependen; upon each participant':; rate oi'adapt;aiioi~ to ihe ynjgs.:rnaa. Dele io the low-to-f:li initial aerobic fitness levels oi' subjecis ;end to the need io itcclinm~iete subject:: r the aerobic comyson~esiat of the c:;erci:;e pr-cpgras~i, c::crcisc inlcnsity began ni level between 50 and 60% of estimated ma:tin-m~nm laeart rate reserve (HiiPsa~:: reserve) in a manner consisterat with ACSM reconnmendabioras (1991). 1 8 ~ ~ . .

Reinforcement Based Exercise 153
exercise on the cycle ergometer, this translated into exercising at a power output of approximately 50 watts. Subjects pedaled on the cycle ergometer at a frequency of 50 rpm.
During Stage 2, the improvement stage, participants progressed at a more rapid rate (ACSM, 1991). The frequency and magnitude of increases were dictated by how the participant adapted to the conditioning program. The goal was to have subjects exercise at an intensity of between 65 to 85% of HRmax reserve. Training heart rate (THR) was determined by the following formula: THR = (MHR - RHR) x Intensity % + RHR (MHR = maximum heart rate, which was estimated by the formula 220 - age; RHR = resting heart rate). Resting heart rates were taken with subjects sitting in a quiet room early in the morning. Heart rates were taken three mornings in succession and the values were averaged.
The primary rationale for using this method over the more commonly used method of HRmax is that research has shown that the percentage of HRmax reserve correlates more closely with actual metabolic equivalents (METs) deter- mined on a graded exercise test (see Davis & Convertino, 1975; Karvonen, Kentala, & Musta, 1957; Pollock & Wilmore, 1990, pp. 380-387). If greater workloads resulted in a reduction in exercise performance, difficulty in meeting new exercise demands, and/or labored breathing, they were reduced. Two aerobic exercise modes were used to decrease participant boredom and increase participant motivation to exercise (Croce, 1990).
Participants ranlwalked outdoors twice a week (Monday and Wednesday) and cycled indoors on a cycle ergometer (Monark ergometer model 78062, Monark Crescent, Varberg, Sweden) twice a week (Tuesday and Thursday). During all exercise sessions, the research assistant or experimenter accompanied subjects and provided verbal encouragement. Each subject's elapsed time, dis- tance run (or pedaled), and approximate exercise intensity during the exercise session, which was determined by heart rate, were logged on a cumulative chart and served as a goal for the next exercise session. On those days when subjects pedaled on the cycle ergometer, exercise intensities were appropriately adjusted by a force knob on the cycle ergometer.
Subjects' pulse rates were monitored at either the carotid artery during cycle ergometry exercise or the carotid or radial artery during running/walking by either the research assistant or one of the experimenters (all had experience taking pulse rates). Pulse checks were taken prior to beginning exercise, at 6-min intervals into the exercise session, and at 1-min postexercise. These pulse checks were important not only from a safety standpoint but also for determining whether subjects were exercising at the appropriate intensity level zone (65 to 85% of HRmax reserve). If the heart rate was below the target zone of 65 to 85% of HRmax reserve, the subject was encouraged to exercise at a higher intensity level.
The resistance exercise component of the intervention program was per- formed three times a week (Monday, Tuesday, and Thursday). The resistance phase of the exercise program consisted of a series of exercises using surgical tubing (THERABAND, the Hygenic Corp., Akron, OH). Exercises were geared to increase elbow extension, elbow flexion, shoulder transverse adduction, and shoulder abduction strength. Only upper limb exercises were included, due to time factors and the fact that subjects would be exercising their lower limbs during the aerobic phase of the exercise program. Subjects performed three sets of from 8 to 12 repetitions to volitional failure (i.e., 8-12 RM).

154 Croce and Howat
General principles o f overload, progression, specificity, and volume were adhered to based on the recommendations of Fleck and HCraemer (1987) for developing resistance exercise programs for untrained individuals. Resistance was increased by using a THEMBAND with a greater resistance. THERABAND comes in six levels o f resistance. Subjects initiated the resistance exercise program at Level 1 for all movements and gradually progressed up to Level 3 on all but the shoulder abduction exercise, where subjects reached Level 2. Subjects additionally performed two sets o f bent-knee abdominal curls to volitional termination.
Subjects attended 89% o f the exercise sessions throughout treatment. Subject I attended 50 out o f a possible 56 scheduled sessions, Subject 2 attended 38 out o f a possible 44 scheduled sessions, and Subject 3 attended 30 out o f a possible 32 scheduled sessions. Testing was conducted each Friday afternoon.
P~*etr.aining. Several researchers have encountered problenns with persons with mental retardation being unable to maintain and fo'sllow required testing cadences on a variety of maximal and submaximal cardiovascular tests (Bar-Or et al., 197 8 ; Nordgren, 197 1 ). Seidl, Reid, and Montgoanery ( 1987) ~aotecl that extreme fluctuations in scores may better represent changes in motivation andlor learning o f the resting protocol rather than physio8ogical functioning. Further, Fernhall and Tymeson (1987) and Ravay, Reid, and Cressler-Chaviz (1990) stmngly suggested faaniliarizing subjects with the test setting, testing protocols, and adn-a~inistrator to avoid the pl-obPeln of cond'ounading factors to the data collection^.
For the previously mentioned reasoaas, training sessions were conducted by one o f the experimenters and the research assistant prior to initialing baseline to determine whether subjects were capable o f completing tlae exercise program, to determine whether subjects could complete the required cardiovascular testing protocol with the appropriate cadence and complete tlae isonnetsic rrnuscular str-elagtia tests, and to minimize learning effects on test data.
When all subjects were able to complete each exercise ancl test protocol correctly on cue as defined by the experimenters, baseline began. Pretraining consisted o f daily scssiolas lasting approximately 30 minubcs. Pnct~-aiming lasted nine sessions for Subject I , six sessions for Subject 2, and seven sessions for Sub-ject 3. A similar protocol was used by Croce (1990) and expedited data collection significaeatly.
B~se/ii?p ~1761' Ti .~a t tn~ i~ t . Baseline data were g:ailael.ed lor the three partici- pants for the five dependent variables. Since the treatment program for this investigation i~avolvecl a syste~natically applied exercise progrann, physiological data (i.e., predicted linax V 0 2 and composite isometric strelagtla) were used as determinants for initiating treatment (exercise progrann) to each subject. After baseline measures in these variables stabilized to the point at which only minor variations iia the data could be seen (see Hersen & Barlow, l976, Or a detailed description on baseline stabilization iaa single-subject tlesigms), treatment \was initiated for Ilae first randonaaly selected participant, Subject I ; treatment for Subject 1 lasted 14 weeks. As changes in physica! pe~-lorrn;u~ce levels were observed for the first participant, treatment was begun for. the seconacl r:andomly selected participant, Subject 2; treatment Basted P 1 weeks. Treatment P'or Subject 3 was initiated as changes in physical performance were noted in Subject 2; intervention for Sub.ject 3 lasted 8 weeks. Retention (maintenance) was measured up to 5 weeks posttreatment.

Response Measures and Data Collection. Numerous attempts have been made to predict maximal oxygen uptake from heart rate and other variables during standardized submaximal exercise loads (Nagle, 1973). An estimate of maximal cardiovascular function can be achieved without undue stress on subjects, without the need for high motivational levels required in tests that press subjects to maximal levels (a major problem with individuals who are mentally retarded), and without the need for complex, time-consuming direct oxygen uptake measurements (impractical to do at centers or sheltered workshops for individuals with mental retardation). Although these tests usually provide a close approximation of maximal oxygen uptake, they are subject to a 10% prediction error (Nagle, 1973).
Since a major component of the fitness training program incorporated cycle ergometry, the Astrand Bicycle Ergometer Test (ABET) (Astrand, 1960) was used as a predictor of maximal aerobic capacity (cardiovascular fitness). This test is a predictor of maximal oxygen uptake specific to pedaling a cycle ergometer that is adjustable for power output. Simplicity and familiarity of cycling, espe- cially since subjects partially trained on a cycle ergometer, made this test a desirable method for measuring aerobic fitness. Moreover, since in single-subject designs repeated tests are given over an extended period of time, ease of administration made this test propitious.
The protocol followed procedures outlined by Astrand (1960, 1988) and Adams (1990) and utilized modifications suggested by Lavay, Reid, and Cressler- Chaviz (1990). These modifications included (a) a tape recording of the prescribed workload to monitor pedal frequency, (b) a visual cue in the form of a piece of tape placed over the speedometer at the prescribed workload, (c) physical prompting by an assistant to make sure subjects maintained proper pedal frequen- cies, and (d) verbal encouragement.
In brief, the ABET is a sophisticated field~lab based test that predicts maximal oxygen consumption based on the steady-state heart rate (pulse rate) of an individual exercising at a submaximal power level for 6 minutes. This test is dependent on the direct relationships between power level, oxygen consumption, and heart rate. Normal duration of the ABET is approximately 6 minutes. Because of pretest training on the testing protocol (subjects went through several trials of the protocol) and the use of verbal and physical prompting by the research assistant and/or experimenter, subjects adhered to necessary metronome cadences with only slight variations. As noted previously, pulse rates were ascertained from the subject's carotid artery (for more details on the test protocol, see Adams, 1990).
Cycle ergometry has been shown to be a reliable method for measuring the cardiovascular fitness of individuals with mental retardation (Bundschuh & Cureton, 1982; Cressler, Lavay, & Giese, 1988; DePauw, Hiles, Mowatt, & Goc- Karp, 1985). In a more recent investigation, Montgomery, Reid, and Koziris (in press) compared the reliability and validity of three submaximal cardiovascular tests for nondisabled adults and adults with mental retardation. For the individuals with mental retardation, Montgomery et al. found an intraclass reliability coeffi- cient across five trials of a cycle ergometry test at r = .93.
Validity was examined by comparing the submaximal cycle ergometry test against the V02 max value obtained from a maximal treadmill test. Pearson product-moment correlations were low for both the nondisabled (r = .6Q) and

156 Croce and Howat
mentally handicapped (r = .39) groups. However, this could be attributed partially to differences in muscle groups used in testing (leg and arm for treadmill exercise and leg for cycle ergometry) and, as Montgomery et al. noted, the fact that peak V02 values obtained on the maximal treadmi!l test did not represent a maximal effort, as standard criteria for reaching max V02 were infrequently obtained by the subjects with mental retardation. Since the predicted max V02 on the cycle ergometer did not require a maximal effort, one might argue that this mode of testing was influenced least by motivational factors and is in fact more representa- tive of the cardiovascular fitness found in this population (Montgomery et al., in press).
It is important to note that although submaximal tests based on heart rate have routinely been used in a myriad of field based research with individuals who are mentally retarded (see Lavay, Reid, & Cressler-Chaviz, 1990; Seidl et al., 1987), their overall accuracy has been questioned (Fernhall & Tymeson, 1987; Pitetti & Campbell, 1991; Pitetti & Tan, 1990). According to Pitetti and Campbell, predicting cardiovascular fitness from submaximal heart rates from age related formulas (e.g., 220 - age) may overpredict expected maximal heart rates and, consequently, may have an impact on the accuracy of submaximal cardiovascular fitness tests.
Although the reasons for these lower-than-expected heart rates is unclear and speculation abounds, a lack of motivation to perform an all-out exercise bout is often given as a partial explanation for these lower values (Bennett ef a]., 1989; Montgomery et al., in press). Montgomery et al. postulated that peak V02 values often do not represent a true maximum test since standard criteria for reaching VO, max are rarely obtained; consequently, these values may not be truly representative of the cardiovascular fitness of these individuals. At present this question remains unresolved.
Strength measurements were procured with a Nicholas Manual Muscle Tester (NMMT) (Lafayette Instruments, Lafayette, IN). A break test procedure was used to evaluate elbow extension (triceps), elbow flexion (biceps), shoulder abduction (deltoid), shoulder transverse adduction, and thoracic flexion (abdomi- nal) strength. Test positions were based on those outlined by Kendall and McCreary (1983), with the mean of three trials on each position recorded for the data analysis. Data from each test position were combined to give a composite isometric strength profile (i.e., sum of elbow extension, elbow flexion, shoulder abduction, shoulder transverse adduction, and thoracic flexion in kg of work). According to Blimkie (1989), measures of composite strength or the total strength scores from many muscle groups provide an assessment of overall general strength. Obtaining a composite score also represented a feasible method for facilitating the graphing and analysis of the data.
Reliability of hand-held dynamometry has recently been established in able-bodied individuals at r = .85-.99 (Agre et al., 1987) and r = .98 (Sullivan, Chesley, Hebert, McFaull, & Scullion, 1988). Investigators have also established that hand-held dynamometry exhibits face, concurrent, and predictive validity (see Bohannon, 1990). For example, Sullivan et al, reported that an analysis of variance did not reveal any significant differences between mean peak torques obtained between hand-held dynamometry and cybex dynamometry. Suomi, Surburg, Lecius, and Poppy (1991) recently reported statistically significant reliability scores on test-retest NMMT data (r = .97-.98) as well as a statistically

Reinforcement Based Exercise 157
significant relationship between NMMT data and peak force isokinetic measure- ments (r = .67-30) in adults with mental retardation.
Prior to the present investigation, intertester reliability for NMMT measure- ments was demonstrated by comparing scores obtained by the research assistant to those simultaneously taken by one of the experimenters on a random sample of 20 individuals with mental retardation from local public schools. Reliability on composite isometric strength scores was ascertained at r = 32.
Percent body fat was determined from the percentage of body fat estimation for men for age and the sum of chest, abdominal, and thigh skinfolds (Pollock, Schmidt, & Jackson, 1980) calculated by the standard formula of Siri (1956). Skinfold measurements were taken with a Lange skinfold caliper (Cambridge Scientific Industries, Cambridge, MD). Each subject's body density was based on the mean score of three measurements. Similar to muscle testing, intertester reliability for measuring percent body fat was demonstrated by comparing scores obtained by the research assistant to those simultaneously taken by the experimenter on a random sample of 20 individuals with mental retardation from 1ocal public schools. Intertester reliability was ascertained at r = 94. Height and weight measurements were taken with subjects in their stocking feet using a Detecto scale (Lafayette Instruments, Lafayette, IN) that was calibrated prior to initiating the investigation.
The on-site work task involved screwing jar lids on plastic jars and placing the jars into cardboard boxes, 12 jars per box. The plastic jars ranged in size from 1 to 8 oz. Subjects had to fold the boxes into which the plastic jars were placed in an upright position and stack the filled boxes. A task analysis involved the following: fold box, lift jar and jar lid, close lid on jar, place assembled jar in box (12 per box), close box and, finally, stack boxes. Data represented the number of jars correctly assembled and placed into boxes during a 6-hour workday. Data were collected under norhal working conditions with no additional reinforcement or verbal cueing given to subjects.
Retention. After each subject completed the task under the supervision of the research assistant and the experimenter, treatment was withdrawn to determine retention over a 5-week period. Data were collected in the maintenance situation as in treatment. All data (i.e., body weight, percent body fat, predicted max VO~, composite strength, and pieces of work completed) were collected weekly on Friday afternoons.
Behavior Reinforcement System. To facilitate the subjects' participation in the exercise program, a token economy system similar to that used by Croce (1990) and Lavay and colleagues (Lavay, 1984; Lavay & McKenzie, 1991; Lavay, Zody, Solko, & Era, 1990) was used. This system was crucial for cultivating the subjects' motivation to exercise and is consistent with Knapp's (1988) conclusion that strategies to enhance initial involvement in exercise programs are essential for providing the catalyst necessary for exercise interven- tion strategies to succeed. As the behavior management system used in the present study has been discussed in previous communications (Croce, 1990; Lavay, 1984), it will only be briefly elaborated upon at this time.
Subjects received verbal reinforcement contingent on time on task, or time actually spent exercising, both during and at the end of each exercise session. During exercise the verbal reinforcement (e.g., "good job") was administered each time the subjects were on task and focused on the importance of time on

158 Croce and Horvat
task. Social reinforcement administered after each exercise session focused on overall session performance. Positive comments included "good job," "you did better than last time," and "you are doing a great job."
These comments were made when subjects improved their exercise scores (time exercising) from the previous exercise session (e.g., subjects pedaled on the cycle ergometer for a longer time than in the prior session, ranlwalked for a greater distance than in the prior session, or performed more repetitions on the resistance exercises than in the prior session). Negative comments (reproofing) were, "you will have to try harder next time if you want to do better," and "I know you can do better if you try a little harder next time." These comments were used when subjects showed a decrement in their exercise performance scores from the previous exercise session, such as pedaling on the cycle for a shorter time than in the prior exercise session.
Consequently, social reinforcement was used both as a type of concurrent (during exercise) and terminal (after exercise) augmented feedback. According to Sage (1984), even if the task itself supplies feedback regarding an individual's performance, supplemental information can function as a powerful reinforcer, sustaining effort and increasing performance.
In addition to verbal reinforcement, tokens were awarded to subjects who met criterion for time on task (time exercising). The system for earning tokens toward a reinforcer was similar to that used by Croce (1990) and Lavay (1984). For exercise sessions on the cycle ergometer, tokens earned were based on each subject's performance during the exercise session and whether or not the subject achieved or surpassed the level of exercise established during the prior cycle ergometer exercise session. For example, if time on task on the cycle ergometer was 10 minutes for the third exercise session, the criterion time on task for the next exercise session on the cycle ergometer would be 10 minutes.
At the end of each exercise session, subjects received one token for reaching criterion and one additional token for each 30 seconds they exercised beyond criterion. In other words, subjects received tokens both for reaching and exceeding criterion and, furthermore, the criterion level changed for each exercise session. Thus, criterion for receiving tokens increased as length of time exercising increased. Criterion levels were readjusted after resistance levels on the cycle ergometer were increased.
Subjects were encouraged to cycle for as long as they could while main- taining their heart rate at the established training intensities. The research assistant assisted subjects in maintaining the proper cycling cadence, provided encouragement throughout the exercise bout, and monitored pulse rates (Croce, 1990) at the carotid artery.
A similar protocol was used when subjects ranlwalked during the aerobic component of the exercise program, with the sole difference being that the criterion for receiving tokens was based on laps completed rather than time exercising (Lavay & McKenzie, 1991). Subjects were encouraged to run/walk for as long as they could while maintaining their heart rate at the established training intensities. The research assistant helped them with proper pacing techniques, provided encouragement throughout the exercise bout, and monitored pulse rates (Lavay, Giese, Bussen, & Dart, 1987; Lavay & McKenzie, 1991). Pulse rates were monitored at either the carotid or radial artery.
Tokens earned were based on each subject's performance during the

Reinforcement Based Exercise 159
exercise session and whether the subject equaled or surpassed the number of laps completed during the previous run/walk session. At the conclusion of the exercise session, the subject received one token for reaching criterion and one additional token for each quarter lap he exercised beyond criterion. Subjects rantwalked around the perimeter of a local park. One lap was equal to approximately 200 yards.
Tokens earned for the resistance-exercise component of the exercise pro- gram were based on whether the subject equaled or surpassed the number of repetitions completed by the subject for each exercise during the previous exercise session. Subjects received one token for reaching criterion and one additional token for each repetition performed beyond criterion. Criterion level was reestab- lished when the subject increased the resistance level for the exercise.
Prior to exercising (e.g., cycle ergometer), each subject was told, "Would you like to earn some more tokens today? To receive these tokens you must stay on the bicycle machine for as long as you can [the experimenter or research assistant would then point to the tokens, the cycle ergometer, and show the subject gifts he would exchange for the tokens]. The longer you exercise, the more tokens you receive." The subject was then instructed to "get ready" and the exercise period began. Similar instructions were given to subjects when they ranlwalked for that exercise session and prior to performing the resistance exercises.
After each exercise session, tokens earned were recorded along with the total number of tokens accumulated. Subjects were constantly informed of the total number of tokens accumulated. At the end of each week the tokens were exchanged for tangible rewards, which subjects chose from a reinforcement menu. Selection of reinforcers was predetermined by a discussion with the center staff. According to Bishop and French (1982), this system assures selection of high preference reinforcers and increases attending behaviors in subjects with mental retardation. Croce (1990) and Bennett et al. (1989) reported that such a token economy system was extremely effective in motivating individuals with mental retardation to exercise.
Data Analysis Intervention effectiveness was evaluated by its effects on the five dependent variables: body weight, percent body fat (body composition), oxygen consumption (predicted max VOz in ml/kg/min), composite isometric strength (in kg of force), and work productivity (pieces of work completed). Data trends within and across phases were determined by visual inspection and statistical analysis of the celeration line (Ottenbacher, 1986). Statistical significance was determined by procedures outlined by Ottenbacher and are described briefly below.
To ascertain whether there was any change in each subject's physiological (e.g., strength scores) and behavioral (e.g., work productivity) responses to treatment, it was necessary to measure each subject's performance over each phase. To accomplish this, a trend or "celeration line9'was computed for the baseline phase and extended into treatment and retention phases. The reason for extending the celeration line into these phases was to predict the trend of the subject's behaviors (measurements) (Ottenbacher, 1986).
A finding that the proportion of data points above or below the celeration line during treatment or retention from that of baseline suggested a change in

160 Croce and Horvat
the subject's response pattern. According to Ottenbacher (1986), two simple methods for determining whether changes from baseline are statistically signifi- cant are to compute a simple binomial test or use the probability table of Bloom (1975). According to Ottenbacher, "The probability table is more conservative than the binomial test and represents the best method to determine a quantitative index related to a client change based on statistical probability when the celeration line procedure is used" (p. 185). Essentially, this technique involves quantification of the number of treatment observations above or below the celeration line that are required to demonstrate a statistically significant effect at the .05 level.
Figures 1, 2, 3, 4, and 5 visually display the data for the dependent measures. A mean baseline score and a final score for treatment and retention phases were also calculated for each variable to determine percent changes at the terrnination of each phase (Figure 6 and Tables 2, 3, and 4). Although the percent of change found in each variable is largely dependent on initial scores, it nevertheless has been used by prior investigators (e.g., Beasley, 1982; Bennett et al., 1989; Croce, 1990; Lavay 8r McKenzie, 1991; Schurrer et al., 1985; Skrobak-Maczynski & Vavik, 1980) and pennits one to compare changes observed in one study to those reported in similar investigations.
It must be noted that the length of treatment varied for each subject: treatment lasted 14 weeks for Subject 1 , I I weeks for Subject 2, and 8 weeks for Subject 3. Further, all three subjects were initially classified as having either low or.fairfitness levels. Consequently, the fairly substantial increases in preclicted max V 0 2 must be considered in light of initial aerobic fitness data (ACSM, 1990).
Physiological Data
Data analysis irrclicaled that changes in body weight and pelrent body 1'111 wer-c inconsistent across all subjects and phases. Subject 1 showed a decrease in both body weight and percent body fat from baseline to treatment (-3.00 and -8.42% change, respectively) and from baseline to retention (-1.85 and -6.2 1 %I change, respectively). Body weight decreases were statistically significant for both the baseline-to-treatment and baseline-to-retention phases ( 1 ~ 0 5 ) . For- percent body fat, only the baseline-to-retention phase was statistically significant (p<.05).
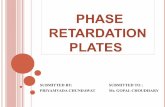
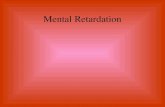
As displayed in Figure 2, Subject 1 did not display a decrease in percent body fat over baseline measurements until the 7th week of treatment; consequently, half of the data points remained above the celeration line, leading to a nonsignificant treatment effect. During the retention phase, however, data points were bclow the celeration line, resulting in a significant baseline-to-retention effect.
Subject 2 showed a decrease in both body weight and percenl body fat from baseline-to-treatment (-3.54 and -10.80% change, respectively) and baseline-to-relegation (-1.81 and -10.00% change, respectively) phases. Body weight decreases were nonsignificant for the baseline-to-treatment phase ( p . 0 5 ) but were statistically significant for the baseline-to-retention phase (p<.05). Percent body fat changes were statistically significant for both phases (p<.05).
As displayed in Figure I , Subject 2 did not display a decrease in body

Reinforcement Based Exercise
96 - 94 - 92 -
90 -
Weeks of Program
Baseline Treatment Retention
A A* 6 -
- Body Weight S-1 1 . 1 . 1 . 1 . 1 . 1 . 1 . 1 . ~ . ~ . 1 . ~ - "
97 -r
95 - 93 - 91 -
Figure 1 - Comparison of subjects' body weight scores during baseline, treatment, and retention phases with celeration trend lines.
0 2 4 6 8 1 0 1 2 14 1 6 1 8 2 0 22 24
89 - - - -- Body Weight S J ~ . I . I . I . I - I - ~ - ~ . I . I . ~ . I . I * 0 2 4 6 8 10 1 2 14 16 18 20 22 24

162 Croce and Horvat
35 - Baseline Treatment Retention
29 - 27 - - PermntFd S-1
I . , . , . , . , . , . , . I . , . I . , . , +
0 2 4 6 8 1 0 1 2 14 16 18 2o 22 24
30
28
26
24
Perrmt Fat S -3
0 2 4 6 8 10 1 2 14 16 18 2 0 2 2 24
Weeks of Program
Figure 2 -Comparison of subjects' percent body fat scores during baseline, treat- ment, and retention phases with celeration trend lines.

Reinforcement Based Exercise
0 2 4 6 8 1 0 12 14 16 1 8 20 22 24
Weeks of Program
32 : 30 - 28 '
26 - 24 - 22 - 20 -
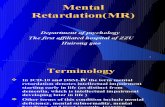
Figure 3 - Comparison of subjects' predicted maximum oxygen consumption (max VOz) scores during baseline, treatment, and retention phases with celeration trend lines.
Baseline Treatment Retention
,I - msxS02s-1 1 . 1 . 1 . 1 . 1 . 1 . 1 . 1 - ' . ' . ' . ' - ' -
0 2 4 6 8 10 1 2 14 1 6 18 20 22 24

164 Croce and Howat
Strength
0 2 4 6 8 1 0 1 2 14 1 6 1 8 2 0 22 24
Weeks s f Program
Figure 4 - Comparison of subiects' composite isoinetric strength (Strength) scores during basesine, treatment, and retention phases with celeration trend lines.

Reinforcement Based Exercise
480 7 Baseline Treatment Retention
470 - 460 - 450 - 440 - 430 : 420 : 410 : 400 :
-t
r . I . I . I . l . I . I . l . l I
0 2 4 6 8 1 0 12 14 16 18 20 22 24
Work Output S- 1
wo* Oulput 5-3
Weeks of Program
Figure 5 - Comparison of subjects' work output scores during baseline, treatment, and retention phases with celeration trend lines.

Croce and Howat
1 Body Wt. Percent Fat Strength max $02 Work Output
Figure A
Subject 1
Subject 2
Subject 3
Figure I4
Subject 1
Subject 2 @ Subject 3
Figure. 6 - Percent changes in ru$jects' laredictetl maxinsum oxygen conwmption (max VOz), isometric composite strength (Strength), work output, percent body fat (Percent Fat), and body weight (Wotly Wt.) from baseline to treatment ( A ) and baseline to retention (8) phases.

Reinforcement Based Exercise
Table 2
Body Weight and Percent Body Fat Measurements During Baseline, Intervention, and Retention Phases
Measure Subject
1 2 3 Mean SD
Body weight Baseline (BL) Treatment (TR) Retention (RT) Percent change (BL-TR) Percent change (BL-RT)
Percent body fata Baseline (BL) Treatment (TR) Retention (RT) Percent change (BL-TR) Percent change (BL-RT)
Note. Baseline scores are based on mean of baseline measurements; treatment scores are based on final measurement during treatment; retention scores are based on final measure- ment during retention phase. a~ased on sum of three skinfolds (chest, abdominal, and thigh) and age (Pollock et al., 1980).
weight over baseline measurements until the 7th week of treatment; hence half of the data points remained above the celeration line, leading to a nonsignificant treatment effect. Similar to the percent fat change in Subject 1, during the retention phase the data points were below the celeration line, resulting in a significant baseline-to-retention effect.
On the other hand, Subject 3 showed an increase in both body weight and percent body fat. Body weight increased from baseline to treatment by 2.58% and from baseline to retention by 3.00%. Percent body fat increased from baseline to treatment by 3.84% and from baseline to retention by 6.50%. Body weight and percent body fat changes were statistica!ly nonsignificant (p.05) across all phases.
Data analysis on predicted max V02 values indicated that subjects showed marked improvements in cardiovascular fitness levels from baseline to treatment (pc.05). However, only Subjects 2 and 3 displayed significant baseline-to- retention effects @<.05), and data indicated that values were regressing back toward baseline measures. More specifically, Subject 1 showed a 27.58% increase in predicted max V02 from baseline to treatment and a 10.00% increase from baseline to retention; Subject 2 showed a 19.74% increase from baseline to treatment and a 7.14% increase from baseline to retention; and Subject 3 showed a 12.69% increase from baseline to treatment and a 6.90% increase from baseline to retention (see Figures 3 and 6 and Table 3).
Reported increases suggested the aerobic portion of the exercise program was of sufficient intensity and duration to elicit increases in cardiovascular fitness

168 Croce and Hon/at
Table 3
Composite Strength and O~rygeri Consumption Measurements During Baseline, Unterventlon, and Retention Phases
Subject Measure 1 2 3 Mean
Composite strengtha Baseline (BL) Treatment (TR) Retention (RT) Percent change (EL-TR) Percent change (BL-RT)
Max vo (m~/kg/min)~ 2
Baseline (BL) Treatment (TR) Retention (RT) Percent change (BL-TR) Percent change (BL-RT)
Note. Baseline scores are based on mean of baseline measurements; treatment scores are based on final measurement during treatment; retention scores are based on final measure- ment during retention phase. ascores represent the sum of elbow extension, elbow flexion, shoulder abduction, shoulder
b transverse adduction, and thoracic flexion isometric strength in kilograms. Values predicted from heart rate at a subma)timal workload based on the Astrand bicycle test (1960).
Work Output During BaseOine, Ooaterwev~tion, and Retention Phases
Subject Measure 1 2 3 Mean SD
Work completed (in pieces) Baseline (BL) 407.00 636.00 571 .OO 538.00 1 18.01 Treatment (TR) 451 .OO 666.00 61 3.00 576.70 11 2.01 Retention (RT) 436.00 661 .OO 599.00 565.33 1 16.21 Percent change (EL-TR) 10.80 4.76 7.35 7.60 3.03 Percent change (BL-RT) 7.12 3.97 4.90 5.33 1.61
Note. Work output initial scores are based on mean of baseline measurements; treatment scores are based on final measurement during treatment; retention scores are based on linal measurement during retention phase.

Reinforcement Based Exercise
Exercise Sessions Attended
Figure 7 -Time on task (min) pedaling on a cycle ergometer relative to maximal power output attained in watts (W) during each 20-min cycle ergometry exercise session. All subjects initiated treatment at a power output of 50 watts. Arrows indicate points where power output changed and represented changes in exercise intensity. Due to staggered baselines and absences, the number of sessions attended by subjects differed (see text for details).

170 Croce and Horvat
l9 1 - Run/Wdk S-I
Exercise Sessions Attended
Figure 8 -Laps completed during each 20-min runlwalk exercise session. All laps were completed at an outdoor park. Each lap was equal to approximately 200 yards. Due to staggered baselines and absences, the number of sessions attended by subjects differed (see text for details).

Reinforcement Based Exercise 171
levels in subjects. Figures 7 and 8 display subjects' performances during the cycle ergometer and run/walk components of the exercise program. Subjects' performances on both modes of aerobic exercising increased systematically throughout the treatment program. However, the time pedaling on the cycle ergometer tended to deteriorate during those exercise sessions when the subject's power output increased and all subjects required a degree of verbal prompting and physical guidance to maintain appropriate exercise intensity levels. Similar results were noted by Tomporowski and Jameson (1985) with lower functioning individuals with mental retardation (mean IQ = 23).
Subjects additionally showed marked improvements in composite isometric strength scores @<.05) across both treatment and retention phases. Results suggested that the resistance exercise portion of the program was at an intensity level sufficient to elicit increases in strength. Subject 1 showed a 34.58% increase in composite isometric strength from baseline to treatment and a 7.57% increase from baseline to retention; Subject 2 showed a 14.25% increase from baseline to treatment and a 6.20% increase from baseline to retention; and Subject 3 showed a 21.65% increase from baseline to treatment and a 10.92% increase from baseline to retention (see Figures 4 and 6 and Table 3). Similar to predicted max V O ~ values, data were regressing back toward baseline levels in all subjects.
Work Productivity Data
Finally, subjects showed modest improvements in work productivity from base- line to treatment (p<.05), while only Subject 3 displayed a significant baseline- to-retention effect (p<.05). More specifically, Subject 1 showed a 10.80% increase in work output from baseline to treatment and a 7.12% increase from baseline to retention; Subject 2 showed a 4.76% increase from baseline to treatment and a 3.97% increase from baseline to retention; and Subject 3 showed a 7.35% increase from baseline to treatment and a 4.90% increase from baseline to retention (see Figures 5 and 6 and Table 4). Consequently, results indicated that the exercise program had an impact on subjects' work productivity levels.
Discussion The present investigation was undertaken to determine whether a reinforcement based exercise program would have significant positive effects on selected physical fitness parameters and work productivity in three men with mental retardation and below average fitness levels. From a physiological standpoint, the major findings were that subjects were able to demonstrate substantial improvements over baseline data in cardiovascular fitness and composite isomet- ric strength scores resulting from training.
Strength increases were statistically significant (pc.05) up to 5 weeks posttreatment, albeit the trend in the data indicated that subjects were regressing back toward baseline levels. Nonetheless, at 5 weeks posttreatment the strength data points were above the celeration line, indicating that subjects' composite isometric strength scores were maintained above baseline levels. On the other hand, cardiovascular fitness levels were only maintained by two of the three subjects and, similar to the strength data, there was a downward trend in the data toward baseline in all subjects.
Results of this study are congruent with those of previous research with

172 Croce and Howat
individuals who were mentally retarded (Bennett et a]., 1989; Combs & Jansma, 1990; Croce, 1990; Pitetti & Tan, 1991; Schurrer et al., 1985) and indicate that a systematically applied, daily, reinforcement based exercise program can have a positive impact on these fitness parameters. Significance of the iarge increases in aerobic capacity must be viewed with reference to the particular individuals who participated in the study, as they had 'extremely low initial max V 0 2 levels. In addition, changes in heart rate responses could have been explained in part by a change in physiological efficiency and/or a learning effect as subjects were exposed to repeated testing (Seidl et al., 1987). This would decrease submaximal heart rates at particular workloads. However, to avoid this potential confounding factor, subjects were thoroughly familiarized with testing protocol, test setting, and administrators of the test prior to the investigation (Fernhall & Tymeson, 1 987).
Nevertheless, improvements observed in this study are encouraging and have been reported elsewhere in the literature (Croce, 1990; Schurrer et al., 1985). For example, using asimilar single-subject paradigm, Croce found a mean increase in predicted max V 0 2 of 29.80% while Schurrer et al. found a slightly higher mean increase (43%). A mean increase of 20% was found in the present study.
The training protocol utilized in this investigation was developed according to pretest data and was individualized for each subject. Moreover, the exercise program was continually adjusted throughout the study to meet each subject's changing exercise capacity. This was accomplished through the use of a token economy system whereby tokens earned were based on each subject's perfor- mance during the exercise session. The intent of this protocol was to motivate subjects to exercise and facilitate maximum participation and progress. A similar protocol was employed by Combs and Jansma (1990) and Croce (1990).
Improvements in subjects' composite isometric strength scores are also noteworthy, as few researchers (see Rimmer & Kelly, 199 1 ; Skrobak-Kaczynski & Vavik, 1980) have directly investigated the effects of a systematically applied rcsistance exercise program over a number of specified muscle groups. In the past, researchers often looked at strength only indirectly through a standing long jump (Oliver, 1958), softball throw (Corder, 1966) or sit-ups and push-ups (Solomon & Pangie, 1967). Skrobak-Kaczynski and Vavik (1980) reported significant improvements in trunk extension (26% increase) and flexion (28% increase) force resulting from a 6-week circuit training program. Improvements in isometric strength encountered in the present study (meanincrease-of 23.49%) are therefore consistent with those reported by Skrobak-Kaczynski and Vavik.
Results of the data analysis additionally indicated that the exercise program did not have a significant impact on body weight and percent fat loss and that changes in body weight and body composition were discordant across sub.jects. These results are not surprising and are consistent with the findings of many researchers in weight control and energy dynamics. Exercise alone appears to be largely ineffective in weight loss and almost certainly must be coupled with caloric restriction (Pacy, Webster, & Garrow, 1986) to make a major impact on weight control. The hypothesis is that combining diet and exercise will accelerate fat loss, preserve fat-free weight (i.e., lean body tissue), and decelerate or prevent decline of postexercise resting metabolic rate (Poehlman, Melby, & Goran, 1991; Walberg, 1989). Although exercise alone is not as beneficial in weight reduction

Reinforcement Based Exercise 173
as is caloric restriction and exercise in combination (Hagan, 1988), increased physical activity should be encouraged to promote long-term lifestyle changes that are conducive to weight loss, a feeling of well-being, and health related fitness (Pacy et al., 1986).
Based on the literature reviewed, Hagan (1988) concluded that well controlled multiple-group studies clearly indicate that exercise combined with caloric restriction was the best method for body weight and fat reduction. Exercise conditioning without caloric restriction has been shown to reduce body weight; however, this occurs only when energy expenditure is substantially elevated and exercise sessions are of long duration.
In the present study this was not the case. The aerobic phase of the exercise program lasted approximately 20 minutes and subjects worked at moderate workloads (i.e., between 65 and 85% of HRmax reserve). As has been shown by Croce (1990), the combination of exercise and diet is the most propitious way to effect significant changes in body weight and body composition in this population.
A major finding of the present study is that subjects improved their work productivity during treatment, albeit this increase was temperate. This finding is consistent with research findings involving nondisabled individuals (see Shep- hard, 1989) as well as with individuals with mental retardation (Beasley, 1982; Coleman et al., 1976). In the most systematic investigation to date, Beasley determined that adults with mental retardation who participated in a jogging program increased their work performance-as measured by the individual's rate of production in assembling heat clips-by nearly 11.5% over subjects in a nonexercise control group. In the present investigation it was found that subjects showed a mean percent increase in work output of 7.60%. Unfortunately, only Subject 3 showed a significant retention of treatment effects 5 weeks posttreatment. To date, no other investigation has determined retention of work productivity after termination of an exercise program.
Conclusions
Data suggest that with a simple token economy system, men with mental retardation respond to a progressive exercise program in much the same way as their nonretarded peers. According to Bennett et al. (1989), a token economy can be considered an instructional strategy that can be used to increase exercise behavior, especially with unfit and poorly motivated subjects.
These findings have direct applicability to currently employed training methods for individuals with mental retardation at institutions, residential centers, or public schools. Individuals with mental retardation living in institutions or attending public schools generally are in poorer physical condition and a greater percentage of these individuals are overweight or obese compared to their nonretarded peers (Fernhall, Tymeson, & Webster, 1988; Kelly et al., 1986). Further, most special education training programs tend to foster a sedentary lifestyle that is characterized by idle time most of the day.
Since individuals with mental retardation are typically required to use physical rather than cognitive skills in the work place, enhanced physical capacities can make a significant contribution to their overall vocational and social development (Williams, 1977). Consequently, structured exercise programs

1 74 Croce and Horvat
ought to become a significant and essential component of the individual's daily education or treatment plan to foster functional independence and a healthy lifestyle. Since retention of training effects were modest and mixed and the data trends indicated that subjects were regressing back toward baseline levels at 5 weeks posttreatment, it would appear that individuals with mental retardation need to be continually involved in some type of exercise program for exercise effects to be maintained posttreatment.
References
Adams, G.A. (1990). Exercise physiology labor-atory manual. Dubuque, IA: W.C. Brown. Agre, J., Magness, J., Hull, S., Wright, K., Baxter, T., Patterson, R., & Stradel, L. (1987).
Strength testing with a portable dynamometer: Reliability for upper and lower extremities. Archives oj'Physica1 Medicine and Rehabilitation, 68, 454-458.
American College of Sports Medicine. (1990). The recommended quantity and quality of exercise for developing and maintaining cardiorespiratory and lnuscular fitness in healthy adults. Medicine and Science in Sports, 22, 265-274.
American College of Sports Medicine. (1991). Guidelines ji)r exercise testing atrd prescr-iption (4th ed.). Philadelphia: Lea & Febiger.
Astrand, 1. (1960). Aerobic work capacity in men and women with special reference to age. Acta Physiologica Scandinavica, 49 (Suppl.) 169, 1-92.
Astrand, P.O. (1988). Work tests with the bicycle ergometer. Varberg, Sweden: Monarch Crescent AB.
Bar-Or, O., Skinner, J.S., Bergsteinova, V., Shearbum, C., Royer, D., Bell, W., Hass, J., & Buskirk, E.R. (1971). Maximal aerobic capacity of 6-15-year-old girls and boys with subnormal intelligence quotients. ACTA Paediatrica Sc~ut~clitro~~ir~a (Suppl.) 217, 108-1 13.
Baun, W.B., Bernacki, E.J., & Tsai, S.P. (1986). A preliminary investigation: Effcc~ of a corporate fitness program on absenteeism and health care cost. .lorrr.tral of'
Occupational Medicine, 28, 18-22. Beasley, C.R. (1982). Effects of a jogging program on cardiovascular fitness imtl work
performance of mentally retarded adults. American Jouniul of Mc,trttrl L)c;fic.ieirc:v, $6, 609-6 13.
Bennett, F., Eisenman, P., French, R., Henderson, J., & Shultz, B. (1989). Thc cflcct of a token econorny on the exercise behavior of individuals with Down synclromc. Adaptecl Pl1vsic.01 Actil~itv Qrrarterl.y, 6 , 230-246.
Bishop, P., & French, R. (1982). Effects of reinforcers on attending behavior o f scvercly handicapped boys in physical education. Journal i?f'Sl~cc.ial E(lrrc.trtiotr, 18, 48-58.
Blimkie, C.J.R. (1989). Age- and sex-associated variation in strength during childhood: Anthropometric, niorphologic, neurologic, biomechanical, endocrinologic, genetic, and physical activity correlates. In C.V. Gosilfi & D.R. Lamb (Eds.), P~r.sl~cc.ti~~c,.s ill c~xerc~ise scienr.e f l f ~ d s/?orts medicine, Volunie 2: Yorrth, cl.\-ei.c.isc,, trtrcl .s[~oi.l (pp. 99-1 62). Indianapolis: Benchmark Press.
Bloom, M. ( 1975). TlrcJ parac1o.1- of lrelpirig: Introclrrc~tioti to // I ( ' plrilo.so/~ly sc.ic,trt~fic. /nxic'tic,e. New York: MacMillan.
Bohannon, R.W. (1990). Muscle strength testing with hand-hcld dyna~no~netcrs. In L.R. Amundsen (Ed.), Mrrsr~lc str~errgtlr testirlg: Irrstt.rrnrc~ltctl orrd ~rotritr.str~ottc~~~/c~(l systems (pp. 69-85). New York: Churchill Livingstone.
Brown, B.J. (1977). The effect of an isometric strength program on the intellectual and

Reinforcement Based Exercise 175
social development of trainable retarded males. American Corrective Therapy Journal, 31, 44-48.
Bundschuh, E.L., & Cureton, K.J. (1982). Effects of bicycle ergometer conditioning on the physical work capacity of mentally retarded adolescents. American Corrective Therapy Journal, 36, 159-163.
Buono, M.J., McKenzie, T.L., & McKenzie, R.E. (1988). Effects of a diet and exercise program on blood lipids, cardiorespiratory function, and body composition in obese women. Clinical Kinesiology, 42, 22-26.
Buskirk, E.R. (1987). Obesity. In J.S. Skinner (Ed.), Exercise testing and exercise prescription for special cases: Theoretical basis and clinical application (pp. 149- 173). Philadelphia: Lea & Febiger.
Cohen, J.S. (1963). Employer attitudes toward hiring mentally retarded individuals. American Journal of Mental Deficiency, 67, 705-713.
Coleman, A.E., Ayoub, M.M., & Friedrich, D.W. (1976). Assessment of the physical work capacity of institutionalized mentally retarded males. American Journal of Mental Deficiency, 80, 629-635.
Coleman, R.S., & Whitman, T.L. (1984). Developing, generalizing, and maintaining physical fitness in mentally retarded adults: Toward a self-directed program. Analysis and Intervention in Developmental Disabilities, 4, 109-127.
Combs, C.C., & Jansma, P. (1990). The effects of reinforcement-based fitness training on adults who are institutionalized and dually diagnosed. Adapted Physical Activity Quarterly, 7, 156-169.
Corder, W.O. (1966). Effects of physical education on intellectual, physical, and social development in educable mentally retarded boys. Exceptional Children, 32, 357- 364.
Cressler, M., Lavay, B., & Giese, M. (1988). The reliability of four measures of cardiovascular fitness with mentally retarded adults. Adapted Physical Activity Quarterly, 5, 285-292.
Croce, R. (1990). Effects of exercise and diet on body composition and cardiovascular fitness in adults with severe mental retardation. Education and Training in Mental Retardation, 25, 176-187.
Danielson, R., & Danielson, K. (1982). Exerciseprogram effects on productivity offorestry firefighters. Toronto: Ontario Ministry of Tourism and Recreation.
Davis, J.A., & Convertino, V.A. (1975). A comparison of heart rate methods for predicting endurance training intensity. Medicine and Science in Sports, 7, 295-298.
DePauw, K.P., Hiles, M., Mowatt, M., & Goc-Karp, G. (1985, October). Cardiovascular endurance of mentally retarded adolescents as assessed by the 12-minute run and cycle ergometer. Paper presented at the 5th International Symposium on Adapted Physical Activity, Toronto.
Fernhall, B., & Tymeson, G.T. (1987). Graded exercise testing of mentally retarded adults: A study of feasibility. Archives of Physical Medicine and Rehabilitation, 68, 363- 365.
Fernhall, B., Tymeson, G.T., & Webster, G.E. (1988). Cardiovascular fitness of mentally retarded individuals. Adapted Physical Activity Quarterly, 5, 15-28.
Figoni, S.F. (1990). Single-subject clinical research: Bridging the gap between therapy and science. Clinical Kinesiology, 44, 63-71.
Fleck, S.J., & Kraemer, W.J. (1987). Designing resistance training programs. Champaign, IL: Human Kinetics.
Foss, M.L., & Strehle, D.A. (1984). Exercise testing and training for the obese. In J.

176 Croce and Horvat
Storlie & H.A. Jordon (Eds.), Nutrition and exercise in obesity management (pp. 93-121). New York: Medical and Scientific Books.
Fox, R., & Rotatori, A.F. (1982). Prevalence of obesity among mentally retarded adults. American Journal of Mental Deficiency, 87, 228-230.
Hagan, R.D. (1988). Benefits of aerobic conditioning and diet for overweight adults. Sports Medicine, 5, 144-155.
Halle, J.W., Silverman, N.A., & Regan, L. (1983). The effects of a data-based exercise program on physical fitness of retarded children. Education and Training of the Mentally Retarded, 18, 221-225.
Hersen, M., & Barlow, D.H. (1976). Single case experimental designs. New York: Pergamon Press.
Karvonen, M., Kentala, K., & Musta, 0. (1957). The effects of training heart rate: A longitudinal study. Annales Medicinae Experimentalis et Biologiae Fenniae, 35, 307-315.
Kelly, L.E., Rimmer, J.H., & Ness, R.A. (1986). Obesity levels in 553 institutionalized mentally retarded adults. Adapted Physical Activity Quarterly, 3, 167-176.
Kendatl, F.P., & McCreary, E. (1983). Muscles testing andfunction (3rd ed.). Baltimore: Williams & Wilkins.
Knapp, D.N. (1988). Behavioral management techniques and exercise promotion. In R. Dishman (Ed.), Exercise adherence: Its impact on public health (pp. 203-235). Champaign, IL: Human Kinetics.
Larsson, B., Bjorntorp, P., & Tibblin, G. (1981). The health consequences of moderate obesity. International Journal of Obesity, 5, 97-1 16.
Lavay, B. (1984). The effects of two types of reinforcement programs on the physical task performance of trainable mentally handicapped students (Doctoral dissertation, University of New Mexico, 1983). Dissertation Abstracts International, 45, 1684A.
Lavay, B., Giese, M., Bussen, M., & Dart, S. (1987). Comparison of three measures of predictor V02 maximum protocols with mentally retarded adults: A pilot study. Mental Retardation, 25, 39-42.
Lavay, B., & McKenzie, T. (1991). Development and evaluation of a systematic run/walk program for men with mental retardation. Education and Training in Mental Retardation, 26, 333-341.
Lavay, B., Reid, G., & Cressler-Chaviz, M. (1990). Measuring the cardiovascular endur- ance of persons with mental retardation: A critical review. In K.B. Pandolf (Ed.), Exercise andsports sciences reviews (Vol. 18) (pp. 263-290). Baltimore: Williams & Wilkins.
Lavay, B., Zody, J., Solko, C., & Era, K. (1990). Effect of a 7-month runlwalk program on the physiological fitness parameters of adults with mental retardation. In G. Doll-Tepper, C . Dahms, B. Doll, & H.v. Selzam (Eds.), Adaptedphysical activity: An interdisciplinary approach (pp. 289-298). Berlin: Springer-Verlag.
Leatt, P., Hattin, H., West, C., & Shephard, R.J. (1988). Seven year follow-up of employee fitness program. Canadian Journal of Public Health, 79, 20-25.
Maurer, J.F., Hussey, C., & Schofield, L.J. (1976). Physical education training for adult retardates in a sheltered workshop setting. Journal of Clinical Psychology, 32,701- 705.
Metropolitan Life Insurance Company. (1983). Height and weight tables: How to appron'- mateframe size and ideal weight. New York: Metropolitan Life Insurance Company.
Montgomery, D.L., Reid, G., & Koziris, L.P. (in press). Reliability and validity of three

Reinforcement Based Exercise 177
cardiovascular fitness tests for mentally handicapped adults. Canadian Journal of Sport Sciences.
Nagle, F.J. (1973). Physiological assessment of maximal performance. Exercise and Sports Science Reviews, 1, 313-338.
Nordgren, B. (1970). Physical capabilities in a group of mentally retarded adults. Scandinavian Journal of Rehabilitation Medicine, 2, 125-132.
Nordgren, B. (1971). Physical capacity and training in a group of young adult mentally retarded persons. ACTA Paediatrica Scandinavica (Suppl.) 2 17, 1 19-1 21.
Nordgren, B., & Backstrom, L. (1971). Correlations between muscular strength and industrial work performance in mentally retarded persons. Acta Paediatrica Scandi- navica (Suppl.) 217, 122-126.
Oliver, J.N. (1958). The effects of physical conditioning exercises and activities on the mental characteristics of educationally sub-normal boys. British Journal of Educational Psychology, 28, 155-165.
Ottenbacher, K. (1986). Evaluating clinical change: Strategies for occupational and physical therapists. Baltimore: Williams & Wilkins.
Pacy, P.J., Webster, J., & Garrow, J.S. (1986). Exercise and obesity. Sports Medicine, 3, 89-113.
Pitetti, K.H., & Campbell, K.D. (1991). Mentally retarded individuals-A population at risk? Medicine and Science in Sports and Exercise, 23, 586-593.
Pitetti, K.H., & Tan, D.M. (1990). Cardiorespiratory responses of mentally retarded adults to air-brake ergometry and treadmill exercise. Archives of Physical Medicine and Rehabilitation, 71, 319-321.
Pitetti, K.H., & Tan, D.M. (1991). Effects of a minimally supervised exercise program for mentally retarded adults. Medicine and Science in Sports and Exercise, 23,594- 601.
Poehlman, E.T., Melby, C.L., & Goran, M.I. (1991). The impact of exercise and diet restriction on daily energy expenditure. Sports Medicine, 11, 78-101.
Polednak, A.P., & Auliffe, J. (1976). Obesity in institutionalized adult mentally retarded populations. Journal of Mental Deficiency Research, 20, 9-15.
Pollock, M.L., Schmidt, D.H., & Jackson, A.S. (1980). Measurement of cardiorespiratory fitness and body composition in the clinical setting. Comprehensive Therapy, 6(9), 12-27.
Pollock, M.L., & Wilmore, J.H. (1990). Exercise in health and disease: Evaliration and prescription for prevention and rehabilitation (2nd ed.). Philadelphia: W.R. Saunders.
Reid, G., Montgomery, D.L., & Seidl, C. (1985). Performance of mentally retarded adults on the Canadian Standardized Test of Fitness. Canadian Journal of Public W~ahh, 76, 187-190.
Rimmer, J.H., & Kelly, L.E. (1991). Effects of a resistance training program on adult8 with mental retardation. Adapted Physical Activity Quarterly, 8, 146-153.
Sage, G.H. (1984). Motor learning and control: A neuropsychological approach. T)u
IA: Wm. C. Brown. Schurrer, R., Weltman, A,, & Brammell, H. (1985). Effects of physical €mi
cardiovascular fitness and behavior patterns of mentally retarded adults. A Journal of Mental Deficiency, 90, 167-169.
Seidl, C., Reid, G., & Montgomery, D.L. (1987). A critique of cardiova testing with mentally retarded persons. Adapted Physical Activity Qua 116.

178 Croce and Horvat
Shellock, F.G., & Prentice, W.E. (1985). Warming-up and stretching for improved physical performance and prevention of sports-related injuries. Sports Medicine, 2,267-278.
Shephard, R.J. (1985). The impact of exercise upon medical costs. Sports Medicine, 2, 133-143.
Shephard, R.J. (1986a). The economic benefits of enhancedfitness. Champaign, IL: Human Kinetics.
Shephard, R.J. (1986b). Fitness in health and industry. Basel: Karger. Shephard, R.J. (1989). Current perspectives on the economics of fitness and sport with
particular reference to worksite programmes. Sports Medicine, 7, 286-309. Shephard, R.J. (1990). The costs and benefits of exercise: An industrial perspective. In
M. Kaneko (Ed.), Fitness for the aged, disabled, and industrial worker (pp. 189- 204). Champaign, IL: Human Kinetics.
Sin, W.E. (1956). The gross composition of the body. Advances in Biological Medical Physics, 4, 239-280.
Skrobak-Kaczynski, J., & Vavik, T. (1980). Physical fitness and trainability of young male patients with Down's syndrome. In K. Berg & B.O. Encksson (Eds.), Children and exercise IX (pp. 300-316). Baltimore: University Park Press.
Solomon, A., & Pangle, R. (1967). Demonstrating physical fitness improvement in the EMR. Exceptional Children, 34, 177-181.
Stainback, S., Stainback, W., Wehman, P., & Spangiers, L. (1983). Acquisition and generalization of physical fitness exercises in the profoundly retarded adults. TASH Journal, 8, 47-55.
Sullivan, S., Chesley, A., Hebert, G., McFaull, S., & Scullion, D. (1988). The validity and reliability of hand-held dynamometry in assessing isometric external rotator performance. Journal of Orthopaedic and Sports Physical Therapy, 10, 2 13-2 17.
Suomi, R., Surburg, P., Lecius, P., & Poppy, W. (1991). The relationship and reliability of isokinetic and isometric measures in mentally retarded men. Unpublished manuscript, Indiana University.
Tomporowski, P.D., & Ellis, N.R. (1984). Effects of exercise on the physical fitness, intelligence, and adaptive behavior of institutionalized mentally retarded adults. Applied Research in Mental Retardation, 5, 329-337.
Tomporowski, P.D., &Ellis, N.R. (1985). The effects of exercise on the health, intelligence, and adaptive behavior of institutionalized severely and profoundly mentally retarded adults: A systematic replication. Applied Research in Mental Retardation, 6,465- 473.
Tomporowski, P.D., & Jameson, L.D. (1985). Effects of a physical fitness training program on the exercise behavior of institutionalized mentally retarded adults. Adapted Physical Activity Quarterly, 2, 197-205.
Walberg, J.L. (1989). Aerobic exercise and resistance weight-training during weight reduction: Implications for obese persons and athletes. Sports Medicine, 6, 343- 456.
Watkinson, E.J., & Wasson, D.L. (1984). The use of single-subject time-series designs in adapted physical education. Adapted Physical Activity Quarterly, 1, 19-29.
Williams, H. (1977). Effect of a physical activity program on the fitness level of a selected group of moderately retarded students (Doctoral dissertation, University of Missouri, Columbia). Dissertation Abstracts International, 36, 1308.
Winnick, J.P. (1979). Early movement experiences and development: Habilitation and rc~mediation. Philadelphia: W.B. Saunders.